RT 255 14 Veno IVC
89
1 Venograph y Rt 255 Spring rev 2010 Week 2 - 2014 D. Charman Purpose Anatomy Pathology Veno Procedure Contrast Patient Care Other Modalities & Procedures
-
Upload
susanti-shanty -
Category
Documents
-
view
226 -
download
5
description
fghfgh
Transcript of RT 255 14 Veno IVC

1 Venography
Rt 255 Spring rev 2010
Week 2 - 2014D. Charman
PurposeAnatomyPathologyVeno ProcedureContrastPatient CareOther Modalities & Procedures

2 Vein anatomy – lower ext

3

4 Purpose of Venography
Venography is an x-ray exam that provides an image of the veins (leg) after a contrast is injected into a vein in the patient's foot
Enables the condition of the deep leg veins to be assessed
Primarily performed to diagnose deep vein thrombosis DVT

5 Indications Distinguish blood clots
from obstructions in the veins
Evaluate congenital vein problems
Assess the functioning of deep leg vein valves
Identify a vein for arterial bypass grafting (CABG)

6
is a common but elusive illness that can result in suffering and death if not recognized and treated effectively.
DVT occurs in ~2 million Americans each year. Death can occur when the venous thrombi
break off and form pulmonary emboli, which pass to and obstruct the arteries of the lungs.
DVT and pulmonary embolism (PE) most often complicate the course of sick, hospitalized patients but may also affect ambulatory and otherwise healthy persons.
Deep vein thrombosis (DVT)

7 DVT Deep vein thrombosis is a major complication in
orthopedic surgical patients and patients with cancer and other chronic illnesses.
DVT can be a chronic disease. Patients who survive the initial episode of DVT
are prone to chronic swelling of the leg and pain because the valves in the veins can be damaged by the thrombotic process, leading to venous hypertension.

8 LOWER LIMB DVT Venous thrombosis in the lower
limb can involve the superficial leg veins,
the deep veins of the calf (calf vein thrombosis),
the more proximal veins, including popliteal veins, the superficial femoral,
common femoral, and iliac veins.
Less commonly, thrombosis involves other veins in the body

9 PE It is estimated that each year 600, 000
patients develop PE and that 60,000 die of this complication. This number exceeds the number of
American women who die each year from breast cancer.
PE is now the most frequent cause of death associated with childbirth. Women are a prime target for PE, being affected more often than men.

10 Pulmonary Embolism
Occurs when a clot forms or becomes lodged in the pulmonary artery
Most commonly thrombus originates in the lower limbs and migrates
Can lead to resp distress, heart failure or cardiogenic shock
Symptoms are acute:Sudden coughingSOBChest pain

11
DVT & PE
DVT usually occurs in lower leg. Impedes normal blood flow. DVT is stationary. PE is the result of a DVT breaking apart.

12 The Danger of PE’s 3rd leading cause of cardiovascular death in U.S.

13 Pulmonaryembolism

14 Venous Thrombosis CH 8 Pathology
venous thrombosis- the formation of blood clots within a vein These clots commonly form in the veins of the lower extremities
and result from a slowing of the blood return to the heart. The contraction of the leg muscles assists with venous blood
return; therefore, postoperative or bedfast patients are especially prone to this disorder.
Phlebitis, an inflammation of the vein, is often associated with venous thrombosis - the combination of these disorders is thrombophlebitis.
The thrombus formation generally begins in the valves of the deep calf veins where thromboplastin traps red blood cells to create the blood clot. Patients may be placed on anticoagulant drugs or receive thrombolytic therapy.

