Pathogenesis of Glomerulonephritis
68
PATHOGENESIS OF GLOMERULONEPHRITIS ADETUNJI TA
-
Upload
adetunji-adesegun -
Category
Documents
-
view
149 -
download
9
Transcript of Pathogenesis of Glomerulonephritis

PATHOGENESIS OF GLOMERULONEPHRITIS
ADETUNJI TA

OUTLINE
• INTRODUCTION• EPIDEMIOLOGY• RELEVANT ANATOMY• DEFINITION OF TERMS• CLASSIFICATION• PATHOGENESIS• HISTOLOGY• MANAGEMENT• CONCLUSION

INTRODUCTION
• GN can be defined as a spectrum of renal diseases
of varied etiology and clinical presentations that are
characterized by clinical and histological evidence of
glomerular damage.
•Note that despite the “itis” in GN, inflammation per se
may not feature in many GNs. Associated terms include:
•Glomerulonephritides
•Glomerulopathy
•Nephritis
GLO
ME
RU
LON
EP
HR
ITID
ES
– The pathophysiology
GLO
ME
RU
LON
EP
HR
ITID
ES
– The pathophysiology
INTRODUCTION
The term Glomerulonephritis and Glomerulopathy are
usually used interchangeably to denote glomerular injury,
although some authorities reserve the former term for injury
with evidence of inflammation such as leucocyte infiltration,
antibody deposition, and complement activation
•It encompasses a group of disorders with wide-ranging
clinical presentations,severity,causes and
immunopathogenetic mechanisms
•GN is an important cause of both acute and chronic
kidney Disease worldwide.

STRUCTURE OF THE KIDNEY
•The functioning unit of the kidney is the nephron
•Each kidney has about one million nephrons
•The number of nephrons is established during prenatal
development.
•After birth, no new nephron can develop and a lost
nephron cannot be replaced.

Gross Anatomy • KIDNEYS– Paired organ– Each weigh 120 – 200g
– Dimensions: 10 – 12 cm vertically, 5 -7 cm transversely, and 3 cm anteroposteriorly.
– The outer surface can be divided into anterior side, dorsal side, upper pole and lower pole
– The lateral surface is convex.
– The medial surface is concave, deeply grooved (renal sinus) and forms the renal hilum
– The ureter/renal pelvis, renal artery, renal vein, lymphatic vessels and nerves enter or exit through the renal hilum the kidney.

GENERAL ARCHITECTURE OF THE KIDNEY
•Kidney
–Outer cortex
–Inner medulla
•Vasculature
–the arterial system
–Venous system
–the resistance vessels
•THE GLOMERULUS
•Structural characteristics of the
glomerular capillary wall
–the endothelial cell
–the glomerular visceral epithelial cell
–the mesangial cell
–the extracellular matrix: basement
membrane, (GBM’s and mesangial matrix)
•Filtration depends on
–Hydrostatic pressure difference
–Size of the molecule
–Charge on the molecule
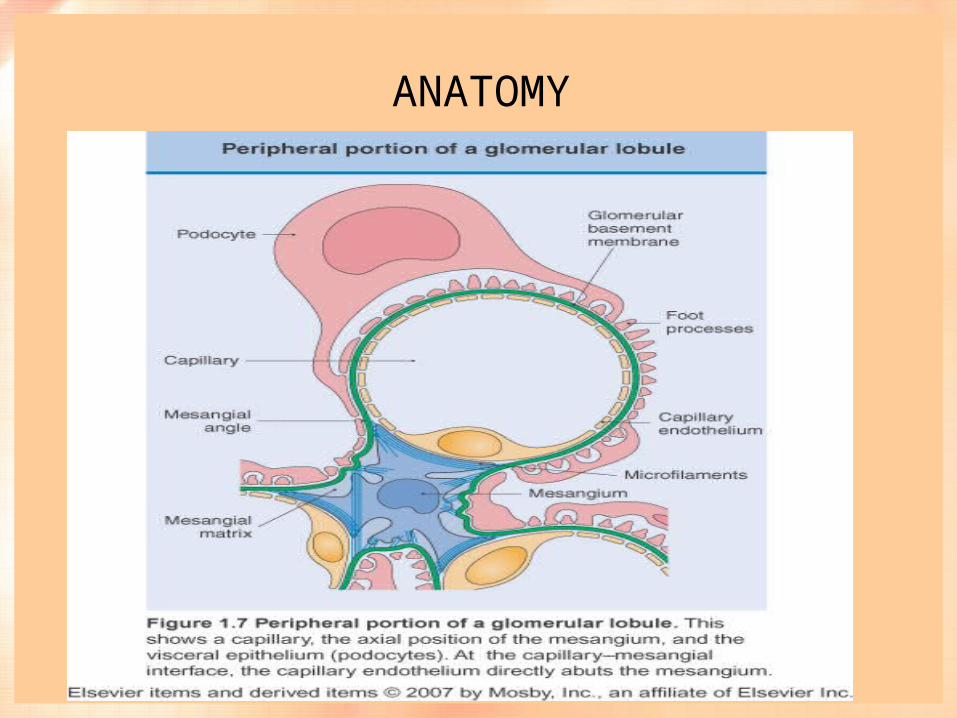
ANATOMY

