New Cancer Prevention & Early Detection Facts & Figures 2005 Diseases... · 2007. 1. 8. · Cancer...
60
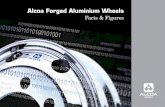
AL AZ AR CA CO CT DE FL GA ID IL IN IA KS KY LA ME MD MA MN MS MO MT NE NV NH NJ NM NY NC ND OH OK OR PA RI SC SD TN TX UT VT VA WA WV WI WY DC HI AK Tobacco Excise Tax by State, 2004* Equal to or above the national average of 79 cents per pack Below the national average in the range of 35 to 78 cents per pack Far below the national average up to 34 cents per pack *Data current as of October 2004. Source: National Government Relations Department, American Cancer Society, 2004 MI Cancer Prevention & Early Detection Facts & Figures 2005
Transcript of New Cancer Prevention & Early Detection Facts & Figures 2005 Diseases... · 2007. 1. 8. · Cancer...

AL
AZAR
CA CO
CT
DE
FL
GA
ID
IL IN
IA
KS
KY
LA
ME
MD
MA
MN
MS
MO
MT
NENV
NH
NJ
NM
NY
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WIWY
DC
HI
AK
Tobacco Excise Tax by State, 2004*
Equal to or above the national average of 79 cents per pack
Below the national average in the range of 35 to 78 cents per pack
Far below the national average up to 34 cents per pack*Data current as of October 2004.
Source: National Government Relations Department, American Cancer Society, 2004
MI
Cancer Prevention& Early Detection
Facts & Figures 2005

ContentsPreface 1
Children and Adolescents 3
Youth Tobacco Use 3
Overweight and Obesity, Physical Inactivity, and Nutrition Among Youth 8
Sun Protection 15
Adult Cancer Prevention 17
Adult Tobacco Use 17
Overweight and Obesity, Physical Inactivity, and Nutrition Among Adults 25
American Cancer Society Guidelines on Nutrition and Physical Activity for Cancer Prevention 26
Cancer Screening 35
Breast Cancer Screening 35
Screening Guidelines for the Early Detection of Cancer in Asymptomatic People 36
Cervical Cancer Screening 37
Colon and Rectum Cancer Screening 39
Prostate Cancer Screening 44
Barriers and Opportunities to Improve Cancer Screening 44
Statistical Notes 47
Survey Sources 49
References 50
List of Tables and Figures 56
Acknowledgments 57
©2005, American Cancer Society, Inc. All rights reserved, including the right to reproduce thispublication or portions thereof in any form. For written permission, address the American CancerSociety, 1599 Clifton Road, NE, Atlanta, GA 30329-4251.
This publication attempts to summarize current scientific information about cancer. Except whenspecified, it does not represent the official policy of the American Cancer Society.
Suggested citation: American Cancer Society. Cancer Prevention & Early Detection Facts &Figures 2005. Atlanta: American Cancer Society, 2005.
For more information, contact:Vilma Cokkinides, PhD, MSPHJessica Albano, MPHAlicia Samuels, MPHElizabeth M.Ward, PhDMichael J. Thun, MD, MS
Department of Epidemiology and Surveillance Research

Preface
Tobacco use, physical inactivity, obesity, and poor nutri-tion are major preventable causes of cancer and otherdiseases in the US. The American Cancer Society esti-mates that in 2005, more than 168,140 cancer deaths willbe caused by tobacco use alone. In addition, scientistsestimate that approximately one-third (190,090) of the570,280 cancer deaths expected to occur in 2005 will berelated to poor nutrition, physical inactivity, overweight,obesity, and other lifestyle factors.1-3 Many deaths fromcancers of the breast, colon, rectum, and uterine cervixcould also be prevented by greater utilization of estab-lished screening tests. While these categories overlapand cannot simply be added to determine the total num-ber of fatal cancers that could be prevented, a conserva-tive estimate is that at least half of all cancer deathscould in principle be avoided by the application of exist-ing knowledge.
To support cancer control efforts, the American CancerSociety has published Cancer Prevention & EarlyDetection Facts and Figures (CPED) annually since 1992.CPED is intended to be a resource for American CancerSociety staff, volunteers, and others working tostrengthen cancer prevention and early detection effortsat the local, state, and/or national levels. CPED comple-ments the companion publication, Cancer Facts &Figures, by providing current information on the preva-lence of modifiable risk factors for cancer and the uti-lization of screening tests that can detect cancer early,when treatment is most effective. It includes informa-tion on the burden of disease, death, and economic costsattributable to factors such as tobacco use, obesity, phys-ical inactivity, and under-usage of established screeningtests. It identifies social, legislative, and economic fac-tors that influence individual behaviors that affectcancer risk. It describes best practices for reducingtobacco usage by adults and children and highlightssuccess stories in community efforts to reduce tobaccodependence, increase physical activity, and improvedietary patterns. Although the report is divided into sep-arate sections that discuss cancer prevention in childrenand adolescents and prevention and early detection inadults, these topics are interrelated; many of the strate-gies that foster positive behaviors at one age continue tohave a beneficial effect on health throughout life.
Issues relating to cancer prevention and early detectionare central to the American Cancer Society’s mission andits 2015 goals. The Society is dedicated to eliminating
cancer as a major public health problem by preventingcancer, saving lives, and diminishing suffering fromcancer, through research, education, advocacy, andservice.
In 1999, the Society set bold challenge goals for thenation that, if met, would significantly lower cancerincidence and mortality rates and improve the quality oflife for all cancer survivors by 2015. The AmericanCancer Society has also developed nationwide objectivesthat set the framework for achieving the 2015 goals (seesidebar, page 2). These objectives can be achieved byimproved collaboration among government agencies,private companies, nonprofit organizations, health careproviders, policymakers, insurers, and the Americanpublic.
One example of collaboration is a groundbreaking part-nership of the American Cancer Society, the AmericanDiabetes Association, and the American HeartAssociation, called Everyday Choices for a HealthierLifeTM. This initiative, launched in June 2004, combinesthe efforts of the three organizations to address com-mon risk factors, such as tobacco use, obesity, physicalinactivity, poor nutrition, and under-utilization of effec-tive screening tests. Collectively, cancer, cardiovasculardisease, and diabetes account for approximately two-thirds of all deaths in the United States and about $700billion in direct and indirect economic costs each year.4
By working together, the three organizations can moreeffectively address common goals such as preventing theinitiation of tobacco use, facilitating cessation, promot-ing proper nutrition and weight control, improvingnutrition, increasing physical activity, and establishingroutine use of effective screening tests. The collabora-tion also seeks to increase the focus on preventionamong health care providers, and to support legislationthat increases funding for and access to prevention pro-grams and support for research. More information aboutthis initiative can be found at www.everydaychoices.org.
There is increasing recognition of the impact of commu-nity and environmental factors on individual healthbehaviors.5,6 Physical activity, good nutrition, and cancerscreening can all be influenced through legislation,public health policies, and adequate funding for pro-grams, similar to comprehensive tobacco control.7
Public policy and legislation at the federal, state, andlocal levels can increase access to preventive health serv-ices, including cancer screening.8 For example, at thefederal level, the American Cancer Society has advocatedfor increased funding of the Centers for Disease Control
Cancer Prevention & Early Detection Facts & Figures 2005 1

and Prevention’s National Breast and Cervical CancerEarly Detection Program (NBCCEDP) to help low-income and uninsured women obtain screening. At boththe federal and state levels, the American Cancer Societyhas advocated for laws requiring insurers to provide cov-erage for recommended cancer screening in health careplans, such as coverage for the full range of colorectal
cancer screening tests. In addition, the Society hasworked at both the state and federal levels to ensureMedicaid coverage for the treatment of breast and cervi-cal cancer cases diagnosed through the NBCCEDP.8
These and other community, policy, and legislative ini-tiatives are highlighted in this publication.
2 Cancer Prevention & Early Detection Facts & Figures 2005
American Cancer Society Goals and Objectives
2015 Challenge Goals• A 50% reduction in age-adjusted cancer mortality rates
• A 25% reduction in age-adjusted cancer incidence rates
• A measurable improvement in the quality of life (physi-cal, psychological, social, and spiritual), from the time of diagnosis and for the balance of life, of all cancersurvivors
2015 Nationwide ObjectivesAdult Tobacco Use: Reduce to 12% the proportion ofadults (18 and older) who use tobacco products.
Youth Tobacco Use: Reduce to 10% the proportion ofyoung people (under 18) who use tobacco products.
Nutrition: Increase to 75% the proportion of persons whofollow American Cancer Society guidelines with respect toconsumption of fruits and vegetables as published in theAmerican Cancer Society Guidelines on Nutrition andPhysical Activity for Cancer Prevention.
Physical Activity: Increase to 90% the proportion of youth(high school students) and to 60% the proportion of adultswho follow American Cancer Society guidelines withrespect to the appropriate level of physical activity aspublished in the American Cancer Society Guidelines onNutrition and Physical Activity for Cancer Prevention.
Comprehensive School Health Education: Increase to50% the proportion of school districts that provide acomprehensive or coordinated school health educationprogram.
Sun Protection: Increase to 75% the proportion of peopleof all ages who use at least two or more of the followingprotective measures which may reduce the risk of skincancer: avoid the sun between 10 a.m. and 4 p.m.; wearsun-protective clothing when exposed to sunlight; usesunscreen with an SPF 15 or higher; and avoid artificialsources of ultraviolet light (e.g., sun lamps, tanningbooths).
Breast Cancer Early Detection: Increase to 90% theproportion of women aged 40 and older who have breastscreening consistent with American Cancer Society guide-lines (by 2008).
Colorectal Cancer Early Detection: Increase to 75% theproportion of people aged 50 and older who have colorectalscreening consistent with American Cancer Societyguidelines.
Prostate Cancer Early Detection: Increase to 90% theproportion of men aged 50 and older who follow AmericanCancer Society detection guidelines for prostate cancer.

