2-medical treatment of endometrial hyperplasia and endometrial cancer
Upload
barrie-andersonCategory
view
214download
1
Obesity and prognosis in endometrial cancer
Barrie Anderson, MDflJoseph P. Connor, MD," Janet I. Andrews, MDfl Charles S. Davis, PhD, b Richard E. Buller, MD, PhD, ~ ~Joel I. Sorosky, MD," andJo A. Benda, MD ~' d
Iowa City, Iowa
OBJECTIVE: We tested the null hypothesis that morbid obesity as measured by the Quetelet index has no influence on survival in endometrial cancer. STUDY DESIGN: A retrospective study of 492 women with endometrial carcinoma was performed. Age, height, weight, Quetelet index, stage, cell type, grade, node status, peritoneal cytologic findings, and depth of myometrial invasion were analyzed for influence on survival. RESULTS-" Mean Quetelet index was 34 (range 16 to 89). Quetelet index was <30 in 45% of patients, 30 to 40 in 33%, and >40 in 22%. Five percent of those with a Quetelet index >40 had positive nodes, but 64% of patients with a Quetelet index >40 did not have lymph node sampling done. Lack of sampling of lymph nodes in the entire group had no adverse effect on survival. In a proportional hazards regression model for time from diagnosis to death from disease, grade, node status, myometrial invasion, and stage had highly significant effects. When Quetelet index was analyzed as a continuous variable, as Quetelet index increased, time to recurrence was significantly increased (p = 0.0136), and significance was approached for survival (p = 0.0645). Quetelet index was strongly related to grade (p = 0.013), depth of myometrial invasion (p = 0.031), negative cytologic findings (p = 0.004), and stage (p = 0.011) with obese patients having better differentiated, less invasive tumors of lower stage with negative washings. CONCLUSIONS: Morbid obesity positively affects survival in endometrial carcinoma. This effect is accounted for by the association of obesity with less aggressive disease. Morbid obesity is not associated with increased death from other causes. Lack of sampling of negative lymph nodes does not adversely affect survival. (AM J OaSTET GyNECOL 1996;174:1171-9.)
Key words: Obesity, endometrial cancer, prognosis
Whereas obesity is a known risk factor for the develop- ment of endometrial adenocarcinoma, ]-3 studies evaluat- ing the relationship of obesity to other prognostic factors and the effect of obesity on prognosis itself have not been published.
Morbid obesity can negatively influence surgical man- agement through difficulty in exposure, especially through the laparoscope and through increased intraop- erative and postoperative complications. Retroperitoneal fat deposits may impair adequate lymph node sampling by both the surgeon and the pathologist, resulting in underestimation of disease extent. Some may consider medical conditions associated with obesity to represent a greater threat to life than the cancer itself, leading to less aggressive treatment.
Obesity may also hinder the delivery of adequate adju- vant radiation treatment. Standard teletherapy machines
Prom the Departments of Obstetrics and Gynecology, a Preventive Medi- cine and Environmental Health, h Pharmacology, c and Pathology, ~ Uni- versity of Iowa College of Medicine. Presented by invitation at the Fourteenth Annual Meeting of the Ameri- can Gynecological and Obstetrical Society, Napa, California, September 7-9, 1995. Reprint requests: Barrie Anderson, MD, Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, 4630 JCP, University of Iowa, 200 Hawkins Dr., Iowa City, IA 52242. Copyright �9 1996 by Mosby-Year Book, Inc. 0002-9378/96 $5.00+ 0 6/6/71137
may be unable to deliver appropriate depth doses of radiation, and equipment such as treatment tables may have weight limitations.
One study, not yet duplicated, suggested that when lymph nodes are not removed, prognosis may be worse than whey they are, regardless of the status of those nodes. 4 While some debate this, if it is true, then failure to
sample nodes in morbidly obese women could worsen prognosis by this mechanism, as well as by failure to identify and treat metastatic cancer.
On the basis of the results of studies of the Gynecologic Oncology Group assessing pathologic factors predicting lymph node involvement in endometrial cancer, ~' 6 cur-
rent International Federation of Gynecology and Obstet- rics staging mandates surgical removal of pelvic and para- aortic lymph nodes. Even in the "ideal" case this is a controversial requirement. With no clearly proved sur- vival benefit, lymph node sampling confers potential morbidity including increased intraoperative blood loss, transfusion requirements, intraoperative complications, anesthesia time, and postoperative complications. 7 These problems are compounded in the obese person, s' 9
Because of a clinical impression that a significant num- ber of patients with endometrial cancer seen by the Gy- necologic Oncology Service of the University of Iowa Hospitals and Clinics were morbidly obese, we estab-
1171

1172 Anderson et al. April 1996 Am J Obstet Gynecol
Table I. Population characteristics: A
I Mean Range
Age (yr) 62 32-92 Gravidity 2.85 0-13 Paris, 2.5 0-11 Height (cm) 161 109-184 Weight (kg) 87 44-222 Quetelet index 34 16-89
Table II. Populat ion characteristics: B
ofpatients No. %
Height <155 cm 70 14 155-165 cm 261 53 >165 160 33
Weight <70 kg 137 28.0 70-100kg 215 44.0 >100 137 28.0
Queteletindex <30 220 45 30-40 162 33 >40 107 22
lished a database for endometr ia l cancer to test the null
hypothesis that morbid obesity has no effect on survival in
endometr ia l cancer.
