SOUTH REGION EARLY INTERVENTION IN PSYCHOSIS … · 6 of 20 | South Region Early Intervention in...
20
SOUTH REGION EARLY INTERVENTION IN PSYCHOSIS PROGRAMME PROGRAMME REPORT 2015-16
Transcript of SOUTH REGION EARLY INTERVENTION IN PSYCHOSIS … · 6 of 20 | South Region Early Intervention in...
SOUTH REGION EARLY INTERVENTION IN PSYCHOSIS PROGRAMMEPROGRAMME REPORT 2015-16
2 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
Document Owner Document Status
Sarah Amani FINAL
Forum Chair
Preparedness Clinical Group Prof. Belinda Lennox
Preparedness Programme Board Fiona Edwards
South Region Mental Health Priority Board (NHS England) Julia Davison
Name Title, Organization
Fiona Edwards CEO, Surrey and Borders Partnership NHS Foundation Trust & Chair of EIP Preparedness Board
Prof Belinda Lennox South Region EIP Preparedness Senior Responsible Officer
Document Ownership and Status
Document Review Distribution List
Document Approval [Persons designated to approve and sign off of this document]
3 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
1. Introduction 4 1.1. Clinical Background 4 1.2. Purpose of Document 4
2. EIP Preparedness Programme 5
3. Summary 5
4. EIP Audit 6 4.1. Specification 6
5. Findings 6
5.1. EIP Investment 7
5.2. Status of Service Development and Improvement Planning (SDIP) 10
5.3. EIP Structures 11
5.4. Percentage of Caseload Allocated an EIP Care Coordinator within 14 Days of Referral 12
5.5. NICE Concordance 13
5.6. Workforce 14
5.7. Performance and Outcomes 15
6. Discussion 16
7. Recommendations 17
8. Appendix 1 - EIP Preparedness Programme Clinical Group 18
8.1. Appendix 2 - Information Technology and Information Management Representatives 19
8.2. Appendix 3 - EIP Preparedness Programme Board 19
Table of Contents
4 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
1. Introduction
1.1. Clinical Background
1.2. Purpose of Document
Waiting times and access standards can be used to measure and improve services as well as identifying an expected standard of care. In physical health, the NHS Constitution guarantees patients’ right not to wait more than 18 weeks for consultant-led treatment, but mental health treatment has historically been excluded. For the first time, in April 2015 NHS England committed to waiting time standards for mental healthcare, supported by £80 million of investment targeting first episode psychosis in 2015/16. The new access and waiting time standards require health systems to ensure >50% of people with suspected first episode psychosis receive a NICE recommended package of care within 14 days of referral.
Early Intervention in Psychosis (EIP) Teams were originally set up as part of the National Service Framework for mental health in the late 90’s but despite mounting evidence of their effectiveness, have seen a significant decline in resources over the years. The new EIP access and waiting time standards mandate a reinstatement of EIP teams, with a statute to deliver the range of evidence based NICE recommended interventions.
The Independent Schizophrenia Commission (20141), established by the mental health charity Rethink Mental Illness, reported many deficiencies in the services for people with psychosis resulting in:
• Death 15-20 years earlier than the general population.
• Only 1 in 10 who might benefit from cognitive behavioural therapy has access to it.
• Lack of employment opportunities; only 8% in employment.
• Inadequate support and recognition of the role of carers.
• Problems in the services for those with African-Caribbean or African backgrounds.
• A need to extend Early Intervention for Psychosis services.
• A need for improved prescribing.
Developed in partnership with members of the South Region EIP Preparedness Clinical Group (Appendix 1), the purpose of this paper is to provide the reader with a single report that establishes local levels of psychosis incidence, current levels of performance against the new standard and the workforce skill mix and related training needs. The report intends to identify key areas of focus and also good practice, to help ensure equitable EIP services across the South Region.
1 Schizophrenia Commission, 2012
5 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
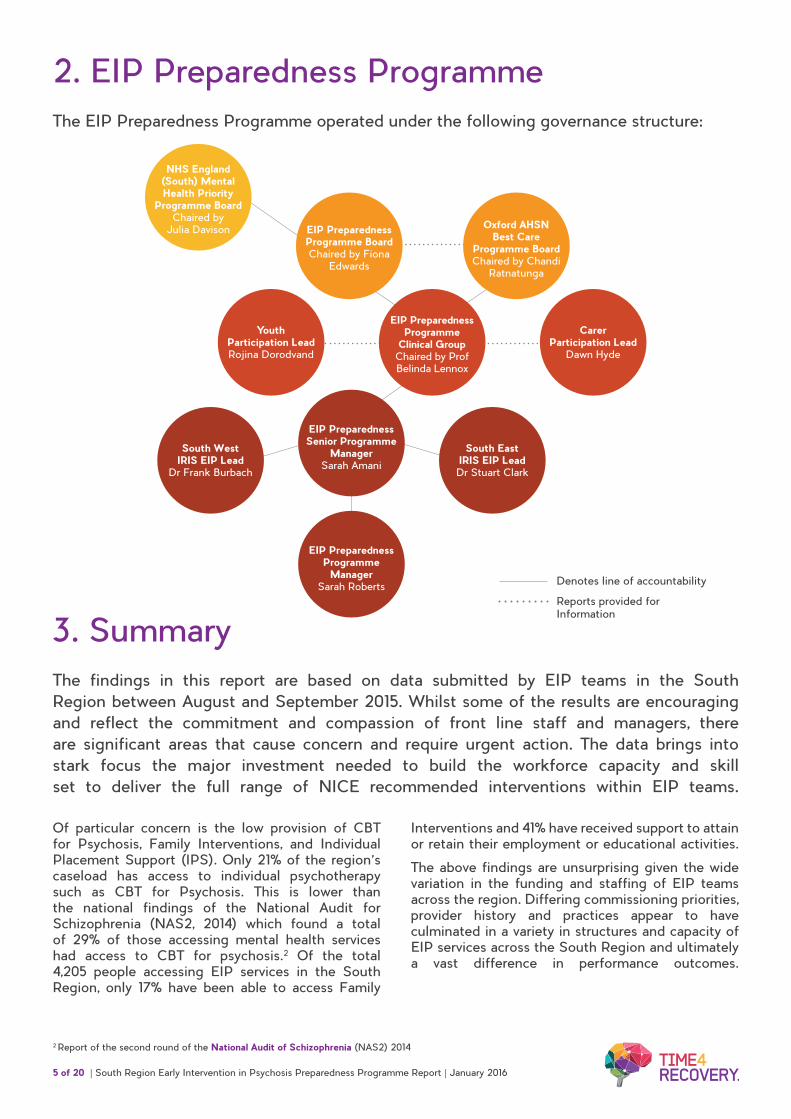
2. EIP Preparedness ProgrammeThe EIP Preparedness Programme operated under the following governance structure:
Denotes line of accountability
Reports provided for Information
NHS England (South) Mental Health Priority
Programme Board Chaired by
Julia Davison
EIP Preparedness Programme
Clinical Group Chaired by Prof Belinda Lennox
EIP Preparedness Senior Programme
Manager Sarah Amani
EIP Preparedness Programme
Manager Sarah Roberts
Carer Participation Lead
Dawn Hyde
South East IRIS EIP Lead Dr Stuart Clark
Youth Participation Lead Rojina Dorodvand
South West IRIS EIP Lead
Dr Frank Burbach
EIP Preparedness Programme Board Chaired by Fiona
Edwards
Oxford AHSN Best Care
Programme Board Chaired by Chandi
Ratnatunga
3. SummaryThe findings in this report are based on data submitted by EIP teams in the South Region between August and September 2015. Whilst some of the results are encouraging and reflect the commitment and compassion of front line staff and managers, there are significant areas that cause concern and require urgent action. The data brings into stark focus the major investment needed to build the workforce capacity and skill set to deliver the full range of NICE recommended interventions within EIP teams.