The health of young people, and the adults they willbecome, is critically linked to the establishment ofhealthy behaviors in childhood.9 Risk factors such astobacco addiction, unhealthy dietary patterns, and phys-ical inactivity during childhood and adolescence canresult in life-threatening cancers, cardiovascular disease,and other major illnesses later in life.9 Children whoadopt healthy habits at an early age are more likely tocontinue these behaviors throughout life. It is far easierto establish healthy practices initially than to changebehaviors later. For example:
• About half of youngsters who are overweight as chil-dren will remain overweight in adulthood,10 and 70%of those who are overweight by adolescence willremain overweight as adults.6
• Physically active children are more likely to grow up tobe physically active adults, whereas inactive childrenand youth are much more inclined to be sedentaryadults.11
• Almost 90% of current adult smokers became addictedto tobacco at or before age 18.12
Childhood is not only a formative period; it also presentsan opportunity to teach children healthy lifestyle habitsin school. There are more than 50 million students cur-rently enrolled in the nation’s public and private elemen-tary and high schools (grades K-12). The 129,000 schoolsin the US provide an organizational structure throughwhich health information and prevention programs canbe delivered.9
Furthermore, children are greatly influenced by theirsocial environment, which in turn is strongly influencedby public policies. For instance, adolescents are morelikely to initiate smoking if their film idols smoke in themovies, their favorite sport is sponsored by a tobaccocompany, they see people smoking around them, andtobacco products are cheap and readily available.12
Similarly, children are more likely to engage in sports andother forms of physical activity if safe and enjoyable par-ticipation in these activities is encouraged at school, inafter-school care programs, and in their communities.13
Children who can walk or bike to school safely are morelikely to do so.13 Community support, public health pol-icy, and legislation offer multiple opportunities toimprove the health behavior of future generations.
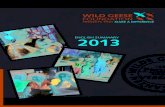
Youth Tobacco UseAlmost everyone who uses tobacco in the US began as anadolescent. In 2003, 21.9% of US high school studentsreported smoking at least one day in the last 30 days,with 9.7% reporting frequent smoking or smoking for 20or more of the last 30 days (Table 1A).14 According to theMonitoring the Future survey, cigarette smoking variesby race/ethnicity among US 12th graders, with the high-est prevalence among non-Hispanic whites, intermedi-ate prevalence among Hispanics/Latinos, and the lowestprevalence among African Americans (Figure 1A).
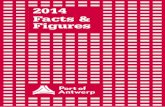
Trends Over TimeThe prevalence of current cigarette smoking hasdecreased among white, African American, andHispanic/Latino high school students from 1997 to 2003(Figure 1B).15 The decrease has occurred despite a majorincrease in tobacco company expenditures for promo-tion of cigarettes. Promotions specifically target youngpeople by sponsoring sporting events and by giving or
Cancer Prevention & Early Detection Facts & Figures 2005 3
Figure 1A. Current* Cigarette Smoking Among 12th Graders, by Race/Ethnicity, 1977-2003
Perc
ent
American Cancer Society, Surveillance Research
*Used cigarettes in the last 30 days.
Source: Monitoring the Future Survey, 1975-2003, National Institute on Drug Abuse.
12th grade, non-Hispanic white
12th grade, African American
12th grade, Hispanic/Latino
Year
0
5
10
15
20
25
30
35
40
45
200319971992198719821977
Children and Adolescents

4 Cancer Prevention & Early Detection Facts & Figures 2005
Table 1A. Tobacco Use, High School Students, by State and City, 2003% Current % Frequent % Current % Current smokeless
cigarette smoking* Rank† cigarette smoking‡ cigar use§ tobacco use ||
United States 21.9 9.7 14.8 8.7
State (out of 32 states)Alabama 24.7 21 12.6 13.0 10.5Alaska 19.2 5 8.0 7.8 11.2Arizona 20.9 10 7.3 14.2 4.8Delaware 23.5 17 12.1 12.2 3.4Florida 18.1 3 7.5 13.4 4.8Georgia 20.9 11 8.7 13.9 7.6
Idaho 14.0 2 6.1 8.7 5.7Indiana 25.6 25 12.4 14.7 7.2Kentucky 32.7 32 18.4 18.7 13.7Maine 20.5 9 10.1 11.1 4.3Massachusetts 20.9 12 9.5 11.8 4.1
Michigan 22.6 15 11.3 13.6 6.5Mississippi 25.0 24 12.0 18.4 8.2Missouri 24.8 22 13.6 13.3 5.7Montana 22.9 16 10.8 14.1 13.2Nebraska 24.1 19 11.2 18.2 10.1
Nevada 19.6 7 8.8 N/A 3.6New Hampshire 19.1 4 9.6 13.5 4.3New York 20.2 8 9.2 8.5 4.2North Carolina 24.8 23 12.4 N/A N/ANorth Dakota 30.2 31 16.0 13.0 10.3
Ohio 22.2 14 11.0 13.6 8.0Oklahoma 26.5 27 12.8 17.4 12.7Rhode Island 19.3 6 9.0 10.5 4.6South Dakota 30.0 30 14.7 13.8 15.3Tennessee 27.6 28 14.7 16.6 12.1
Texas¶ 24.3 20 7.9 14.6 6.8Utah 7.3 1 3.0 7.3 3.1Vermont 22.1 13 10.9 11.9 5.2West Virginia 28.5 29 17.7 13.3 13.6Wisconsin 23.6 18 11.6 N/A 7.9Wyoming 26.0 26 13.3 14.7 13.3
City (out of 18 cities)Boston, MA 13.1 6 3.8 8.8 2.2Chicago, IL 16.9 16 5.6 15.6 3.5Dallas, TX 18.1 18 4.0 17.0 2.7Dekalb County, GA 9.5 3 2.5 8.8 2.3Detroit, MI 9.1 1 1.7 7.2 3.2District of Columbia 13.2 7 3.8 11.2 5.0
Ft. Lauderdale, FL 13.4 9 5.3 10.6 3.7Los Angeles, CA 14.4 13 2.4 10.7 2.8Memphis, TN 9.2 2 2.3 13.1 1.5Miami, FL 13.5 10 4.6 10.2 2.4Milwaukee, WI 13.6 11 6.3 N/A 5.5New Orleans, LA 11.5 4 4.1 8.9 3.6
New York City, NY 14.8 14 5.3 5.5 1.6Orange County, FL 16.0 15 5.2 11.1 2.4Palm Beach, FL 17.0 17 8.2 14.2 3.5Philadelphia, PA 13.9 12 5.9 5.2 2.4San Bernardino, CA 12.4 5 3.1 10.4 3.7San Diego, CA 13.2 8 3.4 12.0 2.5
*Smoked cigarettes on one or more of the 30 days preceding the survey. †Rank is based on % current cigarette smoking. ‡Smoked cigarettes on 20 ormore of the 30 days preceding the survey. §Smoked cigars, cigarillos, or little cigars on one or more of the 30 days preceding the survey. ||Used chewingtobacco or snuff on one or more of the 30 days preceding the survey. ¶Survey did not include students from one of the state's largest school districts. N/A = Data not available. Note: Data are not available for all states since participation in the Youth Risk Behavior Surveillance System is a voluntarycollaboration between a state's departments of health and education.
Source: Youth Risk Behavior Surveillance System, 2003, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Controland Prevention. MMWR Morb Mortal Wkly Rep. 2004;53(SS-2).
American Cancer Society, Surveillance Research

exchanging for empty cigarette packs T-shirts, caps,sunglasses, key chains, and sporting goods bearing acigarette brand’s logo.16 In 2002, advertising and promo-tional expenditures topped $12 billion, nearly double theamount spent in 1997.17
The decreases in smoking among high school studentscan be attributed, at least in part, to rising cigaretteprices, restrictions on public smoking, and counter-advertising.18-20 In 2002 alone, 21 states – more statesthan in the previous 5 years combined – raised theircigarette taxes.19
Patterns of Smoking Initiation in YouthMany young people begin to experiment with cigarettesat very young ages. About 36% of middle or junior highschool students21 and 58% of high school students14 havetried cigarette smoking. Figure 1C shows that the pro-gression to established (current) smoking among adoles-cents is strongly associated with age. Experimentationappears to peak at age 13-14 while the proportion ofadolescents who are established smokers rises steadilyfrom age 11-18.22 The addictive and toxic properties oftobacco smoke may be even worse for adolescents,whose lungs are still developing, than for adults.
Recent research documents the highly addictive natureof cigarettes among adolescents.23 Progression to nico-tine dependence, once thought to develop over severalyears, has been shown to develop soon after initiationand to lead to smoking intensification. One studyshowed that approximately 20% of adolescents reported
nicotine dependence symptoms within 1 month ofinitiating regular smoking, with a median consumptionlevel at the onset of symptoms of only 2 cigarettes on 1day per week.24 Even adolescents who had smoked onlya couple of times reported some symptoms of nicotinedependence which increased in frequency with morefrequent smoking.25 These findings should be high-lighted in educating young people about the dangers ofexperimenting with tobacco.
Studies show that being exposed to tobacco industrypromotions increases the likelihood that adolescentswill experiment with cigarettes and transition fromexperimentation to regular smoking.22,26 One studyshowed that young people who were exposed to tobaccomarketing (owned a promotional item displaying atobacco logo or were able to name a brand whose adver-tisements attracted their attention) were more likely toinitiate smoking and more than twice as likely tobecome established smokers.26
Comprehensive Approach to Youth TobaccoControlAlthough recent trends in youth smoking have beenfavorable, US prevalence remains high.14 In the absenceof intervention, most adolescent smokers continuesmoking as adults.12 Studies have shown that compre-hensive tobacco control programs, including increasesin excise taxes, reduce the rates of adolescent smoking.5
States that have imposed higher excise taxes, thus rais-ing the price of cigarettes, generally have lower youth
Cancer Prevention & Early Detection Facts & Figures 2005 5
Figure 1B. Current* Cigarette Smoking Among High School Students, by Race/Ethnicity and Gender, 1991-2003Pe
rcen
t
American Cancer Society, Surveillance Research
*Smoked cigarettes on one or more of the 30 days preceding the survey.
Source: Youth Risk Behavior Surveillance System. MMWR Morb Mortal Wkly Rep. 2004;53(23):499-502.
0
5
10
15
20
25
30
35
40
45
50
1991 1995 1997
40 3940
32 31 30
37
32
26
38
33
11 12
17 18
13 14
28 28
22
16
23
33 32
28
35 3634
27
Hispanic/Latino male
Hispanic/Latina female
African American (non-Hispanic)
female
African American (non-Hispanic)
male
White (non-Hispanic)female
White (non-Hispanic)male
40
30
35
27
32
23
1411
1619
27
18 19
1993 2001 20031999