Material and methods
Obesity can be measured in a number of ways for
different purposes and with differing degrees of com-
plexity of assessmenc ~~ Percentage of standard height-
weight by age in a populat ion and percentage of ideal
body weight are commonly used in the insurance indus-
try. Body density is used in sports medicine. Distribution
of body fat has significance in de termining risk for some
diseases and can have a major impact on surgical deci-
sions. Weight-height ratios are easy to calculate for large
populations but are more correctly measures of over-
weight, reflecting several tissue components including
bone and muscle in addit ion to fat. In the general popu-
lation the most accurate definition of obesity is measure-
ment of subcutaneous fat thickness.
Data from the National Health Survey of 1983 have
shown that a combinat ion of skin fold measurements and
a we igh t /he igh t ratio provides a model for estimation of
obesity and overweight) ~ Although there are differences
in these measures in the lower percentiles, those differ-
ences become less significant above the 85th percenti le
and nonexis tent in the 95th percentile. Others have also
concluded that in the absence of skin fold measurements
the most satisfactory relative weight is the Quete le t index,
also known as the body mass index. ~2 This measure is
calculated by dividing the weight in kilograms by the
square of the height in meters. As examples, an individual
5 feet 5 inches tall (165 cm) with a Quetele t index of 20
would weigh 120 pounds (54 kg). At a Quete le t index of
25 this same individual would weigh 150 pounds (68 kg).
Table I lL Tumor characteristics
No. o] patients %
Cell type Adenocarcinoma 417 85 Adenosquamous car- 41 8
cinoma Papillary serous adeno- 19 4
carcinoma Clear cell adenocar- 14 3
cinoma Grade
1 208 43 2 167 34 3 112 23
Depth of invasion None 88 18.8 Inner one third 167 35.6 Middle one third 97 20.7 Outer one third 117 24.9
Pelvic cytologic findings Negative 364 89 Positive 47 11
With a Quete le t index of 30 she would weigh 180 pounds
(82 kg), and at a Quetele t index of 40, 235 pounds (109
kg).
Because the Quete le t index is being used increasingly
in the gynecologic literature as a measure of obesity and
because of the close approximation to skin fold estimates
in the upper weight categories, we chose the Quetele t
index for the obesity measure for our analysis. We defined
obesity as a Quete le t index of >30 and morbid obesity as
>40.
Charts of all patients entered into the University of
Iowa Hospitals and Clinics Tumor Registry with uterine
cancer from Nov. 1, 1978, through Dec. 31, 1993, were
abstracted. Seven hundred two patients were identified.
Two hundred ten were excluded because of a second
primary malignancy, diagnosis of a nonepithel ial malig-
nancy (e.g., sarcoma), or no hysterectomy done. All pa-
thology results were reviewed by a gynecologic patholo-
gist, and all patients were reviewed by the Gynecologic
Oncology Tumor Board prospectively. Treatment prin-
ciples followed during this t ime included primary hyster-
ectomy for clinical stages I and III with postoperative
radiation given for myometrial invasion of greater than
one third, occult cervical involvement, or positive lymph
nodes. Vaginal brachytherapy was added for occult cervi-
cal or lower uterine segment involvement. Peritoneal
washings that contained cancer cells in the absence of
o ther high-risk factors did not usually result in treatment,
al though several patients did receive progestational
agents or intraperi toneal radioactive chromic phosphate.
Patients with clinical stage II disease were given preopera-
tive external beam pelvic radiation, and one had intra-
cavitary brachytherapy placement.
Data collected on 492 patients included age at diagno-
sis, height, weight, calculated body mass index according
to the Quete le t index, race, stage, staging method, cell

Volume 174, Number 4 Anderson et al. 1173 Am J Obstet Gynecol
Table IV. Node sampling and status
Node status
All patients
No. [ %
Quetelet index > 40
No. ] %
Sampled 313 64 38 36 Negative 278 89 36 95.2 Positive 37 12 2 4.8
Not sampled 179 36 69 64
Table V. Inf luence of grade on pe r fo rmance of lymph node sampling
Node sampling done
Grade Quetelet index <30 (%) I Quetelet index 30-40 (%) Quetelet index >40 (%)
1 70 63.5 34 2 75 75 15 3 86 73 20
Table VI. Inf luence o f myometr ial invasion on pe r fo rmance of lymph node sampling
Node sampling done
Depth of myometrial invasion
Quetelet index <30 Quetelet index 30-40 (%) (%)
Quetelet index >40 (%)
None 72 40 28 Inner one third 81.5 81 45 Middle one third 81 62.5 28.5 Outer one third 64 65 50
type, grade, node status, depth of myometrial invasion,
per i toneal cytologic results, status at last follow-up, t ime
from diagnosis to recurrence , site of recurrence, t ime
f rom recur rence to death, and t ime from diagnosis to
date o f last follow-up or to death f rom cancer or o ther
CaUSeS.
