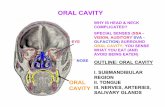
Oral Cavity carcinoma
53
Oral Cavity 1 Mar. 2006 Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme Oral Cavity carcinoma
Transcript of Oral Cavity carcinoma

Oral Cavity 1Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Cavity carcinoma

Oral Cavity 2Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Cavity carcinoma
•• WorkWork--up procedureup procedure
•• TNM stagingTNM staging
•• Primary treatmentPrimary treatment
•• FollowFollow--upup
•• Treatment of recurrent and/or Treatment of recurrent and/or metastaticmetastatic diseasedisease
•• Appendix: surgical techniquesAppendix: surgical techniques
•• ReferencesReferences

Oral Cavity 3Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Standard clinical evaluation Evidence Option
l Complete history of the diseasel Alcohol and tobacco consumptionl Weight and weight lossl Performance status (Karnofsky or WHO scale)l Neck examinationl Evaluation of cranial nerves V2 ,V3, VII, XIIl Drawing of all lesions on a common templatel Biopsy under local anesthesia
Type CType CType CType CType CType CType CType C
Std.Std.Std.Std.Std.Std.Std.Std.

Oral Cavity 4Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Advanced clinical evaluation Evidence Option
• Dental examination by oral surgeon • Panendoscopy under general anesthesia • Prosthetic rehabilitation (if maxillectomy) • Nutritional assessment • PEG
Type C Type C Type C Type C
Type C
Std. Std. Std. Std.
Individ

Oral Cavity 5Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Laboratory tests Evidence Option
l Hemogram, ionogram, coagulation tests, liver enzymes, Kidney function
l Thyroid function: TSH (if radiotherapy scheduled)
Type C
Type C
Std.
Std.

Oral Cavity 6Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Local imaging and metastatic work-up Evidence Option
• Orthopantomogram (+dental X-rays ifneeded)
• MRI ± CT scan1 (oral cavity and neck)• Chest X-ray and thoracic spiral CT• Esogastroscopy• Additional examination based on
previous findings• PET scan
Type C
Type CType CType CType C
Type 3
Std.Std.Std.Std.Ind.Std.
Invest.
1See guidelines for loco-regional imaging

Oral Cavity 7Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Cavity carcinoma
•• WorkWork--up procedureup procedure
•• TNM stagingTNM staging
•• Primary treatmentPrimary treatment
•• FollowFollow--upup
•• Treatment of recurrent and/or Treatment of recurrent and/or metastaticmetastatic diseasedisease
•• Appendix: surgical techniquesAppendix: surgical techniques
•• ReferencesReferences

Oral Cavity 8Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Staging Evidence Option
l TNM classification (5 th ed., 1997)l WHO International Classification of Diseases for
Oncology (ICD-O 9 or ICD-O 10)
Type C
Type C
Std.
Std.

Oral Cavity 9Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
•• TisTis: Carcinoma in situ: Carcinoma in situ•• T1: Tumor 2 cm or less in greatest dimensionT1: Tumor 2 cm or less in greatest dimension•• T2: Tumor > 2 cm but T2: Tumor > 2 cm but ≤≤ 4 cm in greatest dimension4 cm in greatest dimension•• T3: Tumor > 4 cm in greatest dimensionT3: Tumor > 4 cm in greatest dimension•• T4 (lip) Tumor invades adjacent structures (through cortical boT4 (lip) Tumor invades adjacent structures (through cortical bone,ne,
inferior alveolar nerve, floor of mouth, skin of face)inferior alveolar nerve, floor of mouth, skin of face)•• T4 (oral cavity) Tumor invades adjacent structures (through corT4 (oral cavity) Tumor invades adjacent structures (through corticaltical
bone, into deep muscle of tongue, maxillary sinus, skin.)bone, into deep muscle of tongue, maxillary sinus, skin.)(Superficial erosion alone of bone/tooth socket by gingival p(Superficial erosion alone of bone/tooth socket by gingival primaryrimaryis not sufficient to classify as T4)is not sufficient to classify as T4)
TNM/AJCC 1997 StagingTNM/AJCC 1997 Staging

Oral Cavity 10Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
TNM/AJCC 1997 StagingTNM/AJCC 1997 Staging
• N0: no regional node metastasis• Nx: regional nodes cannot be assessed• N1: single ipsilateral node, ≤ 3 cm• N2a: single ipsilateral node, > 3 cm and ≤ 6 cm• N2b: multiple ipsilateral nodes, ≤ 6 cm• N2c: controlateral or bilateral nodes, ≤ 6 cm• N3: node > 6 cm

Oral Cavity 11Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
TNM/AJCC 1997 StagingTNM/AJCC 1997 Staging
•• Mx: Distant Mx: Distant metastasismetastasis cannotcannot bebe assessedassessed•• M0: No distant M0: No distant metastasismetastasis•• M1: Distant M1: Distant metastasismetastasis

Oral Cavity 12Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Cavity carcinoma
•• WorkWork--up procedureup procedure
•• TNM stagingTNM staging
•• Primary treatmentPrimary treatment
•• FollowFollow--upup
•• Treatment of recurrent and/or Treatment of recurrent and/or metastaticmetastatic diseasedisease
•• Appendix: surgical techniquesAppendix: surgical techniques
•• ReferencesReferences

Oral Cavity 13Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of lip carcinoma Evidence Option
l T1-T2 N0 :Surgery T (only)Brachytherapy (T<3cm, no ulceration, no infiltration, dry vermillion)
l T3-T4 N0:Surgery T + SOH ND ± post- operative RxTh1
l T1-T4 N1:Surgery T + SOH or radical modified ND± post-operative RxTh1
l T1-T4 N2a-N3:Surgery T + radical modified ND2 ± post-operative RxTh1
Type 3Type 3
Type 3
Type 3
Type 3
Std.Std.
Std.
Std.
Std.
1See guidelines for post-operative radiotherapy2Radical or extended neck dissection might be required (e.g. N3)