smoking prevalence. In addition to supporting increasedexcise taxes, advocacy for smoke-free school environ-ments and restrictions on youth access to tobaccoproducts are important factors in decreasing smokinginitiation and encouraging youth to quit smoking.5
School-based smoking prevention programs can beeffective as part of comprehensive tobacco control pro-grams.5 Because of the early age of cigarette initiation,smoking prevention classes must be taught from ele-mentary school to high school.5 The Surgeon Generalrecommends that tobacco use prevention begin at orbefore sixth grade. Currently, however, 25% of states donot require that tobacco use prevention be taught in ele-mentary schools.27 Because the long-term consequencesof smoking may seem remote to adolescent smokers,smoking prevention materials geared to youth shouldfocus on both short- and long-term consequences ofsmoking, such as lower sports performance, breath odor,being manipulated and exploited by the tobacco compa-nies, and reduced physical attractiveness due to stainingof teeth and fingers.23,28
Evidence suggests that antismoking media campaignsare effective in reducing smoking initiation in earlyadolescence.29 Children aged 12-13 years who reportexposure to effective counter-advertising on televisionare significantly less likely to progress to establishedsmoking over a 4-year period, with no effect observed
among older adolescents (14 to 15 years).29 States thathave utilized extensive paid media campaigns in com-bination with other anti-tobacco activities have seenrapid declines in youth smoking prevalence.30 In devel-oping its “Truth” campaign, the Florida Governor’sOffice worked with teen advisors to develop a mediacampaign that countered the image perception ofsmoking as cool and rebellious. Significant declines insmoking prevalence were reported among middle andhigh school students following implementation of theprogram,5 with a 40% reduction over 2 years among mid-dle school students.30
The state of Massachusetts initiated a multi-facetedyouth tobacco control program that included commu-nity-based efforts, statewide media campaigns, andschool-based tobacco education. The implementation ofthese efforts was associated with a decline in youthsmoking prevalence from 36% in 1995 to 30% in 1999.31
The television component of Massachusetts’ media cam-paign has been identified as an essential element inslowing the rate of progression to established smokingamong young adolescents.29
Recently, several of the most effective comprehensivetobacco control programs in the nation have beenjeopardized by severe budget cuts. The tobacco controlbudget in Massachusetts was cut from $48 million in2002 to $2.5 million in 2004; in Florida, the budget was
6 Cancer Prevention & Early Detection Facts & Figures 2005
Figure 1C. Progression to Established Smoking of US Youth by Age, 1999-2000Pe
rcen
t
American Cancer Society, Surveillance Research
*Students who have never smoked but are open to smoking and students who have tried a cigarette but have smoked fewer than 26 cigarettes in their lifetime. †Students who have smoked at least 100 cigarettes and smoked on 1 or more days in the 30 days preceding the survey. ‡Students who have smoked 100 cigarettes or more but have not smoked in the past 30 days.
Source: National Youth Tobacco Survey, 1999-2000. Centers for Disease Control and Prevention. Mowery et al. Progression to established smoking among US youths. Am J Public Health. 2004;94(2):331-337.
Experimenter* Current† Former‡
44.0
0
10
20
30
40
50
60
1817161514131211Age
26.9
39.3
48.7 50.2
45.6
41.038.0
13.8
1.61.22.5 2.9 3.7
18.8
22.9
28.2
7.8
3.30.40.9 0.20.4 0.0

cut from $37.5 million in 2003 to $1 million in 2004.32
After operating for 3 years, Minnesota’s Target Marketyouth anti-tobacco campaign ended in 2003, whenfunding was cut by more than 75%.33 Adolescents aged12-17 years were surveyed several times throughout thecampaign to ascertain their susceptibility to smoking(i.e., the percentage of youth who agree with the state-ment, “You will smoke a cigarette in the next year”). Sixmonths after the campaign was stopped, susceptibilityto smoking among adolescents had significantlyincreased from 43% to 53%.33
Cessation support is important for adolescents who arealready addicted to tobacco.34 In 2000, nearly 60% ofadolescent smokers made an unsuccessful attempt toquit in the previous year.21 School-based cessationprograms are an effective way to reach the majority ofadolescent smokers and equip them with the motivationand skills to quit.35
In order to increase the likelihood of successful cessa-tion, a full range of options, including pharmacotherapy,should be considered in treating nicotine dependence inadolescents.25 Although research on smoking-cessationinterventions for adolescents has been extremely lim-ited,36 a recent study showed that treatment with anicotine replacement patch appears effective in helpingadolescents quit.37
Parental guidance is important to maintain smoke-freehouseholds, set early nonsmoking expectations, monitoradolescents for signs of smoking, limit exposure to adultmedia, and counteract the influence of smokingdepicted in movies and other media as glamorous orgrown up.38 Prevention and cessation programs shouldaddress other tobacco products in addition tocigarettes.39
Other Tobacco ProductsWhile cigarettes remain the primary tobacco productused by youth, smokeless tobacco and cigars have gainedpopularity. Cigars are the second most popular type of
tobacco in all states, except South Dakota and Alaska,where smokeless tobacco is second to cigarettes.14
Tobacco usage varies by race and gender. Non-Hispanicwhite and Hispanic/Latino students smoke predomi-nantly cigarettes, while non-Hispanic AfricanAmericans are equally likely to smoke cigarettes andcigars. Male and female students were equally likely tosmoke cigarettes, but males were 5 times more likely touse smokeless tobacco and 2 times more likely to smokecigars than females. Table 1A provides data on currentand frequent cigarette smoking, current cigar use, andsmokeless tobacco use among high school students instates and cities for which these data are available for2003. A total of 27.5% of high school students reporteduse of any tobacco product in 2003.14 Other reports showthat among middle school students surveyed in 2002,13.3% reported current use of any tobacco product.Cigarette use was most commonly reported (10.1%),followed by cigars (6.0%), smokeless tobacco (3.7%), andpipes (3.5%).40
Alternative tobacco products such as bidis (small browncigarettes from India made of tobacco wrapped in a leafand tied with a thread) and kreteks (flavored cigarettescontaining tobacco and clove extract) are used less com-monly.40 Less than 5% of middle (2.4%) and high (2.6%)school students used bidis on one or more of the 30 dayspreceding the survey.40 Similarly, less than 5% of middle(2.0%) and high (2.7%) school students used kreteks onone or more of the 30 days preceding the survey.40 Allforms of tobacco are addictive and cause cancer andother life-threatening diseases. Moreover, use of othertobacco products among youth smokers may hasten theonset of nicotine dependence.41
Cancer Prevention & Early Detection Facts & Figures 2005 7
Youth-oriented counter-advertising is effective athelping decrease smoking prevalence among highschool students by changing perceptions about thesocial acceptability of cigarette use.

Overweight and Obesity, PhysicalInactivity, and Nutrition Among Youth
Overweight and ObesityThe proportion of children aged 6-19 who are overweighthas tripled over the past 3 decades (Figure 1D). Thepotential consequences to the health of the populationare enormous. Some of the adverse health conditionsseen in overweight and obese adults, such as type IIdiabetes and high cholesterol levels, are now alsoappearing in overweight and obese adolescents.44 Inaddition, because overweight children tend to becomeoverweight adults,6,10 the current increase in childhoodoverweight and obesity will result in future adult popu-lations with increased risk of developing cancer, heartdisease, type II diabetes, and other serious chronicdiseases.45,46
The dramatic increase in the percentage of overweightchildren and adolescents has occurred among boys andgirls of all age groups and races/ethnicities, althoughMexican Americans and African Americans experiencedthe greatest increase.47 Table 1B shows the percentagesof youth who are either at risk for overweight or who areoverweight in states and major cities in the US.
Obesity occurs when caloric intake exceeds caloricexpenditures (for metabolism and physical activity) overtime. Even a small excess in caloric intake consumed
over time may upset this delicate balance.48 Physicalactivity, by itself, cannot offset large excesses in caloricintake. For example, 45 minutes of moderate physicalactivity are needed to burn off the calories in a 20-ouncesoda.49 The largest sugar-containing soft drink servingand its free refill in some fast-food chains provide half ofan adult’s daily caloric (but not nutritional) needs.49
There is broad consensus among medical and publichealth experts that countering the obesity epidemicamong children and adolescents ought to be a nationalhealth priority. A Surgeon General’s report in 2001, andmore recently a report by the Institute of Medicine(IOM), have emphasized the need to develop a compre-hensive approach to address the problem.6,50 The IOMreport, Preventing Childhood Obesity: Health in theBalance, calls for coordinated efforts across schools,communities, industry, and governmental and non-governmental agencies to prevent and reduce obesity inAmerican youth.50
A combination of increasing physical activity and reduc-ing excess calorie consumption is needed to preventobesity in children. In 2003 the American Academy ofPediatrics released specific recommendations for theprevention of obesity in children.44 These include:
• Limiting television and video time to a maximum of 2hours per day
8 Cancer Prevention & Early Detection Facts & Figures 2005
Figure 1D. Overweight* Children and Adolescents, by Age Group, 1971-2002
Perc
ent
American Cancer Society, Surveillance Research
*Body mass index at or above the 95th percentile of growth chart for age and sex.
Source: National Health and Nutrition Examination Survey, 1971-1974, 1976-1980, 1988-1994, 1999-2000, 2001-2002, National Center for Health Statistics, Centers for Disease Control and Prevention. Hedley et al. Prevalenceof overweight and obesity among US children, adolescents, and adults, 1999-2002. JAMA. 2004;291(23):2847-2850.
1971-1974
1976-1980
1988-1994
1999-2002
0
2
4
6
8
10
12
14
16
18
12-19 years6-11 years2-5 yearsAge group
5.0 5.0
7.2
4.0
10.3
6.5
11.3
15.8
5.06.1
10.5
16.1
Success StoryHealthy Hawaii Initiative:Investing in PreventionHealthy Hawaii Initiative (HHI) is a school health programcreated in 1999 through funds from the MasterSettlement Agreement (MSA*) to promote health andreduce chronic disease among students and faculty. In itsfirst 3 years, the program provided professional develop-ment and teaching resources to health educators in avariety of settings, facilitated conferences to addressstatewide school health, and piloted and implementedcoordinated school health programs.42 In addition to theHHI, 25% of MSA funds were allocated for tobaccoeducation, prevention, and cessation programs.
*The 1998 settlement of a lawsuit launched by 46 stateAttorney Generals against large tobacco companies fortheir deceptive practices and to recover Medicaidexpenses due to smoking-induced illnesses43

