Lecture 23 24 parekh peroneal pathology
59
Treatment of Peroneal Tendon Pathology Selene G. Parekh, MD, MBA Associate Professor of Surgery Partner, North Carolina Orthopaedic Clinic Department of Orthopaedic Surgery Adjunct Faculty Fuqua Business School Duke University Durham, NC 919.471.9622 http://seleneparekhmd.com Twitter: @seleneparekhmd
-
Upload
selene-g-parekh-md-mba -
Category
Documents
-
view
1.085 -
download
0
Transcript of Lecture 23 24 parekh peroneal pathology

Treatment of Peroneal
Tendon Pathology
Selene G Parekh MD MBAAssociate Professor of Surgery
Partner North Carolina Orthopaedic Clinic
Department of Orthopaedic Surgery
Adjunct Faculty Fuqua Business School
Duke University
Durham NC
9194719622
httpseleneparekhmdcom
Twitter seleneparekhmd
Peroneal Tendon Tears
bull Commonly unrecognized source of lateral ankle pain
bull 40 initially misdiagnosed (Dombek et al J Foot Ankle Surg 2003)
bull Early recognitionrepair is often associated with good results
bull Less predictable surgical resultsChronic degeneration
Involvement of both tendons
Tears gt50 cross-sectional area
bull OptionsAutologous transfer
Tenodesis
Immediate vs staged intercalary graft reconstruction
Anatomy
bull Peroneus Brevis
and Longus
bull Main evertors of
the hindfoot
bull Dynamically
maintain
alignment of
hindfoot
Anatomy
bull Peroneus Brevis
bull Innervation
bull SPN
bull Action
bull Eversion
bull Location
bull Deep and
anterior to the
longus
Anatomy
bull Peroneus Longus
bull Innervation
bull SPN
bull Action
bull Plantarflex 1st ray
bull Evert foot
bull Location
bull Posterior and
lateral to the
peroneus brevis
Peroneal Tenosynovitis and
Tearsbull Etiology
bull Hypertrophy of the peroneal tubercle
bull Trauma
bull Overuse
bull Inflammatory arthropathy
bull Injury to the Os Peroneum
History and Physical
bull Pain
bull Posterolateral hindfoot
bull Worse with activity
bull Cutting activity
bull Exam
bull TTP over peroneals
bull Palpable thickening
bull Pain with passive inversion
bull Pain with resisted eversion
bull Visualized dislocated peroneal
Imaging
bull APlatoblique weightbearing views ankle
bull Os peroneum
bull Ultrasound
bull MRI
bull CT
Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
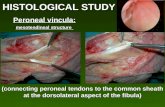
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Peroneal Tendon Tears
bull Commonly unrecognized source of lateral ankle pain
bull 40 initially misdiagnosed (Dombek et al J Foot Ankle Surg 2003)
bull Early recognitionrepair is often associated with good results
bull Less predictable surgical resultsChronic degeneration
Involvement of both tendons
Tears gt50 cross-sectional area
bull OptionsAutologous transfer
Tenodesis
Immediate vs staged intercalary graft reconstruction
Anatomy
bull Peroneus Brevis
and Longus
bull Main evertors of
the hindfoot
bull Dynamically
maintain
alignment of
hindfoot
Anatomy
bull Peroneus Brevis
bull Innervation
bull SPN
bull Action
bull Eversion
bull Location
bull Deep and
anterior to the
longus
Anatomy
bull Peroneus Longus
bull Innervation
bull SPN
bull Action
bull Plantarflex 1st ray
bull Evert foot
bull Location
bull Posterior and
lateral to the
peroneus brevis
Peroneal Tenosynovitis and
Tearsbull Etiology
bull Hypertrophy of the peroneal tubercle
bull Trauma
bull Overuse
bull Inflammatory arthropathy
bull Injury to the Os Peroneum
History and Physical
bull Pain
bull Posterolateral hindfoot
bull Worse with activity
bull Cutting activity
bull Exam
bull TTP over peroneals
bull Palpable thickening
bull Pain with passive inversion