Frequency distributions were calculated for each of the
variables. Pearson's Z ~ test was used to assess the associa-
tion between categoric variables, and one-way analysis of
variance was used to compare the distributions of con-
t inuous variables.~3 The Kaplan-Meier me thod ~4 was used
to estimate survival curves, and the log-rank statistic 15 was
used to compare survival distributions. The Cox propor-
tional hazards regression modeP 6 was used to mode l the
jo in t effects of explanatory variables on survival. All sta-
tistical tests were p e r f o r m e d with the SAS system. '7
Results
Populat ion characteristics are shown in Tables I and II.
Mean age was 62 years, mean gravidity 2.85, and mean
parity 2.5. Racial distribution of patients was similar to
that of our hospital populat ion with 479 white (97.4%), 5
black (1%), 1 Hispanic (0.2%), and 7 unknown (1.4%).
Height was known in 491 patients with a mean of 161 cm.
Four teen percen t were <155 cm tall, 53% were f rom 155
to 165 crn tall, and 33% were taller than 165 cm. Weight
was known in 489 patients. Mean weight was 87 kg.
Twenty-eight percent weighed <70 kg, 44% weighed be-
tween 70 and 100 kg, and 28% weighed >100 kg. Quete le t
Table VII. Inf luence o f high-risk factors* on
node positivity
High-risk factors
Positive nodes
No. %
0 1 3 1 7 19 2 21 57 3 8 22
TOTAL 37
*Grade 2 or 3, more than one-third myometrial invasion, and stage II to IV.
index was calculated on 489 patients and ranged f rom 16
to 89 with a mean of 34. The Quete le t index was <30 in
45% of patients, 30 to 40 in 33%, and >40 in 22%.
T u m o r characteristics are shown in Table III. Histo-
logic type was adenocarc inoma in 85%, adenosquamous
carc inoma in 8%, and papillary serous or clear cell ad-
enocarc inoma in 7%. Grade 1 disease was present in 43%,
grade 2 in 34%, and grade 3 in 23%. Myometrial invasion
was measured in 469 patients (95%). No myometr ial in-
vasion was found in 19% of those measured: there was
inner one third invasion in 36%, middle one third in
21%, and outer one third in 25%. Pelvic washings were
done in 84% of all patients. Cytologic testing was negative
for mal ignant cells in 89% of those in whom washings
were taken and positive in 11%.
Lymph nodes were sampled in 313 patients (64%) and
contained cancer in 37 (12% of those sampled)

1174 Anderson et al. April 1996 Am J Obstet Gynecol
Table VIII. Staging and staging method
Surgical Clinical 7btal
% % No. [ % Stage No I No.
I 204 63 120 37 324 67 II 20 30 48 70 68 14 III 64 89 8 11 72 15 IV 17 90 2 10 19 4 TO[AL 305 63 178 37 483 100
Table IX. Complications by quetelet index
Quetelet index
<3O(%) 30-40 (%) >40 (%)
Excess blood loss 13 10 25 Wound infection or sepsis 5 13 25 Bladder or bowel laceration 3 2 3 Pneumonia 3 4 0 Small bowel obstruction 2 0 1 Phlebitis 0.5 0.6 4 Cardiac 1 0.6 1 Death 0 0.6 0
Table X. Follow-up intervals
Mean ] Median ] Range
Length of follow-up 4.6 yr 3.97 yr 14 days--15.5 yr Disease-free interval 22.5 mo 14.3 mo 41 days-11 ~a" Time from recurrence to death 22.5 mo 10 mo 0 days--10.1 yr
Table XI. Survival
Status 1 No, of patients I %
No evidence of disease 372 77 Dead of disease 74 15 Dead of other causes 36 7 Alive with disease 6 l
(Table IV). Notes were not sampled in 179 patients
(36%). In patients with a Quete le t index >40, 64% did not
have node sampling done. In the 36% of patients with a
Quete le t index >40 who had nodes sampled, 4.8% (2
patients) had lymph node metastasis. Grade and myome-
trial invasion had no influence on whether lymph node
sampling was done ei ther in the group as a whole or
within Quete le t index groups (Tables V and VI). How-
ever, grade 2 or 3, greater than one-third myometrial
invasion, and stage II to IV were high-risk factors predict-
ing node involvement when nodes were sampled (Table
VII). Seventy-nine percent of patients whose nodes were
positive had at least two high-risk factors. Only one pa-
tient had no high-risk factors.
