
Optimizing Nursing Management of Hepatic Veno-Occlusive Disease
45
Optimizing Nursing Management of Hepatic Veno - Occlusive Disease Phyllis McKiernan, APN, MSN, OCN ® Advanced Practice Nurse John Theurer Cancer Center Michelle N. Rickard, DNP, CPNP-AC, CHPPN, BMTCN, CPON Assistant Professor, College of Nursing University of Tennessee Health Science Center
Transcript of Optimizing Nursing Management of Hepatic Veno-Occlusive Disease
Optimizing Nursing Management of
Hepatic Veno-Occlusive Disease
Phyllis McKiernan, APN, MSN, OCN®
Advanced Practice Nurse
John Theurer Cancer Center
Michelle N. Rickard, DNP, CPNP-AC, CHPPN, BMTCN, CPON
Assistant Professor, College of Nursing
University of Tennessee Health Science Center
Jointly provided by USF Health and i3 Health
ACCREDITATION
USF Health is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s
Commission on Accreditation.
A maximum of 1.0 contact hour may be earned by learners who successfully complete this continuing nursing education activity.
No prerequisites are required for this activity.
INSTRUCTIONS TO RECEIVE CREDIT
In order to receive credit for this activity, participants must:
1. Participate in the live webinar
2. Complete and submit the posttest and activity evaluation via the link provided after the webinar
3. Download or print their Certificate of Credit
UNAPPROVED USE DISCLOSURE
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the
FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the
planners. Please refer to the official prescribing information for each product for discussion of approved indications,
contraindications, and warnings.
DISCLAIMER
The information provided in this CE activity is for continuing education purposes only and is not meant to substitute for the
independent medical/clinical judgment of a healthcare provider relative to diagnostic and treatment options of a specific patient’s
medical condition.
COMMERCIAL SUPPORT
This activity is supported by an independent educational grant from Jazz Pharmaceuticals Inc.
Disclosures
▶ Phyllis McKiernan has no commercial relationships
to disclose
▶ Michelle N. Rickard has no commercial
relationships to disclose
Learning Objectives
▶ Describe the pathophysiology of VOD
▶ Assess the risk for VOD in cancer patients
undergoing HSCT
▶ Evaluate evidence-based supportive care plans to
mitigate VOD in pediatric and adult patients with
cancer
VOD = veno-occlusive disease; HSCT = hematopoietic stem cell transplant.
VOD: Scope of the Problem
▶ Also known as sinusoidal obstruction syndrome
▶ Affects up to 60% of patients following HSCT
▶ Mortality rates: ◼ Severe VOD >80%◼ Moderate VOD >20%
▶ Associated with multiorgan failure
Dalle et al, 2016; Richardson et al, 2013.
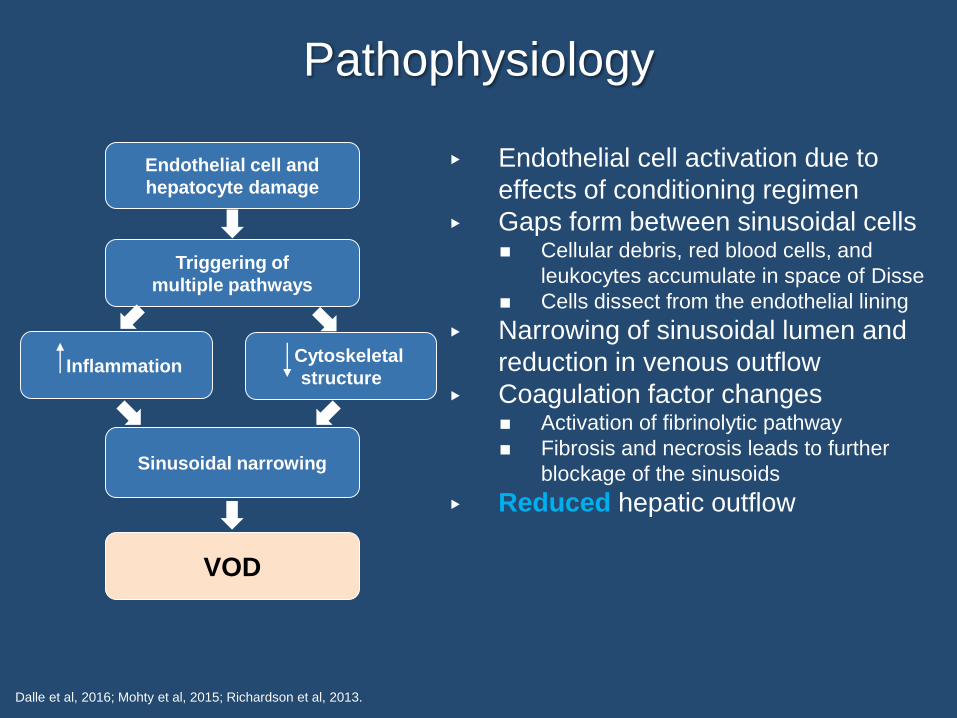
Pathophysiology
▶ Endothelial cell activation due to
effects of conditioning regimen
▶ Gaps form between sinusoidal cells◼ Cellular debris, red blood cells, and
leukocytes accumulate in space of Disse
◼ Cells dissect from the endothelial lining
▶ Narrowing of sinusoidal lumen and
reduction in venous outflow
▶ Coagulation factor changes◼ Activation of fibrinolytic pathway
◼ Fibrosis and necrosis leads to further
blockage of the sinusoids
▶ Reduced hepatic outflow
Dalle et al, 2016; Mohty et al, 2015; Richardson et al, 2013.
Endothelial cell and
hepatocyte damage
Triggering of
multiple pathways
InflammationCytoskeletal
structure
Sinusoidal narrowing
VOD
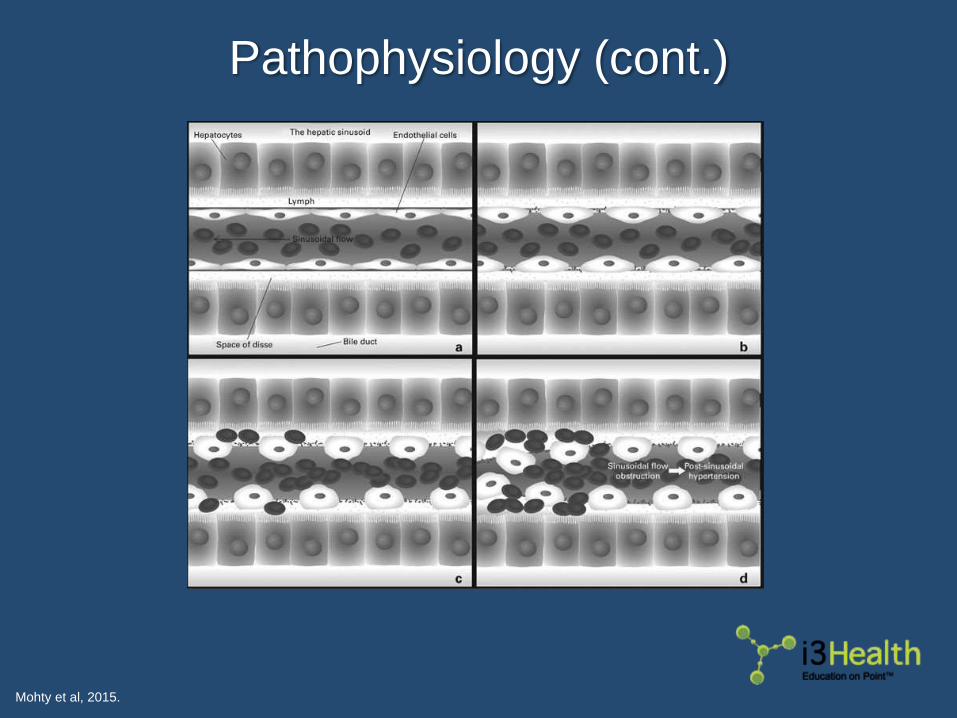
Pathophysiology (cont.)
Mohty et al, 2015.
