Pediatric Blunt Abdominal Trauma Does this patient need an Abdominal CT?
Upload
yana-puckett-mdCategory
view
283download
8description

Pediatric Abdominal Trauma
Yana Puckett, MD

Topics to Discuss
• Labs• Diagnostic Modalities –Ultrasound, CT, Laparoscopy• Treatment Modalities –Angiography• Liver and Spleen Management• Pancreas Injury• Renal Injury• Duodenal Injury• Hollow Viscus Injury• Gallbladder Injury• Urinary Bladder Injury

Abdominal Trauma
• Falls are the most frequent mechanism in children.
• MVC abdominal trauma is most deadly.• Anatomically smaller size of children & less
fatty tissue surrounding major organs results in increased abdominal trauma with less velocity than in adults.

Initial Evaluation and Diagnosis of Abdominal Injuries
• Thorough History and Physical
• Seatbelt Sign, Handle Bar Mark suspicious for abdominal injuries.
• Vital signs – can lose up to 45% of circulating blood volume, and exhibit tachycardia as only abnormal vital sign.

Laboratory Testing
• CBC, CMP, Amylase, Lipase, Coag Studies, Urinalysis.
• Elevated AST/ALT with positive physical exam highly predictive for abdominal trauma in some studies - not diagnostic for a particular injured organ *.
• Interestingly, routine amylase and lipase determinations do not appear to be very reliable or cost effective screening tools*.
*Capraro AJ, Mooney D, Waltzman ML. The use of routine laboratory studies as screening tools in pediatric abdominal trauma. Pediatr Emerg Care 2006;22:480–4.

Laboratory Testing
• Overall: laboratory panels in the evaluation of children at risk for intra-abdominal injuries are best utilized in conjunction with physical examination findings and as a screen to determine those children who might require further diagnostic testing, particularly imaging. *
*Capraro AJ, Mooney D, Waltzman ML. The use of routine laboratory studies as screening tools in pediatric abdominal trauma. Pediatr
Emerg Care 2006;22:480–4.

Computed Tomography
• CT Abdomen with IV contrast is preferred modality for diagnosis of intra-abdominal injuries in hemodynamically stable children (1).
• Intestine and Pancreas are more difficult to definitvely diagnose by CT – request coronal reconstructions.
• Addition of oral contrast to the standard IV contrast may be helpful, especially in evaluating the duodenum and pancreatic head(2).

Computed Tomography• Radiation exposure during CT of major concern in children.
• Over 7 million scans performed in children over last decade, mostly for trauma and appendicitis.
• Longitudinal, population-based study in Great Britain demonstrated an increased incidence of leukemia and brain cancer after repeated CT scans in children (3).
• Models extrapolated from radiation exposure from atomic bomb explosions- one fatal cancer per 1000 CT scans performed in young children estimated (3).

Computed Tomography
• Children have a longer life expectancy than adults, resulting in a larger window of opportunity for expressing radiation damage.
• Children may receive a higher radiation dose than necessary if CT settings are not adjusted for their smaller body size.

Ultrasound
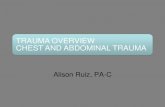
• FAST examination developed to assess the presence of intra-abdominal free fluid (with examination of Morrison’s pouch, the pouch of Douglas, and the left flank) or fluid within the pericardial sac (subxiphoid view), thus indicate the need for operative exploration.
• In multiple studies, traditional FAST examination has been found to have a low sensitivity and specificity for the diagnosis of injury in children (4-5).

FAST

Laparoscopy
• Allows for direct visualization of bowel, mesentery, and diaphragmatic surfaces - regions that CT has traditionally not been as accurate.
• Child with free fluid without evidence of solid organ injury, especially if physical exam finding of seatbelt or handlebar mark is found.
• In two relatively large reviews, laparoscopy was found to be safe and beneficial by avoiding laparotomy in a significant number of patients (6,7).

Liver and Spleen Injury Management
• 90–95% injuries to liver and spleen in children managed non-operatively.
• Child should have normal hemodynamics, be monitored closely for signs of ongoing hemorrhage.
• Most children who fail nonoperative management do so within four hours of injury as a result of shock, peritonitis, or persistent bleeding (8).

Liver and Spleen Injury Management

Pancreatic Injuries



Liver and Spleen Management

Liver and Spleen Management
• Splenectomy easily controls bleeding in hemodynamically unstable patient with active exsanguination from a massively damaged spleen, although at the theoretical cost of a long-term risk of postsplenectomy sepsis.
• Partial splenectomy, spenorhaphy obtions if not in shock.

Postsplenectomy Sepsis
• The reported incidence is around 0.23% a year, with an increased incidence in children less than 2 years of age, and those that underwent splenectomy for hematologic reasons (9).
• Vaccination with 23-valent pneumococcal vaccine, meningococcus vaccine, and H. Influenza B after splenectomy required.