Of particular concern is the low provision of CBT for Psychosis, Family Interventions, and Individual Placement Support (IPS). Only 21% of the region’s caseload has access to individual psychotherapy such as CBT for Psychosis. This is lower than the national findings of the National Audit for Schizophrenia (NAS2, 2014) which found a total of 29% of those accessing mental health services had access to CBT for psychosis.2 Of the total 4,205 people accessing EIP services in the South Region, only 17% have been able to access Family
Interventions and 41% have received support to attain or retain their employment or educational activities.
The above findings are unsurprising given the wide variation in the funding and staffing of EIP teams across the region. Differing commissioning priorities, provider history and practices appear to have culminated in a variety in structures and capacity of EIP services across the South Region and ultimately a vast difference in performance outcomes.
2 Report of the second round of the National Audit of Schizophrenia (NAS2) 2014
6 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
4. EIP Audit
4.1. Specification
5. FindingsFollowing nominations to a region wide board, an inaugural meeting with representatives from commissioners and providers from the South of England was held on 15th May 2015 (Appendix 3). One of the first decisions made by the board related to benchmarking the South of England EIP workforce, current demand and provision of services. It was decided that in the absence of any other EIP specific benchmarking tool that reflected the new standards, the programme would develop its own and encourage transparency in order to gather accurate data and share best practice. An online audit (the EIP Matrix: http://time4recovery.com/eip-matrix/) was developed in partnership with the Preparedness Clinical Group.
The content of the EIP Matrix was generated by the nominated members of the EIP Preparedness Clinical Group (Appendix 1) who provided their expertise to develop the specification. The first section of the audit asked providers to list their EIP services, indicating the current caseload, age ranges and annual budget. The audit was further divided into three subsections covering:
1. NICE Concordance
2. Performance and Outcomes
3. Staffing and Workforce Training
The EIP Matrix calculates percentages, using denominators and agreed thresholds to produce colour coded bar charts which indicate levels of achievement against NICE standards. Following its seventh and final iteration, the EIP Matrix (http://time4recovery.com/eip-matrix/ ) was tested by the Oxford AHSN informatics team to verify accuracy and reliability.
Instructions to register to use the Matrix were sent to the clinical group with guidance following final board approval. Access to the EIP matrix was controlled via unique identifiers and passwords assigned to EIP Clinical Leads as part of the registration process. Data submissions were received between 3rd August and 1st September 2015.
Between 3rd August and 1st September 2015. The level of completeness of the audit by providers was generally high; however as with all self-reporting audits there were some issues with accuracy. Where there were discrepancies, the programme team verified the data with the submitting clinical leads. Some areas where the data was questionable included smoking cessation and carers support, this was identified as an issue in a number of organisations and was a result of smokers and carers not being identified and recorded accurately.
There was one organisation unable to provide the data due to technical difficulties with their Electronic Health Record (EHR) and the fact that this organisation’s EIP services are currently provided within a generic Community Mental Health Team (CMHT), making information difficult to extract. All providers and constituent CCGs were given individual reports, analysed and graphed to support service improvement and development planning (page 17).
7 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
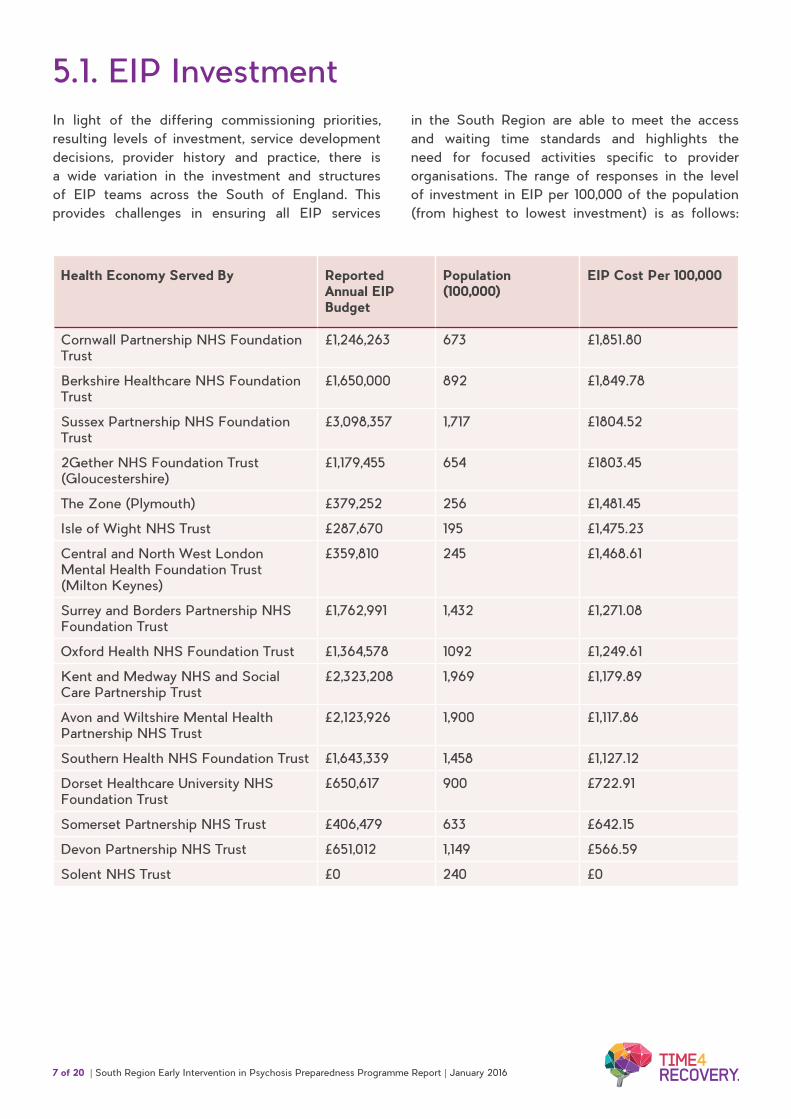
Health Economy Served By Reported Annual EIP Budget
Population (100,000)
EIP Cost Per 100,000
Cornwall Partnership NHS Foundation Trust
£1,246,263 673 £1,851.80
Berkshire Healthcare NHS Foundation Trust
£1,650,000 892 £1,849.78
Sussex Partnership NHS Foundation Trust
£3,098,357 1,717 £1804.52
