Decreased Cerebral Perfusion in Carotid Artery Stenosis, Carotid
date post
15-Jan-2016Category
view
217download
0
Renal Artery Stenosis – The Good, The Bad and The Different
Rick Stouffer MD
University of North Carolina

Disclosure
I will discuss off-label uses No financial conflicts of interest

The ‘classic’ patient for renal artery revascularization
55 year old male HTN, known CAD (prior PCI) Admitted with CP/SOB, BP 194/124 mm Hg BP Rx: ACEI, beta blocker, nitrate Creatinine 1.6 mg/dl, HCT 41.8% Referred for cardiac catheterization

Renal angiography + hemodynamic assessment
AortaAortaAortaAorta
Right renal arteryRight renal arteryRight renal arteryRight renal artery

Renal artery revascularization
• Accelerated HTN
• Mild elevation in creatinine
• Symptoms

Did We Benefit This Patient?

Outline
Types of RAS Atherosclerotic RAS Natural history of the patient with RAS Treatment of RAS

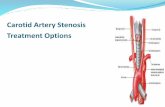
Renal Artery Stenosis
Atherosclerotic (90%) Fibromuscular dysplasia (10%)
– Medial fibroplasia (90%)» classic "string of beads" appearance » middle-to-distal portion of the artery
– Perimedial fibroplasia» focal stenoses
– Intimal/Medial fibroplasia » a focal, concentric stenosis
Aortorenal dissection Vasculitis involving the renal artery (i.e. PAN) AVMs involving the renal artery Irradiation of the renal artery Scleroderma

FMD – Anatomy and Pathophysiology
70 year old female with chest pain and 4-drug hypertension.
Circulation. 2005;112:e278-9.

Before balloon angioplasty After balloon angioplasty

A Cautionary Tale 37-year-old male admitted with headache of six
months duration that had worsened in the last week and was accompanied by blurry vision, dyspnea on exertion and weakness in his legs.
No significant PMH, was not taking any medications and had never been diagnosed with hypertension. No history of alcohol or drug use.
FH - mother with hypertension and a sister with migraine headaches.
Brachial BP was 252/160 mm Hg with no significant difference between arms.

A Cautionary Tale BP = 252/160 mm Hg Ophthamology consultant - Grade IV retinopathy
including marked AV nicking and venous dilatation, cotton wool spots, large areas of choroidal ischemia, delayed vascular filling, blind spots and papilledema in both eyes.
MRI of the brain - No evidence of intracerebral mass but increased signal abnormality within the pons, consistent with hypertensive encephalopathy.
MRI/MRA of the abdomen showed normal kidney size, no renal or adrenal masses and ‘No evidence of renal artery stenosis.’

FMD not visualized on MRI/MRA
Balloon angioplasty with resolution of pressure gradient
J Invasive Cardiol. 2007;19:E31-3.

5 years later - He has run marathons and climbed Mount Kilimanjaro. Home systolic BPs of 130 mm Hg on HCTZ 20 mg daily, enalapril 10 mg daily and Norvasc 10 mg twice daily.

Outline
Types of RAS Atherosclerotic RAS Natural history of the patient with RAS Treatment of RAS

Atherosclerotic RAS
• Usually ostial
• Associated with diseased aorta
• Can be unilateral or bilateral

Prevalence of Atherosclerotic RAS
Unselected autopsies 4-27% Hypertensives 1-4% Aged 65 years and older 6.8% Diabetics 8%
– 6.8% in healthy adults > 65 years old– Evaluation with renal artery duplex of 834 patients consecutive patients who were participants in the Forsyth county cohort of the Cardiovascular Health Study (J Vasc Surg. 2002;36:443–51).

RAS is common in patients with vascular disease
Prevalence of RAS – Proven MI 12%– Undergoing cardiac catheterization 6-19%– Lower extremity PVD 22-59%
Predictors of RAS in patients undergoing cardiac catheterization – CAD; Age; PVD; serum creatinine; hypertension

Traditional Paradigm of Renal Artery Stenosis
Renal Angio(anatomic)
Revascularization
Severe HTN
Physiologic testing for RAS

The Changing Paradigm of Renal Artery Stenosis
Renal Angio(anatomic)
Revascularization
Severe HTN
Physiologic testing for RAS
Evaluation for Vascular Disease
(usually CAD)
Chest pain, dyspnea, etc