bull Pain with resisted eversion
bull Visualized dislocated peroneal
Imaging
bull APlatoblique weightbearing views ankle
bull Os peroneum
bull Ultrasound
bull MRI
bull CT
Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Anatomy
bull Peroneus Brevis
and Longus
bull Main evertors of
the hindfoot
bull Dynamically
maintain
alignment of
hindfoot
Anatomy
bull Peroneus Brevis
bull Innervation
bull SPN
bull Action
bull Eversion
bull Location
bull Deep and
anterior to the
longus
Anatomy
bull Peroneus Longus
bull Innervation
bull SPN
bull Action
bull Plantarflex 1st ray
bull Evert foot
bull Location
bull Posterior and
lateral to the
peroneus brevis
Peroneal Tenosynovitis and
Tearsbull Etiology
bull Hypertrophy of the peroneal tubercle
bull Trauma
bull Overuse
bull Inflammatory arthropathy
bull Injury to the Os Peroneum
History and Physical
bull Pain
bull Posterolateral hindfoot
bull Worse with activity
bull Cutting activity
bull Exam
bull TTP over peroneals
bull Palpable thickening
bull Pain with passive inversion
bull Pain with resisted eversion
bull Visualized dislocated peroneal
Imaging
bull APlatoblique weightbearing views ankle
bull Os peroneum
bull Ultrasound
bull MRI
bull CT
Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Anatomy
bull Peroneus Brevis
bull Innervation
bull SPN
bull Action
bull Eversion
bull Location
bull Deep and
anterior to the
longus
Anatomy
bull Peroneus Longus
bull Innervation
bull SPN
bull Action
bull Plantarflex 1st ray
bull Evert foot
bull Location
bull Posterior and
lateral to the
peroneus brevis
Peroneal Tenosynovitis and
Tearsbull Etiology
bull Hypertrophy of the peroneal tubercle
bull Trauma
bull Overuse
bull Inflammatory arthropathy
bull Injury to the Os Peroneum
History and Physical
bull Pain
bull Posterolateral hindfoot
bull Worse with activity
bull Cutting activity
bull Exam
bull TTP over peroneals
bull Palpable thickening
bull Pain with passive inversion
bull Pain with resisted eversion
bull Visualized dislocated peroneal
Imaging
bull APlatoblique weightbearing views ankle
bull Os peroneum
bull Ultrasound
bull MRI
bull CT
Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Anatomy
bull Peroneus Longus
bull Innervation
bull SPN
bull Action
bull Plantarflex 1st ray
bull Evert foot
bull Location
bull Posterior and
lateral to the
peroneus brevis
Peroneal Tenosynovitis and
Tearsbull Etiology
bull Hypertrophy of the peroneal tubercle
bull Trauma
bull Overuse
bull Inflammatory arthropathy
bull Injury to the Os Peroneum
History and Physical
bull Pain
bull Posterolateral hindfoot
bull Worse with activity
bull Cutting activity
bull Exam
bull TTP over peroneals
bull Palpable thickening
bull Pain with passive inversion
bull Pain with resisted eversion
bull Visualized dislocated peroneal
Imaging
bull APlatoblique weightbearing views ankle
bull Os peroneum
bull Ultrasound
bull MRI
bull CT
Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Peroneal Tenosynovitis and
Tearsbull Etiology
bull Hypertrophy of the peroneal tubercle
bull Trauma
bull Overuse
bull Inflammatory arthropathy
bull Injury to the Os Peroneum
History and Physical
bull Pain
bull Posterolateral hindfoot
bull Worse with activity
bull Cutting activity
bull Exam
bull TTP over peroneals
bull Palpable thickening
bull Pain with passive inversion
bull Pain with resisted eversion
bull Visualized dislocated peroneal
Imaging
bull APlatoblique weightbearing views ankle
bull Os peroneum
bull Ultrasound
bull MRI
bull CT
Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