EPIDEMIOLOGY
•GN is recognized as the second commonest cause of
CKD worldwide.
•In developed countries, it is still the 3rd commonest
cause of ESRD in many countries.
•In developing countries, it ranks 2nd or 1st
•For every patient with clinically apparent GN receiving
medical care, an estimated additional 5 to 10 patients have
undiagnosed sub-clinical disease.

EPIDEMIOLOGY ... NIGERIA
•GN is more common in the male than in the female
population 1.4 : 1
•Peak incidence for AGN is usually October – January
( Etuk et al)
•Case average of 7.5/year calabar - to 14.5/year in
UPTH.
•GN is the commonest cause of CKD in Nigeria from
available reports
GLOSSARY OF DESCRIPTIVE TERMS
•All glomeruli
–Diffuse: Involving ≥ 50% of the glomeruli
–Focal: Involving <50% of glomeruli
•Individual glomerulus
–Global: if all or almost all of the glomerular tuft are
involved
–Segmental: if only part of the glomerulus is involved.
GLOSSARY OF DESCRIPTIVE TERMS
•Sclerosis refers to an increase in the amount of
homogenous non-fibrillar extracellular material of similar
composition to GBM and mesangial matrix.
•Fibrosis refers to deposition of collagen type I and III
and is more commonly a consequence of healing of
crescents or tubulointerstitial inflammation.

GLOSSARY OF DESCRIPTIVE TERMS
•Proliferative is used to describe an increase in glomerular cell
number, which can be either
–true proliferation of resident glomerular cells or
–glomerular hypercellularity caused by infiltration of
leucocytes.
•Proliferation of resident glomerular cells is classified as
– intracapillary or endocapillary when referring to
endothelial or mesangial cells and
–extracapillary when referring to cells in Bowman’s space.

GLOSSARY OF DESCRIPTIVE TERMS
•A crescent is a half-moon-shaped collection of cells in
Bowman’s space, usually composed of proliferating parietal
epithelial cells and infiltrating macrophages.
•Because crescentic GN is often associated with renal
failure that progresses rapidly over weeks to months, the
clinical term rapidly progressive GN and the pathologic
term crescentic GN are often used interchangeably.

