Physical Health Care SOP 01: Early Intervention in Psychosis
18
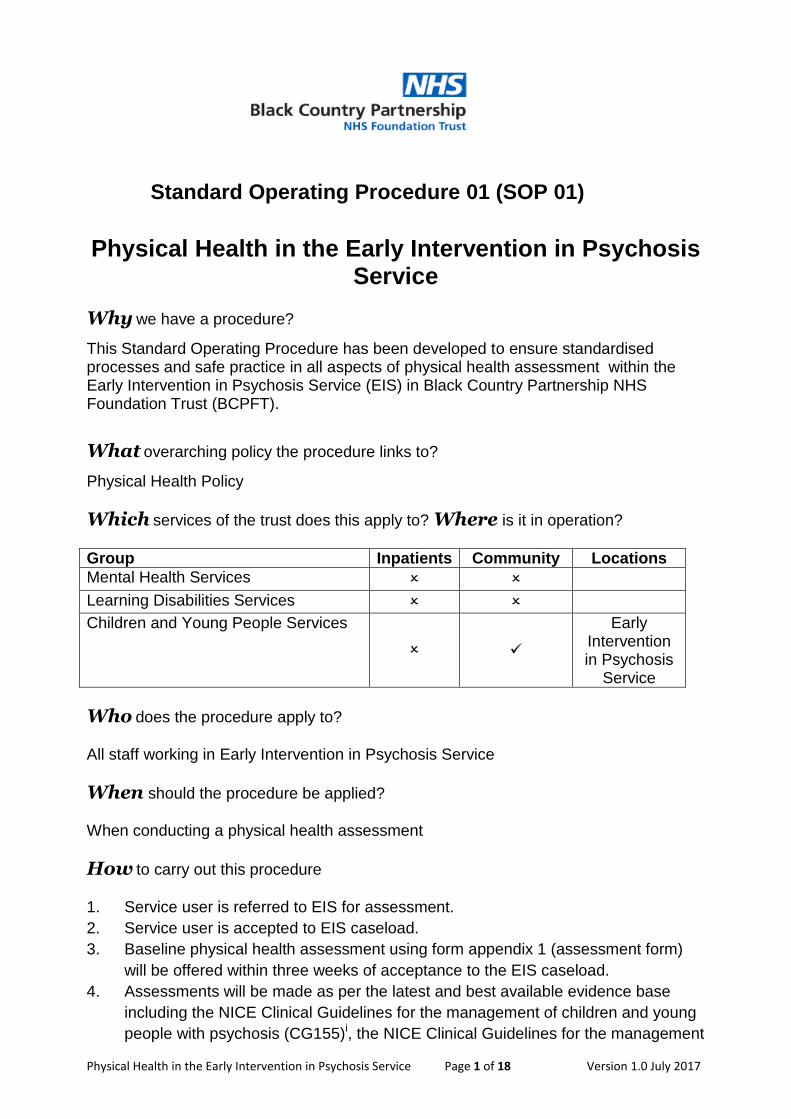
Physical Health in the Early Intervention in Psychosis Service Page 1 of 18 Version 1.0 July 2017 Standard Operating Procedure 01 (SOP 01) Physical Health in the Early Intervention in Psychosis Service Why we have a procedure? This Standard Operating Procedure has been developed to ensure standardised processes and safe practice in all aspects of physical health assessment within the Early Intervention in Psychosis Service (EIS) in Black Country Partnership NHS Foundation Trust (BCPFT). What overarching policy the procedure links to? Physical Health Policy Which services of the trust does this apply to? Where is it in operation? Group Inpatients Community Locations Mental Health Services Learning Disabilities Services Children and Young People Services Early Intervention in Psychosis Service Who does the procedure apply to? All staff working in Early Intervention in Psychosis Service When should the procedure be applied? When conducting a physical health assessment How to carry out this procedure 1. Service user is referred to EIS for assessment. 2. Service user is accepted to EIS caseload. 3. Baseline physical health assessment using form appendix 1 (assessment form) will be offered within three weeks of acceptance to the EIS caseload. 4. Assessments will be made as per the latest and best available evidence base including the NICE Clinical Guidelines for the management of children and young people with psychosis (CG155) i , the NICE Clinical Guidelines for the management
Transcript of Physical Health Care SOP 01: Early Intervention in Psychosis
Physical Health in the Early Intervention in Psychosis Service Page 1 of 18 Version 1.0 July 2017
Standard Operating Procedure 01 (SOP 01)
Physical Health in the Early Intervention in Psychosis
Service
Why we have a procedure?
This Standard Operating Procedure has been developed to ensure standardised processes and safe practice in all aspects of physical health assessment within the Early Intervention in Psychosis Service (EIS) in Black Country Partnership NHS Foundation Trust (BCPFT).
What overarching policy the procedure links to?
Physical Health Policy
Which services of the trust does this apply to? Where is it in operation?
Group Inpatients Community Locations
Mental Health Services
Learning Disabilities Services
Children and Young People Services
Early Intervention in Psychosis
Service
Who does the procedure apply to?
All staff working in Early Intervention in Psychosis Service
When should the procedure be applied?
When conducting a physical health assessment
How to carry out this procedure
1. Service user is referred to EIS for assessment.
2. Service user is accepted to EIS caseload.
3. Baseline physical health assessment using form appendix 1 (assessment form)
will be offered within three weeks of acceptance to the EIS caseload.
