Prevención de la enfermedad perinatal por Streptococcus agalactiae

of 36
-
Upload
lilianagomezgamboa -
Category
Documents
-
view
224 -
download
0
Transcript of Prevención de la enfermedad perinatal por Streptococcus agalactiae
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
1/36
department of health and human services
Centers for Disease Control and Prevention
Recommendations and Reports November 19, 2010 / Vol. 59 / No. RR-10
Morbidity and Mortality Weekly Reportwww.cdc.gov/mmwr
Prevei Periaal Grup B
Srepcccal DiseaseRevised Guidelies rm CDC, 2010
Continuing Education Examination available athttp://www.cdc.gov/mmwr/cme/conted.html
http://www.cdc.gov/mmwrhttp://www.cdc.gov/mmwr/cme/conted.htmlhttp://www.cdc.gov/mmwr/cme/conted.htmlhttp://www.cdc.gov/mmwr -
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
2/36
MMWR
Te MMWR series o publications is published by the Oce oSurveillance, Epidemiology, and Laboratory Services, Centers orDisease Control and Prevention (CDC), U.S. Department o Healthand Human Services, Atlanta, GA 30333.
Suggested Citation: Centers or Disease Control and Prevention.[itle]. MMWR 2010;59(No. RR-#):[inclusive page numbers].
Ceers r Disease Crl ad PreveiTomas R. Frieden, MD, MPH
Director
Harold W. Jae, MD, MAAssociate Director or Science
James W. Stephens, PhDOce o the Associate Director or Science
Stephen B. Tacker, MD, MScDeputy Director or
Surveillance, Epidemiology, and Laboratory Services
Stephanie Zaza, MD, MPH
Director, Epidemiology Analysis and Program Oce
Edirial ad Prduci SaRonald L. Moolenaar, MD, MPH
Editor, MMWRSeries
Christine G. Casey, MDDeputy Editor, MMWRSeries
eresa F. RutledgeManaging Editor, MMWRSeries
David C. JohnsonLead echnical Writer-Editor
Jerey D. Sokolow, MAProject Editor
Martha F. BoydLead Visual Inormation Specialist
Malbea A. LaPete
Stephen R. Spriggserraye M. StarrVisual Inormation Specialists
Quang M. Doan, MBAPhyllis H. King
Inormation echnology Specialists
Edirial BardWilliam L. Roper, MD, MPH, Chapel Hill, NC, Chairman
Virginia A. Caine, MD, Indianapolis, INJonathan E. Fielding, MD, MPH, MBA, Los Angeles, CA
David W. Fleming, MD, Seattle, WAWilliam E. Halperin, MD, DrPH, MPH, Newark, NJ
King K. Holmes, MD, PhD, Seattle, WADeborah Holtzman, PhD, Atlanta, GA
John K. Iglehart, Bethesda, MDDennis G. Maki, MD, Madison, WIPatricia Quinlisk, MD, MPH, Des Moines, IA
Patrick L. Remington, MD, MPH, Madison, WIBarbara K. Rimer, DrPH, Chapel Hill, NCJohn V. Rullan, MD, MPH, San Juan, PR
William Schaner, MD, Nashville, NAnne Schuchat, MD, Atlanta, GA
Dixie E. Snider, MD, MPH, Atlanta, GAJohn W. Ward, MD, Atlanta, GA
ContEntS
Introduction .............................................................................. 1
Methods ................................................................................... 2
Invasive Group B Streptococcal Disease ...................................... 3
Prevention o Early-Onset Group B Streptococcal Disease ............. 4
Identifcation o Candidates or Intrapartum Antibiotic Prophylaxis .. 6Specimen Collection and Processing or GBS Screening ............... 7
Secondary Prevention o Early-Onset GBS Among Inants .......... 10
Implementation and Impact o GBS Prevention Eorts ................. 11
Recommendations ................................................................... 14
Future o GBS Prevention ......................................................... 23
Reerences .............................................................................. 23
Disclsure Relaiship
CDC, our planners, and our content experts wish to disclose they haveno nancial interests or other relationships with the manuacturers ocommercial products, suppliers o commercial services, or commerciasupporters. Presentations will not include any discussion o the unla-beled use o a product or a product under investigational use.
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
3/36
Vol. 59 / RR-10 Recommendations and Reports 1
Te material in this report originated in the National Center orImmunization and Respiratory Diseases, Anne Schuchat, MD, Director,and the Division o Bacterial Diseases, Rana Hajjeh, MD, Director.Corresponding preparer: Jennier R. Verani, MD, National Centeror Immunization and Respiratory Diseases, CDC, 1600 Cliton Road,N.E., MS C-23, Atlanta, GA 30333. elephone: 404-639-8652; Fax:404-639-3970; E-mail:[email protected].
Prevei Periaal Grup B Srepcccal Disease
Revised Guidelies rm CDC, 2010Prepared by
Jennier R. Verani, MDLesley McGee, PhD
Stephanie J. Schrag, DPhilDivision o Bacterial Diseases, National Center or Immunization and Respiratory Diseases
Summary
Despite substantial progress in prevention o perinatal group B streptococcal (GBS) disease since the 1990s, GBS remains theleading cause o early-onset neonatal sepsis in the United States. In 1996, CDC, in collaboration with relevant proessional soci-eties, published guidelines or the prevention o perinatal group B streptococcal disease (CDC. Prevention o perinatal group Bstreptococcal disease: a public health perspective. MMWR 1996;45[No. RR-7]); those guidelines were updated and republished in2002 (CDC. Prevention o perinatal group B streptococcal disease: revised guidelines rom CDC. MMWR 2002;51[No. RR-11]).In June 2009, a meeting o clinical and public health representatives was held to reevaluate prevention strategies on the basis odata collected ater the issuance o the 2002 guidelines. Tis report presents CDCs updated guidelines, which have been endorsedby the American College o Obstetricians and Gynecologists, the American Academy o Pediatrics, the American College o Nurse-
Midwives, the American Academy o Family Physicians, and the American Society or Microbiology. Te recommendations weremade on the basis o available evidence when such evidence was sucient and on expert opinion when available evidence wasinsucient. Te key changes in the 2010 guidelines include the ollowing: expandedrecommendationsonlaboratorymethodsfortheidenticationofGBS, claricationofthecolony-countthresholdrequiredforreportingGBSdetectedintheurineofpregnantwomen, updatedalgorithmsforGBSscreeningandintrapartumchemoprophylaxisforwomenwithpretermlabororpretermpre-
mature rupture o membranes, achangeintherecommendeddoseofpenicillin-Gforchemoprophylaxis, updatedprophylaxisregimensforwomenwithpenicillinallergy,and arevisedalgorithmformanagementofnewbornswithrespecttoriskforearly-onsetGBSdisease.Universal screening at 3537 weeks gestation or maternal GBS colonization and use o intrapartum antibiotic prophylaxis has
resulted in substantial reductions in the burden o early-onset GBS disease among newborns. Although early-onset GBS disease hasbecome relatively uncommon in recent years, the rates o maternal GBS colonization (and thereore the risk or early-onset GBSdisease in the absence o intrapartum antibiotic prophylaxis) remain unchanged since the 1970s. Continued eforts are needed tosustain and improve on the progress achieved in the prevention o GBS disease. Tere also is a need to monitor or potential adverseconsequencesofintrapartumantibioticprophylaxis(e.g.,emergenceofbacterialantimicrobialresistanceorincreasedincidenceorseverity o non-GBS neonatal pathogens). In the absence o a licensed GBS vaccine, universal screening and intrapartum antibioticprophylaxis continue to be the cornerstones o early-onset GBS disease prevention.
colonization with GBS in the genitourinary or gastrointestinatracts is the primary risk actor or disease. Beginning in themid 1980s, clinical trials and well-designed observational stud-ies demonstrated that administering intravenous antibiotics
during labor to women at risk or transmitting GBS to theirnewborns could prevent invasive disease in the rst week o lie(i.e., early-onset disease) (611). As a result o the collaborativeeorts o clinicians, researchers, proessional organizationsparent advocacy groups, and the public health communityin the 1990s, recommendations or intrapartum prophylaxisto prevent perinatal GBS disease were issued in 1996 by theAmerican College o Obstetricians and Gynecologists (ACOG)(12) and CDC (13) and in 1997 by the American Academy o
IrduciIn the 1970s, the bacterium group B Streptococcus(GBS)
emerged as the leading inectious cause o early neonatal mor-bidity and mortality in the United States (14). Initial case
series reported case-atality ratios as high as 50% (5). Maternal
mailto:[email protected]:[email protected] -
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
4/36
2 MMWR November 19, 2010
Pediatrics (AAP) (14). Revised guidelines or the prevention oearly-onset GBS disease issued in 2002 recommended universalculture-based screening o all pregnant women at 3537 weeksgestation to optimize the identication o women who shouldreceive intrapartum antibiotic prophylaxis (15).
Beore active prevention was initiated, an estimated 7,500
cases o neonatal GBS disease occurred annually in the UnitedStates (16). Striking declines in disease incidence coincidedwith increased prevention activities in the 1990s (17), and aurther reduction occurred ollowing the issuance o the rec-ommendation or universal screening in 2002 (18). However,GBS disease remains the leading inectious cause o morbidityand mortality among newborns in the United States (19,20).Te continued burden o disease and newly available data rel-evant to early-onset GBS disease prevention rom the elds oepidemiology, obstetrics, neonatology, microbiology, molecularbiology, and pharmacology prompted revision o the guidelinesor early-onset GBS disease prevention.
MehdsIn November 2008, CDC ormed a technical working
group* to revise the 2002 guidelines (15). Te group consistedo representatives rom the ACOG Committee on ObstetricPractice, the American College o Nurse-Midwives (ACNM),the AAP Committee on Inectious Diseases and Committeeon the Fetus and Newborn, the American Academy o FamilyPhysicians (AAFP), the Society or Healthcare Epidemiologyo America, the American Society or Microbiology (ASM),
and CDCs Active Bacterial Core surveillance system, as well
as experts in GBS epidemiology, clinical microbiology, andpharmacology. Te group held regular telephone conerencecalls to identiy potential areas o change in the recommendations to prevent GBS disease, and to dene sources o newlyavailable data (published and unpublished) to inorm therevision o the guidelines.