GLOSSARY OF DESCRIPTIVE TERMS
•Sub-epithelial – Located between the glomerular
basement membrane and the podocytes.
•Intra-membranous – within the basement membrane
•Sub-endothelial - Between the glomerular basement
membrane and the endothelium
•Mesangial – within the mesangium

CLASSIFICATION ACCORDING TO AETIOLOGY
•Primary: idiopathic but usually immune mediated
•Secondary: there is a known cause

CLASSIFICATION ACCORDING TO CELLULAR RESPONSE/APPEARANCE OF
THE GLOMERULAR TUFT
•Non-proliferative
•Proliferative

CLASSIFICATION ACCORDING TO HISTOLOGIC PATTERN
•Focal segmental
•Diffuse
•MCD
•Membranous
•Menbranousproliferative

CLASSIFICATION OF ACCORDING TO DURATION OF DISEASE
•Acute GN refers to glomerular injury occurring over
days to weeks.
•Sub-acute or rapidly progressive GN refers to
glomerular injury occurring over weeks or a few months.
•Chronic GN refers to glomerular injury occurring over
months or years.

CLASSIFICATION BASED ON IMMUNOFLUORESCENCE
•Immune
•Pauci immune

GN….BASIC DIVISION
•Non- Proliferative
•Minimal change
•Membranous
•FSGS
•Diabetes
•Amyloidosis
•Proliferative
•Diffuse proliferative
•(crescents)
•Mesangiocapillary
•Focal and segmental
proliferative.
All these are Histological patterns and NOT a diagnosis

PATHOGENESIS OF GLOMERULAR INJURY
•Pathogenesis of glomerular injury involves a complex interplay between
•Genetic factors eg congenital Nephrotic syndrome
•Acquired: Immune and Non—immune Factors
Immune Mechanisms
–Cellular immunity
–Humoral immunity
–Complement system/cascade
–Coagulation cascade
–Soluble factors
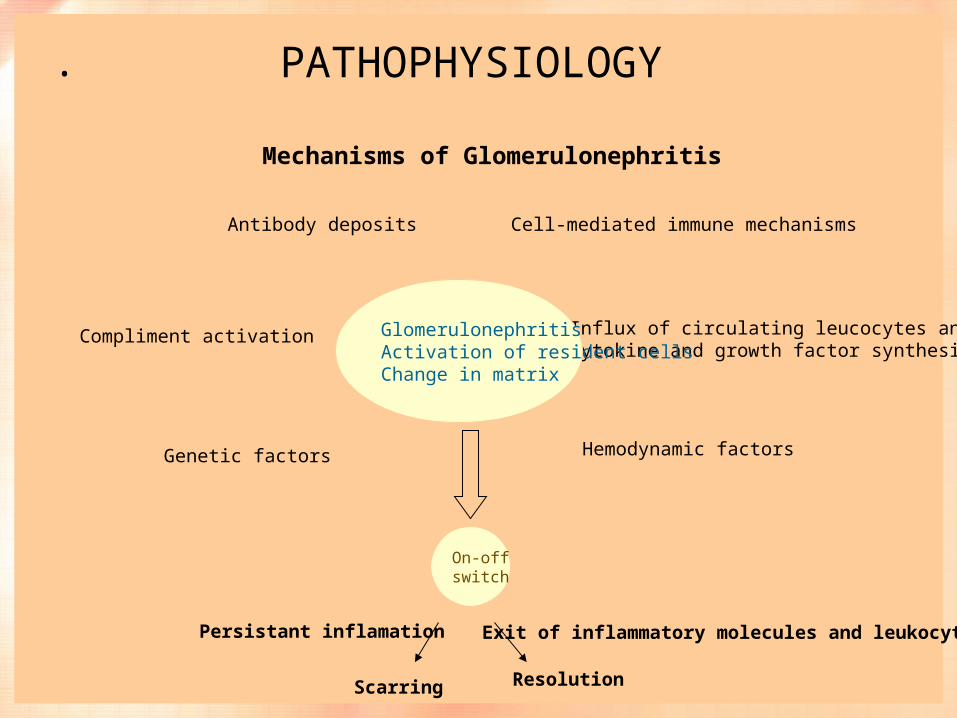
Mechanisms of Glomerulonephritis
Cell-mediated immune mechanismsAntibody deposits
Compliment activation Influx of circulating leucocytes and cytokine and growth factor synthesis
GlomerulonephritisActivation of resident cellsChange in matrix
On-offswitch
Scarring Resolution
Persistant inflamation Exit of inflammatory molecules and leukocytes
Genetic factors Hemodynamic factors
PATHOPHYSIOLOGY.