Oral Cavity 14Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of buccal mucosa carcinoma Evidence Option
l T1N0 :Surgery T (only)Brachytherapy
l T2N0 :Surgery + SOH NDBrachytherapy (T< 3 cm, no oral commissure extension) + SOH ND
l T1-T4 N1-N3 :Surgery + SOH or radical modified ND± post-operative RxTh2
Type 3Type 3
Type 3Type 3
Type 3
Std.Std.
Std.Std.
Std.
1Radical or extended neck dissection might be required (e.g. N3)2See guidelines for post-operative radiotherapy

Oral Cavity 15Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of oral sulcus carcinoma Evidence Option
l T1N0-N1:Surgery T + SOH or radical modified ND1
l T1 N2-N3:Surgery T + radical modified ND1, 2 ± post-operative RxTh3
l T2-T4 N0-N1:Surgery T + alveolar resection + reconstruction +SOH ND2 ± post-operative RxTh3
l T2-T4 N2-N3:Surgery T + alveolar resection + reconstruction + radical modified ND1, 2 ± post-operative RxTh3
Type 3
Type 3
Type 3
Type 3
Std.
Std.
Std.
Std.
1Bilateral neck dissection for midline tumors2Radical or extended neck dissection might be required (e.g. N3)3See guidelines for post-operative radiotherapy

Oral Cavity 16Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of upper alveolar rim carcinoma Evidence Option
l T1-T4 N0 :Surgery T (only)
l T1-T4 N1 :Surgery T + SOH ND ± post-operative RxTh1
l T1-T4 N2-N3 :Surgery T + radical modified ND2 ± post-operative RxTh1
Type 3
Type 3
Type 3
Std.
Std.
Std.
1See guidelines for post-operative radiotherapy2Radical or extended neck dissection might be required (e.g. N3)

Oral Cavity 17Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of lower alveolar rim and retromolartrigone carcinoma
Evidence Option
l T1 N0-N1:Surgery T + SOH ND1 ± post-operative RxTh2
l T1 N2-N3:Surgery T + radical modified ND1, 3 ± post-operative RxTh2
l T2-T4 N0-N1:Surgery T + reconstruction + SOH ND1 ± post-operative RxTh2
l T2-T4 N2-N3:Surgery T + reconstruction + radical modifiedND1, 3 ± post-operative RxTh2
Type 3
Type 3
Type 3
Type 3
Std.
Std.
Std.
Std.
1 Bilateral neck dissection for midline tumors2 See guidelines for post-operative radiotherapy3 Radical or extended neck dissection might be required (e.g. N3)

Oral Cavity 18Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of hard palate carcinoma Evidence Option
l T1-T3 N0 :Surgery T ± reconstruction ± post-operative RxTh1
l T1-T3 N1 :Surgery T ± reconstruction + bilateral SOH ND ± post-operative RxTh1
l T4 N0-N1 :Surgery T + reconstruction + bilateral SOH ND +post-operative RxTh1
l T1-T4 N2-N3 :Surgery T ± reconstruction + bilateral radical modified ND2 ± post-operative RxTh1
Type 3
Type 3
Type 3
Type 3
Std.
Std.
Std.
Std.
1 See guidelines for post-operative radiotherapy2 Radical or extended neck dissection might be required (e.g. N3)

Oral Cavity 19Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of mobile tongue (dorsum, apex, ventral side) carcinoma Evidence Option
l T1 N0-N1 :Surgery T + bilateral levels I-IV ND ± post-operative RxTh1
Brachytherapy + bilateral SOH NDRxTh (T+levels I-III) + brachytherapy T
l T2 N0-N1 :Surgery T ± reconstruction + bilateral levels I-IV ND ± post-operative RxTh1
l T1-T2 N2-N3 :Surgery T ± reconstruction +bilateral radical modified ND2 +post-operative RxTh1
“Locally advanced” RxTh protocols (T+N)3 ± ND4
l T3-T4 N0-N3 :“Locally advanced” RxTh protocols (T+N)3 ± ND4
Surgery T + reconstruction +bilateral ND + post-operative RxTh1
Type 3Type 3Type 3
Type 3
Type 3
Type 3
Type 3Type 3
Std.Std.Std.
Std.
Std.
Std.
Std.Std.
1 See guidelines for post-operative radiotherapy 2 Radical or extended neck dissection might be required (e.g. N3) 3 See guidelines for organ preservation protocols 4 See guidelines for post-radiotherapy ND (slide 27)

Oral Cavity 20Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of mobile tongue (lateral border) carcinoma Evidence Option
l T1 N0 :Surgery T + unilateral SOH NDSurgery TBrachytherapy T
l T1 N1 :Surgery T + unilateral levels I-IV ND ± post-operative RxTh1
Brachytherapy + unilateral levels I-IV ND or RxThl T2 N0-N1 :
Surgery T ± reconstruction + unilateral levels I-IV ND ± post-operative RxTh1
l T1-T2 N2-N3 :Surgery T ± reconstruction +unilateral radical modified ND2 +Post-operative RxTh1
“Locally advanced” RxTh protocols (T+N)3 ± ND4
l T3-T4 N0-N3 :“Locally advanced” RxTh protocols (T+N)3 ± ND4
Surgery T + reconstruction +unilateral ND2 + post-operative RxTh1
Type 3Type 3Type3
Type 3Type 3
Type 3
Type 3
Type 3
Type 3Type 3
Std.Std.Std.
Std.Std.
Std.
Std.
Std.
Std.Std.
1 See guidelines for post-operative radiotherapy2 Radical or extended neck dissection might be required (e.g. N3)3 See guidelines for organ preservation protocols4 See guidelines for post-radiotherapy ND (slide 27)