2Gether NHS Foundation Trust (Gloucestershire)
£1,179,455 654 £1803.45
The Zone (Plymouth) £379,252 256 £1,481.45
Isle of Wight NHS Trust £287,670 195 £1,475.23
Central and North West London Mental Health Foundation Trust (Milton Keynes)
£359,810 245 £1,468.61
Surrey and Borders Partnership NHS Foundation Trust
£1,762,991 1,432 £1,271.08
Oxford Health NHS Foundation Trust £1,364,578 1092 £1,249.61
Kent and Medway NHS and Social Care Partnership Trust
£2,323,208 1,969 £1,179.89
Avon and Wiltshire Mental Health Partnership NHS Trust
£2,123,926 1,900 £1,117.86
Southern Health NHS Foundation Trust £1,643,339 1,458 £1,127.12
Dorset Healthcare University NHS Foundation Trust
£650,617 900 £722.91
Somerset Partnership NHS Trust £406,479 633 £642.15
Devon Partnership NHS Trust £651,012 1,149 £566.59
Solent NHS Trust £0 240 £0
5.1. EIP InvestmentIn light of the differing commissioning priorities, resulting levels of investment, service development decisions, provider history and practice, there is a wide variation in the investment and structures of EIP teams across the South of England. This provides challenges in ensuring all EIP services
in the South Region are able to meet the access and waiting time standards and highlights the need for focused activities specific to provider organisations. The range of responses in the level of investment in EIP per 100,000 of the population (from highest to lowest investment) is as follows:
8 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
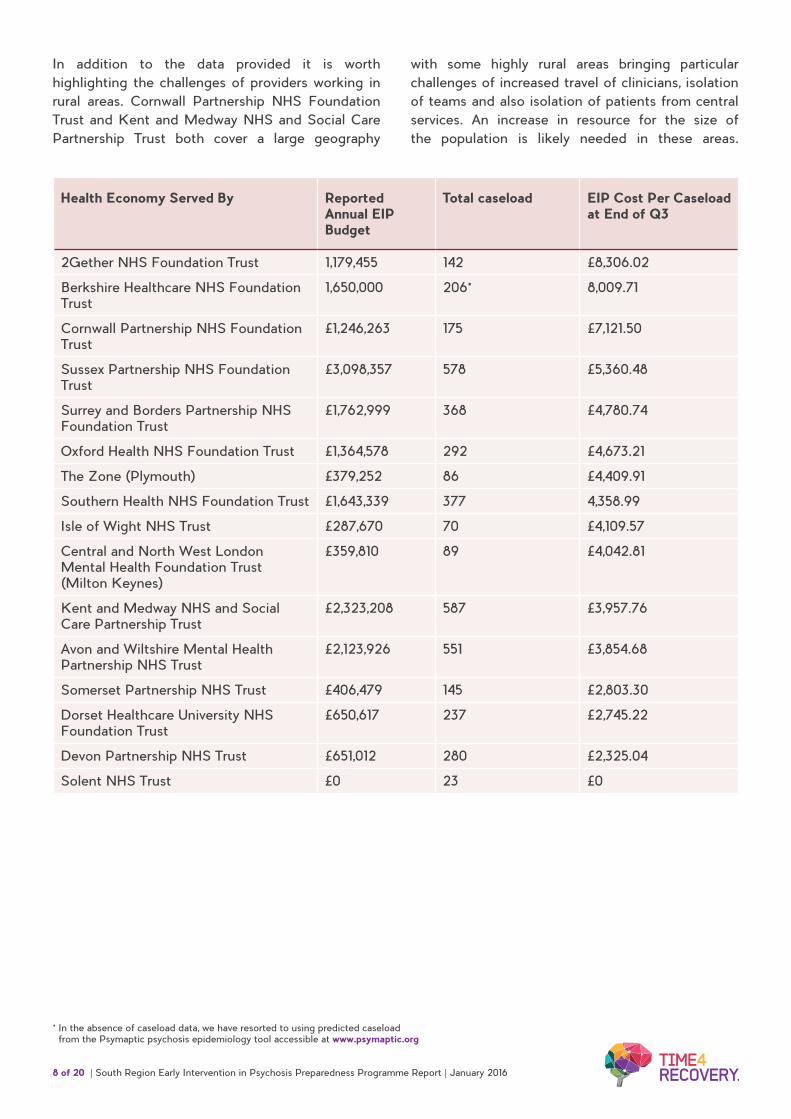
Health Economy Served By Reported Annual EIP Budget
Total caseload EIP Cost Per Caseload at End of Q3
2Gether NHS Foundation Trust 1,179,455 142 £8,306.02
Berkshire Healthcare NHS Foundation Trust
1,650,000 206* 8,009.71
Cornwall Partnership NHS Foundation Trust
£1,246,263 175 £7,121.50
Sussex Partnership NHS Foundation Trust
£3,098,357 578 £5,360.48
Surrey and Borders Partnership NHS Foundation Trust
£1,762,999 368 £4,780.74
Oxford Health NHS Foundation Trust £1,364,578 292 £4,673.21
The Zone (Plymouth) £379,252 86 £4,409.91
Southern Health NHS Foundation Trust £1,643,339 377 4,358.99
Isle of Wight NHS Trust £287,670 70 £4,109.57
Central and North West London Mental Health Foundation Trust (Milton Keynes)
£359,810 89 £4,042.81
Kent and Medway NHS and Social Care Partnership Trust
£2,323,208 587 £3,957.76
Avon and Wiltshire Mental Health Partnership NHS Trust
£2,123,926 551 £3,854.68
Somerset Partnership NHS Trust £406,479 145 £2,803.30
Dorset Healthcare University NHS Foundation Trust
£650,617 237 £2,745.22
Devon Partnership NHS Trust £651,012 280 £2,325.04
Solent NHS Trust £0 23 £0
In addition to the data provided it is worth highlighting the challenges of providers working in rural areas. Cornwall Partnership NHS Foundation Trust and Kent and Medway NHS and Social Care Partnership Trust both cover a large geography
with some highly rural areas bringing particular challenges of increased travel of clinicians, isolation of teams and also isolation of patients from central services. An increase in resource for the size of the population is likely needed in these areas.
* In the absence of caseload data, we have resorted to using predicted caseload from the Psymaptic psychosis epidemiology tool accessible at www.psymaptic.org

9 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
£9,000.00
2Get
her N
HS Fou
ndat
ion Tr
ust
Bersk
shire
Hea
lthca
re N
HS Fou
ndat
ion Tr
ust
Cornw
all P
artne
rship
NHS Fou
ndat
ion Tr
ust
Susse
x Part
nersh
ip NHS F
ound
ation
Trus
t
Surre
y and
Bor
ders
Partne
rship
NHS Fou
ndat
ion Tr
ust
Oxford
Hea
lth N
HS Fou
ndat
ion Tr
ust
The Z
one (
Plymou
th)
South
ern H
ealth
NHS F
ound
ation
Trus
t
Isle o
f Wigh
t NHS Tr
ust
Centra
l and
Nor
th W
est L
ondo
n Men
tal...
Kent a
nd M
edway
NHS an
d Soc
ial C
are...
Avon a
nd W
iltsh
ire M
enta
l Hea
lth...
Somer
set P
artne
rship
NHS Trus
t
Dorse
t Hea
lthca
re U
niver
sity N
HS Trus
t
Devon
Part
nersh
ip NHS Tr
ust
Solent
NHS Tr
ust
£8,000.00
£7,000.00
£6,000.00
£5,000.00
£4,000.00
£3,000.00
£2,000.00
£1,000.00
Current National Mean of £6,926Required cost per patient in a fully compliant EIP team - £8250
£0.00
The above table and bar chart details the EIP cost per case across the 16 providers in the South Region. This ranges from £2,325.04 to £8,009.71. Solent does not currently have a budget for EIP as it is a very small service with 2 staff based within a CMHT.