Outline
Types of RAS Atherosclerotic RAS - Prevalence and 'Risk factors' Natural history of the patient with RAS Treatment of RAS

A tale of two patients

RAS is a marker of a poor prognosis

Dismal Prognosis Associated with RAS
3 year mortality – 26% in patients treated with stents (Circulation 1998;98:642-647)– 28% in patients managed medically (Mayo Clin Proc 2000;75:437)
4 year mortality– 43% in patients with RAS discovered incidentally at cardiac
catheterization (Kidney International 2001;60:1490-1497)
– 35% in patients with RAS discovered incidentally at cardiac catheterization (JASN 1998;9:252-256)
– 26% in a multi-center study of patients undergoing percutaneous renal revascularization (Circulation 1998;98:642-647)
5 year mortality– 33% in a single-center study of patients undergoing percutaneous
renal artery revascularization (Catheter Cardiovasc Interv. 2007;69:1037)

Ries LAG et al. SEER Cancer Statistics Review, 1973-1998. National Cancer Institute. September 2000.Ries LAG et al. SEER Cancer Statistics Review, 1973-1998. National Cancer Institute. September 2000.
Su
rviv
al
0
20
40
60
80
100
RAS BreastCancer
Colorectal Cancer
Non-HodgkinsLymphoma
Effect of RAS on Prognosis – Relative Five year Survival

Clinical Events in Patients With RAS
J Am Coll Cardiol Intv 2009;2:175-182
Claims data from a 5% random sample of the United States Medicare population were used to select patients without atherosclerotic renovascular disease in the 2 years preceding December 31, 1999 (N= 1,085,250), followed until December 31, 2001.

The $64000 Question
Is RAS a marker of severe atherosclerosis and thus portends a poor prognosis?
or
Does RAS contribute to progression of vascular disease - thus implying that effective treatment may improve clinical outcomes?

Outline
Types of RAS Atherosclerotic RAS Natural history of the patient with RAS Treatment of RAS

Optimal Medical Treatment
ARB + diuretic to get BP to target– <140/90 mm Hg– <130/80 mm Hg with DM
LDL to goal– Currently <100 (or 70) mg/dl
Diabetes Management– HbA1c to target (<7%)
Smoking Cessation Anti-platelet therapy (aspirin
+/- clopidogrel/prasugrel)

What role does revascularization play?

Percutaneous Treatment of RAS
1978 - Gruentzig and colleagues report first balloon angioplasty of renal artery stenosis– Gruentzig A, Kuhlmann U, Vetter W. Treatment of renovascular
hypertension with percutaneous transluminal dilatation of a renal artery stenosis. Lancet 1978; 1:801-802.
Fall 1978 - first renal artery angioplasty in US at UVa. - Patient referred by Carlos Ayers to Charles Tegtmeyer who obtained angioplasty balloon from Gruentzig in exchange for fishing equipment.– Tegtmeyer CJ, Dyer R, Teates CD, Ayers CR, Carey RM,
Wellons HA Jr, Stanton LW. Percutaneous transluminal dilatation of the renal arteries: techniques and results. Radiology 1980; 135(3);589-599

Treatment of RAS
Surgery
PTRA
Stents
EP
1950 1960 1970 1980 1990 2000 2010
Surgery
PTRA
Stents
EP

Evidence-based Medicine

Evidence-based Medicine
Reviewed 55 studies “Almost two thirds of the studies that we reviewed were of
poor methodologic quality; none was deemed to be of good quality.”
“More than half of the studies had limited applicability to patients commonly seen in practice or to modern management strategies.”
“No study directly compared angioplasty with stent placement and "aggressive" medical treatment with currently available antihypertensive, antiplatelet, and lipid-lowering agents.”