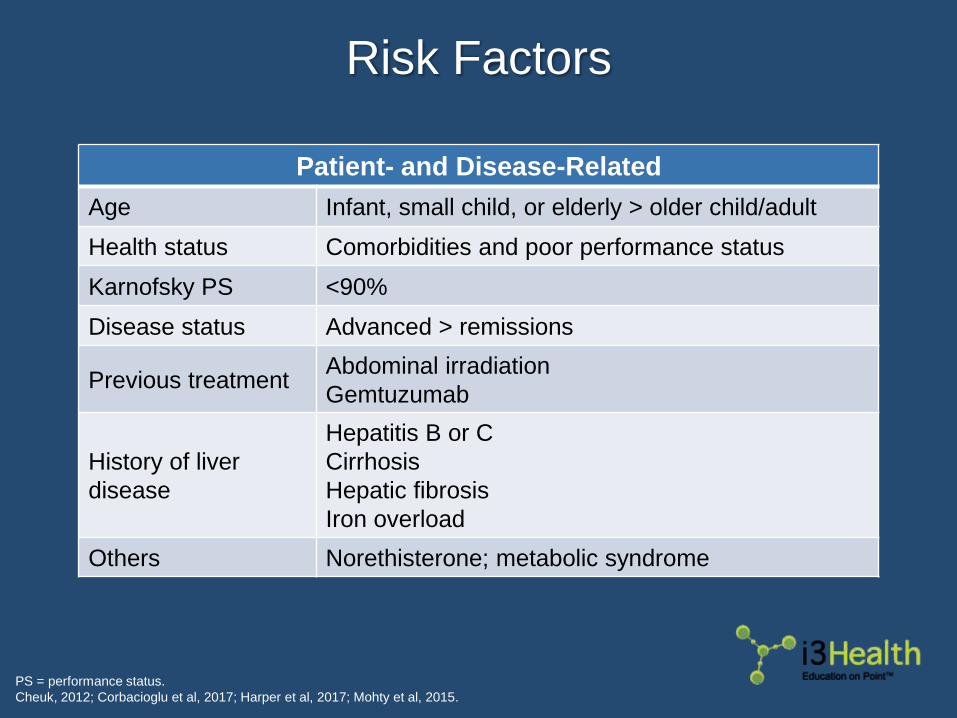
Risk Factors
PS = performance status.
Cheuk, 2012; Corbacioglu et al, 2017; Harper et al, 2017; Mohty et al, 2015.
Patient- and Disease-Related
Age Infant, small child, or elderly > older child/adult
Health status Comorbidities and poor performance status
Karnofsky PS <90%
Disease status Advanced > remissions
Previous treatmentAbdominal irradiation
Gemtuzumab
History of liver
disease
Hepatitis B or C
Cirrhosis
Hepatic fibrosis
Iron overload
Others Norethisterone; metabolic syndrome
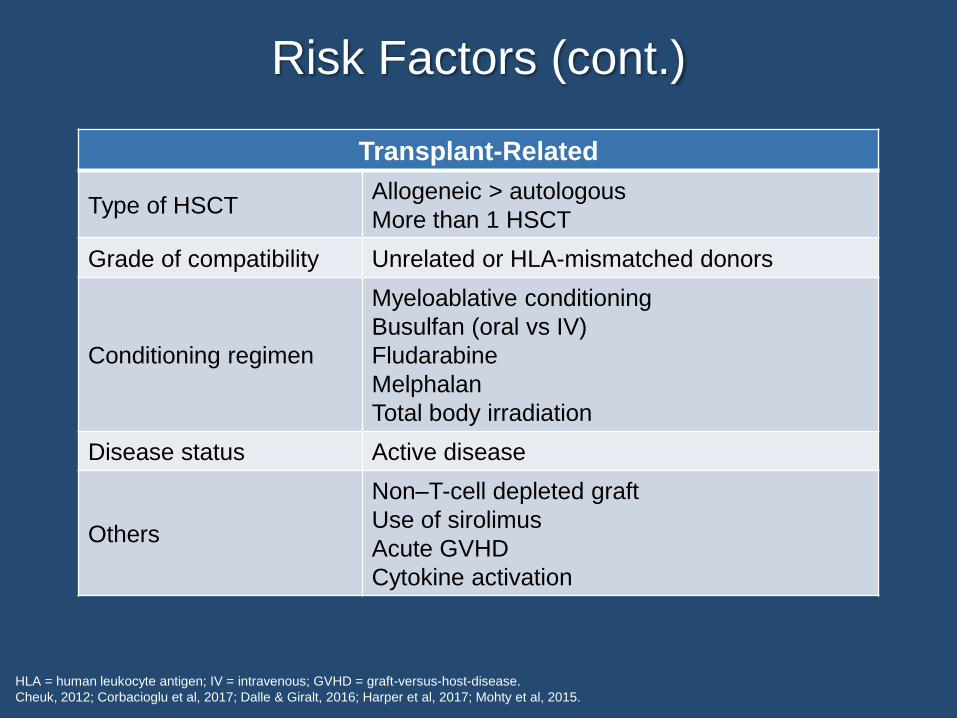
Risk Factors (cont.)
HLA = human leukocyte antigen; IV = intravenous; GVHD = graft-versus-host-disease.
Cheuk, 2012; Corbacioglu et al, 2017; Dalle & Giralt, 2016; Harper et al, 2017; Mohty et al, 2015.
Transplant-Related
Type of HSCTAllogeneic > autologous
More than 1 HSCT
Grade of compatibility Unrelated or HLA-mismatched donors
Conditioning regimen
Myeloablative conditioning
Busulfan (oral vs IV)
Fludarabine
Melphalan
Total body irradiation
Disease status Active disease
Others
Non–T-cell depleted graft
Use of sirolimus
Acute GVHD
Cytokine activation
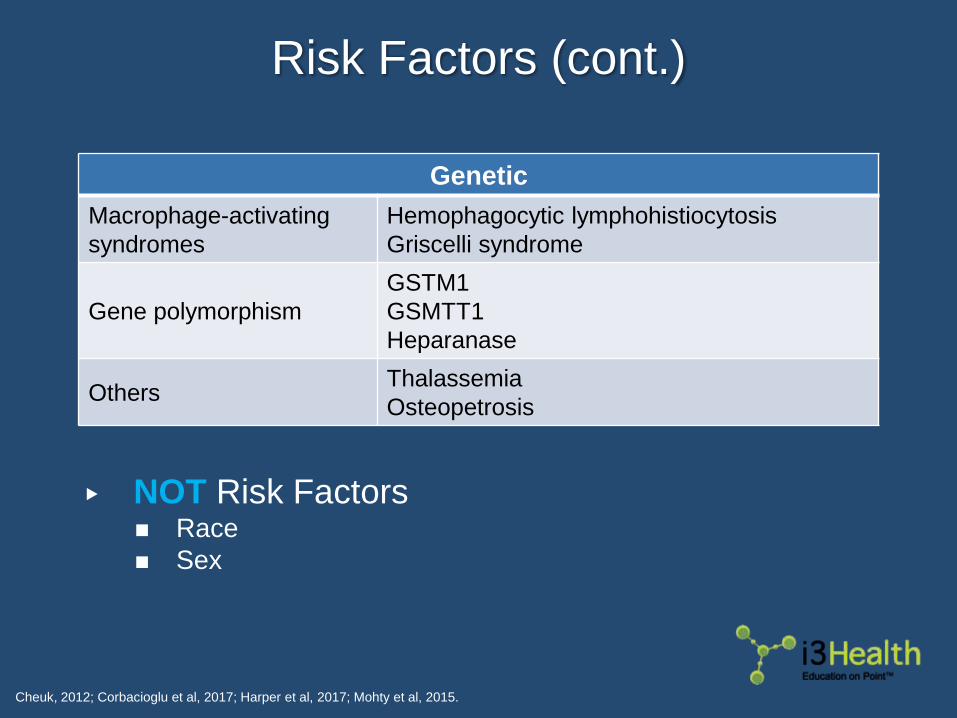
Risk Factors (cont.)
Cheuk, 2012; Corbacioglu et al, 2017; Harper et al, 2017; Mohty et al, 2015.
Genetic
Macrophage-activating
syndromes
Hemophagocytic lymphohistiocytosis
Griscelli syndrome
Gene polymorphism
GSTM1
GSMTT1
Heparanase
OthersThalassemia
Osteopetrosis
▶ NOT Risk Factors◼ Race
◼ Sex
Pop Quiz Question 1
When do VOD symptoms typically occur following
HSCT?
a. Within 10 days
b. Within 30 days
c. Within 50 days
d. Within 70 days
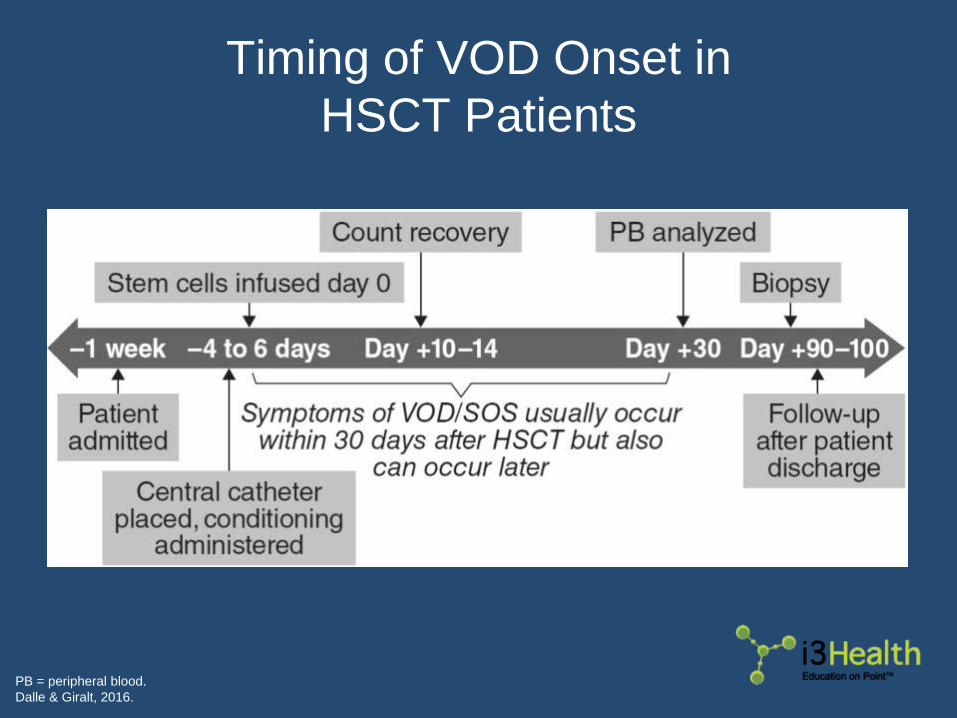
Timing of VOD Onset in
HSCT Patients
PB = peripheral blood.