The estimated annual cost for treatment in a fully compliant early intervention team is £8,2503. By these calculations only 2gether Trust meets this level of investment. The NHS Benchmarking Network report ‘Mental Health Benchmarking Early Intervention in Psychosis Analysis’ finds the mean spend across the country for 2014/15 as £6,926 and the median as £6,808.
3 2015/16 National Tariff Engagement Document (2015) Accessed at: https://www.england.nhs.uk/resources/pay-syst/ted-1516/
EIP Investment per Person Accessing EIP Service
10 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
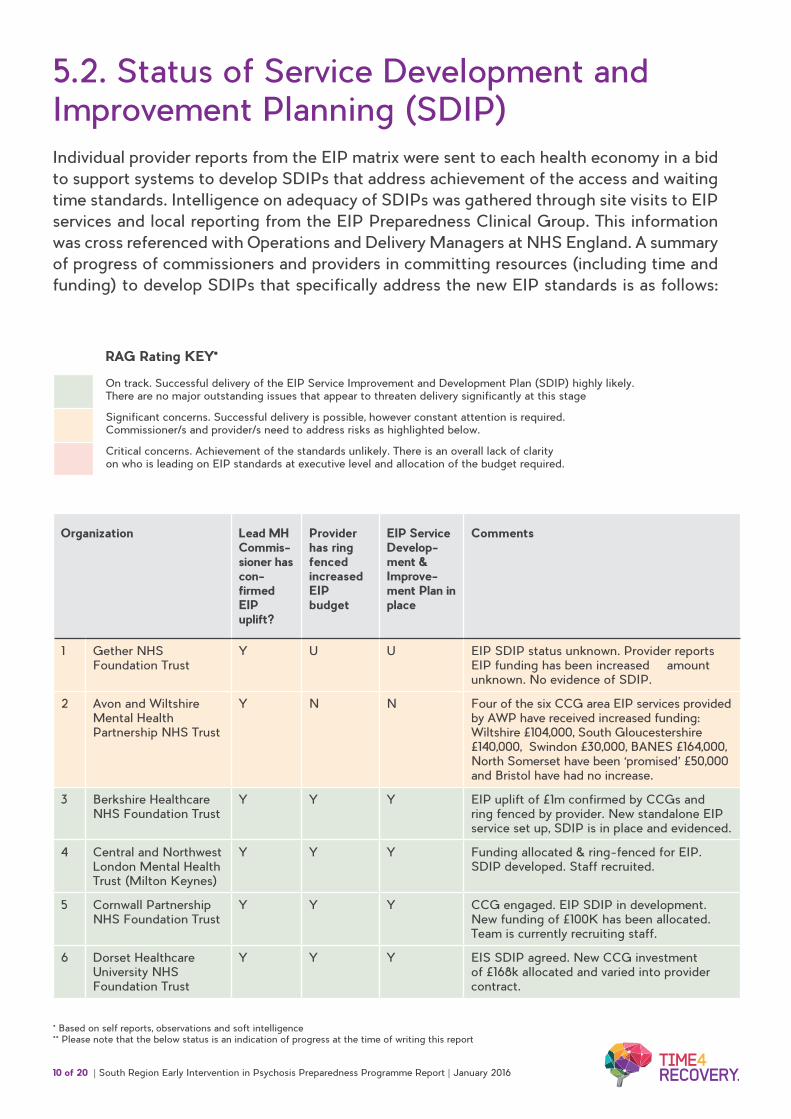
5.2. Status of Service Development and Improvement Planning (SDIP)Individual provider reports from the EIP matrix were sent to each health economy in a bid to support systems to develop SDIPs that address achievement of the access and waiting time standards. Intelligence on adequacy of SDIPs was gathered through site visits to EIP services and local reporting from the EIP Preparedness Clinical Group. This information was cross referenced with Operations and Delivery Managers at NHS England. A summary of progress of commissioners and providers in committing resources (including time and funding) to develop SDIPs that specifically address the new EIP standards is as follows:
Organization Lead MH Commis-sioner has con-firmed EIP uplift?
Provider has ring fenced increased EIP budget
EIP Service Develop-ment & Improve-ment Plan in place
Comments
1 Gether NHS Foundation Trust
Y U U EIP SDIP status unknown. Provider reports EIP funding has been increased – amount unknown. No evidence of SDIP.
2 Avon and Wiltshire Mental Health Partnership NHS Trust
Y N N Four of the six CCG area EIP services provided by AWP have received increased funding: Wiltshire £104,000, South Gloucestershire £140,000, Swindon £30,000, BANES £164,000, North Somerset have been ‘promised’ £50,000 and Bristol have had no increase.
3 Berkshire Healthcare NHS Foundation Trust
Y Y Y EIP uplift of £1m confirmed by CCGs and ring fenced by provider. New standalone EIP service set up, SDIP is in place and evidenced.
4 Central and Northwest London Mental Health Trust (Milton Keynes)
Y Y Y Funding allocated & ring-fenced for EIP. SDIP developed. Staff recruited.
5 Cornwall Partnership NHS Foundation Trust
Y Y Y CCG engaged. EIP SDIP in development. New funding of £100K has been allocated. Team is currently recruiting staff.
6 Dorset Healthcare University NHS Foundation Trust
Y Y Y EIS SDIP agreed. New CCG investment of £168k allocated and varied into provider contract.
* Based on self reports, observations and soft intelligence ** Please note that the below status is an indication of progress at the time of writing this report
On track. Successful delivery of the EIP Service Improvement and Development Plan (SDIP) highly likely. There are no major outstanding issues that appear to threaten delivery significantly at this stage
Significant concerns. Successful delivery is possible, however constant attention is required. Commissioner/s and provider/s need to address risks as highlighted below.
Critical concerns. Achievement of the standards unlikely. There is an overall lack of clarity on who is leading on EIP standards at executive level and allocation of the budget required.
