
Placenta previa Placenta previa Placental abruption Women ’ s Hospital School of Medicine Zhejiang...
36
Placenta previa Placenta previa Placental abruption Women’s Hospital School of Medicine Women’s Hospital School of Medicine Zhejiang University Zhejiang University Wang Zhengping Wang Zhengping
-
Upload
bartholomew-morris -
Category
Documents
-
view
236 -
download
2
Transcript of Placenta previa Placenta previa Placental abruption Women ’ s Hospital School of Medicine Zhejiang...

Placenta previaPlacenta previa Placental abruption
Placenta previaPlacenta previa Placental abruption
Women’s Hospital School of Medicine Women’s Hospital School of Medicine Zhejiang UniversityZhejiang University
Wang ZhengpingWang Zhengping

Antepartum Hemorrhage
• Third-trimester bleedingObstetric: Placental separationPlacental Previa Placenta Abruption Uterine Rupturevasa previa : Fetal Vessel RuptureNo obstetric: Acute vaginitis/cervicitis,
Cervical polyp, Cervical cancer, Trauma

Placenta previaPlacenta previa
Definition
• Placenta previa: The inferior edge of placenta load at
the lower uterine segment, or even reach the internal cervical os after 28 weeks gestation.
• Incidence rate: Internal : 0.24%~1.57% ; International : 0.5%~0.9% 。

Etiology• High-risk group
Age of gravida>35 Multipara Pregnancy women used to tobacco or dope
• Initial etiologic agnet Damage of endometria Development of the trophoblastic layer of fertilized ovum delayed Anomaly of placenta Cicatricial uterus due to cesarean
section ,e.g.