15Venous Thrombosis
Cause Incidence Phlebitis Thrombus Thrombophlebitis

16 Deep Vein Thrombosis Primarily involves
lower limbs Major source of fatal
PE Risks
Restricted mobility Surgery Obesity Pregnant BC pills Long trips
PlaneCar

17 Thrombosis & Embolism
Intravascular clot Commonly in veins
more than arteries 3 factors
Where blood is slow
Change in the wall of vessels
Change in the blood itself
Thrombus that becomes detached from the vessel wall
Can easily flow to heart causing PE
Severity depends on location of embolism

18
DVT &
Phlebitis - Embolus

19 DVT

20 Deep Vein Thrombosis

21 DVT

22 Varicose Veins Dilated, elongated
and tortuous vessels
Most common to superficial veins of leg
Multiple bluish nodules just under skin
Development of collateral veins

23 Varicose Veins Valves are unable to prevent backflow Valves cease to function increasing blood volume is these veins
VaricoseVeins : http://www.youtube.com/watch?v=GpjhgpFc8DY&list=PLFA1CFBF548099911

24 Varicose veins are diseased blood vessels that have become
permanently dilated and can no longer efficiently
carry blood back to the heart. Arteries carry blood away
from the heart while veins return blood back to the heart.
Varicose veins can arise when this system gets backed up
Varicose veins are dilated, elongated, and tortuous vessels that most commonly involve the superficial veins of the leg just under the skin

25 Varicose Veins
Multiple round and oval calcifications in soft tissues (phleboliths) represent calcified thrombi
Shows the degree of collateral circulation
Demonstrates patency of the deep venous system

26 Repair

27 Spider Veins
Risk factors for spider veins are similar to those for varicose veins –
age, heredity, pregnancy, hormonal changes, obesity and extended periods of standing –
as well as sun exposure, particularly in fair-skinned people, and injuries to the skin surface.
Some physicians believe that exercise, weight loss and the wearing of support hose and flat shoes instead of high heels can reduce the incidence of spider veins.

28 Phlebitis Inflammation of a vein Often associated with
venous thrombosis US usually used to
diagnose Treated with
anticoagulants

29
LOWER LIMB VENOGRAMS
Unilateral or Bilateral study
Venogram – The Procedure

30Venogram - RT LegVenous Study – The Procedure

31 Prior to Procedure Pt should fast or drink only
clear fluids for four hours before the test - WHY
Thorough PT history obtained Informed consent If pt is nervous about the
doctor may give a sedative.

32 Explanation of Procedure: Legs The catheter is inserted into PT vein
(usually a vein in the foot) Contrast is slowly injected. Tourniquet may be tied around the ankle of the foot
the contrast is injected into - may also place one on the thigh
The procedure takes about 30 - 45 minutes

33

34 Contrast injected into top of foot Local anesthetic May be unilateral or bilateral Flush with saline mark syringe w/ band aid
Always label syringes!!!

35
The patient is asked to keep the leg still Radiologist may use fluoroscopy A series of images taken via fluoro and/or overheads films are taken fill the deep venous system with contrast The body may be tilted
Venogram Procedure

36
Post contrast Imaging may be done with Fluoro and/or “overhead” images

37 FILMING VARIES WITH RADIOLOGIST MAY NEED SCOUT FILMS 14 X 17 Cassettes starting at Ankles, Knees, Femurs, Pelvis, Abdomen & Chest may also be
taken What will the ABD film demonstrate?
(Delay 15 Min – IVP Film)
Overheads or 14x14 Fluoro Cassettes Or Digital
Images taken With & Without Tourniquets

38

39 AP & LATTAKEN

40

41

42

43

44
4444
Atherosclerosis Left LegArterial Study
How does this study compare to Venography?

45
Less money More reactions
More money Less reactions
Refresher on Contrast Media
CONSENTS
SIGNED AND WITNESSED AFTER PROCEDURE HAS BEEN EXPLAINED CHECK DEPARTMENT PROTOCOL WHO’S RESPONSIBLE ??????
SPECIAL PROCEDURESARE INVASIVEALWAYS GET PATIENT’S
HISTORY AND CONSENT
BEFORE BEGINNING OR
GIVING ANY CONTRAST MEDIA

46 •Contrast Media (non-ionic)
•Saline
•Xylocanine

47 CONTRAST MEDIA CONTRAST INJECTABLE WATER SOLUABLE IONIC VS NON IONIC VENOUS INJECTON
Saline Strength Sterile Labeled Stings during injection
1. What should be checked before2. Drawing up the contrast?3. How many times should you check the label?