RAG Rating KEY*
11 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
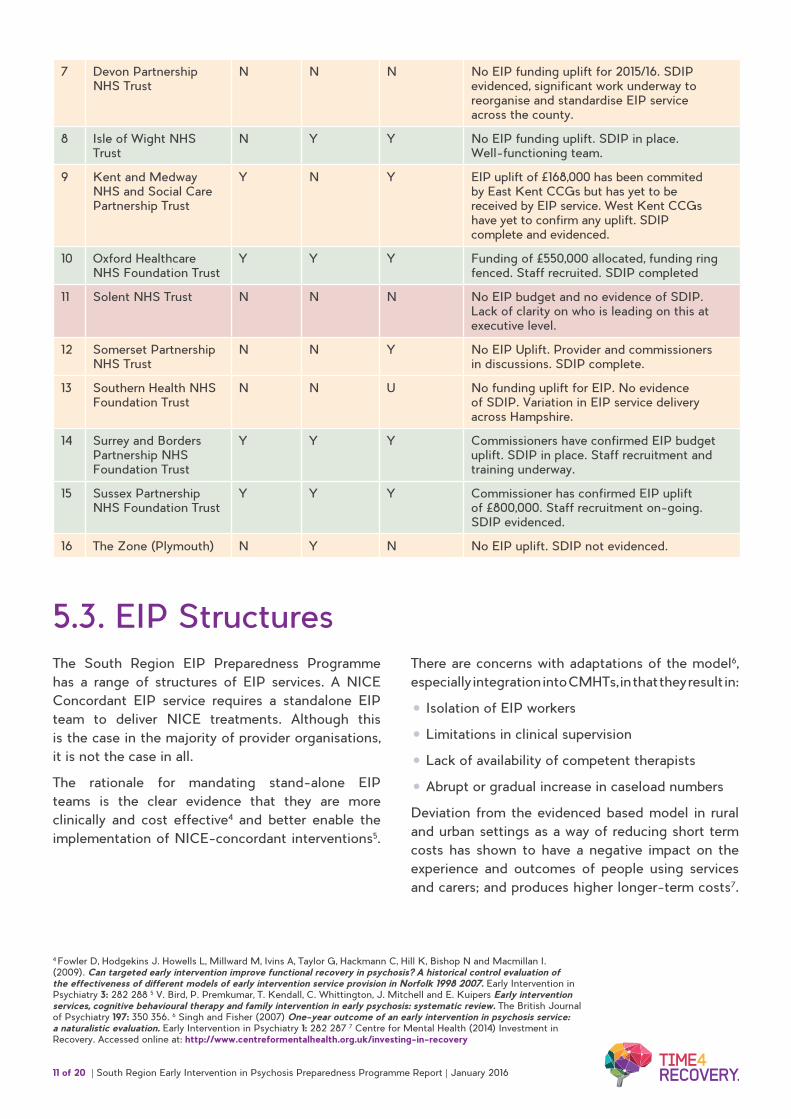
7 Devon Partnership NHS Trust
N N N No EIP funding uplift for 2015/16. SDIP evidenced, significant work underway to reorganise and standardise EIP service across the county.
8 Isle of Wight NHS Trust
N Y Y No EIP funding uplift. SDIP in place. Well-functioning team.
9 Kent and Medway NHS and Social Care Partnership Trust
Y N Y EIP uplift of £168,000 has been commited by East Kent CCGs but has yet to be received by EIP service. West Kent CCGs have yet to confirm any uplift. SDIP complete and evidenced.
10 Oxford Healthcare NHS Foundation Trust
Y Y Y Funding of £550,000 allocated, funding ring fenced. Staff recruited. SDIP completed
11 Solent NHS Trust N N N No EIP budget and no evidence of SDIP. Lack of clarity on who is leading on this at executive level.
12 Somerset Partnership NHS Trust
N N Y No EIP Uplift. Provider and commissioners in discussions. SDIP complete.
13 Southern Health NHS Foundation Trust
N N U No funding uplift for EIP. No evidence of SDIP. Variation in EIP service delivery across Hampshire.
14 Surrey and Borders Partnership NHS Foundation Trust
Y Y Y Commissioners have confirmed EIP budget uplift. SDIP in place. Staff recruitment and training underway.
15 Sussex Partnership NHS Foundation Trust
Y Y Y Commissioner has confirmed EIP uplift of £800,000. Staff recruitment on-going. SDIP evidenced.
16 The Zone (Plymouth) N Y N No EIP uplift. SDIP not evidenced.
4 Fowler D, Hodgekins J. Howells L, Millward M, Ivins A, Taylor G, Hackmann C, Hill K, Bishop N and Macmillan I. (2009). Can targeted early intervention improve functional recovery in psychosis? A historical control evaluation of the effectiveness of different models of early intervention service provision in Norfolk 1998 2007. Early Intervention in Psychiatry 3: 282 288 5 V. Bird, P. Premkumar, T. Kendall, C. Whittington, J. Mitchell and E. Kuipers Early intervention services, cognitive behavioural therapy and family intervention in early psychosis: systematic review. The British Journal of Psychiatry 197: 350 356. 6 Singh and Fisher (2007) One-year outcome of an early intervention in psychosis service: a naturalistic evaluation. Early Intervention in Psychiatry 1: 282 287 7 Centre for Mental Health (2014) Investment in Recovery. Accessed online at: http://www.centreformentalhealth.org.uk/investing-in-recovery
5.3. EIP StructuresThe South Region EIP Preparedness Programme has a range of structures of EIP services. A NICE Concordant EIP service requires a standalone EIP team to deliver NICE treatments. Although this is the case in the majority of provider organisations, it is not the case in all.
The rationale for mandating stand-alone EIP teams is the clear evidence that they are more clinically and cost effective4 and better enable the implementation of NICE-concordant interventions5.
There are concerns with adaptations of the model6, especially integration into CMHTs, in that they result in:
• Isolation of EIP workers
• Limitations in clinical supervision
• Lack of availability of competent therapists
• Abrupt or gradual increase in caseload numbers
Deviation from the evidenced based model in rural and urban settings as a way of reducing short term costs has shown to have a negative impact on the experience and outcomes of people using services and carers; and produces higher longer-term costs7.

12 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
50% of Caseload Allocated an EIP Care Coordinator within 14 days of Referral to EIP Services - Access and Waiting Time Standard from April 2016
Avon and Wiltshire Mental Health Partnership NHS…
Oxford Health NHS Foundation Trust
Berkshire Healthcare NHS Foundation Trust
Solent NHS Trust
Central and North North West London Mental…
Somerset Partnership NHS Trust
Cornwall Partnership NHS Foundation Trust
Southern Health NHS Foundation Trust
Devon Partnership NHS Trust
Surrey and Borders Partnership NHS Foundation…
Dorset Healthcare University NHS Foundation Trust
Sussex Partnership NHS Foundation Trust
Isle of Wight NHS Trust
The Zone (Plymouth)
2Gether NHS Foundation Trust
0 20 8040 10060 120
Kent and Medway NHS and Social Care Partnership…
5.4. Percentage of Caseload Allocated an EIP Care Coordinator within 14 Days of Referral
Although 8 of the 15 Trusts appear to be able to allocate a care coordinator within 14 days of referral for >50% of referrals, the fact that almost half of providers are unable to meet the standard is a key concern. This metric likely reflects a number of possible problems in the delivery of a stand-alone EIP service, including insufficient staffing levels and access delays.
Delays in the clinical pathway (usually between initial assessment at a single point of entry/ ward admission/ initial outpatient appointment to first appointment with the EIP team) are shown to account for the sub-optimal performance in many trusts8. It is clear that funding is not the only factor that determines good performance. Other factors such as communication between EIP and it’s referrers, IT infrastructure and data quality need to be optimised to achieve best possible outcomes.
