Radiologia Para Neumonias

of 12
-
Upload
alejandra-yanez -
Category
Documents
-
view
229 -
download
0
Transcript of Radiologia Para Neumonias
-
7/27/2019 Radiologia Para Neumonias
1/12
European Journal of Radiology 51 (2004) 102113
Radiology of bacterial pneumonia
Jos Vilar, Maria Luisa Domingo, Cristina Soto, Jonathan Cogollos
Radiology Department, Hospital Universitario Doctor Peset, Valencia, Spain
Received 23 February 2004; received in revised form 26 February 2004; accepted 1 March 2004
Abstract
Bacterial pneumonia is commonly encountered in clinical practice. Radiology plays a prominent role in the evaluation of pneumonia. Chest
radiography is the most commonly used imaging tool in pneumonias due to its availability and excellent cost benefit ratio. CT should beused in unresolved cases or when complications of pneumonia are suspected. The main applications of radiology in pneumonia are oriented
to detection, characterisation and follow-up, especially regarding complications. The classical classification of pneumonias into lobar and
bronchial pneumonia has been abandoned for a more clinical classification. Thus, bacterial pneumonias are typified into three main groups:
Community acquired pneumonia (CAD), Aspiration pneumonia and Nosocomial pneumonia (NP).The usual pattern of CAD is that of the
previously called lobar pneumonia; an air-space consolidation limited to one lobe or segment. Nevertheless, the radiographic patterns of CAD
may be variableand are oftenrelated to the causative agent. Aspiration pneumonia generally involves the lower lobeswith bilateral multicentric
opacities. Nosocomial Pneumonia (NP) occurs in hospitalised patients. Theimportance of NP is related to its high mortality and, thus, the need
to obtaina prompt diagnosis. Therole of imaging in NP is limited butdecisive. Themost valuableinformation is when thechestradiographsare
negative and rule out pneumonia. The radiographic patterns of NP are very variable, most commonly showing diffuse multifocal involvement
and pleural effusion. Imaging plays also an important role in the detection and evaluation of complications of bacterial pneumonias. In many
of these cases, especially in hospitalised patients, chest CT must be obtained in order to better depict these associate findings.
2004 Elsevier Ireland Ltd. All rights reserved.
Keywords: Pneumonia; Bacterial pneumonia; Pulmonary CT; Nosocomial pneumonia
1. Introduction
Bacterial pneumonias account for a large percentage of
all pneumonias. They have been classified into three main
groups: lobar pneumonia, bronchopneumonia and acute in-
terstitial pneumonia [1]. Lobar pneumonias are characterised
by confluent areas of focal airspace disease, usually limited
to one lobe or segment. Bronchopneumonia has a multi-
focal distribution with nodules that tend to join producing
air-space consolidations affecting one or more lobes. Acute
interstitial pneumonias are produced by involvement of thebronchial and bronchiolar wall, and of the pulmonary inter-
stitium, and are most commonly caused by viral organisms
and Mycoplasma pneumoniae.
This classic morphologic classification is of limited use-
fulness because the radiographic pattern often cannot be
used to predict the causative organism. The appearance of
new infective organisms, the increasing age of the popula-
tion and the wide use of antibiotics have changed the pat-
Corresponding author.
E-mail address: vilar [email protected] (J. Vilar).
terns of this disease [2]. This is why most authors prefer
to classify pneumonias from the perspective of the mecha-
nism of origin. Thus, we will refer to three main groups of
pneumonias: community acquired pneumonia (CAP), noso-
comial pneumonia (NP) and aspiration pneumonia.
Streptococcus pneumoniae is the most common cause of
CAP while Gram-negative bacteria and Staphylococcus au-
reus are more often responsible for hospital acquired pneu-
monia [2]. Aspiration pneumonias are usually produced by
micro-organisms that colonize the oropharynx which include
Gram-positive cocci, Gram-negative rods, and rarely, anaer-
obic bacteria.
This article will review the most common and some un-
usual radiographic presentations of bacterial pneumonia in
inmunocompetent patients.
2. Imaging pneumonia
In patients with suspected pneumonia, imaging plays a
major role in the detection, characterisation and follow-up
of the disease.