Te working group identied a subset o topics or in-depthreview, including areas in which new technologies and/orevidence had become available since the publication o the2002 guidelines, areas in which implementation o the 2002guidelines was ound to be suboptimal on the basis o pub-lished and unpublished data, and areas in which interpretationo the 2002 guidelines was ound to be variable on the basiso inquiries received at CDC and the experience o experts inthe eld. For these topics, a thorough review was conducted opublished literature through PubMed searches, other source(including abstracts and conerence proceedings), and unpub-lished data rom ongoing surveillance and research activitieso which the working group was aware. For topics on whichseveral sources o data were available, evidence was summarizedin tables. For topics on which relatively little new evidencewas available, summaries o pertinent data were provided toworking group members. Expert opinion was sought romworking group members regarding topics on which no newevidence was available.
In June 2009, an in-person meeting o the technical workinggroup was held to review available data and develop updatedrecommendations using an evidence-based approach whenpossible and relying on expert scientic opinion when sucien
data were lacking (able 1). Tese updated guidelines replaceCDCs 2002 guidelines. Tey are intended or providers oprenatal, obstetric, and neonatal care; supporting microbiol-* A list o the members appears on page 32 o this report.
TABLE 1. Evidence-based rating system used to determine strength o recommendations
Category Defnition Recommendation
Strength o recommendation
A Strong evidence or ecacy and substantial clinical benet Strongly recommended
B Strong or moderate evidence or ecacy but only limited clinical benet Generally recommended
C Insucient evidence or ecacy or ecacy does not outweigh possible adverse consequences Optional
D Moderate evidence against ecacy or or adverse outcome Generally not recommended
E Strong evidence against ecacy or or adverse outcome Never recommendedQuality o evidence supporting recommendation
I Evidence rom at least one well-executed randomized, controlled trial or one rigorously designed laboratory-basedexperimental study that has been replicated by an independent investigator
II Evidence rom at least one well-designed clinical trial without randomization, cohort or case-controlled analyticstudies (preerably rom more than one center), multiple time-series studies, dramatic results rom uncontrolledstudies, or some evidence rom laboratory experiments
III Evidence rom opinions o respected authorities based on clinical or laboratory experience, descriptive studies, orreports o expert committees
Source: Adapted rom LaForce FM. Immunizations, immunoprophylaxis, and chemoprophylaxis to prevent selected inections. US Preventive Services Task ForceJAMA 1987;257:246470.
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
5/36
Vol. 59 / RR-10 Recommendations and Reports 3
ogy laboratories, hospital administrators, and managed-careorganizations; childbirth educators; public health authorities;and expectant parents and their advocates.
Ivasive Grup B Srepcccal
DiseaseGroup B Streptococcus, or Streptococcus agalactiae, is a gram-
positive bacterium that causes invasive disease primarily ininants, pregnant or postpartum women (19,2127), and olderadults, with the highest incidence among young inants (19).Inections in newborns occurring within the rst week o lieare designated early-onset disease. Late-onset inections occurin inants aged >1 week, with most inections evident duringthe rst 3 months o lie. Because o the burden o diseaseamong inants and the availability o eective interventionsto prevent early-onset GBS disease, these guidelines concern
only early-onset disease. Te measures used to prevent early-onset GBS disease also might prevent some perinatal maternalinections (17,28); however, they do not prevent late-onsetinant disease (29).
Early-ose GBS DiseaseGBS is the leading inectious cause o
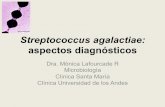
morbidity and mortality among inants inthe United States. As a result o preventioneorts, incidence o GBS has declined dra-matically over the past 15 years, rom 1.7
cases per 1,000 live births in the early 1990sto 0.340.37 cases per 1,000 live births inrecent years (Figure 1). On the basis o datarom CDCs Active Bacterial Core surveil-lance (ABCs) system, a network o 10 sitesacross the United States that conduct active,population-based surveillance, CDC esti-mates that in recent years, GBS has causedapproximately 1,200 cases o early-onsetinvasive disease per year (30); approximately70% o cases are among babies born at term(37 weeks gestation) (19).
Inants with early-onset GBS disease gener-ally present with respiratory distress, apnea,or other signs o sepsis within the rst 2448hours o lie (3,31). he most commonclinical syndromes o early-onset disease aresepsis and pneumonia; less requently, early-onset inections can lead to meningitis. Tecase-atality ratio o early-onset disease hasdeclined rom as high as 50% in the 1970s
(5) to 4%6% in recent years, primarily because o advancesin neonatal care (17,19). Mortality is higher among preterminants, with case-atality rates o approximately 20% and ashigh as 30% among those 33 weeks gestation, comparedwith 2%3% among ull-term inants (17,19).
Early-onset inections are acquired vertically through
exposure to GBS rom the vagina o a colonized womanNeonatal inection occurs primarily when GBS ascends romthe vagina to the amniotic fuid ater onset o labor or ruptureo membranes, although GBS also can invade through intacmembranes (32,33). GBS can be aspirated into the etalungs, which in turn can lead to bacteremia. Inants also canbecome inected with GBS during passage through the birthcanal; inants who are exposed to the organism through thisroute can become colonized at mucus membrane sites in thegastrointestinal or respiratory tracts, but these colonized inantsmost commonly remain healthy.
Risk Facrs r Early-ose GBSDisease
Maternal intrapartum GBS colonization is the primary riskactor or early-onset disease in inants. A classic prospectivecohort study conducted during the 1980s revealed that preg-nant women with GBS colonization were >25 times more likely
FIGURE 1. Incidence o early- and late-onset invasive group B streptococcal (GBS) disease Active Bacterial Core surveillance areas, 19902008, and activities or prevention o GBSdisease
Abbreviations:ACOG = American College o Obstetricians and Gynecologists and AAP = American Acad-emy o Pediatrics.Source: Adapted rom Jordan HT, Farley MM, Craig A, et al. Revisiting the need or vaccine prevention olate-onset neonatal group B streptococcal disease. Pediatr Inect Dis J 2008;27:105764.* Incidence rates or 2008 are preliminary because the live birth denominator has not been nalized.
Early-onset
Late-onset
0.0
0.5
1.0
1.5
2.0
1990 1992 1994 1996 1998 2000 2002 2004 2006 2008
Incidence
per1,0
00
live
births
Year
1st ACOG & AAP statements
Consensus
guidelines
Revised
guidelines
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
6/36
4 MMWR November 19, 2010
than pregnant women with negative prenatal cultures to deliverinants with early-onset GBS disease (34). In the absence oany intervention, an estimated 1%2% o inants born to colo-nized mothers develop early-onset GBS inections (13,34,35).Approximately 10%30% o pregnant women are colonizedwith GBS in the vagina or rectum (3638). GBS colonization
during pregnancy can be transient, intermittent, or persistent(3941). Although some women with GBS colonization duringa pregnancy will be colonized during subsequent pregnancies,a substantial proportion will not (42,43). Te gastrointestinaltract serves as the primary reservoir or GBS and is the likelysource o vaginal colonization. Heavy colonization, dened asculture o GBS rom direct plating rather than rom selectivebroth only, is associated with higher risk or early-onset disease(44,45). GBS identied in clean-catch urine specimens dur-ing any trimester is considered a surrogate or heavy maternalcolonization and also is associated with a higher risk or early-onset GBS disease (4650).
In addition to maternal colonization with GBS, other actorsthat increase the risk or early-onset disease include gestationalage 99.5F (>37.5C)had 6.5 times the risk or having an inant with early-onset
GBS disease compared with women who had none o theserisk actors (34). O note, women who had one o these riskactors but who had negative prenatal screening cultures wereat relatively low risk or early-onset GBS disease (incidence:0.9 cases per 1,000 births) compared with women who werecolonized prenatally but had none o the risk actors (incidence:5.1 cases per 1,000 births) (34).
Some observational studies have reported an associationbetween early-onset GBS disease and certain obstetric pro-cedures, such as the use o internal etal monitoring devices(58,63) and more than ve or six digital vaginal examinationsater onset o labor or rupture o membranes (55,63). However,
lack o randomization in observational studies can result inconounding, because certain procedures might be used morerequently in high-risk settings (64). Although concern hasbeen raised about perorming other obstetric procedures (e.g.,membrane stripping and mechanical and/or pharmacologiccervical ripening) on GBS-colonized women, available data arenot sucient to determine whether these procedures are associ-ated with an increased risk or early-onset disease (65,66).
Prevei Early-ose Grup BSrepcccal Disease
Iraveus Iraparum AibiicPrphylaxis
Te use o intravenous intrapartum antibiotic prophylaxisto prevent early-onset GBS disease in the inant was rststudied in the 1980s. Clinical trials and well-designed obser-vational studies ound that intrapartum antibiotic prophylaxireduced vertical transmission o GBS, as measured by inantcolonization (6,8,11,67) or by protection against early-onsetdisease (611). Early trials suggested an ecacy o 100% orintrapartum antibiotic prophylaxis to prevent early-onsetdisease among inants born to women with GBS colonization(7,8,10,11). Subsequent observational studies have ound theeectiveness to be 86%89% among inants born to womenwho received intrapartum GBS prophylaxis (62,68).
Other strategies to reduce maternal colonization and verti-cal transmission have been studied, including intramuscularintrapartum antibiotic prophylaxis (67), antenatal (oral orintramuscular) antibiotics (6971), and chlorhexidine vagi-nal wipes or douches (7276); however, none has proven tobe eective at preventing early-onset disease. Although somenonrandomized studies on chlorhexidine have yielded promis-ing results (72,75), randomized clinical trials have ound noprotection against early-onset GBS disease or neonatal sepsis(76,77).