8 Birchwood et al (2013) Reducing duration of untreated psychosis: care pathways to early intervention in psychosis services. British Journal of Psychiatry; 2013 (1): 58-64
13 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
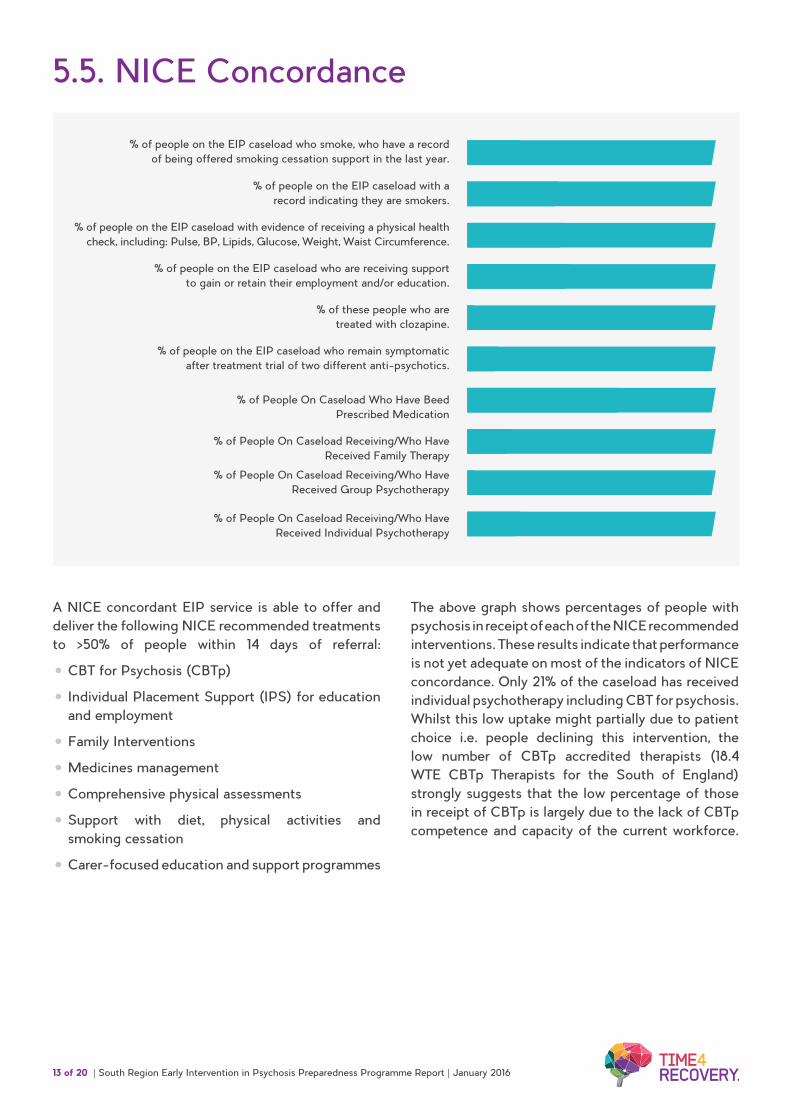
5.5. NICE Concordance
% of people on the EIP caseload who smoke, who have a record of being offered smoking cessation support in the last year.
% of people on the EIP caseload with a record indicating they are smokers.
% of people on the EIP caseload with evidence of receiving a physical health check, including: Pulse, BP, Lipids, Glucose, Weight, Waist Circumference.
% of people on the EIP caseload who are receiving support to gain or retain their employment and/or education.
% of people on the EIP caseload who remain symptomatic after treatment trial of two different anti-psychotics.
% of these people who are treated with clozapine.
% of People On Caseload Who Have Beed Prescribed Medication
% of People On Caseload Receiving/Who Have Received Family Therapy
% of People On Caseload Receiving/Who Have Received Group Psychotherapy
% of People On Caseload Receiving/Who Have Received Individual Psychotherapy
21
36
38
41
2
2
21
12
62
17
A NICE concordant EIP service is able to offer and deliver the following NICE recommended treatments to >50% of people within 14 days of referral:
• CBT for Psychosis (CBTp)
• Individual Placement Support (IPS) for education and employment
• Family Interventions
• Medicines management
• Comprehensive physical assessments
• Support with diet, physical activities and smoking cessation
• Carer-focused education and support programmes
The above graph shows percentages of people with psychosis in receipt of each of the NICE recommended interventions. These results indicate that performance is not yet adequate on most of the indicators of NICE concordance. Only 21% of the caseload has received individual psychotherapy including CBT for psychosis. Whilst this low uptake might partially due to patient choice i.e. people declining this intervention, the low number of CBTp accredited therapists (18.4 WTE CBTp Therapists for the South of England) strongly suggests that the low percentage of those in receipt of CBTp is largely due to the lack of CBTp competence and capacity of the current workforce.
14 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
5.6. Workforce
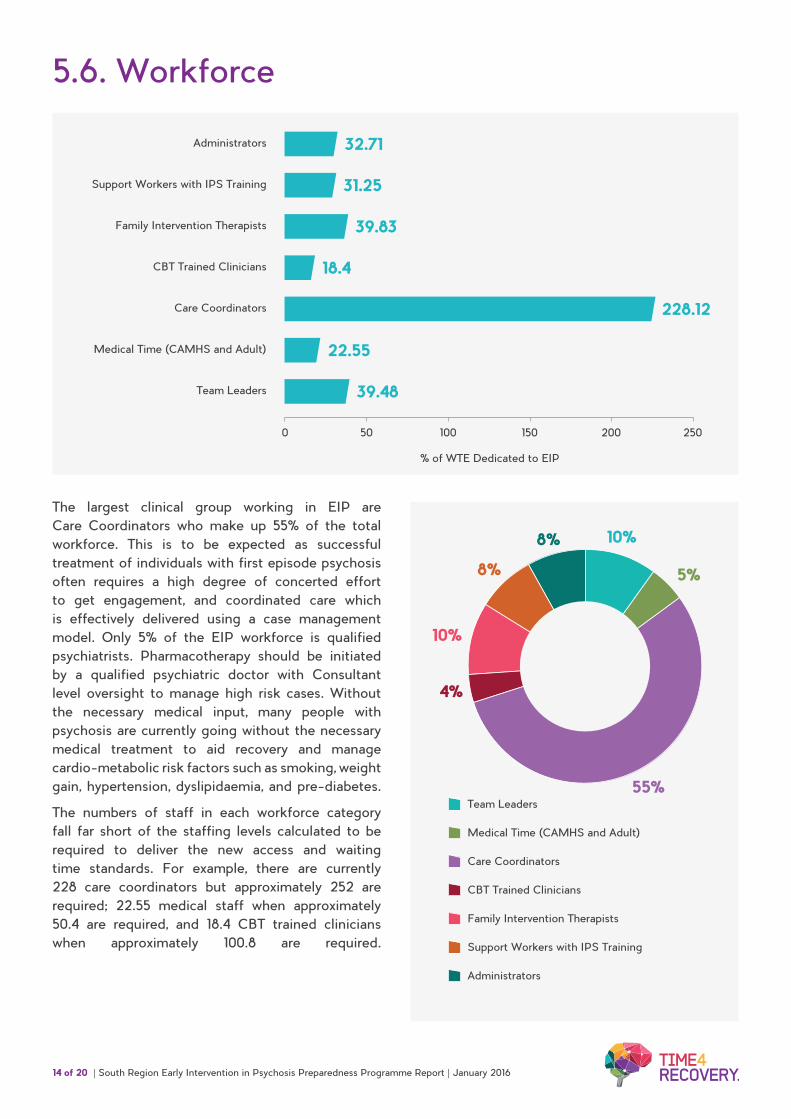
The largest clinical group working in EIP are Care Coordinators who make up 55% of the total workforce. This is to be expected as successful treatment of individuals with first episode psychosis often requires a high degree of concerted effort to get engagement, and coordinated care which is effectively delivered using a case management model. Only 5% of the EIP workforce is qualified psychiatrists. Pharmacotherapy should be initiated by a qualified psychiatric doctor with Consultant level oversight to manage high risk cases. Without the necessary medical input, many people with psychosis are currently going without the necessary medical treatment to aid recovery and manage cardio-metabolic risk factors such as smoking, weight gain, hypertension, dyslipidaemia, and pre-diabetes.