0720-048X/$ see front matter 2004 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.ejrad.2004.03.010
-
7/27/2019 Radiologia Para Neumonias
2/12
J. Vilar et al. / European Journal of Radiology 51 (2004) 102 113 103
2.1. Detection
The basic and most diffused imaging tool to diagnose
pneumonia remains the chest radiograph. Indeed pulmonary
infections are the most common reason for obtaining an
emergency chest film. Pneumonia may present with a
wide spectrum of symptoms and often the initial clinicalmanifestations are clear. Although the chest radiograph is
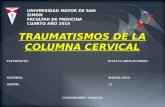
Fig. 1. Additional value of CT: CAP (a) chest radiograph: there is a paratracheal opacity in the right upper lobe. (b) CT of the same patient shows
clearly the opacity due an air-space consolidation.
often regarded as the reference standard for the diagnosis
of community-acquired pneumonia, its reliability is lim-
ited by significant interobserver variability in radiographic
interpretation [3].
Other techniques like computed tomography (CT) can be
useful, showing some infiltrates not visualised in the chest
radiographs (Fig. 1) and can assure the existence of cavita-tion or other complications, [4] but the use of CT is only
-
7/27/2019 Radiologia Para Neumonias
3/12
104 J. Vilar et al. / European Journal of Radiology 51 (2004) 102113
recommended in cases uncertain to the chest film, complica-
tions of pneumonia or suspicion of an underlying additional
lesion such as bronchogenic carcinoma.
Magnetic resonance imaging (MRI) can demonstrate pul-
monary consolidations. It can be used as an alternative to CT
in patients who should not be exposed to ionising radiation.
2.2. Characterisation
Is imaging reliable for distinguishing the infective or-
ganism? Tew et al. [5] reviewed 31 patients with bacte-
rial and non-bacterial pneumonias. The diagnostic accuracy
was 67% for bacterial pneumonia and 65% for non-bacterial
pneumonia. The authors concluded that radiology alone was
unable to distinguish bacterial from non-bacterial pneumo-
nias. In a review of 114 cases of pneumonia, Reittner et al.
concluded that CT is also unable to differentiate the aeti-
ology of various types of pneumonia except Pneumocystis
carinii [6]. The characterisation of some NP may be quite
difficult, especially in patients with assisted ventilation whenother pulmonary conditions may coincide [7]. Despite these
limitations, imaging may be of great help in detecting the as-
sociated findings. A study by Albaum et al. [3] showed that
the chest radiograph reliability for detecting pleural fluid and
multiple infiltrates was good. This is important since both
findings are related to a worse prognosis.
2.3. Follow-up
Most pnemonias will resolve in 1 or 2 weeks. Slow reso-
lution can occur when there are certain associated conditions
such as chronic obstructive pulmonary disease, alcoholism,diabetes and immune-deficiency. Otherwise, if the pneumo-
nia does not resolve, an underlying pathology should be sus-
pected, especially bronchogenic carcinoma. In these cases,
as mentioned previously, CT is recommended [8,9].
3. Community acquired pneumonia (CAP)
The aetiology of CAP varies widely according to the
different reviews published. It is highly influenced by the
geographic area, the population studied and the diagnos-
tic methods used [10]. The most common bacterial agents
responsible for CAP are S. pneumoniae, M. pneumoniae,
Chlamydia pneumoniae and Legionella pneumophila. S.
aureus may complicate a viral pneumonia. CAP may be
caused by Gram-negative organisms in elderly patients,
alcoholics, patients with cardiopulmonary disease and due
to the widespread use of broad-spectrum antibiotics [1].
The incidence of these organisms varies according to the
different authors. Thus, in a study by Lim et al. [11], the
most common agent producing CAP was S. pneumoniae
(48%) followed by virus (19%), C. pneumoniae (13%),
Haemophilus influenzae (20%) and M. pneumoniae (3%),
while another publication [2] reported S. pneumoniae
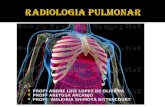
Fig. 2. Community acquired pneumonia (Streptococcus pneumoniae) (a)
and (b): PA and lateral chest films show consolidation in the lateral
segment of the middle lobe, abutting the major and minor fissures.
-
7/27/2019 Radiologia Para Neumonias
4/12
J. Vilar et al. / European Journal of Radiology 51 (2004) 102 113 105
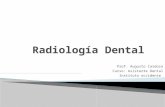
Fig. 3. PA chest radiograph shows an alveolar consolidation involving the right and left lower lobes in a patient infected by Streptococcus pneumoniae.
(920%), M. pneumoniae (1337%) and C. pneumoniae
(17%) as most common agents.
The usual imaging finding in CAP coincides with the clas-
sic presentation of lobar pneumonia: an airspace consolida-
tion in one segment or lobe, limited by the pleural surfaces
(Fig. 2). CT may additionally show ground glass attenua-
tion, centrilobular nodules, bronchial wall thickening and
centrilobular branching structures [4] (Fig. 1b).
Fig. 4. Mycoplasma pneumonia: chest radiograph. There is a diffuse peripheral and bilateral interstitial involvement.