PATHOPHYSIOLOGY….schematics

Genetic Factors
• Congenital Nephrotic Syndrome - Mutations in nephrin- Mutation in podocin- Mutation in alpha Actinin 4• Alport Syndrome• Thin basement membrane Disease

Immune Factors
•Central to the pathogenesis GN is inflammation which
is often immune mediated.
•Glomeruli have three properties that make them
vulnerable to immunological attack:
–they “filter” and trap immune complexes
–they contain immunologically competent cells capable
of processing antigen
–they have structures like the GBM and mesangial cells
which can act as “targets” for antibodies

Circulating Immune Complex
• In conditions such as - SLE- HBV Infection- Malaria P. Falciparum and Malariae- Syphillis- Strptococcal infection• Deposition of immune complexes in the glomerulus
which leads to complement activation, leucocytes recruitment, coagulation cascade activation and inflammation ensues

In-Situ Immune Complexes• Seen in Anti-GBM Ab GN• Ab directed to fixed antigens on the GBM• Ab may also react in situ with previously planted non-
glomerular antigens such as DNA, IgG, bacterial products• Ab deposition shows a linear pattern while planted antigens
induce a granular pattern of immunoglobulin deposition on immunoflorescence
• Ant-GBM can also cross react with alveolar basement membrane leading to simultaneous kidney/lung lesions as obtained in GoodPasture Syndrome.
• Α3 chain of type IV collagen is the target antigen in anti-GBM disease (Goodpasture’s syndrome

Cell mediated Immune GN
•Cell-mediated immune mechanisms
•A direct role of T cells in mediating proteinuria and
crescent formation been suggested
•T cells sensitized to endogenous or exogenous antigen
present in the glomeruli recruit macrophages, resulting in a
local delayed type hypersensitivity reaction.
•There maybe no ab or immune complex deposition and
and when present may not correlate with disease severity.

Mediators Of Immune Injury
•Main pathway of Ab-mediated injury is complement-leucocyte mediated
•Acute injury: Predominant infiltrating cells are neutrophils and monocytes
•Chronic injury:Predominant cells are monocytes/macrophages and T cells.
•The primary mechanism for attracting these cells is the secretion of chemokines and the expression of leucocyte adhesion molecules by local endothelial and resident cells;
•Local release of complement activation fragments (C5a) is very crucial(Chemotactic agent)

Soluble Factors
•Soluble factors play a role in the pathogenesis of glomerular
disease.
•Examples of soluble factors are; cytokines, chemokines,
growth factors vasoactive mediators, reactive oxygen
species, proteases, proteins in the coagulation cascade
•These factors
–promote recruitment and activation of inflammatory cells,
–activate resident glomerular cells,
–directly cause tissue injury,
–stimulate production of matrix proteins (which forms the
basis of scarring).

Non-immune Factors
• Podocyte Injury• Nephron Loss
- Any renal condition causing significant nephron destruction and reduced GFR
- Adaptive changes in the kidney such as hypertrophy to remain renal fxn occurs
- Associated maladaptive haemodynamic changes utimately perpertutes renal damage and a vicious cycle ensues