Iraparum Aibiic Prphylaxis Ages
Te ecacy o both penicillin (10) and ampicillin (7) asintravenously administered intrapartum agents or the prevention o early-onset neonatal GBS disease was demonstrated inclinical trials. Penicillin has a narrower spectrum o antimi-crobial activity and thereore might be less likely to select orresistant organisms, although one clinical trial ound that penicillin and ampicillin administered intravenously intrapartumwere associated equally with the presence o ampicillin-resistantgram-negative organisms on postpartum vaginal-perineaculture (78). Te dosages o penicillin and ampicillin used orintrapartum GBS prophylaxis are aimed at achieving adequatelevels in the etal circulation and amniotic fuid rapidly whileavoiding potentially neurotoxic serum levels in the motheror etus (7983). Although the exact duration o antibiot-ics needed to prevent vertical transmission o GBS has beendebated (84,85), beta-lactam antibiotics or GBS prophylaxisadministered or 4 hours beore delivery have been ound tobe highly eective at preventing vertical transmission o GBS(86) and early-onset GBS disease (68). Shorter durations oappropriate antibiotics might provide some protection; in
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
7/36
Vol. 59 / RR-10 Recommendations and Reports 5
particular, colonization data suggest durations o 2 hoursbeore delivery might coner some protection (86).
Te ecacy o alternatives to penicillin or ampicillin thathave been used to prevent early-onset GBS disease amonginants born to penicillin-allergic mothers (including ceazolin,clindamycin, erythromycin, and vancomycin) has not been
measured in controlled trials. Ceazolin has a relatively narrowspectrum o activity, similar pharmacokinetics and dynamicsto penicillin and ampicillin, and achieves high intra-amnioticconcentrations (8789). However, an estimated 10% o per-sons with penicillin allergy also have immediate hypersensitiv-ity reactions to cephalosporins (90). In contrast, data on theability o clindamycin, erythromycin and vancomycin to reachbactericidal levels in the etal circulation and amniotic fuidare very limited; available data suggest that erythromycin andclindamycin provided to pregnant women do not reach etaltissues reliably (9195).
SaeyMaternal anaphylaxis associated with GBS intrapartum
chemoprophylaxis occurs but is suciently rare that any mor-bidity associated with anaphylaxis is oset greatly by reductionsin the incidence o maternal and neonatal invasive GBS disease.Anaphylaxis-related mortality is likely to be a rare event becausethe majority o women receiving intrapartum antibiotics willbe in hospital settings where rapid intervention is readily avail-able. Allergic reactions occur in an estimated 0.7%4.0% o alltreatment courses with penicillin, the most common o whichis a maculopapular rash (96). Estimates o the rate o anaphy-laxis caused by penicillin range rom our per 10,000 to ourper 100,000 recipients (96). Maternal anaphylaxis associatedwith GBS prophylaxis was reported in the early 1990s (97);since the release o the 1996 guidelines, our reports o nonatalcases o anaphylaxis associated with GBS chemoprophylaxis inthe United States have been published (98101). In a CDCmultistate sample o approximately 5,000 live births occurringduring 19981999, a single, nonatal anaphylactic reactionwas noted among the 27% o deliveries in which intrapartumantibiotics were administered (62). In that case, a single doseo penicillin was administered approximately 4 hours beorea preterm cesarean delivery, and an anaphylactic reaction
occurred shortly ater the mother received a single dose o acephalosporin ollowing umbilical cord clamping. A similarsample o approximately 7,600 live births occurring during20032004 revealed no cases o anaphylaxis among the 32%o deliveries in which mothers received intrapartum antibioticprophylaxis or GBS (102).
Because a etus or newborn is unlikely to have had a previousexposure to the antibiotic, and because specic maternal IgEantibodies are not transmitted across the placenta (103), there
is no risk or anaphylaxis in the etus or newborn resultingrom intrapartum antibiotic prophylaxis. Although limiteddata are available on the impact o intrapartum antibioticson neonatal gastrointestinal fora, one study comparing stoorom inants born to women who received intrapartum GBSprophylaxis with stool rom inants whose mothers received
no intrapartum antibiotics ound no signicant dierence incolonization with antibiotic-resistant enterobacteria betweenthe two groups (104).
Aibiic Resisace GBS
Te widespread use o intrapartum antibiotic prophylaxis toprevent early-onset GBS disease has raised concern about thedevelopment o antibiotic resistance among GBS isolates. GBScontinues to be susceptible to penicillin, ampicillin, and rst-generation cephalosporins (19,105109). However, isolateswith increasing minimum inhibitory concentrations (MICs)to penicillin or ampicillin have been reported, including 14
noninvasive isolates during 19952005 among adults in Japan(110), and 11 (0.2%) o 5,631 invasive isolates recovered dur-ing 19992005 rom patients o varying ages in the UnitedStates (111). Alterations in a penicillin-binding protein (PBP2X) were ound in all o the isolates rom Japan and our othose rom the United States. Te measured MICs rom the 11invasive isolates rom the United States are just at the thresholdo susceptibility (0.12g/ml or penicillin and 0.25g/mor ampicillin) (112), but the clinical signicance o these MICvalues is as yet unclear.
Relatively elevated MICs to ceazolin (1 g/ml) also werereported among three (0.05%) o 5,631 invasive GBS iso-lates collected through CDCs active surveillance during19992005; two o the three isolates also had elevated MICsto penicillin (0.12 g/ml) (111). Although Clinical andLaboratory Standards Institute guidelines do not speciy sus-ceptibility breakpoints or ceazolin, they recommend that alisolates susceptible to penicillin be considered susceptible toceazolin (112). As with the elevated MICs to penicillin andampicillin, the clinical signicance o higher MICs to ceazolinamong GBS isolates remains unclear.
Te proportions o GBS isolates with in vitro resistance toclindamycin or erythromycin have increased over the past 20
years. Te prevalence o resistance among invasive GBS isolatein the United States ranged rom 25% to 32% or erythromycinand rom 13% to 20% or clindamycin in reports publishedduring 20062009 (19,106,108). Resistance to erythromycinis associated requently but not always with resistance to clin-damycin. One longitudinal study o GBS early-onset sepsisound that although the overall rate o GBS early-onset diseasedeclined over time, erythromycin-resistant GBS caused anincreasing proportion o disease during this interval; however
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
8/36
6 MMWR November 19, 2010
the incidence o antibiotic-resistant GBS early-onset sepsisremained stable (105).
Vaccies Preve GBS DiseaseGBS vaccines have been investigated as a tool or reduc-
ing maternal colonization and preventing transmission toneonates (113,114); however, no licensed vaccine is availablecurrently. Sucient amounts o GBS capsular polysaccharidetype-specic serum IgG in mothers have been shown to protectagainst invasive disease in their inants (51,115118). PhaseI and II clinical trials among healthy, nonpregnant adults omonovalent polysaccharide-protein conjugate vaccines o GBSdisease-associated types have shown these vaccines to be welltolerated and immunogenic (116121). A recent, double-blindrandomized trial o a conjugate vaccine against GBS serotypeIII among nonpregnant women o reproductive age ound asignicant delay in acquisition o colonization with the vaccine-
serotype among vaccine recipients (122). Although an eectiveGBS vaccine would be a powerul tool against GBS disease,no licensed vaccine is yet available.
Ideifcai Cadidaes rIraparum Aibiic Prphylaxis
Culure- Versus Risk-Based ScreeigEarly guidelines recommended the use o one o two
approaches to identiying women who should receive intra-partum antibiotic prophylaxis: a risk-based approach or a
culture-based screening approach (13). Providers using therisk-based method identiied candidates or intrapartumchemoprophylaxis according to the presence o any o theollowing intrapartum risk actors: delivery at
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
9/36
Vol. 59 / RR-10 Recommendations and Reports 7
period in GBS-colonized women with preterm prematurerupture o membranes or preventing early-onset GBS diseasein the inant.
Baceriuria
GBS is ound in the urine o 2%7% o pregnant women(4648,129,130). GBS bacteriuria in a pregnant woman isa marker or heavy genital tract colonization, and maternalGBS bacteriuria (including pure and predominant growth oGBS in the urine) has been associated with GBS colonizationand an increased risk or early-onset disease in the newborn(4650,129). Although some women receive antibiotics totreat GBS bacteriuria during pregnancy, antibiotics do noteliminate GBS rom the genitourinary and gastrointestinaltracts, and recolonization ater a course o antibiotics is typical(71,131,132). Studies have ound that some women with GBSbacteriuria during the rst trimester might not have vaginal-
rectal colonization detected at 3537 weeks gestation (130) orat the time o delivery (133). However, maternal GBS bacte-riuria at any point during pregnancy is a recognized risk actoror early-onset GBS disease and thereore has been includedas an indication or intrapartum antibiotic prophylaxis since1996 (13,15).
Te 1996 guidelines did not speciy a colony-count thresh-old or dening GBS bacteriuria. In 2002, the guidelinesrecommended that laboratory personnel report GBS presentin any concentration in the urine. Most data on the risk orearly-onset GBS disease among inants born to women withGBS bacteriuria are derived rom studies o signicant GBS
bacteriuria (generally >105 colony-orming units per millimetero urine) (4749). Although lower concentrations (
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
10/36
8 MMWR November 19, 2010
Specime ClleciSwabbing both the lower vagina and rectum (through the
anal sphincter) increases the culture yield substantially com-pared with sampling the cervix or the vagina without also swab-bing the rectum (40,141146). Although a small number o
studies have examined the ability o perianal or vaginal-perianalcultures to detect GBS colonization (147,148), the availabledata on their perormance compared with vaginal-rectal cul-tures are limited. Studies have indicated that when women inthe outpatient clinic setting collect their own vaginal-rectalscreening specimens, with appropriate instruction, GBS yieldis similar to when specimens are collected by a health-careprovider (149152).
Te use o appropriate transport media can help sustainthe viability o GBS in settings where immediate laboratoryprocessing is not possible (153,154). GBS isolates can remainviable in transport media or several days at room temperature;
however, the recovery o isolates declines during 14 days, par-ticularly at high temperatures. Even when appropriate transportmedia are used, the sensitivity o culture is greatest when thespecimen is stored at 4C beore culture and processed within24 hours o collection (139,155157).