Oral Cavity 21Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of anterior floor of mouth carcinoma Evidence Optionl T1 N0 :
Surgery T + bilateral SOH NDBrachytherapy + bilateral SOH ND
l T2 N0 :Surgery T ± reconstruction + bilateral SOH ND ± post-operative RxTh1
l T1-T2 N1 :Surgery T ± reconstruction + bilateral SOH or radical modified ND ± post-operative RxTh1
l T1-T2 N2-N3:Surgery T ± reconstruction + bilateral radical modified ND2 ± post-operative RxTh1
“Locally advanced” RxTh protocols (T+N)3 ± ND4
1 See guidelines for post-operative radiotherapy2 Radical or extended neck dissection might be required (e.g. N3)3 See guidelines for organ preservation protocols4 See guidelines for post-radiotherapy ND (slide 27)
Type 3Type 3
Type 3
Type 3
Type 3
Type 3
Std.Std.
Std.
Std.
Std.
Std.

Oral Cavity 22Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of anterior floor of mouth carcinoma Evidence Optionl T3-T4 (no bone invasion), N0-N3 :
“Locally advanced” RxTh protocols (T+N)3 ± ND4
Surgery T ± reconstruction + bilateral radical modified ND2 ± post-operative RxTh1
l T4 (bone invasion), N0-N3 :Surgery T ± reconstruction + bilateral radical modified ND2 ± post-operative RxTh1
Type 3Type 3
Type 3
Std.Std.
Std.
1 See guidelines for post-operative radiotherapy2 Radical or extended neck dissection might be required (e.g. N3)3 See guidelines for organ preservation protocols4 See guidelines for post-radiotherapy ND (slide 27)

Oral Cavity 23Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of posterior floor of mouth carcinoma Evidence Optionl T1 N0 :
Surgery T + unilateral SOH ND1
l T2 N0 :Surgery T ± reconstruction + unilateral SOH ND ± post-operative RxTh2
l T1-T2 N1 :Surgery T ± reconstruction + unilateral SOH or radicalmodified ND ± post-operative RxTh2
l T1-T2 N2-N3:Surgery T ± reconstruction + unilateral radical modified ND3 ± post-operative RxTh2
“Locally advanced” RxTh protocols (T+N)4 ± ND5
Type 3
Type 3
Type 3
Type 3
Type 3
Std.
Std.
Std.
Std.
Std.
1 Bilateral neck dissection for midline tumors2 See guidelines for post-operative radiotherapy3 Radical or extended neck dissection might be required (e.g. N3)4 See guidelines for organ preservation protocols5 See guidelines for post-radiotherapy ND (slide 27)

Oral Cavity 24Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Treatment of posterior floor of mouth carcinoma Evidence Optionl T3-T4 (no bone invasion), N0-N3 :
“Locally advanced” RxTh protocols (T+N)4 ± ND5
Surgery T ± reconstruction + unilateral radical modified ND3 ± post-operative RxTh2
l T4 (bone invasion), N0-N3 :Surgery T ± reconstruction + unilateral radical modified ND3 ± post-operative RxTh2
Type 3Type 3
Type 3
Std.Std.
Std.
1 Bilateral neck dissection for midline tumors2 See guidelines for post-operative radiotherapy3 Radical or extended neck dissection might be required (e.g. N3)4 See guidelines for organ preservation protocols5 See guidelines for post-radiotherapy ND (slide 27)

Oral Cavity 25Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
InvestInvest..StdStd..
Type 3Type 3Type 3Type 3
•• SentinelSentinel nodenode biopsybiopsy•• ComprehensiveComprehensive neck neck nodenode dissection/irradiationdissection/irradiation
accordingaccording to to thethe recommendationsrecommendations for for eacheach subsitessubsites**
**SeeSee guidelines for guidelines for targettarget volumes on volumes on slideslide 2727
Option Option EvidenceEvidenceProceduresProcedures for neck for neck nodenode treatmenttreatment

Oral Cavity 26Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Primary treatment: RxTh regimen Evidence Optionl Target volumes
T: CTV = GTV + 1.5-0.5 cm margin depending on anatomical barriersN: see table on node levels according to T site
l Technique-conformal radiotherapy-IMRT radiotherapy
l Dose / fractionation / treatment time- Early stage:1
-prophylactic dose: 50 Gy,-therapeutic dose: 66-70 Gy, 2 Gy daily
-"moderately advanced"2 / "locally advanced"3 stage-on protocol: GORTEC 99-02 / IMCL CP02-9815-off protocol: moderately accelerated regimen (concomitant boost)
- post-operative RxTh-dose: 60-64 Gy, 2 Gy daily4
Type 3Type 3
Type CType C
-Type 1
Type 2
Std.Invest.
Std.Std.
Invest.Std.
Std.1T1 N0-N12T2 N0-N13any T N2a-N34See guidelines for post-operative radiotherapy

Oral Cavity 27Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Target Volumes: oral cavityTarget Volumes: oral cavityLevel of evidence : type 3 / option : standardLevel of evidence : type 3 / option : standard
Stage Ipsilateral neck Controlateral neck
N0-N1 I-II1-III + IV for ant. I-II1-III + IV for ant. tongue tumor or oroph. ext. tongue tumor or oroph. ext.
N2a-N2b I-II-III-IV-V2 I-II1-III + IV for ant. tongue tumor or oroph. ext.
N2c According to N stage on According to N stage oneach side of the neck each side of the neck
N3 I-II-III-IV-V ± adjacent I-II1-III + IV for ant. structures according to clinical tongue tumor or oroph. ext.
and radiological data1level IIb could be omitted for N0 patients2Level V could be omitted if only level I-III are involved