Dalle & Giralt, 2016.
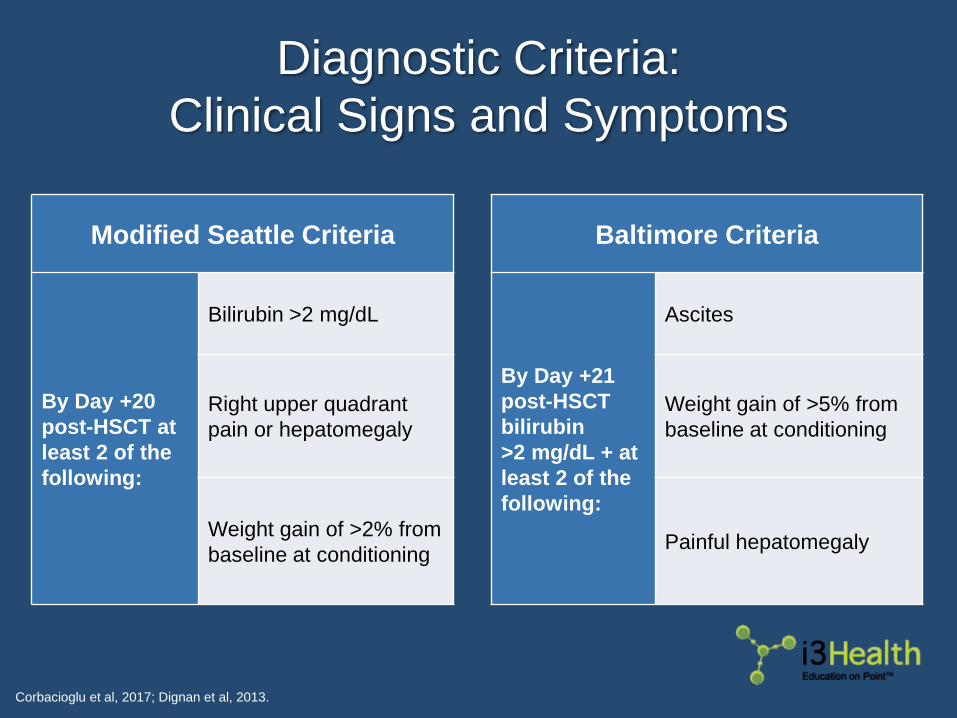
Diagnostic Criteria:
Clinical Signs and Symptoms
Corbacioglu et al, 2017; Dignan et al, 2013.
Modified Seattle Criteria
By Day +20
post-HSCT at
least 2 of the
following:
Bilirubin >2 mg/dL
Right upper quadrant
pain or hepatomegaly
Weight gain of >2% from
baseline at conditioning
Baltimore Criteria
By Day +21
post-HSCT
bilirubin
>2 mg/dL + at
least 2 of the
following:
Ascites
Weight gain of >5% from
baseline at conditioning
Painful hepatomegaly
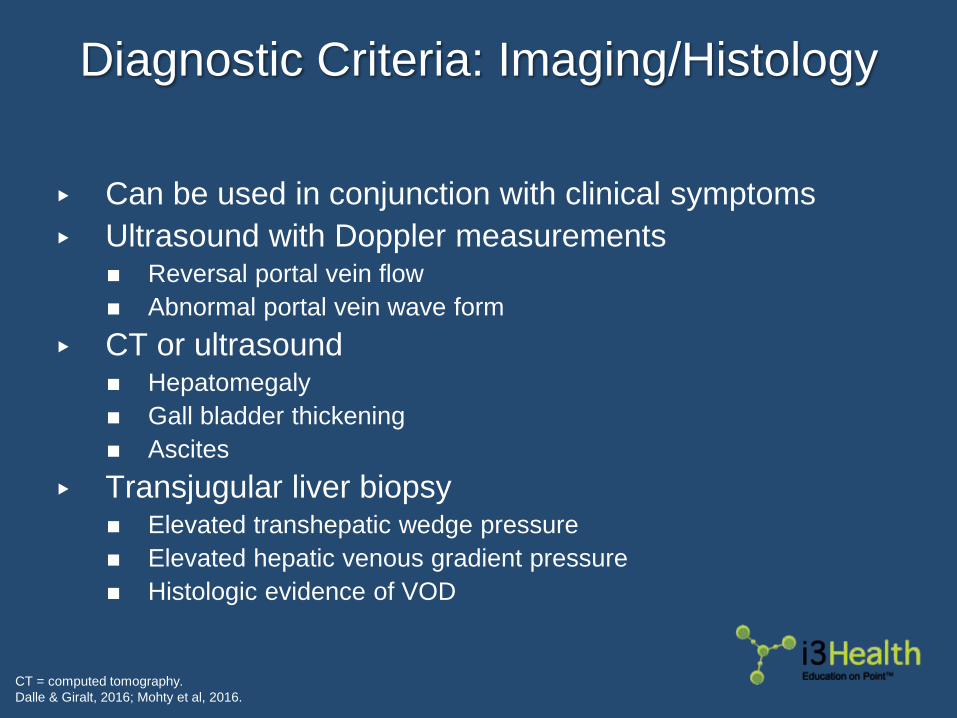
Diagnostic Criteria: Imaging/Histology
▶ Can be used in conjunction with clinical symptoms
▶ Ultrasound with Doppler measurements◼ Reversal portal vein flow
◼ Abnormal portal vein wave form
▶ CT or ultrasound◼ Hepatomegaly
◼ Gall bladder thickening
◼ Ascites
▶ Transjugular liver biopsy◼ Elevated transhepatic wedge pressure
◼ Elevated hepatic venous gradient pressure
◼ Histologic evidence of VOD
CT = computed tomography.
Dalle & Giralt, 2016; Mohty et al, 2016.
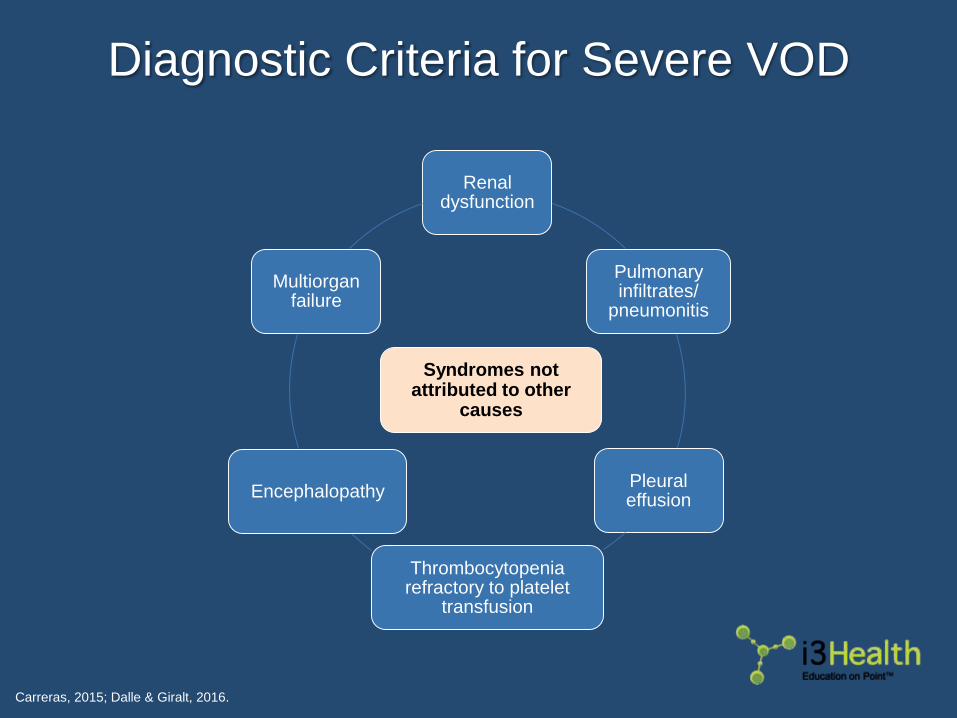
Diagnostic Criteria for Severe VOD
Carreras, 2015; Dalle & Giralt, 2016.