Interventional Radiology in Abdominal Trauma
• Angioembolization frequently used in adults with splenic or liver vascular injuries.
• Multiple studies in children, however, demonstrate that a contrast blush is associated with the need for operative intervention in less than 20% of splenic injuries .*
*Lutz N, Mahboubi S, Nance ML, et al. The significance of con- trast blush on computed tomography in children with splenic injuries. J Pediatr Surg 2004;39:491–4.
• On the other hand, small single-center studies and case reports demonstrate that interventional radiological techniques are safe in children, and have been effective when utilized.*
*Kiankhooy A, Sartorelli KH, Vane DW, et al. Angiographic embolization is safe and effective therapy for blunt abdominal solid organ injury in children. J Trauma 2010;68:526–31.
• The pediatric population that seems most amenable to this technique are children with evidence of ongoing bleeding but are hemodynamically stable, or those that develop bleeding later in their hospital course.


Pancreatic Injury Management
• Occur in fewer than 5% of pediatric abdominal injuries, and can be difficult to diagnose.
• Blunt mechanism MCC: MVC, handlebar of bike.
• Epigastric pain and bilious emesis, particularly in the case of injuries that have a delayed presentation .
• Contusions, without evidence of pancreatic ductal injury, can be managed nonoperatively with nothing by mouth.

Pancreatic Injury Management
• Trends in serum amylase and lipase may be helpful, although the absolute value of these tests does not correlate with outcome (10).
• Child should be followed clinically as an oral diet is reintroduced.
• Management of ductal transection is currently controversial.




Pancreatic Injury Management
• Distal pancreas duct injury – spleen preserving distal pancreatectomy.
• High morbidity: endocrine insufficiency.
• Roux-en-Y distal pancreaticojejunostomy to drain distal pancreas has been advocated.
• Nonoperative approach with percutaneous or endoscopic drainage of subsequent pseudocysts has been proposed by several studies.

Pancreatic Trauma Management• APSA Trauma Committee retrospective review compared operative and
nonoperative management.
• Demonstrated similar length of hospitalization, but higher rate of pseudocyst formation and days on TPN in nonoperative group (11).
• Grade I and II– conservative treatment.
• Grade II and III and even IV- drainage of pancreatic bed.
• Grade V- unclear, needs further research.
• Patients undergoing NOM often require ERCP to define the ductal anatomy, perform sphincterotomy, and potentially stent the pancreatic duct, as well as percutaneous or endoscopic drainage of pseudocysts.

Renal Trauma• Most commonly injured GU organ.
• Blunt trauma accounts for 80-90% of renal injuries in children.
• In several series, the most severe grade of injury was related to dirt bikes, ATV rollovers, and bicycles (14-15).
• Stable patients with high grade injury are typically placed at bed rest with serial exams, blood counts, and close hemodynamic monitoring until the gross hematuria resolves.
• However, there are no evidence-based guidelines regarding length of activity restriction in these patients.




Renal Trauma• Present with gross hematuria and flank pain.
• The diagnosis is confirmed by abdominal CT scan which is highly sensitive.
• Expectant NOM is widely accepted for hemodynamically stable grade I-III renal injuries which do not have urinary extravasation.
• The main indications for immediate explo- ration in a child with a renal injury are hemodynamic instability.
• Selective angioembolization of renal artery branches has been successful in nearly 80% of cases with delayed hemorrhage (16).



Renal Trauma
• Penetrating renal injury in children is rare, but typically requires exploration for management. Selective observation for penetrating renal trauma, however, is also being investigated.
• Hemodynamically unstable patients with penetrating injury or patients with an expanding retroperitoneal hematoma require renal exploration.
• During exploration, a one-shot IVP may be helpful to identify the injured area and confirm the pres- ence of a functioning contralateral kidney.

Diaphragmatic Injury• Rarely occurs in isolation.
• Emergent exploration in patients with diaphragm injury indicated in hemodynamically unstable patient with multiple organ injury.
• Repair of diaphragmatic defect is typically possible after debridement of any compromised tissue.
• If large defects are found, prosthetic patch may be needed to minimize tension.
• Successful laparoscopic or thoracoscopic repair of diaphragmatic injuries can be performed in hemodynamically stable children or delayed diagnoses.

Hollow Viscus Injury
• Areas of mesenteric fixation - proximal jejunum near ligament of Treitz, distal ileum near ileocecal valve, rectosigmoid junction are particularly vulnerable to injury via acceleration/deceleration shearing forces.
• Seat belt sign markers of severe deceleration injury to the abdomen.
• CT findings suggestive of hollow viscus injury include bowel wall thickening and enhancement, mesenteric stranding, and free intraperitoneal fluid in the absence of solid organ injury.

Hollow Viscus Injury
• Hemodynamically stable patients with evidence of bowel injury or in equivocal cases with concerning physical signs or symptoms - diagnostic laparoscopy is a very reasonable approach.
• In cases with penetrating trauma, local wound exploration to identify penetration of the anterior abdominal fascia is recommended as the initial diagnostic maneuver – if unclear, diagnostic laparoscopy.

