
Nonhuman Primates in Biomedical Research || Xenotransplantation
12
Chapter 16 Xenotransplantation David K.C. Cooper* and Robert Wagner y * Thomas E. Starzl Transplantation Institute, University of Pittsburgh, Pittsburgh, PA, USA, y Division of Laboratory Animal Resources, University of Pittsburgh, Pittsburgh, PA, USA Chapter Outline Introduction 391 The Pig as a Potential Source of Organs/Cells for Clinical Transplantation 391 The Significance of Gal Antigen Expression in Pigs 391 History 392 Pathobiology of Pig-To-Primate Organ Transplantation 393 The Innate Immune Response 393 Coagulation Dysfunction 393 The Adaptive Immune Response 393 The Pig-to-Nonhuman Primate Model 393 Intravascular Catheter Placement and Fluid/Drug Administration 393 Immunosuppressive Therapy 396 Results and Complications 397 Results 397 Complications 397 Genetic Modification of Pigs 399 Summary 400 Acknowledgments 400 References 400 INTRODUCTION Organ allotransplantation (alloTx) for patients with end- stage organ failure was one of the success stories of the second half of the twentieth century. One of the major limitations of this form of surgical therapy is the shortage of suitable donor organs, which are largely from deceased humans. Furthermore, during the past decade, islet alloTx for the treatment of type 1 diabetes has become moderately successful, but the shortage of suitable pancreata from deceased humans has limited this form of therapy to less than 1000 of the estimated 2 million type 1 diabetics in the USA during the past decade. In an effort to resolve the problem of shortage of organs and cells, increasing atten- tion has been directed towards an exploration of the use of animals as potential sources of tissues for clinical transplantation. The Pig as a Potential Source of Organs/ Cells for Clinical Transplantation Xenotransplantation (xenoTx), or the transplantation of organs, tissues, or cells across species barriers, has some- times been divided into the transplantation of organs between concordant or discordant species. Concordant species, e.g., monkey-to-baboon, are those in which, following an organ transplant, hyperacute rejection does not commonly occur, whereas discordant species, e.g. pig- to-baboon, are those in which hyperacute rejection is almost universal. Despite the problem of hyperacute rejection, for a number of logistic and ethical reasons (reviewed in Cooper and Lanza, 2000 and Cooper et al., 2002)(Table 16.1), the pig has been determined to be the most suitable source of such organs, tissues, or cells for clinical use. Almost all research of direct clinical relevance today is being carried out in pig-to-nonhuman primate models, although in vitro and small animal studies continue to play important roles in providing initial data. The Significance of Gal Antigen Expression in Pigs Studies in the 1990s determined that, when the recipient was a nonhuman primate or human, hyperacute rejection was largely related to the expression in pigs of a carbohy- drate antigen, Gala1,3Gal (Gal) (Cooper, 1992; Cooper et al., 1993; Oriol et al., 1993), which is not present in Old World nonhuman primates and humans (Galili, 1988). As a result of its absence in these species, they develop natural Nonhuman Primates in Biomedical Research. DOI: 10.1016/B978-0-12-381365-7.00016-9 Copyright Ó 2012 Elsevier Inc. All rights reserved. 391
Transcript of Nonhuman Primates in Biomedical Research || Xenotransplantation

Chapter 16
Xenotransplantation
David K.C. Cooper* and Robert Wagnery*Thomas E. Starzl Transplantation Institute, University of Pittsburgh, Pittsburgh, PA, USA, yDivision of Laboratory Animal Resources,
University of Pittsburgh, Pittsburgh, PA, USA
No
Co
Chapter Outline
Introduction 391
The Pig as a Potential Source of Organs/Cells for Clinical
Transplantation 391
The Significance of Gal Antigen Expression in Pigs 391
History 392
Pathobiology of Pig-To-Primate Organ Transplantation 393
The Innate Immune Response 393
Coagulation Dysfunction 393
The Adaptive Immune Response 393
The Pig-to-Nonhuman Primate Model 393
nhuman Primates in Biomedical Research. DOI: 10.1016/B978-0-12-381365-7.00016-9
pyright � 2012 Elsevier Inc. All rights reserved.
Intravascular Catheter Placement and Fluid/Drug
Administration 393
Immunosuppressive Therapy 396
Results and Complications 397
Results 397
Complications 397
Genetic Modification of Pigs 399
Summary 400
Acknowledgments 400
References 400
INTRODUCTION
Organ allotransplantation (alloTx) for patients with end-stage organ failure was one of the success stories of thesecond half of the twentieth century. One of the majorlimitations of this form of surgical therapy is the shortageof suitable donor organs, which are largely from deceasedhumans. Furthermore, during the past decade, islet alloTxfor the treatment of type 1 diabetes has become moderatelysuccessful, but the shortage of suitable pancreata fromdeceased humans has limited this form of therapy to lessthan 1000 of the estimated 2 million type 1 diabetics in theUSA during the past decade. In an effort to resolve theproblem of shortage of organs and cells, increasing atten-tion has been directed towards an exploration of the useof animals as potential sources of tissues for clinicaltransplantation.
The Pig as a Potential Source of Organs/Cells for Clinical Transplantation
Xenotransplantation (xenoTx), or the transplantation oforgans, tissues, or cells across species barriers, has some-times been divided into the transplantation of organsbetween concordant or discordant species. Concordant
species, e.g., monkey-to-baboon, are those in which,following an organ transplant, hyperacute rejection doesnot commonly occur, whereas discordant species, e.g. pig-to-baboon, are those in which hyperacute rejection isalmost universal. Despite the problem of hyperacuterejection, for a number of logistic and ethical reasons(reviewed in Cooper and Lanza, 2000 and Cooper et al.,2002) (Table 16.1), the pig has been determined to be themost suitable source of such organs, tissues, or cells forclinical use. Almost all research of direct clinical relevancetoday is being carried out in pig-to-nonhuman primatemodels, although in vitro and small animal studies continueto play important roles in providing initial data.