4. Assessments will be made as per the latest and best available evidence base
including the NICE Clinical Guidelines for the management of children and young
people with psychosis (CG155)i, the NICE Clinical Guidelines for the management

Physical Health in the Early Intervention in Psychosis Service Page 2 of 18 Version 1.0 July 2017
of adults with psychosis (CG178)ii, the EIP Self-Assessment Tooliii, the EIP
standardsiv, the Maudsley Prescribing Guidelines for anti-psychoticsv and the
Lester toolvi. The tests will include:
Bloods (U&Es, FBC, Lipid profile, Fasting Glucose, HbA1C, Prolactin, LFT,
CPK, TFT)
ECG
Blood Pressure/Pulse
Weight (Weekly for first 6 weeks on anti-psychotic)
Personal history (cardio-vascular disease, hypertension, LESTER TOOL)
Family history (cardiovascular disease, hypertension)
Lifestyle factors (substance use, alcohol, smoking, exercise/physical
activity, diet/health eating)
Height
BMI
Waist circumference
Hip circumference
Side effects of medication including movement disorder
current side effects if already prescribed medication i.e. GASS tool
Adherence to medication
Would you like written information?
Has verbal information been provided?
Do you take over the counter medications?
Do you take complimentary medications/therapies?
Offer information relating to interactions of above with prescribed
medications/therapy/psychology
Are you prescribed PRN medications? Medication to take as and when
required
Does this take client medication above BNF maximum?
5. Service users under the care of the inpatient services at the point of referral to EIS
should already have baseline assessments undertaken by inpatient staff. In this
case, records to be collated by EIS nursing staff for inclusion in EIS assessment
data.

Physical Health in the Early Intervention in Psychosis Service Page 3 of 18 Version 1.0 July 2017
6. Physical health baseline assessments using form appendix 1 will be repeated and
reviewed at 3 months, 6 months, 12 months then every 6 months until discharge
from EIS.
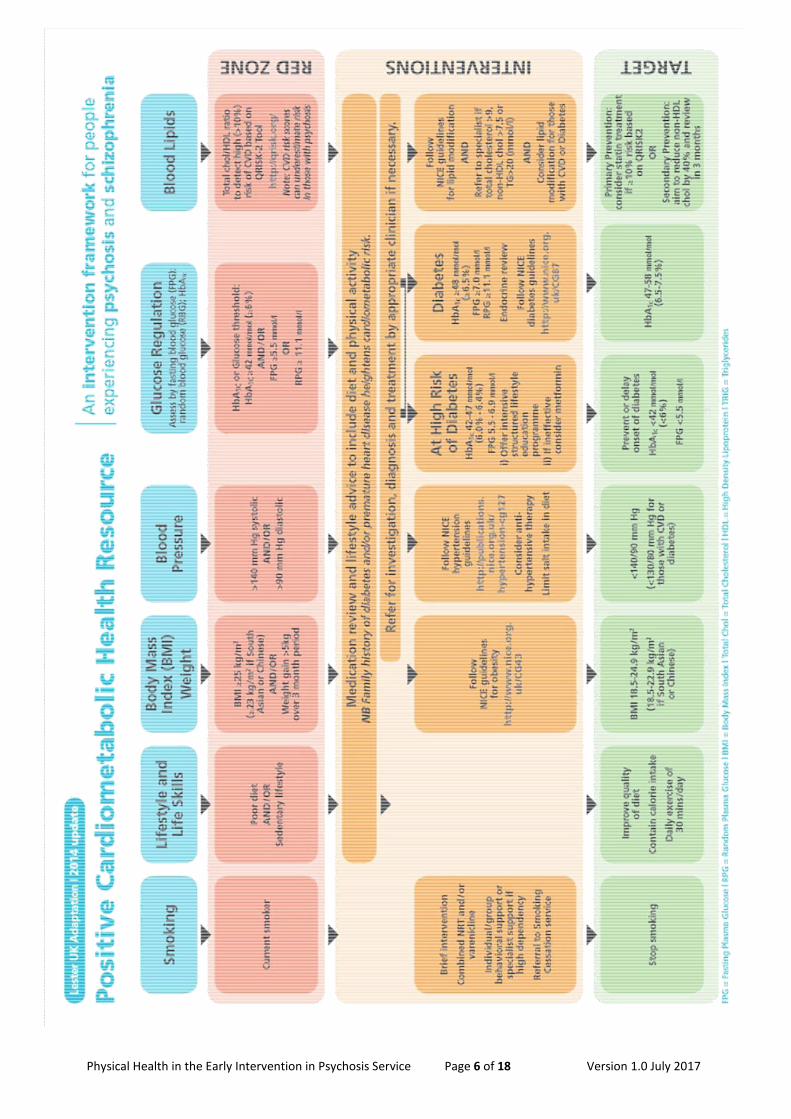
7. Cardiometabolic Health Screen and Intervention Framework (appendix 2) will be
completed at the same intervals by the assessing nurse and information gathered
will be inputted onto the QRisk2-2016 form found online at https://qrisk.org/2016/
8. Missing data indicates further assessment should be arranged once information is
available and QRisk2-2016 should be recalculated.
9. QRisk2-2016 score confirmed by website should be inputted onto team physical
health database by assessing nurse. (Note: the tool does not work for <25s – the
reason for exception should be recorded instead).
10. All information gathered at physical health assessment to be inputted into physical
health database by assessing nurse.
11. Assessment forms once complete, to be filed in the “investigations” section of the
service user’s nursing notes.
12. Accurate details of assessments made will be recorded as a clinical entry in the
nursing record.
13. Information/outcomes from physical health assessment to be fed back into wider
MDT via weekly multi-disciplinary team meetings, to include update to prescribing
staff.
14. Feedback to be provided to the service user’s GP using letter appendix 3
(standard feedback letter) within two weeks of assessment.