Renal dysfunction
Pulmonary infiltrates/
pneumonitis
Pleural effusion
Thrombocytopenia refractory to platelet
transfusion
Encephalopathy
Multiorgan failure
Syndromes not attributed to other
causes
Pop Quiz Question 2
Which of the following would you NOT recommend for
a patient experiencing multiorgan failure following
HSCT for VOD prophylaxis?
a. Unfractionated heparin
b. Low-molecular-weight heparin
c. tPA
d. Ursodeoxycholic acid
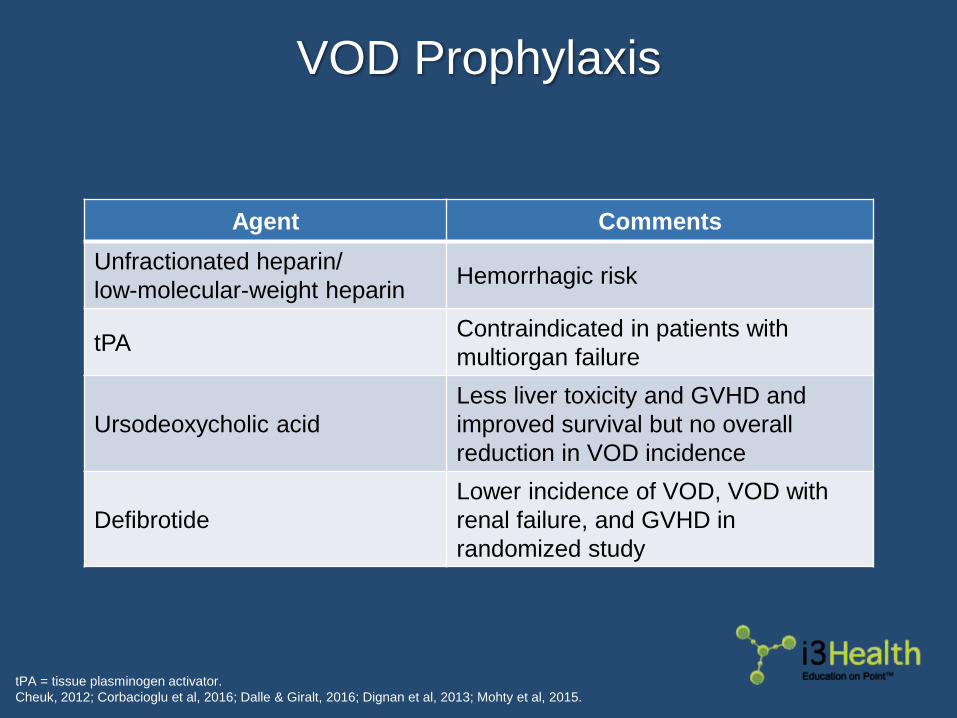
VOD Prophylaxis
tPA = tissue plasminogen activator.
Cheuk, 2012; Corbacioglu et al, 2016; Dalle & Giralt, 2016; Dignan et al, 2013; Mohty et al, 2015.
Agent Comments
Unfractionated heparin/
low-molecular-weight heparinHemorrhagic risk
tPAContraindicated in patients with
multiorgan failure
Ursodeoxycholic acid
Less liver toxicity and GVHD and
improved survival but no overall
reduction in VOD incidence
Defibrotide
Lower incidence of VOD, VOD with
renal failure, and GVHD in
randomized study
VOD Prophylaxis (cont.)
▶ Close monitoring of busulfan levels
▶ Avoid hepatotoxic concomitant drugs
▶ Reduced-intensity conditioning when appropriate
▶ Hyperfractionated TBI recommended
▶ Use of donors with the highest degree of
compatibility or use of T-cell depleted grafts
▶ Close monitoring of weight (≥once daily)◼ Maintenance of baseline weight should be goal
TBI = total body irradiation.
Cheuk, 2012; Corbacioglu et al, 2016; Dalle & Giralt, 2016; Dignan et al, 2013; Mohty et al, 2015.
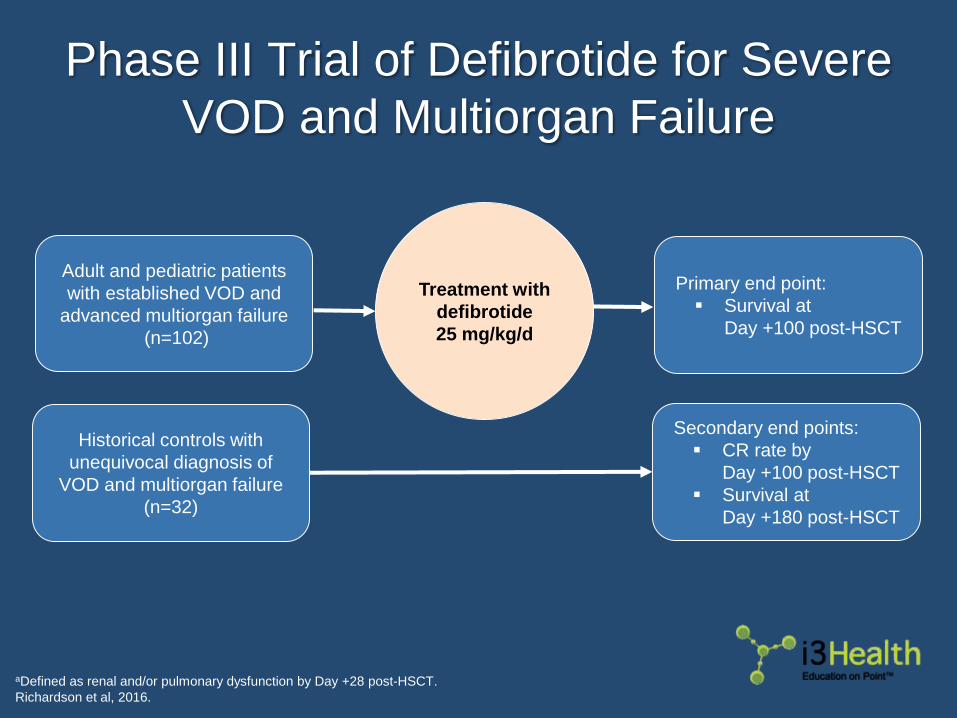
Phase III Trial of Defibrotide for Severe
VOD and Multiorgan Failure
aDefined as renal and/or pulmonary dysfunction by Day +28 post-HSCT.
Richardson et al, 2016.
Adult and pediatric patients
with established VOD and
advanced multiorgan failure
(n=102)
Historical controls with
unequivocal diagnosis of
VOD and multiorgan failure
(n=32)
Primary end point:
Survival at
Day +100 post-HSCT
Secondary end points:
CR rate by
Day +100 post-HSCT
Survival at
Day +180 post-HSCT
Treatment with
defibrotide
25 mg/kg/d
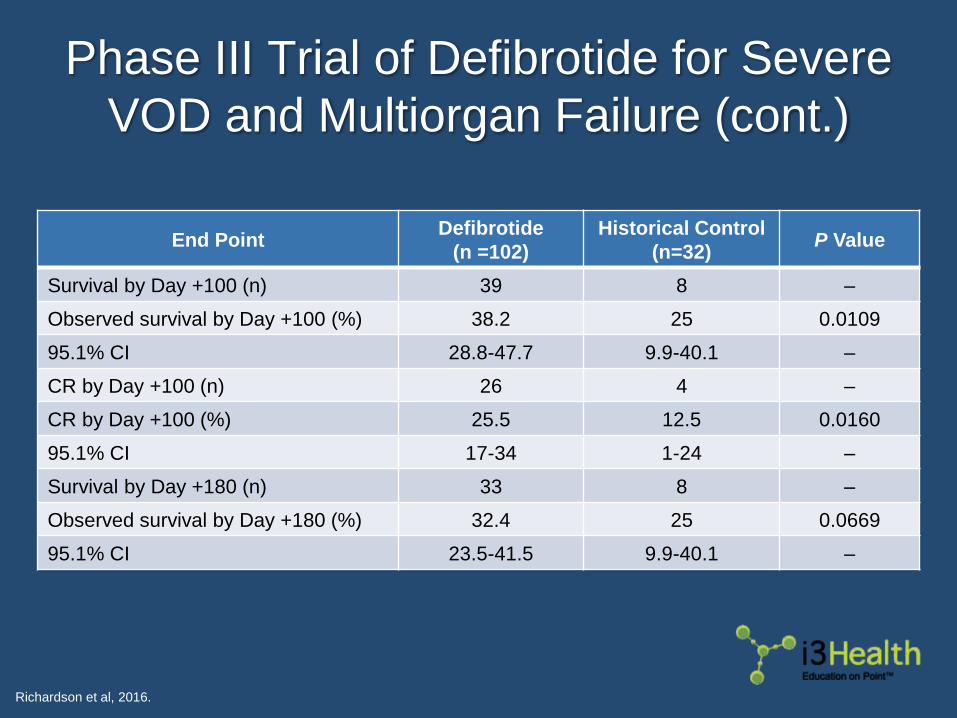
Phase III Trial of Defibrotide for Severe
VOD and Multiorgan Failure (cont.)
