Peripheral Nerve Injuries Ulnar, median and common peroneal nerves.
16
Peripheral Nerve Injuries Ulnar, median and common peroneal nerves.
-
Upload
clifford-armstrong -
Category
Documents
-
view
230 -
download
1
Transcript of Peripheral Nerve Injuries Ulnar, median and common peroneal nerves.

Peripheral Nerve Injuries
Ulnar, median and common peroneal nerves.

Peripheral nerve disorders
• Is defined as alteration in function and structure of the motor, sensory or autonomic components of a peripheral nerve.
Etiology: Traumatic-compression, crush injury, fractures,
laceration, stretch/traction, thermal injury, high velocity trauma.
Hereditary/geneticNutritional, infection, ischemic, thermal.

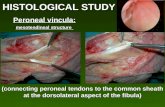
Pathophysiology
• Peripheral nerves are made up of multiple axons surrounded by myelin, Schwann cells and their covering sheaths. Individual axons are either myelinated or nonmyelinated. In neuropathies the nerves may be damaged at three main sites: the axon, the myelin and the cell body.
• Brachial plexus is responsible for cutaneous (sensory) and muscular (motor) innervation of the entire upper limb.
• 5 main nerves arise from brachial plexus: axillary, musculocutaneous, radial, median & ulnar nerve

Ulnar Nerve

Ulnar Nerve
• Arise from medial cord of brachial plexus.• Root C8-T1 (mostly C7)• Innervations: flexor carpi ulnaris, median half
of the flexor digitorum profundus, and intrinsic muscles of the hand
• Sensory distribution: Dorsal and volar surfaces of the little finger and ulnar half of the dorsal and volar surface of the ring finger.

• May be damaged in the groove behind the medial epicondyle either by trauma or entrapment.
• Leads to partial or completely loss of muscular and sensory innervations.
• >27% of nerve lesions in upper limb involve ulnar nerve.
• Leads to claw hand deformity.

Claw Hand Deformity
• Inability to extend the IP joints when extending the ring & little finger.
• Unopposed action of the extensors and FDP because lumbricals of digits 4&5 are paralyzed.
• Pt. Is unable to flex the MCP and extend IP joints of the digits.
• Seen especially when patient is asked to extend the fingers.

Presentation of ulnar claw hand
• Hyperextension at MCP joints & flexion at IP joints.
• Flattening of hypothenar eminence.• Loss of sensation along the ulnar nerve
distribution.• The most frequent symptoms are tingling,
numbness and pain in the little and ring finger.


Testing ulnar nerve
Positive Froments in hand B
Froment’s sign-patient is asked to grasped a piece of paper between the thumb and the lateral aspect of the index finger. The affected thumb will flex as the adductor pollicis muscles are weak ( pt is trying to compensate by using the flexor pollicis longus supplied by median nerve).

Treatment
• Aim is to achieve flexion at MCP joints & extension at IP joints.
• Education and avoidance of resting on elbow• During initial conservative phase the joints
must be stabilize with splints to prevent the further accentuation of deformity.
• Non surgical- meds to reduce pain and swelling, OT,PT.

Lumbrical bar splint

• Surgical-nerve repair or decompression where possible is the treatment of choice.
• if the nerve is very compressed or if there is muscle wasting surgery is done around the elbow and the wrist or both. More commonly, the nerve is moved from its place behind the elbow to a new place in front of the elbow know as anterior transposition of the ulnar nerve.

• If the nerves are unrepairable or repairs have failed, tendon transfers can be considered to restore the function of the hand and to substitute the paralyzed muscles.

Prognosis
• If there is no recovery after nerve division, hand function is significantly impaired.
• Grip strength is lost because the primary MCP flexors are lost.
• Pinch is poor because thumb adduction and index finger is weakened.

References
• http://accessphysiotherapy.mhmedical.com/data/Multimedia/grandRounds/brachial/media/brachial_print.html
• http://www.authorstream.com/Presentation/chaman-1869480-ulnar-nerve-injury-lal-karotia-ck/
• Anatomy & Physiology in Health and Illness by Ross and Wilson (11th Edition).