15. Appendix 3 (feedback letter) to be uploaded onto CareNotes/Oasis systems within
five days of assessment
Physical Health in the Early Intervention in Psychosis Service Page 4 of 18 Version 1.0 July 2017
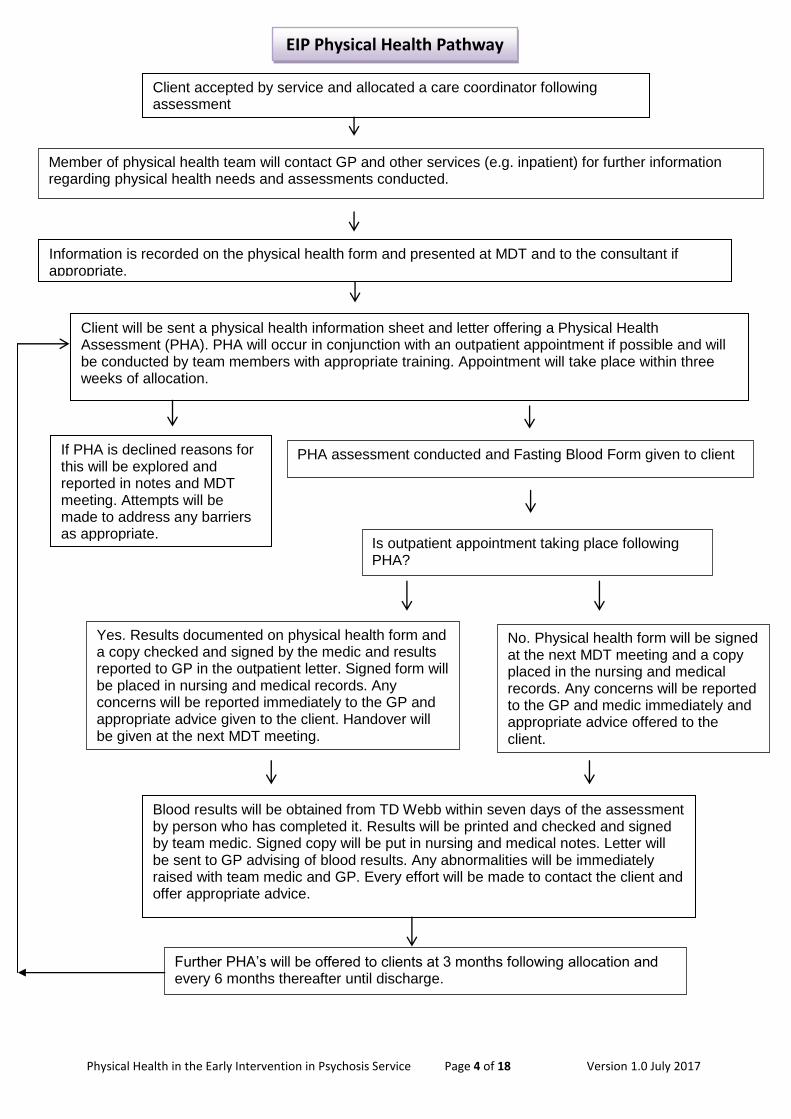
Client will be sent a physical health information sheet and letter offering a Physical Health Assessment (PHA). PHA will occur in conjunction with an outpatient appointment if possible and will be conducted by team members with appropriate training. Appointment will take place within three weeks of allocation.
Client accepted by service and allocated a care coordinator following assessment
Member of physical health team will contact GP and other services (e.g. inpatient) for further information regarding physical health needs and assessments conducted.
Information is recorded on the physical health form and presented at MDT and to the consultant if appropriate.
If PHA is declined reasons for this will be explored and reported in notes and MDT meeting. Attempts will be made to address any barriers as appropriate.
Blood results will be obtained from TD Webb within seven days of the assessment by person who has completed it. Results will be printed and checked and signed by team medic. Signed copy will be put in nursing and medical notes. Letter will be sent to GP advising of blood results. Any abnormalities will be immediately raised with team medic and GP. Every effort will be made to contact the client and offer appropriate advice.
PHA assessment conducted and Fasting Blood Form given to client
Is outpatient appointment taking place following PHA?
Yes. Results documented on physical health form and a copy checked and signed by the medic and results reported to GP in the outpatient letter. Signed form will be placed in nursing and medical records. Any concerns will be reported immediately to the GP and appropriate advice given to the client. Handover will be given at the next MDT meeting.
No. Physical health form will be signed at the next MDT meeting and a copy placed in the nursing and medical records. Any concerns will be reported to the GP and medic immediately and appropriate advice offered to the client.
Further PHA’s will be offered to clients at 3 months following allocation and every 6 months thereafter until discharge.