Specime PrcessigRegardless o the test selected to identiy GBS, use o an
enrichment broth improves detection substantially. Whendirect agar plating is used instead o selective enrichmentbroth, as many as 50% o women who are GBS carriers have
alse-negative culture results (143,144,158,159). Exampleso selective enrichment broths include odd-Hewitt brothsupplemented either with gentamicin (8g/ml) and nalidixicacid (15g/ml) [ransVag broth] or with colistin (10g/ml)and nalidixic acid (15 g/ml) [Lim broth] (160). AlthoughransVag and Lim broth media are oten available withoutblood, the addition o 5% sheep blood can increase therecovery o GBS (161). Selective enrichment broth also cancontain chromogenic substrates that provide or a change incolor in the setting o beta-hemolytic GBS. Such broths canacilitate the identication o beta-hemolytic GBS; however,nonhemolytic isolates will not be detected by these broths
alone (162168). Among 265 GBS isolates rom invasiveearly-onset cases that occurred in the 10 ABCs system areasduring 20062008, a total o 4% were nonhemolytic (CDC,unpublished data, 20062008).
Following enrichment, the conventional means or identiy-ing GBS is through isolation on subculture to blood agar platesand presumptive identication by the CAMP test (169) orserologic identication using latex agglutination with group Bstreptococcal antisera (170). More recently, chromogenic agars
that undergo color change in the presence o beta-hemolyticcolonies o GBS have become available (171,172). As withpigmented enrichment broths, these chromogenic agars canacilitate detection o beta-hemolytic GBS, but the majoritywill not detect nonhemolytic strains. In addition more rapidtechniques or identiying GBS directly rom enrichment
broth, or ater subculture have been developed, including DNAprobes (173176) and nucleic acid amplication tests (NAA)such as polymerase chain reaction (177,178).
Published studies on the perormance o commerciallyavailable NAA on nonenriched samples have demonstratedvarying sensitivities (range: 62.5%98.5%) and specicities(range: 64.5%99.6%) compared with the gold standard oenrichment ollowed by subculture (179188) (able 2). Treestudies have compared both intrapartum NAA on nonen-riched samples and late antepartum enriched culture results tointrapartum enriched culture (179,182,185). When comparingswabs collected at the two dierent time points, two o thestudies ound intrapartum NAA to be slightly more sensitive(95.8% and 90.7%, respectively) than antepartum culture(83.3% and 84.3%, respectively) (182,185), although withwidely overlapping condence intervals. One study reporteda statistically signicant dierence between the sensitivity oswabs collected intrapartum and tested with NAA (94.0%compared with enriched culture perormed on swabs collectedprenatally (54.3%) (179). Te sensitivity o NAA or GBSincreases to 92.5%100.0% with use o an enrichment stepbeore testing the sample (177,178,188). Use o an enrichmentstep lengthens the time to obtain a nal result; however, or
antenatal testing, the accuracy o results is much more impor-tant than timeliness.Despite the availability o NAA or GBS, utility o such
assays in the intrapartum setting remains limited. Although ahighly sensitive and specic test with rapid turnaround timecould be used to assess intrapartum GBS colonization andthereore obviate the need or antenatal screening, data oncurrently available assays do not support their use in replace-ment o antenatal culture or risk-based assessment o womenwith unknown GBS status on admission or labor. Te addi-tional time required or enrichment o samples makes it noteasible or intrapartum testing, and the sensitivity o assays
in the absence o enrichment is not adequate in comparisonto culture. In addition, concerns remain regarding real-worldturnaround time, test complexity, availability o testing at altimes, stang requirements, and costs. In settings that canperorm NAA, such tests might prove useul or the limitedcircumstance o a woman at term with unknown colonizationstatus and no other risk actors. Even optimal NAA wouldhave drawbacks in the intrapartum setting, including a delayin administration o antibiotics while waiting or the result
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
11/36
Vol. 59 / RR-10 Recommendations and Reports 9
and no antimicrobial susceptibility testing or penicillin-allergicwomen. Other rapid tests in addition to NAA have been
developed to detect GBS rapidly rom nonenriched samples,including optical immunoassays and enzyme immunoassays;however, none is suciently sensitive when used on a directspecimen to detect GBS colonization reliably in the intrapar-tum setting (180,189192).
Aimicrbial Suscepibiliy tesigAntimicrobial susceptibility testing o GBS isolates is crucial
or appropriate antibiotic prophylaxis selection or penicillin-
allergic women who are at high risk or anaphylaxis becauseresistance to clindamycin, the most common agent used in
this population, is increasing among GBS isolates. In addi-tion, appropriate methodologies or susceptibility testingare important because inducible clindamycin resistance canoccur in some strains that appear susceptible in broth suscep-tibility tests (193,194). D-zone testing using the double-diskdiusion method has been used to identiy isolates that areerythromycin-resistant and clindamycin-susceptible, yet haveinducible resistance to clindamycin (195). Isolates that areD-zone positive are considered to have inducible clindamycin
TABLE 2. Perormance o Nucleic Acid Amplifcation Tests* (NAAT) compared with enriched culture or detecting group B Streptococcus (GBS)
Swab or NAAT and culture
No. positiveby NAAT/
No. positiveby culture
NAATsensitivity
No. negativeby NAAT/
No. negativeby culture
NAATspecifcityTest Timing Type
NAAT perormed on nonenriched samples
IDI-Strep IP VR 140/149 94.0% 626/653 95.9%
IDI-Strep IP V 35/56 62.5% 252/259 97.3%IDI-Strep** AP/IP VR 59/68 86.8% 157/165 95.2%
GeneXpert IP VR 23/24 95.8% 20/31 64.5%IDI-Strep AP/IP VR 149/188 79.3% 575/603 95.4%
GeneXpert AP/IP VR 173/190 91.1% 570/594 96.0%
BD GeneOhm AP V 64/83 77.1% 99/117 84.6%BD GeneOhm*** IP VR 49/54 90.7% 121/124 97.6%
GeneXpert AP/IP V 135/137 98.5% 723/726 99.6%
IDI-Strep IP VR 38/42 90.5% 148/154 96.1%
NAAT perormed on enriched samplesBD GeneOhm**** AP VR 49/53 92.5% 136/147 92.5%
BD GeneOhm AP VR 100.0% 99.3%
BD GeneOhm AP VR 92.5% 99.3%
BD GeneOhm AP V/VR 136/141 96.4% 349/357 97.8%
Abbreviations: AP = antepartum, IP = intrapartum, V = vaginal only, and VR = vaginal-rectal.
* Includes only those NAAT that are approved or use by the Food and Drug Administration. Compared with enriched culture o specimen collected at the same time as that used or NAAT. Source: Davies HD, Miller MA, Faro S, Gregson D, Kehl SC, Jordan JA. Multicenter study o a rapid molecular-based assay or the diagnosis o group B Streptococcu
colonization in pregnant women. Clin Inect Dis 2004;39:112935. Source: Aziz N, Baron EJ, DSouza H, Nourbakhsh M, Druzin ML, Benitz WE. Comparison o rapid intrapartum screening methods or group B streptococcal vagina
colonization. J Matern Fetal Neonatal Med 2005;18:2259.** Source: Atkins KL, Atkinson RM, Shanks A, Parvin CA, Dunne WM, Gross G. Evaluation o polymerase chain reaction or group B Streptococcus detection using an
improved culture method. Obstet Gynecol 2006;108(3 Pt 1):48891. Source: Gavino M, Wang E. A comparison o a new rapid real-time polymerase chain reaction system to traditional culture in determining group B Streptococcu
colonization. Am J Obstet Gynecol 2007;197:388e14. Source: Edwards RK, Novak-Weekley SM, Koty PP, Davis T, Leeds LJ, Jordan JA. Rapid group B streptococci screening using a real-time polymerase chain reaction
assay. Obstet Gynecol 2008;111:133541. Source: Smith D, Perry JD, Laine L, Galloway A, Gould FK. Comparison o BD GeneOhm real-time polymerase chain reaction with chromogenic and conventiona
culture methods or detection o group B Streptococcus in clinical samples. Diagn Microbiol Inect Dis 2008;61:36972.*** Source: Money D, Dobson S, Cole L, et al. An evaluation o a rapid real time polymerase chain reaction assay or detection o group B Streptococcus as part o
neonatal group B Streptococcus prevention strategy. J Obstet Gynaecol Can 2008;30:7705. Source: El Helali N, Nguyen JC, Ly A, Giovangrandi Y, Trinquart L. Diagnostic accuracy o a rapid real-time polymerase chain reaction assay or universal intrapartum
group B Streptococcusscreening. Clin Inect Dis 2009;49:41723. Source: Ala MJ, Sepehri S, De Gagne P, Helawa M, Sandhu G, Harding GK. Real-time PCR assay provides reliable assessment o intrapartum carriage o group BStreptococcus. J Clin Microbiol 2010;48:30959.
Duration o incubation in selective enrichment broth varied (range: 424 hours).**** Source: Goodrich JS, Miller MB. Comparison o culture and 2 real-time polymerase chain reaction assays to detect group B Streptococcus during antepartum
screening. Diagn Microbiol Inect Dis 2007;59:1722. Source: Block T, Munson E, Culver A, Vaughan K, Hryciuk JE. Comparison o carrot broth- and selective Todd-Hewitt broth-enhanced PCR protocols or real-tim
detection oStreptococcusagalactiae in prenatal vaginal/anorectal specimens. J Clin Microbiol 2008;46:361520. Primary data unavailable. Source: Scicchitano L, Bourbeau P. Comparative evaluation o the AccuProbe group B Streptococcus culture test, the BD GeneOhm Strep B assay, and culture o
detection o group B streptococci in pregnant women. J Clin Microbiol 2009;47:30213.
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
12/36
10 MMWR November 19, 2010
resistance and are presumed to be resistant although the clinicalsignicance o this resistance is not clear (196).
Secdary Prevei Early-ose GBS Amg Ias
Currently available GBS prevention strategies will not pre-vent all cases o early-onset disease. Rapid detection o neonatalinections and initiation o appropriate treatment is neededto minimize morbidity and mortality among the cases thatcontinue to occur. Te detection o early-onset GBS diseaseposes certain clinical challenges, because neonatal providersmust take into account the clinical appearance o the inant,the presence o maternal risk actors or GBS disease, and inantexposure to intrapartum antibiotics.
