PREVAIL: 5-Year Outcomes From a Randomized Trial of …€¢ Both protocols specified 5 years of...
28
PREVAIL : 5 - Year Outcomes From a Randomized Trial of Left Atrial Appendage Closure vs Medical Therapy in Patients With Nonvalvular Atrial Fibrillation Dr . Saibal Kar , MD TCT 2017 Late Breaking Clinical Trial Denver, CO USA Authors : V Reddy, S Doshi; S Kar, D Gibson, M Price, K Huber, R Horton, M Buchbinder, P Neuzil, N Gordon, DR Holmes Jr on behalf of the PREVAIL and PROTECT-AF Investigators
-
Upload
nguyenthuy -
Category
Documents
-
view
214 -
download
1
Transcript of PREVAIL: 5-Year Outcomes From a Randomized Trial of …€¢ Both protocols specified 5 years of...

PREVAIL: 5-Year Outcomes From a Randomized Trial of Left Atrial Appendage Closure vs Medical
Therapy in Patients With NonvalvularAtrial Fibrillation
Dr. Saibal Kar, MD
TCT 2017 Late Breaking Clinical Trial
Denver, CO USA
Authors: V Reddy, S Doshi; S Kar, D Gibson, M Price, K Huber, R
Horton, M Buchbinder, P Neuzil, N Gordon, DR Holmes Jr on behalf of
the PREVAIL and PROTECT-AF Investigators

Disclosures
• Dr. Kar
Has received research grants from and
served as a consultant for Abbott Vascular
and Boston Scientific;
Has served as a member of the advisory
board for left atrial appendage closure;
Is the national principal investigator of the
Continuous Access Registries (CAP & CAP2);
Has served as a proctor for Boston Scientific.

Background
• PROTECT AF and PREVAIL were RCTs comparing left atrial
appendage closure (LAAC) with WATCHMAN to warfarin
• PROTECT-AF demonstrated similar stroke reduction to
warfarin (at a mean of 3.8 years follow up)
JAMA 312:1988-98 (2014)
• PREVAIL produced inconclusive findings due to a warfarin
cohort with an implausibly low ischemic stroke rate, relatively
few patients and relatively short follow up (~10 months)
JACC 64:1-12 (2014)
• Both protocols specified 5 years of follow-up for all patients
5 year follow up completed in 2013 (final)
5 year follow up completed in 2017 (final)

Objectives
• To report the final, 5 year results of
PREVAIL, both alone and as part of a
patient-level meta-analysis with
PROTECT-AF final 5 year data

Methods
PREVAIL
PREVAIL efficacy endpoints were never designed to be analyzed
without the informative prior from PROTECT AF.
• 1st Primary efficacy: Comparison of rate ratios of 18-month event
rates for composite of stroke, SE, and CV/Unexplained death; Upper
CrI 1.75 for NI
• 2nd primary efficacy: 1-tailed test, either the ratio or the difference
between rates of ischemic stroke or SE >7 days post implant in the
two arms satisfied the non-inferiority criteria, using 95% upper
credible intervals (CrI) <2.0 and <0.0275, respectively, and posterior
probability for non-inferiority ≥ 97.5%.
• All analyses ITT; rates are events per 100 patient-years (indicated for
simplicity by %).
All PREVAIL analysis were pre-specified to use an informative
prior that included a portion of PROTECT AF

Methods
Patient-Level Meta-Analysis
• ITT: censoring data from patients without events at the time of the
last known status
• Disabling Strokes: increase in the Modified Rankin Score (MRS)
by at least 2 points
• Comparison of Event Rates: Cox proportional hazards model
with confidence intervals (CIs)
Stratified by study to account for differences in risk profiles
Kaplan-Meier curves used for graphical assessment of time-
dependent events
Frequentist statistics and 2-sided p-values nominally significant at p <
0.05, without adjustment for multiple comparisons