PATHOPHYSIOLOGY… minimal change dxs


VARIANT OF FSGS

PATHOPHYSIOLOGY…MEMBRANOUS NEPHROPATHY

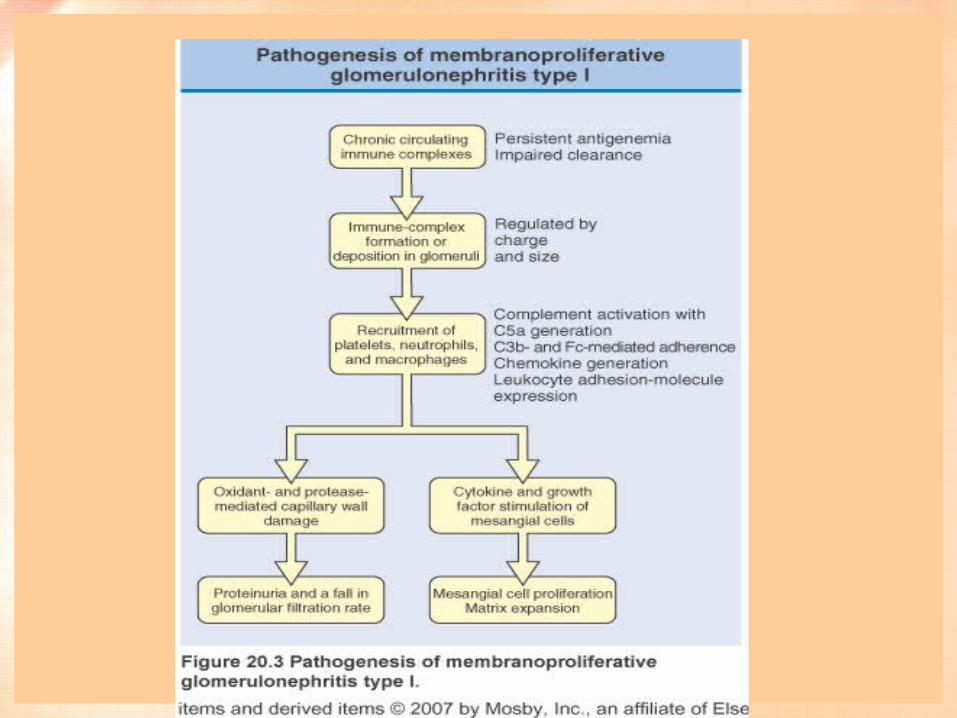
PATHOPHYSIOLOGY… MEMBRANOPROLIFERATIVE

PATHOPHYSIOLOGY…. GOODPASTURE DISEASE

LIGHT MICROGRAPH OF A NORMAL GLOMERULUS.
There are only 1 or 2 cells per capillary tuft, the capillary lumens are open, the thickness of the glomerular capillary wall (long arrow) is similar to that of the tubular basement membranes (short arrow), and the mesangial cells and mesangial matrix are located in the central or stalk regions of the tuft (arrows).

HISTOLOGY ....MESANGIAL PROLIFERATIVE
Normal glomerulusMesangial proliferative

HISTOLOGY ....MESANGIAL PROLIFERATIVE
•Normal •Mesangial proliferative
Light micrograph in membranoproliferative glomerulonephritis showing a lobular appearance of the glomerular tuft with focal areas of increased glomerular cellularity (large arrows), mesangial expansion (*), narrowing of the capillary lumens, and diffuse thickening of the glomerular capillary walls (small arrows).

HISTOLOGY .... DIFFUSE
•Normal glomerulus Diffuse endocapillary hypercellularity:
post-streptococcal GN

HISTOLOGY ....MEMRANOUS NEPHROPATHY

HISTOLOGY ..... FOCAL SEGMENTAL GLOMERULOSCLEROSIS

HISTOLOGY... FOCAL SEGMENTAL GLOMERULOSCLEROSIS

HISTOLOGY... SCLEROSED GLOMERULAR TUFTS

PATHOGENESIS – CHRONIC PROGRESSIVE PHASE
•Renal damage in the chronic-progressive phase of GN
is mediated by non-immune mechanisms that develop as a
result of loss of filtering-surface with accompanying
increases in glomerular pressures in remaining nephrons.
•These features lead to glomerular sclerosis as well as
to chronic interstitial fibrosis, which is a consequence of
multiple injurious events including ischaemia, glomerular
cytokine release, and toxic effects of increased protein
filtration on tubules
MGT:HISTORY
•Family history of kidney disease and hearing difficulties
(Alport syndrome)
•Medication e.g NSAID’s ACEI, penicillamine, gold,
mercury in some skin lightening creams.
•Recent throat infection PSGN or Viral Wegener’s
granulomatosis, IgA.
•Cancer - Solid tumors, Hodgkin’s (minimal change) or
non Hodgkin’s (MPGN)