Sixty-seven percent of 483 patients in whom staging
was done had stage I disease, 14% stage II, 15% stage III,
and 4% stage IV (Table VIII). Surgical staging was used in
the 63% of patients with sufficient available information,
and clinical staging was used in the 37% lacking complete
surgical staging information. Surgical staging was used in
Table XII. Site of recurrence I No. of Site of recurrence patients %
Vagina Alone 9 1.8 Plus abdominal and distant 7 0.2
Pelvis Alone 3 0.6 Plus abdominal and distant 4 0.8
Abdomen Alone 19 3.8 Plus distant 3 0.6
Distant alone 35 7 Abdominal and distant (TOTM.) 68 13.8
63% of patients in stage I, 30% in stage It, 89% in stage
III, and 90% in stage IV. Clinical staging was used in 37%
of patients in stage I, 70% in stage II, 11% in stage lit , and
10% in stage IV.
Surgical complications were more c o m m o n in the mor-
bidly obese group. Excess blood loss (25%), wound infec-
tion or separation (25%), and phlebitis (4%) occurred
more often than in the o ther two Quete le t index groups
(Table IX). There were no differences in the incidences
of bladder or bowel lacerations, pneumonia , small bowel
obstruction, or cardiac or o ther medical events across the
Quete le t index groups. The only postoperative death oc-
curred in a patient with a Quete le t index of 40.
Follow-up was available on 488 patients (99%), with a

Volume 174, Number 4 Arldergorl et aL 1175 Am J Obstet Gynecol
Table XIII. Recurrences by node status
Node status No.
Recurrences
All patients Quetelet index >40
No. } % Sampled 50 16 1 2.6
Negative 31 11 1 2,7 Positive 19 52 0
Not sampled 3._00 17 6 8.6 TO IAL 80 16 7 6.5
Table XIV. Inf luence of risk factors on
recur rence in node-posit ive patients
High-*isk factors*
Recurrences with positive nodes
No. [ %
0 0 0 1 2 11 2 4 21 3 13 68
TOTAl, 19 68
*Grade 2 or 3, greater than one-third myometrial invasion, stage iI to IV.
mean length of follow-up of 4.6 years and a median of
3,97 years (Table X). Disease recur red in 80 patients
(16%). In 79 patients with known date of recurrence,
disease-free survival interval ranged from 41 days to 11
years with a mean of 22.5 months and a median of 14.3
months. Time front recur rence to death ranged from 0
days to 10.1 years with a mean of 22.5 months and a
median of 10 months. Sixty-four patients (15%) were
dead of disease and 6 (1%) were alive with disease at the
t ime of the review (Table XI). Thirty-six patients (7%)
were dead of o ther causes. Disease recur red in the vagina
alone in 11 patients (11% of recurrences and 1.8% of all
cases), in the pelvis a lone in 8 (3.5% and 0.6%), in the
abdomen alone in 28 (24% and 3.8%), and in distant sites
a lone in 33 (44% and 7%) (Table XII). A total of 85.5% of
all patients had recurrences outside the t rea tment area at
a distant site, e i ther a lone or in combinat ion with local-
regional sites.
Patients with positive nodes weI'e at greater risk for
recur rence (46%) than those whose nodes were negative
(11.7%) or not sampled (17%) (Table XIII). Risk factors
for recur rence in patients with positive nodes included
grade 2 or 3, greater than one- th i rd myometr ial invasion,
and stage II to IV. Sixty-eight percent of patients with
positive nodes who had recur rence had all three risk
factors, 21% had two, 11% had one, and none had zero
risk factors (Table XIV). Patients whose nodes were not
sampled did not have a greater chance of abdominal or
distant metastasis.
A propor t ional hazards regression mode l for time from
diagnosis to death caused by disease was fit with the use of
Table XV. Factors inf luencing survival
Sigvdficance
Grade p - 0.0001 Node status p = 0.0031 Myometrial invasion p - 0.0022 Stage p = 0.0001 Height NS Qnetelet index NS (p = 0.0645) Nodes removed NS
NS, Not significant.
the covariates grade, nodes, myometr ial invasion, and
stage (Table XV). In this model the effects of grade,
myometrial invasion, and stage were highly significant. In
the model that included these variables we also evaluated
the effect of height, weight, and Quete le t index. In this
multivariate analysis there was no inf luence of he ight or
weight on survival when we control led for grade, myome-
trial invasion, stage, and node status. Significance was
approached in the relationship between Quete le t index
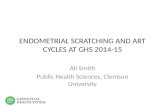
as a cont inuous variable and survival (p = 0.0645) (Fig. 1).