Follow-up
TrialNumber of Patients
TotalMean Follow-
up (months)
Total
Patient
YearsDevice Control
PROTECT AF 463 244 707 47.6 ± 21.3 2,717
PREVAIL-only* 269 138 407 47.9 ± 19.4 1,626
Total 732 382 1114 4,343* Does not include PROTECT AF informative prior from Bayesian model

Demographics: Combined Cohort Endpoint
for Patient-Level Meta Analysis Characteristic
Device
N=732
Control
N=382p-value
Age, years 72.6±8.4 73.5±8.6 0.09
Sex, male 69.4 71.7 0.42
CHADS2 Score 2.3±1.1 2.4±1.2 0.06
CHA2DS2-Vasc Score 3.6 ± 1.4 3.9 ± 1.5 0.02
Risk Factors
CHF 25.5 25.7 0.97
Hypertension 89.2 92.7 0.06
Age ≥ 75 years 40.4 43.2 0.38
Diabetes 27.9 29.6 0.55
Prior Stroke/TIA 22.1 23.6 0.59
AF Pattern
Paroxysmal 45.2 44.5 0.82
Persistent 24.9 23.3 0.56
Permanent 27.6 30.1 0.38
Unknown 1.4 0.8 0.56
Paced 1.0 1.3 0.56

Demographics: Combined Cohort Endpoint
for Patient-Level Meta Analysis Characteristic
Device
N=732
Control
N=382p-value
Age, years 72.6±8.4 73.5±8.6 0.09
Sex, male 69.4 71.7 0.42
CHADS2 Score 2.3±1.1 2.4±1.2 0.06
CHA2DS2-Vasc Score 3.6 ± 1.4 3.9 ± 1.5 0.02
Risk Factors
CHF 25.5 25.7 0.97
Hypertension 89.2 92.7 0.06
Age ≥ 75 years 40.4 43.2 0.38
Diabetes 27.9 29.6 0.55
Prior Stroke/TIA 22.1 23.6 0.59
AF Pattern
Paroxysmal 45.2 44.5 0.82
Persistent 24.9 23.3 0.56
Permanent 27.6 30.1 0.38
Unknown 1.4 0.8 0.56
Paced 1.0 1.3 0.56

RESULTS

Results
PREVAIL Efficacy
Dataset
Device
18-Month
Rate
Control
18-Month
Rate
18-Month Rate
Ratio
(95% CrI)
Criteria Met?
95% CrI Upper
Bound < 1.75
Posterior
Probability
Non-
inferiority
(PNI ≥97.5%)
First Primary Endpoint (ITT) - stroke, SE, and CV/Unexplained Death
Primary analysis
(Jan 2013)0.064 0.063
1.07
(0.57, 1.89)No 93%
1st Post Hoc Analysis
(Jun 2014)0.065 0.057
1.21
(0.69, 2.05)No 93%
Final 5-Year Analysis
(Sep 2017)0.066 0.051
1.33
(0.78, 2.13)No 88.4%
Dataset
Device
18-Month
Rate
Control
18-Month
Rate
18-Month Rate
Ratio
(95% CrI)
Criteria Met?
95% CI Upper
Bound < 2.0
18-Month Rate
Difference
(95% CrI)
Criteria Met?
95% CrI
Upper Bound
< 0.0275
Posterior
Probability
Non-
inferiority
(PNI ≥97.5%)
Second Primary Endpoint (ITT) – ischemic stroke or SE >7 days Must meet at least one criteria
Primary analysis
(Jan 2013)0.0253 0.0200
1.6
(0.5, 4.2)No
0.0053
(-0.0190, 0.0273)Yes 97.6
1st Post Hoc Analysis
(Jun 2014)0.0294 0.0131
2.8
(0.9, 7.3)No
0.0163
(-0.0023, 0.0342)No 89.2
Final 5-Year Analysis
(Sep 2017)0.0255 0.0135
2.2
(0.8, 4.9)No
0.0120
(-0.0036, 0.0275)Yes 97.5%
* Upper CrI is displayed as 0.0275, but if all significant digits were displayed, it is less than upper bound of 0.0275