Oral Cavity 28Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Std.Type 3•• Planned ND (SND, RMND, RND or extended ND) 2-3 months after completion of RxTh in patients with acontrolled primary site and in case of residual or
suspected residual, resectable N disease irrespective of the initial N stage
OptionEvidencePrimary treatment: neck dissection following a primary radiotherapy

Oral Cavity 29Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Cavity carcinoma
•• WorkWork--up procedureup procedure
•• TNM stagingTNM staging
•• Primary treatmentPrimary treatment
•• FollowFollow--upup
•• Treatment of recurrent and/or Treatment of recurrent and/or metastaticmetastatic diseasedisease
•• Appendix: surgical techniquesAppendix: surgical techniques
•• ReferencesReferences

Oral Cavity 30Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Follow-up Evidence Option
l Clinical examination of head and neck mucosa(including fiberoptic ) and neck palpation / performance status / nutritional assessmentevery 2 months (first 2 years),every 6 months (years 3-5),once a year (> 5 year)
l Dental examination and orthopantomogram every6 months
l Chest X-ray every yearl Chest spiral CT every yearl Laboratory tests: TSH every year (if Radiotherapy
delivered)l Evolution of late toxicity (EORTC/RTOG) scale
Type C
Type C
Type CType CType C
Type C
Std.
Std.
Std.Invest.
Std.
Std.

Oral Cavity 31Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Cavity carcinoma
•• WorkWork--up procedureup procedure
•• TNM stagingTNM staging
•• Primary treatmentPrimary treatment
•• FollowFollow--upup
•• Treatment of recurrent and/or Treatment of recurrent and/or metastaticmetastatic diseasedisease
•• Appendix: surgical techniquesAppendix: surgical techniques
•• ReferencesReferences

Oral Cavity 32Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Salvage treatment for recurrent disease Evidence Option
l Lip, mobile tongue, floor of mouth: rT1 N0 : Brachytherapy
Surgeryl Any other T, any other N
Surgery + radical ND ± post-operative RxTh1 if not previously deliveredRxThPalliative care
l Metastasis :Chemotherapy + best supportive care
Type 3Type 3
Type 3
Type 3Type 3
Type 3
Std.Std.
Std.
Indiv.Indiv.
Std.1See guidelines for post-operative radiotherapy

Oral Cavity 33Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Cavity carcinoma
•• WorkWork--up procedureup procedure
•• TNM stagingTNM staging
•• Primary treatmentPrimary treatment
•• FollowFollow--upup
•• Treatment of recurrent and/or Treatment of recurrent and/or metastaticmetastatic diseasedisease
•• Appendix: surgical techniquesAppendix: surgical techniques
•• ReferencesReferences

Oral Cavity 34Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Labial Labial surgerysurgery-- vermillionectomyvermillionectomy : : mucosalmucosal advancementadvancement flapflap-- full full thicknessthickness resectionresection : :
-- < 1/3 < 1/3 liplip : : primaryprimary closureclosure, V, V--Y or W Y or W plastyplasty-- < 2/3 < 2/3 liplip : : flapsflaps-- total total resectionresection : free : free flapsflaps (composites)(composites)
-- mandibulectomymandibulectomy ......
Appendix: surgical techniquesAppendix: surgical techniques

Oral Cavity 35Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
MandibulectomyMandibulectomy-- notnot if T if T clinicallyclinically >> 1 cm1 cm-- interruptinginterrupting ifif --T4T4
-- recurrencerecurrence-- previousprevious RTRT-- T T clinicallyclinically < 1 cm < 1 cm with evidencewith evidence of of bonybonyextensionextension-- atrophic mandibular heightatrophic mandibular height < 1 cm< 1 cm
-- non non interruptinginterrupting if T if T clinicallyclinically < 1 cm < 1 cm andand no no evidenceevidence of of bonybonyextension extension oror only evidenceonly evidence forfor alveolar bone defectalveolar bone defect of expansive type of expansive type ((andand not ofnot of erosiveerosive type) type)
Appendix: surgical techniquesAppendix: surgical techniques

Oral Cavity 36Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
MandibularMandibular reconstructionsreconstructions-- clean clean marginsmargins are are predictiblepredictible Type 3Type 3-- primaryprimary : :
--vascularizedvascularized bonebone : 1rst : 1rst choicechoice Type 3Type 3-- fibulafibula-- iliaciliac crestcrest-- scapulascapula
-- reconstruction plate + reconstruction plate + muscularmuscular pedicledpedicled flapflap, , pectoralispectoralis major or major or latissimuslatissimus dorsidorsi : 2nd : 2nd choicechoice
Appendix: surgical techniquesAppendix: surgical techniques

Oral Cavity 37Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
-- reconstruction plate reconstruction plate ::Type 3 Type 3 -- AO : AO :
-- skin/skin/mucosamucosa perforations 9%perforations 9%-- plate fracture 4,5%plate fracture 4,5%-- screw looseningscrew loosening 32%32%
-- THORPTHORP-- alwaysalways ifif mandibular heightmandibular height < 10 mm< 10 mm afterafter marginal marginal resectionresection
-- secondary secondary -- samesame techniquestechniques-- Vascularized bone afterVascularized bone after RTRT-- OsteogenousOsteogenous distractiondistraction
Appendix: surgical techniquesAppendix: surgical techniques

Oral Cavity 38Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Buccal Buccal tumortumor surgerysurgery-- local local transoraltransoral tumorectomytumorectomy : : mucosalmucosal advancementadvancement flapflap, , evtevt. . Stensen’s Stensen’s ductduct transpositiontransposition-- resectionresection of of buccinatorbuccinator muscle : Bichat muscle : Bichat flapflap, + skin , + skin graftgraft,….,….-- full full thicknessthickness resectionresection : :
-- free free fasciocutaneousfasciocutaneous flapsflaps (composites)(composites)-- myocutaneousmyocutaneous pedicledpedicled flapsflaps, , pectoralispectoralis major or major or latissimuslatissimusdorsidorsi
-- maxillectomymaxillectomy or or mandibulectomymandibulectomy ……
Appendix: surgical techniquesAppendix: surgical techniques