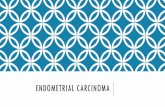
Al though patients who had lymph nodes removed had a
slightly lower hazard of death than patients with no nodes
removed, the difference was not statistically significant
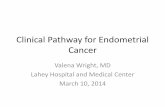
(p = 0.2045) (Fig. 2). Once disease recurred, there was no
difference in time to death on the basis of any factor
analyzed (Fig. 3).
To fur ther assess the relat ionship of obesity to progno-
sis, the relat ionship of Quete le t index to known major
prognostic factors was analyzed (Table XVI). As Quete le t
index increased, there was a decreasing chance of node
positivity with a 10.5% incidence of positive nodes when
Quete le t index was <30, 13.2% when Quete le t index was
30 to 40, and 4.8% when Quete le t index was >40, How-
ever, these differences did not achieve statistical signifi-
cance, probably because of the tact that only two patients
in the group with Quete le t index >40 had positive nodes.
Increasing height was associated with a lesser l ikel ihood
of nodes being positive (p= 0.018).
Quete le t index was strongly related to grade (p = 0.013)
and stage (p = 0.011) with heavier patients having better-
different iated tumors of lower stage. A statistically signifi-
cant association of Quete le t index to decreasing depth o f
myometrial invasion was also fbund (p = 0.018). Positive

1176 Anderson et al. April 1996 Am J Obstet Gynecol
100 90 80 70
60 50 40 30 20 10
0 I I I I I I [ i I t
0 2 yr 4 yr 6 yr 8 yr 10 yr
Fig. 1. Influence of Quetelet index on survival.
- . -<30 -0- 30-40
-*- >40
100
90 80 70 60 50
40 30 20 10
0
- . - Pos
--- Neg
- , - Not Done
I I I I I I I I I
2 yr 4 yr 6 yr 8 yr 10 yr
Fig. 2. Influence of node status on survival.
cytologic results were less likely in patients with a higher
Quetele t index (p= 0.004). Although recurrences de-
creased as Quete le t index increased, the difference was
not statistically significant. Time to recurrence was signifi-
cantly increased as Quete le t index increased (p = 0.0136).
Survival also increased as Quete le t index increased, al-
though it was not statistically significant.
Although patients with Qnete le t index <30 were some-
what more likely to have papillary serous or clear cell
histologic types than were those with Quetele t index >40
(8.7% vs 4.6%), the difference in proport ions was not
significant (p = 0.129) (Table XVII).
Qnete le t index was known in 79 patients with recur-
rence and was <30 in 42 patients (53% of recurrences and
19% of patients in this group), 30 to 40 in 28 patients
(35% and 17%), and >40 in 9 patients (12% and 8%). In
36 patients dead of o ther causes, Quete le t index was <30
in 12 patients (34% of those dead of o ther causes and
5.5% of patients in this group), 30 to 40 in 15 patients
(41% and 9.3%), and >40 in 9 patients (24% and 8.4%).
Age had no influence on survival when patients were
grouped into age <55, 55 to 65, and >65. In addition there
was no difference in survival among these age groups
when viewed by Quete le t index groups <30, 30 to 40, >40.
Comment
The mechanism by which obesity is thought to increase
the risk of endometr ia l cancer is through increased levels
of serum estrogen unopposed by progesterone. This re-
sults f rom both anovulation with peripheral storage of
estrogen in fat deposits and from conversion of adrenal
andros tenedione to estrone by aromatase in fat. TM Serum
estrone and estradiol, but not androstenedione, have
been significantly correlated with body mass index
among women with endometr ia l carcinoma compared
with controlsJ Upper-body fat localization has been iden-
tified as a significant risk factor for endometr ia l cancer in
women matched for age and Quetele t index. 1~' However, a
prospective population-based assessment of women in
the Iowa Women 's Health Study concluded that endome-
trial cancer risk is increased in relation to the amount but
not the distribution of adiposity. '-'~
Most studies assessing obesity and endometr ia l carci-
noma have grouped patients by categories of equal num-
bers of individuals in quartiles or quintiles. A prospective
assessment of the relationship of incidence of endome-
trial carcinoma and body mass index found a two to three
times greater relative risk for women in the 5th body mass
index quintile of a populat ion of 570,000 women. ~ How-

Volume 174, Number 4 Anderson et al. 1177 Am J Obstet Gynecol
100% 90% 80% 70% 60% 60% 40% 30% 20% 10%
0%
0 yr
l r I I I I ] I
2 yr 4 yr 6 yr 8 yr I I
10 yr
Fig. 3. Survival after recurrence.
Table XVI. Inf luence of Quete le t index: A
Increasing Quetelet index Significance
Grade Decreased p = 0.013 Stage Decreased p = 0.011 Depth of myometrial invasion Decreased p = 0.018 Positive cytologic findings Decreased p = 0.004 Recurrence Decreased NS Time to recurrence Increased p = 0.0136 Survival Increased p = 0.0645
NS, Not significant.
