Ophthalmology Market Access by Dr Steven Bradshaw
24
©2015 Market Access Solutions Ltd. All rights reserved. Market Access Solutions, Ltd Market Access Strategies for the Global Healthcare Environment Therapeutic landscape in posterior segment disease: opportunities for patients, clinicians and for industry Presented at the 15 th EURETINA Congress NICE; 17 th September 2015: #FP-7265 Steven Bradshaw BSc (Hons), MB BChir, MRCOphth European Director, Market Access Solutions
-
Upload
dr-steven-bradshaw -
Category
Health & Medicine
-
view
750 -
download
0
Transcript of Ophthalmology Market Access by Dr Steven Bradshaw

©2015 Market Access Solutions Ltd. All rights reserved.
Market Access Solutions, Ltd Market Access Strategies for the Global Healthcare Environment
Therapeutic landscape in posterior segment disease: opportunities for patients, clinicians and for industry
Presented at the 15th EURETINA Congress NICE; 17th September 2015: #FP-7265
Steven Bradshaw BSc (Hons), MB BChir, MRCOphthEuropean Director, Market Access Solutions

©2015 Market Access Solutions Ltd. All rights reserved.
Disclosure
Disclosure
2
Market Access Solutions (Market Access Solutions Ltd and Market Access Solutions LLC) receive fees from industry for consulting on new and existing medicines
We did not receive any sponsorship to attend or present at EURETINA We will not be endorsing any particular product

©2015 Market Access Solutions Ltd. All rights reserved.
1. Bringing a new eye therapy to market2. White space assessment in retinal disease• Objectives and methods• Findings• Considerations for clinical development in dry AMD
4. Conclusions and recommendations
3
Overview
Report Content

©2015 Market Access Solutions Ltd. All rights reserved.
Once upon a time … efficacy and safety used to be enough
Background
4
... provided that pharmaceutical products were safe and effective, doctors could prescribe them, patients could get their prescriptions filled, and payers would reimburse the costs

©2015 Market Access Solutions Ltd. All rights reserved.
Now a number of challenges exist … payers need to balance healthcare demands with budgetary constraints
Background
5
To optimize market access, pharma companies also need to demonstrate the value of the product during national and regional pricing and reimbursement negotiations … the requirements of payers are different to those of regulators
Phase 1 Phase 2 Phase 3
Clinical Development
MA P&R Launch
Commercialisation
Quality
Safety
Efficacy
Payer value = Market access
To achieve market authorisation/regulatory approval, pharma companies need to demonstrate that a product is safe, effective and meets quality standards
4th hurdle
The difference between market access and marketing is that market access requires evidence that payers value ...

©2015 Market Access Solutions Ltd. All rights reserved.
What payers need to know … and what they tend not to consider
Background
6
Is the product needed? (unmet clinical need) Does it work? (clinical efficacy) How well does it work? (clinical effectiveness) Can we control its use? (patient population) Is it worth it? (cost effectiveness) Can we afford it? (budget impact)
Tolerability Mechanism of action Pharmacokinetics Societal costs Route of administration Convenience for patients Indirect costs
Usually not factored in payer decision makingUsual factors in payer decision making

©2015 Market Access Solutions Ltd. All rights reserved.
1. Bringing a new eye therapy to market2. White space assessment in retinal disease• Objectives and methods• Findings• Considerations for clinical development in dry AMD
4. Conclusions and recommendations
7
Overview
Report Content

©2015 Market Access Solutions Ltd. All rights reserved.
Assessing opportunities for new retinal therapies was the ultimate aim of this research
Objectives and Methods
Overarching goal Understand access opportunities for new entrants in posterior segment disorders
Key focus areas of the assessment
Understand the preceding and current/future clinical and market perspectives Identify the remaining unmet needs in each indication Outline the value drivers for access for future entrants Review HTA recommendations for each publically available evaluation Key insights for clinical trial design and launch in multiple indications and how
future agents can expect to achieve access and price
Indications Wet AMD, dry AMD, DME, non-infectious posterior uveitis and vitreomacular traction
8

©2015 Market Access Solutions Ltd. All rights reserved. 9
Secondary research and qualitative interviews with 15 payers, decision makers and key opinion leaders across three major markets in Europe, plus Canada and Japan
Objectives and Methods
JapanFrance
Germany
United Kingdom
Market in scope
Canada

©2015 Market Access Solutions Ltd. All rights reserved.
1. Bringing a new eye therapy to market2. White space assessment in retinal disease• Objectives and methods• Findings• Considerations for clinical development in dry AMD
4. Conclusions and recommendations
10
Overview
Report Content