The Significance of Gal Antigen Expressionin Pigs
Studies in the 1990s determined that, when the recipientwas a nonhuman primate or human, hyperacute rejectionwas largely related to the expression in pigs of a carbohy-drate antigen, Gala1,3Gal (Gal) (Cooper, 1992; Cooperet al., 1993; Oriol et al., 1993), which is not present in OldWorld nonhuman primates and humans (Galili, 1988). Asa result of its absence in these species, they develop natural
391
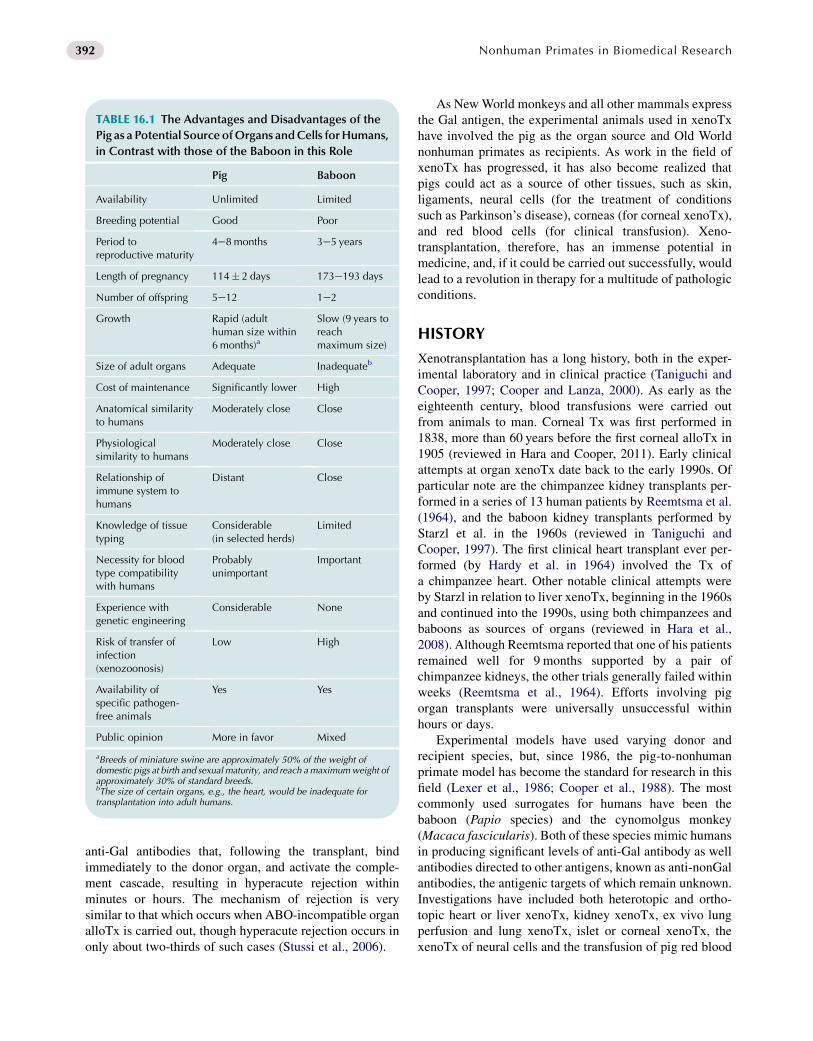
TABLE 16.1 The Advantages and Disadvantages of the
Pig as a Potential SourceofOrgans andCells forHumans,
in Contrast with those of the Baboon in this Role
Pig Baboon
Availability Unlimited Limited
Breeding potential Good Poor
Period toreproductive maturity
4e8months 3e5 years
Length of pregnancy 114� 2 days 173e193 days
Number of offspring 5e12 1e2
Growth Rapid (adulthuman size within6months)a
Slow (9 years toreachmaximum size)
Size of adult organs Adequate Inadequateb
Cost of maintenance Significantly lower High
Anatomical similarityto humans
Moderately close Close
Physiologicalsimilarity to humans
Moderately close Close
Relationship ofimmune system tohumans
Distant Close
Knowledge of tissuetyping
Considerable(in selected herds)
Limited
Necessity for bloodtype compatibilitywith humans
Probablyunimportant
Important
Experience withgenetic engineering
Considerable None
Risk of transfer ofinfection(xenozoonosis)
Low High
Availability ofspecific pathogen-free animals
Yes Yes
Public opinion More in favor Mixed
aBreeds of miniature swine are approximately 50% of the weight ofdomestic pigs at birth and sexual maturity, and reach amaximumweight ofapproximately 30% of standard breeds.bThe size of certain organs, e.g., the heart, would be inadequate fortransplantation into adult humans.
392 Nonhuman Primates in Biomedical Research
anti-Gal antibodies that, following the transplant, bindimmediately to the donor organ, and activate the comple-ment cascade, resulting in hyperacute rejection withinminutes or hours. The mechanism of rejection is verysimilar to that which occurs when ABO-incompatible organalloTx is carried out, though hyperacute rejection occurs inonly about two-thirds of such cases (Stussi et al., 2006).
As NewWorld monkeys and all other mammals expressthe Gal antigen, the experimental animals used in xenoTxhave involved the pig as the organ source and Old Worldnonhuman primates as recipients. As work in the field ofxenoTx has progressed, it has also become realized thatpigs could act as a source of other tissues, such as skin,ligaments, neural cells (for the treatment of conditionssuch as Parkinson’s disease), corneas (for corneal xenoTx),and red blood cells (for clinical transfusion). Xeno-transplantation, therefore, has an immense potential inmedicine, and, if it could be carried out successfully, wouldlead to a revolution in therapy for a multitude of pathologicconditions.
HISTORY
Xenotransplantation has a long history, both in the exper-imental laboratory and in clinical practice (Taniguchi andCooper, 1997; Cooper and Lanza, 2000). As early as theeighteenth century, blood transfusions were carried outfrom animals to man. Corneal Tx was first performed in1838, more than 60 years before the first corneal alloTx in1905 (reviewed in Hara and Cooper, 2011). Early clinicalattempts at organ xenoTx date back to the early 1990s. Ofparticular note are the chimpanzee kidney transplants per-formed in a series of 13 human patients by Reemtsma et al.(1964), and the baboon kidney transplants performed byStarzl et al. in the 1960s (reviewed in Taniguchi andCooper, 1997). The first clinical heart transplant ever per-formed (by Hardy et al. in 1964) involved the Tx ofa chimpanzee heart. Other notable clinical attempts wereby Starzl in relation to liver xenoTx, beginning in the 1960sand continued into the 1990s, using both chimpanzees andbaboons as sources of organs (reviewed in Hara et al.,2008). Although Reemtsma reported that one of his patientsremained well for 9 months supported by a pair ofchimpanzee kidneys, the other trials generally failed withinweeks (Reemtsma et al., 1964). Efforts involving pigorgan transplants were universally unsuccessful withinhours or days.
Experimental models have used varying donor andrecipient species, but, since 1986, the pig-to-nonhumanprimate model has become the standard for research in thisfield (Lexer et al., 1986; Cooper et al., 1988). The mostcommonly used surrogates for humans have been thebaboon (Papio species) and the cynomolgus monkey(Macaca fascicularis). Both of these species mimic humansin producing significant levels of anti-Gal antibody as wellantibodies directed to other antigens, known as anti-nonGalantibodies, the antigenic targets of which remain unknown.Investigations have included both heterotopic and ortho-topic heart or liver xenoTx, kidney xenoTx, ex vivo lungperfusion and lung xenoTx, islet or corneal xenoTx, thexenoTx of neural cells and the transfusion of pig red blood

393Chapter | 16 Xenotransplantation
cells. A more recent introduction is pig artery patch xeno-grafting, which is much simpler than an entire organtransplant, yet which is susceptible to the same immuneresponse.
PATHOBIOLOGY OF PIG-TO-PRIMATEORGAN TRANSPLANTATION
The Innate Immune Response
When the pig organ is unmodified, i.e., not geneticallymodified, and no immunosuppressive therapy is given to therecipient, hyperacute rejection occurs in the majority ofcases (Figure 16.1A) (Rose et al., 1991; Rose and Cooper,1996, 2000). Hyperacute rejection has been defined asantibody-mediated complement activation, leading todestruction of the graft within 24 hours; it frequently occurswithin the first hour. It is known to be associated with thebinding of anti-Gal IgM to the Gal epitopes on the pig organ,with activation of the complement cascade. However, it hasbeen described after the use of organs from pigs in which theGal antigen is not expressed (a1,3-galactosyltransferasegene-knockout [GTKO] pigs), and therefore can be initiatedby binding of anti-nonGal antibodies.
If hyperacute rejection is prevented, either by a geneticmanipulation of the pig, or by immunoadsorption of anti-pig antibodies from the recipient, acute humoral xenograftrejection (sometimes known as acute vascular rejection ordelayed xenograft rejection), usually develops within days.This is again usually associated with antibody binding andcomplement activation, but there is probably a greater roleof innate immune cells, such as neutrophils and macro-phages, but the end result is largely the same (Ezzelarab2009).
Coagulation Dysfunction
In both these phenomena, it is increasingly clear thatabnormal coagulation within the vessels of the graft playsa significant role, and this may well be associated withmolecular incompatibilities between the pig and primatewith regard to the coagulation systems (Bach et al., 1994;Robson et al., 2000; Chen and Dorling, 2005). Forexample, pig tissue factor pathway inhibitor does notsuccessfully inhibit primate factor Xa, pig thrombomodulindoes not catalyze primate protein C, and pig von Wille-brand factor is associated with excessive primate plateletaggregation.
Even if early rejection is avoided, these incompatibili-ties can result in the development of a thrombotic micro-angiopathy, in which the vasculature of the organ is steadilyoccluded by thrombus, resulting in ischemic necrosis ofthe tissues (Figure 16.1B) (Houser et al., 2004). Theconsumption of clotting factors in this process can lead to
a consumptive coagulopathy in the nonhuman primaterecipient.
The Adaptive Immune Response
If both hyperacute and acute humoral xenograft rejectionare prevented, but immunosuppressive therapy is inade-quate, there is likely to be a T-cell-dependent elicitedantibody response, resulting in high levels of anti-pig IgG(Dorling and Lechler, 1998; Mirenda et al., 2005). Bindingof these antibodies to the vascular endothelium initiateshistopathological changes indistinguishable from acutehumoral xenograft rejection. Surprisingly, acute cellularrejection, as seen in the majority of allotransplants, hasvirtually never been recorded after pig-to-nonhumanprimate organ xenoTx. This is most likely because thehumoral response overwhelms the cellular response,though T and B cells may well be seen in the graft.