Results
PREVAIL 2nd Endpoint Met
Dataset
Device
18-Month
Rate
Control
18-Month
Rate
18-Month Rate
Ratio
(95% CrI)
Criteria Met?
95% CrI Upper
Bound < 1.75
Posterior
Probability
Non-
inferiority
(PNI ≥97.5%)
First Primary Endpoint (ITT) - stroke, SE, and CV/Unexplained Death
Primary analysis
(Jan 2013)0.064 0.063
1.07
(0.57, 1.89)No 93%
1st Post Hoc Analysis
(Jun 2014)0.065 0.057
1.21
(0.69, 2.05)No 93%
Final 5-Year Analysis
(Sep 2017)0.066 0.051
1.33
(0.78, 2.13)No 88.4%
Dataset
Device
18-Month
Rate
Control
18-Month
Rate
18-Month Rate
Ratio
(95% CrI)
Criteria Met?
95% CI Upper
Bound < 2.0
18-Month Rate
Difference
(95% CrI)
Criteria Met?
95% CrI
Upper Bound
< 0.0275
Posterior
Probability
Non-
inferiority
(PNI ≥97.5%)
Second Primary Endpoint (ITT) – ischemic stroke or SE >7 days Must meet at least one criteria
Primary analysis
(Jan 2013)0.0253 0.0200
1.6
(0.5, 4.2)No
0.0053
(-0.0190, 0.0273)Yes 97.6
1st Post Hoc Analysis
(Jun 2014)0.0294 0.0131
2.8
(0.9, 7.3)No
0.0163
(-0.0023, 0.0342)No 89.2
Final 5-Year Analysis
(Sep 2017)0.0255 0.0135
2.2
(0.8, 4.9)No
0.0120
(-0.0036, 0.0275)Yes 97.5%
* Upper CrI is displayed as 0.0275, but if all significant digits were displayed, it is less than upper bound of 0.0275

Results
PROTECT AF and PREVAIL Event Rates
PROTECT-AF Subjects PREVAIL Subjects
Device
(n=463)
Control
(n=244)
Device
(n=269)
Control
(n=138)
No. of
Events Rate *
No. of
Events Rate * p-value
No. of
Events Rate *
No. of
Events Rate * p-value
2:1 Randomization
Primary Efficacy:
Stroke/SE/CV Death40 / 1787.7 2.24 34 / 929.4 3.66 0.04 37 / 1038.3 3.65 15 / 530.4 2.94 0.47
All Stroke 26 / 1781.7 1.46 20 / 929.4 2.15 0.23 19 / 1042.4 1.97 7 / 530.4 1.29 0.32
Ischemic Stroke 24 / 1781.7 1.35 10 / 932.8 1.07 0.49 17 / 1043.1 1.68 4 / 533.3 0.73 0.13
Hemorrhagic Stroke 3 / 1837.7 0.16 10 / 945.6 1.06 0.005 2 / 1084.6 0.18 3 / 538.0 0.54 0.23
Systemic Embolism 3 / 1837.1 0.16 0 n/a n/a 1 / 1080.6 0.09 0 / 540.9 n/a n/a
CV/Unexplained Death 19 / 1843.2 1.03 22 / 948.9 2.32 0.009 18 / 1084.7 1.79 10 / 540.9 1.98 0.76
* Events are per 100 patient-years

PROTECT AF ResultsWATCHMAN Superior Efficacy, Hemorrhagic
Stroke, CV Death
PROTECT-AF Subjects PREVAIL Subjects
Device
(n=463)
Control
(n=244)
Device
(n=269)
Control
(n=138)
No. of
Events Rate *
No. of
Events Rate * p-value
No. of
Events Rate *
No. of
Events Rate * p-value
2:1 Randomization
Primary Efficacy:
Stroke/SE/CV Death40 / 1787.7 2.24 34 / 929.4 3.66 0.04 37 / 1038.3 3.65 15 / 530.4 2.94 0.47
All Stroke 26 / 1781.7 1.46 20 / 929.4 2.15 0.23 19 / 1042.4 1.97 7 / 530.4 1.29 0.32
Ischemic Stroke 24 / 1781.7 1.35 10 / 932.8 1.07 0.49 17 / 1043.1 1.68 4 / 533.3 0.73 0.13
Hemorrhagic Stroke 3 / 1837.7 0.16 10 / 945.6 1.06 0.005 2 / 1084.6 0.18 3 / 538.0 0.54 0.23
Systemic Embolism 3 / 1837.1 0.16 0 n/a n/a 1 / 1080.6 0.09 0 / 540.9 n/a n/a
CV/Unexplained Death 19 / 1843.2 1.03 22 / 948.9 2.32 0.009 18 / 1084.7 1.79 10 / 540.9 1.98 0.76
* Events are per 100 patient-years