Ias wih Sigs SepsisAs use o intrapartum antibiotics to prevent early-onset GBS
disease increased, concern was expressed that signs o sepsis inthe newborn could be delayed or masked, impairing the abil-ity o clinicians to detect early-onset GBS disease (197199).However, several studies conducted since 1996 have ound nosignicant dierence in the clinical presentation o early-onsetGBS disease between inants exposed to intrapartum antibiot-ics and those not exposed (200204). Approximately 90% ocases o early-onset disease continue to maniest within therst 24 hours o lie.
Although maternal GBS colonization might increase clinical
suspicion or early-onset GBS disease in an inant, in the erao universal screening, >60% o early-onset GBS cases haveoccurred among inants born to women who had a negative pre-natal GBS culture screen (102,203,204). False-negative cases arenot unexpected because culture at 3537 weeks gestation willail to detect some women with intrapartum GBS colonization.As eective prevention strategies are increasingly implemented,a growing proportion o the remaining relatively low burden odisease will refect inherent limitations in the strategies. Signs osepsis in any newborn can be an indication o early-onset GBSdisease, regardless o maternal colonization status.
Among inants with signs o early-onset disease, the detection
o GBS can be increased by perorming culture o both bloodand cerebrospinal fuid (CSF). Blood cultures can be sterile inas many as 15%33% o newborns with meningitis (205209),and the clinical management o an inant with abnormal CSFndings diers rom that o an inant with normal CSF.
Ias Br Wmewih Chriamiiis
Chorioamnionitis is an important risk actor or early-onset GBS disease in women with GBS colonization andcan refect an intrauterine onset o inection in the neonate
(45,63,210212). Intrapartum ever, one sign o chorioamni-onitis in parturient women, has been associated with ailure ointrapartum antibiotics to prevent GBS disease in the newborn(68,213). Intrapartum treatment o chorioamnionitis canprevent neonatal sepsis (214,215). Te diagnosis o chorio-amnionitis usually is made clinically on the basis o signs andsymptoms such as ever (which might be low-grade), uterinetenderness, etal tachycardia, maternal tachycardia, and oul-smelling or purulent amniotic fuid. In an eort to avert neo-natal inections, maternal ever alone in labor may be used asa sign o chorioamnionitis and hence indication or antibiotictreatment, particularly among women with a signicant risk
actor or chorioamnionitis (e.g., prolonged labor or prolongedrupture o membranes).
Because an association has been observed between epi-dural labor analgesia and ever, chorioamnionitis might beoverdiagnosed in women with epidurals, which could lead tounnecessary diagnostic evaluations and unnecessary exposureto empirical antibiotics in neonates (216). However, multistatesurveillance data suggest that although epidural use is com-mon (in 67% o births), intrapartum temperature o 100.4F[38.0C] (3.3% o births) and physician diagnoses o cho-rioamnionitis (3.1% o births) remain relatively rare (102)(CDC, unpublished data, 2009). Consultation with obstetric
providers to determine whether chorioamnionitis is suspectedis important or guiding neonatal management.
Well-Appearig Ias Expsed Iadequae Iraparum Aibiics
Te management o well-appearing inants whose moth-ers received inadequate intrapartum antibiotic prophylaxis(because o either a short duration o exposure beore deliveryor use o an agent with limited ecacy data) can be challeng-ing. Previous GBS prevention guidelines have recommendedthat inants whose mothers received inadequate intrapartum
antibiotic prophylaxis and those
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
13/36
Vol. 59 / RR-10 Recommendations and Reports 11
high, the positive predictive value is low, particularly amonghealthy-appearing term inants (219221). Te sensitivity othe CBC is lowest immediately ater birth, and its perormanceas a screen or sepsis can be improved by obtaining the bloodspecimen between 612 hours o lie (220,222,223). Clinicalsigns o sepsis have been ound to be a more sensitive indicator
o neonatal sepsis than hematologic tests (201).Certain centers provide intramuscular penicillin to asymp-
tomatic inants within 1 hour o birth; this practice is basedon results o observational studies demonstrating declines inearly-onset GBS disease coincident with a policy o univer-sal administration o intramuscular penicillin to newborns(224226). However, because the studies used historic controlgroups and were conducted at a single center that does notscreen pregnant women routinely or antenatal GBS coloniza-tion, the ndings are not generalizable to other settings.
Implemeai ad Impac GBS Prevei Ers
Implemeai he 2002Guidelies
Ater the issuance o the 2002 recommendation or universalculture screening, implementation was rapid and widespread.Te most robust evaluation comes rom a multistate, popula-tion-based analysis o 819,000 live births during 20032004(102) and a similarly designed studyo births during 19981999 (62). Te
proportion o inants whose mothers were screened or GBS colonizationbeore delivery increased rom 48.1%during 19981999 to 85.0% during20032004 (Figure 2); among womenscreened during 20032004, a total o98.4% had a result available at labor.Among screened women, 24.2% weredocumented as GBS-positive, withinthe range o expected colonizationrates. Te proportion o mothers withan indication or intrapartum antibiotic
prophylaxis who received them alsoincreased substantially, rom 73.8%during 19981999 to 85.1% during20032004 (Figure 3).
Despite widespread uptake o uni-versal screening, implementation ellshort in several key areas. Inants bornpreterm have an elevated risk or early-onset disease, and because antenatal
screening is recommended at 3537 weeks o gestation, only50.3% o women delivering preterm had a known coloniza-tion status at the time o hospital admission. Although it isrecommended that women with unknown GBS status whodeliver preterm receive intrapartum antibiotic prophylaxisonly 63.4% received prophylaxis. In addition, intrapartum
antibiotic prophylaxis administration or the indications oGBS bacteriuria or having delivered a previous inant withGBS disease was also low (73.5%) among preterm deliveriesIntrapartum antibiotic prophylaxis was provided to a greaterproportion (84.5%) o women delivering preterm who had apositive GBS screening result. Screening or GBS on admissionamong women with threatened preterm delivery and unknowncolonization status was suboptimal; only 18% o womenwho progressed to delivery and 31% o women who did noprogress to delivery were screened despite a recommendationto perorm cultures or GBS at hospital admission or thispopulation (15,102).
As anticipated, the proportion o laboring women whoreceived intrapartum antibiotics increased only slightly, rom26.8% to 31.7%, under universal screening. Penicillin andampicillin, the recommended agents or intrapartum GBS pro-phylaxis or women with no allergy to penicillin, remained themost common agents administered (76.7% o women receiv-ing intrapartum antibiotic prophylaxis received these agents)However, among penicillin-allergic women, the agents mostoten administered did not refect the 2002 recommendations
FIGURE 2. Percentage o pregnant women screened or group B streptococcal colonization Active Bacterial Core surveillance areas, 19981999 and 20032004*
Source: Van Dyke MK, Phares CR, Lyneld R, Thomas AR, Arnold KE, Craig AS, et al. Evaluation o universaantenatal screening or group B Streptococcus. N Engl J Med 2009;360:262636.*Reported values are weighted to account or the stratied survey design. The number o charts abstracted
was 5,144 or 19981999 and 7,691 or 20032005. 95% condence inerval. Data or 19981999 not available.
19981999
Percentage
Area
20032004
0
10
20
30
40
50
60
70
80
90
100
Tennessee California Oregon Minnesota New York Georgia Connecticut Maryland Colorado New Mexic
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
14/36
12 MMWR November 19, 2010
In particular, only 13.8% o penicillin-allergic women whowere not at high risk or anaphylaxis received ceazolin, despitea recommendation that this more eective agent be used.Clindamycin remained the leading agent among penicillin-allergic women (69.9% o those at low risk or anaphylaxisand 83.5% o those at high risk). Among women receiving
clindamycin or prophylaxis, clindamycin and erythromycinsusceptibility testing were perormed rarely despite recommen-dations that susceptibility testing be conducted on all vaginal-rectal specimens rom women who are allergic to penicillin andat high risk or anaphylaxis (15,102). A single-hospital studyin Rhode Island reported similar ndings (227).
Te multistate population-based study conducted during20032004 also identied a greater-than-expected numbero cases o early-onset GBS occurring among inants born towomen with negative prenatal screening results (61% observedcompared with 23%46% expected cases o early-onset GBSdisease among ull-term inants) (102). Some alse-negativeresults are expected because culture is not perectly sensitive andGBS can be acquired by the mother during the period betweenscreening and delivery. However, the high proportion o casesborn to women with negative screening results suggests possibleproblems in the steps required to identiy GBS colonization.Suboptimal specimen collection timing, methods, transport,and/or laboratory processing might be contributing actors.
FIGURE 3. Percentage o women with an indication who received intrapartum antibioticprophylaxis Active Bacterial Core surveillance areas, 19981999 and 20032004*
Source: Van Dyke MK, Phares CR, Lyneld R, Thomas AR, Arnold KE, Craig AS, et al. Evaluation o universalantenatal screening or group B Streptococcus. N Engl J Med 2009;360:262636.*Reported values are weighted to account or the stratied survey design. The number o charts abstracted
was 5,144 or 19981999 and 7,691 or 20032005. 95% condence inerval. Data or 19981999 not available.
19981999
Percentage
Area
20032004
0
10
20
30
40
50
60
70
80
90
100
Tennessee California Oregon Minnesota New York Georgia Connecticut Maryland Colorado New Mexico
Among screened women, the date othe antenatal screening test was missingrom 36% o labor and delivery chartsDocumentation o the date allows oran assessment o whether screening wasperormed during the recommended
gestation time window.
treds i neaal GBSDisease
Incidence o invasive early-onset GBSdisease has declined approximately80% (Figure 1) since the early 1990swhen implementation o intrapartumantibiotic prophylaxis to prevent GBSdisease began. Nationally representativehospital discharge diagnostic code data
also demonstrated a steady decrease inclinical sepsis rates during 19902002with a marked decline in clinical sepsisamong term inants during the 2 yearsollowing the issuance o the 1996 GBSprevention guidelines (228); these data
suggest that the observed decline in early-onset GBS disease is aresult o prevented cases o illness and not simply o sterilizationo neonatal blood cultures as a result o exposure to maternaantibiotics. During 19992001, incidence o early-onset GBSdisease achieved a plateau o approximately 0.5 cases per 1,000live births. Ater the 2002 guidelines were issued, incidencedeclined urther and in recent years has ranged rom 0.3 to 0.4cases per 1,000 live births. Tis additional decline o 20%40%is consistent with that predicted or the transition rom the1996 prevention strategy to the universal screening approachrecommended in 2002 (62). Similar trends have been reportedamong inants delivered in all U.S. military hospitals (229)However, the disparity in early-onset GBS disease incidencebetween black and white inants has persisted (Figure 4) andis evident among both term and preterm inants (18,20)Preliminary surveillance data rom 2008 suggest that theracial disparity was reduced somewhat in 2008 (30). Incidence
among all black inants declined to 0.49 cases per 1,000 livebirths, showing progress towards the Healthy People 2010objective o 0.5 cases per 1,000 live births or all racial andethnic groups (230). However nal data rom 2008, includ-ing enhanced race/ethnicity reporting on cases and the 2008live birth denominators, and more years o data are needed todetermine whether this trend is sustained.