48 Aftercare Patients should drink large amounts
of fluids to flush the remaining contrast solution from their bodies.
The area around the incision will be sore for a few days.
If there is swelling, redness, pain, or fever, the doctor should be notified.
Pain medication may be needed. In most cases, the patient can resume normal activities the next day.

49 Risks & Complications
phlebitis / infection at injection site tissue damage Formation of deep vein thrombosis
in a healthy leg. A rare side effect in up to 8% of
cases is a severe allergic reaction to the contrast.
This usually happens within 30 minutes after injection

50 Possible Post Procedure Complications
Congestive heart failure
Acute renal insufficiency
Venous thrombosis in a healthy leg
Dislodging a clot, perhaps resulting in pulmonary embolus or other complications

51 Abnormal resultsAbnormal venography results show well-defined filling defects in veins
Findings include: Blood clots Consistent filling defects An abrupt end of a
vessel Major deep veins that
are unfilled Contrast flow that is
diverted - These results confirm a diagnosis of deep vein thrombosis.

52 Venous Circulation
•Venograms typically are done for the lower legs –
•Injection of contrast into the venous system can also be used for larger venous systems

53 Types of Other Venogram Procedures
Leg (lower extremity) MOST COMMON Arm (upper extremity) Inferior Vena Cavagram Superior Vena Cavagram Adrenal Renal Saphenous Vein

54 Central Venography

55
Catheter injection directly for upper leg

56 DVT of Iliac Vein On x-ray appears as a
constant filling defect
Largely replaced by duplex color doppler ultrasound Demonstrates the
velocity of the venous blood flow

57 Post Femoral Vein Puncture Orders
Bed rest for 2-4 hours with affected leg straight. (Physician will specify)
Check puncture site for sign of bleeding.
Check B.P. q 1 hour x 4 hours. Encourage fluids. Resume pre-venography
activity

58 Arteriogram – subclavian injection
Upper Extremity Venogram – (valves present)

59 Review Anatomy of Upper Limb (RT 255 & 93

60 Inferior Vena Cavogram To view the inferior vena
cava to determine strictures, tumor blockage and location of blood clots.
A catheter is inserted in the femoral vein & positioned in the common iliac vein or the inferior aspect of the inferior vena cava.
• The contrast is injected through a multiple side hole catheter.

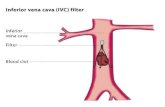
61 What is an IVC filter? An IVC Filter is a
“wire basket” that is used to trap emboli.
Several types available

62

63 Indications for IVC Filter Existing deep vein
thromboses, history of pulmonary embolism.
Surgical weight loss. Some cancer
patients. When anticoagulation
therapy is contraindicated.
Prolonged bed rest/ immobility.

64 IVC Filter Placement
• Utilized to trap deadly Pulmonary Embolism’s • Filter placed when anticoagulation
therapy contraindicated. This Procedure SAVES Lives. RISKS – CAN PUNCTURE!

65
Use of carbon dioxide (CO2) as a contrast medium is demonstrated (appearing white along the right of the spine) on a frail 75-year-old man.
inferior vena cavogram

66 Inferior Vena Cava Filter Placement
Designed to trap thrombus before causing an embolization
When anticoagulants are contraindicated this can be used

67 Inferior Vena Cava Filter Placement

68 Superior VenaCavogram
•The contrast medium may be injected through a needle or an angiographic catheter introduced into a vein in an antecubital fossa,
•superior opacification results from injection through a catheter positioned in the axillary or subclavian vein.
contrast 30-50ml at 10-15ml/sec

69 Superior Venacavogram Primarily done to rule out thrombus or occlusion X-rays should include:
Brachicephalic vein Subclavian vein Superior vena cava RT Atrium
Stenosis on a Superior Venacavogram

70
Cerebral Venous system is visualized in Angio- How does the contrast exit the cranium?

71

72 Post- Procedure Care-
Apply pressure to puncture site 5-20 min. Patient monitored 6-8 hours in hospital.
BEDREST. Watched for hematoma.
Minimal activity for the 1st couple of days after discharge.