Cancer Prevention & Early Detection Facts & Figures 2005 9
Table 1B. Overweight and Related Factors, High School Students, by State and City, 2003% Watched % % % Eating
% three or % % Attended Played five or more At risk for more hours Moderate Vigorous physical on one or fruits andbecoming % per day of physical physical education more sports vegetables
overweight* Overweight† Rank‡ television§ activity|| activity¶ classes daily teams# a day**
United States 15.4 13.5 38.2 24.7 62.6 28.4 57.6 22.0
State out of 31 statesAlabama 14.5 13.5 24 41.7 18.6 58.0 33.3 56.3 14.5Alaska 14.4 11.0 14 27.5 28.2 67.8 18.2 62.8 16.1Arizona 13.6 10.8 12 36.6 29.2 66.9 23.2 51.7 20.4Delaware 16.7 13.5 25 45.4 22.6 57.2 28.7 53.4 19.5Florida 14.0 12.4 19 42.7 22.3 60.8 27.3 51.2 20.7Georgia 15.1 11.1 15 42.4 25.4 59.0 29.1 53.1 16.8Idaho 11.3 7.4 3 23.7 29.5 66.4 29.5 58.5 19.0Indiana 14.2 11.5 17 32.9 26.5 62.3 23.7 57.1 20.3
Kentucky 15.3 14.6 29 30.8 21.3 56.1 23.8 50.9 13.2Maine 14.6 12.8 22 26.3 24.6 60.6 8.2 56.7 22.6Massachusetts 13.8 9.9 8 31.3 23.5 61.3 13.7 53.7 N/AMichigan 15.0 12.4 20 34.8 25.6 62.3 27.5 N/A 18.4Mississippi 15.7 15.7 31 54.1 18.0 53.3 23.4 54.0 20.4Missouri 14.9 12.1 18 32.4 28.1 66.6 33.2 51.8 15.0Montana 11.6 8.1 4 25.3 23.9 62.3 32.6 60.5 16.7Nebraska 14.7 10.4 10 28.0 26.7 64.7 36.4 62.0 16.3
Nevada N/A N/A N/A N/A 27.2 66.6 N/A N/A N/ANew Hampshire 13.4 9.9 9 26.4 26.1 64.1 N/A 56.9 N/ANew York 15.4 12.9 23 43.6 22.8 64.5 18.5 57.7 24.3North Carolina 14.7 12.5 21 N/A 22.3 61.2 30.5 N/A 17.8North Dakota 11.0 9.3 5 21.3 29.0 63.6 37.2 60.8 17.3Ohio 13.1 13.9 27 32.1 N/A 67.6 31.5 62.6 N/AOklahoma 14.2 11.1 16 36.7 25.1 64.3 29.8 55.6 14.3Rhode Island 14.5 9.8 7 31.9 22.3 62.2 21.1 55.5 28.4
South Dakota 14.5 9.4 6 28.1 26.5 62.2 16.3 64.9 17.1Tennessee 14.8 15.2 30 44.3 24.0 61.1 28.7 50.7 18.1Texas†† 16.4 13.9 28 44.1 20.2 59.9 29.7 54.0 17.5Utah 11.3 7.0 1 22.9 29.3 71.1 25.8 62.9 20.3Vermont 14.1 10.8 13 N/A 26.6 65.4 14.6 N/A 26.5West Virginia 15.1 13.7 26 33.9 27.4 66.3 28.6 52.7 20.6Wisconsin 13.7 10.4 11 N/A 28.2 63.4 N/A 61.7 N/AWyoming 11.7 7.2 2 26.6 28.3 67.7 23.2 56.3 22.5
City out of 18 citiesBoston, MA 18.0 14.2 11 50.0 19.2 50.2 9.2 44.5 N/AChicago, IL 17.9 13.9 10 52.5 18.4 46.3 49.9 51.9 17.7Dallas, TX 19.9 15.9 16 57.5 16.2 54.2 11.2 46.6 16.1Dekalb County, GA 16.6 12.1 5 55.8 23.2 57.9 25.9 55.8 17.2Detroit, MI 19.5 19.9 18 65.0 22.4 49.8 28.5 N/A 18.5Dist. of Columbia 16.8 13.5 8 56.7 15.5 44.4 18.8 45.3 21.3
Ft. Lauderdale, FL 16.0 9.3 1 50.6 20.4 54.7 27.0 46.5 22.5Los Angeles, CA 17.0 15.8 14 50.4 20.8 58.8 51.0 47.9 19.1Memphis, TN 18.6 15.8 15 65.5 21.3 53.9 24.0 48.5 14.5Miami, FL 15.3 12.9 6 53.7 17.1 53.5 13.9 44.1 22.2Milwaukee, WI 19.3 16.2 17 N/A 23.0 52.3 N/A 51.5 N/ANew Orleans, LA 18.2 13.8 9 64.9 14.9 40.1 22.6 44.5 29.1
New York City, NY 16.2 13.3 7 59.1 22.9 61.0 48.9 45.5 25.9Orange County, FL 14.2 10.9 3 43.7 22.9 58.2 22.3 48.9 17.9Palm Beach, FL 14.9 11.2 4 44.2 20.8 57.9 18.8 49.4 23.1Philadelphia, PA 18.6 15.1 12 59.9 21.2 50.6 24.5 45.1 17.1San Bernardino, CA 20.6 15.4 13 51.5 22.2 57.3 48.0 49.8 18.9San Diego, CA 15.7 9.6 2 41.8 27.2 65.8 44.9 52.4 18.7
*Body mass index at or above the 85th percentile but below the 95th percentile of growth chart for age and sex. †Body mass index at or above the 95th percentile ofgrowth chart for age and sex. ‡Rank is based on % overweight. §During an average school day. ||Activities that did not make students sweat and breathe hard for 30 min-utes or more on 5 or more of the 7 days preceding the survey. ¶Activities that made students sweat and breathe hard for 20 minutes or more on 3 or more of the 7 dayspreceding the survey. #During the 12 months preceding the survey. **Had eaten 5 or more servings per day of green salad, potatoes (excluding French fries, fried potatoes,or potato chips), carrots or other vegetables, 100% fruit juice, or fruit during the 7 days preceding the survey. ††Survey did not include students from one of the state'slargest school districts. N/A = Data not available. Note: Data are not available for all states since participation in the Youth Risk Behavior Surveillance System is a voluntarycollaboration between a state's departments of health and education.Source: Youth Risk Behavior Surveillance System, 2003, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention.MMWR Morb Mortal Wkly Rep. 2004;53(SS-2).
American Cancer Society, Surveillance Research

• Routinely promoting physical activity, includingunstructured play at home, in school, in childcaresettings, and throughout the community
• Encouraging parents and caregivers to promotehealthy eating patterns by offering nutritious snacks,such as vegetables and fruits, low-fat dairy foods, andwhole grains; encouraging children’s autonomy in self-regulation of food intake and setting appropriate lim-its on choices; and modeling healthy food choices
10 Cancer Prevention & Early Detection Facts & Figures 2005
• Identifying children and adolescents in the health caresetting who are at risk due to family history, birthweight, or socioeconomic, ethnic, cultural, or environ-mental factors and tracking them annually by calcu-lating and plotting BMI
• Enlisting policymakers from local, state, and nationalorganizations and schools to support healthy lifestylesfor all children, including proper diet and adequateopportunities for regular physical activity
Television Viewing: A Modifiable Risk FactorWatching television is one modifiable factor that maycontribute to obesity in children.52 On average, childrenand adolescents spend more time in front of a televisionthan in any other activity besides sleeping.53 Televisionwatching competes with other activities that involvephysical activity. It bombards children and adolescentswith advertisements for high-calorie, low-nutrient foods,and it encourages between-meal snacking.54 The ThirdNational Health and Nutrition Examination Survey, con-ducted from 1988 to 1994, found that more than 25% ofchildren in the US watched at least 4 hours of televisionper day; children who watched 4 or more hours of tele-vision per day had a significantly greater body massindex than those who watched less than 2 hours perday.55 Having a television in a child’s bedroom is a strongpredictor of the child being overweight.44
Three or more hours oftelevision watching perday is considered indica-tive of sedentary behavior.The proportion of highschool students whowatch 3 hours or more oftelevision daily correlatedsignificantly with the pro-portion who were over-weight or at risk ofbecoming overweight inthe 28 states for whichdata were available in2003 (Figure 1E). Itshould be noted that theassociation between theprevalence of overweightyouth and the proportionof high school studentswho watch 3 or morehours of television per day
Figure 1E. Combined Youth Overweight* Versus Three or More Hours of Television Watching, by State, 2003
Wat
ched
th
ree
or
mo
re h
ou
rs o
f te
levi
sio
n p
er d
ay (
per
cen
t)
American Cancer Society, Surveillance Research
*Body mass index at or above the 85th percentile of growth chart for age and sex. Note: See Statistical Notes on page 47 for explanation of correlation.
Source: Youth Risk Behavior Surveillance System, 2003, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2004;53(SS-2).
Overweight and at risk for becoming overweight (percent)
R2 = 0.6028
p < 0.01
0 5 10 15 20 25 30 350
10
20
30
40
50
60
Body Mass Index (BMI) for Youth andAdolescentsAs children grow and mature, their body compositionchanges dramatically. The definitions of overweight andobesity are different for youth than for adults. Growthcharts showing the entire distribution of height, weight,and body mass index were revised in 200051 and areavailable at the CDC’s National Center for Health statisticsWeb site at www.cdc.gov/growthcharts. These growthcharts are the recommended approach to evaluate over-weight and obesity in children and youth. In this report,the following definitions are used:
• Overweight: 95th or higher percentile for BMI
• At risk of becoming overweight: 85th to 94th percentilefor BMI