Richardson et al, 2016.
End PointDefibrotide
(n =102)
Historical Control
(n=32)P Value
Survival by Day +100 (n) 39 8 –
Observed survival by Day +100 (%) 38.2 25 0.0109
95.1% CI 28.8-47.7 9.9-40.1 –
CR by Day +100 (n) 26 4 –
CR by Day +100 (%) 25.5 12.5 0.0160
95.1% CI 17-34 1-24 –
Survival by Day +180 (n) 33 8 –
Observed survival by Day +180 (%) 32.4 25 0.0669
95.1% CI 23.5-41.5 9.9-40.1 –
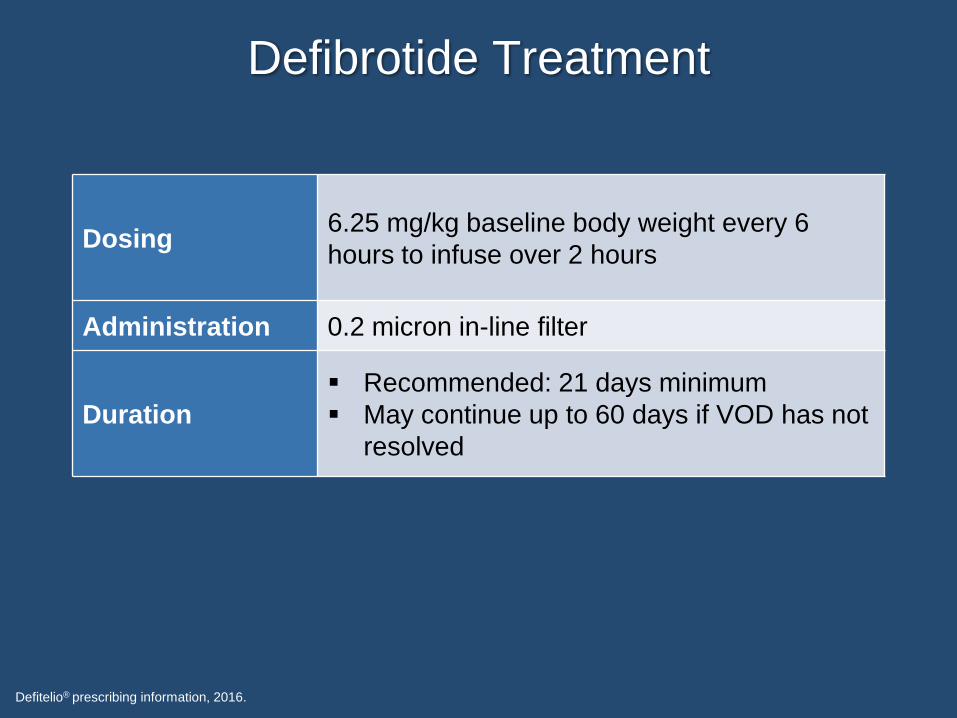
Defibrotide Treatment
Defitelio® prescribing information, 2016.
Dosing6.25 mg/kg baseline body weight every 6
hours to infuse over 2 hours
Administration 0.2 micron in-line filter
Duration
Recommended: 21 days minimum
May continue up to 60 days if VOD has not
resolved
Defibrotide Contraindications,
Warnings, and Precautions
▶ Concomitant use of defibrotide with
antithrombotic or fibrinolytic drugs is
contraindicated due to increased risk of
hemorrhage
▶ Delay the administration of defibrotide
until effects of previously administered
anticoagulant have abated
Defitelio® prescribing information, 2016.
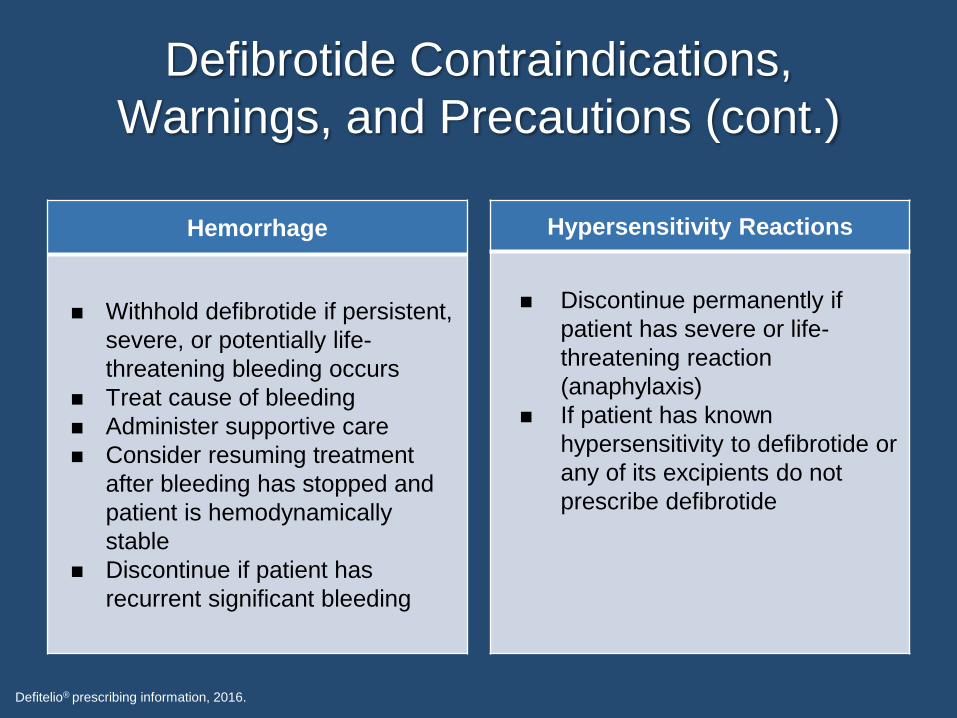
Defibrotide Contraindications,
Warnings, and Precautions (cont.)
Defitelio® prescribing information, 2016.
Hypersensitivity Reactions
◼ Discontinue permanently if
patient has severe or life-
threatening reaction
(anaphylaxis)
◼ If patient has known
hypersensitivity to defibrotide or
any of its excipients do not
prescribe defibrotide
Hemorrhage
◼ Withhold defibrotide if persistent,
severe, or potentially life-
threatening bleeding occurs
◼ Treat cause of bleeding
◼ Administer supportive care
◼ Consider resuming treatment
after bleeding has stopped and
patient is hemodynamically
stable
◼ Discontinue if patient has
recurrent significant bleeding
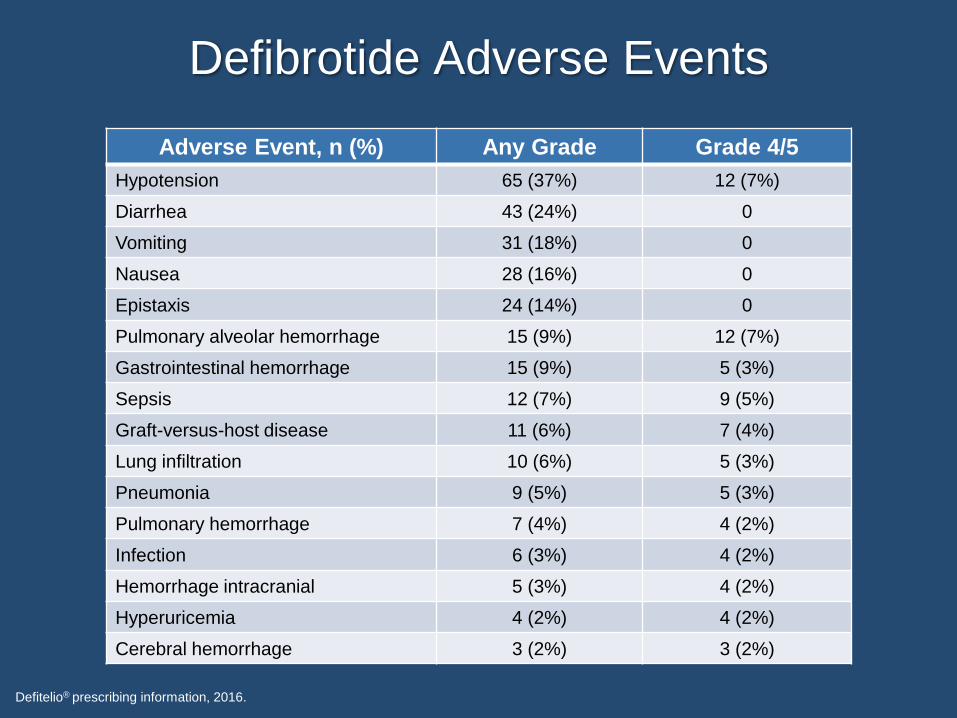
Defibrotide Adverse Events
Defitelio® prescribing information, 2016.