Classification Classified according to the
relationship between the edge of placenta and the internal cervical os :
complete ( central ) placenta previa partial placenta previa marginal placenta previa
Time to determine classification : the last examination before managed
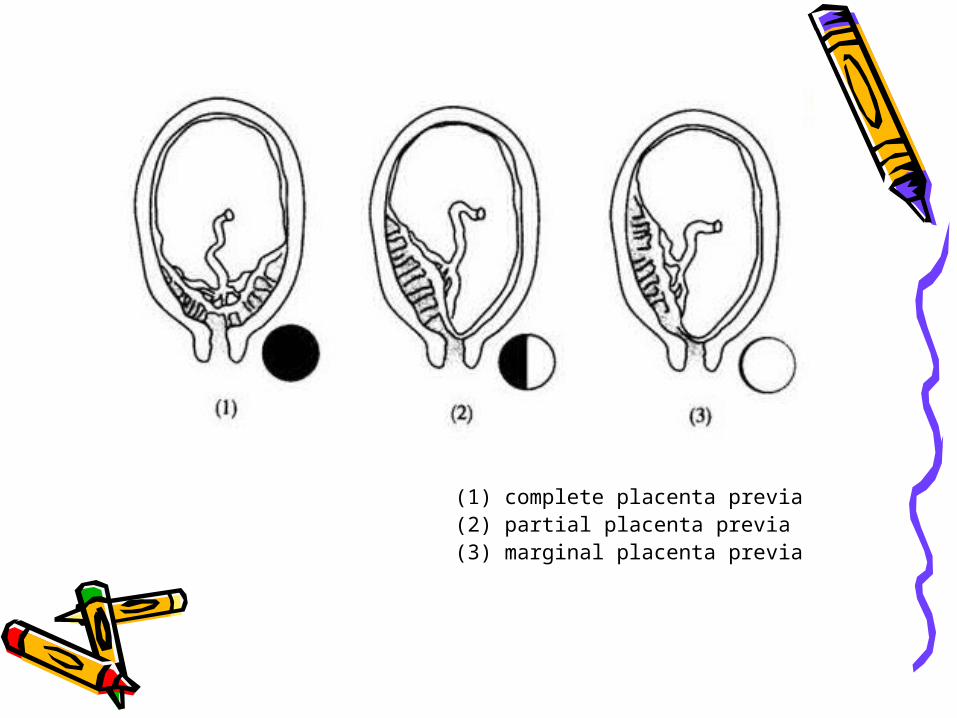
(1) complete placenta previa (2) partial placenta previa (3) marginal placenta previa
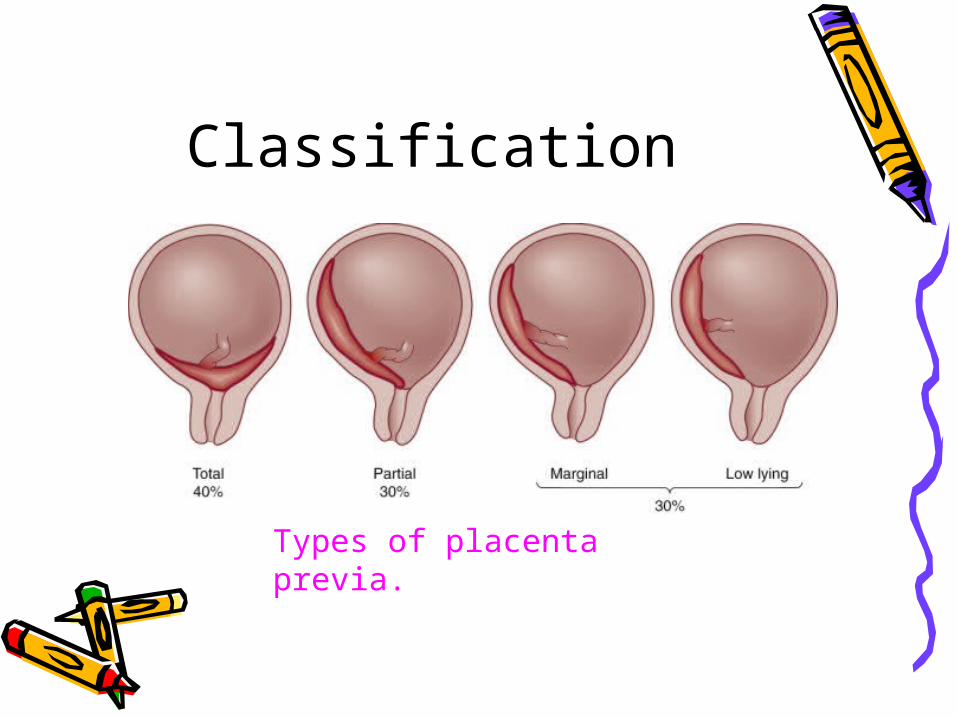
Classification
Types of placenta previa.
Clinical Features Painless 、 recurrent vaginal bleeding in
the second or third trimester of pregnancy
Anemia,shock or even death corresponded to the volume of vaginal bleeding
The uterus is usually soft and relaxed Anomaly of fetal condition Per vagina examination