replaced by more sedentary activities, such as playingvideo games, watching television or videotapes, or usinga computer. Although participation in organized sportsoffers many social and physical benefits to children whoparticipate,62 it is critical that schools and communitiesoffer a wide range of physical activities (i.e., dance, mar-tial arts, walking or running clubs) to all children, notonly to those who are athletic.
The potential influence of the physical environment onhealth has been recognized only recently.63 Urbansprawl, one aspect of the physical environment, reducesopportunities to walk or bike from home to school,shopping, or other destinations.64 According to the 2001National Household Travel Survey, children’s walkingtrips have declined by 60% since 1977; walking andbiking to school have declined by 50% since 1969.48 Arecent study found that fewer than 10% of WestVirginian students walked to school and that those whodid spent less than 10 minutes walking.65 In NorthCarolina, 12.1% of middle school and 6.4% of high schoolstudents walked or biked to school at least once a week,while only 3.5% of middle school and 1.6% of high schoolstudents walked to school 5 times a week.66 Distance,traffic safety, and fear of crime are factors that con-tribute to the declining rates of physical activity64,67 andthat must be addressed. Improvements in neighborhoodsafety are essential to provide children with opportuni-ties for physical activities.68
For many communities, environmental changes such asincreased housing density, walking and bicycle trails,and urban redesign will require long-term planning andinvestment.69 Recently, the Institute of Medicine rec-ommended that local governments, working with devel-opers and community groups, should increaseopportunities for physical activity by revising zoningordinances to increase availability and accessibility ofphysical activity in new developments, prioritizing capi-tal improvements to increase physical activity in existingareas, and building schools where they can be reachedsafely on foot by the communities they serve.50
One place to start fostering an environment that pro-motes physical activity is in schools, where childrenspend the majority of their time.70 A study conducted inSan Diego found that children in middle schools withadequate space, facilities, equipment, and supervisionwere 4 to 5 times more likely to be physically active atschool during free time than children in schools withinadequate space and supervision.71
Cancer Prevention & Early Detection Facts & Figures 2005 11
does not prove causation. However, it does identify animportant issue for further study.
Television viewing has been associated with poor eatinghabits and greater consumption of fast food and softdrinks. One study found that daily servings of fruits andvegetables decreased significantly among adolescentswith each additional hour of television viewed per day.56
Physical ActivityThere are no national estimates of physical activity levelsamong children younger than 12 because self-reports inthis age group are less reliable than in older children oradolescents.57 Based on Youth Risk Behavior Sur-veillance System data from 2003, more than half of highschool students are considered vigorously active, and20%-25% are moderately active on a regular basis (Table1B). Nationally, 57.6% of high school students reportedplaying on one or more sports teams during 2003, withhigher participation rates among males (64.0%) thanfemales (51.0%).14
Limited data suggest that physical activity decreasesprogressively from ages 12 to 21.58 One longitudinalstudy has documented that only a small proportion ofUS adolescents who achieved the recommended amountof physical activity continued to do so into adulthood.59
Another longitudinal study reported substantialdeclines in physical activity levels among white andAfrican American girls from ages 9-10 to ages 19-20.60
The decrease was largest among African American girlsover the 10-year period. This study also found thatsmoking initiation in adolescence was associated with adecline in physical activity levels.60 Other factors con-tributing to declines in physical activity among youthinclude the increasingly sedentary nature of leisure-timeactivities, decreases in daily-living activities such aswalking or biking to school and doing household chores,and changes in availability and requirements of schoolphysical education programs.44,61 Vigorous physicalactivity, such as playing basketball, may have been

Many schools have increased time for academic instruc-tion and limited recess, unstructured playtime, andphysical education classes. Most school districts do notprovide time for daily physical education for students inkindergarten through 12th grades.11 In 2003, only 28.4%of high school students attended physical educationclass daily (Table 1B),14 down from 41.6% in 1991.72
Nationwide in 2000, only 8% of elementary schools, 6.4%of middle/junior high schools, and 5.8% of senior highschools provided daily physical education, althoughnearly three-quarters (71.4%) of elementary schoolsprovided regularly scheduled recess to all students.27
Results from a recent study suggest that participation inschool-based physical activity may help to prevent over-weight in youth. The study followed a nationally repre-sentative cohort of children from kindergarten to first
grade and found that increasing physical educationinstruction time by one hour in first grade comparedwith kindergarten significantly reduced BMI amonggirls who were overweight or at risk for overweight.73
This effect was not seen among boys due to boys beingmore active than girls at young ages. Furthermore, thestudy estimated that if school physical education pro-grams nationwide were expanded so that every kinder-garten child receives a minimum of 5 hours of PEinstruction weekly, the prevalence of overweight amonggirls could be decreased by 43% and the prevalence ofchildren who are at risk for overweight could bedecreased by 60%.73 Parents can advocate for schoolpolicies that require daily physical education or thatencourage the development of competitive and non-competitive activities.74
12 Cancer Prevention & Early Detection Facts & Figures 2005
Success StoriesWith the increasing recognition of childhood obesity, manyprograms have begun to address the problem. This sectionhighlights some of these efforts.
CDC’s Kids Walk-to-School ProgramSince only 1 out of every 10 trips to school are made by walk-ing or bicycling, the Centers for Disease Control and Prevention(CDC)’s Kids Walk-to-School program seeks to increase oppor-tunities for daily physical activity by encouraging children towalk to and from school in groups accompanied by adults.75
Another goal of the program is to encourage communities to create an environment that supports safe walking and biking to school. The online guide (available at www.cdc.gov/nccdphp/dnpa/kidswalk) provides step-by-step details on howto organize a Kids Walk-to-School Program, including safetyinformation and an extensive list of resources to assist withprogram development.
The PATH ProgramPATH (Physical Activity and Teenage Health) is a school-basedintervention focused on urban teenage girls in New York Citythat has shown significant improvements in heart healthknowledge, eating habits, percentage of body fat, and bloodpressure compared with traditional school physical educationprograms.76 The PATH program presents a school-based healthpromotion and personal wellness program intended to reducethe occurrence of unhealthy behaviors, and to prevent theonset of risk factors for coronary artery disease among urbangirls through an integrated program of exercise and hearthealth-related education. Many of the risk factors addressed bythis program also apply to cancer.
CDC’s VERBTM CampaignVERB, a 5-year media campaign initiated by the CDC inOctober 2002, promotes physical activity through research,media, partnership, and community efforts. VERB advertise-ments aimed at children portray physical activity as being“cool,” fun, and socially appealing, while advertisementsaimed at parents encourage them to engage in physical activ-ity with their children and suggest ways to overcome perceivedbarriers to physical activity. This campaign also addresses otherimportant environmental factors, such as access to safe andaffordable opportunities for both leisure-time and organizedphysical activities.
The outcomes of this media campaign are being measured 3times by the Youth Media Campaign Longitudinal Survey(YMCLS), a telephone survey of children aged 9 to 13 and theirparents. Baseline data from spring 2002 showed that whilemost participants engage in some free-time physical activity(77.4%), the majority of children 9-13 years do not participatein any organized physical activity outside of school (61.5%).Data from the spring 2003 and spring 2004 surveys have notbeen published. However, initial evaluation data from thespring 2003 survey indicate that the program shows potentialin shrinking the gap in physical activity levels between boys andgirls. Communities receiving enhanced levels of VERB market-ing activity showed even more promise. Future YMCLS reportswill provide more insight into the effectiveness of the mediacampaign. More information about the VERB campaign is avail-able at www.cdc.gov/youthcampaign.
While these results are encouraging, continued awareness andincreased participation rates in both free-time and organizedphysical activities are needed to curb the youth obesityepidemic.

Several new initiatives are attempting to consolidate andmake available resources to help individuals, communi-ties, organizations, and politicians address the obesityproblem of America’s youth.
• SAY (Shaping America’s Youth) is a nationwideinfrastructure that has begun to identify and central-ize information about organizations, agencies, andbusinesses that address inactivity and obesity amongyouth. More than 1,800 active programs, representingall 50 states, have registered to be included in thesearchable database available at www.shapingameric-asyouth.com.
• Action for Healthy Kids (AFHK) assists schools infinding solutions to improve students’ health andreadiness to learn through daily physical activity,quality health and physical education, and increasedavailability of healthy foods and beverages. A reportfrom the AFHK program documenting successes inimproving school attendance, raising standardizedtest scores, and reducing behavior problems can beaccessed at www.actionforhealthykids.org.
• PAY (Physical Activity for Youth Policy Initiative)provides advocates and policymakers with the ration-ale, recommended policy options, and examples ofcurrent programs, legislation, or laws in order to assistwith the integration of physical activity awareness andaction in afterschool programs, community programs,community design, and school programs. The docu-ment and accompanying policy resource guide can be obtained at www.ncppa.org/publicaffairspolicy_index.asp.
Healthy Eating PatternsMajor changes in the diet of youth have been docu-mented over the past 2 decades, including increases inoverall energy intake, added sugars, sodium, soft drinks,fruit juices, and fast foods and decreases in the amountsof fruits, vegetables, and milk consumed.77-79 Snack foodconsumption has doubled in the last 20 years, andAmerican children are consuming more meals awayfrom home.78,80 Less than one-fourth (22%) of US highschool students ate 5 or more servings of vegetables andfruits per day in 2003 (Table 1B).
Among the recommendations to improve eating pat-terns among children and adolescents are to: 1) limitchildren’s consumption of fast foods; 2) promote health-ier food choices in school cafeterias; 3) decrease avail-ability and consumption of sugar-sweetened beverages;and 4) limit and monitor food and beverage advertisingto children.6,44,50
1. Limit children’s consumption of fast foods.
Meals eaten away from home are generally less healthythan home-cooked food.78 Research shows that 30% ofchildren and adolescents consume fast food on a typicalday.81 Children who eat fast food consume more totalcalories, total fat, and added sugars, as well as moresugar-sweetened beverages, less milk, and fewer fruitsand nonstarchy vegetables.81 A recent study found thatwhen eating fast food, adolescents, regardless of theirbody weight, tended to eat too much, consuming roughly60% of their estimated total daily caloric needs in asingle sitting.82 Unlike leaner participants, those whowere overweight did not reduce their energy intakeduring the rest of the day, consuming an average of 400excess calories. Eating fast food may maintain or exacer-bate obesity.82 Parents should limit their children’sconsumption of fast food and ensure that healthy foodchoices are available and accessible at home for mealsand snacks.83
2. Promote healthier food choices in school cafeterias.
Foods high in fat, sugar, sodium, and calories are not onlypopular among adolescents but also generate substan-tial revenue for schools.84 In 43% of elementary schools,74% of middle schools, and 98% of high schools, studentshave access to vending machines and/or snack barswhere they can purchase food or beverages that are highin fat, salt, and added sugar.27 A study of students transi-tioning from elementary to junior high (where theygained access to school snack bars) documented dra-matic decreases in the consumption of fruit (33%),
Cancer Prevention & Early Detection Facts & Figures 2005 13