The numbers of staff in each workforce category fall far short of the staffing levels calculated to be required to deliver the new access and waiting time standards. For example, there are currently 228 care coordinators but approximately 252 are required; 22.55 medical staff when approximately 50.4 are required, and 18.4 CBT trained clinicians when approximately 100.8 are required.
Administrators
Support Workers with IPS Training
Family Intervention Therapists
CBT Trained Clinicians
Care Coordinators
Medical Time (CAMHS and Adult)
Team Leaders
% of WTE Dedicated to EIP
32.71
31.25
39.83
18.4
22.55
39.48
228.12
0 50 100 150 200 250
10%
5%
55%
4%
10%
8%
8%
Team Leaders
Care Coordinators
Family Intervention Therapists
Medical Time (CAMHS and Adult)
CBT Trained Clinicians
Support Workers with IPS Training
Administrators

15 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
50% of EIP Caseload in employment or education (outcome indicator of a good service)
Avon and Wiltshire Mental Health Partnership NHS…
Oxford Health NHS Foundation Trust
Berkshire Healthcare NHS Foundation Trust
Solent NHS Trust
Central and North North West London Mental…
Somerset Partnership NHS Trust
Cornwall Partnership NHS Foundation Trust
Southern Health NHS Foundation Trust
Devon Partnership NHS Trust
Surrey and Borders Partnership NHS Foundation…
Dorset Healthcare University NHS Foundation Trust
Sussex Partnership NHS Foundation Trust
Isle of Wight NHS Trust
The Zone (Plymouth)
2Gether NHS Foundation Trust
0 10 4020 5030 60 70
Kent and Medway NHS and Social Care Partnership…
5.7. Performance and Outcomes
Engagement in employment or education is a key functional outcome for EIP services and the best services have embedded staff members that are trained to provide IPS (Individual Placement Support). Some trusts, e.g. Cornwall, are highly successful with 68% of people who access their EIP service in education in employment. In a bid to understand the factors influencing for the success seen in Cornwall, the EIP Preparedness Team made a visit to the EIP service and its commissioners in December 2015. The Cornwall EIP service has a formal contract
with Pentreath Limited. The charity’s vocational workers are embedded within the EIP service so that they can provide timely and coordinated Individual Placement Support (IPS) to everyone referred to the service. As a result of the visit, the Cornwall EIP service has produced a video to share best practice with the rest of the South Region. The majority of trusts achieve over 30% employment or education, however, which indicates that with a bit more focus on this area, the >50% target is achievable.
Percentage of EIP Caseload in Employment or Education

16 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
6. DiscussionThe key finding from this report is that only half of the South Region EIP providers and commissioners are able to meet the 14 day access and waiting time standard for >50% of all referrals. There is also low concordance to what NICE recommends as effective treatments for psychosis with only 21% of individuals with psychosis accessing EIP services able to access CBTp and 17% of families having received Family Interventions. Key factors emerging on analysis of the data are:
• Investment in EIP
• Team Structures & Pathway Design
• Workforce Training and Development,
• Technology to record and report accurately on the EIP access and waiting time standards
These areas are issues across the South Region to differing degrees and are treated with different levels of urgency dependent on local leadership and competing demands. Vastly differing levels of investment will inevitably lead to a disparity in the service that can be provided. Only 3 trusts in the South region have invested in EIP to above the national mean spend of £6,926 with the majority of investment falling significantly below this national mean. NHS England has calculated that the provision of a NICE compliant service costs £8,250 for each patient which means that trusts such as Devon, Dorset and Somerset might need a 60% increase in funding to meet the access and waiting time standards for psychosis. Whilst these statistics might at least partially reflect a range of efficiencies and innovations in the delivery of EIP services, it is unrealistic to expect such poorly funded services to be able to achieve the expected outcomes.
Services which are currently poorly resourced will be unable to meet even the relatively simple NICE
standards such as a focus on smoking cessation. Only a minority of services, whatever their current levels of funding, are providing specialist Family Interventions and CBT for psychosis and this is the area in which the greatest new investment is required. For better funded services some of the existing staff could be trained to provide these specialist interventions but for services with low staffing levels the existing staff will need to spend all their existing time on care coordination and therefore employing new staff will be the only way of ensuring the new standards are met.
Some teams plan to meet the provision of specialist intervention through internal referral to other services e.g. psychological departments. There is a likelihood that when interventions are ‘outsourced’ they will not be offered in sufficient quantity, and with sufficient flexibility to engage this particularly challenging group. In such services specific arrangements will be required to promote successful engagement in therapies like CBTp, it is not sufficient to simply offer the intervention.
Although some services have employed assistant practitioners, many services would benefit from expanding the non-professionally qualified workforce. We would recommend employing both peer support workers (people with lived experience of psychosis) and workers who can be trained to provide specialist employment support. These employment support workers should be integrated within the EIP teams to provide an evidence-based IPS service.
Some of the other identified shortcomings- such as the relatively low level of medical time available in many services may reflect local service structures. Many services rely on accessing geographically deployed psychiatrists and the solution may simply involve the redeployment of existing staff. Another common issue is the unavailability of appropriately configured Electronic Health Records that can report on achievement of the standards and the NICE interventions delivered.
17 of 21
7. Recommendations1. Providers and Commissioners should take
cognisance of the need to increase staffing levels, particularly staff able to deliver specialist family Interventions and CBT for psychosis.
2. Providers and Commissioners should work closely together on an ongoing basis to identify the main local service deficiencies and agree a service development and improvement plan with appropriate investment.
3. The existing workforce and newly appointed staff need to be provided with an ongoing programme of training. HEE investment in EIP training in 2015-16 is very much welcomed. Ongoing funding for training will be required if the improvement in services intended by the introduction of the access and waiting time standards is to be realised.
4. Accurate data gathering and reporting capabilities from Electronic Health Records need to be developed as some of the data in this report may have been overestimated and the deficiencies may actually be greater.
5. The exercise to gather information using the EIP Matrix, develop by the South Region EIP Preparedness Team, should be repeated post April 2016. This will give up to date information on workforce, NICE concordance and outcomes, as well as quantifying progress made towards achieving the access and waiting time standards.