EIP Physical Health Pathway

Pathways For Cardiometabolic Risks
If agreed refer for diet/exercise advice
Health trainers (Wolverhampton)
My time active (Sandwell)
Advise relevant Medical Team for medication review if deemed appropriate
Yes
If agreed, refer for advice and support to;
Recovery Near You (Wolverhampton)
IRIS - Alcohol
Swanswell – Substance (Sandwell)
Brief Intervention/ Lifestyle advice
Brief Intervention/ Lifestyle advice Offer *BHF Leaflets on diet and exercise
If agreed refer for smoking cessation
Health trainers (Wolverhampton)
Quit51 (Sandwell)
Blood Lipids Cholesterol >9, non-HDL chol >7.5 or TG.20)mmol/l) And/or QRISK >10%
Brief Intervention/ Offer *BHF Leaflet on smoking
Glucose HbA1c ≥ 42 mmol/mol
And/or FPG ≥ 5.5mmol/l
Or RPG ≥ 11.1mmol/l
Blood Pressure >140 mm Hg systolic
And /or >90 mm Hg diastolic
Substance Misuse And /or
Alcohol Misuse >14 units alcohol weekly
Lifestyle and Life Skills Poor Diet and/or Sedentary Lifestyle
BMI/Weight BMI>25 and/or weight gain >5kg over 3 month period
Smoking
Yes
Yes
Yes
Yes
Yes
Brief Intervention/ Lifestyle advice Offer *BHF Leaflet on diabetes and your heart
Advise relevant medical team, consider anti-hypertensive therapy, advise GP for action
Brief Intervention/ Lifestyle advice Offer * BHF Leaflet on blood pressure/ reducing salt intake
Advise relevant medical team and GP for action May require repeat monitoring
All in
form
atio
n to
be
forw
ard
ed
to G
P fo
llow
ing
ph
ys
ica
l he
alth
clin
ic a
pp
oin
tme
nt o
r dis
ch
arg
e fro
m in
patie
nt s
erv
ice
s
Brief Intervention/ Lifestyle advice Offer *BHF Leaflet on reducing cholesterol
Consider lipid modification, advise GP for action
Physical Health in the Early Intervention in Psychosis Service Page 6 of 18 Version 1.0 July 2017
Patient Name: Or personal details sticker to override this section: DOB: NHS Number: Oasis Number:
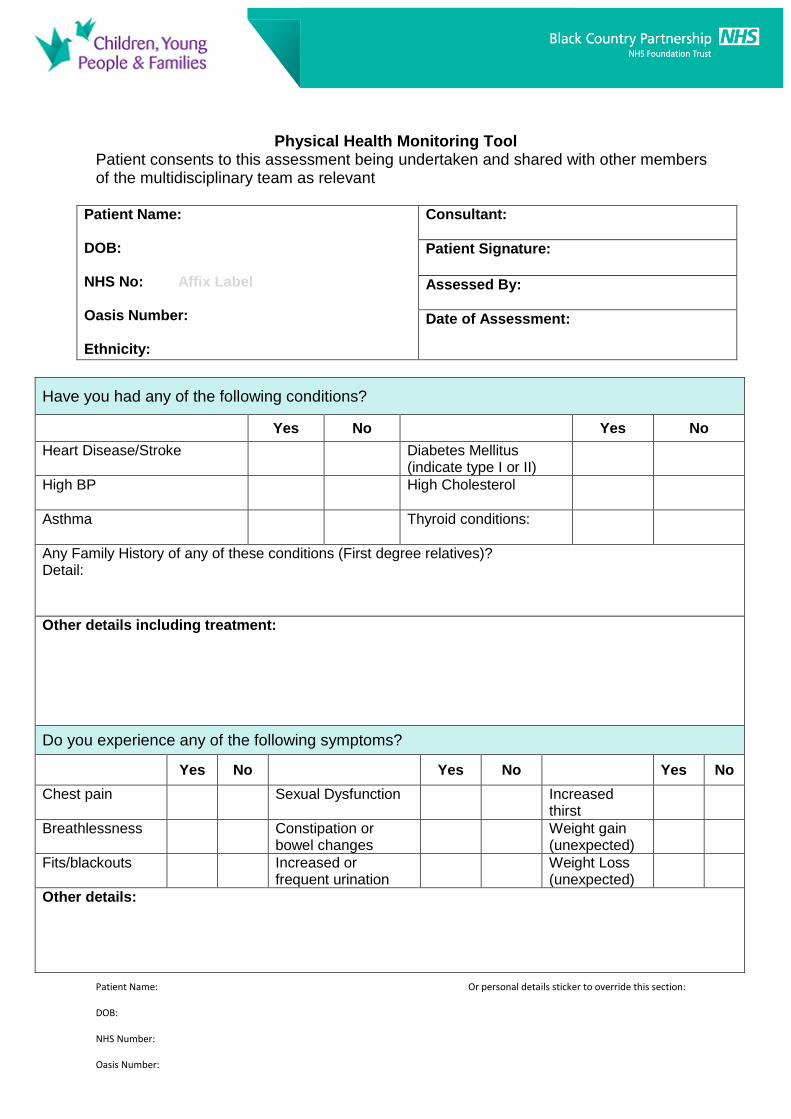
Physical Health Monitoring Tool Patient consents to this assessment being undertaken and shared with other members of the multidisciplinary team as relevant
Patient Name: DOB: NHS No: Affix Label Oasis Number: Ethnicity:
Consultant:
Patient Signature:
Assessed By:
Date of Assessment:
Have you had any of the following conditions?
Yes No Yes No
Heart Disease/Stroke
Diabetes Mellitus (indicate type I or II)
High BP
High Cholesterol
Asthma Thyroid conditions:
Any Family History of any of these conditions (First degree relatives)? Detail:
Other details including treatment:
Do you experience any of the following symptoms?
Yes No Yes No Yes No
Chest pain Sexual Dysfunction
Increased thirst
Breathlessness Constipation or bowel changes
Weight gain (unexpected)
Fits/blackouts Increased or frequent urination
Weight Loss (unexpected)
Other details:

Patient Name: Or personal details sticker to override this section: DOB: NHS Number: Oasis Number:
Have you had dental checks in past year?
Yes
No*
Details: *Refer to Dentist directory for local services if required
Have you had optical check-up in past 2 years?
Yes No*
Details: *Refer to Optician directory for local services if required
Have you had a smear test in the last 3 years?
Yes
No*
N/A
Date Last Menstrual Cycle (If Known) *Advise patient to see GP if referral required
Do you have any problems with skin or feet?
Yes
No
Details: Complete pressure sore risk calculator (Waterlow), and request to see skin integument
Do you have any swallowing / speech difficulties?
Yes No
Details:
Do you have any mobility issues?
Yes
No
Details:
Do you have pain which is not managed?
Yes
No
Details:
Do you experience any side effects from your medication? i.e. sedation, tremors, muscle stiffness
Complete Glasgow Antipsychotic Side-Effect Scale (GASS)
Yes
No
Details: Dependent on severity/urgency, refer to consultant or defer to next OPA
Do you have any allergies or sensitivities? Yes No Details:
Enter alert onto CareNotes system
Do you use herbal or over the counter medication? i.e. non-prescription
Yes
No
Details: Advise prescriber of details if “yes”
Are you prescribed any regular or “as required” medication?
Yes
No
Details: Include: does the person take medication as prescribed? Is the dose above BNF limit?
Have you received written or verbal information about your prescribed medication?
