Psgn _acute Glomerulonephritis

of 46
-
Upload
dy-hoc-shing -
Category
Documents
-
view
222 -
download
0
Transcript of Psgn _acute Glomerulonephritis
-
8/2/2019 Psgn _acute Glomerulonephritis
1/46
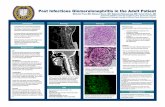
ACUTE
GLOMERULONEPHRITIS
CASE PRESENTATION
-
8/2/2019 Psgn _acute Glomerulonephritis
2/46
General Objective
To present a case of Acute Glomerulonephritis
-
8/2/2019 Psgn _acute Glomerulonephritis
3/46
Specific Objectives
To discuss Acute Glomerulonephritis as todefinition, etiology, epidemiology, andpathophysiology
To generate appropriate differential diagnosis To recognize the typical clinical manifestations
To provide the proper management and
prognosis of the disease
-
8/2/2019 Psgn _acute Glomerulonephritis
4/46
GENERAL DATA
J.R.N., 5 years old, EDS
Roman Catholic
Born on June 18, 2002
1st time admission on March 1, 2008
-
8/2/2019 Psgn _acute Glomerulonephritis
5/46
CHIEF COMPLAINT:
abdominal distention
-
8/2/2019 Psgn _acute Glomerulonephritis
6/46
History of Present Illness
1 month PTA pyodermal lesions on both legs
no asstd signs & symptoms
(-) consult
self-medicated with Penicillin
10 days PTA warm, erythematous, pruritic lesionswere noted on the left leg
No asstd signs & symptoms
(-) consultliniments
9 days PTA lesions spread to trunk and extremities
(+) abdominal painno consult done nor medications
taken
-
8/2/2019 Psgn _acute Glomerulonephritis
7/46
8 days PTA (+) facial and periorbitaledema
(-) changes in urine colorand frequency
self-medicated withDicycloverine 5ml q6
hours x 2 days7 days PTA (+)Facial and periorbital edema -
receding
5 days PTA edema persisted now associated
with abdominal distentionNo consult nor medications
-
8/2/2019 Psgn _acute Glomerulonephritis
8/46
1 day PTA (+) abdominal distention, puffy eyelids andfacial edema
(+) bipedal edema
(-) change in color of the urine
Consult: Fort Magsaysay Station Hospital(-) laboratory examinationsDx: Allergic Reaction
Meds:Chlorphenamine maleate2mg/5ml, 5ml TID
(+) abdominal pain
Few hours PTA persistence of symptomsconsult: private physician
Dx: Acute Glomerulonephritis
Urinalysis
transferred to our institution
admitted
Color AmberTransparency turbid
Reaction 5.0Sp. Gravity 1.015Sugar -Protein +4RBC plentyPus cells 80-90
-
8/2/2019 Psgn _acute Glomerulonephritis
9/46
PRENATAL Hx:
Cognizant at 1 month AOG
regular PNCU at public hospital in CabanatuanCity
regular intake of multivitamins and ferroussulfate
denies any exposure to radiation, infections,
communicable diseases, intake of teratogenicdrugs
-
8/2/2019 Psgn _acute Glomerulonephritis
10/46
NATAL Hx:
born to a 29 y/o G5P5 (5005), FT
delivered via NSD at Fort Magsaysay
BW of 2.7kg
good cry and activity
no fetomaternal complications noted
-
8/2/2019 Psgn _acute Glomerulonephritis
11/46
FEEDING Hx:
Birth 1 mos old pure breastfeeding
1mos 6 mos - BONNA
6mos 16 mos pure breastfeeding
16mos - present Bear brand
weaning - 7 months
solid foods at 10 months
At present - 1 cup of rice per meal and
prefers to eat hotdog, salted fish. Drinks 1-2 glasses of milk formula (Bearbrand) perday
-
8/2/2019 Psgn _acute Glomerulonephritis
12/46
IMMUNIZATION
BCG
OPV3
DPT3 Measles
*local health center
-
8/2/2019 Psgn _acute Glomerulonephritis
13/46
GROWTH AND DEVELOPMENT
Gross motor
- Can ride a tricycle, jump
Fine motor
- Imitate a circle and draw lines, can write name Language
- Can count 1-10, can identify colors
Personal/social
- Plays interactive games, washes and drieshand
-
8/2/2019 Psgn _acute Glomerulonephritis
14/46
PAST MEDICAL Hx
8 mos old admitted for 5 days at PJN(Cabanatuan City) due to Bronchopnuemonia
2-3 episodes of cough and colds a year lasting
for 5-7 days
no allergy to foods and drugs
no childhood diseases noted