vegetables (42%), and milk (35%), while the amount offried vegetables and sweetened beverages consumedincreased by 68% and 62%, respectively.85 Another studyfound that students attending schools without “a lacarte” programs consumed a diet higher in fruits andvegetables compared with students who had access to “ala carte” programs.86 This study also found that students’mean intake of fruit and vegetable servings declined by11% for each additional snack vending machine presentin a school.86
3. Decrease availability and consumption of sugar-sweetened beverages, including soft drinks.
Between 56% and 85% of school-age children consumeat least one nondiet soft drink daily, adding calories withno nutritive value to their diet.87 A 19-month follow-upstudy of Massachusetts school children found significantincreases in both body mass index (BMI) and obesity foreach additional daily serving of a sugar-sweeteneddrink.88 A longitudinal study of adolescents found thatsoda consumption was significantly related to BMI.89
NHANES data also shows that the contribution of softdrinks to total energy (calorie) intake is highest amongoverweight children.90 A targeted, school-based educa-tional intervention that reduced the number of carbon-ated drinks consumed also prevented further weightgain in the children compared to the controls.91
One intervention that has been adopted by a number ofschool districts (including Los Angeles, New York City,Oakland, and Philadelphia) is to eliminate sales of sugar-sweetened drinks in schools. A report issued from the USGeneral Accounting Office stated that food sales werethe most prevalent form of commercial activity in
14 Cancer Prevention & Early Detection Facts & Figures 2005
Success StoriesUSDA’s Fruit and Vegetable Pilot Program(FVPP)The USDA (a partner in the 5 A Day for Better HealthProgram) created the FVPP through a $6 million grant fromthe 2002 Farm Act to provide fresh and dried fruits andvegetables free to children in 107 elementary and second-ary schools in 4 states as well as in 1 tribal organization.These foods are delivered through classroom service,kiosks, and free vending machines. Schools participating ina 1-year pilot program reported that 80% of studentswere very interested in the program and that more than90% of fruit and vegetable offerings were consumed.One-third of the schools reported that the programincreased the likelihood of student participation in theschool meal program, and almost 80% of schools reportedthat the program increased the acceptance of fruits andvegetables offered as part of school meals. Virtually all ofthe schools advocated for continuation of the program,and in June of 2004, Congress passed legislation makingthe program permanent and expanding it to include 8states and 3 tribal organizations with an additional $3 mil-lion in annual funding.96 For more information about thisand other 5 A Day for Better Health programs, see page32 in the adult section on fruit and vegetable consumptionor visit www.5aday.gov.
TACOS (Trying Alternative Cafeteria Optionsin Schools)TACOS is a high-school-based intervention that was ableto increase the number of lower-fat “a la carte” foodoptions by 50% in target schools located in theMinneapolis-St. Paul metropolitan area. The program doc-umented increased sales of these foods and increasedacceptability of lower-fat foods by students and schoolpersonnel. The findings indicate that changes in the schoolenvironment can positively influence food choices with noadverse effects on food service revenues.97
Florida – Eat Your Colors EverydayThis school-based pilot program, initiated in 2002 througha grant from the Florida Department of Agriculture andConsumer Services, has continued to expand throughoutFlorida and into other states across the nation (Kansas,Oregon, and South Carolina in 2003-2004). The programis designed to increase student consumption of fresh fruitsand vegetables by implementing, enhancing, and expand-ing salad bars, salad options, and nutrition educationactivities in elementary, middle, and high schools.Evaluations of the pilot program found an increase instudent fruit and vegetable consumption ranging from 9%to 31% at the school level, as well as an increase in thepercent of students eating more than 50% of their fruitsand vegetables following the intervention. More informa-tion can be obtained at www.5aday.com/html/industry/floridastats.php.

schools; these were primarily soft drinks sold from vend-ing machines and at fundraising events.92 Fifty percentof school districts have contracts with companies thatallow the companies to sell soft drinks in the schools andto advertise in schools and on school grounds. In return,schools and districts receive incentives and/or a per-centage of the sales revenue.27 Only 19 states havepolicies regarding commercial marketing activities inschools.92 A new policy statement from the AmericanAcademy of Pediatrics recommends that school districtsconsider restricting the sale of soft drinks to safeguardagainst health problems that result from overconsump-tion among children.87 Nutritious alternatives such aswater, real fruit juice, and low-fat milk can be sold inplace of soft drinks to help maintain school revenues.87
4. Limit and monitor food and beverage advertisingto children.
Studies have reported that students in grades 7-12 whofrequently eat fast food tend to watch more televisionthan other students93 and that middle-school childrenwho watch more television tend to consume more softdrinks.94 One factor that may explain these associationsis increased exposure to youth-directed food advertisingamong children who watch more television. A study offood advertising directed at youth during Saturdaymorning children’s television programming found thatalmost one-third of the ads were for foods high in fat andsugar, such as candy, soft drinks, chips, cookies, fastfoods, and high-sugar breakfast cereals. During this timeframe, an estimated exposure to food advertising occursonce every 5 minutes.95 The Institute of Medicine hasrecommended that national guidelines be developedconcerning food and beverage advertising and market-ing to children. These guidelines would be implementedby industry and monitored by the Federal TradeCommission.50
Sun ProtectionThe vast majority of skin cancers are due to unprotectedand excessive ultraviolet (UV) radiation exposure. WhileUV exposure is associated with a small percentage of allcancer deaths,98 the American Cancer Society estimatesthat UV exposure is associated with more than 1 millioncases of basal and squamous cell cancers and 59,580cases of malignant melanoma annually.1 Artificialsources, such as tanning booths, add to UV exposure.The short-term adverse effects from unprotected UVexposure are sunburn and tanning, while long-termexposure can cause prematurely aged skin, wrinkles, andskin cancer. Though it was once believed that dark
brown or black skin prevented melanoma, more recentresearch indicates that darker-skinned people candevelop this cancer, especially on the hands, soles of thefeet, and under the nails.
Regular practice of sun protection behaviors can lead tosignificant reductions in sun exposure and risk of skincancer (see sidebar on page 16). Sunburn during child-hood and intense, intermittent sun exposure increasethe risk of melanoma and other skin cancers.99-101
Because much exposure to sunlight occurs during child-hood and adolescence, protection behaviors shouldbegin early in life. However, a CDC study revealed that25% of parents did not require their children aged 12 oryounger to use sun protective behaviors, and the pro-portion of children who used one or more protectivebehaviors decreased with age.102
Adolescence is a period of heightened unprotected sunexposure.103 An American Cancer Society study showedthat less than one-third of youth aged 11 to 18 used anytype of sun protection measures.104 The Youth RiskBehavior Surveillance System found that only 15% ofpublic and private high school students used sunscreenof SPF 15 or higher “most of the time” or “always” whenthey were outdoors in the sun for more than an hour.105
In another study, almost three-quarters (72%) of youthreported getting sunburned during the summer months.Of those, more than one-third (39%) reported usingsunscreen lotion of SPF 15 or higher when they gotburned.106 It is important that adolescents be educatedabout proper application and re-application intervals forsunscreen.107,108
Cancer Prevention & Early Detection Facts & Figures 2005 15

To improve sun protection practices among children andadolescents, the CDC has made recommendations todevelop comprehensive programs that include schoolintervention components.109 However, policies for sunsafety programs do not exist in the majority of elemen-
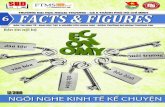
tary, junior/middle, or senior high schools (Figure 1F). Instates where UV exposure is high year-round, parentsshould work with schools to develop sun protectionprograms at all grade levels and should establish propersun protection practices for their own children.
16 Cancer Prevention & Early Detection Facts & Figures 2005
Source: Centers for Disease Control and Prevention. School Health Policies and Programs Study, 2000. National Center for Chronic Disease Prevention and Health Promotion.
Figure 1F. Policies for Required Sun Safety or Skin Cancer Prevention in Schools, by State, 2000
AL
AZAR
CA CO
CT
DE
FL
GA
ID
IL IN
IA
KS
KY
LA
ME
MD
MA
MI
MN
MS
MO
MT
NENV
NH
NJ
NM
NY
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WIWY
DC
HI
AK
Elementary and middle or high schools
Middle or high schools only
No policies
Risk Factors and Prevention Measures for Melanoma and Other Skin Cancers
Risk factors for melanoma110
• Light skin color
• Family history of melanoma
• Personal history of melanoma
• Presence of moles and freckles
• History of severe sunburn occurring early in life
Risk factors for basal and squamous cell cancers110
• Chronic exposure to the sun
• Family history of skin cancer
• Personal history of skin cancer
• Light skin color
Measures to prevent skin cancer• Avoid direct exposure to the sun between the hours
of 10 a.m. and 4 p.m., when ultraviolet rays are themost intense.
• Wear hats with a brim wide enough to shade the face, ears, and neck, as well as clothing thatcovers as much as possible of the arms, legs, andtorso.
• Cover exposed skin with a sunscreen lotion with a sun protection factor (SPF) of 15 or higher.
• Avoid tanning beds and sun lamps, which providean additional source of UV radiation.

Cancer Prevention & Early Detection Facts & Figures 2005 17
Tobacco UseTobacco use is the single largest preventable cause ofdisease and premature death in the US. Each year,according to the Surgeon General, it accounts for an esti-mated 440,000 premature deaths related to smoking,38,000 deaths in nonsmokers as a result of exposure tosecondhand smoke, and $157.7 billion in health-relatedeconomic losses.111 Tobacco use causes increased risk ofcancer of the lung, mouth, nasal cavities, larynx, phar-ynx, esophagus, stomach, liver, pancreas, kidney, bladder,and uterine cervix, as well as myeloid leukemia.112 Thirtypercent of cancer deaths, including 87% of lung cancerdeaths, can be attributed to tobacco (Figure 2A).2,112,113
Both cigarette consumption and the prevalence of smok-ing in the US have declined since the release of the firstUS Surgeon General’s Report on Smoking and Health in1964, although recent decreases have been greater fortobacco consumption than for prevalence.114 Per-capitacigarette consumption is currently lower than at anypoint since the start of World War II. Nonetheless, an
estimated 25% of men and 20% of women still smokecigarettes, with approximately 82% of these individualssmoking daily.115
Smoking prevalence varies by level of education.Interestingly, though, this relationship has reversed overtime. In the early 1960s, college-educated adults had thehighest smoking prevalence. By 2002, only 9.9% of collegegraduates were current smokers, compared to 31% ofthose who did not graduate from high school (Figure2B).116 Smoking prevalence is higher among men thanwomen, and varies by race, ethnicity, and socioeconomicstatus (Table 2A). The prevalence of smoking is highest
Adult Cancer PreventionC
ance
r si
te
Figure 2A. Annual Number of Cancer Deaths* Attributable to Smoking, Males and Females, by Site, US, 1995-1999
*Among men and women 35 and older.
Source: US Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office of Smoking and Health, 2004. American Cancer Society, Surveillance Research
0 20 40 60 80 100
Male
Number of deaths (in thousands)
Oropharynx
Esophagus
Stomach
Pancreas
Larynx
Lung
Bladder
Kidney
Myeloid leukemia
Can
cer
site
0 20 40 60 80 100
Female
Number of deaths (in thousands)
Oropharynx
Esophagus
Stomach
Pancreas
Larynx
Lung
Bladder
Kidney
Myeloid leukemia
Cervix
Attributable to cigarette smoking
Other causes