PREVAIL ResultsWATCHMAN Comparable For Efficacy
Control Group Continued To Overperform
PROTECT-AF Subjects PREVAIL Subjects
Device
(n=463)
Control
(n=244)
Device
(n=269)
Control
(n=138)
No. of
Events Rate *
No. of
Events Rate * p-value
No. of
Events Rate *
No. of
Events Rate * p-value
2:1 Randomization
Primary Efficacy:
Stroke/SE/CV Death40 / 1787.7 2.24 34 / 929.4 3.66 0.04 37 / 1038.3 3.65 15 / 530.4 2.94 0.47
All Stroke 26 / 1781.7 1.46 20 / 929.4 2.15 0.23 19 / 1042.4 1.97 7 / 530.4 1.29 0.32
Ischemic Stroke 24 / 1781.7 1.35 10 / 932.8 1.07 0.49 17 / 1043.1 1.68 4 / 533.3 0.73 0.13
Hemorrhagic Stroke 3 / 1837.7 0.16 10 / 945.6 1.06 0.005 2 / 1084.6 0.18 3 / 538.0 0.54 0.23
Systemic Embolism 3 / 1837.1 0.16 0 n/a n/a 1 / 1080.6 0.09 0 / 540.9 n/a n/a
CV/Unexplained Death 19 / 1843.2 1.03 22 / 948.9 2.32 0.009 18 / 1084.7 1.79 10 / 540.9 1.98 0.76
* Events are per 100 patient-years
2:1 randomization
Control Group continues to overperform
Rate = 0.7%
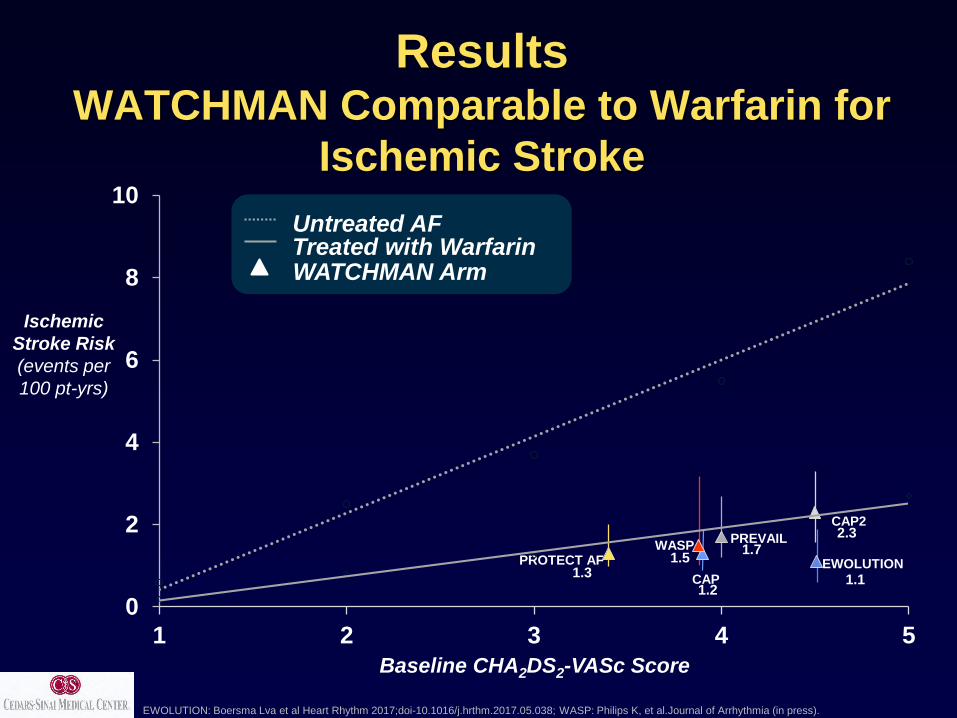
Ischemic
Stroke Risk
(events per
100 pt-yrs)
PREVAIL
PROTECT AF
Untreated AFTreated with WarfarinWATCHMAN Arm
CAP2
CAP
Baseline CHA2DS2-VASc Score
EWOLUTION
WASP
ResultsWATCHMAN Comparable to Warfarin for
Ischemic Stroke
EWOLUTION: Boersma Lva et al Heart Rhythm 2017;doi-10.1016/j.hrthm.2017.05.038; WASP: Philips K, et al.Journal of Arrhythmia (in press).
1.3
1.2
1.7
2.3
1.1
1.5
0
2
4
6
8
10
1 2 3 4 5

