
OLIGO-MENORRHEA: WHAT IS HER RISK
24
OLIGO-MENORRHEA: WHAT IS HER RISK FOR ENDOMETRIAL CANCER? Angela Liang, MD Department of OB/GYN Michigan Medicine
Transcript of OLIGO-MENORRHEA: WHAT IS HER RISK

OLIGO-MENORRHEA: WHAT IS HER RISK
FOR ENDOMETRIAL CANCER?
Angela Liang, MD Department of OB/GYN Michigan Medicine

NO DISCLOSURES

OBJECTIVES
1. Identify patients with anovulatory cycles
2. Identify patients at risk for endometrial hyperplasia or cancer and recognize when endometrial sampling is necessary
3. Understand treatment for anovulatory bleeding, and precursors to endometrial cancer
4. Discuss treatment options for patients that decline hormonal therapy or women that desire fertility
OVULATORY CYCLE – WHAT’S NORMAL? • Between 21-35 days
• <=7 days, with most blood loss within the first 3 days
• Predictable, but can vary by a few days each month


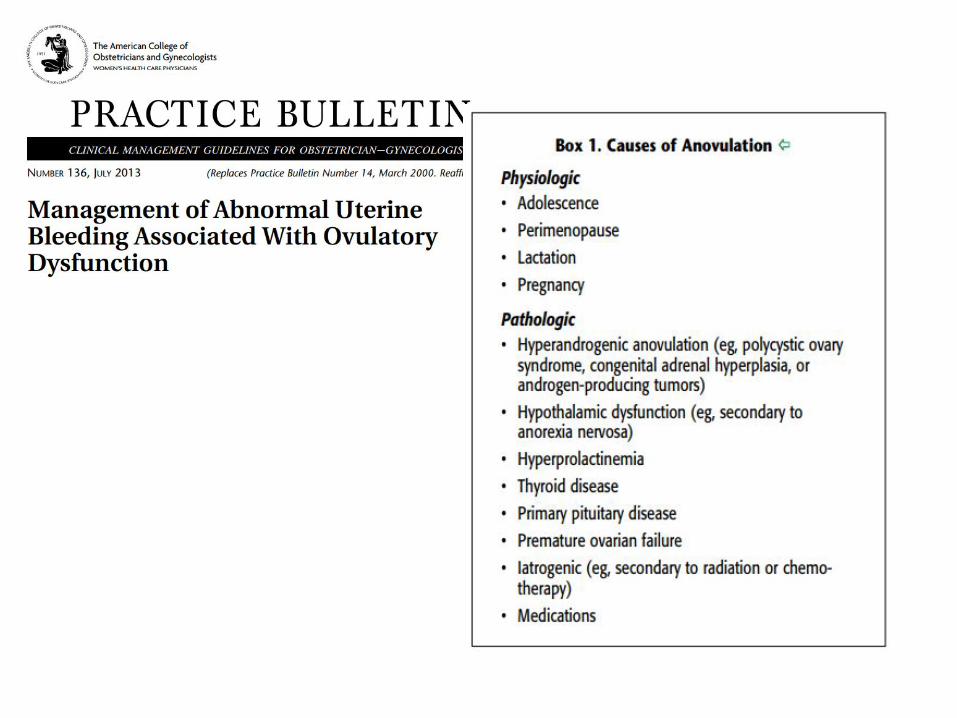
ANOVULATION - WHAT CAUSES ABNORMAL BLEEDING? • Endometrial proliferation without orderly shedding
• Orderly shedding depends on progesterone (no corpus luteum if no ovulation)
• Non-cyclic, unpredictable, inconsistent in volume (as one area begins to heal, another one begins to slough)

OVULATORY VS. ANOVULATORY CYCLES HOW TO DIFFERENTIATE?
HISTORY & PHYSICAL is critical!
Ovulatory Anovulatory
Regular cycle length Unpredictable cycle length
Predictable bleeding pattern Unpredictable bleeding pattern
Mittleschmertz
Breast tenderness
Increased mucoid vaginal discharge
Premenstrual cramping and bloating
Positive ovulation predictor kits

ANOVULATORY CYCLES CONFIRMING THE DIAGNOSIS & RECOMMENDED ASSESSMENT
• Pregnancy testing for sexually active women
• Rule out structural etiology • Ultrasound • Hysteroscopy • Saline-infusion sonohystography
• TSH
• Prolactin
• Endometrial biopsy for women with risk factors for endometrial hyperplasia or malignancy