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
15/36
Vol. 59 / RR-10 Recommendations and Reports 13
treds i n-GBSPahges
Decreases in the incidence o early-onsetGBS sepsis have not been accompaniedby increases in incidence o early-onset
sepsis caused by other pathogens, includ-ing those that are antimicrobial-resistant.Most studies, including population-basedmulticenter studies, have ound stable(231239) or decreasing (240,241) rateso non-GBS early-onset sepsis during aperiod o increasing use o intrapartumantibiotic prophylaxis or GBS. Increasesin invasive Escherichia coliinections havebeen reported among preterm and low-birth-weight or very low-birth-weightinants (242246), and some studies
have ound an increasing proportion oampicillin-resistant isolates among pre-term or very low birth-weight inants withE. colisepsis (235,245,247). However, thetrends have not been consistent over timeor across studies. A multicenter study o sepsis in preterm inantsthat reported an increase in E. coliincidence rom 19911993to 19982000 (246) ound stable rates oE. colisepsis rom19982000 to 20022003 and reported no signicant changein the proportion oE. coliisolates that were resistant to ampicil-lin (248). Whether any observed increase in ampicillin-resistantE. coliis attributable to the use o intrapartum antibiotics or
GBS prophylaxis is unclear because ampicillin resistance amongE. coliisolates has increased communitywide (249). Currentlyavailable evidence does not suggest any increase in non-GBSearly-onset sepsis among term inants.
An association between intrapartum antibiotic exposure andampicillin resistance in newborns with E. colior other non-GBSearly-onset sepsis has been observed in several studies among allnewborns (55,239,242,250252) and among preterm or verylow birth-weight inants (245,246). However, studies usinginants inected with nonresistant pathogens as a control groupdo not account or ampicillin-susceptible inections preventedby intrapartum antibiotic prophylaxis and thereore mightoverestimate an association between antibiotic exposure andantibiotic resistance (253). A multicenter case-control study oearly-onset E. colicases that enrolled uninected inants born atthe same hospitals ound no association between intrapartumantibiotic prophylaxis exposure and inection with ampicillin-resistant E. coli(254).
Te reported increases in E. coliearly-onset sepsis amongpreterm inants and antibiotic-resistant early-onset inectionsare not o sucient magnitude to outweigh the benets ointrapartum antibiotic prophylaxis to prevent early-onset GBSdisease. Among all neonates, rates oE. coliearly-onset sepsishave remained stable and lower than those o GBS early-onsetdisease, despite declines in GBS (CDC, unpublished data
2009). However, to ensure early detection o increases in therate o disease or deaths caused by organisms other than GBScontinued surveillance o neonatal sepsis caused by organismsother than GBS is needed.
Impac GBS Prevei Ers Ia Maageme
Provider surveys conducted in the early to mid 1990s indi-cated that pediatricians and neonatologists were more likely toconduct diagnostic evaluations and initiate empiric antibioticsor an inant whose mother received intrapartum antibiotic
prophylaxis than they were or an inant whose mother who didnot receive prophylaxis (197199). Results o studies conductedduring 19962002 were inconsistent, reporting increased (255)stable (256), or decreased (257) use o health services (including diagnostic tests, antibiotics, and/or length o hospital stay)or neonates born to women receiving intrapartum antibioticsNo studies have reported on the impact o the 2002 guidelines
FIGURE 4. Incidence o early-onset invasive group B streptococcal disease, stratifed byrace and term Active Bacterial Core surveillance areas, 20002007
Source:Adapted rom CDC. Trends in perinatal group B streptococcal diseaseUnited States, 20002006MMWR 2009;58:10912.
Term white infants
Term black infants
0
1.0
2.0
3.0
4.0
2000 2001 2002 2003 2004 2005 2006 2007
Incidence
per1,0
00
liveb
irths
Year
Preterm white infants
Preterm black infants
.5
1.5
2.5
3.5
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
16/36
14 MMWR November 19, 2010
on health-care services or neonates. Continued monitoringo the infuence o GBS prevention recommendations on themanagement o newborns is needed.
RecmmedaisTe ollowing updated recommendations or the prevention
o early-onset GBS disease are based on critical appraisal odata that have become available since publication o previousCDC (13,15) and ACOG (258) recommendations and replaceprevious recommendations rom CDC. Tese recommenda-tions have been endorsed by ACOG, AAP, ACNM, AAFP, andASM. Ater each recommendation, its strength (indicated bya letter) and the quality o supporting evidence (indicated bya Roman numeral) are shown in parentheses according to theevidence-based rating system used (able 1).
Obstetric and neonatal health-care providers, in conjunction
with supporting laboratories and labor and delivery acilities,should adopt the ollowing recommendations or the preven-tion o early-onset GBS disease.
Ideifcai Cadidaes rIraparum Aibiic Prphylaxis
Uiversal Screeig r GBS
Candidates to receive intrapartum antibiotic prophylaxis toprevent early-onset GBS disease should be identied accordingto the indications and nonindications provided (able 3).
he ollowing are key components o the screeningstrategy: WomenwithGBSisolatedfromtheurineatanytimedur-
ing the current pregnancy or who had a previous inant withinvasive GBS disease should receive intrapartum antibioticprophylaxis and do not need third trimester screening or
GBS colonization (AII). Women with symptomatic orasymptomatic GBS urinary tract inection detected duringpregnancy should be treated according to current standardso care or urinary tract inection during pregnancy andshould receive intrapartum antibiotic prophylaxis to prevenearly-onset GBS disease (AIII).
All otherpregnantwomenshould bescreenedat 3537weeks gestation or vaginal and rectal GBS colonization(AII).
Atthetimeoflabororruptureofmembranes,intrapartumantibiotic prophylaxis should be given to all pregnant womenwho tested positive or GBS colonization (AII), except inthe instance o cesarean delivery perormed beore onset olabor on a woman with intact amniotic membranes.
Forcircumstancesinwhichscreeningresultsarenotavail-able at the time o labor and delivery, intrapartum antibioticprophylaxis should be given to women who are
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
17/36
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
18/36
16 MMWR November 19, 2010
FIGURE 6. Algorithm or screening or group B streptococcal (GBS)colonization and use o intrapartum prophylaxis or women withpreterm* premature rupture o membranes (pPROM)
* At 5 weeks prior, she shouldbe rescreened and managed according to this algorithm at that time.
Patient entering labor?
Continue antibiotics
until delivery
Continue antibiotics per standard
of care if receiving for latency
or
continue antibiotics for 48 hours**
if receiving for GBS prophylaxis
Not available prior
to labor onset
Obtain vaginal-rectal swab for GBS culture and start
antibiotics for latency or GBS prophylaxis
NoYes
Obtain GBS culture results
NegativePositive
GBS prophylaxis at
onset of true labor
No GBS prophylaxis at onset of true
labor; repeat vaginal-rectal culture
if patient reaches 3537 weeks
gestation and has not yet delivered
point it is determined that she is not in true labor or i theGBS culture at admission is negative (AII).
NegativeGBScolonization status should notaect theadministration o antibiotics or other indications (AIII).
WomenwiththreatenedpretermdeliverywhohaveaGBSscreen perormed that is positive and do not deliver at that
time should receive GBS prophylaxis when true labor begins(AII).
WomenwiththreatenedpretermdeliverywhohaveaGBSscreen perormed that is negative but do not deliver at thattime should undergo repeat screening at 3537 weeks ges-tation. I such women are re-admitted at a later date withthreatened preterm delivery, they should undergo repeatscreening i the previous culture was perormed >5 weeksprior (AIII).he ollowing key changes were made rom the 2002
guidelines: SeparatealgorithmsarepresentedforGBSprophylaxisinthe
setting o threatened preterm delivery, one or spontaneouspreterm labor (Figure 5) and one or preterm prematurerupture o membranes (Figure 6).
GBSprophylaxisprovidedtowomenwithsignsandsymp-toms o preterm labor should be discontinued i it is deter-mined that the patient is not in true labor (AI).
Antibioticsgiventoprolonglatencyforpretermprematurerupture o membranes with adequate GBS coverage (speci-cally 2 g ampicillin administered intravenously ollowed by1 g administered intravenously every 6 hours or 48 hours)are sucient or GBS prophylaxis i delivery occurs while the
patient is receiving that antibiotic regime (CIII). Oral anti-biotics alone are not adequate or GBS prophylaxis (DII).Womenwith pretermprematureruptureofmembranes
who are not in labor and are receiving antibiotics to prolonglatency with adequate GBS coverage should be managedaccording to standard o care or preterm premature ruptureo membranes; GBS testing results should not aect theduration o antibiotics (BIII).
Womenwithpretermprematureruptureofmembraneswhoare not in labor and are not receiving antibiotics to prolonglatency (or are receiving antibiotics that do not have adequateGBS coverage) should receive GBS prophylaxis or 48 hours
unless a GBS screen perormed within the preceding 5 weekswas negative (CIII). I the results rom a GBS screen per-ormed on admission become available during that 48-hourperiod and are negative, then GBS prophylaxis should bediscontinued at that time.
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
19/36
Vol. 59 / RR-10 Recommendations and Reports 17
GBS Specime Clleciad Prcessig
GBS specimen collection and processing should beconducted according to the recommendations provided(Boxes 13 and Figure 7).