Oral Cavity 39Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Oral sulcussulcus tumortumor surgerysurgery-- local local transoraltransoral tumorectomytumorectomy : : primaryprimary closureclosure, , mucosalmucosal advancementadvancementflapflap-- alveolaralveolar resectionresection : : primaryprimary closureclosure, Bichat , Bichat flapflap, , secondarysecondary healinghealing, , skin skin graftgraft......-- maxillectomymaxillectomy or or mandibulectomymandibulectomy......
Appendix: surgical techniquesAppendix: surgical techniques

Oral Cavity 40Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
MaxillaryMaxillary reconstructionsreconstructions-- obturatorobturator prosthesisprosthesis-- temporalistemporalis muscle muscle flapsflaps-- Bichat Bichat flapflap-- buccinatorbuccinator flapflap-- free free flapsflaps
-- fasciocutaneousfasciocutaneous-- vascularizedvascularized bonebone
Appendix: surgical techniquesAppendix: surgical techniques

Oral Cavity 41Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
AnteriorAnterior tonguetongue andand floorfloor of the of the mouthmouth reconstructions reconstructions Type 3Type 3--1. free 1. free fasciocutaneousfasciocutaneous flapsflaps ((sensatesensate))
-- radialradial-- brachial brachial extext-- cubitalcubital
-- 2. 2. MyocutaneousMyocutaneous or or musculousmusculous pedicledpedicled flapsflaps : : pectoralispectoralis major or major or latissimuslatissimus dorsidorsi
-- 3. 3. nasolabialnasolabial flapflap, , perper secundarysecundary healinghealing, skin , skin graftgraft
Appendix: surgical techniquesAppendix: surgical techniques

Oral Cavity 42Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
Oral Cavity carcinoma
•• WorkWork--up procedureup procedure
•• TNM stagingTNM staging
•• Primary treatmentPrimary treatment
•• FollowFollow--upup
•• Treatment of recurrent and/or Treatment of recurrent and/or metastaticmetastatic diseasedisease
•• Appendix: surgical techniquesAppendix: surgical techniques
•• References References

Oral Cavity 43Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
References• Ash CS, Nason RW, Abdoh AA, Cohen MA. Prognostic Implications of Mandibular Invasion in
Oral Cancer. Head Neck 2000; 22 : 794-798.• Bailey BJ. Management of carcinoma of the lip. Laryngoscope. 87:250-60, 1977.• Baker SR. Cancer of the lip. In Cancer of the Head and Neck, 2nd ed., Churchill Livingston, New
York, 383-413, 1989.• Breitbart W. Identifying patients at risk for, and treatment of major psychaitric complications of
cancer Support Care Cancer 1995; 3 : 45-60.• Brown JS, Browne RM. Factors influencing the patterns of invasion of the mandible by oral
squamous cell carcinoma. Int J Oral Maxillofac Surg 1995; 24 : 417-426.• Brown JS. T2 tongue: reconstruction of surgical defect. Br J Oral Maxillofac Surg 1999; 37 : 194-
199.• Byers RM, Newman R, Russell N, and Yue A. Results of Treatment for Squamous Carcinoma of the
Lower Gum. Cance, 47: 2236-2238, 1981.• Cariou JL. Les transferts ou lambeaux libres de et avec péroné ou fibula. Anatomie chirurgicale,
techniques de prélèvement et de préparation, indications. Ann Chir Plast Esthét 2000; 46 : 219-271.• Chandu A, Smith AC, Douglas M. Percutaneous endoscopic gastrostomy in patients undergoing
resection for oral tumors: a retrospective review of complications and outcomes. J Oral Maxillofac Surg 2003; 61: 1279-1284.
• Chaturvedi SK, Shenoy A, Prasad KM, Senthilnathan SM, Premlatha BS. Concerns, coping and quality of life in head and neck cancer patients. Support Care Cancer 1996; 4 : 186-190.

Oral Cavity 44Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
• Chen J, Scully C, Eisenberg E, Krutchkoff DJ, Katz RV. Changing Trends in Oral Cancer in the UnitedStates, 1935 to 1985: A Connecticut Study. J Oral Maxillofac Surg 1991; 49 : 1152-1158.
• Clarke LK. Rehabilitation for the head and neck cancer patient. Oncology Huntingt 1998; 12 : 81-89.• Cordeiro PG, Disa JJ, Hidalgo DA, Hu Q. Reconstruction of the Mandible with Osseous Free Flaps: A
10-Year Experience with 150 Consecutive Patients. Plast Reconstr Surg 1999; 104 : 1314-1320.• Cowan CG, Gregg TA, Kee F. Prevention and detection of oral cancer: the views of primary care
dentists in Northern Ireland. Br Dent J 1995; 179 : 338-342.• Day GL, Blot WJ. Second Primary Tumors in Patients With Oral Cancer. Cancer 1992; 70 : 14-19.• de Leeuw JRJ, de Graeff A, Ros WJG, Blijham GH, Hordijk G-J, Winnubst JAM. Prediction of
Depressive Symptomatology after Treatment of Head nad Neck Cancer: the Influence of Pre-Treatment Physical and Depressive Symptoms, Coping, and Social Support. Head Neck 2000; 22 : 799-807.
• de vries N, Pastorino U, van Zandwijk N. Chemoprevention of Second Primary Tumours in Head andNeck Cancer in Europe : EUROSCAN. Oral Oncol, Eur J Cancer 1994; 30B : 367-368.
• Deleyiannois FW, Thomas BD, Vaughan TL, et al. Alcoholism: independent predictor of survival in patients with head and neck cancer. J Natl Cancer Inst 1996; 88 : 542-549.
• Dickenson AJ, Currie WJR, Avery BS. Screening for syphilis in patients with carcinoma of the tongue. Br J Oral Maxillofac Surg 1995; 33 : 319-320.
References