Yes
No
Details: Include: written, verbal or both? And if “no” would they like this?

Patient Name: Or personal details sticker to override this section: DOB: NHS Number: Oasis Number:
Are you a smoker?
Yes
No Ex-
Smoker
Details:
Would you like to be referred for smoking cessation advice?
Yes No
N/A
If so, refer via appropriate service. Detail:
Do you take recreational drugs? i.e. cannabis, amphetamines
Yes No Details:
Do you drink alcohol? Recommended daily units: Maximum 2
Yes No
Detail Units Per Week: (Use drinks calculator https://www.alcoholconcern.org.uk/unit-calculator)
Do you want and agree a referral to the Addictions service?
Yes No
Details:
Do you undertake physical activity? - How often? What?
Yes
No
Details:
Do you consider yourself to eat a healthy diet? – i.e. 5 a day
Yes
No
Details:
Do you wish referred for diet and exercise advice?
Yes
No
Already under
services
Details:
Baseline observations: Please record if any observations are refused
Height cm Weight kg BMI kg/m2
Weight Gain >5kg over 3 month period Detail:
Yes No Temp (If indicated)
Blood Pressure mm Hg
Pulse Respirations bpm /min
QRISK-2 score (%) Calculator found at http://qrisk.org
Waist Circumference cm
Hip Circumference cm
Cholesterol (If Known) Cholesterol/HDL ratio – Total Cholesterol – Non–HDL -
Glucose (Random or Fasting) HbA1c – FPG/RPG -
Waterlow Risk Score See SOP for calculator, and action to take
Do you know date of last blood test? Yes No Detail: Check TD Web for blood test results
Do you consent to having bloods taken? Yes No
N/A
N/A – If completed in last 3 months Yes - To include FBC,U&E’s, LFT’s, TFT’s, Lipid profile, HbA1c, glucose
Do you consent to ECG? Yes No N/A N/A – If completed in last 3 months
Has ECG been requested? Yes No N/A
Patient Name: Or personal details sticker to override this section: DOB: NHS Number: Oasis Number:
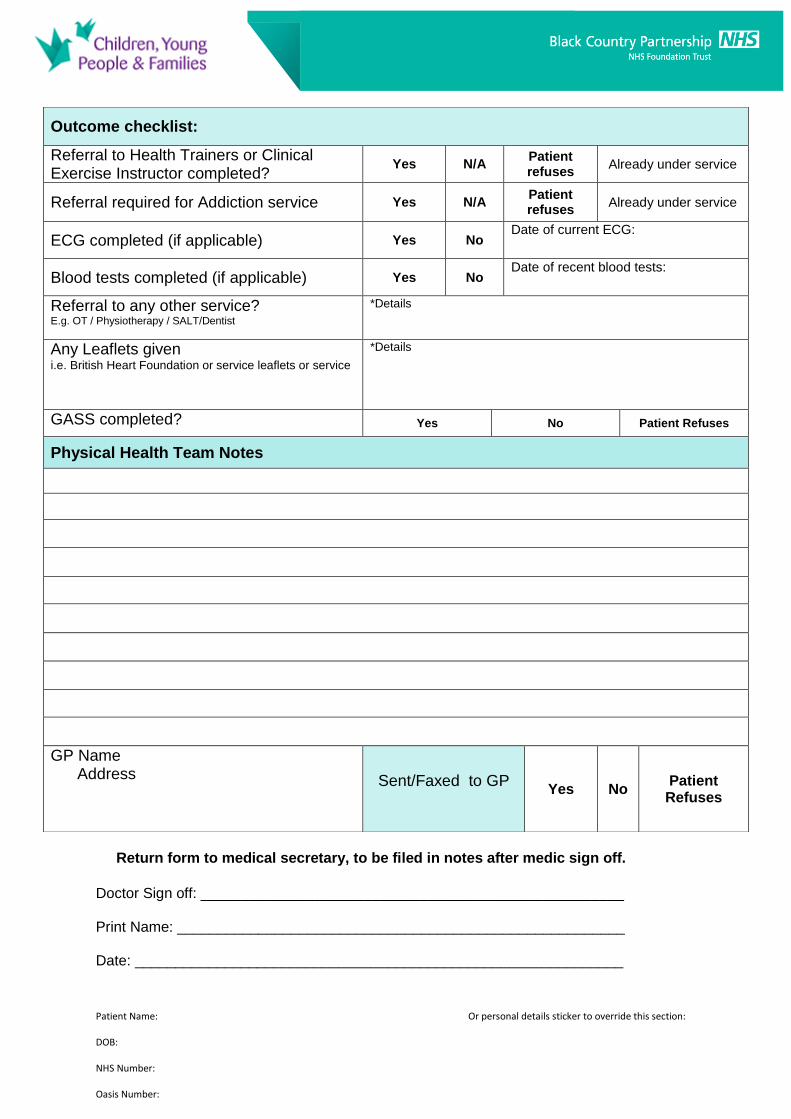
Return form to medical secretary, to be filed in notes after medic sign off.
Doctor Sign off: ____________________________________________________ Print Name: _______________________________________________________ Date: ____________________________________________________________
Outcome checklist:
Referral to Health Trainers or Clinical Exercise Instructor completed?