In pig heart grafts that have survived for more thanapproximately 3 months, graft vasculopathy develops(Figure 16.1C) (Kuwaki et al., 2005; Tseng et al., 2005), asseen in human allografts that have survived for manymonths or years (chronic rejection). This form of chronicrejection is as poorly understood in xenoTx as it is inalloTx.
With the introduction of genetically engineered pigs thatare partially resistant to the primate antibody-mediatedresponse, it is becoming clear that the coagulation dysfunc-tion between the two species is playing an increasing role.Indeed, aberrant coagulation may be a muchmore importantcausative factor in the development of acute humoral xeno-graft rejection than previously anticipated (Chen et al.,2004). However, it is likely that it is initiated by immunefactors, such as antibody binding to the vascular endothe-lium, leading to endothelial activation (Bach, 1994).
THE PIG-TO-NONHUMAN PRIMATEMODEL
The pig-to-nonhuman primate model is very demandingand requires considerable resources in both personneland facilities. In the majority of cases, a tether system isused to enable indwelling intravascular catheters to beavailable throughout the course of the experiment formonitoring blood pressure, blood draws, and drug infusion(e.g., inotropic or immunosuppressive agents) (Figure 16.2)(Cooper et al., 1994).
Intravascular Catheter Placement andFluid/Drug Administration
At operation, under full inhalational anesthesia, Tygoncatheters are placed in the carotid artery and jugular veins

FIGURE 16.1 Summary of the known immunologic barriers to pig-to-primate heart transplantation. (Reproduced with permission from Zhu X et al.,
J Heart Lung Transplant 2007;26:210e218.)
394 Nonhuman Primates in Biomedical Research
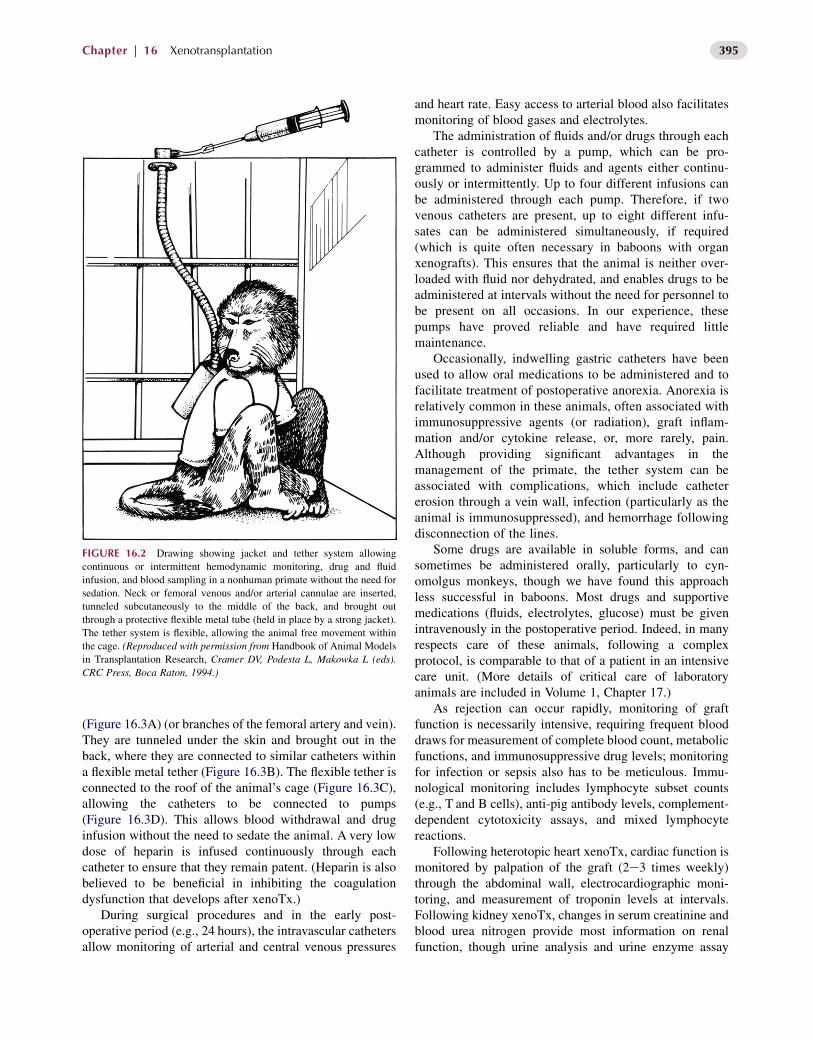
FIGURE 16.2 Drawing showing jacket and tether system allowing
continuous or intermittent hemodynamic monitoring, drug and fluid
infusion, and blood sampling in a nonhuman primate without the need for
sedation. Neck or femoral venous and/or arterial cannulae are inserted,
tunneled subcutaneously to the middle of the back, and brought out
through a protective flexible metal tube (held in place by a strong jacket).
The tether system is flexible, allowing the animal free movement within
the cage. (Reproduced with permission from Handbook of Animal Models
in Transplantation Research, Cramer DV, Podesta L, Makowka L (eds).
CRC Press, Boca Raton, 1994.)
395Chapter | 16 Xenotransplantation
(Figure 16.3A) (or branches of the femoral artery and vein).They are tunneled under the skin and brought out in theback, where they are connected to similar catheters withina flexible metal tether (Figure 16.3B). The flexible tether isconnected to the roof of the animal’s cage (Figure 16.3C),allowing the catheters to be connected to pumps(Figure 16.3D). This allows blood withdrawal and druginfusion without the need to sedate the animal. A very lowdose of heparin is infused continuously through eachcatheter to ensure that they remain patent. (Heparin is alsobelieved to be beneficial in inhibiting the coagulationdysfunction that develops after xenoTx.)
During surgical procedures and in the early post-operative period (e.g., 24 hours), the intravascular cathetersallow monitoring of arterial and central venous pressures
and heart rate. Easy access to arterial blood also facilitatesmonitoring of blood gases and electrolytes.
The administration of fluids and/or drugs through eachcatheter is controlled by a pump, which can be pro-grammed to administer fluids and agents either continu-ously or intermittently. Up to four different infusions canbe administered through each pump. Therefore, if twovenous catheters are present, up to eight different infu-sates can be administered simultaneously, if required(which is quite often necessary in baboons with organxenografts). This ensures that the animal is neither over-loaded with fluid nor dehydrated, and enables drugs to beadministered at intervals without the need for personnel tobe present on all occasions. In our experience, thesepumps have proved reliable and have required littlemaintenance.
Occasionally, indwelling gastric catheters have beenused to allow oral medications to be administered and tofacilitate treatment of postoperative anorexia. Anorexia isrelatively common in these animals, often associated withimmunosuppressive agents (or radiation), graft inflam-mation and/or cytokine release, or, more rarely, pain.Although providing significant advantages in themanagement of the primate, the tether system can beassociated with complications, which include cathetererosion through a vein wall, infection (particularly as theanimal is immunosuppressed), and hemorrhage followingdisconnection of the lines.
Some drugs are available in soluble forms, and cansometimes be administered orally, particularly to cyn-omolgus monkeys, though we have found this approachless successful in baboons. Most drugs and supportivemedications (fluids, electrolytes, glucose) must be givenintravenously in the postoperative period. Indeed, in manyrespects care of these animals, following a complexprotocol, is comparable to that of a patient in an intensivecare unit. (More details of critical care of laboratoryanimals are included in Volume 1, Chapter 17.)
As rejection can occur rapidly, monitoring of graftfunction is necessarily intensive, requiring frequent blooddraws for measurement of complete blood count, metabolicfunctions, and immunosuppressive drug levels; monitoringfor infection or sepsis also has to be meticulous. Immu-nological monitoring includes lymphocyte subset counts(e.g., T and B cells), anti-pig antibody levels, complement-dependent cytotoxicity assays, and mixed lymphocytereactions.