History and Physical
bull Pain
bull Posterolateral hindfoot
bull Worse with activity
bull Cutting activity
bull Exam
bull TTP over peroneals
bull Palpable thickening
bull Pain with passive inversion
bull Pain with resisted eversion
bull Visualized dislocated peroneal
Imaging
bull APlatoblique weightbearing views ankle
bull Os peroneum
bull Ultrasound
bull MRI
bull CT
Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Imaging
bull APlatoblique weightbearing views ankle
bull Os peroneum
bull Ultrasound
bull MRI
bull CT
Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Conservative Treatment
bull Immobilization
bull Short leg cast vs boot
bull 3-4 weeks
bull Careful cortisone injection in sheath
bull Risk of rupture
bull Immobilize after injection
bull PRP injections
bull No data to support
Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Conservative Treatment
bull Orthotic
bull Lateral post
bull Physical therapy
bull NSAIDS
bull Topical
bull PO
bull Activity modification
Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Surgical Treatment
bull Steps
bull Synovectomy amp debridement
bull Tendon repair
bull +- Augmentation or reconstruction
bull Groove deepening
bull Excision
bull Peroneal tubercle Os peroneum
bull Closure retinaculum
Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Tendoscopy
Synovectomy Debridement Release of Adhesions and
Removal of Peroneal Tubercle
Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Open Technique
Incision
Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Retinaculum incised
Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Tendon Repair
Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Groove Deepening
bull Significant reduction in pressure within peroneal
groove(Title CI Hung-Geun J Parks BG Schon LC Foot Ankle Int 2005)
bull May minimize recurrence
Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Groove Deepening
Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Hypertrophic Peroneal
Tubercle
Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Tubercle Excision
Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Tubercle Excision
Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Final Appearance
Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Outcomes
bull Persistent pain
bull Recurrent tears
bull Progressive tendinopathy
Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Augmentation Options
bull Allograft
bull Dermal - Graft jacket Memoderm Puros TenSix
bull Amniotic ndash Neox Reset
bull Xenograft
bull Porcine ndash Matristem Conexa Zimmer Patch
Restore
bull Bovine - Tenoglide
bull Equine - OrthAdapt
Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Theoretical Advantages
bull Augment repair
bull Allows for stronger repair
bull Allows for earlier rehab
bull Minimize adhesion formation and inflammation
Rapley JH Crates J Barber A Foot Ankle Int 2010 Feb31(2)136-40
Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Tenoglide
Photo Courtesy of Stuart Miller MD and Integra
Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Neox
Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Neox
Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Neox
Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Neox
Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Revision
bull Peroneal tenodesis
bull FHL transfer to the base of the 5th metatarsal
bull Primary
bull Staged reconstruction w Hunter rods
bull Allograftautograft reconstruction
bull Semitendinosis
Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Revision
bull FHL transfer to the base of the 5th Metatarsal
bull Recreates dynamic eversion of the peroneals
bull Does not recreate PF of the 1st Ray
bull Lose one level of strength
Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull First reported by Wapner in 1994 (AAOS)
bull Long term follow up gt 5 years
bull 7 patients
Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull Incision from 5th base
to tip to distal fibula
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull Expose and free up the peroneal tendons
bull Both tendons encased in scar and split
bull Excision of remaining portion of peroneals from myotendinous junction to distal tendon
bull Debridement of area of old sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull Measure Hunter rod
and excise remaining
peroneus brevis
bull Attach distal end of
Hunter rod to stump of
peroneus brevis
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull Close the sheath and
check to be sure the
rod glides
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull Patients performed passive range of motion
exercises four times a day for 20 minutes for
three months
bull Protected weight bearing in cast walker
bull Return to OR for stage two - transfer of FHL
tendon
Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull Harvest FHL from
midfoot
bull Pull FHL tendon into
posterior incision
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull Open proximal lateral incision
bull Identify Hunter rod
bull Pull FHL through into lateral incision
bull Open distal incision and release Hunter rod
bull Pull FHL through new sheath
Photo Courtesy of Keith Wapner MD
Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Staged Reconstruction
bull Anastamose the FHL
to the stump of the
peroneus brevis
Photo Courtesy of Keith Wapner MD
Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Results
bull 4 excellent
bull 2 good
bull 1 poor
bull All said they would repeat the procedure
Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Allograft Reconstruction
Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Materials and Methods
bull Retrospective chart review (July 2007-2012)
bull Patients who underwent reconstruction of tears involving gt50 cross sectional area
bull Mechanism of injury
bull Concomitant operative procedures
bull Strength (MRC)
bull VAS pain
bull SF-12 physical health
bull LEFS
bull Complications
bull Imaging
bull Statistical Analysis
bull Two-tailed Student t-test
Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Surgical Technique
Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Study Population
bull 14 patients
bull Pre-operative MRI
bull 20 (314) acute
bull Mean age 54 years (22-70)
bull Ruptures 12 Pb 5 Pl 3 Both
bull Reconstructions 11Pb 2 Pl 1 Both
bull Concomitant procedures
bull Pl tenosynovectomy (5) Brostrom-Gould (2) Fibular
groove deepening (2) Dwyer (1) Tenodesis PlPb
(1)
Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Outcomes
bull Mean graft length 108cm (6-20cm)
bull Mean fu 17 months (Range 7-47 Median 12)
bull 4 sural sensory nerve palsies ( 2 transient)
bull No wound complications infections reruptures re-operations
bull No allograft associated complications
bull 614 underwent high resolution sonography-intactindependent glide
bull All patients returned to preinjury activity level
bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

bull p= 000001
Subjective Outcomes
p= 002
p= 00005
Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Eversion Strength
bull p=
00
03
bull 914 (64) 55 strength
Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Discussion
bullLimitations
bullSample size
bullRelatively short term
follow-up
bullLack of control
bullComparison to autologous
transfer
bullTenodesis
bullKinematics comparison
bullConsiderations
bullCost
bullAutograft options
bullOperative time
bullDonor site morbidity
bullAllograft related
complications
bullRerupture
bullDisease transmission
bullInfection
bull First report of single stage intercalary segment allograft reconstruction
Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Conclusionsbull Allograft reconstruction of the peroneal tendons can
safely
Restore strength
Restore function
Improve pain
bull Low risk of complicationsbull Allograft
bull Surgical
bull No donor site morbidity
bull Further investigation
Long term outcomes
Kinematic comparison to treatment alternatives
Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Reversal Restore Power
bull 3 patients
bull Pain and loss of strength from tenodesis
bull Reversal
bull Allograft
bull Find stumps and recreate
Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Reversal Restore Power
Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

Out There
Primary Repair with Allograft
RE
ECTthe ankle
the foot

RE
ECTthe ankle
the foot