73 Hepatic Venogram
Performed to rule out stenosis or thrombus of the hepatic veins
Obtain pressure measurements of the veins inside the liver
Usually catheter enters jugular vein or upper limb veins

74 Transjugular Intrahepatic Portosystemic Shunt
Intervention for creating an artificial low-pressure pathway Between portal & hepatic
veins Hepatic venogram usually
preformed b before placement US also useful

75 Portal Venogram
Portal System

76 Renal Venogram Rule out thrombosis of renal vein
Renal vein catheterized to take blood Measure the production of
renin Catheter insertion site:
femoral vein Contrast injected 8ml/sec
for 16ml total 2 images per second for 4
seconds

77
Renal Venogram: To view the renal veins for the presence of thrombosis.Can you distinguish the difference in the Procedures?

78 It is nearly 100% sensitive and specific in making this
diagnosis (pulmonary embolism is diagnosed in other ways).= HOW?
Accuracy is crucial since deep vein thrombosis can lead to pulmonary embolism, a condition that can be fatal.
It is especially useful when there is a strong suspicion of deep vein thrombosis, but non-invasive tests (ultrasound) have failed to identify the disease.
Doppler U.S. used to determine presence of DVT. MRI & CT can also be used.
Fluoroscopy in the Angio suite used for insertion of filters for IVC.
Leg Venography & Other Modalities

79 Venography is not used often,
because it is painful & expensive Venography takes between 30-45 minutes + up to 10 min of beam on – fluoro time May be done in a physician's office, or a hospital. US – Now modality of choice Unless results are inconclusive

80 PROCEDURES DONE w/ US
Peripheral Vascular Ultrasound Upper/Lower Arterial Evaluation Upper/Lower Venous Evaluation Carotid Ultrasound Renal Duplex Imaging
Because venography is an invasive technique, other modalities have been developed for detecting DVT.
Duplex color Doppler ultrasound, which demonstrates changes in the velocity of venous blood flow with 95% accuracy, is now the preferred initial imaging modality

81 VASCULAR ULTRASOUNDnon-invasive - no contrastno radiation

82 BENEFITS RISKS Less Expensive ? Non Invasive/Painless
(If No Health Problems) Soft Tissue Visualized Tortuous Veins Well
Visualized Has Replaced Venography Capable Of Replacing Angio
Someday (?)
Sometimes Inconclusive or Unclear
Vein Is Totally Closed Off Or Not?
Unable To See Deep Vessels
THE END of Venogram Lecturetry the Review questions……

83 Venous thrombosis most often affects the:
A) Deep veins of the upper extremities
B) Deep veins of the lower extremities
C) Superficial veins of the upper extremities
D) Superficial veins of the lower extremities

84
Which term refers to an inability of the heart to propel blood at a sufficient rate and volume?
A) Congestive heart failure
B) Pulmonary edema
C) Valvular disease
D) Valvular stenosis

85The invasive procedure for determining deep vein thrombosis is:
A) Doppler ultrasound
B) Venography
C) CT
D) Arteriography

86
What is a life threatening pathology that can occur from a dislodged thrombus?
A) Deep venous thrombosis
B) Atherosclerosis
C) Pulmonary edema
D) Pulmonary embolism

87 Which of the following are symptoms or PE?
1) Cough
2) Fever
3) Chest pain
A) 1 & 2
B) 1 & 3
C) 2 & 3
D) All the above

88 What is the purpose of a IVC filter?
A) To decrease blood flow to diseased liver
B)To graft a blocked artery in the pulmonary artery
C) To prevent thrombus from migrating to heart

89
With varicose veins, the valves are working harder to keep a constant flow of blood to the heart.
A) True
B) False