18 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
8. Appendix 1 - EIP Preparedness Programme Clinical GroupProf. Belinda Lennox, Senior Responsible Officer, South Region EIP Preparedness Programme
Rojina Dorodvand, Youth Participation Lead, South Region EIP Preparedness Programme
Sarah Amani, Senior Programme Manager, South Region EIP Preparedness Programme
Dawn Hyde, Carer Participation Lead, South Region EIP Preparedness Programme
Sarah Roberts, Programme Manager, South Region EIP Preparedness Programme
Jane Hainsworth, Programme Coordinator, South Region EIP Preparedness Programme
Henrietta Mbeah-Bankas, Professional Advisor - EI Programme Mental Health Nurse, Health Education England
Alison Griffiths, Programme Manager (Mental Health), Wessex AHSN
Gabby Cooper, Team Manager, 2gether NHS Foundation Trust
Anthony Lacny, Consultant Nurse, Avon and Wiltshire Mental Health NHS Foundation Trust
Rachel Esposito, Service Manager, Avon and Wiltshire Mental Health NHS Foundation Trust
Alexandra Luke, Service Manager/ Consultant Psychiatrist, Berkshire Healthcare NHS Foundation Trust
Sasha King, Senior Occupational Therapist and Quality Champion, Central & North West London Mental Health Foundation Trust
Wayland Lousley, Mental Health Transformation Manager, Milton Keynes Clinical Commissioning Group
Suzy Dion, Business Transformation Manager, Champion Central & North West London NHS Foundation Trust
Angela Hawke, Clinical Team Manager, Cornwall Partnership NHS Foundation Trust
Paul Bell Operations Manager, Community Mental Health, Cornwall Partnership NHS Foundation Trust
Tracy Read, Team Manager, Dorset Healthcare University NHS Foundation Trust
Brenda McCauley, Service Manager, Devon Partnership NHS Trust
Su Tomkins, Team Manager, Isle of Wight NHS Trust
Elaine Doyle, Clinical Team Lead and Consultant Psychiatrist, Isle of Wight NHS Trust
Collette Chamberlain, Acting Service Manager, Kent and Medway NHS and Social Care Partnership Trust
Matt McMillan, Nurse Team Leader, Kent and Medway NHS and Social Care Partnership Trust
Vicky Green, Nurse Team Leader, Kent and Medway NHS and Social Care Partnership Trust
Steve Bell, Service Manager, Oxford Health NHS Foundation Trust
Louise Johns, Consultant Academic Clinical Psychologist, Oxford Health NHS Foundation Trust
Helena Laughton, Chartered Counselling Psychologist/Deputy Team Manager Oxford Health NHS Foundation Trust
Jo Tedbury, Clinical Psychologist, Solent NHS Trust
Helen Courtney, Psychologist, Solent NHS Trust
Frank Burbach, Clinical Lead Somerset Partnership NHS Foundation Trust
Jeremy Rowlands, Consultant Psychiatrist Southern Health NHS Foundation Trust
Chris Woodfine, Service Improvement Project manager, Southern Health NHS Foundation Trust
Jo Lynch, General Manager, Surrey & Borders Partnership NHS Foundation Trust
Kate Sigov, Team Manager, Surrey & Borders Partnership NHS Foundation Trust
Peter Williams, Service Lead, Surrey & Borders Partnership NHS Foundation Trust
Rick Fraser, Consultant Psychiatrist, Sussex Partnership NHS Foundation Trust
Stuart Clark, Clinical Psychologist, Sussex Partnership NHS Foundation Trust
Gary Sargent, Team Manager, The Zone (Plymouth)
19 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
8.1. Appendix 2 - Information Technology and Information Management Representatives
8.2. Appendix 3 - EIP Preparedness Programme Board
Paul Williams, IT Manager, Plymouth CIC
Emily Carter, Data Analyst, NHS England South
Nigel Holland, Information Delivery Manager, Somerset Partnership NHS Foundation Trust
Dave West, Deputy Director of Performance and Information, Sussex Partnership NHS Foundation Trust
Sarah Powlesland, Performance Manager, Cornwall Partnership NHS Foundation Trust
Bill Johnston, IT Manager, Berkshire Healthcare NHS Foundation Trust
Paul Samain, IT Manager, Southern Health NHS Foundation Trust
Nigel Lowther, IT Manager, Kent & Medway NHS and Social Care Partnership Trust
Judith Stone, Systems Trainer / Data Quality Officer, Central & North West London Mental Health Foundation Trust
Will Marchbank, Senior Information Analyst, Avon & Wiltshire Mental Health Partnership Trust
Lindsey White, Business Partner, Business & Performance, Dorset Healthcare University NHS Foundation Trust
Dave Godley, Business Intelligence Developer, Devon Partnership NHS Trust
Samantha Luboff, Senior Information Manager, Surrey and Borders Partnership NHS Foundation Trust
Charlotte Hunt, Information Manager, Oxford Health NHS Foundation Trust
Fiona Edwards, Chief Executive, Surrey & Borders Partnership NHS Foundation Trust
Prof. Belinda Lennox, Senior Responsible Officer,South Region EIP Preparedness Programme
Sarah Amani, Senior Programme Manager, South Region EIP Preparedness Programme
Justine Faulkner, Senior Programme Manager, NHS England South
Sarah Roberts, Programme Manager, South Region EIP Preparedness Programme
Emma Wilton, Education and Workforce Development Manager, Health Education England Thames Valley
Marguerite Macfarlane, South East Strategic Clinical Network
Jan Furniaux, Service Director, 2gether NHS Foundation Trust
Rosemary Neale, Service Director, 2gether NHS Foundation Trust
Kate Lavington, Head of Community Commissioning, South Gloucestershire CCG
Andrew Keefe, Associate Director, South Gloucestershire CCG
Aly Fielden, Mental Health & Learning Disability, Commissioning Manager Bristol CC
Ian Mundy, West Berkshire Locality Director, Berkshire Healthcare NHS Foundation Trust
Nadia Barakat, Head of Mental Health Commissioning, East Berkshire CCG
Cathy Phippard, Director for Mental Health, Central & North West London Mental Health Foundation Trust
Colin Quick, Associate Director of Functional Community Services, Cornwall Partnership NHS Foundation Trust
Ellen Wilkinson, Medical Director, Cornwall Partnership NHS Foundation Trust
Sam Wilson, Contracts Lead, Kernow CCG
20 of 20 | South Region Early Intervention in Psychosis Preparedness Programme Report | January 2016
Sandra Miles, Team Manager, Kernow CCG
Mike Kelly, Head of Mental Health, Dorset Healthcare University NHS Foundation Trust
Tim Francis, Mental Health Commissioning Manager, NEW Devon CCG
Jacquie Mowbray-Gould, Deputy Director of Operations, Devon Partnership NHS Trust
Lin Walton, Mental Health Commissioner, West Locality New Devon CCG
Alexis Bower, Medical Director, Isle of Wight NHS Trust
Louise Chapman, Kent and Medway NHS and Social Care Partnership
Andy Oldfield, Head of East Kent Mental Health Commissioning, NHS South Kent Coast Clinical Commissioning Group
Roger Edmonds, Contracts Manager, Kent and Medway NHS and Social Care Partnership Trust
Angus Gartshore, Director - Community Recovery Service Line, Kent & Medway NHS Partnership Trust
Rob Bale, Clinical Director, Oxford Health NHS Foundation Trust
Matthew Hall, Operation Director, Solent NHS Trust
Tim Archer, Associate Director- Joint Commissioning, Somerset CCG
Andrew Dayani, Medical Director, Somerset Partnership NHS Foundation Trust
Katy Bartolomeo, Senior Commissioner (Mental Health & Substance Misuse), Southampton Integrated Commissioning Unit
Jeremy Rowlands, Consultant Psychiatrist, Southern Health NHS Foundation Trust
Diane Woods, Head of Mental Health and Learning Disability Commissioning, NHS North East Hampshire and Farnham CCG
Linda McQuaid, Director of Children & Young People’s Services, Surrey & Borders Partnership NHS Foundation Trust
David McKenzie, Adult Mental Health Commissioning Lead, Horsham and Mid Sussex CCG
Kay Mcdonald, Clinical Academic Director, Sussex Partnership NHS Foundation Trust
Lisa Gimingham, Deputy Locality Manager Citywide Services, Plymouth Community Healthcare
Mike Jarman, Chief Executive, The Zone (Plymouth)
Commissioned by NHS England (South)