©2015 Market Access Solutions Ltd. All rights reserved. 11
Characteristic Wet AMD Dry AMD DME Non-infectious posterior uveitis
Vitreomacular traction
Prevalence 170 per 10,000 and increasing
380+ per 10,000 and increasing
Average of 7% of diabetics affected 38 per 100,000 22.5 per 100 000
Disease burden A leading cause of blindness
Minor progressive symptoms
Major cause of visual impairment
Debilitating in acute phase
Symptoms are mild and develop slowly
Economic burden / Therapy costs
High cost anti-VEGF drugs
No reimbursed treatment
High cost anti-VEGF drugs
Low cost drugs available
One off surgical costs
Unmet needBurdensome
disease but good treatments
No current therapies
Burdensome disease but good
treatmentsTreatments
availableTreatments
available
Competitive environment (pipeline)
Fovista and biosimilars
Lampalizumab and other products in
pipelineSeveral licensed
products launchedFew treatments in
pipelineFew treatments in
pipeline
Payer management PAS required for cost-effectiveness
No cost control but no available budget
PAS required for recommendation
Off-label products available
PAS maybe required for
recommendation
HTA challenges Current therapies required PAS
Unknown environment
Population restrictions likely
Low incentive to review
Payers more aware since Jetrea
Overall opportunity of entering therapy area
MEDIUM: Competitive and
highly managed with effective SoC
HIGH: First to market product could have significant impact
MEDIUM: High population but
treatments available
LOW: Small population with off-
label treatments used
LOW: Small population and increased Payer
awareness
Opportunity Assessment
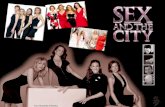
Opportunity in posterior segment disorders based on multicriteria assessment of perceived clinical burden, unmet need, market dynamics and payer environment
PAS = patient access scheme; SoC = standard of care

©2015 Market Access Solutions Ltd. All rights reserved. 12
Opportunity Assessment
The market landscape is expected to transform should one or more pipeline developments prove successful
Lampalizumab is expected to be the first drug to enter the dry AMD market• 20.4% reduction in geographic
atrophy progression from month 6 through month 18 in its phase II study
• phase III is ongoing and includes patients that are positive for the complement factor I biomarker; the primary endpoint is reduction in the rate of geographic atrophy progression
Cell therapies are still in early phase of development, showing promising results and indicate a high price tag
Therapies being developed for dry AMD - Clinicatrials.gov Dec ’14
The key challenge for any product to reach patients, is to demonstrate clinical and economic outcomes that resonate with payers ...

©2015 Market Access Solutions Ltd. All rights reserved.
1. Bringing a new eye therapy to market2. White space assessment in retinal disease• Objectives and methods• Findings• Considerations for clinical development in dry AMD
4. Conclusions and recommendations
13
Overview
Report Content

©2015 Market Access Solutions Ltd. All rights reserved. 14
1 2 3 4 5
Payers (n=4) KOLs (n=10)
Clinical Development Considerations
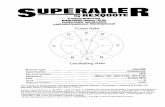
Perceptions vary between payers and KOLs, with the former suggesting change in BCVA and the latter change in GA as the optimal primary efficacy measure in dry AMD
Change in Best Corrected Visual Acuity (BCVA)
Functional
Change in central visual fields
Near acuity/ Reading speed
Contrast sensitivity
Visual Function Questionnaire (VFQ-25)
AMSLER testing
Change in drusen size/ area
AnatomicalHyper/ hypo-pigmentation
Central retinal thickness
Rate of change in the area of geographical atrophy (GA)
← Value →
Notes on interpretation: Interviewees were asked to score the value of each endpoint on a scale of 1 (low) to 5 (high). Scores were averaged for payers (n=4) and KOLs (n=10).
Low High
Perceptions of dry AMD endpoints
1 2 3 4 5
Payers (n=4) KOLs (n=10)
=Payer-preferred =KOL-preferred