-
8/2/2019 Psgn _acute Glomerulonephritis
15/46
FAMILY Hx:
Father- 40 y/o, soldier Mother- 35 y/o, housewife
Siblings
1- 16 y/o, female 2- 14y/o, female
3- 11y/o, female 4- 8y/o, male5- index patient 6- 4y/o, male
(+) DM and (+) HPN maternal grandfather
(+) bladder stone maternal grandfather (+) BA maternal uncle
(+) kidney diseases maternal cousins
(-) malignancy, PTB
-
8/2/2019 Psgn _acute Glomerulonephritis
16/46
PERSONAL AND SOCIAL Hx:
5th of 6 siblings
lives with 8 other household members
bungalow type of house with 3 BR and 2 CR
Mother primary caregiver
Water source - deep well
Garbage - disposed properly
-
8/2/2019 Psgn _acute Glomerulonephritis
17/46
REVIEW OF SYSTEMS:
Constitutional: (-) fever, (-) weakness
HEENT: (-) blurring of vision, (-) sorethroat, (-) nasal obstruction
Respiratory: (-) hemoptysis, (-) shortness
of breath GIT: (-) vomiting, (-) constipation,
(-) diarrhea
GUT: (-) dysuria, (-) urethral discharge NS: (-) headache, (-) LOC, (-) numbness
Extremities: (-) stiffness of joints
-
8/2/2019 Psgn _acute Glomerulonephritis
18/46
PHYSICAL EXAMINATION:
General Survey: conscious, coherent, ambulatory,afebrile, not in distress
Vital Signs:
BP- 150/100 CR- 98 RR- 32 T- 36.80C
Anthropometrics:
Wt 20 kg (p75) IBW 18 kg
Ht 106 cm (p25) IBH 112 cmG - 111% S - 94.6% W - 114.3%
-
8/2/2019 Psgn _acute Glomerulonephritis
19/46
Skin: warm, moist, good skin turgor and elasticity,CRT < 2sec
HEENT: pink palpebral conjunctivae, anictericsclera, intact tympanic membrane AU, no naso-aural discharge, no tonsillopharyngeal
congestion, (+) facial edema, (+) puffy eyelids
Neck: supple, no palpable lymph nodes
-
8/2/2019 Psgn _acute Glomerulonephritis
20/46
Chest/Lungs: symmetrical chest expansion, clear breath
sounds, no retractions, good air entryHeart: adynamic precordium, normal rate, regular
rhythm, no murmur
Abdomen: distended, slit-like umbilicus, AC = 52cm,
soft, non-tender, no organomegaly, (-) fluid waveExtremities: no gross deformities, full and equal pulses,
bipedal edema, (+) healed pyodermal lesions, nocyanosis
-
8/2/2019 Psgn _acute Glomerulonephritis
21/46
ASSESSMENT:
Acute Glomerulonephritis prob Post
Streptococcal Glomerulonephritis
-
8/2/2019 Psgn _acute Glomerulonephritis
22/46
Salient Features:
5 years old, male
History of pyodermal lesions
PE: Abdominal pain and distention
Edema periorbital, bipedal
Slit like umbilicus Hypertension
-
8/2/2019 Psgn _acute Glomerulonephritis
23/46
Laboratory:- Urinalysis
Hematuria (microscopic)
Proteinuria Pyuria
-
8/2/2019 Psgn _acute Glomerulonephritis
24/46
COURSE IN THE WARDS:
Upon admission
Laboratory examinations Urinalysis
C3, ASO CBC
Serum electrolytes BUN, Crea TPAG KUB UTZ
Therapeutics Furosemide 1mkdose
Pen G 100,000 u/kg/day Nifedipine 5mg prn for BP >120/80
Color: dark yellow
Transparency : turbidReaction: 6.0Sp. Gravity: 1.010Sugar: -Protein: +3RBC: 20-30Pus cells: 40-50
ASO negative
Hgb 110Hct 0.33RBC 4.31WBC 19.9Plt count 313S 0.58L 0.28E 0.14
Na 142.9K 5.14
Cl
116.9Crea 40.3
TP 55.5Albumin 26.4Globulin 27.1
-
8/2/2019 Psgn _acute Glomerulonephritis
25/46
1st hospital day
S > with hypertensive episodesabdominal pain
O > conscious, ambulatory
BP 150-120/80-90 CR 80-88 bpm RR 20
cpm Temp 36.5-37.10Cslit like umbilicus, AC = 52cm
bipedal edema
facial edema
A > AGN prob PSGN
P > HL
Meds: Pen G 100,000u/kg/day
Furosemide q12H
-
8/2/2019 Psgn _acute Glomerulonephritis
26/46
2nd hospital day
S/O > (+) facial and bipedal edema - receding
(-) abdominal pain
BP 110-130/70-100
AC = 51 cm (52cm)Adequate urine output (1.6 cc/kg/hr)
A > AGN prob PSGN
P > Oral fluid intake limited to 190ml qshift
Furosemide 1mkdose q12 hours
Pen G continued
-
8/2/2019 Psgn _acute Glomerulonephritis
27/46
3rd hospital day