3.1. Pneumococcal pneumonia
S. pneumoniae is the most frequent micro-organism caus-
ing CAP [2,11]. The usual presentation is a lobar pneumo-
nia involving one segment or lobe. Nowadays, the use of
antibiotics has changed the appearance of Pneumoccoccal
pneumonia, and it may appear as patchy confluent areas that
may be multilobar or bilateral (Fig. 3). Kantor [12] found
-
7/27/2019 Radiologia Para Neumonias
5/12
106 J. Vilar et al. / European Journal of Radiology 51 (2004) 102113
Fig. 5. (a) Legionella pneumonia: chest radiograph of a patient with fever, dyspnea and myalgias. There is a smooth bilateral perihilar consolidation. (b)
Chest radiograph obtained 48 h later, notice the rapid extension of the consolidation. (c) and (d) On CT, the consolidations are multiple and bilateral.
-
7/27/2019 Radiologia Para Neumonias
6/12
J. Vilar et al. / European Journal of Radiology 51 (2004) 102 113 107
Fig. 5. (Continued).
-
7/27/2019 Radiologia Para Neumonias
7/12
108 J. Vilar et al. / European Journal of Radiology 51 (2004) 102113
that the patterns of lobar pneumonia and bronchopneumo-
nia were equally frequent in Pneumococcal pneumonia. An-
other common finding in Pneumococcal pneumonia is the
presence of small pleural effusions that are usually reactive.
3.2. Mycoplasma pneumonia
The incidence of Mycoplasma infection is variable ac-
cording to different series and may be influenced by epi-
demics. Every 48 years, the incidence may reach up to
50%. This is a pneumonia of children, adolescents and
adults below 40 years of age [13]. Mycoplasma pneumo-
nia has variable radiographic appearances. In 1975, Putnan
et al. [14] identified two main clinical and radiographic
groups: one group had unilateral or bilateral air-space dis-
ease with a lobar or segmental distribution, while the other
with a longer duration of symptoms, had a diffuse bilateral
reticulo-nodular pattern (Fig. 4). A review of 31 cases of M.
pneumoniae in outpatients revealed no predominant radio-
graphic pattern (interstitial or alveolar) with more frequentinvolvement of the lung bases [15].
3.3. Chlamydia pneumonia
The radiographic appearance ofC. pneumoniae is similar
to that of M. pneumoniae, most commonly as a localised
area of consolidation which may be patchy or homogeneous.
Chlamydia and Mycoplasma often coexist [1].
3.4. Legionella pneumonia
Legionnella pneumophila is responsible for Legionnellapneumonia or Legionnaires disease. These infections are
acquired by breathing droplets of contaminated water. The
disease may be sporadic or may occur in outbreaks, most
frequently in places where the population is exposed to air
conditioning towers, water distribution systems and humid-
ifiers colonised by the germ [16]. The clinical features of
Legionella pneumonia are typical, consisting in diarrhoea,
headache, myalgias, dyspnea and cough. The radiographic
findings are often those of segmental peripheral consolida-
tions that spread rapidly producing opacification of one or
more lobes (Fig. 5). They become bilateral in half of the
cases [17].
3.5. Unusual patterns of CAP
3.5.1. Round pneumonia (Fig. 6)
It was described in children but occasionally it may hap-
pen in adults. In the presence of a pulmonary nodule, round
pneumonia should be suspected especially if no previous
films are available, a rapid growth is observed or there are
signs of infection [18]. A variant of this could be the cases
described in screening for lung cancer where some small
pulmonary nodules detected will disappear after the antibi-
otic treatment [19].
Fig. 6. Round pneumonia: a consolidation is seen in the right lower lobe
lung of this adult patient. Streptococcus pneumoniae was obtained in the
sputum cultures.
3.5.2. Bilateral or multilobar pneumonia
CAP can be diffuse and bilateral in patients with underly-
ing chronic obstructive pulmonary disease due to the distor-
tion and destruction of the pulmonary parenchyma (Fig. 7).
Some of these cases will present as a linear pattern that could
be confused with other aetiologies.
4. Aspiration pneumonia
Aspiration is the inhalation of orofaringeal or gastric con-
tents into the larynx and lower respiratory tract. If the in-halation is of regurgitated sterile gastric contents, aspiration
pneumonitis is caused; and if it is of colonised oropharingeal
material, aspiration pneumonia occurs [20].
Factors that predispose to aspiration pneumonitis are
those that produce disturbance of consciousness such as
drug abuse, seizures, massive cerebrovascular accident, or
the use of anaesthesia. Aspiration pneumonia is conditioned
by neurologic disphagia, anatomic abnormalities of the up-
per aerodigestive tract, gastroesophageal reflux in elderly
persons, or poor oral care.