Following heterotopic heart xenoTx, cardiac function ismonitored by palpation of the graft (2e3 times weekly)through the abdominal wall, electrocardiographic moni-toring, and measurement of troponin levels at intervals.Following kidney xenoTx, changes in serum creatinine andblood urea nitrogen provide most information on renalfunction, though urine analysis and urine enzyme assay

(A) (B)
(C) (D)
FIGURE 16.3 (A) With the baboon lying supine, with the head turned slightly to the left (under the towel at the left of the figure), the right carotid artery
and internal jugular vein have been identified and isolated. The external jugular vein is isolated separately (not shown), and all three vessels are can-
nulated. (B) The three catheters are tunneled subcutaneously and brought out through the skin of the back, where they are attached to similar catheters
within the flexible metal tether (lower right in figure). The catheters are securely sutured to the skin to ensure they do not protrude below the jacket. (C)
When the baboon is returned to the cage, the tether is connected to the roof of the cage, and (D) the three catheters connected to pumps. (Courtesy of
Burcin Ekser, MD.)
396 Nonhuman Primates in Biomedical Research
(particularly gamma glutamyltransferase [GGT]) can behelpful. In addition, ultrasound studies have been founduseful in determining whether the heart remains contract-ing, or whether blood flow persists through the heart orkidney. Liver function after xenoTx can be monitored byfrequent measurement of protein synthesis, detoxification,and coagulation. (Pre-Tx liver failure in the nonhumanprimate can be induced by a variety of toxins [aflatoxins,alcohol, D-galactosamine] or radiation, although nativehepatectomy often suffices for the needs of the experi-ment.) In all cases, tissue biopsies are carried out atintervals, either through an open operative procedure ofby percutaneous transvenous (heart) or percutaneousfine needle (kidney or liver) techniques; these biopsyprocedures can all be associated with complications,particularly bleeding.
When islet xenoTx is performed, which is usually intothe portal vein so that the islets reside in the liver, theintravascular lines are frequently maintained in situ onlyduring the phase of initiation of diabetes by streptozotocinuntil the islet graft is clearly functioning, at which time they
are removed (van der Windt et al., 2009). Monitoring of pigislet function is by frequent measurement of blood glucoseand porcine C-peptide (which can be clearly differentiatedfrom monkey C-peptide); insulin levels can also bemeasured. To measure blood glucose, monkeys can bemonitored by skin prick, and can be trained to cooperate inthis form of monitoring.
Immunosuppressive Therapy
Immunosuppressive therapy, directed against both thehumoral response, e.g., anticomplement agents, such ascobra venom factor, and the cellular response, e.g., standardpharmacologic immunosuppressive agents, such as tacro-limus and mycophenolate mofetil, or the newer co-stimu-latory blockade agents, such as anti-CD154mAb orCTLA4-Ig, is usually initiated pre-Tx and continuedthroughout the course of the experiment (Kuwaki et al.,2005; Tseng et al., 2005). Table 16.2 provides an exampleof an immunosuppressive regimen with the supportivetherapy required. Increasingly, anticoagulant or antiplatelet

TABLE 16.2 Representative Immunosuppressive and
Supportive Drug Regimen used in Pig-to-Nonhuman
Primate Heart or Kidney Transplantation Experiments at
the University of Pittsburgh
Agent/Dose
1. Antithymocyte globulin (ATG) 1e10mg/kg x2 i.v. (days e3and e1) to reduce the CD3þ T cell count to <500/mm2.
2. Human antihuman CD154mAb 25mg/kg i.v. (on days e1,0, 4, 7, 10, 14, 19, and weekly) to maintain a trough level of>400 mg/ml.
3. Mycophenolate mofetil (MMF) by continuous i.v. infusion tomaintain a trough level of 3e6 mg/ml.
4. Methylprednisolone 5mg/kg/day i.m. on the days of ATGadministration and on day 0 (day of Tx) and day 1, taperingto 0.5mg/kg/day i.m. by day 6, and to 0.1mg/kg/day i.m. byday 10 (maintained throughout period of follow-up)
5. Prostacyclin 20 ng/kg/min by continuous i.v. infusion for48 hours.
6. Dopamine 2e7 mg/kg/min by continuous i.v. infusion for48 hours.
7. Ganciclovir 5 mg/kg/day as prophylaxis against cytomega-lovirus infection for at least the first month.
8. Cimetidine 10mg/kg x2 daily while intravascular cathetersare in situ to prevent peptic ulceration.
9. Heparin to maintain the aPTTat 150 s throughout the periodof follow-up.
10. Buprenorphine 0.01mg/kg will be given 6e12 hourly i.v. forat least the first 72 hours after any surgical procedure.
11. Cefazolin 10mg/kg/x2 days i.v. for 48 hours after anysurgical procedure.
397Chapter | 16 Xenotransplantation
agents are also administered (Kuwaki et al., 2005;Ezzelarab et al., 2009), frequently making the post-Txprotocol a complicated one (an example is illustrated inTable 16.3). A prolonged state of immune suppression canobviously be associated with complications, particularlyinfection.
Efforts are being made by at least one group to inducea state of ‘immunological tolerance’ in which, after initialintensive immunosuppressive therapy, possibly includingwhole body and/or thymic irradiation, all therapy can beslowly withdrawn (Yamada et al., 2005; Griesemer et al.,2009). Based on results in allogeneic models, the theory isthat, when the immune system recovers, it will no longerrespond to donor-specific antigens, but will respond nor-mally to other antigens, e.g., those expressed on bacteriaand viruses. This is clearly the ultimate goal of both alloTxand xenoTx, but in xenoTx it would appear that there areseveral hurdles, such as coagulation dysregulation, thatneed to be surmounted before this approach is likely to besuccessful. Furthermore, the intensive induction therapyrequired can increase the risk of infectious complications.
Antibacterial and antiviral prophylactic agents aretherefore administered routinely (Table 16.2). Antibiotics
are usually administered for 48 or 72 hours after anyinvasive procedure, such as introduction of the intravas-cular catheters or the actual organ transplant. In contrast,antiviral agents, such as ganciclovir, are maintained for atleast 1 month and frequently throughout the course of theexperiment as activation of recipient cytomegalovirus(CMV) has been associated with an increased incidence ofgraft failure (Mueller et al., 2004).
RESULTS AND COMPLICATIONS
Results
XenoTx has made significant progress during the past25 years (Cooper et al., 2007; Zhu et al., 2007; Piersonet al., 2009), though not to the extent that clinical trials oforgan xenoTx are likely to take place within the next yearor two, though tissue xenoTx is already underway andcorneal and islet xenoTx trials are likely to occur in theforeseeable future. With regard to organ xenoTx, hetero-topic heart transplants have functioned for up to 6 months(Kuwaki et al., 2005; McGregor et al., 2005) and orthotopicheart transplants for nearly 2 months (Vial et al., 2000;McGregor et al., 2009). Kidney transplants have beenslightly less successful, largely to an increased incidence ofconsumptive coagulopathy as a result of coagulationdysfunction; graft survival has extended close to 3 months(Cozzi et al., 2003; Yamada et al., 2005; Griesemer et al.,2009). Orthotopic liver xenoTx has been associated with animmediate fall in platelet count to dangerously low levels,resulting in internal hemorrhagic complications within thefirst week despite adequate hepatic function (Ekser et al.,2010). Pig lungs appear to be particularly susceptible toinjury, and graft survival generally remains less than24 hours (Cantu et al., 2007; Nguyen et al., 2007).
More successful results have been obtained in the fieldof islet xenoTx, with diabetic monkeys being maintained ina normoglycemic state for >6 months (Cardona et al.,2006; Hering et al., 2006), with one for >12 months (vander Windt et al., 2009). Very few pig corneal transplantshave been carried out in nonhuman primates, but the resultshave been encouraging with grafts from unmodified pigsremaining viable for several months with local corticoste-roids (Pan et al., 2007). Red blood cells from geneticallymodified pigs have been demonstrated to be preferable toABO-incompatible allo-transfusions, but not yet compa-rable to ABO-compatible transfusions (Long et al., 2009).