S/O > (+) episodes of hypertension
(-) facial edema
(-) bipedal edema
AC = 46cm (51)
A > AGN prob PSGN
P > Nifedipine was discontinued
Furosemide q8H shifted to q6Hwith BP precautions
-
8/2/2019 Psgn _acute Glomerulonephritis
28/46
5th hospital day
S/O > (-) edema
(-) hypertensive episodes
adequate urine output
A > PSGNP > For repeat urinalysis
Furosemide to q8hrs
Pen G D5
Color AmberTransparency turbid
Reaction 6.0Sp. Gravity 1.015
Sugar -Protein -
RBC TNTCPus cells 0-2
C3 430mg/L
-
8/2/2019 Psgn _acute Glomerulonephritis
29/46
6th hospital day
S/O > (-) hypertensive episodes
(-) edema
(-) abdominal pain
A > PSGNP > Pen G IV shifted to Sumapen
250mg/5ml, 6.5 ml q6H
referral to Pedia Nephrologist
(Furosemide q8H then taper)
-
8/2/2019 Psgn _acute Glomerulonephritis
30/46
9th hospital day
S/O > AC = 45cm
wt = 16.2 kg
adequate urine output
stable vital signs
A > PSGNP > Furosemide discontinued
Home meds:
Sumapen 250mg/5ml,6.5 ml q6H x 4 days
MV syrup, 1 tsp OD
KUB UTZ (3/12/08)
-
8/2/2019 Psgn _acute Glomerulonephritis
31/46
Final Diagnosis:
Post Streptococcal Glomerulonephritis
-
8/2/2019 Psgn _acute Glomerulonephritis
32/46
DISCUSSION
-
8/2/2019 Psgn _acute Glomerulonephritis
33/46
ACUTE GLOMERULONEPHRITIS
- Usually signifies an inflammatory processcausing renal dysfunction over days to weeks
that may or may not resolve
Currents, 2003
-
8/2/2019 Psgn _acute Glomerulonephritis
34/46
Sudden onset of gross hematuria, edema,hypertension, and renal insufficiency
One of the most common glomerular causes of
gross hematuria in children
Nelsons, 17th ed
-
8/2/2019 Psgn _acute Glomerulonephritis
35/46
Etiology
Streptococcal pharyngitis (serotype 12) coldweather months
Streptococcal skin infections or pyoderma
(serotype 49) warm weather months
Textbook of Pediatrics and Child Health, 4th ed
-
8/2/2019 Psgn _acute Glomerulonephritis
36/46
Epidemiology
Post -infectious type most common
most common in males (1.7 -2:1) ages 6 to 10 butcan occur at any age
Handbook of Diseases, Copyright 2003
Pathophysiology
-
8/2/2019 Psgn _acute Glomerulonephritis
37/46
Pathophysiology
pyodermal lesions
Ag-Ab complex
Ag-Ab complement complex
Autoimmune/inflam rxn in glomerulus
Na, water balance
ECF expansion
DIURETIC PHASE
CONVALESCENT PHASE
Edema, HPN, CHF
decrease C3
OLIGURIC PHASEInc ASO, antistreptokinase
-
8/2/2019 Psgn _acute Glomerulonephritis
38/46
Clinical Manifestations
Hematuria Proteinuria
Edema
Hypertension
Oliguria
Nonspecific symptoms
Abdominal pain
Malaise
Fever
-
8/2/2019 Psgn _acute Glomerulonephritis
39/46
Stages
- typical course lasts 7-10 days for each ofthe 3 phases
Oliguric phase acute salt and wateroverload
Diuretic phase BP normalizes
Convalescent phase
-
8/2/2019 Psgn _acute Glomerulonephritis
40/46
Diagnosis
Urinalysis
CBC
Blood chemistries
C3, ASO
Renal biopsy
-
8/2/2019 Psgn _acute Glomerulonephritis
41/46
Complications
Acute Renal Failure
Hypertensive encephalopathy
Congestive Heart failure
-
8/2/2019 Psgn _acute Glomerulonephritis
42/46
Treatment
Supportive
Diet low Na, low protein
Activity
Medications
Antibiotic Penicillin, Erythromycin
Anti-hypertensive drugs Furosemide,vasodilators, ACEI
-
8/2/2019 Psgn _acute Glomerulonephritis
43/46
Prognosis
More than 95% of affected children eventuallyrecover totally with conservative therapy aimedat maintaining sodium and water balance.
Robbins, Pathologic Dses, 6th ed
-
8/2/2019 Psgn _acute Glomerulonephritis
44/46
Follow-up Care
Proper education about patients condition
Ff-up every 2 weeks with urinalysis result
8-10 weeks after onset C3 determination
12 mos after onset serum Crea in normal level
-
8/2/2019 Psgn _acute Glomerulonephritis
45/46
SUMMARY
-
8/2/2019 Psgn _acute Glomerulonephritis
46/46
Thank You!