PHYSICAL EXAMINATION
•Inspection – appearance, colour, pitting oedema,
xanthelasma, alopecia, facial rash, purpura, clubbing,
livedo reticularis
•Palpation – pulse, hepatomegaly, palpable kidneys,
splenomegaly, palapable bladder
•Percussion – hepatomegaly, splenomegaly
•Auscultation – renal artery bruits, other bruits, cardiac
lesions, hypertension,

CLINICAL FEATURES OF GN

CLINICAL FEATURES OF GN
• .

.

Useful Blood Tests in Investigations of Glomerular Disease
• FBC – High white cell count in vasculitis, infections.
• E &U,Cr – assesses severity of renal impairment
• Total serum protein, albumin – Low in those with nephrotic syndrome
• Immunoglobulins – High in vasculitis, SLE
• Complement
• Low C3, normal C4 in MPGN (type II) and sometimes SLE.
• high C3, C4 in systemic vasculitis
• Antiglomerular BM antibody – Goodpasture’s disease
• Anti-dsDNA antibodies – SLE
• C3 nephritic factor – MPGN (type II)

Investigations…• Urinalysis
• Urine Microscopy for cellular elements and casts
• 24 hr urinary protein estimation
• Creatinine clearance or estimated GFR
• Renal ultrasound
• HBsAg, anti-HCV, HIV
• ANCA (antineutrophil cytoplasmic antibodies)
• Renal Biopsy
– Light microscopy
– Electron microscopy
– Immunofluorescence



Treatment
•Control of blood pressure
–ACE inhibitors ± ARBs
–Other anti-hypertensives
•Blood pressure goal < 125 / 75 mm Hg if proteinuria is > 1 g /day and < 130 /
80mmHg if proteinuria is < 1 g / day.
•Corticosteroids
–Are effective in several types of GN owing to their ability to inhibit activity of the
transcription factor nuclear factor ĸB and consequently inhibit the proinflammatory effects of
cytokines known to promote glomerular inflammation actively, including interleukin 1β and
tumour necrosis factor α.
–Are useful in several types of GN
•Lipid lowering agents e.g. statins

TREATMENT
•Corticosteroids
•Inhibits activity of the transcription nuclear factors kB and
consequently inhibit the pro-inflammatory effects of cytokines, known
to promote glomerular inflammatory actively, including IL-Iβ and TNFα
•Immunosuppressive therapies – crescentic GN, proliferative GN,
FSGS, MCD, MN, IgAN with deteriorating renal function and
proteinuria.
•Plasmapheresis – removal of preformed antibodies from the
circulation – Goodpasture’s disease

TREATMENT
•Immunosuppressives e.g. cyclophosphamide,
azathioprine, chlorambucil, mycophenolate mofetil,
sirolimus
–Are of proven benefit in crescentic GN, proliferative
lupus nephritis, focal and segmental glomerulosclerosis,
minimal change disease, membranous nephropathy, and in
cases of IgA nephropathy with deteriorating renal function
and proteinuria.





Conclusion
• Glomerulonephritis refers to a spectrum of aetiopathogenesis and varied clinical presentations following glomerular damage
• Results from complex interplay of genetic, immunologic and environmental factors
• Histologic difference abound depending mostly on aetiology
• May result in Acute or Chronic kidney disease
• Leading cause of CKD worldwide, commonest Cause in Nigeria and Sub-Sahara Africa
• Management requires early recognition by meticulous hx taking, examination and appropriate investigation
• Some would require Steroid +/- Immunosuppressants

References
• Basic Pathology By Robins, 8th ed• Harrison’s Principles of Internal Medicine By Longo et al,
18th ed• WACP Revision Course, 2011• www.pubmed.gov

THANK YOU