Oral Cavity 45Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
• Disa JJ, Hidalgo DA, Cordeiro PG, Winters RM, Thaler H. Evaluation of Bone Height in OsseousFree Flap Mandible Reconstruction: An Indirect Measure of Bone Mass. Plast Reconstr Surg 1999; 103 : 1371-1377.
• Effron MZ, Johnson JT, Myers EN, Curtin H, Beery Q, and Sigler B. Advanced Carcinoma of the Tongue: Management by Total Glossectomy Without Laryngectomy. Arch Otolaryngol 107: 694-697, 1981.
• Epstein JB, Oakley C, Millner A, Emerton S, van der Meij E, Le N. The utility of toluidine blueapplication as a diagnostic aid in patients previously treated for upper oropharyngeal carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997; 83 : 537-547.
• Epstein JB, Scully C, Spinelli JJ. Toluidine blue and Lugol's iodine application in the assessmentof oral malignant disease and lesions at risk of malignancy. J Oral Pathol Med 1992; 22 : 160-163.
• Fang F-M, Leung SW, Huang C-C, Liu Y-T, Wang C-J, Chen H-C, Sun L-M, Huang DT. Combined-Modality Therapy for Squamous Carcinoma of the Buccal Mucosa: Treatment Results and Prognostic Factors. Head Neck 1997; 19 : 506-512.
• Fein DA, Mendenhall WM, Parson JT, et al. Carcinoma of the Oral Tongue: A Comparison of Results and Complications of Treatment with Radiotherapy and/or Surgery. Head & Neck 16: 358-365, 1994.
• Fujita M, Hirokawa Y, Naito K, Tagashira N, Yaijn K, Wasa T. Recurrent lower gingival squamous cell carcinoma spreading along the pathway of the inferior alveolar nerve. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995; 80 : 369-375.
References

Oral Cavity 46Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
• Girod SC, Pfahl M. Retinoid actions and implications for prevention and therapy of oral cancer. Int J Oral Maxillofac Surg 1996; 25 : 69-73.
• Guillamondegui OM, Oliver BO, and Hayden R. Cancer of the Anterior Floor of the Mouth. Am JSurg 140: 560-562, 1980.
• Gupta PC, Mehta FS, Pindborg JJ, Bhonsle RB, Murti PR, Daftary DK, Aghi MB. Primary prevention trial of oral cancer in India: a 10-year follow-up study. J Oral Pathol Med 1992; 21 : 433-439.
• Haribhakti VV. The Dentate Adult Human Mandible: An Anatomic Basis for Surgical Decision Making. Plast Reconstr Surg 1996; 97 : 536-541.
• Haughey BH. Tongue Reconstruction: Concepts and Practice. Laryngoscope 103: 1132-1141, 1993.• Hermanek P, Henson DE, Hutter RVP, Sobin LH. (eds) : UICC - TNM Supplement 1993. A
Commentary on Uniform Use. Springer, Berlin, 1993.• Ho CM, Lam KH, Wei WI, Lau SK, and Lam LK. Occult Lymph Node Metastasis in Small Oral
Tongue Cancers. Head & Neck 14: 359-363, 1992.• Hosal IN, Önerci M, Kaya S and Turan E. Squamous cell carcinoma of the lower lip. Am J
Otolaryngol. 13(6):363-65, 1992.• Howaldt H-P, Kainz M, Euler B, Vorast H. Proposal for modification of the TNM staging
classification for cancer of the oral cavity. J Craniomaxillofac Surg 1999; 27 : 275-288.• Hussain M, Kish JA, Crane L et al. The role of infection in the morbidity and mortality of patients
with head and neck cancer undergoing multimodality treatment. Cancer 1991; 67 : 716-721.
References

Oral Cavity 47Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
• Jones AS, Morar P, Phillips DE, Field JK, Husband D, Helliwell TR. Second Primary Tumors in Patients with Head and Neck Squamous Cell Carcinoma. Cancer 1995; 75 : 1343-1353.
• Jones KR, Lodge-Rigal D, Reddick RL, et al. Prognostic factors in the recurrence of stgae I and IIsquamous cell cancer of the oral cavity. Arch Otolaryngol Head Neck Surg 1992; 118 : 483-485.
• Jorgenson K, Elbrond O, Andersen AP. Carcinoma of the lip: A series of 869 cases. Acta Radiol. 12:177, 1973.
• Kligerman J, Lima RA, Soares JR, et al. Supraomohyoid Neck Dissection in the Treatment of T1/T2Squamous Cell Carcinoma of Oral Cavity. Am J Surg 168: 391-394, 1994.
• Kligerman J, Lima RA, Soares JR, et al. Supraomohyoid Neck Dissection in the Treatment of T1/T2Squamous Cell Carcinoma of Oral Cavity. Am J Surg 168: 391-394, 1994.
• Korb LJ, Spaulding CA, and Constable WC. The Role of Definitive Radiation Therapy in Squamous Cell Carcinoma of the Oral Tongue. Cancer 67: 2733-2737, 1991.
• Kondoh T, Hamada Y, Kamei K, Seto K. Transport distraction osteogenesis following marginalresection of the mandible. Int J Oral Maxillofac Surg 2002; 31 : 675-676.
• Lewin F, Norell SE, Johansson H, Gustavsson P, Wennerberg J, Biörklund A, Rutqvist LE. Smoking Tobacco, Oral Snuff, and Alcohol in the Etiology of Squamous Cell Carcinoma of the Head andNeck. A Population-Based Case-Referent Study in Sweden. Cancer 1998; 82 : 1367-1375.
• Linn BS, Robinson DS, Klimas NG. Effects of age and nutritional status on surgical outcomes in head and neck cancer. Ann Surg 1989; 207 : 267-273.
References