Adverse Event, n (%) Any Grade Grade 4/5
Hypotension 65 (37%) 12 (7%)
Diarrhea 43 (24%) 0
Vomiting 31 (18%) 0
Nausea 28 (16%) 0
Epistaxis 24 (14%) 0
Pulmonary alveolar hemorrhage 15 (9%) 12 (7%)
Gastrointestinal hemorrhage 15 (9%) 5 (3%)
Sepsis 12 (7%) 9 (5%)
Graft-versus-host disease 11 (6%) 7 (4%)
Lung infiltration 10 (6%) 5 (3%)
Pneumonia 9 (5%) 5 (3%)
Pulmonary hemorrhage 7 (4%) 4 (2%)
Infection 6 (3%) 4 (2%)
Hemorrhage intracranial 5 (3%) 4 (2%)
Hyperuricemia 4 (2%) 4 (2%)
Cerebral hemorrhage 3 (2%) 3 (2%)
Defibrotide Nursing Considerations
▶ Flush line immediately before and after
administration with 5% dextrose injection
or 0.9% sodium chloride
▶ Do not infuse with other IV drugs
concurrently within same IV line
Defitelio® prescribing information, 2016.
Case Study 1: Adult Patient
▶ 73-year-old male
▶ Primary myelofibrosis◼ Diagnosed fall 2016
◼ JAK2V617F mutation-positive
◼ Splenomegaly
◼ Anemia
▶ Medical history◼ Coronary artery disease
◼ Arthritis
◼ Hypertension
◼ Hyperlipidemia
▶ Received ruxolitinib and demonstrated clinical
improvement
Case Study 1: Adult Patient (cont.)
▶ Unrelated donor identified◼ 10/10 HLA match
◼ Female
◼ ABO: Donor O+, recipient B+
◼ Bone marrow
▶ Renal insufficiency◼ Elevated potassium and uric acid 1 week prior to transplant
◼ Responded to IV fluids and rasburicase
Case Study 1: Adult Patient (cont.)
◼ Fludarabine 30 mg/m2
Day -6 thru -2
◼ Busulfan 130 mg/m2 Day
-3 and -2
◼ rATG 4 mg/kg Day -3 thru
-1
◼ Received 1.67 x 10e6/kg
CD34-positive cells
◼ Serum creatinine
1.0 mg/dL
◼ Bilirubin 0.8 mg/dL
◼ Weight 74 kg
◼ Tacrolimus
◼ Mycophenolate mofetil
◼ Sirolimus
Nonmyeloablative
Conditioning
GVHD
ProphylaxisDay 0
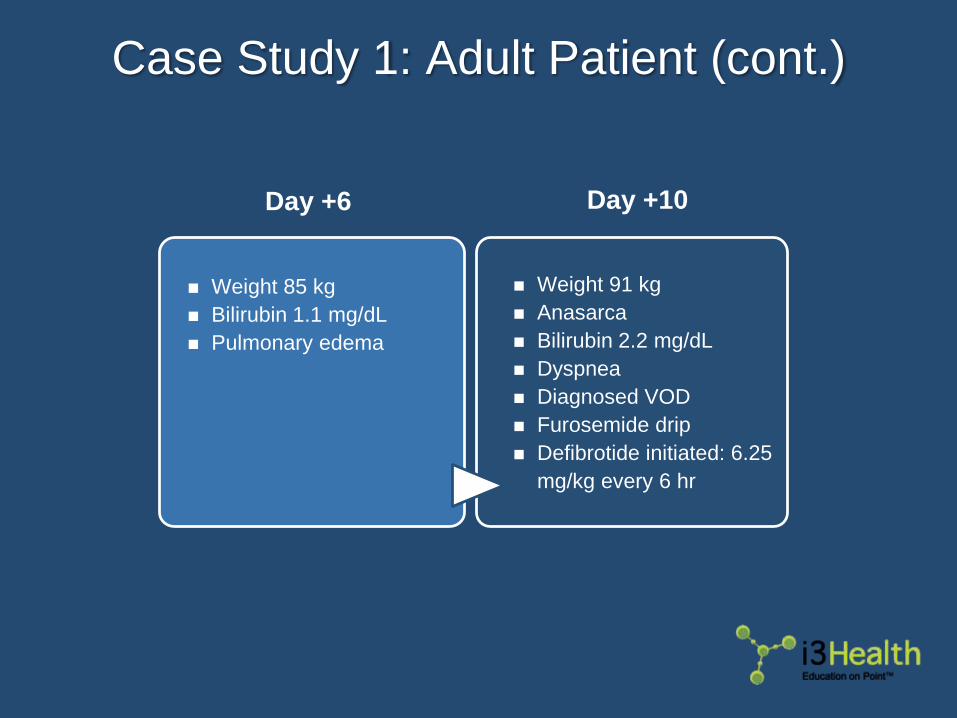
Case Study 1: Adult Patient (cont.)
◼ Weight 85 kg
◼ Bilirubin 1.1 mg/dL
◼ Pulmonary edema
◼ Weight 91 kg
◼ Anasarca
◼ Bilirubin 2.2 mg/dL
◼ Dyspnea
◼ Diagnosed VOD
◼ Furosemide drip
◼ Defibrotide initiated: 6.25
mg/kg every 6 hr
Day +6 Day +10
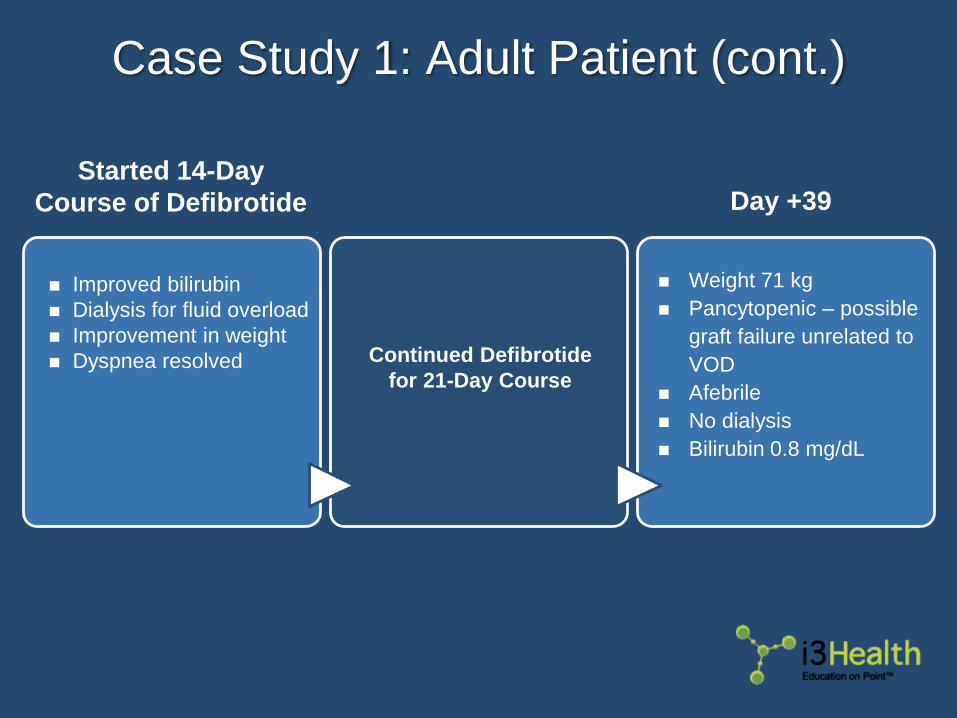
Case Study 1: Adult Patient (cont.)
◼ Improved bilirubin
◼ Dialysis for fluid overload
◼ Improvement in weight
◼ Dyspnea resolved Continued Defibrotide
for 21-Day Course
◼ Weight 71 kg
◼ Pancytopenic – possible
graft failure unrelated to
VOD
◼ Afebrile
◼ No dialysis
◼ Bilirubin 0.8 mg/dL
Started 14-Day
Course of Defibrotide Day +39
Case Study 2: Pediatric Patient
▶ 12-year-old female
▶ Acute lymphocytic leukemia◼ Initially diagnosed at 8 years of age
◼ Relapsed at 11 years of age
▶ Medical history◼ Avascular necrosis of bilateral hip
– Anticipating hip replacements after recovery from HSCT
◼ Abnormal liver enzymes– History of moderate elevation in liver enzymes. Resolve prior to
transplant
Case Study 2: Pediatric Patient (cont.)