Complications
Complications include those associated with intravascularcatheters, as mentioned above. Wound healing has not beena significant problem, even when the recipients have
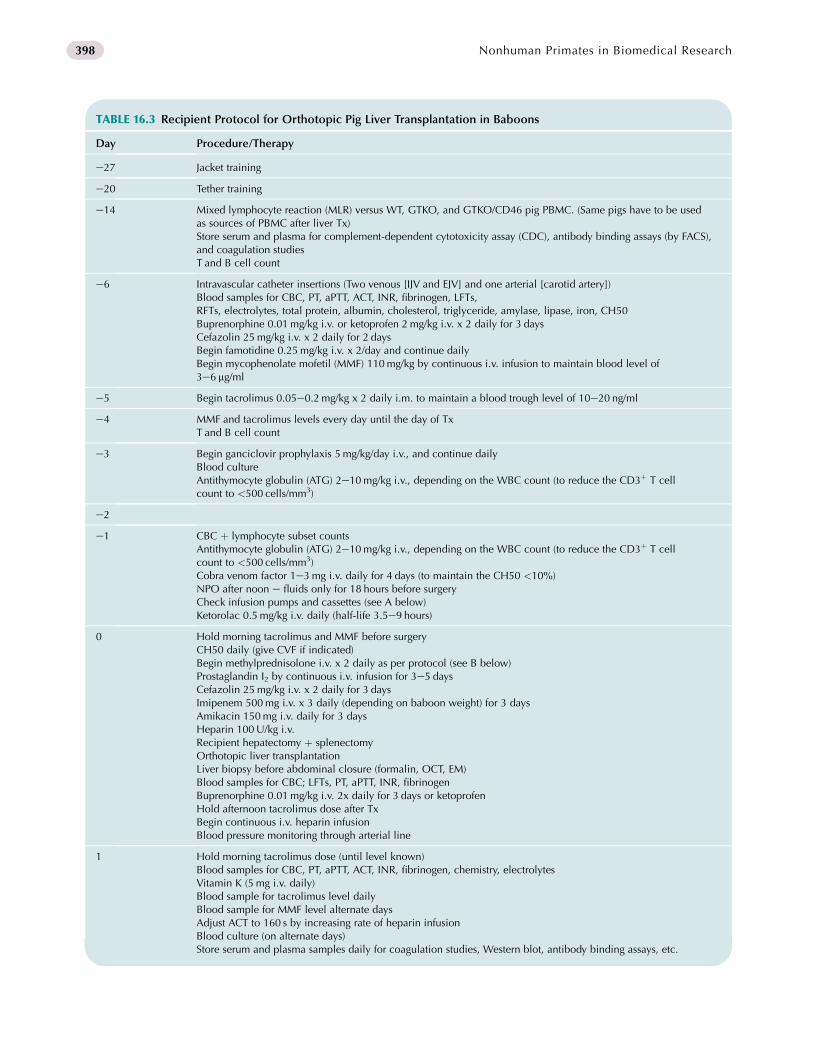
TABLE 16.3 Recipient Protocol for Orthotopic Pig Liver Transplantation in Baboons
Day Procedure/Therapy
e27 Jacket training
e20 Tether training
e14 Mixed lymphocyte reaction (MLR) versus WT, GTKO, and GTKO/CD46 pig PBMC. (Same pigs have to be usedas sources of PBMC after liver Tx)Store serum and plasma for complement-dependent cytotoxicity assay (CDC), antibody binding assays (by FACS),and coagulation studiesT and B cell count
e6 Intravascular catheter insertions (Two venous [IJV and EJV] and one arterial [carotid artery])Blood samples for CBC, PT, aPTT, ACT, INR, fibrinogen, LFTs,RFTs, electrolytes, total protein, albumin, cholesterol, triglyceride, amylase, lipase, iron, CH50Buprenorphine 0.01mg/kg i.v. or ketoprofen 2mg/kg i.v. x 2 daily for 3 daysCefazolin 25mg/kg i.v. x 2 daily for 2 daysBegin famotidine 0.25mg/kg i.v. x 2/day and continue dailyBegin mycophenolate mofetil (MMF) 110mg/kg by continuous i.v. infusion to maintain blood level of3e6 mg/ml
e5 Begin tacrolimus 0.05e0.2mg/kg x 2 daily i.m. to maintain a blood trough level of 10e20 ng/ml
e4 MMF and tacrolimus levels every day until the day of TxT and B cell count
e3 Begin ganciclovir prophylaxis 5 mg/kg/day i.v., and continue dailyBlood cultureAntithymocyte globulin (ATG) 2e10mg/kg i.v., depending on the WBC count (to reduce the CD3þ T cellcount to <500 cells/mm3)
e2
e1 CBC þ lymphocyte subset countsAntithymocyte globulin (ATG) 2e10mg/kg i.v., depending on the WBC count (to reduce the CD3þ T cellcount to <500 cells/mm3)Cobra venom factor 1e3mg i.v. daily for 4 days (to maintain the CH50 <10%)NPO after noon e fluids only for 18 hours before surgeryCheck infusion pumps and cassettes (see A below)Ketorolac 0.5mg/kg i.v. daily (half-life 3.5e9 hours)
0 Hold morning tacrolimus and MMF before surgeryCH50 daily (give CVF if indicated)Begin methylprednisolone i.v. x 2 daily as per protocol (see B below)Prostaglandin I2 by continuous i.v. infusion for 3e5 daysCefazolin 25mg/kg i.v. x 2 daily for 3 daysImipenem 500mg i.v. x 3 daily (depending on baboon weight) for 3 daysAmikacin 150mg i.v. daily for 3 daysHeparin 100U/kg i.v.Recipient hepatectomy þ splenectomyOrthotopic liver transplantationLiver biopsy before abdominal closure (formalin, OCT, EM)Blood samples for CBC; LFTs, PT, aPTT, INR, fibrinogenBuprenorphine 0.01mg/kg i.v. 2x daily for 3 days or ketoprofenHold afternoon tacrolimus dose after TxBegin continuous i.v. heparin infusionBlood pressure monitoring through arterial line
1 Hold morning tacrolimus dose (until level known)Blood samples for CBC, PT, aPTT, ACT, INR, fibrinogen, chemistry, electrolytesVitamin K (5 mg i.v. daily)Blood sample for tacrolimus level dailyBlood sample for MMF level alternate daysAdjust ACT to 160 s by increasing rate of heparin infusionBlood culture (on alternate days)Store serum and plasma samples daily for coagulation studies, Western blot, antibody binding assays, etc.
398 Nonhuman Primates in Biomedical Research

TABLE 16.3 Recipient Protocol for Orthotopic Pig Liver Transplantation in Baboonsdcont’d
Day Procedure/Therapy
2 Blood samples for CBC PT, aPTT, INR, fibrinogen, LFTs, T and B cell countAdjust ACT to 180 s by increasing rate of heparin infusion
3 Adjust ACT to 200 s by increasing rate of heparin infusion
5 T and B cell count
7 Store serum (5ml) for CDCT and B cell countMLR
14 Consider percutaneous liver biopsyStore serum (5ml) for CDC
21 Consider percutaneous liver biopsyMLRStore serum (6ml)Store serum (5ml) for CDC
28 Euthanasia
A: Infusion pumps
Line A: Heparinized normal saline
Line B: Normal saline
Line C: Dopamine
Line D: Phenylephrine
B: Methylprednisolone regimen
Day 0: 10mg/kg i.v.
Day 1: 2.5mg/kg i.v. x 2
Day 2: 1.25mg/kg i.v. x 2
Days 3e6: 0.5mg/kg i.v. x 2
Days 7e13: 0.25mg/kg i.v. x 2 daily
Days 14e20: 0.125mg/kg i.v. x 2 daily
Days 21e27: 0.1 mg/kg i.v. x 2 daily
Days 28 onwards: 0.2mg/kg i.v. daily
399Chapter | 16 Xenotransplantation
received high doses of steroids (though it might becomemore of a problem if rapamycin were to be used morecommonly in this model). Infection remains a complicationof immunosuppressive therapy, and requires constantmonitoring. It can take the form of a positive blood cultureor sepsis around the intravascular catheters. Some unusualinfectious agents have been reported. Lymphoma is rela-tively rare, but is likely to be reported more commonly asthe period of graft and recipient survival increases. In ourown experience, self-mutilation has not been seen, butcomplications such as acute gastric dilatation, collagenouscolitis, and intussusception have occurred.