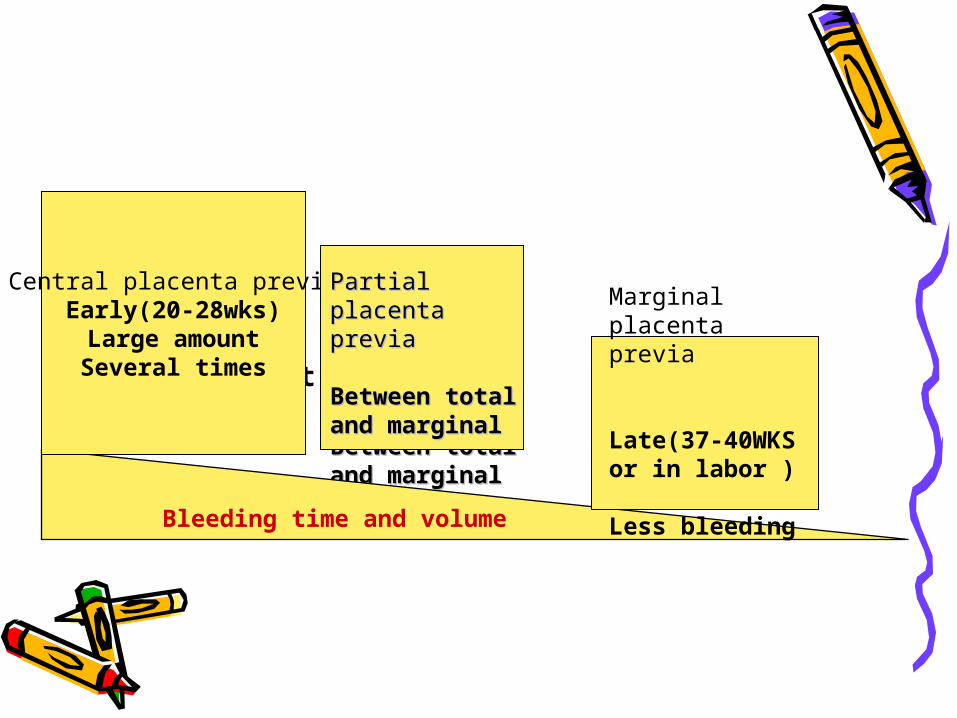
• Total placenta previa
• Early(20-28wks)
• Large amount
• Several times
Partial placenta Partial placenta previaprevia
Between total Between total and marginaland marginal
Marginal placenta previa Late(37-40WKS or in labor ) Less bleeding Bleeding time and volume
Central placenta previaEarly(20-28wks)Large amountSeveral times
Partial placenta Partial placenta previaprevia Between total and Between total and marginalmarginal
Marginal placenta previa Late(37-40WKS or in labor ) Less bleeding
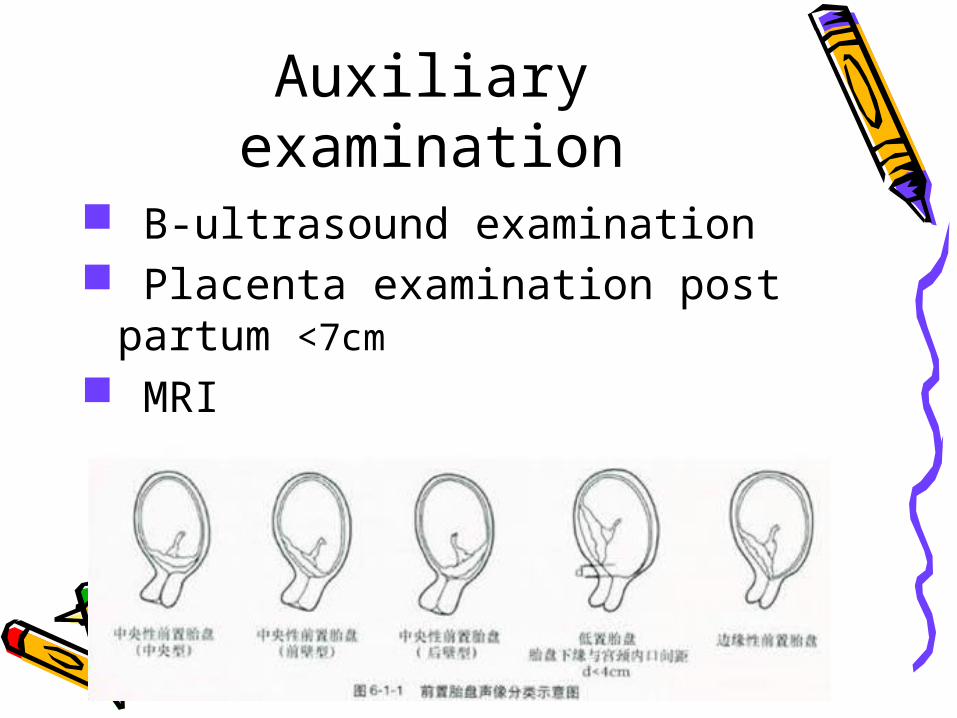
Auxiliary examination B-ultrasound examination Placenta examination post
partum <7cm
MRI