ENDOMETRIAL CANCER • 4th most common cancer in women; American women have a 1 in 38 lifetime chance of developing endometrial cancer1
• Caucasian women 2.81% lifetime risk • African American women 2.48% lifetime risk, more likely to have type II endometrial
carcinoma
• Type 1, endometrioid adenocarcinoma • 80% of cases • Low grade, confined to uterus when diagnosed • Estrogen dependent - Prolonged exposure to unopposed estrogen (Continued
proliferation of the endometrium)
• Type 2, clear cell and papillary serous histology • Increased risk for stage III or IV disease • Poorer prognosis • Papillary serious tumors account for ~10% of cases, but account for almost 40% of
deaths from endometrial cancer
1. Howlader N, Noone AM, Krapcho M, Garshell J, Miller D, Altekruse SF, et al., editors. SEER Cancer Statistics Review, 1975–2011. Bethesda (MD): National Cancer Institute; 2014. Available at: http://seer.cancer.gov/csr/1975_2011. Retrieved January 20, 2014

PRECURSORS OF TYPE 1 INTERNATIONAL ENDOMETRIAL COLLABORATIVE GROUP SCHEMA • Benign endometrial hyperplasia
• 1-5% progress to endometrial cancer
• Endometrial intraepithelial neoplasia (consistent with atypia with WHO94 schema) • 40% of patients with EIN by biopsy have underlying carcinoma on
hysterectomy specimen2
• ~27% progress to endometrial cancer
WHO94 schema: • Simple hyperplasia without atypia • Complex hyperplasia without atypia • Simple hyperplasia with atypia
• Complex hyperplasia without atypia
2. Trimble CL, Kauderer J, Zaino R, Silverberg S, Lim PC, Burke JJ 2nd, et al. Concurrent endometrial carcinoma in women with a biopsy diagnosis of atypical endometrial hyperplasia: a Gynecologic Oncology Group study. Cancer 2006;106:812–9

Obesity - excessive peripheral conversion of androgens to estrone in adipose tissue

WHEN TO BIOPSY BASED ON AGE • Age 13-18 – incidence of endometrial cancer is 0.2/100,000 women
• Age 19-39 – incidence of endometrial cancer still very low, 5% diagnosed before age 40 • 20-34 years 1.6%
• 35-44 years 6.2%
• Age 40-menopause – majority of women diagnosed in menopause • 40-50 years 13.6-24 cases per 100,000 women years
• >45 higher rate of advanced-stage disease, worse prognosis compared to <45 • All women 45 or older should be biopsied when presenting for AUB

WHEN TO BIOPSY BASED ON BMI
• Retrospective cohort study, 916 premenopausal women <55 yo referred to gynecology
Wise, MR. et al. Body mass index trumps age in decision for endometrial biopsy: cohort study of symptomatic premenopausal women AJOG 2016; 215:598.e1 - 598.e8


ENDOMETRIAL BIOPSY
• Endometrial pipelle: samples an average of 4% of the endometrium (range 0-12%)
• Generally better at diagnosing diffuse lesions (>50% of the uterus), rather than focal lesions
• Sensitivity for diagnosis of endometrial cancer by Pipelle in postmenopausal women 99.6%, premenopausal women 91%, atypical hyperplasia 81%3
• PROS: Outpatient, no anesthesia or local anesthesia only, low risk for perforation, less costly
3. Dijkhuizen FP, Mol BW, Brölmann HA, Heintz AP. The accuracy of endometrial sampling in the diagnosis of patients with endometrial carcinoma and hyperplasia: a meta-analysis. Cancer. 2000;89(8):1765.

HOW TO OVERCOME A DIFFICULT ENDOMETRIAL BIOPSY • Cervical stenosis more common in nulliparous or post-menopausal women
• Administer an oral NSAID 60 minutes prior to biopsy (reduces post-procedure pain)
• Use a tenaculum
• Apply a topical cervical anesthetic
• Use dilators
• *Paracervical block may be ineffective, but increases risk of bradycardia & hypotension
• *Misoprostol – unproven benefit

PRINCIPLES OF TREATMENT- PREVENTATIVE STRATEGIES • Considerations in treatment: • Risk factors for progression • Contraceptive needs
• Desire for fertility
• Removal of exogenous sources of unopposed estrogen
• Correcting ovulatory dysfunction/Protection of endometrium • if expected to be a chronic issue (PCOS), consider maintenance therapy • Can be cyclical progestin treatment
• Weight loss and increased exercise • “Both endometrial hyperplasia and cancer are foreseeable and predictable
consequences of obesity”4
• Bariatric surgery - Significant reduction in rate of endometrial cancer following bariatric surgery compare to obese controls (17% vs 62.3%)5
4. Modesitt, SC. Missed Opportunities for Primary Endometrial Cancer Prevention: How to Optimize Early Identification and Treatment of High-Risk Women. Obstet Gyncol 2012;120:989-91. 5. McCawley GM, Ferriss JS, Geffel D, Northup CJ, Modesitt SC. Cancer in obese women: potential protective impact of bariatric surgery. J Am Coll Surg. 2009;208(6):1093.