18 Cancer Prevention & Early Detection Facts & Figures 2005
among American Indian/Alaska Native men andwomen, and lowest among Asian American men andwomen.115 Across the states, smoking prevalence rangesfrom 12% in Utah to 31% in Kentucky (Table 2B).
Comprehensive Tobacco ControlFurther reductions in tobacco use will require imple-mentation of economic, policy, and regulatory interven-tions that reduce tobacco use and protect nonsmokersfrom secondhand smoke.5 The goals of comprehensivetobacco control5 are to:
• Prevent the initiation of tobacco use among youngpeople
• Promote quitting among young people and adults
• Eliminate nonsmokers’ exposure to environmentaltobacco smoke (ETS)
• Identify and eliminate the disparities in tobacco useand its effects among different population groups
• Facilitate smoking cessation
Best practices for comprehensive state tobacco controlprograms have been published by the Centers for DiseaseControl and Prevention (CDC).117 The CDC recommendsthat states establish tobacco control programs that arecomprehensive, sustainable, and accountable. Effectivestate-based programs include the following compo-nents: community and school programs and policies,
Table 2A. Current Cigarette Use*, Adults 18and Older, US, 2002
Characteristic % Men % Women % Total
Age group (years)18 to 24 32.4 24.6 28.525 to 44 28.7 22.8 25.745 to 64 24.5 21.1 22.765 or older 10.1 8.6 9.3
Race/EthnicityWhite (non-Hispanic) 25.5 21.8 23.6African American (non-Hispanic) 27.1 18.7 22.4Hispanic/Latino 22.7 10.8 16.7American Indian/Alaska Native† 40.5 40.9 40.8Asian American‡ 19.0 6.5 13.3
Education (years)§
8 or fewer 25.4 13.5 19.39 to 11 38.1 30.9 34.112 29.8 22.1 25.613 to 15 24.8 21.6 23.116 or more 13.6 10.5 12.1more than 16 7.8 6.4 7.2
Total 25.2 20.0 22.5
*Persons who reported having smoked at least 100 cigarettes or moreand who reported now smoking every day and/or some days.†Estimates should be interpreted with caution because of the smallsample sizes. ‡Does not include Native Hawaiians and other PacificIslanders. §Persons aged 25 or older.
Source: National Health Interview Survey, 2002, National Center forChronic Disease Prevention and Health Promotion, Centers for DiseaseControl and Prevention. Cigarette smoking among adults – UnitedStates, 2002. MMWR Morb Mortal Wkly Rep. 2004;53(20):427-431.
American Cancer Society, Surveillance Research
Figure 2B. Current* Cigarette Smoking by Education, Adults 25 and Older, 1974-2002
Perc
ent
American Cancer Society, Surveillance Research
*Adults 25 and older who have ever smoked 100 cigarettes in their lifetime and who are current smokers (regular and irregular).
Source: National Health Interview Survey, 1974-2002, National Center for Health Statistics, Centers for Disease Control and Prevention. Cigarette smoking among adults – United States, 2002. MMWR Morb Mortal Wkly Rep. 2004;53(20):427-431.
No high school degree
College degree
Some college
Year
High school degree
0
5
10
15
20
25
30
35
40
45
50
200220012000199919981997199519941993199219911990198819871985198319791974

Cancer Prevention & Early Detection Facts & Figures 2005 19
Table 2B. Tobacco Use, Adults 18 and Older, 2003, and Comprehensive Tobacco Control Measures, by State,2001, 2004, and 2005
Cigarette Smoking* Fiscal year Fiscal year Difference in per% Men % Women % 2001 per capita 2005 per capita capita tobacco Cigarette
% 18 State 18 and 18 and Low tobacco control tobacco control control funding tax perand older rank† older older education‡ funding ($) funding ($) (2001-2005) pack ($)§
Alabama 25.35 39 28.54 22.45 33.35 1.35 0.08 -1.27 0.425Alaska 26.30 47 30.32 21.93 46.34 2.23 6.70 4.47 1.60||
Arizona 20.95 15 23.78 18.17 21.73 6.72 4.50 -2.22 1.18¶
Arkansas 24.84 36 27.59 22.31 36.65 6.02 6.58 0.56 0.59#
California 16.80 2 20.48 13.20 17.15 3.38 2.18 -1.20 0.87
Colorado 18.55 4 19.61 17.48 33.00 2.95 1.00 -1.95 0.20Connecticut 18.75 5 19.67 17.90 25.99 0.29 0.02 -0.27 1.51#
Delaware 21.94 22 25.99 18.23 31.92 3.57 11.87 8.30 0.55#
Dist. of Columbia 22.33 27 26.15 19.00 27.84 0.00 0.00 0.00 1.00Florida 23.95 33 25.98 22.06 29.95 2.75 0.06 -2.69 0.339
Georgia 22.82 30 25.84 19.97 36.02 1.93 1.40 -0.53 0.37#
Hawaii 17.26 3 20.08 14.45 22.24 7.68 7.35 -0.33 1.40||
Idaho 18.98 6 19.52 18.46 33.71 0.93 1.47 0.54 0.57#
Illinois 23.41 31 27.18 19.90 27.22 2.30 0.89 -1.41 0.98¶
Indiana 26.14 45 28.57 23.84 38.42 5.76 1.78 -3.98 0.555¶
Iowa 21.74 21 22.83 20.71 31.62 3.21 1.74 -1.47 0.36Kansas 20.36 13 21.04 19.72 32.61 0.19 0.28 0.09 0.79¶
Kentucky 30.85 51 33.77 28.13 38.61 1.44 0.67 -0.77 0.03Louisiana 26.58 48 30.28 23.22 33.29 0.92 2.53 1.61 0.36¶
Maine 23.60 32 23.12 24.05 39.54 14.75 11.14 -3.61 1.00
Maryland 20.21 12 22.98 17.69 35.32 5.66 1.79 -3.87 1.00¶
Massachusetts 19.16 7 20.02 18.38 26.04 6.79 0.60 -6.19 1.51¶
Michigan 26.16 46 30.24 22.35 37.76 0.00 0.00 0.00 2.00||
Minnesota 21.11 17 22.35 19.92 31.69 7.11 3.80 -3.31 0.48Mississippi 25.63 43 31.10 20.67 30.37 10.90 7.03 -3.87 0.18
Missouri 27.32 49 31.15 23.82 35.30 0.00 0.00 0.00 0.17Montana 19.92 11 19.50 20.33 32.44 3.88 2.77 -1.11 0.70#
Nebraska 21.27 19 23.60 19.05 26.16 4.09 1.69 -2.40 0.64¶
Nevada 25.19 38 28.97 21.31 30.84 1.50 2.20 0.70 0.80#
New Hampshire 21.24 18 22.37 20.16 33.71 2.43 0.00 -2.43 0.52
New Jersey 19.48 8 21.17 17.91 23.99 3.57 1.31 -2.26 2.40||
New Mexico 21.96 23 23.56 20.46 33.18 1.26 2.75 1.49 0.91#
New York 21.63 20 24.78 18.79 24.12 1.58 2.08 0.50 1.50¶
North Carolina 24.83 35 27.96 21.87 32.38 0.00 1.86 1.86 0.05North Dakota 20.47 14 21.98 19.00 23.22 0.00 4.83 4.83 0.44
Ohio 25.39 40 26.93 23.98 35.91 5.28 4.69 -0.59 0.55¶
Oklahoma 25.17 37 27.79 22.72 35.16 1.83 1.39 -0.44 0.23Oregon 20.96 16 23.10 18.90 27.61 2.48 1.02 -1.46 1.18Pennsylvania 25.52 41 27.06 24.13 33.66 0.00 3.75 3.75 1.35||
Rhode Island 22.40 28 23.83 21.12 25.45 2.19 2.38 0.19 2.46||
South Carolina 25.53 42 28.49 22.81 34.87 0.45 0.00 -0.45 0.07South Dakota 22.67 29 24.70 20.72 22.73 2.25 1.99 -0.26 0.53#
Tennessee 25.70 44 27.30 24.23 39.10 0.00 0.00 0.00 0.20¶
Texas 22.10 26 26.73 17.62 24.97 0.45 0.35 -0.10 0.41Utah 11.95 1 13.99 9.93 32.87 2.69 3.13 0.44 0.695¶
Vermont 19.58 10 19.82 19.36 31.11 10.68 7.72 -2.96 1.19¶
Virginia 22.06 24 26.41 17.98 38.34 1.78 1.84 0.06 0.20||
Washington 19.54 9 20.93 18.19 29.03 2.54 4.61 2.07 1.425¶
West Virginia 27.39 50 27.60 27.19 28.72 3.26 3.26 0.00 0.55#
Wisconsin 22.07 25 23.97 20.25 30.98 3.95 1.86 -2.09 0.77Wyoming 24.63 34 25.17 24.09 40.64 1.82 7.70 5.88 0.60#
United States** 22.32 25.06 19.74 28.73 3.11 2.76 -0.36 0.46Range 11.95-30.85 13.99-33.77 9.93-28.13 17.15-46.34 0.0-14.75 0.0-11.87 -6.19-8.30 0.03-2.46
*Adults 18 and older who have smoked 100 cigarettes and are current smokers (regular and irregular). †Rank is based on % 18 and older. ‡Adults 25 and older with lessthan a high school education. §Taxes reported as of September 2004. ||Passed tax increase legislation in 2004. ¶Passed tax increase legislation in 2002. #Passed tax increaselegislation in 2003. **See Statistical Notes on page 47 for definition of prevalence measures; average value (including District of Columbia) for taxes and per capita funding.
Source: Cigarette smoking percentages: Behavioral Risk Factor Surveillance System Public Use Data Tape 2003, National Center for Chronic Disease Prevention and HealthPromotion, Centers for Disease Control and Prevention, 2004. Per Capita Funding: calculated by dividing state prevention funding (Campaign for Tobacco-Free Kids, et al. A Broken Promise to Our Children. The 1998 Master Settlement Agreement Five Years Later, National Center for Tobacco-Free Kids, 2004) by US Census state populationcounts (http://www.census.gov). Cigarette Taxes: American Cancer Society. Unpublished information as of October 2004. Washington (DC): American Cancer Society,National Government Relations Department, 2004.
American Cancer Society, Surveillance Research