HR
p-
value
Efficacy 0.82 0.3
All stroke or SE 0.96 0.9
Ischemic stroke or SE 1.7 0.08
Hemorrhagic stroke 0.2 0.0022
Ischemic stroke or SE >7 days 1.4 0.3
CV/unexplained death 0.59 0.03
All-cause death 0.73 0.04
Major bleed, all 0.91 0.6
Major bleeding, non procedure-related 0.48 0.0003
0.01 0.1 1 10
Favors WATCHMAN Favors warfarin
Hazard Ratio (95% CI)
Patient-Level Meta-Analysis
PROTECT AF and PREVAIL 5 years

HR
p-
value
Efficacy 0.82 0.3
All stroke or SE 0.96 0.9
Ischemic stroke or SE 1.7 0.08
Hemorrhagic stroke 0.2 0.0022
Ischemic stroke or SE >7 days 1.4 0.3
CV/unexplained death 0.59 0.03
All-cause death 0.73 0.04
Major bleed, all 0.91 0.6
Major bleeding, non procedure-related 0.48 0.0003
0.01 0.1 1 10
Favors WATCHMAN Favors warfarin
Hazard Ratio (95% CI)
Patient-Level Meta-AnalysisWATCHMAN Comparable To Warfarin For Ischemic Stroke

HR
p-
value
Efficacy 0.82 0.3
All stroke or SE 0.96 0.9
Ischemic stroke or SE 1.7 0.08
Hemorrhagic stroke 0.2 0.0022
Ischemic stroke or SE >7 days 1.4 0.3
CV/unexplained death 0.59 0.03
All-cause death 0.73 0.04
Major bleed, all 0.91 0.6
Major bleeding, non procedure-related 0.48 0.0003
0.01 0.1 1 10
Favors WATCHMAN Favors warfarin
Hazard Ratio (95% CI)
Patient-Level Meta-AnalysisWATCHMAN Superior for Hemorrhagic Stroke, CV Death,
All-Cause Death, Post-procedure Bleeding

Patient-Level Meta-Analysis
WATCHMAN Superior Reduction in Disabling
Strokes
0.00%
0.50%
1.00%
1.50%
2.00%
WATCHMAN warfarin
Disabling/Fatal Strokes Non-Disabling Strokes
Disabling Stroke defined as MRS ≥2
Two strokes in PREVAIL are excluded because the baseline MRS score was unavailable

Patient-Level Meta-Analysis
WATCHMAN Superior Reduction in Disabling
Strokes
0.00%
0.50%
1.00%
1.50%
2.00%
WATCHMAN warfarin
Disabling/Fatal Strokes Non-Disabling Strokes
Disabling Stroke defined as MRS ≥2
Two strokes in PREVAIL are excluded because the baseline MRS score was unavailable
HR 0.45 (0.21 – 0.94)
P=0.03
55%
Reduction