Oral Cavity 48Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
References• Lore JM, Kaufman S, Grabau JC, and Popovic DN. Surgical management and epidemiology of lip
cancer. Otolaryngologic Clinics of North America. 12:81-95, 1979.• Lotan R, Xu X-C, Lippman SM, Ro JY, Lee JS, Lee JJ, Hong WK. Suppression of retinoic acid
receptor-ß in premalignant oral lesions and its up-regulation by isotretinoin. N Engl J Med 1995;332 : 1405-1410.
• Lydiatt DD, Robbins KT, Byers RM, and Wolf PF. Treatment of Stage I and II Oral Tongue Cancer. Head & Neck 15 : 308-312, 1993.
• Lydiatt DD. Mandibular resection. Head Neck 1995; 17 : 247-251.• Lydiatt WM, Anderson PE, Bazzana T, Casale M, Hughes CJ, Huvos AG, Lydiatt DD, Schantz SP.
Molecular Support for Field Cancerization in the Head and Neck. Cancer 1998; 82 : 1376-1380.• Martin D, Pistre V, PInsolle V, Pélissier P, Baudet J. La crête iliaque. le point sur un site donneur de
lambeaux libres exceptionnel, 20 ans après sa description initiale. Ann Chir Plast Esthét 2000; 46 : 201-218.
• Martin D, Pistre V, PInsolle V, Pélissier P, Baudet J. La scapula : un site donneur privilégié de lambeaux libres ou pédiculés. Ann Chir Plast Esthét 2000; 46 : 272-283.
• Mashberg A. Final evaluation of tolonium chloride rinse for screening of high-risk patients with asymptomatic squamous carcinoma. J Am Dent Assoc 1983; 106 : 319-324.
• Matthews TW, Lampe HB, Dragosz KD. Nutritional status in head and neck cancer patients. J Otolaryngol 1995; 24 : 87-91.

Oral Cavity 49Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
References• Mazeron JJ, Martin M, Brun B, et al. Induction chemotherapy in head and neck cancer: results of a
phase III trial. Head Neck 1992; 14 : 85-91.• McGuirt WF, Johnson JT, Myers EN, Rothfield R, and Wagner R. Floor of Mouth Carcinoma. Arch
Otolaryngol Head Neck Surg 121, 278-282, 1995.• McKaig RG, Baric RS, Olshan AF. Human Papillomavirus and Head and Neck
Cancer:Epidemiology and Molecular Biology. Head Neck 1998; 20 : 250-265.• Medina JE and Byers RM. Supraomohyoid Neck Dissection: Rationale, Indications, and Surgical
Technique. Head & Neck, 11: 111-122, 1989.• Mehregan DA, Roenigk RK. Management of superficial squamous cell carcinoma of the lip with
Mohs micrographic surgery. Cancer. 66:463-68, 1990.• Mermelstein HT, Lesko L. Depression in patie,nts with cancer. Psycho-Oncol 1992; 1 : 199-215.• Moadel AB, Ostroff JS, Schantz SP. Head and Neck Cancer. In : HollandJ (ed). Psycho-oncology.
Oxford University Press, New York, 1998, pp 617-323.• Morton RP, Davies AD, Baker J, Baker GA, Stell PM. Quality of life in treated head and neck
cancer patients:a preliminary report. Clin Otolaryngol 1984; 9 : 181-185.• Morton RP, Ferguson CM, Lambie NK, and Whitlock RML. Tumor Thickness in Early Tongue
Cancer. Arch Otolaryngol Head Neck Surg 120: 717-720, 1994.• Moyer GN, Taybos GM, Pelleu GB. Toluidine blue rinse: potential for benign lesions in early
detection of oral neoplasms. J Oral Med 1986; 41 : 111-113.• Munoz Guerra MF, Naval Gias L, Campo FR, Perez JS. Marginal and segmental mandibulectomy in
pptients with oral cancer : a statistical analysis of 106 cases. J Oral Maxillofac Surg 2003; 61: 1289-1296.

Oral Cavity 50Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
References• Muzaffar AR, Adams WP, Hartog JM, Rohrich RJ, Buyrd HS. Maxillary Reconstruction: Functional
and Aesthetic Considerations. Plast Reconstr Surg 1999; 104 : 2172-2183.• Nicotine replacement to aid smoking cessation. Drugs and Therapeutics Bulletin 1999; 37 : 52-54.• Ondrey FG. Arachidonic Acid Metabolism:A Primer for head and Neck Surgeons. Head Neck 1998;
20 : 334-349.• O’Brien CJ, Adams JR, McNeil EB, Taylor P, Laniewski P, Clifford A, Parker GD. Influence of
bone invasion and extent of mandibular resection on local control of cancers of the oral cavity andoropharynx. Int J Oral Maxillofac Surg 2003; 32 : 492-497.
• Prince S, Bailey BMW. Squamous carcinoma of the tongue: review. Br J Oral Maxillofac Surg1999; 37 : 164-174.
• Reilly JJ. Does nutrition management benefit the head and neck cancer patient ? Oncology 1990; 4 : 105-115.
• Reychler H, Mahy P, Thone M. Description nosologique des lésions de la muqueuse orale. RevBelge Med Dent 2000; 55 : 149-238.
• Robbins KT, Favrot S, Hanna D, Cole R. Risk of wound infection in patients with head and neck cancer. Head Neck 1990; 12 : 143-148.
• Rodgers LW, Stringer SP, Mendenhall WH, e al. Management of suqamous carcinoma of the floorof the mouth. Head Neck 1993; 15 : 16-19.
• Rosenberg D, Cretion S. Use of meta-analysis to evaluate tolonium chloride in oral cancerscreening. Oral Surg Oral Med Oral Pathol 1989; 67 : 621-627.