Yes N/A Patient refuses
Already under service
Referral required for Addiction service Yes N/A Patient refuses
Already under service
ECG completed (if applicable) Yes No Date of current ECG:
Blood tests completed (if applicable) Yes No Date of recent blood tests:
Referral to any other service? E.g. OT / Physiotherapy / SALT/Dentist
*Details
Any Leaflets given i.e. British Heart Foundation or service leaflets or service
*Details
GASS completed? Yes No Patient Refuses
Physical Health Team Notes
GP Name Address
Sent/Faxed to GP
Yes No Patient Refuses
Patient Name: Or personal details sticker to override this section: DOB: NHS Number: Oasis Number:
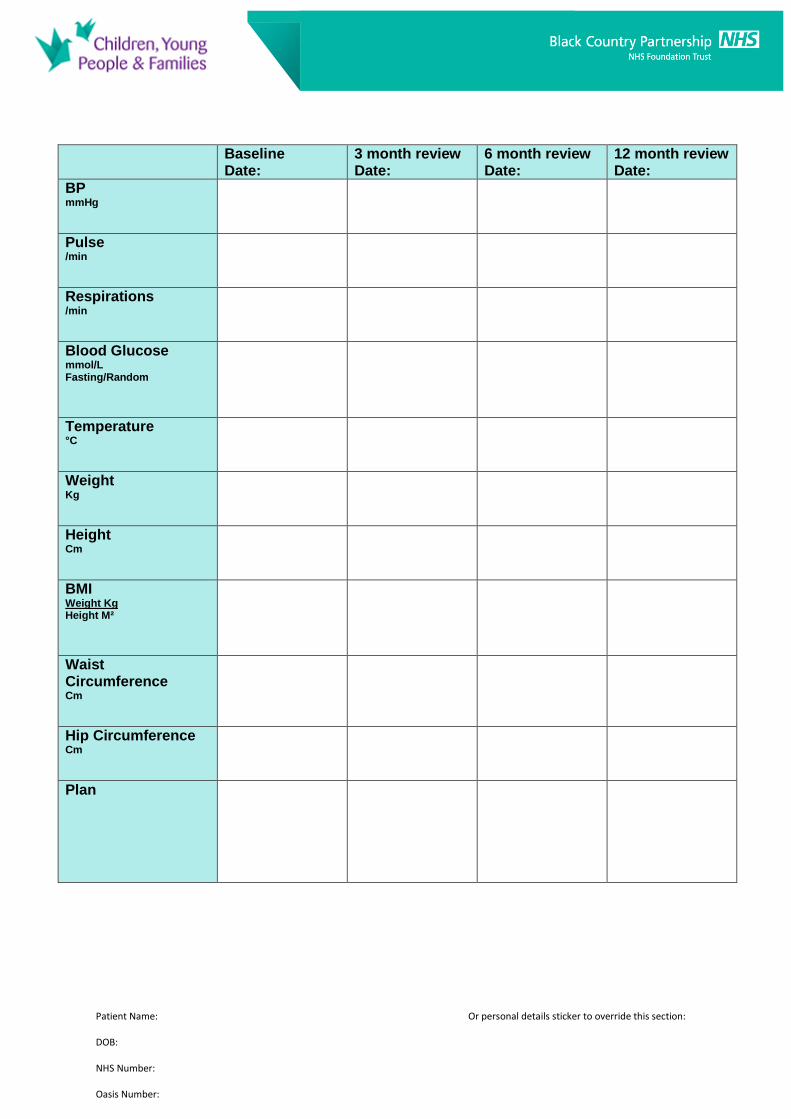
Baseline Date:
3 month review Date:
6 month review Date:
12 month review Date:
BP mmHg
Pulse /min
Respirations /min
Blood Glucose mmol/L Fasting/Random
Temperature °C
Weight Kg
Height Cm
BMI Weight Kg Height M²
Waist Circumference Cm
Hip Circumference Cm
Plan
Patient Name: Or personal details sticker to override this section: DOB: NHS Number: Oasis Number:
18 month Date:
24 month review Date:
30 month review Date:
36 month review Date:
BP mmHg
Pulse /min
Respirations /min
Blood Glucose mmol/L Fasting/Random
Temperature °C
Weight Kg
Height Cm
BMI Weight Kg Height M²
Waist Circumference Cm
Hip Circumference Cm
Plan
To be filed in medical notes following completion
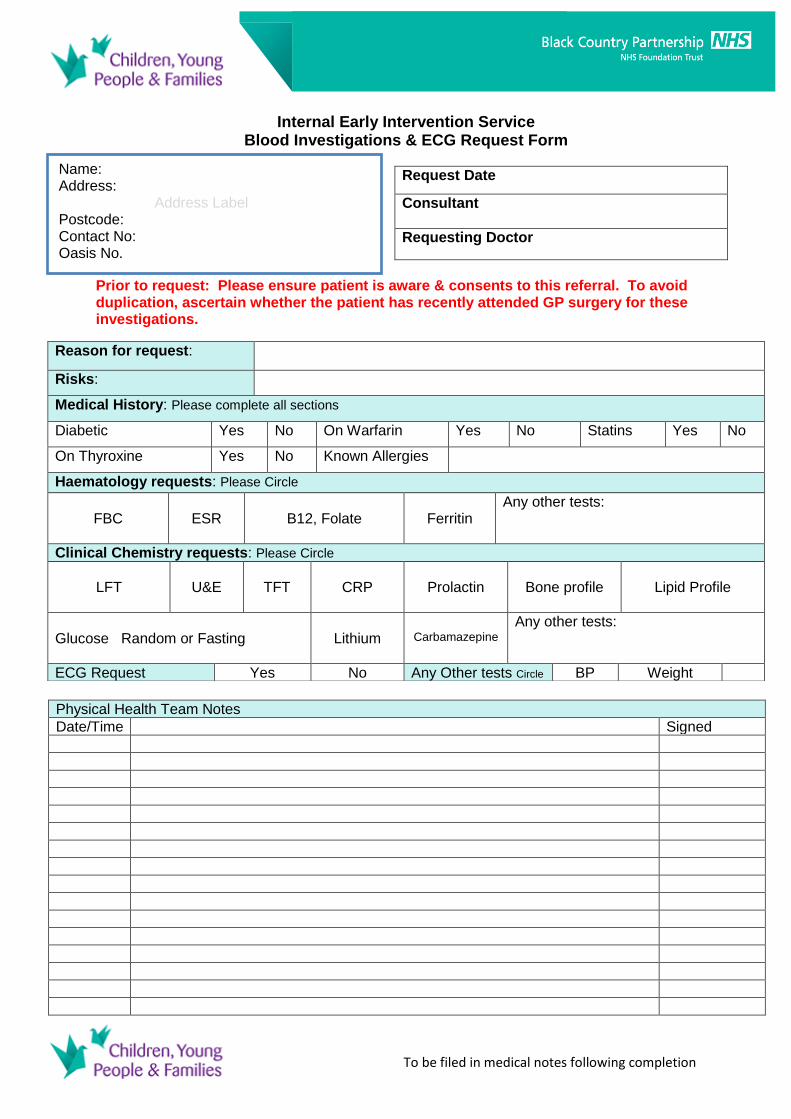
Internal Early Intervention Service
Blood Investigations & ECG Request Form
Request Date
Consultant
Requesting Doctor
Prior to request: Please ensure patient is aware & consents to this referral. To avoid duplication, ascertain whether the patient has recently attended GP surgery for these investigations.