Subgroup
Interaction
p-value
Age< 75
0.98> 75
SexFemale
0.94Male
CHADS2
Score
≤ 30.47
>3
CHA2DS2-
VASc Score
≤ 40.13
>4
HAS-BLED≤ 2
0.054>2
History of TIA
Stroke
No0.35
Yes
Hazard Ratio
Favors WATCHMAN Favors warfarin
Patient-Level Meta-Analysis
No Significant Difference In Outcomes By Patient Subset
0.1 1.0 10.0

Subgroup
Interaction
p-value
Age< 75
0.98> 75
SexFemale
0.94Male
CHADS2
Score
≤ 30.47
>3
CHA2DS2-
VASc Score
≤ 40.13
>4
HAS-BLED≤ 2
0.054>2
History of TIA
Stroke
No0.35
Yes
Hazard Ratio
Favors WATCHMAN Favors warfarin
Patient-Level Meta-Analysis
No Significant Difference In Outcomes By Patient Subset
0.1 1.0 10.0

Summary
PREVAIL 5 year follow-up demonstrates:
• 2nd primary endpoint meets non-inferiority while the 1st
endpoint remains unchanged
• No significant differences between WATCHMAN and warfarin
for primary efficacy measures despite an implausibly low rate
of ischemic stroke (0.73%) in the control arm
Meta-Analysis of PROTECT AF and PREVAIL with 5 year
follow-up demonstrates:
• Comparable efficacy and stroke rates, with no significant
differnce across subgroups
• No significant differences in ischemic stroke rates versus
warfarin
• Significant, superior reductions in disabling strokes, non-
procedural bleeding, and mortality
*Kaplan Meier Rate

Conclusion
Long term 5-year outcomes of 2 RCTs demonstrate
• LAAC with the Watchman device provides stroke
prevention in NVAF patients to a similar degree
as oral anticoagulation
• By minimizing major bleeding, particularly
hemorrhagic stroke, LAAC results in less
disability or death than warfarin
For patients who are poor candidates for long-term oral
anticoagulation, left atrial appendage closure is a reasonable
strategy for stroke prophylaxis

Conclusion
Long term 5-year outcomes of 2 RCTs demonstrate
• LAAC with the Watchman device provides stroke
prevention in NVAF patients to a similar degree
as oral anticoagulation
• By minimizing major bleeding, particularly
hemorrhagic stroke, LAAC results in less
disability or death than warfarin
For patients who are poor candidates for long-term oral
anticoagulation, left atrial appendage closure is a reasonable
strategy for stroke prophylaxis
WE HAVE PREVAILED!