Te ollowing are key components o specimen collectionand processing: GBScolonizationstatusshouldbedeterminedbycollecting
both vaginal and rectal specimens at 3537 weeks gestation.A single combined vaginal-rectal specimen can be collected(AII).
Specimensshould undergo 1824hour incubationat3537C in an appropriate enrichment broth medium toenhance the recovery o GBS (AI).
Accurateresultsaremoreimportantthanrapidturnaroundtime or antenatal screening (AIII).
To ensureproper testingof specimens, cliniciansmust
inorm laboratories when submitted urine specimens arerom pregnant women (AIII).
Antimicrobial susceptibility testingshould beperformedon antenatal GBS isolates rom penicillin-allergic womenat high risk or anaphylaxis because o a history o anaphy-laxis, angioedema, respiratory distress, or urticaria ollow-ing administration o a penicillin or a cephalosporin. (AII)(Box 3).he ollowing key changes were made rom the 2002
guidelines: Specimentransportoptionsandtiminguntilprocessingare
claried.
GBSidenticationoptionsareexpandedtoincludeapositiveidentication rom chromogenic media and identicationdirectly rom enriched broth. NAA, such as commerciallyavailable PCR assays, can also be used ater enrichment, ilaboratories have validated NAA perormance and insti-tuted appropriate quality controls (CII).
Adirect platingoption can beincludedin addition toenriched culture (CII). Direct plating has a lower sensitivitythan enriched culture and should not be used as sole meansto identiy GBS.
Testing for inducible clindamycinresistance shouldbeperormed on antenatal GBS isolates that are susceptible toclindamycin, resistant to erythromycin, and are rom penicillin-allergic women at high risk or anaphylaxis (CIII).
LaboratoriesshouldreportGBSinurineculturespecimens when present at concentrations o 104 colony-ormingunits/ml in pure culture or mixed with a second microorgan-ism (AII) (Box 4).
Iraparum Aibiic PrphylaxisIntrapartum antibiotic prophylaxis agents and dosing should
be administered according to the recommendations provided(Figure 8).
Te ollowing are key components o intrapartum antibioticprophylaxis agents and dosing: Penicillinremainstheagentofchoiceforintrapartumantibi-
otic prophylaxis, with ampicillin as an acceptable alternative(AI).
Penicillin-allergicwomenwhodo nothave ahistoryoanaphylaxis, angioedema, respiratory distress or urticariaollowing administration o a penicillin or a cephalosporinshould receive ceazolin (BII).
Antimicrobialsusceptibilitytestingshouldbeorderedforantenatal GBS cultures perormed on penicillin-allergicwomen at high risk or anaphylaxis because o a history oanaphylaxis, angioedema, respiratory distress or urticaria
BOX 1. Procedures or collecting clinical specimens or culture ogroup B Streptococcus (GBS) at 3537 weeks gestation
Swabthelowervagina(vaginalintroitus),followedbythe rectum (i.e., insert swab through the anal sphincter)using the same swab or two dierent swabs. Cultures
should be collected in the outpatient setting by thehealth-care provider or, with appropriate instruction,by the patient hersel. Cervical, perianal, perirectal orperineal specimens are not acceptable, and a speculumshould not be used or culture collection.
Place theswab(s)into a nonnutritive transportmedium. Appropriate transport systems (e.g., Stuartsor Amies with or without charcoal) are commerciallyavailable. GBS isolates can remain viable in transportmedia or several days at room temperature; howeverthe recovery o isolates declines over one to our days,especially at elevated temperatures, which can lead toalse-negative results. When easible, specimens shouldbe rerigerated beore processing.
Specimen requisitionsshould indicateclearlythatspecimens are or group B streptococcal testing.Patients who state that they are allergic to penicil-lin should be evaluated or risk or anaphylaxis. Ia woman is determined to be at high risk or ana-phylaxis,* susceptibility testing or clindamycin anderythromycin should be ordered.
* Patients with a history o any o the ollowing ater receiving penicillinor a cephalosporin are considered to be at high risk or anaphylaxis:
anaphylaxis, angioedema, respiratory distress, or urticaria.
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
20/36
18 MMWR November 19, 2010
Remove swab(s) fromtransportmedium.* Inoculateswab(s) into a recommended selective broth medium,such as odd-Hewitt broth supplemented with eithergentamicin (8 g/ml) and nalidixic acid (15 g/ml)
[ransVag broth], or with colistin (10g/ml) and nali-dixic acid (15g/ml) [Lim broth]. ransVag broth maybe supplemented with 5% debrinated sheep blood toincrease the recovery o GBS. As an alternative, swabsmay be inoculated into selective enrichment broth thatincorporates chromogenic pigments or the detectiono beta-hemolytic GBS using color detection. Exampleso appropriate commercially available options includeStrepB carrot broth or Granada Biphasic broth.
Incubateinoculated selectivebroth for1824hours3537C in ambient air or 5% CO2.
ForTransVagorLimbroth, subculture the incubated
broth to an appropriate agar plate (e.g., tryptic soy agarwith 5% debrinated sheep blood, Colombia agar withcolistin and nalidixic acid, or a commercial chromogenicagar). For chromogenic broth, monitor or color changeindicative o GBS per product instructions. GBSdetection using chromogenic broth is possible only or
beta-hemolytic strains, and thereore all broths that arenegative (i.e., no color detection) should be subculturedto a sheep blood agar plate with 5% sheep blood or testedor GBS antigen or by DNA probe to urther identiy
nonhemolytic GBS strains. Inspectagarplatesandidentifyorganismssuggestiveof
GBS (e.g., narrow zone o beta hemolysis on blood agar,gram-positive cocci, catalase-negative, and/or hippurate-positive). Note that hemolysis can be dicult to observe,so typical colonies without hemolysis should also beurther tested. I GBS is not identied ater incubationor 1824 hours, then reincubate plates overnight andexamine or suspected GBS colonies.
Variousstreptococcalgroupinglatexagglutinationtestsor other tests or GBS detection (e.g., GBS Accuprobe)may be used or specic identication, or the CAMP test
can be employed or presumptive identication. Optionaldirectbrothtesting:**DetectionofGBScan
be determined directly rom broth media using latexagglutination, probes or nucleic acid amplication tests(NAA) such as PCR.
BOX 2. Procedures or processing clinical specimens or culture o group B Streptococcus (GBS) (see Figure 7)
* Beore the inoculation step, laboratories may choose to roll the vaginal-rectal swab(s) on a blood agar plate with or without colistin and nalidixic acid orcommercially available chromogenic agar (appropriate recommendations include chromID Strepto B [which might detect both hemolytic and nonhemolyticGBS] or Granada Agar [which detects hemolytic GBS]. Source: azi A, Rglier-Poupet H, Dautezac F, Raymond J, Poyart C. Comparative evaluation oStrepto B ID chromogenic medium and Granada media or the detection o group B Streptococcusrom vaginal samples o pregnant women. J MicrobiolMethods 2008;73:2635). Tis approach should be taken only in addition to, and not instead o, inoculation into selective broth. Te directly inoculatedblood agar plate should be streaked or isolation, incubated at 3537C in ambient air or 5% CO2 or 1824 hours and inspected or organisms suggestiveo GBS as described above. I suspected colonies are conrmed as GBS, the selective broth can be discarded, thus shortening the time to obtaining culture
results. Te directly inoculated chromogenic agar should be streaked or isolation and incubated at 3537C or 1824 hours. Hemolytic GBS isolates areidentied by colored colonies as directed by specic manuacturers instructions, and selective broth can be discarded i GBS positive.Source:Fenton LJ, Harper MH. Evaluation o colistin and nalidixic acid in odd-Hewitt broth or selective isolation o groupB streptococci. J Clin Microbiol
1979;9:1679. Although rans-Vag medium oten is available without sheep blood, direct comparison o medium with and without sheep blood has shownhigher yield when blood is added. Lim broth also might benet rom the addition o sheep blood, although the improvement in yield is smaller, and sucientdata are not yet available to support a recommendation.
Sources: Church DL, Baxter H, Lloyd , Miller B, Elsayed S. Evaluation o StrepB carrot broth versus Lim broth or detection o group B Streptococcuscolonization status o near-term pregnant women. J Clin Microbiol 2008;46:27802. Martinho F, Prieto E, Pinto D, Castro RM, Morais AM, Salgado L,Exposto Fda L. Evaluation o liquid biphasic Granada medium and instant liquid biphasic Granada medium or group B Streptococcusdetection. EnermInecc Microbiol Clin 2008;26:6971.
Source: de la Rosa M, Perez M, Carazo C, Pareja L, Peis JI, Hernandez F. New Granada medium or detection and identication o group B streptococci.J Clin Microbiol 1992;30:101921.
** Direct latex agglutination, probe detection or nucleic acid amplication testing on enriched selective broth is an additional option. Sources: Guerrero C,Martinez J, Menasalvas A, Blazquez R, Rodriguez, Segovia M. Use o direct latex agglutination testing o selective broth in the detection o group B streptococcalcarriage in pregnant women. Eur J Clin Microbiol Inect Dis 2004;23:612. Goodrich JS, Miller MB. Comprison o culture and 2 real-time polymerasechain reaction assays to detect group B Streptococcusduring antepartum screening. Diagn Microbiol Inect Dis 2007;59:1722. Block , Munson E, Culver
A, Vaughan K, Hryciuk JE. Comparison o carrot broth- and selective odd-Hewitt broth-enhanced PCR protocols or real-time detection oStreptococcusagalactiaein prenatal vaginal/anorectal specimens. J Clin Microbiol 2008;46:361520. Montague NS, Cleary J, Martinez OV, Procop GW. Detection ogroup B streptococci in Lim broth by use o group B Streptococcuspeptide nucleic acid fuorescent in situ hybridization and selective and nonselective agars.
J Clin Microbiol 2008 46:34702. I a rapid test perormed on enriched broth yields positive results and antimicrobial susceptibility testing is recommended(or penicillan-allergic women at high risk or anaphylaxis), the enriched broth should be subcultured to obtain an isolate.
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
21/36
Vol. 59 / RR-10 Recommendations and Reports 19
ollowing administration o a penicillin or a cephalosporin(AII). o ensure proper testing, clinicians must inorm labo-ratories o the need or antimicrobial susceptibility testingin such cases (AIII).