▶ Haploidentical donor (mother)◼ 8/10 HLA Match
◼ T-cell depleted
◼ ABO: Donor B+, recipient B+
◼ Peripheral stem cells
◼ Donor received G-CSF for mobilization
G-CSF = granulocyte-colony stimulating factor.
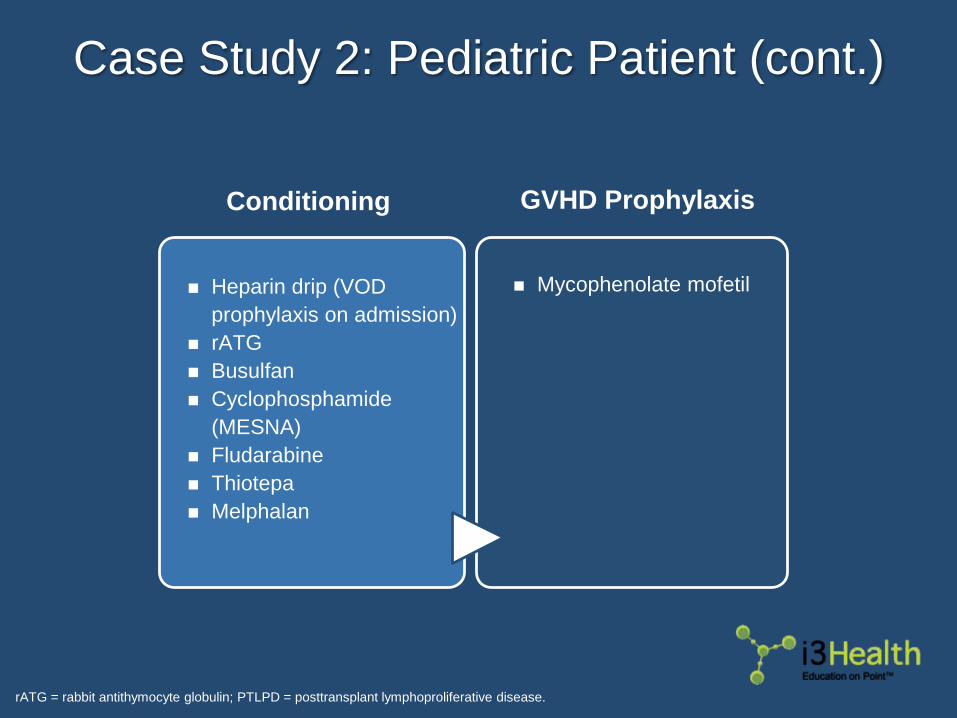
Case Study 2: Pediatric Patient (cont.)
rATG = rabbit antithymocyte globulin; PTLPD = posttransplant lymphoproliferative disease.
◼ Heparin drip (VOD
prophylaxis on admission)
◼ rATG
◼ Busulfan
◼ Cyclophosphamide
(MESNA)
◼ Fludarabine
◼ Thiotepa
◼ Melphalan
◼ Mycophenolate mofetil
Conditioning GVHD Prophylaxis
Pop Quiz Question 3
Which of the following is associated with a lower risk
for VOD in this patient?
a. Busulfan IV
b. T-cell depletion
c. Normal liver enzymes
d. All of the above
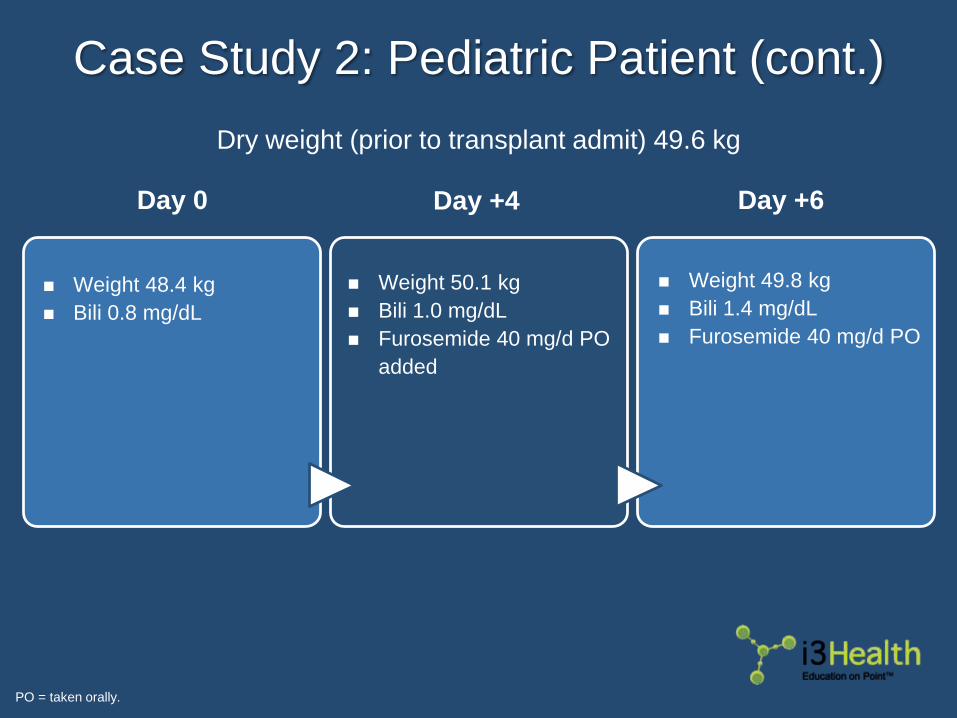
Case Study 2: Pediatric Patient (cont.)
PO = taken orally.
◼ Weight 48.4 kg
◼ Bili 0.8 mg/dL
◼ Weight 50.1 kg
◼ Bili 1.0 mg/dL
◼ Furosemide 40 mg/d PO
added
◼ Weight 49.8 kg
◼ Bili 1.4 mg/dL
◼ Furosemide 40 mg/d PO
Day 0 Day +6Day +4
Dry weight (prior to transplant admit) 49.6 kg
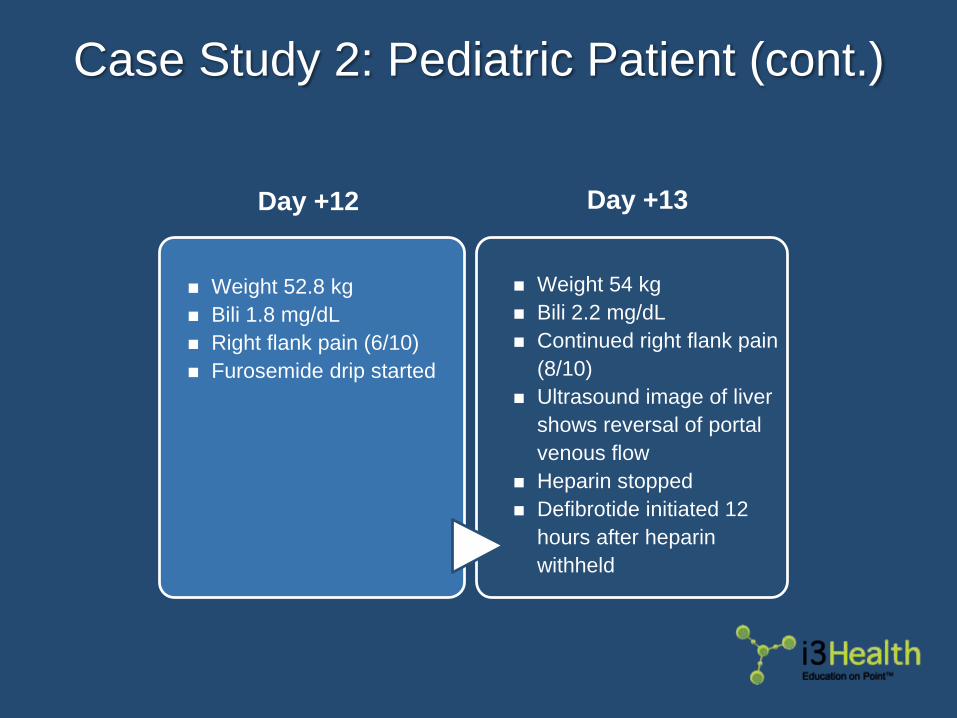
Case Study 2: Pediatric Patient (cont.)