The development of a consumptive coagulopathy asa direct result of coagulation dysfunction is one of the
major complications of organ xenoTx seen today, evenwhen evidence for an immune response is minimal (Buhleret al., 2000; Lin et al., 2008). It can be reversed if the graftis excised before the condition has become too advanced.Aggressive medical management, however, has routinelyfailed to correct consumptive coagulopathy.
GENETIC MODIFICATION OF PIGS
The steadily increasing success of experimental xenoTxhas largely been due to the development of geneticallymodified pigs using nuclear transfer (cloning) tech-nology. Our ability to knock-out a gene, such as thea-1,3galactosyltransferase gene, which is responsible for

400 Nonhuman Primates in Biomedical Research
the production of Gal oligosaccharides, has clearly beenimportant (Phelps et al., 2003; Kolber-Simonds et al.,2004). The insertion of a human gene to provideprotection of a pig organ has also played a major role,particularly in regard to the introduction of a humancomplement-regulatory protein, e.g., CD46 (membranecofactor protein), CD55 (decay-accelerating factor), orCD59, to protect against the effects of complementactivation (Cozzi and White, 1995; Loveland et al.,2004). Today, major efforts are being directed towardsexpressing human anticoagulant, antiplatelet, anti-inflammatory genes, such as tissue factor pathwayinhibitor, thrombomodulin, endothelial cell protein Creceptor, CD39, or hemeoxygenase-1 (HO-1).
An effort is also being made to provide local, rather thansystemic, immune suppression to the graft by, for example,expression of pig or human CLTA4-Ig on graft cells.Expression of this agent results in costimulatory blockade,thus preventing T cell activation, which has been clearlydemonstrated by in vitro assays. However, when pCTLA4-Ig was expressed constitutively, the pigs were found to bepartially immuno-incompetent and susceptible to infectiouscomplications (Phelps et al., 2009). Techniques are nowavailable to overcome this problem in some cases byexpressing the gene only in the tissues to be transplanted,e.g., in the pig islets alone using an insulin promoter.‘Anticoagulant’ or ‘anti-inflammatory’ genes, e.g., tissuefactor pathway inhibitor, CD39, that might similarly beproblematic if expressed widely in the pig, have also beenintroduced only into the islets.
Techniques of genetic engineering that allow a gene tobe ‘switched on’ or ‘off’, such as those using the Cre-Loxsystem, are currently being explored, as this would allowthe gene to be expressed functionally only in the organ afterTx, but not in the pig before organ ‘donation’.
SUMMARY
Wild-type pig tissues, such as small intestinal submucosa(SIS, which is rendered void of cells and is repopulatedwith recipient cells) are already being used extensively inclinical surgical practice. GTKO pig tissues, to which thereis a reduced inflammatory response, will probably be thenext innovation in clinical practice. In view of the world-wide shortage of human corneas for Tx, the pig cornea islikely to find a significant role in the treatment of cornealblindness, particularly in less-developed countries; thegenetically modified pigs can be bred and housed ina country with the necessary resources, and the corneasshipped to the centers where they will be transplanted.
Clinical trials of islet xenoTx will probably take placewithin the next few years (Hering, 2009). The need is vast,and the supply of human islets limited. The xenoTx ofdopamine-producing neural cells for the treatment of
neurodegenerative conditions, such as Parkinson’s disease,underwent clinical trials more than a decade ago, and thesemay be resumed if current experiments prove encouraging(Badin et al., 2010). With both islet and neural cell trans-plantation, the risks to the patient are small, but the benefitscould be considerable.
XenoTx of whole organs requires further significantadvances in the laboratory before it can be ethically intro-duced into the clinic, but bridging of patients in fulminantliver failure by a pig liver while they await a human organmay well be feasible within a few years (Ekser et al., 2009),as may bridging with a pig heart in patients who areawaiting human heart transplantation (Cooper et al., 2000).
The potential of xenoTx is so great that experimentalresearch is likely to continue and expand. However, it ispersonnel-intensive, time-consuming, and expensive. Asthe only relevant model is the pig-to-nonhuman primatemodel, progress will inevitably be relatively slow. Ourincreasing ability to genetically engineer pigs for thispurpose, however, provides optimism that the remainingproblems will be overcome.
ACKNOWLEDGMENTS
We are most grateful to Burcin Ekser, MD, for kindly providing
Figure 16.3. Work on xenotransplantation in the Thomas E. Starzl
Transplantation Institute of the University of Pittsburgh is supported
in part by NIH grants U01 AI068642 and R21 A1074844, and by
Sponsored Research Agreements between the University of Pittsburgh
and Revivicor, Inc., Blacksburg, VA, USA.
REFERENCES
Bach, F. H., Robson, S. C., Ferran, C., Winkler, H., Millan, M. T.,
Stuhlmeier, K. M., Vanhove, B., Blakely, M. L., van der Werf, W. J.,
& Hofer, E. (1994). Endothelial cell activation and thromboregulation
during xenograft rejection. Immunol Rev, 141, 5e30.
Badin, R. A., Padoan, A., Vadori, M., et al. (2010). Long-term clinical
recovery in Parkinsonian monkey recipients of CTLA4-Ig transgenic
porcine neural precursors. Transplantation, 90(Suppl. 2), 47,
(Abstract LB-3288).
Buhler, L., Basker, M., Alwayn, I. P., Goepfert, C., Kitamura, H.,
Kawai, T., Gojo, S., Kozlowski, T., Ierino, F. L., Awwad, M.,
Sachs, D. H., Sackstein, R., Robson, S. C., & Cooper, D. K. (2000).
Coagulation and thrombotic disorders associated with pig organ and
hematopoietic cell transplantation in nonhuman primates. Trans-
plantation, 70, 1323e1331.
Cantu, E., Balsara, K. R., Li, B., et al. (2007). Prolonged function of
macrophage, von Willibrand factor-deficient porcine pulmonary
xenografts. Am J Transplant, 7, 66e75.
Cardona, K., Korbutt, G. S., Milas, Z., Lyon, J., Cano, J., Jiang, W., Bello-
Laborn, H., Hacquoil, B., Strobert, E., Gangappa, S., Weber, C. J.,
Pearson, T. C., Rajotte, R. V., & Larsen, C. P. (2006). Long-term
survival of neonatal porcine islets in nonhuman primates by targeting
costimulation pathways. Nat Med, 12, 304e306.

401Chapter | 16 Xenotransplantation
Chen, D., & Dorling, A. (2005). Microcoagulation processes after xeno-
transplantation. Curr Opin Organ Transplant, 10, 240e245.
Chen, D., Weber, M., McVey, J. H., Kemball-Cook, G.,
Tuddenham, E. G., Lechler, R. I., & Dorling, A. (2004). Complete
inhibition of acute humoral rejection using regulated expression of
membrane-tethered anticoagulants on xenograft endothelium. Am J
Transplant, 4, 1958e1963.
Cooper, D. K. C., Dorling, A., Pierson, R. N., III, Rees, M., Seebach, J.,
Yazer, M., Ohdan, H., Awwad, M., & Ayares, D. (2007). Alpha1,3-
galactosyltransferase gene knockout pigs for xenotransplantation:
where do we go from here? Transplantation, 84, 1e7.
Cooper, D. K. C., Keogh, A. M., Brink, J., Corris, P. A., Klepetko, W.,
Pierson, R. N., Schmoeckel, M., Shirakura, R., & Warner Stevenson, L.
(2000). Warner Stevenson L. Report of the Xenotransplantation
Advisory Committee of the International Society for Heart and Lung
Transplantation: the present status of xenotransplantation and its
potential role in the treatment of end-stage cardiac and pulmonary
diseases. J Heart Lung Transplant, 19, 1125e1165.
Cooper, D. K. C., Human, P. A., Lexer, G., Rose, A. G., Rees, J.,
Keraan, M., & Du Toit, E. (1988). Effects of cyclosporine and anti-
body adsorption on pig cardiac xenograft survival in the baboon.
J Heart Transplant, 7, 238e246.
Cooper, D. K. C., & Lanza, R. P. (2000). Xeno - The Promise of Trans-
planting Animal Organs into Humans. New York: Oxford University
Press. 1e274.