marginal placenta previa

partial placenta previa
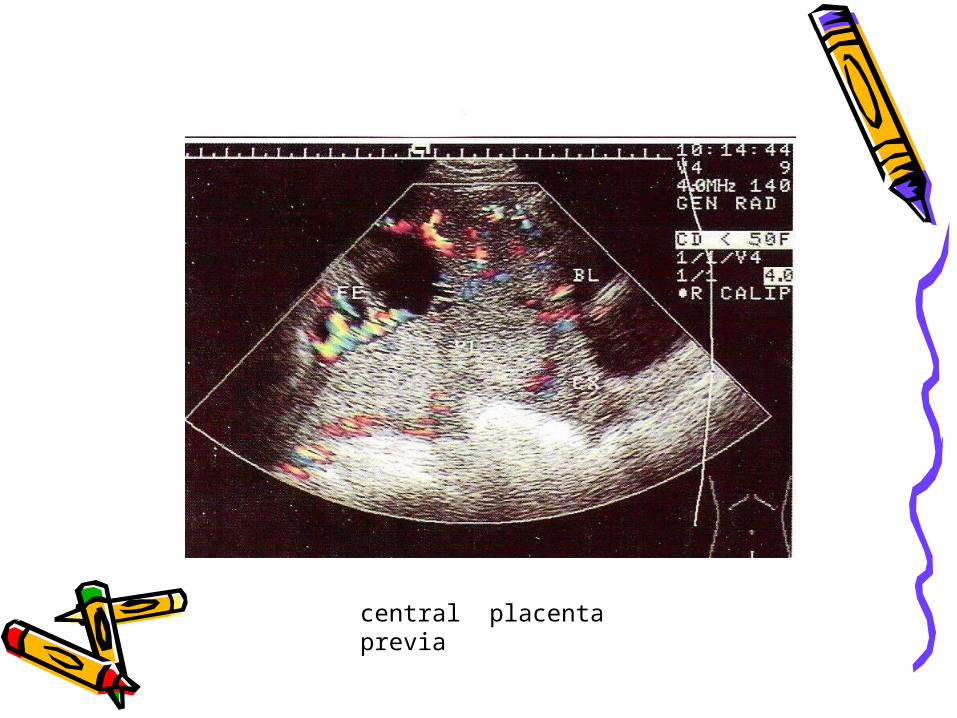
central placenta previa

Differential diagnosis• Placental abruption• Disruption of vasa previa• Cervical polyp or erosion• Cancer of cervix
Complication of mother and fetus
Bleeding at or post partum Implantation of placenta Anemia and puerperal infection Premature delivery

Implantation of placenta
Management expectant treatment
Indication: Fewer vaginal bleeding
Patient’s condition stabilization <36 weeks gestation, fetal weight<2300g
Management: Lying in bed to take a rest
Inhibition of uterine contraction Treatment aim at symptoms Promote development of fetus Prevention of infection

Termination of pregnancyIndication: 1.Severe vaginal bleeding 2.Gestation age >36 weeks, or fetal lung function been matured
Mode of labor:According to the type of placenta previa,volume of vaginal bleeding and condition of gravia, et al.Cesarean delivery is necessary in practically all
women with placental previa


Transport in emergency condition
In the neighborhood Initiatory management

Placental abruption
Definition
Placental abruption: placenta in normal site strip from the uterine parietal partially or completely before the fetus expulsion,after 20 weeks gestation or in the delivery procedure.
Incidence rate: 0.46%~2.1% Neonatal mortality: 200‰~428‰

Etiology
Angiopathy of vasa basalis Mechanical agent Venous pressure of uterus elevated
abruptly Volume of uterus deflated abruptly Others: Age of gravida>35,multipara, tobacco,dope