Duodenal Injuries• Majority of duodenal injuries in children result from blunt
mechanisms .
• Abdominal CT is the test of choice to evaluate for duodenal injury.
• Duodenal hematomas may be found on CT or upper GI studies revealing transmural thickening with lumenal duodenal narrowing, or partial obstruction without evi- dence of extravasation of air or contrast .
• Typically managed nonoperatively with nasogastric decompression and TPN over one to three weeks.

Grades of Duodenal Injury


Duodenal Injury
• When high clinical suspicion for duodenal injury exists and initial radiographs and abdominal CT scans do not reveal significant injury, serial CT scans may be indicated to look for the delayed development of retroperitoneal air (12).
• Delay in diagnosis of greater than 24 hours is
associated with established peritoneal inflammation, poor tissue integrity, and higher leak rate following primary repair (12).


Duodenal Injury• Operative intervention for duodenal injuries should be made based
on clinical judgment.
• Most full-thickness injuries with minimal tissue destruction repaired primarily.
• In patients with a complex duodenal injury, diversion and drainage may be needed.
• Earlier diagnosis of duodenal injuries may make the injury more amenable to primary repair while a significant delay in diagnosis (>24 hours), or those with a grade III or greater injury, may warrant proximal drainage via a gastrojejunostomy and pyloric exclusion (12).

Injury to Stomach
• Very rare, but blunt injury to the stomach can occur and is typically seen in the patient who has just eaten, as the full stomach is more vulnerable to burst injury.
• When gastric rupture occurs, usually located along the greater curvature with a blow-out or stellate configuration.
• Debridement with repair of the injury is sufficient.

Gallbladder Injury
• Gallbladder is rarely injured in children.
• Predisposing factors for gallbladder trauma are a thin-walled normal gallbladder, a distended gallbladder after a meal, and alcohol ingestion.
• If identified, a cholecystectomy is usually per- formed. This may be performed via laparoscopy or laparotomy.

Urinary Bladder Injury
• Second most common GU injury in children.
• CT Cystoscopy is used to evaluate a suspected bladder injury.
• Prompt repair for intraperitoneal ruptures – two layered closure with absorbable suture material and either transurethral or suprapubic drains.
• Extraperitoneal ruptures- uretheral catheter drainage is sufficient.

References
1. Trauma AcoSCo. Advanced Trauma Life Support for Doctors, Student Course Manual. In: American College of Surgeons Committee on Trauma. Chicago; 2004. p. 251.
2. Nastanski F, Cohen A, Lush SP, et al. The role of oral contrast administration immediately prior to the computed tomographic evaluation of the blunt trauma victim. Injury 2001;32:545–9.
3. Pearce MS, Salotti JA, Little MP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: A retrospective cohort study. Lancet 2012;380: 499–505.
4. Benya EC, Lim-Dunham JE, Landrum O, et al. Abdominal sonography inexamination of children with blunt abdominal trauma. AJR Am J Roentgenol 2000;174:613–1616.
5. Coley BD, Mutabagani KH, Martin LC, et al. Focused abdominal sonography for trauma (FAST) in children with blunt abdominal trauma. J Trauma 2000;48:902–6.
6. Feliz A, Shultz B, McKenna C, et al. Diagnostic and therapeutic laparoscopy in pediatric abdominal trauma. J Pediatr Surg 2006;41:72–7. 7. Marwan A, Harmon CM, Georgeson KE, et al. Use of laparos- copy in the management of pediatric abdominal trauma. J Trauma 2010;69:761–4. 8. Holmes JH 4th, Wiebe DJ, Tataria M, et al. The failure of non- operative management in pediatric solid organ injury: A multi- institutional
experience. J Trauma 2005;59:1309–13. 9. Morgan TL, Tomich EB. Overwhelming post-splenectomy infec- tion (OPSI): A case report and review of the literature. J Emerg Med 2012;43:758–
63. 10. Herman R, Guire KE, Burd RS, et al. Utility of amylase and lipase as predictors of grade of injury or outcomes in pediatric patients with pancreatic
trauma. J Pediatr Surg 2011;46:923–6. 11. Paul MD, Mooney DP. The management of pancreatic injuries in children: Operate or observe. J Pediatr Surg 2011;46:1140–3. 12. Ladd AP, West KW, Rouse TM, et al. Surgical management of duodenal injuries in children. Surgery 2002;132:748–53. 13. Nelson R, Singer M. Primary repair for penetrating colon injuries. Cochrane Database Syst Rev 2003:CD002247. 14. Kluemper C, Rogers A, Fallat M, et al. Genitourinary injuries in pediatric all-terrain vehicle trauma–a mechanistic relationship? Urology
2010;75:1162–4. 15. Wu HY, Gaines BA. Dirt bikes and all-terrain vehicles: The real threat to pediatric kidneys. J Urol 2007;178:1672–4. 16. Goffette PP, Laterre PF. Traumatic injuries: Imaging and inter- vention in post-traumatic complications (delayed intervention). Eur Radiol
2002;12:994–1021.