Cooper, D. K. C., Gollackner, B., & Sachs, D. H. (2002). Will the pig
solve the transplantation backlog? Ann Rev Med, 53, 133e147.
Cooper, D. K. C., Ye, Y., & Niekrasz, M. (1994). Heart transplantation in
primates. In L. Makowka, D. V. Cramer, & L. Sher (Eds.), Experi-
mental Techniques in Transplantation (pp. 173e200). Boca Raton:
C.R.C. Press.
Cooper, D. K. C. (1992). Depletion of natural antibodies in non-human
primates - a step towards successful discordant xenografting in man.
Clin Transplantation, 6, 178e183.
Cooper, D. K. C., Good, A. H., Koren, E., Oriol, R., Malcolm, A. J.,
Ippolito, R. M., Neethling, F. A., Ye, Y., Romano, E., & Zuhdi, N.
(1993). Identification of a-galactosyl and other carbohydrate epitopes
that are bound by human anti-pig antibodies: relevance to discordant
xenografting in man. Transpl Immunol, 1, 198e205.
Cozzi, E., & White, D. J. G. (1995). The generation of transgenic pigs as
potential organ donors for humans. Nat Med, 1, 964e969.
Cozzi, E., Vial, C., Ostlie, D., Farah, B., Chavez, G., Smith, K. G.,
Bradley, J. R., Thiru, S., Davies, H. F., Wallwork, J., White, D. J.,
Goddard, M., & Friend, P. J. (2003). Maintenance triple immuno-
suppression with cyclosporin A, mycophenolate sodium and steroids
allows prolonged survival of primate recipients of hDAF porcine
renal xenografts. Xenotransplantation, 10, 300e310.
Dorling, A., & Lechler, R. I. (1998). T cell-mediated xenograft rejection:
specific tolerance is probably required for long term xenograft
survival. Xenotransplantation, 5, 234e245.
Ekser, B., Gridelli, B., Tector, A. J., & Cooper, D. K. C. (2009). Pig liver
xenotransplantation as a bridge to allotransplantation in acute liver
failure: which patients might benefit? Transplantation, 88, 1041e1049.
Ekser, B., Long, C., Echeverri, G. J., Hara, H., Ezzelarab, M., Lin, C. C.,
de Vera, M. E., Wagner, R., Klein, K., Wolf, R. F., Ayares, D.,
Cooper, D. K. C., & Gridelli, B. (2010). Impact of thrombocytopenia
on survival of baboons with genetically-modified pig liver trans-
plants: clinical relevance. Am J Transplant, 10, 273e285.
Ezzelarab, M., Garcia, B., Azimzadeh, A., Sun, H., Lin, C. C., Hara, H.,
Kelishadi, S., Zhang, T., Lin, Y. J., Tai, H.-C., Long, C., Wagner, R.,
Thacker, J., Murase, N., McCurry, K., Barth, R. N., Ayares, D.,
Pierson, R. N., III, & Cooper, D. K. C. (2009). The innate immune
response and activation of coagulation in a1,3-galactosyltransferase
gene-knockout xenograft recipients. Transplantation, 87, 805e812.
Galili, U., Shohet, S. B., Kobrin, E., Stults, C. L., & Macher, B. A. (1988).
Man, apes, and Old World monkeys differ from other mammals in the
expression of alpha-galactosyl epitopes on nucleated cells. J Biol
Chem, 263, 17755e17762.
Griesemer, A. D., Hirakata, A., Shimizu, A., Moran, S., Tena, A.,
Iwaki, H., Ishikawa, Y., Schule, P., Arn, J. S., Robson, S. C.,
Fishman, J. A., Sykes, M., Sachs, D. H., & Yamada, K. (2009).
Results of Gal-knockout porcine thymokidney xenografts. Am J
Transplant, 9, 2669e2678.
Hara, H., Gridelli, B., Lin, Y. J., Marcos, A., & Cooper, D. K. C. (2008).
Liver xenografts for the treatment of acute liver failure e clinical and
experimental experience and remaining immunologic barriers. Liver
Transplantation, 14, 425e434.
Hara, H., & Cooper, D. K. C. (2010). Xenotransplantation e the future of
corneal transplantation? Cornea. Nov 17. Epub ahead of print.
Hardy, J. D., Chavez, C. M., Kurrus, F. D., Neely, W. A., Eraslan, S.,
Turner, M. D., Fabian, L. W., & Labecki, T. D. (1964). Heart trans-
plantation in man:developmental studies and report of a case. JAMA,
188, 1132e1140.
Hering, B. J., Cooper, D. K. C., Cozzi, E., Schuurman, H.-J.,
Korbutt, G. S., Denner, J., O’Connell, P. J., Vanderpool, H. Y., &
Pierson, R. N., III (2009). The International Xenotransplantation
Association consensus statement on conditions for undertaking clin-
ical trials of porcine islet products in type 1 diabetes e Executive
summary. Xenotransplantation, 16, 196e202.
Hering, B. J., Wijkstrom, M., Graham, M. L., Hardstedt, M.,
Aasheim, T. C., Jie, T., Ansite, J. D., Nakano, M., Cheng, J., Li, W.,
Moran, K., Christians, U., Finnegan, C., Mills, C. D.,
Sutherland, D. E., Bansal-Pakala, P., Murtaugh, M. P., Kirchhof, N.,
& Schuurman, H. J. (2006). Prolonged diabetes reversal after intra-
portal xenotransplantation of wild-type porcine islets in immuno-
suppressed nonhuman primates. Nat Med, 12, 301e303.
Houser, S. L., Kuwaki, K., Knosalla, C., Dor, F. J. M. F., Gollackner, B.,
Cheng, J., Shimizu, A., Schuurman, H.-J., & Cooper, D. K. C. (2004).
Thrombotic microangiopathy and graft arteriopathy in pig hearts
following transplantation into baboons. Xenotransplantation, 11,
416e425.
Kolber-Simonds, D., Lai, L., Watt, S. R., Denaro, M., Arn, S.,
Augenstein, M. L., Betthauser, J., Carter, D. B., Greenstein, J. L.,
Hao, Y., Im, G. S., Liu, Z., Mell, G. D., Murphy, C. N., Park, K. W.,
Rieke, A., Ryan, D. J., Sachs, D. H., Forsberg, E. J., Prather, R. S., &
Hawley, R. J. (2004). a1,3-galactosyltransferase null pigs via nuclear
transfer with fibroblasts bearing loss of heterozygosity mutations.
Proc Natl Acad Sci USA, 19, 7335e7340.
Kuwaki, K., Tseng, Y.-L., Dor, F. J. M. F., Shimizu, A., Houser, S. L.,
Sanderson, T. M., Lancos, C. J., Prabharasuth, D. D., Cheng, J.,
Moran, K., Hisash, Y., Mueller, N., Yamada, K., Greenstein, J. L.,
Hawley, R. J., Patience, C., Awwad, M., Fishman, J. A.,
Robson, S. C., Schuurman, H.-J., Sachs, D. H., & Cooper, D. K. C.
(2005). Heart transplantation in baboons using a1,3-galactosyl-
transferase gene-knockout pigs as donors: initial experience. Nat
Med, 11, 29e31.

402 Nonhuman Primates in Biomedical Research
Lexer, G., Cooper, D. K. C., Rose, A. G., Wicomb, W. N., Rees, J.,
Keraan, M., & Du Toit, E. (1986). Hyperacute rejection in a discor-
dant (pig to baboon) cardiac xenograft model. J Heart Transplant, 5,
411e418.
Lin, C. C., Chen, D., McVey, J. H., Cooper, D. K. C., & Dorling, A.
(2008). Expression of tissue factor and initiation of clotting by human
platelets and monocytes after incubation with porcine endothelial
cells. Transplantation, 86, 702e709.
Long, C., Hara, H., Pawlikowski, Z., Koike, N., d’Arville, T., Yeh, P.,
Ezzelarab, M., Ayares, D., Yazer, M., & Cooper, D. K. C. (2009).
Genetically-engineered pig red blood cells for clinical transfusion:
initial in vitro studies. Transfusion, 49, 2418e2429.