The radiographic appearance of aspiration pneumonia and
pneumonitis is variable [21] but the most common pattern
is that of bilateral and multicentric opacities, particularlyin the right lung, with a perihilar and basal distribution
(Fig. 8).
5. Nosocomial pneumonias
Nosocomial pneumonia or hospital acquired pneumonia
is defined as a pneumonia occurring 48 h after hospital ad-
mission, excluding any infection that is incubating at the
time of hospital admission, and also a pneumonia which
occurs within 48 h after discharge from the hospital [22].
-
7/27/2019 Radiologia Para Neumonias
8/12
J. Vilar et al. / European Journal of Radiology 51 (2004) 102 113 109
Fig. 7. (a) Chest radiograph of a patient with bullous emphysema. (b) The same patient with pneumonia in the left upper lobe. An airfluid level (arrows)
within the bullae mimics cavitation. (c) CT of this area showing the fluid filled bulla.
Fig. 8. Aspiration pneumonia: chest radiograph of a patient in a comatose
condition due to drug abuse. Bilateral lower lobe consolidations.
According to the literature, the incidence of NP is vari-
able, probably because the groups of patients studied differ
and the diagnostic criteria vary. These variations depend
greatly on the type of hospitalisation and wards (surgical or
medical).
Risk factors involved in NP are the previous condition of
the patient, age, severity of the underlying disease, the length
of hospitalisation and the instrumentation used in invasive
techniques. The most common micro-organisms responsible
for NP are aerobic Gram-negative bacilli (Enterobacteriae,
E. coli, Pseudomona aeruginosa), and some Gram-positive
cocci such as S. aureus and S. pneumoniae. Anaerobic or-
ganisms are less common. Quite often, multiple different
germs are found [23].
In patients hospitalised in Intensive Care Units, these
pneumonias are more frequent, and the mortality is very
high (1050%). Mechanical ventilation constitutes a great
risk factor for NP since it can facilitate the growth and
-
7/27/2019 Radiologia Para Neumonias
9/12
110 J. Vilar et al. / European Journal of Radiology 51 (2004) 102113
Fig. 9. Ventilator assisted pneumonia: chest radiograph of a patient obtained after 5 days of mechanical ventilation. There is a right perihilar consolidation.
Acinetobacter was obtained from bronchoaspirate cultures.
dissemination of germs and the cough mechanism is re-
duced. This has been denominated as ventilator associated
pneumonia (VAP). Nevertheless, NP in the Intensive Care
Units may also occur in non-ventilated patients. Thus NP
has been classified in two groups: ventilator associated
pneumonia and pneumonia in non-ventilated patients [24].The incidence and mortality of the former is much higher
Fig. 10. Nosocomial pneumonia: chest radiograph shows patchy and peripheral areas of consolidation in a hospitalised non-ventilated patient under a
long-term treatment with steroids. The responsible organism was Pseudomona aeruginosa.
than that of NP in non-ventilated patients, and they also
differ in their treatment. Micro-organisms responsible for
VAP vary according to the duration of mechanical venti-
lation: VAP occurring in the first 5 days of ventilation is
usually due to S. pneumoniae, H. influenzae or Moxarella
catarrhalis and uncommonly by anaerobes, while VAP oc-curring after 5 days (Fig. 9) of ventilation is most commonly
-
7/27/2019 Radiologia Para Neumonias
10/12
J. Vilar et al. / European Journal of Radiology 51 (2004) 102 113 111
produced by Pseudomonas aeruginosa, Acitenobacter or
Enterobacter spp., or methicillin-resistant S. aureus [25].
The radiographic pattern of NP may be quite variable
These pneumonias are most commonly bilateral with diffuse
or multiple foci of consolidation not limited to one lobe [7].
They may frequently associate pleural effusion (Fig. 10).
The role of portable chest films in cases of suspected NPis limited, since the presence of focal alveolar consolida-
tions is quite frequent in these patients, and often caused
by atelectasis, pulmonary infarction, oedema or acute res-
piratory distress syndrome (ARDS). The radiographic signs
of NP are non-specific. A study by Wunderink et al. found
that the only reliable sign of pneumonia was the pres-
ence of air bronchograms, except in patients with ARDS
[26]. Atelectasis may solve rapidly, especially after vigor-
ous physiotherapy. In patients with ARDS, the diagnosis
of pneumonia becomes very difficult [27,28]. Generally,
ARDS is bilateral, symmetric and more evident in depen-
dent areas [29].The presence of focal areas of consolidation
favours the diagnosis of pneumonia but asymmetry may alsooccur in ARDS [29]. Additionally, the agreement between
Fig. 11. Hospital acquired pneumonia: pulmonary gangrene produced by
Klebsiella pneumoniae in a hospitalised patient. Notice sloughed lung
tissue due to extensive necrosis in a large cavity with an airfluid level.
readers in this pathology is very low, and other factors such
as the technique used to obtain the chest radiograph and the
ventilator settings may influence the results [30].