◼ Weight 52.8 kg
◼ Bili 1.8 mg/dL
◼ Right flank pain (6/10)
◼ Furosemide drip started
◼ Weight 54 kg
◼ Bili 2.2 mg/dL
◼ Continued right flank pain
(8/10)
◼ Ultrasound image of liver
shows reversal of portal
venous flow
◼ Heparin stopped
◼ Defibrotide initiated 12
hours after heparin
withheld
Day +12 Day +13
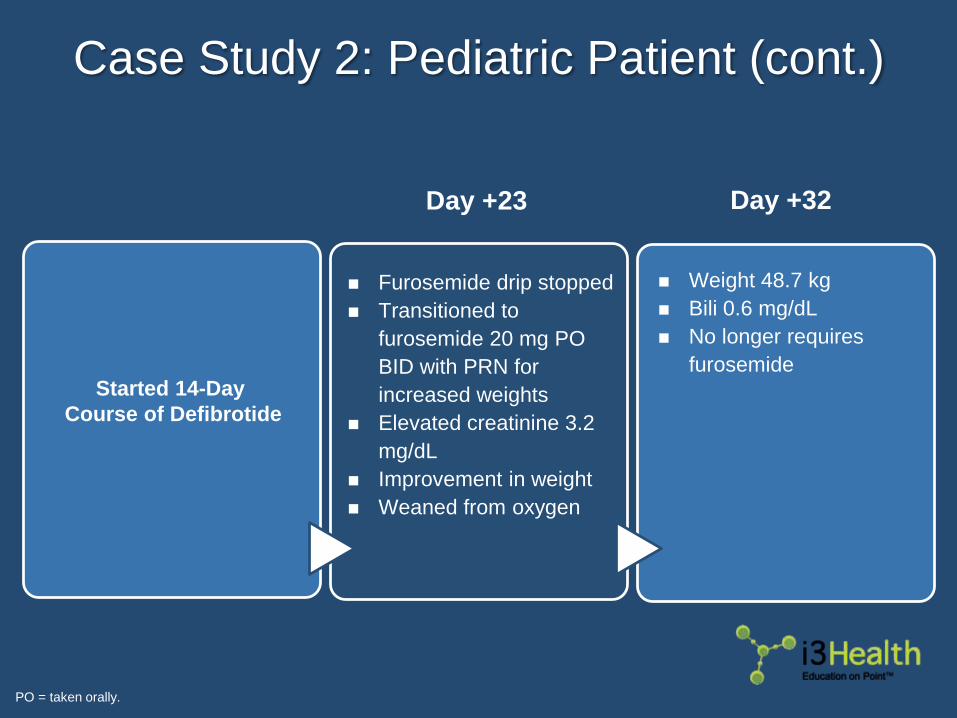
Case Study 2: Pediatric Patient (cont.)
PO = taken orally.
◼ Furosemide drip stopped
◼ Transitioned to
furosemide 20 mg PO
BID with PRN for
increased weights
◼ Elevated creatinine 3.2
mg/dL
◼ Improvement in weight
◼ Weaned from oxygen
◼ Weight 48.7 kg
◼ Bili 0.6 mg/dL
◼ No longer requires
furosemideStarted 14-Day
Course of Defibrotide
Day +32Day +23
Future Considerations
▶ Prevention◼ Increase use of reduced-intensity conditioning regimens
◼ Decrease toxicity of myeloablative conditioning regimens– Order of medications
– Hyperfractionated TBI
◼ HLA compatible donors
◼ Ursodeoxycholic acid
◼ Chelation for iron overload prior to HSCT
◼ Prophylaxis with defibrotide for high-risk patients
Carreras, 2015; Mohty et al, 2016.
Future Considerations (cont.)
▶ Early diagnosis and intervention◼ Update criteria for diagnosis
◼ Separate criteria for adult vs pediatric patients
◼ Classic vs late-onset VOD
▶ Identification of patients at risk for severe VOD◼ Kinetics of symptoms – when symptoms first appear to
diagnosis
◼ High number of risk factors
◼ Multiorgan involvement/failure
◼ Doubling of bilirubin from baseline within 48 hours
▶ Improved imaging
Carreras, 2015; Mohty et al, 2016.
Future Considerations (cont.)
▶ Combination therapy with defibrotide◼ Low-molecular-weight heparin
◼ N-acetylcysteine
◼ Antithrombin III
◼ Novel antithrombotics
▶ Genetic polymorphisms to individualize conditioning
regimens
▶ Identification of biomarkers◼ Endothelial injury
Carreras, 2015; Mohty et al, 2016.
Key Takeaways
▶ VOD affects many patients undergoing HSCT
▶ Can progress to multiorgan failure and death in
patients posttransplant
▶ Early diagnosis and prompt treatment is key to
preventing multiorgan failure and improving patient
outcomes
▶ Transplant centers should develop diagnostic
criteria and clinical pathways for VOD treatment
based on current evidence to guide management
Audience Q&AsUse the Questions section of your Control Panel
to submit questions to the faculty.

To receive CE credit visit:
www.i3health.com/VOD
References
Carreras E (2015). How I manage sinusoidal obstruction syndrome after haematopoietic cell transplantation. Br J Haematol, 168(4):481-491.
DOI:10.1111/bjh.13215
Chalandon Y, Roosnek E, Mermillod B, et al (2004). Prevention of veno-occlusive disease with defibrotide after allogeneic stem cell
transplantation. Biol Blood Marrow Transplant, 10(5):347-354.
Cheuk DL (2012). Hepatic veno-occlusive disease after hematopoietic stem cell transplantation: prophylaxis and treatment controversies. World
J Transplant, 2(2):27-34. DOI:10.5500/wjt.v2.i2.27
Corbacioglu S, Carreras E, Ansari M, et al (2017). Diagnosis and severity criteria for sinusoidal obstruction syndrome/veno-occlusive disease in
pediatric patients: a new classification from the European Society for Blood and Marrow Transplantation. Bone Marrow Transplantation.
[Epub ahead of print] DOI:10.1038/bmt.2017.161
Corbacioglu S, Carreras E, Mohty M, et al (2016). Defibrotide for the treatment of hepatic veno-occlusive disease: final results from the
International Compassionate-Use Program. Biol Blood Marrow Transplant, 22(10):1874-1882. DOI:10.1016/j.bbmt.2016.07.001
Coppell JA, Richardson PG, Soiffer R, et al (2010). Hepatic veno-occlusive disease following stem cell transplantation: incidence, clinical
course, and outcome. Biol Blood Marrow Transplant, 16(2):157-168. DOI:10.1016/j.bbmt2009.08.024
Dalle JH & Giralt SA (2016). Hepatic veno-occlusive disease after hematopoietic stem cell transplantation: Risk factors and stratification,
prophylaxis, and treatment. Biol Blood Marrow Transplant, 22(3):400-409. DOI:10.1016/j.bbmt.2015.09.024
Defitelio® (defibrotide) prescribing information, 2016. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/208114lbl.pdf
Dignan F, Gujral D, Ethell M, et al (2007). Prophylactic defibrotide in allogeneic stem cell transplantation: minimal morbidity and zero mortality
from veno-occlusive disease. Bone Marrow Transplant, 40(1):79-82.
Dignan FL, Wynn RF, Hdzic N, et al (2013). BCSH/BSBMT guidelines: diagnosis and management of veno-occlusive disease (sinusoidal
obstruction syndrome) following haematopoietic stem cell transplantation. Br J Haematol, 163(4):444-457. DOI:10.111/bjh.12558
Harper JL & Corbacioglu S (2016). Veno-occlusive hepatic disease. Available at: http://emedicine.medscape.com/article/989167-overview
Mohty M, Malard F, Abecassis M, et al (2016). Revised diagnosis and severity criteria for sinusoidal obstruction syndrome/veno-occlusive
disease in adult patients: a new classification from the European Society for Blood and Marrow Transplantation. Bone Marrow
Transplant, 51(7):906-912. DOI:10.1038/bmt.2016.130
References
Mohty M, Malard F, Abecassis M, et al (2015). Sinusoidal obstruction syndrome/veno-occlusive disease: current situation and perspectives – a
position statement from the European Society for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant, 50(6):781-789.
DOI:10.1038/bmt2015.52
Myers KC, Dandoy C, El-Bietar J, et al (2015). Veno-occlusive disease of the liver in the absence of elevation in bilirubin in pediatric patients
after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant, 21(2):379-381. DOI:10.1016/jbbmt.2014.09.026
Richardson PG, Ho VT, Cutler C, et al (2013). Hepatic veno-occlusive disease after hematopoietic stem cell transplantation: Novel insights to
pathogenesis, current status of treatment, and future directions. Biol Blood Marrow Transplant, 19(1):S88-S90.
DOI:10/1016/j.bbmt.2012.10.023
Richardson PG, Riches ML, Kernan NA, et al (2016). Phase 3 trial of defibrotide for the treatment of severe veno-occlusive disease and multi-
organ failure. Blood, 127(13):1656-1665. DOI:10.1182/blood-2015-10-676924


