Effect of RA Revascularization on HTN
Study Device N Cure Improved Klinge stent 134 10% 68% Lossino stent 153 12% 51% DRASTIC balloon 106 7% 68% Rocha stent 150 6% 50% Dorros stent 145 1% 52%

Effects of RA Revascularization on Ischemic Nephropathy
Prog Cardiovasc Dis 2007;50:136

Angioplasty and STent for Renal Artery Lesions
NEJM 2009;361:1953-1962

ASTRAL Trial
Substantial atherosclerotic RAS
Suitable for endovascular revascularization
Patient's doctor was uncertain that the patient would benefit from revascularization
No revascularisation(n = 403)
Medical treatment according to local protocol
Revascularisation (n = 403)
with angioplasty and/or stent (and medical treatment)

PATIENT CHARACTERISTICS
Revasc. Medical P-value
Mean age (range) 70 (42 – 86) 71 (43 – 88) 0.7
Male 63% 63% 0.9
Current smoker 20% 22% 0.5
Diabetes 31% 29% 0.5
CHD 49% 48% 0.2
PVD 41% 40% 0.7
GFR (ml/min) 40.3
(5.4 – 124.5)
39.8
(7.1 – 121.7)
0.7

Blood Pressure, Cholesterol, Stenosis

Procedural Complications
38 periprocedural complications in 31 of the 359 patients (9%) who underwent revascularization (including 1 of the 24 patients in the medical-therapy group who crossed over to revascularization)
Nineteen of these events (in 17 patients) were considered to be serious complications – Pulmonary edema (1) and Myocardial infarction (1)– Renal embolizations (5), Renal arterial occlusions (4) and Renal-
artery perforations (4)– Femoral-artery aneurysm (1)– Cholesterol embolism leading to peripheral gangrene and
amputation of toes or limbs (3)

Medications at One Year
Revasc. Medical P-value
Any Anti-hypertensives 97% 99% 0.03
Diuretic 64% 69%
Ca2 antagonist 63% 71%
Beta-blocker 46% 55% 0.02
ACE-I, A-II antagonist 50% 43% 0.05
Alpha-blocker 39% 38%
Mean no. anti-hypertensives 2.77 (1 - 6) 2.99 (1 - 6) 0.03

Serum Creatinine

• “An important limitation of our trial concerns the population that we studied. As noted, patients were enrolled in the trial only if their own physician was uncertain as to whether revascularization would provide a worthwhile clinical benefit.”
• Patient selection (single center)– 508 patients with atherosclerotic renovascular disease – Of these, 283 patients had renal-artery stenosis of more than 60%– 71 underwent randomization– 24 underwent revascularization outside the trial
• poorly controlled hypertension• rapidly declining renal function,
– 188 received medical treatment only.

RAS and stenting – has the question been answered?

Criticisms of ASTRAL
1. Selection bias and inexperienced operators ‘On average, 2 patients per center per year underwent
randomization, which indicates serious selection bias or inexperienced staff at centers with very low intervention rates. This concern is supported by a low rate of technical success (317 of 403 patients [79%] in the revascularization group) and a high rate of serious complication in 23 of 280 patients (8%) as compared with reports in the literature of 98% and 2%, respectively.’
NEJM 2010;362:762

Criticisms of ASTRAL
2. There was a reduction in the number of antihypertensive drugs in stent treated patients
‘The study design implies that optimal medical therapy was used to achieve normalized blood pressure in both groups. Thus, not only the blood pressure values but also the number of antihypertensive drugs used to achieve this goal should be taken into account. The … significantly lower number of antihypertensive drugs administered in the revascularization group (P=0.03) preclude the definitive conclusion that renal-artery revascularization provides no clinical benefit.’
NEJM 2010;362:762

Criticisms of ASTRAL
3. Patients with severe RAS were not enrolled ‘The results of the ASTRAL investigation should be read
and interpreted critically. As with the COURAGE (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation) trial, the take-home message should be that for patients with a moderate degree of renal-artery stenosis, medical management is as effective as revascularization over a 5-year follow-up period. Patients seen as requiring anatomical correction were not enrolled; only those deemed suitable for randomization to stenting or medical therapy were included. Thus, the patients most likely to benefit from stenting (those with subocclusive lesions or with very severe disease in one or both kidneys) were not part of this study.’
NEJM 2010;362:762

Criticisms of ASTRAL
4. More concern about high complication rate ‘Another concern is the prohibitively high rate of
amputation and embolization in this study. This calls into question the appropriateness and safety of the techniques currently used to perform the procedure. In more than 200 consecutive cases in which the technique known as "no touch"1 was used (with a guidewire in the aorta preventing the guide catheter from dislodging aortic plaque), I have not seen amputation, limb ischemia, or any evident embolization.’ NEJM 2010;362:762