Table XVII. Inf luence of Quete le t index: B
Factor
@tetelet index
< 3 0 ( % ) 1 3 0 - 4 0 ( % ) ] >40(%) &gnifieanee
Papillary serous or clear cell histologic type 8.6 5 4.6 NS Positive nodes 10.5 13.2 4.8 NS Recurrence 19 17 8 NS Dead of other causes 5.5 9.3 8.4 NS
NS, Not significant.
ever, in this study the 5th Quete le t index quinti le began at
only 25 at age 30 to 34 and rose to 31 at age 65 to 69. In
ano the r study only 20% of patients had a body mass index
of >28 (5 feet 5 inches tall, 167 pounds ) J
The cur ren t study is the first to include sufficient pa-
tients in the h igher reaches of the Quete le t index to
provide statistically significant data. In this study the
Quete le t index in 55% of patients was >30, a commonly
used cutoff for obesity, and >40 in 22%. In this morbidly
obese group the prognosis was not compromised but was
actually bet ter than in the less obese or even slender
patients. The rate of comorb id diseases was similar in all
groups. T ime- to - recur rence rates were longer in the
obese groups. The explanat ion for improved prognosis
appears to be the significant tendency for less aggressive
disease as indicated by the h igher incidence of better-
differentiated, less-invasive adenocarc inomas with less-
f requen t lymph node metastases and fewer positive pelvic
washings. This is suppor ted by the observation that estro-
gen- induced cancers in women taking exogenous estro-
gen have a better prognosis because of the greater likeli-
hood of well-differentiated tumors. ~
This study does not support the view that removal of
lymph nodes has a beneficial effect on prognosis whether
those nodes do or do not contain metastatic disease. The
small difference could be accounted for by assuming that
a small p ropor t ion of those nnsampled nodes had un-
identif ied and therefore unt rea ted metastases.
Our data also have implications for the possibility of
laparoscopic managemen t of these patients. Proponents
of laparoscopic surgical staging have r e c o m m e n d e d limi-
tation of the procedure to individuals whose body mass
index is <30. ''~ This would exclude more than half (55%)
of our patients. Whether this is true in o ther populat ions
remains to be seen. In laparotomy for lymph node sam-
piing weight has been a l imiting factor in o ther reports,
with a median weight of 69 kg for those having nodes
sampled compared with a median weight of 74.9 kg for

1178 Anderson et al. April 1996 AmJ Obstet Gynecol
those without sampling. 7 In our study the median weight
of the entire group was 87 kg. Those who had nodes
sampled had a median weight of 76 kg compared with 94
kg in those without sampling. These differences of 7 and
20 kg in each group may represent regional variations but
must be taken into account when recommendat ions for
surgical procedures are made.
A correlated finding was the tendency toward the pres-
ence of poor prognostic factors in individuals with a
Quetele t index of <30 compared with those having a
Quete le t index of ei ther 30 to 40 or >40. This may repre-
sent the existence of two biologically different variants of
endometr ia l carcinoma appearing in two phenotypically
different groups.
We conclude that morbid obesity (Quetelet index >40)
in endometr ia l cancer has a positive effect on survival in
endometr ia l cancer through its association with less ag-
gressive disease. Thinness is associated with more aggres-
sive disease. Lymph node sampling adds more important
information in the thin patient than in the morbidly
obese. Lack of node sampling does not adversely affect
survival. Because lymph node sampling in the obese pa-
tient is a potentially morbid procedure, its use should be
confined to those patients who will benefi t as a result of
the knowledge gained. As has been noted previously,
node positivity and overall prognosis are best predicted
by grade and depth of myometrial invasion. Because little
useful information is added in the morbidly obese, lymph
node sampling should be limited to only those with
higher*grade and more deeply invasive disease, avoiding
fur ther treatment-related complications in the morbidly
obese.
REFERENCES
1. Tretli S, Magnus K. Height and weight in relation to uterine corpus cancer morbidity and mortality: a follow-up study of 570,000 women in Norway. IntJ Cancer 1990;46:165-72.
2. Austin H, AustinJM, Partridge EE, et al. Endometrial cancer, obesity and body fat distribution. Cancer Res 1991;51:568- 72.
3. Tornberg SA, Carstensen JM. Relationship between Quete- let's index and cancer of breast and female genital tract in 47,000 women followed for 25 years. BrJ Cancer 1994;69: 358-61.
4. Kilgore LC, Partridge EE, Alvarez RD, et al. Adenocarci- noma of the endometrium: survival comparisons of patients with and without pelvic node sampling. Gynecol Onco11995; 56:29-33.