Penicillin-allergicwomenathighriskforanaphylaxisshouldreceive clindamycin i their GBS isolate is susceptible to clin-damycin and erythromycin, as determined by antimicrobialsusceptibility testing; i the isolate is sensitive to clindamycinbut resistant to erythromycin, clindamycin may be usedi testing or inducible clindamycin resistance is negative(CIII). Penicillin-allergic women at high risk or anaphylaxisshould receive vancomycin i their isolate is intrinsicallyresistant to clindamycin as determined by antimicrobialsusceptibility testing, i the isolate demonstrates inducibleresistance to clindamycin, or i susceptibility to both agentsis unknown (CIII) (Box 3).
he ollowing key changes were made rom the 2002guidelines:edenition ofhighrisk for anaphylaxisis clarieda
a history o anaphylaxis, angioedema, respiratory distressor urticaria ollowing administration o a penicillin or acephalosporin.
erecommendeddosingregimenofpenicillinGis5mil-lion units intravenously, ollowed by 2.53.0 million unitintravenously every 4 hours (AII). Te range o 2.53.0 million units is recommended to achieve adequate drug levelsin the etal circulation and amniotic fuid while avoidingneurotoxicity. Te choice o dose within that range shouldbe guided by which ormulations o penicillin G are read-ily available in order to reduce the need or pharmacies tospecially prepare doses.
eClinicalandLaboratoryStandardsInstitute(CLSI)recommends disk diusion or broth microdilution testingor susceptibility testing o GBS.*Commercial systems
that have been cleared or approved or testing o strep-tococci other than S. pneumoniaealso may be used. Toensureaccurateresults,laboratoriesshouldinclude
a test or detection o inducible clindamycin resistance.he double-disk diusion method (D-zone test) isrecommended or testing erythromycin-resistant andclindamycin-susceptible GBS. Other validated tests todetect inducible clindamycin resistance in GBS may beused in place o the D-zone test.
Useacottonswabtomakeasuspensionfrom1824hourgrowth o the organism in saline or Mueller-Hinton brothequal to a 0.5 McFarland turbidity standard.
Within15minutesof adjustingtheturbidityatroomtemperature, dip a sterile cotton swab into the adjustedsuspension. Te swab should be rotated several times andpressed rmly on the inside wall o the tube above thefuid level. Use the swab to inoculate the entire suraceo a plate o Mueller-Hinton agar with 5% sheep blood.
Ater the plate is dry, use sterile orceps to place a clin-damycin (2g) disk and an erythromycin (15 g) disk12 mm apart or D-zone testing (Note: Tis diers rom
recommended 1526 mm or staphylococci and a diskdispenser cannot be used to place disks on the plate orstreptococci testing).
Incubateinoculatedagarplateat35C in 5% CO2 or2024 hours.
Isolateswith bluntingof theinhibitionzone aroundthe clindamycin disk adjacent to the erythromycin disk(D-zone positive) should be considered to have inducibleclindamycin resistance and are presumed to be resistant.(Note: Other validated tests to detect GBS with inducibleclindamycin resistance may be used.)
efollowingcommentcouldbeincludedinpatientreports
or isolates that show inducible clindamycin resistance:Tis isolate is presumed to be resistant on the basis odetection o inducible clindamycin resistance. Clindamycinstill might be eective clinically in some cases.
BOX 3. Procedures or clindamycin and erythromycin susceptibility testing o group B streptococcal (GBS) isolates, when ordered orpenicillin-allergic patients
*Source: Clinical and Laboratory Standards Institute. Perormance standard or antimicrobial susceptibility testing, M100-S20, able 2H-1, Wayne, Pa:Clinical and Laboratory Standards Institute; 2010. CLSI recommends disk diusion (M-2) or broth microdilution testing (M-7) or susceptibility testingo GBS. Commercial systems that have been cleared or approved or testing o streptococci other than S. pneumoniaemay also be used. Interpret accordingto CLSI guidelines or Streptococcus spp. Beta-hemolytic Group (2010 breakpoints or disk-diusion: or clindamycin: 19 mm = susceptible, 1618 mm =intermediate, and 15 mm = resistant; or erythromycin: 21 mm = susceptible, 1620 mm = intermediate, and 15 = resistant; or broth microdilution:clindamycin: 0.25g/ml = susceptible, 0.5g/ml = intermediate, and 1.0g/ml = resistant; and or erythromycin: 0.25g/ml = susceptible, 0.5g/ml =intermediate, and 1.0g/ml = resistant).
Sources:
ang P, Ng P, Lum M, et al. Use o the Vitek-1 and Vitek-2 systems or detection o constitutive and inducible macrolide resistance in Group Bstreptococci. J Clin Microbiol 2004;42:22824. Richter SS, Howard WJ, Weinstein MP, et al. Multicenter evaluation o the BD Phoenix automated microbiologysystem or antimicrobial susceptibility testing o Streptococcus species. J Clin Microbiol 2008;45:286371.
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
22/36
20 MMWR November 19, 2010
Erythromycin isno longer anacceptable alternative forintrapartum GBS prophylaxis or penicillin-allergic womenat high risk or anaphylaxis.
oher obseric Maageme Issues AvailabledataarenotsucienttosuggestthatGBScoloni-
zation should dierentially aect the use o obstetric proce-
dures or monitoring, cervical ripening or labor inductionTese procedures should be reserved or appropriate indications and not altered or GBS-colonized women (CIII).
Dataarenotsucienttomakerecommendationsregardingthe timing o procedures intended to acilitate progressiono labor, such as amniotomy, in GBS-colonized womenIntrapartum antibiotic prophylaxis is optimal i administered
FIGURE 7. Algorithm or recommended laboratory testing or prenatal screening or group B streptococcal (GBS) colonization*
* See Boxes 13 or details on specimen processing and antimicrobial susceptibility testing. Direct plating with appropriate media may be done in addition to enriched culture. Direct plating should not be used as the sole means to identiy GBS.
Vaginal-rectal swab
Enrichment broth (can use nonigmented or pigmented broth)Incubate 1824 hrs at 3537C
Subculture to appropriate media;
incubate 1824 hrs at 3537C
DNA probe, latex agglutination or
nucleic acid amplication test (NAAT)
Nonpigmented broth Pigmented broth
Further testing (cansubculture or use
rapid tests) No indicator color growth GBS indicator color observed
Identify GBS byrecommended method*
GBS+GBS-
Reincubate overnight
Report as GBS-
GBS-
GBS+Report as GBS+
GBS+GBS-
Report as GBS-
Antimicrobial susceptibility testing if penicillin-allergic and at high risk for anaphylaxis*
Report as GBS+
-
8/3/2019 Prevencin de la enfermedad perinatal por Streptococcus agalactiae
23/36
Vol. 59 / RR-10 Recommendations and Reports 21
or at least 4 hours beore delivery; thereore, such proceduresshould be timed accordingly, i possible (CIII).
Nomedically necessaryobstetricprocedure should bedelayed in order to achieve 4 hours o GBS prophylaxisbeore delivery (AIII).
Secdary PreveiAmg Ias
o detect potential sepsis cases in newborns as early as pos-sible, newborns should be managed according to the algorithmprovided (Figure 9).Te ollowing arekey components o the neonatal man-agement algorithm: Anynewbornwith signs of sepsis
should receive a ull diagnostic evalu-ation and receive antibiotic therapypending the results o the evaluation.
Te evaluation should include a bloodculture; a CBC including white bloodcell dierential and platelet count;a chest radiograph i any abnormalrespiratory signs are present; and alumbar puncture i the newborn isstable enough to tolerate the procedureand sepsis is suspected. Terapy or theinant should include antimicrobialagents active against GBS (includingintravenous ampicillin) as well as otherorganisms that might cause neonatalsepsis, such as E. coli(AII).
Well-appearingnewbornswhosemoth-ers had suspected chorioamnionitisshould undergo a limited evaluationand receive antibiotic therapy pendingculture results (AII). Te evaluationshould include a blood culture and aCBC including white blood cell di-erential and platelet count; no chestradiograph or lumbar puncture isneeded. Consultation with obstetric
providers to assess whether chorioam-nionitis was suspected is importantto determine neonatal management(CIII).
Well-appearinginfantswhosemoth-ers had no chorioamnionitis andno indication or GBS prophylaxisshould be managed according toroutine clinical care (CIII).
BOX 4. Identifcation o group B Streptococcus (GBS) bacteriuria inpregnant women
Routine screening for asymptomaticbacteriuria isrecommended in pregnant women, and laboratoriesshould screen urine culture specimens or the presenceo GBS in concentrations o 104 colony-orming units(cu)/ml or greater.
Laboratories should identifyGBSwhenpresent at104 cu/ml in pure culture or mixed with a secondmicroorganism.
FIGURE 8. Recommended regimens or intrapartum antibiotic prophylaxis or prevention oearly-onset group B streptococcal (GBS) disease*
Abbreviation: IV = intravenously.* Broader spectrum agents, including an agent active against GBS, might be necessary or treatment o
chorioamnionitis. Doses ranging rom 2.5 to 3.0 million units are acceptable or the doses administered every 4 hours ol
lowing the initial dose. The choice o dose within that range should be guided by which ormulations openicillin G are readily available to reduce the need or pharmacies to specially prepare doses.
Penicillin-allergic patients with a history o anaphylaxis, angioedema, respiratory distress, or urticariaollowing administration o penicillin or a cephalosporin are considered to be at high r isk or anaphylaxi
and should not receive penicillin, ampicillin, or ceazolin or GBS intrapartum prophylaxis. For penicillinallergic patients who do not have a history o those reactions, ceazolin is the preerred agent becausepharmacologic data suggest it achieves efective intraamniotic concentrations. Vancomycin and clindamycin should be reserved or penicillin-allergic women at high risk or anaphylaxis.
I laboratory acilities are adequate, clindamycin and erythromycin susceptibility testing (Box 3) should beperormed on prenatal GBS isolates rom penicillin-allergic women at high risk or anaphylaxis. I no susceptibility testing is perormed, or the results are not available at the time o labor, vancomycin is the pree