Criticisms of ASTRAL
5. Were the right patients enrolled? ‘The primary outcome was the change in renal function,
inferred from the reciprocal of the serum level of creatinine. However, serum creatinine is only a rough indicator of the glomerular filtration rate. Furthermore, patients with major indications for revascularization were excluded from the study, whereas patients with either insignificant vascular lesions or advanced renal disease (kidneys 6 cm in length), for whom no benefit from revascularization could be expected, were enrolled. Moreover, intraparenchymal resistance, a relevant predictor of the success of revascularization, was not evaluated.’
NEJM 2010;362:762

Criticisms of ASTRAL
6. Were the patients on the right drugs?
‘only about 40 to 50% of the patients were treated with drugs that block the pathway of the renin–angiotensin–aldosterone system; the use of such drugs is currently recommended in any patient with atherosclerotic renal-artery stenosis.’
NEJM 2010;362:762

Criticisms of ASTRAL
7. Severe RAS was not confirmed prior to entry into the study
‘A major limitation of the ASTRAL trial was its inclusion of patients whose diagnosis of renal artery stenosis was made on the basis of noninvasive imaging alone. No attempt was made to confirm the severity of stenosis with digital subtraction angiography or to assess its functional significance before randomization.’
NEJM 2010;362:762

Criticisms of ASTRAL
8. Not all patients in the intervention group had stenting
‘Furthermore, 17% of the patients in the revascularization group did not proceed to revascularization after invasive angiography.’
NEJM 2010;362:762

“be actuated by that perfect impartiality, which has ever been considered most favorable to correct decisions.”
Abraham Lincoln
Circulation 2007;115;271-276Circulation 2007;115;263-270

• NIH Funded Trial
• Prospective, multi-center, two armed, randomized, unblinded survival (time to event) clinical trial
• To test the hypothesis that optimal medical therapy + stenting reduces the incidence of cardiovascular and renal events compared to optimal medical therapy alone in patients with systolic hypertension
• >100 centers participating
• 1080 patients

Documented history of systolic hypertension (>155 mm Hg) on 2 or more antihypertensive medications One or more renal artery stenosis (> 60% stenosis) All patients receive OMT - Randomization to stent vs no stent
Large and with long term follow-up Clinically important outcomes
– Cardiovascular or Renal Death– Stroke– Myocardial Infarction– Hospitalization from CHF– Progressive Renal Insufficiency– Renal Replacement Therapy
All patients receive ‘optimal medical therapy’

Where do we stand now? In the absence of trials showing benefit from
revascularisation over conventional therapy and the significant risk of complications it seems reasonable to restrict procedures to patients who fail medical therapy with:– resistant or poorly-controlled hypertension– recurrent flash pulmonary edema– dialysis-dependent kidney failure resulting from renal artery
stenosis– chronic renal insufficiency and bilateral renal artery stenosis– renal artery stenosis to a solitary functioning kidney.
Agency for Healthcare Research and Quality (AHRQ)
Available at www.guideline.gov

Where do we stand now? In the absence of significant differences in long-term
outcome measures, given the rates of restenosis following simple balloon angioplasty and the complications and costs of surgical intervention, it would seem reasonable to consider angioplasty with stenting as the revascularisation procedure of choice for medically recalcitrant renal artery stenosis. (Level IV evidence)
The above clinical guidelines refer to patients with significant de novo renal artery stenosis (generally more than 50%–80% reduction in luminal diameter). There have been no studies in patients identified with lesser degrees of stenosis. It seems reasonable to offer medical therapy in these individuals, given the natural history of progressive stenosis in atherosclerotic renal disease.
Agency for Healthcare Research and Quality (AHRQ)
Available at www.guideline.gov

Are we asking the wrong question?
Does RAS contribute to progression of vascular disease?
Are there different phases of RAS with potentially different treatments?
Will optimal treatment differ based on patient characteristics?
What constitutes optimal medical therapy? What outcomes should we measure? Is the disease more than just BP and Ang II?

Data from Animal Model of Renal Artery Stenosis
Activation of renin/Ang system
CKD
Unilateral RAS
Ischemic damage to ipsilateral
kidney
Damage to contralateral
kidney
Time

Summary
RAS is an unusual cause of hypertension but a common finding in patients with vascular disease
RAS identifies patients with very poor prognosis and a high risk of cardiovascular events
Revascularization will benefit select patients with RAS but convincing evidence of improved cardiovascular outcomes in most patients is lacking
A better understanding of the pathophysiology of RAS is needed in order to design more effective therapies

RAS – Still much to learn!