5. Boronow RC, Morrow CE Creasman WT, et al. Surgical staging in endometrial carcinoma: clinico-pathologic find- ings of a prospective study. Obstet Gynecol 1984;63:825-32.
6. Morrow CP, Bundy BN, Kurman R l, et al. ReIationship be- tween surgicakpathologic risk factors and outcome in clini- cal stage I and lI carcinoma of the endometrium: a Gyneco- logic Oncology Group Study. Gynecol Oncol 1991;40:55-65.
7. Cliby WA, Clarke-Pearson DL, Dodge R, et al. Acute morbid- ity and mortality associated with selective pelvic and para- aortic lymphadenectomy in the surgical staging of endome- trial adenocarcinoma. J Gynecol Tech 1995;1:19-26.
8. Pitkin RM. Abdominal hysterectomy in obese women. Surg Gynecol Obstet 1976;142:532-36.
9. Foley K, Lee RB. Surgical complications of obese patients with endometrial carcinoma. Gynecol Oncol 1990;39:171-4.
10. Keys A, Fidanza F, Karvonen M], et al. Indices of relative weight and obesity.J Chron Dis 1972:25:329-43.
11. National Center for Health Statistics. Obese and overweight adults in the United States. Washington: US Government Printing Office, 1983; National Health Survey series 1 I, no 230; DHHS publication no (PHS) 83-1680.
12. Thomas AE, McKey DA, Cutiip MB. A nomograph method for assessing body weight. AmJ Clin Nutr 1976;29:302-4.
13. Rosner B. Fundamentals of biostatistics. Behnont, California: Wadsworth, 1995.
14. Kaplan EL, Meier P. Nonparametric estimation from incom- plete observations. J Am Star Assoc 1958;53:457-81.
15. Mantel N. Evaluation ofsurvival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 1966; 50:163-70.
16. Cox DR. Regression models and life tables (with disc ussion). J R Star Soc B 1972;34:187-220.
17. SAS Institute. SAS/STAT guide for personal computers, ver- sion 6 edition. Cary, North Carolina: SAS Institute, 1987.
18. ElwoodJM, Cole E Rothman K, et al. Epidemiology of en- dome trial cancer. J Natl Cancer Inst 1977;59:1055-60.
19. Schapira DV, Kumar NB, Lyman GH, et al. Upper-body fat distribution and endometrial cancer risk. JAMA 1991;266: 1808-11.
20. Folsom AR, Kaye SA, PonerJD, et al. Association of incident carcinoma of the endometrium with body weight and fat distribution in older women: early findings of the Iowa Wom- en's Health Study. Cancer Res 1989;49:6828-31.
21. Hulka BS, Kaufman DG, Fowler WC, et al. Predominance of early endometrial cancer after long-term estrogen use. .lAMA 1980;244:2419-22.
22. Childers JM, Hatch KD, Tran A-N, et aI. Obstet GynecoI 1993;82:741-7.
Discussion
Dl~ HOWARD W. JoNEs III, Nashville, Tennessee. Dr. Anderson and her colleagues are to be congratulated on the excel lent results they have achieved in a less than ideal patient population. In several large studies only about 20% of the patients had a Quete le t or body mass index of >30. However, in the Iowa series of women with endometr ia l cancer 55% of the patients were classified as obese with a Quete le t index of >30. Although obesity is a well-known risk factor for the development of endometr ia l cancer, the effect of overweight on prognosis or survival has not been previously studied. Al though Dr. Anderson 's study found that "calorically chal lenged" women tend to have a better survival, obesity per se did not affect prognosis.
In 1967 Dr. Leo Dunn and Dr.James Bradbury] at that t ime members of the faculty at The University of Iowa College of Medicine, identified obesity as a common characteristic in their studies of the endocr ine factors associated with endometr ia l cancer. It has been well shown that estrogen-treated women in whom endome- trial cancer develops have a favorable prognosis. ~ There- fore, if we hypothesize that endometr ia l cancer develops more commonly in obese women because of increased peripheral conversion and storage o f endogenous estro- gens in adipose tissue, then we might expect that obese women would also have a good prognosis and higher incidence of well-differentiated, early-stage cancers. This is what Dr. Anderson has shown.
Because patients with endometr ia l cancer tend to have excellent survival rates, there is increasing pressure from

Volume 174, Number 4 Aflderson ot al. 1179 Am J Obstet Gynecol
third-party payors to "treat these patients at home," with primary gynecologists to manage their care and do their surgery. It is therefore most helpful to examine all the clinical risk factors so that "high-risk" characteristics can be identified to help the primary care provider select those women at increased risk who should definitely be referred to a gynecologic oncologist.
So the question is, "Axe obese women at high risk or low risk?" Although their outcome is generally good, obese patients, especially morbidly obese women, are at increased risk for complications and often present a tech- nical challenge for the surgeon or radiation oncologist. Therefore, because of the operative difficulties that may be anticipated, obese patients with endometrial cancer are probably best managed by gynecologic oncologists.