Classification
Classify according to vaginal bleeding or nor:
Dominant/Recessive/Mixed Classify according to severity degree: Light type < 1/3 Severe type > 1/3; > 1/2, Dead
fetus
Uteroplacental apoplexy: widespread extravasation of blood
into the uterine musculature and beneath the uterine serosa
Clinical Features
Abruptly,persistent abdominal pain with vaginal bleeding
Maternal compromise/ shock(Volume of vaginal bleeding not correspond to patient condition)
Anomaly of fetal condition The uterus touched hard with pain The size of uterus is bigger than it
should be in that gestation age

Auxiliary examination
Diagnotic examination: B-ultrasound examination
Placenta examination post partumBlood Rt,Blood
coagulation,blood examination of hepatic and renal function
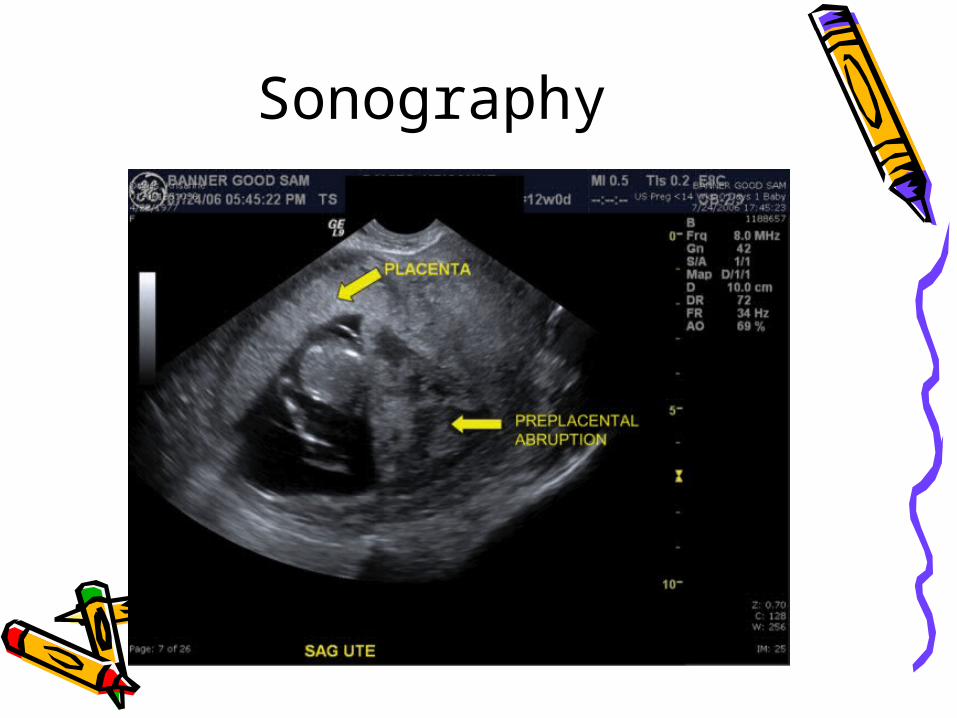
Sonography

Differential diagnosis
• Placental previa• Uterus rupture
Complications
DIC,dysfunction of coagulationPost partum hemorrhagic/shockAmniotic fluid embolismAcute renal failureFetal death

Management
Treatment depends on: • Condition of the mother and fetus• Gestational age of the fetus• Cervical examinationPrinciple: If diagnosed,fetus will be
deliveried immediately
Management
Mature fetus DeliverCompromised mother Deliver Immature fetus Expectant, if mother stable

Expectant Management
• Bed rest• Ongoing maternal monitoring• Fetal assessment: age, growth, well
being• Deliver if recurrent signs /
symptoms• Deliver at fetal maturation

Severe placental abruption:
• Resuscitation• Evaluate and treat coagulation
defect• Deliver the fetus: Cesarean section • Prevention of PPH• Monitor renal status closely



