Physical Health Team Notes
Date/Time Signed
Reason for request:
Risks:
Medical History: Please complete all sections
Diabetic Yes No On Warfarin Yes No Statins Yes No
On Thyroxine Yes No Known Allergies
Haematology requests: Please Circle
FBC
ESR
B12, Folate
Ferritin
Any other tests:
Clinical Chemistry requests: Please Circle
LFT
U&E
TFT
CRP
Prolactin
Bone profile
Lipid Profile
Glucose Random or Fasting
Lithium
Carbamazepine
Any other tests:
ECG Request Yes No Any Other tests Circle BP Weight
Name: Address: Address Label Postcode: Contact No: Oasis No.
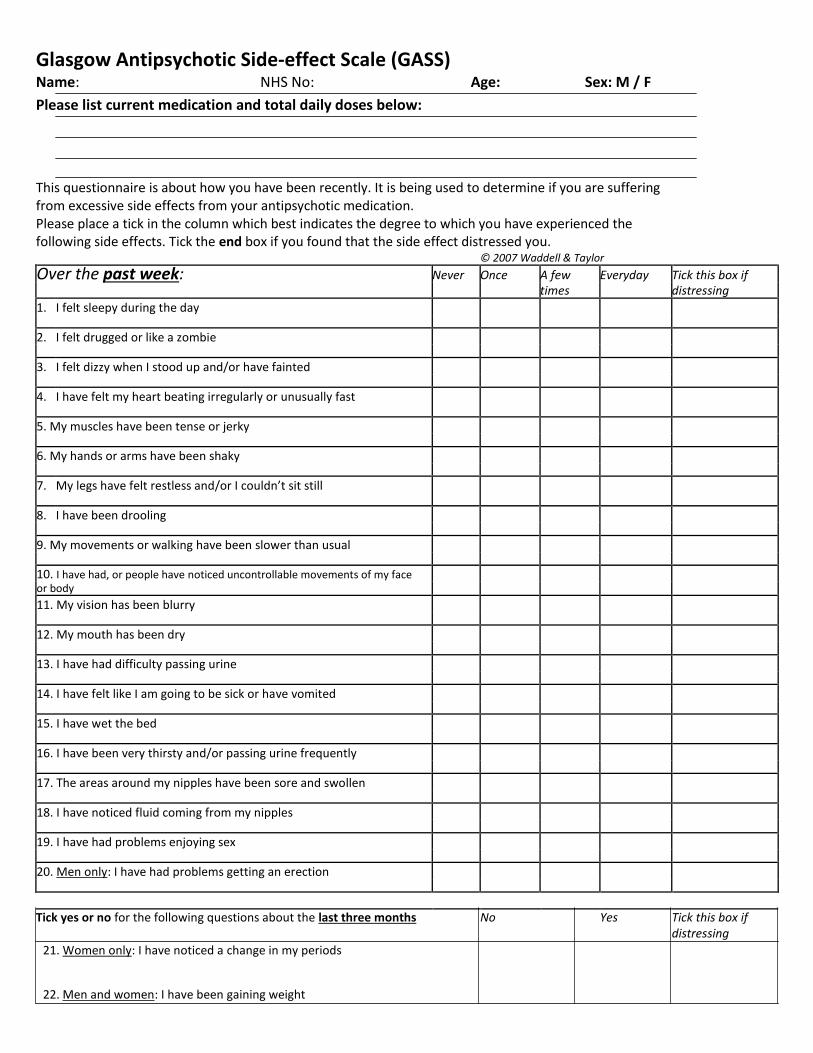
Glasgow Antipsychotic Side‐effect Scale (GASS) Name: NHS No: Age: Sex: M / F Please list current medication and total daily doses below:
This questionnaire is about how you have been recently. It is being used to determine if you are suffering from excessive side effects from your antipsychotic medication. Please place a tick in the column which best indicates the degree to which you have experienced the following side effects. Tick the end box if you found that the side effect distressed you. © 2007 Waddell & Taylor
Over the past week: Never Once A few Everyday Tick this box if times distressing
1. I felt sleepy during the day
2. I felt drugged or like a zombie
3. I felt dizzy when I stood up and/or have fainted
4. I have felt my heart beating irregularly or unusually fast
5. My muscles have been tense or jerky
6. My hands or arms have been shaky
7. My legs have felt restless and/or I couldn’t sit still
8. I have been drooling
9. My movements or walking have been slower than usual
10. I have had, or people have noticed uncontrollable movements of my face or body
11. My vision has been blurry
12. My mouth has been dry
13. I have had difficulty passing urine
14. I have felt like I am going to be sick or have vomited
15. I have wet the bed
16. I have been very thirsty and/or passing urine frequently
17. The areas around my nipples have been sore and swollen
18. I have noticed fluid coming from my nipples
19. I have had problems enjoying sex
20. Men only: I have had problems getting an erection
Tick yes or no for the following questions about the last three months No Yes Tick this box if distressing
21. Women only: I have noticed a change in my periods
22. Men and women: I have been gaining weight
Physical Health in Early Intervention in Psychosis Service Page 15 of 18 Version 1.0 July 2017
Staff Information
1. Allow the patient to fill in the questionnaire themselves. Questions 1‐20 relate to
the previous week and questions 21‐22 to the last three months.