However, in their analysis of prognostic characteristics, Dr. Anderson and her colleagues have omitted an impor- tant prognostic factor--treatment. For example, obese women seem to have generally favorable prognostic fac- tors, and therefore a low incidence of postoperative pel- vic radiation is found in this group. If postoperative ra- diation is effective and is used predominantly in non- obese women, this selective treatment might improve the survival of nonobese patients, thus obscuring a real dif- ference in survival between obese and nonobese women. Why did you decide not to include treatment in your proportional hazards regression analysis of prognostic factors?
I will also comment on the value, or lack of value, of selective pelvic and /o r paraaortic Iymphadenectomy in the management of endometrial cancer. To begin, there is no definition of the technique to be used. How thor- ough a dissection should be done? Clearly, the number of nodes removed and the pathologic sectioning of these nodes will greatly influence the incidence of nodal me- tastases identified, but nowhere is the recommended technique specified. And which patients should undergo staging lymphadenectomy? Several studies, including a recent study by Cliby et al. ~ from Duke University School of Medicine, have demonstrated an increased risk of complications associated with "selective lymphadenec- tomy." Not only is there an increased risk of complica- tions, but the therapeutic value of this procedure remains in doubt. In a recent study from the University of Ala- bama, Kilgore et a l . 4 reported improved survival ibr pa- tients who had a thorough staging lymphadenectomy compared with patients who did not. On the other hand, in this study from Iowa and others ~' ~ there appears to be no survival benefit to lymphadenectomy. The reason for these different results is undoubtedly related to patient selection and different surgical techniques from one institution to another. Perhaps it is time for the Inter- national Federation of Gynecology and Obstetrics to define more precisely the technique and the patients in whom staging lymphadenectomy is indicated. My final question for Dr. Anderson is, "As a result of this study, have you modified your indications for staging lyin- phadenectomy to exclude obese patients?"
REFERENCES
1. Dunn LJ, Bradbury JT. Endocrine factors in endometrial carcinoma: a preliminary report. A~LJ O~STET G'mEcot 1967; 97:465-71.
2. Hulka BS, Kaufman DG, Fowler WC, et al. Predominance of early endometrial cancer after long-term estrogen use.JAMA 1980;244:2419-22.
3. Cliby WA, Clarke-Pearson DL, Dodge R, et al. Acute morbidity and mortality associated with selective pelvic and para-aortic lymphadenectomy in the surgical staging of endometrial adenocarcinoma. J Gynecol Tech 1995; 1:19-26.
4. Kilgore LC, Partridge EE, Alvarez RD, et al. Adenocarcinoma of the endometrimn: survival comparison of patients with and without pelvic node sampling. Gynecol Oncol 1995;56:29-33.
5. BelinsonJL, Lee KR, Badger GJ, et al. Clinical stage I adeno- carcinoma of the endometrium--analysis of recurrences and the potential benefit of staging lymphadenectomy. Gynecol Oncol 1992;44:17-23.
6. Kim ~ , NiloffJM. Endometrial carcinoma: analysis of recur- rence in patients treated with a strategy minimizing lymph node sampling and radiation therap}: Obstet Gynecol 1993; 82:175-80.
DI~ A~mERSON (Closing). We did not include treatment in our analysis because it was dependent on the observed risk factors of grade, depth ofmyometrial invasion, lymph node involvement, extent of disease, and histologic type. Our standard of care was to treat all patients with those high-risk factors regardless of weight or body hahitus. I think you're absolutely right that the reason that the obese patients did better was because they had lower-risk disease.
Of interest, the two patients in the morbidly obese group who did have positive nodes both had high-risk factors predicting that presence. They both had deep myometrial invasion (onter third by our definition) and grade 2 or 3 disease. Both received postoperative pelvic radiation, and neither had recurrence of disease.
Our surgical technique was a selective lymphadenec- tomy. We have not changed our overall approach to choosing candidates for lymphadenectomy on the basis of the data presented. We have followed the findings of Gynecologic Oncology Group Protocol No. 33, and any changes have been on the basis of those data. The find- ings of the study presented do make us feel better about patients in whom we are technically unable to obtain lymph nodes. I do think, however, that it's very important to try to get lymph nodes, even in these large patients, when high-risk factors are present. We recently had an- other morbidly obese patient outside this study in whom we removed pelvic and paraaortic tissue. We did not think there were any nodes present. We were surprised that every sample contained nodes and all nodes contained metastatic disease. This emphasizes the difficulty of rely- ing on palpation as a guide to node positivity, both in general and particularly in the morbidly obese. These patients are a challenge.
I agree completely that nodal data may have little effect on prognosis when all other factors are considered. These data help us identify patients for whom we can safely exclude lymphadenectomy.