Oral Cavity 51Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
References• Schwartz GJ, Mehta RH, Wenig BL, Shaligram C, Portugal LG. Salvage Treatment for Recurrent
Squamous Cell Carcinoma of the Oral Cavity. Head Neck 2000; 22 : 34-41.• Scully C. Oral Precancer: Preventive and Medical Approaches to Management. Oral Oncol, Eur J
Cancer 1995; 31B : 16-26.• Shaha AR. Preoperative Evaluation of the Mandible in Patients with Carcinoma of the Floor of Mouth.
Head & Neck 13: 398-402, 1991.• Sherman AC, Simonton S, Adams DC, Vural E, Hanna E. Coping with Head and Neck Cancer During
Different Phases of Treatment. Head Neck 2000; 22 : 787-793.• Shpitzer T, Neligan PC, Gullane PJ, Boyd BJ, Gur E, Rotstein LE, Brown DH, Irish JC, Freeman JE.
The Free Iliac Crest and Fibula Flaps in Vascularized Oromandibular Reconstruction: Comparison andLong-term Evaluation. Head Neck 1999; 21 : 639-647.
• Silverman S Jr, Migliorati C, Barbosa J. Toluidine blue staining in the detection of oral precancerous and malignant lesions. Oral Surg Oral Med Oral Pathol 1984; 57 : 379-382.
• Sobin LH, Witekind CH. (eds) : UICC - TNM Classification of Malignant Tumours. Wiley, New York, 1997.
• Spiro RH, Huvos AG, Wong GY, Spiro JD, Gnecco CA, and Strong EW. Predictive Value of Tumor Thickness in Squamous Carcinoma Confined to the Tongue and Floor of the Mouth. Am J Surg 152: 345-350, 1986.
• Stepnick DW. Cancer of the lip. In Current Therapy in Otolaryngology - Headand Neck Surgery, 5thed., Mosby, St Louis, 257-61, 1994.
• Tei K, Totsuka Y, Iizuka T, Ohmori K. Marginal resection for carcinoma of the mandibular alveolus and gingiva where radiologically detected bone defects do not extend beyond the mandibular canal. J Oral Maxillofac Surg 2004; 62 : 834-839.

Oral Cavity 52Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
• Urken ML, Weinberg H, Vickery C, et al. Oromandibular Reconstruction Using MicrovascularComposite Free Flaps. Arch Otolaryngol Head Neck Surg 117: 733-744, 1991.
• Vacher C, Legens M, Rueff B, Lezy J-P. Dépistage des lésions cancéreuses et précancéreuses de la muqueuse buccale dans une population à risque. Rev Fr Stomatol Chir Maxillofac 1999; 100 : 180-183.
• van Bokhorst-van der Schueren MAE, van Leeuwen PAM, Sauerwein HP, Kuik DJ, Snow GB, QuakJJ. Assessment of Malnutrition Parameters in Head and neck Cancer and their relation toPostoperative Complications. Head Neck 1997; 19 : 419-425.
• von Meyenfeldt MF, Meijerink WJHJ, Rouflart MMJ, Buil-Maassen MTHJ, Soeters PB.perioperative nutritional support: a randomised clinical trial. Clin Nutr 1992; 11 : 180-186.
• Wallner PE, Hanks GE, Kramer S et al. Patterns of care study: analysis of outcome survey data-anterior two-thirds of tongue and floor of mouth. Am J Clin Oncol 1986; 9 : 50-57.
• Westin T, Ahlbom E, Johansson E, Sandström B, Karlberg I, Edström S. Circulating levels ofselenium and zinc in relation to nutritional status in patients with head and neck cancer. Arch Otolaryngol Head Neck Surg 1989; 115 : 1079-1082.
• Westin T, Jansson A, Zenckert C, Hallström T, Edström S. Mental depressions is associated withmalnutrition in patients with head and neck cancer. Arch Otolaryngol Head Neck Surg 1988; 114 : 1449-1453.
• Woederman LAE, Chaplin BJ, Griffioen FMM, Bos KE. Sensate Osteocutaneous Fibula Flap:Anatomic Study of the Innervation Pattern of the Skin Flap. Head Neck 1998; 20 : 310-314.
References

Oral Cavity 53Mar. 2006
Catholic University of Louvain, St - Luc University HospitalHead and Neck Oncology Programme
• Yuen APW, Lam KY, Wei WI, Lam KY, Ho CM, Chow TL, Yuen WF. A Comparison of the Prognostic Significance of Tumor Diameter, Length, Width, Thickness, Area, Volume and Clinicopathological Features of Oral Tongue Carninoma. Am J Surg 2000; 180 : 139-143.
• Zhao Z, Li S, Yan Y, Li Y, Yang M, Mu L, Huang W, Liu Y, Zhai H, Jin J, Ma X. New Buccinator Myomucosal Island Flap: Anatomic Study and Clinical Application. Plast Reconstr Surg 1999; 104 : 55-65.
References











![Oral Cavity - kankerregister.org · retromolar gingiva (Figure 1) [1]. Figure 1. Anatomy of the Oral Cavity In Belgium for incidence year 2008, 612 patients are diagnosed with a carcinoma](https://static.fdocuments.in/doc/165x107/5cb2972d88c99395718be5be/oral-cavity-retromolar-gingiva-figure-1-1-figure-1-anatomy-of-the-oral.jpg)