2. Scoring:
For questions 1‐20 award 1 point for the answer “once”, 2 points for the answer
“a few times” and 3 points for the answer “everyday”.
Please note zero points are awarded for an answer of “never”.
For questions 21 and 22 award 3 points for a “yes” answer and 0 points for a
“no”.
Total for all questions=
3. For male and female patients a total score of:
0‐12 = absent/mild side effects
13‐26 = moderate side effects over 26 = severe side effects
4. Side effects covered by questions
1‐2 sedation and CNS side effects
3‐4 cardiovascular side effects
5‐10 extra‐pyramidal side effects
11‐13 anticholinergic side effects
14 gastro‐intestinal side effects 15 genitourinary side effects 16 screening for diabetes mellitus 17‐21 prolactinaemic side effects 22 weight gain
The column relating to the distress experienced with a particular side effect is not
scored, but is intended to inform the clinician of the service user’s views and
condition.
Physical Health in Early Intervention in Psychosis Service Page 16 of 18 Version 1.0 July 2017
Early Intervention Service 44 Pond Lane
Wolverhampton West Midlands
WV2 1HG Tel: 01902 443993
Fax: 0121 612 3746
Doctor Name
Address
Dear Dr
Re: Name of Patient, DOB Address NHS number: Oasis Number: The above patient recently undertook a physical health assessment with our Service. The results were: Blood Pressure: / mmHg Pulse: /minute Weight: . kg Temperature: . °c Respiration rate: /minute BMI: Hip Circumference: cm Waist Circumference: cm Blood Glucose: . mmol/l pre diet/post diet Summary of history provided Yours sincerely Names of nurses Community Mental Health Nurses Early Intervention Service
Physical Health in Early Intervention in Psychosis Service Page 17 of 18 Version 1.0 July 2017
References i National Collaborating Centre for Mental Health. (2013). Psychosis and Schizophrenia in children and young people: recognition and management: The NICE Guideline on Treatment and Management. CG155. London: National Institute for Health and Clinical Excellence [Online]. [Accessed 13
th October
2016]. Available at: www.nice.org.uk/guidance/cg155 ii National Collaborating Centre for Mental Health. (2014). Psychosis and Schizophrenia in adults: The
NICE Guideline on Treatment and Management. CG178. London: National Institute for Health and Clinical Excellence [Online]. [Accessed 13th October 2016]. Available at: https://www.nice.org.uk/guidance/cg178/resources/cg178-psychosis-and-schizophrenia-in-adults-full-guideline-appendices2 iii Royal College of Psychiatrists (2016). Early Intervention in Psychosis Network Self Assessment Tool.
London: EIPN, Royal College of Psychiatrists Centre for Quality improvement [Online]. [Accessed 13th
October 2016]. Available at: http://www.rcpsych.ac.uk/workinpsychiatry/qualityimprovement/ccqiprojects/earlyinterventionpsychosis/theselfassessment.aspx iv Royal College of Psychiatrists (2016). Standards for Early Intervention in Psychosis Services. Pilot
Edition. London: EIPN, Royal College of Psychiatrists Centre for Quality improvement [Online]. [Accessed 13
th October 2016]. Available at:
http://www.rcpsych.ac.uk/workinpsychiatry/qualityimprovement/ccqiprojects/earlyinterventionpsychosis/standardsforeipservices.aspx v Taylor, D., Paton, C. and Kapur, S. (2015). The Maudsley Prescribing Guidelines in Psychiatry. 12th
Edition. West Sussex: Wiley Blackwell vi Shiers, D.E.., Rafi, I., Cooper, S.J., Holt, R.I.G.. (2014). Update (with acknowledgement to the late
Helen Lester for her contribution to the original 2012 version). Positive Cardiometabolic Health Resource: an intervention framework for patients with psychosis and schizophrenia.2014 Update. Royal College of Psychiatrists London.
Where do I go for further advice or information?
Roles and responsibilities of key staff in relation to this procedure Training Staff may receive training in relation to this procedure, where it is identified in their appraisal as part of the specific development needs for their role and responsibilities. Please refer to the Trust’s Mandatory & Risk Management Training Needs Analysis for further details on training requirements, target audiences and update frequencies Monitoring / Review of this Procedure In the event of planned change in the process(es) described within this document or an incident involving the described process(es) within the review cycle, this SOP will be reviewed and revised as necessary to maintain its accuracy and effectiveness.
Equality Impact Assessment Please refer to overarching policy
Data Protection Act and Freedom of Information Act Please refer to overarching policy

Physical Health in Early Intervention in Psychosis Service Page 18 of 18 Version 1.0 July 2017
Standard Operating Procedure Details
Unique Identifier for this SOP is BCPFT-PH-SOP-04-1
State if SOP is New or Revised New
Policy Category Physical Health
Executive Director whose portfolio this SOP comes under
Executive Director of Nursing and AHPs
Policy Lead/Author Job titles only
Team Leader Sandwell & Wolverhampton Early Intervention Service
Committee/Group Responsible for Approval of this SOP
CYPF Quality and Safety Group
Month/year consultation process completed
May 2017
Month/year SOP was approved July 2017
Next review due July 2020
Disclosure Status ‘B’ can be disclosed to patients and the public
Review and Amendment History
Version Date Description of Change
1.0 Jul 2017
New SOP developed to support overarching Physical Health Policy specifically for use by Early Intervention in Psychosis Service