BENIGN ENDOMETRIAL HYPERPLASIA (PROLONGED ESTROGEN EXPOSURE) § Surveillance § if risk of occult cancer or progression low § if the inciting factor that resulted in endometrial proliferation has been eliminated § Once benign hyperplasia has regressed, can continue progestin maintenance therapy
§ Progestin therapy - route and dose not well-defined § Progestins counterbalance proliferative effects of estrogens and induce secretory
differentiation § Contraindications: § Megestrol acetate, medroxyprogesterone acetate, micronized prometrium, norethindrone,
levonorgestrel IUD § Continuous dosing favored to cyclic
§ Combined estrogen-progestin therapy (OCPs) in premenopausal women – inadequate data
§ Follow up: repeat biopsy q 3-6 months, especially if bleeding pattern does not normalize; expect regression after 6 month of progestin therapy

ENDOMETRIAL INTRAEPITHELIAL NEOPLASIA (PRECANCEROUS)
• Goals of treatment: • Rule out concurrent adenocarcinoma • Prevent progression to cancer
• Surgery – total hysterectomy; definitive assessment of a possible concurrent carcinoma and effectively treats premalignant lesions • Patients should be counseled regarding risk for additional surgery to
complete staging if carcinoma is identified

ENDOMETRIAL INTRAEPITHELIAL NEOPLASIA (PRECANCEROUS) • Non-surgical treatment– reserved for women who desire future fertility, or poor surgical candidates; no consensus! • Reasonable first options: Levonorgestrel IUD or oral progestin x 6 months
• GOG-224 – EMB at 12 weeks, treatment continues for additional 12 weeks if biopsy results is positive; continue biopsy or curettage every 3-6 months until 3 negative biopsy results are obtained
• Biopsy 1-2 weeks after progestin withdrawal bleed to minimize progesterone effects that can confound histologic interpretation
• Hormone therapy resistance up to 30%
• Experimental: Metformin - Antiproliferative effects, reduce insulin resistance Ovulation induction (clomiphene or aromatase inhibitors) – in reproductive age
women, will help form corpus luteum GnRH agonists

CASE #1
31 yo nulligravida who presents to clinic for irregular menses and difficulty conceiving. She reports for the last 5-6 years, her bleeding has been irregular. She has light spotting that occurs intermittently throughout the day. Over the course of a week, she estimates bleeding episodes every other day.
PMH: obesity (BMI 47), subclinical hypothyroidism
Ultrasound demonstrates diffusely heterogeneous lining measuring 1.3 cm
Do you biopsy?
Pathology: endometrioid adenocarcinoma, FIGO grade 2

CASE #2
41 yo G4P3 presents to clinic with heavy menstrual bleeding, which has worsened over the last few months. She also notes spotting a couple times during this time. She is obese with a BMI of 31. She is otherwise healthy.
Ultrasound is unremarkable
Do you biopsy?
Pathology: complex and simple hyperplasia without atypia
She starts daily norethindrone – When do you biopsy again?
3-6 months, pathology: regression of disease

REFERENCES • Endometrial intraepithelial neoplasia. Committee Opinion No. 631. American College of Obstetricians and Gynecologists. Obstet Gynecol 2015;125;1272-8.
• Practice Bulletin No. 149: Endometrial cancer. Obstet Gynecol 2015; 125; 1006-26.
• Practice bulletin no. 136: Management of Abnormal Uterine Bleeding Associated with Ovulatory Dysfunction. Obstet Gynecol 2013; 122;176-85.
• Giuntoli, RL, Zacur, HA. Classification and diagnosis of endometrial hyperplasia. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (2016)
• Trimble et al. Obstet Gynecol 2012; 120:1160-75.
• Crane, JMG. How to overcome a resistant cervix for hysteroscopy and endometrial biopsy. OBG Management 2007; 19(11): 37-45.


