©2015 Market Access Solutions Ltd. All rights reserved. 15
1 2 3 4 5
Payers (n=4) KOLs (n=10)
Clinical Development Considerations
Other anatomical endpoints with no clear relevance to patient outcomes are scored lower in value, especially by payers
Anatomical endpoints are scored low in value because:• Payers are unfamiliar with terms and clinical meaningfulness of these changes
and how vision is affected as a direct consequence
• KOLs are not sure about the objectivity of these measurements and question their correlation to dry AMD progression
“These are just surrogate endpoints and so far I have not seen convincing reasons for why they are important. If there were publications to suggest otherwise then my opinion would be different. The first thing I do when evaluating a new therapy is to put down the manufacturer’s submission and look at PubMed to see the validity of the claims for myself.”– Payer, Germany
“Can usually use OCT for AMD and DME but it is not clear what is the best measure to use for dry AMD and which one best correlates with disease progression. Nothing good at the moment.”– KOL, Germany
← Value →Low High
Perceptions of dry AMD endpoints
1 2 3 4 5
Payers (n=4) KOLs (n=10)
Notes on interpretation: Interviewees were asked to score the value of each endpoint on a scale of 1 (low) to 5 (high). Scores were averaged for payers (n=4) and KOLs (n=10).
Change in drusen size/area
AnatomicalHyper/hypo-pigmentation
Central retinal thickness

©2015 Market Access Solutions Ltd. All rights reserved.
1. Bringing a new eye therapy to market2. White space assessment in retinal disease• Objectives and methods• Findings• Considerations for clinical development in dry AMD
4. Conclusions and recommendations
16
Overview
Report Content

©2015 Market Access Solutions Ltd. All rights reserved. 17
Conclusions and Recommendations
Majority of threats and payer uncertainty to funding patient access can be mitigated through clinical community support of effective therapies and payer education
Uncertainty around acceptability of predominantly anatomic endpoints
Publish, even if it is obvious to ophthalmologists that GA size matters, because payers need evidence to support their decisions
Size of patient population may necessitate restriction to subgroups to control budget impact
Help get therapies to those groups with higher need through research and publications
Once treatments come to market, later entrants will require H2H trials
Champion effective and safe treatments to best inform industry so that future trials use the most appropriate comparator and patients will be able to access the best medicines
Slower progression rates and reduced burden for earlier stages means that payers may be initially apprehensive about up front payments
Work to develop real world data from registries or small local studies to help to support access to therapies that are safe and effective, particularly for high cost medicines

©2015 Market Access Solutions Ltd. All rights reserved.
Market Access Strategies for the Global Healthcare Environment
For further information
Steve Bradshaw, Director Market Access Solutions
1000 Great West Road, London, TW8 9DW
Tel: +44.203.675.8995
.mktxs.com

©2015 Market Access Solutions Ltd. All rights reserved. 19
Conclusions and Recommendations
Dry AMD represents a considerable market opportunity especially for agents that can successfully target and prevent the progression of geographic atrophy
Opportunities Threats
Large and increasing patient population with no satisfactory therapies
Payers’ willingness to pay is thought to be high due to high unmet need and potential to avoid progression to expensive-to-treat wet AMD
Initial clinical outcome requirements may be more relaxed due to current lack of comparative treatments; for the first entrant a placebo-controlled trial will be satisfactory
Market opportunity is estimated at US$5 billion globally
Uncertainty around acceptability of predominantly anatomic endpoints
Size of patient population may necessitate restriction to subgroups to control budget impact
Once new treatments penetrate the market, later entrants will require H2H trials
Slower progression rates and reduced burden for earlier stages means that payers may be initially apprehensive about up front payments – especially for high-cost regenerative medicines
×

©2015 Market Access Solutions Ltd. All rights reserved. 20
Clinical Development Considerations
From a combined payer-KOL perspective, a placebo-controlled trial of at least 2 years in patients with moderate visual loss represents the best design (for a first entrant)
Feature Requirement Rationale
Pivotal design Placebo control (first entry) Because no SoC available, placebo trial would be acceptable Vitamin supplements can be used in both arms, as usually recommended
Duration 2 years minimum As a slowly progressing disease 2 years is judged the minimum acceptable Most interviewees also ask for an additional 1-3 years extension trial
PopulationStage: IntermediateSize: 250+ patients per armExclusions: Late-stage, other retinal diseases
Intermediate stage patients with moderate visual loss (e.g., 20/80 vision) recommended as motivated to complete study and likely to see better differentiation between study arms than early or late stage
Primary endpoints
Payers: BCVA stab/improvementKOLs: GA progression
BCVA most important for licensing and for payers GA progression (as measured) is a KOL favourite, but correlation with VA
would be needed to improve payer acceptance
Outcomes 3 lines difference in ETDRS20% relative change in GA
Payers familiar with 3 lines gain on ETDRS from previous experience with wet AMD trials; % change in GA in line with lampalizumab’s outcomes
Safety Ocular AEs: e.g., infectionsOther AEs: e.g., immunological
Any therapy requiring an invasive procedure in patients with early disease and low-moderate disease burden must have few side effects
“There’s no treatment at the moment so sham study is fine, but you compare against nutritional supplementation … and, because it's a slowly progressing disease I’d want data for 5 years.”– KOL, France
“The best ones are those with some element of visual loss and then you'd see a gradual decline in the control group. These patients are also more highly motivated to see out the trial because they have the early signs.” – KOL, UK
Requirements for a dry AMD clinical trial based on interviewee responses