ABBREVIATED STATEMENT (US)
WATCHMANTM Left Atrial Appendage Closure Device
with Delivery System and WATCHMAN Access System
INDICATIONS FOR USE
The WATCHMAN Device is indicated to reduce the risk of thromboembolism from the left atrial appendage in patients with non-valvular atrial fibrillation who:
• Are at increased risk for stroke and systemic embolism based on CHADS2 or CHA2DS2-VASc scores and are recommended for anticoagulation therapy;
• Are deemed by their physicians to be suitable for warfarin; and
• Have an appropriate rationale to seek a non-pharmacologic alternative to warfarin, taking into account the safety and effectiveness of the device compared to warfarin.
The WATCHMAN Access System is intended to provide vascular and transseptal access for all WATCHMAN Left Atrial Appendage Closure Devices with Delivery Systems.
CONTRAINDICATIONS
Do not use the WATCHMAN Device if:
• Intracardiac thrombus is visualized by echocardiographic imaging.
• An atrial septal defect repair or closure device or a patent foramen ovale repair or closure device is present.
• The LAA anatomy will not accommodate a device. See Table 46 in the DFU.
• Any of the customary contraindications for other percutaneous catheterization procedures (e.g., patient size too small to accommodate TEE probe or required catheters) or conditions (e.g., active infection,
bleeding disorder) are present.
• There are contraindications to the use of warfarin, aspirin, or clopidogrel.
• The patient has a known hypersensitivity to any portion of the device material or the individual components (see Device Description section) such that the use of the WATCHMAN Device is contraindicated.
WARNINGS
• Device selection should be based on accurate LAA measurements obtained using fluoro and ultrasound guidance (TEE recommended) in multiple angles (e.g., 0º, 45º, 90º, 135º).
• Do not release the WATCHMAN Device from the core wire if the device does not meet all release criteria.
• If thrombus is observed on the device, warfarin therapy is recommended until resolution of thrombus is demonstrated by TEE.
• The potential for device embolization exists with cardioversion <30 days following device implantation. Verify device position post-cardioversion during this period.
• Administer appropriate endocarditis prophylaxis for 6 months following device implantation. The decision to continue endocarditis prophylaxis beyond 6 months is at physician discretion.
• For single use only. Do not reuse, reprocess, or resterilize.
PRECAUTIONS
• The safety and effectiveness (and benefit-risk profile) of the WATCHMAN Device has not been established in patients for whom long-term anticoagulation is determined to be contraindicated.
• The LAA is a thin-walled structure. Use caution when accessing the LAA and deploying the device.
• Use caution when introducing the WATCHMAN Access System to prevent damage to cardiac structures.
• Use caution when introducing the Delivery System to prevent damage to cardiac structures.
• To prevent damage to the Delivery Catheter or device, do not allow the WATCHMAN Device to protrude beyond the distal tip of the Delivery Catheter when inserting the Delivery System into the Access Sheath.
• If using a power injector, the maximum pressure should not exceed 100 psi.
• In view of the concerns that were raised by the RE-ALIGN1 study of dabigatran in the presence of prosthetic mechanical heart valves, caution should be used when prescribing oral anticoagulants other than
warfarin in patients treated with the WATCHMAN Device. The WATCHMAN Device has only been evaluated with the use of warfarin post-device implantation.
ADVERSE EVENTS
Potential adverse events (in alphabetical order) which may be associated with the use of a left atrial appendage closure device or implantation procedure include but are not limited to:
Air embolism, Airway trauma, Allergic reaction to contrast media/medications or device materials, Altered mental status, Anemia requiring transfusion, Anesthesia risks, Angina, Anoxic encephalopathy, Arrhythmias,
Atrial septal defect , AV fistula , Bruising, hematoma or seroma, Cardiac perforation , Chest pain/discomfort, Confusion post procedure, Congestive heart failure, Contrast related nephropathy, Cranial bleed,
Decreased hemoglobin, Deep vein thrombosis, Death, Device embolism, Device fracture, Device thrombosis, Edema, Excessive bleeding, Fever, Groin pain, Groin puncture bleed, Hematuria, Hemoptysis,
Hypotension, Hypoxia, Improper wound healing, Inability to reposition, recapture, or retrieve the device, Infection / pneumonia, Interatrial septum thrombus, Intratracheal bleeding, Major bleeding requiring transfusion,
Misplacement of the device / improper seal of the appendage / movement of device from appendage wall, Myocardia erosion, Nausea, Oral bleeding, Pericardial effusion / tamponade, Pleural effusion, Prolonged
bleeding from a laceration, Pseudoaneurysm, Pulmonary edema, Renal failure, Respiratory insufficiency / failure, Surgical removal of the device, Stroke – Ischemic , Stroke – Hemorrhagic, Systemic embolism, TEE
complications (throat pain, bleeding, esophageal trauma), Thrombocytopenia, Thrombosis, Transient ischemic attack (TIA), Valvular damage, Vasovagal reactions
There may be other potential adverse events that are unforeseen at this time.
CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician. Rx only. Prior to use, please see the complete “Directions for Use” for more information on Indications, Contraindications,
Warnings, Precautions, Adverse Events, and Operator’s Instructions.
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved.1Eikelboom JW, Connolly SJ, Brueckmann M, et al. N Engl J Med 2013;369:1206-14.






![vasc dentopar[1]](https://static.fdocuments.in/doc/165x107/577c7ab51a28abe05495f271/vasc-dentopar1.jpg)