Loveland, B. E., Milland, J., Kyriakou, P., Thorley, B. R.,
Christiansen, D., Lanteri, M. B., Regensburg, M., Duffield, M.,
French, A. J., Williams, L., Baker, L., Brandon, M. R., Xing, P. X.,
Kahn, D., & McKenzie, I. F. (2004). Characterization of a CD46
transgenic pig and protection of transgenic kidneys against hyper-
acute rejection in non-immunosuppressed baboons. Xeno-
transplantation, 11, 171e183.
McGregor, C. G. A., Byrne, G. W., Vlasin, M., Walker, R. C.,
Tazelaar, H. D., Davies, W. R., Chandrasekaran, K., Oehler, E. A.,
Bolison, B. A., Wiseman, B. S., & Logan, J. S. (2009). Early
cardiac function and gene expression after orthotopic cardiac
xenotransplantation (Abstract IXA-O-2.4). Xenotransplantation,
16, 356.
McGregor, C. G. A., Davies, W. R., Oi, K., Teotia, S. S., Schirmer, J. M.,
Risdahl, J. M., Tazelaar, H. D., Kremers, W. K., Walter, R. C.,
Byrne, G. W., & Logan, J. S. (2005). Cardiac xenotransplantation:
recent preclinical progress with 3-month median survival. J Thorac
Cardiovasc Surg, 130, 844e851.
Mirenda, V., Golshayan, D., Read, J., Berton, I., Warrens, A. N.,
Dorling, A., & Lechler, R. I. (2005). Achieving permanent survival
of islet xenografts by independent manipulation of direct and indirect
T-cell responses. Diabetes, 54, 1048e1055.
Mueller, N. J., Kuwaki, K., Dor, F. J. M. F., Knosalla, C., Gollackner, B.,
Wilkinson, R. A., Sachs, D. H., Cooper, D. K. C., & Fishman, J. A.
(2004). Reduction of consumptive coagulopathy using porcine cyto-
megalovirus-free cardiac porcine grafts in pig-to-primate xeno-
transplantation. Transplantation, 78, 1449e1453.
Nguyen, B. N., Azimzadeh, A. M., Zhang, T., Wu, G., Schuurman, H. J.,
Sachs, D. H., Ayares, D., Allan, J. S., & Pierson, R. N., III (2007).
Life-supporting function of genetically-modified swine lungs in
baboons. J Thorac Cardiovasc Surg, 133, 1354e1363.
Oriol, R., Ye, Y., Koren, E., & Cooper, D. K. C. (1993). Carbohydrate
antigens of pig tissues reacting with human natural antibodies as
potential targets for hyperacute vascular rejection in pig-to-man
organ xenotransplantation. Transplantation, 56, 1433e1442.
Pan, Z., Sun, C., Jie, Y., Wang, N., & Wang, L. (2007). WZS-pig is
a potential donor alternative in corneal xenotransplantation. Xeno-
transplantation, 14, 603e611.
Phelps, C., Ball, S., Vaught, T., Vance, A., Mendicino, M., Monahan, J.,
Dandro, A., Cooper, D. K. C., & Ayares, D. (2009). Production and
characterization of transgenic pigs expressing porcine CTLA4-Ig.
Xenotransplantation, 16, 477e485.
Phelps, C. J., Koike, C., Vaught, T. D., Boone, J., Wells, K. D.,
Chen, S. H., Ball, S., Specht, S. M., Polejaeva, I. A., Monahan, J. A.,
Jobst, P. M., Sharma, S. B., Lamborn, A. E., Garst, A. S., Moore, M.,
Demetris, A. J., Rudert, W. A., Bottino, R., Bertera, S., Trucco, M.,
Starzl, T. E., Dai, Y., & Ayares, D. L. (2003). Production of a1,3-
galactosyltransferase-deficient pigs. Science, 299, 411e414.
Pierson, R. N., III, Dorling, A., Ayares, D., Rees, M. A., Seebach, J. D.,
Fishman, J. A., Hering, B. J., & Cooper, D. K. C. (2009). Current
status of xenotransplantation and prospects for clinical application.
Xenotransplantation, 16, 263e280.
Reemtsma, K., McCracken, B. H., Schlegel, J. Y., Pearl, M. A.,
Pearce, C. W., DeWitt, C. W., Smith, P. E., Hewitt, R. L.,
Flinner, R. L., & Creech, O., Jr. (1964). Renal heterotransplantation
in man. Ann Surg, 160, 384e410.
Robson, S. C., Cooper, D. K. C., & d’Apice, A. J. F. (2000). Disordered
regulation of coagulation and platelet activation in xeno-
transplantation. Xenotransplantation, 7, 166e176.
Rose, A. G., Cooper, D. K. C., Human, P. A., Reichenspurner, H., &
Reichart, B. (1991). Histopathology of hyperacute rejection of the
heart - experimental and clinical observations in allografts and
xenografts. J Heart Lung Transplant, 10, 223e234.
Rose, A. G., & Cooper, D. K. C. (1996). A histopathologic grading
system of hyperacute (humoral, antibody-mediated) cardiac
xenograft and allograft rejection. J Heart Lung Transplant, 15,
804e817.
Rose, A. G., & Cooper, D. K. C. (2000). Venular thrombosis is the key
event in the pathogenesis of antibody-mediated cardiac rejection.
Xenotransplantation, 7, 31e41.
Stussi, G., West L Cooper, D. K. C., & Seebach, J. D. (2006). ABO-
incompatible allotransplantation as a basis for clinical xeno-
transplantation. Xenotransplantation, 13, 390e399.
Taniguchi, S., & Cooper, D. K. C. (1997). Clinical xenotransplantation -
past, present and future. Ann R Coll Surg Engl, 79, 13e19.
Tseng, Y.-L., Kuwaki, K., Dor, F. J. M. F., Shimizu, A., Houser, S.,
Hisashi, Y., Yamada, K., Robson, S. C., Awwad, M.,
Schuurman, H. J., Sachs, D. H., & Cooper, D. K. C. (2005). a1,3-
galactosyltransferase gene-knockout pig heart transplantation in
baboons with survival approaching six months. Transplantation, 80,
1493e1500.
van der Windt, D. J., Bottino, R., Casu, A., Campanile, N., Smetanka, C.,
He, J., Murase, N., Hara, H., Ball, S., Loveland, B. E., Ayares, D.,
Lakkis, F. G., Cooper, D. K. C., & Trucco, M. (2009). Long-term
controlled normoglycemia in diabetic non-human primates after
transplantation with hCD46 transgenic porcine islets. Am J Trans-
plant, 9, 2716e2726.
Vial, C. M., Ostlie, D. J., Bhatti, F. N., Cozzi, E., Goddard, M.,
Chavez, G. P., Wallwork, J., White, D. J., & Dunning, J. J. (2000).
Life supporting function for over one month of a transgenic porcine
heart in a baboon. J Heart Lung Transplant, 19, 224e229.
Yamada, K., Yazawa, K., Shimizu, A., Iwanaga, T., Hisashi, Y.,
Nuhn, M., O’Malley, P., Nobori, S., Vagefi, P. A., Patience, C.,
Fishman, J., Cooper, D. K. C., Hawley, R. J., Greenstein, J.,
Schuurman, H.-J., Awwad, M., Sykes, M., & Sachs, D. H. (2005).
Marked prolongation of porcine renal xenograft survival in baboons
through the use of a1,3-galactosyltransferase gene-knockout donors
and the cotransplantation of vascularized thymic tissue. Nat Med, 11,
32e34.
Zhu, X., Dor, F. J. M. F., & Cooper, D. K. C. (2007). Pig-to-nonhuman
primate heart transplantation: immunologic progress over 20 years.
J Heart Lung Transplant, 26, 210e218.










![MicroPET/CTImagingof[18F]-FEPPAintheNonhumanPrimate ...downloads.hindawi.com/archive/2012/261640.pdf · 2019. 7. 31. · including nonhuman primates (NHP) [12–14]. In order to obtain](https://static.fdocuments.in/doc/165x107/5ff9aa3eae70605aac1dd15e/micropetctimagingof18f-feppainthenonhumanprimate-2019-7-31-including.jpg)