©2015 Market Access Solutions Ltd. All rights reserved. 21
Characteristic Wet AMD Dry AMD DME Non-infectious posterior uveitis
Vitreomacular traction
Prevalence
Clinical burden
Economic burden
Unmet need
Competitive environment
Payer management
HTA challenges
Overall opportunity of entering therapy area
MEDIUM: Competitive and
highly managed with effective SoC
HIGH: First to market product could have significant impact
MEDIUM: High population but
treatments available
LOW: Small population with off-
label treatments used
LOW: Small population and increased Payer
awareness
Opportunity Assessment
Opportunity in posterior segment disorders based on multicriteria assessment of perceived clinical burden, unmet need, market dynamics and payer environment
Large Medium SmallKEY:

©2015 Market Access Solutions Ltd. All rights reserved.
Conclusions and Recommendations
To facilitate market access, manufacturers can offer support to physicians and patients in the form of education, administrative assistance and research funding
Markets Focus Manufacturer provided services
Educational programs for patients are well-received by French ophthalmologists and patient groups provide a forum for support
Educational and administrative support programs in place German payers are skeptical of manufacturer involvement at local level, preferring straight
discounting at the national or regional level
Novartis have entered partnerships with the NHS to provide static and mobile eye clinics to improve service to local areas• Currently 3 schemes are running in England and Wales
Novartis and Bayer provide local and personal assistance to patients who may have trouble paying for Lucentis and Eylea through Special Access Programs• If patients do not have full coverage (e.g. they are under 65 years old) then copayment rates of 10-
20% can be prohibitive on expensive VEGF therapies
• Manufacturers will investigate with the health insurers for personal plans so patients can access treatment
• This ensures patients can receive treatment at initial consultation without the need for complicated insurance assessment
Japanese ophthalmologists are open to approach from manufacturers who may offer prescriber/ patient incentives
= Patient-focused= Physician-focused
22

©2015 Market Access Solutions Ltd. All rights reserved. 23
Conclusions and Recommendations
Inherent differences between regenerative medicines and traditional pharmaceuticals present multiple challenges for access and reimbursement
Pricing, reimbursement and access issues Gene therapies
Traditional pharmaceuticals Implications
Involves multiple procedural steps that may be separately reimbursable Often Rarely
• Similar to reimbursement for a device/procedure
• Failure to achieve reimbursement of any component may jeopardize reimbursement of the entire procedure
HTA will focus on the cost-effectiveness of the entire procedure Yes Not often
applicable• Requires HEOR data collection regarding entire
procedure
May involve multiple billing codes/tariffs and/or payment centers for reimbursement of the full procedure
Yes No • Lack of appropriate codes/tariffs or payment may limit or preclude access and uptake
May involve requirements for longer-term data collection to demonstrate value (incl. post-market follow-up data)
Yes Sometimes • This is a top HTA criticism of most regenerative therapies in global markets to date
Strong potential to be more costly than standard of care alternatives Often Sometimes
• Higher cost means that therapies must demonstrate significant outcome improvements vs. standard of care
May enable a disease cure or prolonged therapeutic effect Yes Rarely • Can alter the balance of benefit-cost tradeoffs
in value assessment

©2015 Market Access Solutions Ltd. All rights reserved.
Summary
Conclusions and Recommendations
24
“They need to provide data beyond the regulatory approval standards – it does no good to compare a new and expensive therapy to a placebo if a comparator already exists.” – National Payer, Germany
Ophthalmologists are central to identification of
existing unmet needs, supporting clinical development and
monitoring through research and in shaping
payer beliefs, particularly where there are misconceptions
For high cost regenerative medicines (gene therapies
anticipated to cost>€1 million per dose), ‘payer centric’ clinical development
and consideration of innovative funding models
(pay for performance, annuity-based, risk pools …
even crowd funding) are needed to ensure patient
access
Payers have established their own therapeutic
guidelines, manage access more tightly and scrutinize the price of new therapies,
meaning pharma companies need to provide the
evidence sought by payers, specifically information such
as comparative effectiveness, cost
effectiveness and real world data
Evidence needs Clinical support Funding models