In summary, the role of radiology in NP is limited but
decisive. Delay in treating pneumonia may be fatal and
treating with antibiotics other entities (pulmonary infarction,
oedema) may also have negative results. In hospitalized pa-tients, the chest radiographs are most helpful when they are
normal and rule out pneumonia [7]. CT may be of great help
in some cases when the chest films are inconclusive espe-
cially in patients with ARDS.
6. Complications
All pneumonias, CAP and nosocomial may complicate.
Complications are more common in inmunodepressed pa-
tients and in nosocomial pneumonias.
Fig. 12. (a) Chest radiograph of a 12 months old child, with a consolidation
in left lower lobe. (b) Chest radiograph obtained 4 weeks later. A cystic
space has developed in the area of previous pneumonia, corresponding to
a pneumatocele (arrows).
-
7/27/2019 Radiologia Para Neumonias
11/12
112 J. Vilar et al. / European Journal of Radiology 51 (2004) 102113
Cavitation suggests bacterial disease rather than viral or
Mycoplasma infection. S. aureus, Gram-negative, anaerobic
bacteria are the most common agents.
Pulmonary gangrene is a rare but interesting form of
cavitation that produces sloughed lung within a large cav-
ity secondary to thrombosis of the pulmonary vessels
[17]. S. pneumoniae and Klebsiella are the most com-mon agents responsible for cavitation in inmunocompetent
patients and Aspergillus in the inmunocompromised host
(Fig. 11).
Fig. 13. Loefflers pneumonia: (a) the chest radiograph shows an opacity
in the left upper lobe. (b) Lateral chest radiograph showing posterior
displacement of the major fissure due to abundant exudate by Klebsiella
pneumoniae.
Pneumatocele [1] is an air cystic space that may develop as
a complication of acute staphylococcal infection in children
(Fig. 12).
Care needs to be taken to avoid misdiagnosing cavitation
and pneumatocele formation when the focal lucencies within
the consolidation are due to underlying emphysema (Fig. 7).
6.1. Pleural effusion and empyema
Parapneumonic effusions complicate the course of
2060% of patients hospitalised with bacterial pneumo-
nia. Pleural effusion in CAP is less frequent and usually
reactive. Most of these effusions follow an uncomplicated
course and resolve with antibiotic therapy of the underlying
pneumonia. In 510% cases, they become complicated and
progress to empyema [31].
6.2. Lobar enlargement
This sign was well described by Felson et al. in 1949 and
initially attributed to Klebsiella pneumonia (Friedlanders
pneumonia) [32]. Swellling of a lobe occurs when there is
an extensive exudative process. Other infectious processes
such as tuberculosis and pneumococci can also demonstrate
lobar enlargement (Fig. 13).
7. Conclusions
Pneumonias can be classified in three main groups: com-
munity acquired pneumonia, nosocomial pneumonia and
aspiration pneumonia. The role of the radiologist is to bedecisive in their diagnosis and follow-up. The chest radio-
graph remains a basic tool for this purpose. CT is used as a
complement to plain films and especially in the evaluation
of complications or unfavourable resolution of a pulmonary
infiltrate. The role of radiology in the intensive care unit
patient is more limited since there is a great overlap of
pathologies that can have similar radiographic signs. Close
follow-up of these patients and adequate clinical correla-
tion is mandatory. CT in these cases can add significant
information when portable films are inconclusive.
References
[1] Bhalla M, McLoud TC. Pulmonary infections in the normal host.
In: McLoud TC, editor. Thoracic radiology, the requisites. Mosby,
USA; 1998.
[2] American Thoracic Society. Guidelines for the management of adults
with community-acquired pneumonia. Am J Respir Crit Care Med
2001;163(7):173054.
[3] Albaum MN, Hill LC, Murphy M. Interobserver reliability of chest
radiograph in community-acquired pneumonia. Chest 1996;110:343.
[4] Tanaka N, Matsumoto T, Kuramitsu T, et al. High resolution CT
findings in community-acquired pneumonia. J Comput Assist Tomogr
1996;20:6008.
-
7/27/2019 Radiologia Para Neumonias
12/12