smoke-free policies, counter-marketing campaigns(such as antismoking tobacco ads), and cessation pro-grams and policies (smoking cessation quitlines, bene-fits coverage for tobacco cessation therapies).117
Evidence that supports these recommendations stemsin part from efficacy studies in states that have imple-mented such programs (including California,Massachusetts, Oregon, Maine, Florida, Minnesota, andMississippi).5 These studies document the beneficialimpact of comprehensive tobacco control programs inreducing tobacco use and consumption.118-127 In a studyof the California Tobacco Control Program (CTCP),begun in 1990, analyses of lung cancer incidence inCalifornia between 1975 and 1999 found that there was asignificantly greater rate of decline in lung cancer casesduring the period of 1988 to 1999 than would have beenpredicted from prior lung cancer trends in the state. Thisdecline was also much greater than declines in lungcancer incidence trends (if any) in other areas, measuredby SEER.127 The CTCP has estimated that for every dollarspent on tobacco control between 1990 and 1998, morethan $3.00 was saved in direct medical costs.128
Smoke-free initiatives. Smoke-free initiatives (alsoreferred to as clean air laws or ordinances) are anotherimportant component of comprehensive tobacco con-trol. Clean air laws reduce the exposure of nonsmokersto ETS, change social norms about smoking, and maymotivate addicted smokers to quit or reduce consump-tion by banning smoking in workplaces, bars, and/orrestaurants. Smoke-free initiatives exist at the federal,state, and local levels.5
• Presently in the US, 1,903 cities and municipalitieshave passed smoke-free legislation. Ten states(Delaware, Massachusetts, New York, California,Connecticut, Florida, Idaho, Maine, South Dakota, andUtah) have implemented statewide smoking bans thatprohibit smoking in workplaces and/or restaurantsand/or bars.129 Delaware, New York, and Massachusettsare the only states that provide comprehensivesmoke-free protection – meaning that all workplaces,restaurants, and bars are 100% smoke-free – whileCalifornia, Connecticut, Florida, Idaho, Maine, SouthDakota, and Utah provide some degree of protectionin at least one of these venues (Figure 2C).130
Economic impact of smoke-free laws. There havebeen numerous studies of the economic impact ofsmoke-free legislation on restaurants, bars, and othercomponents of the hospitality industry.131 (For addi-tional information, visit www.no-smoke.org/economic_
20 Cancer Prevention & Early Detection Facts & Figures 2005
impact.html.) Most of these show no adverse effects onthe hospitality industry, despite the claims of thetobacco industry. Even in the tobacco-growing state ofNorth Carolina, where adult smoking rates are higherthan the national average, researchers found thatsmoke-free restaurant ordinances did not adverselyaffect restaurant revenues.132
In 1995, New York City became the largest city in the USto pass a smoke-free restaurant law; studies evaluatingthe effect of this law found that employment levelsamong workers in the hospitality industry increasedafter a smoke-free ordinance was implemented.133,134
Further analysis revealed that the city’s smoke-free lawdid not change sales revenues at New York restaurantsand hotels.135
Similarly, studies assessing the economic impact ofsmoke-free policies in cities and states throughout theUS during different economic cycles have shown thatthese ordinances do not affect tourism or hotel/motelrevenues.135,139,140 The evidence is clear: smoke-free lawsprotect the health of employees and consumers and arenot harmful to business.
Success StoryIn 2003, New York City implemented legislation makingall workplaces, including restaurants and bars, smoke-free. Fueled in part by the tobacco industry’s influence,many restaurant owners believed their businesses wouldfail under the stronger ordinance. One year after the lawwent into effect, New York City bars and restaurants werebooming. Data from the New York City Department ofFinance show that tax receipts increased by 8.7%, orapproximately $1.4 million. Moreover, the New York StateDepartment of Labor found no evidence that restaurantswere closing as a result of the smoke-free law, and therate of restaurant openings remained unchanged sincethe law went into effect.136
The lessons learned from New York, while they are themost recent, are not unusual. Delaware, the first state togo 100% smoke-free on November 27, 2002, had similarsuccess with its smoking ban. According to the DelawareBehavioral Risk Factor Survey (BRFS), Delaware’s adult andyouth smoking prevalence decreased by 11% and 25%,respectively, one year after the law went into effect.137 Alocal study assessing the air quality of eight hospitalityindustry venues (a casino, six bars, and a pool hall) in theWilmington/Delaware metropolitan area showedimprovements in air quality. The level of cancer-causingpollutants in the air dropped by 95% in these venues twomonths into the smoking ban.138

Cancer Prevention & Early Detection Facts & Figures 2005 21
Counter-advertising. Comprehensive tobacco controlprograms use various strategies to counteract the $12.47billion dollars spent by tobacco companies on advertis-ing and promotion in 2002.5,17 Counter-advertising usesmedia advocacy and paid advertisements to discouragetobacco use and expose the industry’s marketing andpromotional tactics. Considerable research has beendone on how to design effective counter-advertising andhealth education campaigns on tobacco.5 Mass mediacampaigns are the most visible component of tobaccocontrol programs in California, Massachusetts, Arizona,Florida, and Minnesota. In California, the statewidemedia campaign promotes core messages (e.g., ‘thetobacco industry lies,’ ‘secondhand smoke kills,’ and‘nicotine is additive’) to restore a social and legal climatein which tobacco use is recognized as undesirable.128
Tobacco cessation. Much of the risk of prematuredeath from smoking could be prevented by smokingcessation. Smokers who quit can expect to live approxi-mately 10 years longer than those who continue tosmoke.112,141 One study showed that quitting smoking atage 60, 50, 40, or 30 years gained, respectively, about 3, 6,
9, or 10 years of life expectancy.141 Nearly 46 millionAmericans (45.8 million) currently smoke; more than40% of these report attempting to quit for at least oneday in the past year.115 Smokers who wish to quit canbenefit from a variety of effective treatments for tobaccodependence (e.g., nicotine replacement products aloneor in combination with antidepressants, counseling, orbehavioral therapies).142 Quitting is more difficult forsome smokers than others, but the chances of successare approximately doubled by use of such treatments.
Health care providers can be especially influential incounseling and offering assistance to their patients whosmoke. Health care insurance benefits for cessationtreatment are important to allow access to the full rangeof treatments for smokers who want to quit.7,143 Publichealth experts recommend that health insuranceinclude coverage for smoking cessation treatment.143
While the most effective tobacco cessation treatmentscombine both counseling and drug therapy,142 a recentnational study showed that only 22% of smokers tryingto quit used any pharmaco- or behavioral therapies fortreating tobacco dependence.144 Under-utilization of
Figure 2C. Smokefree Legislation at the State, County, and City Level
Source: American Nonsmokers' Rights Foundation Local Tobacco Control Ordinance Database: USA©, 1/4/05.
Locality types City
• County
State law type100% smoke-free in all workplaces, restaurants, and bars
100% smoke-free in one or two of the above
No 100% smoke-free state law
AK

tobacco-dependence treatment results from barriersthat affect individual smokers,145 health care pro-viders,146 and health care systems and insurers.7 Healthcare providers are not consistently reimbursed by healthinsurance plans under Medicaid, private insurers, andmanaged care organizations, and are not reimbursed atall by Medicare for cessation therapy.7
Even with insurance, smokers bear a significant portionof the cost of pharmacotherapy because of deductiblesand co-payments. States can encourage use of tobaccocessation therapies by including coverage for smokingcessation treatments in health insurance benefits forstate employees and Medicaid recipients. In 2003, 17states (out of 45 states surveyed) had legislative require-ments in place to ensure health insurance coverage forpharmacotherapy and counseling for state employees.147
In 2002, Medicaid programs covered one or more treat-ments for tobacco dependence in 39 states and theDistrict of Columbia; in 12 states, Medicaid covered notreatments at all (Figure 2D).148
Another strategy to facilitate cessation is the implemen-tation of statewide quitlines that provide telephonecounseling. These toll-free services can deliver effectivebehavioral counseling to large numbers of tobacco users,including low-income, rural, elderly, uninsured, andracial/ethnic subpopulations of smokers.143 Some smok-ers prefer the convenience of using telephone cessationservices rather than face-to-face counseling.149
22 Cancer Prevention & Early Detection Facts & Figures 2005
Currently, statewide quitline services are operated in 37states.150 On November 10, 2004, US Health and HumanServices (HHS) Secretary Tommy G. Thompsonannounced the opening of a national quitline number (1-800-QUITNOW) that puts users in touch with pro-grams that can help them give up tobacco. In addition, anew HHS Web site (www.smokefree.gov) offers onlineadvice and downloadable information to make cessationeasier. Each year, the American Cancer Society’s GreatAmerican Smokeout® urges smokers to give up theircigarettes for at least a day in the hope that they mightstop smoking. (For more information, refer towww.cancer.org or call 1-800-ACS-2345.)
Funding for tobacco control. The CDC has recom-mended base and per-capita levels of funding for statesto address all components of comprehensive tobaccocontrol.117 These range from $7 to $20 per capita insmaller states (population less than 3 million), $6 to $17per capita in medium-sized states (populations from 3to 7 million), and $5 to $16 per capita in larger states(with populations more than 7 million).117 According toCDC estimates for minimal levels of tobacco controlfunding, about $1.6 billion should be spent, but only $538million has been set aside for fiscal year 2005.151 Only 3states met or exceeded the CDC’s Best Practices mini-mum level for funding: Delaware, Maine, andMississippi.151 Ten other states fund tobacco preventionprograms at at least half the minimum levels recom-mended by the CDC. The remaining states fund at lessthan half the recommended amount (Figure 2E).151
Recent budget deficits and other political pressurescaused many states to make cuts in their funding fortobacco control. Over the past 3 years, 29 states havereduced their spending levels for tobacco control, whileonly 8 states have substantially increased their funding(Table 2B). Advocacy efforts are essential to sustain andincrease funding for comprehensive tobacco control.
Tobacco excise taxes. Excise taxes on tobacco serve thedual purpose of raising revenues for tobacco control andof reducing tobacco consumption, especially amongchildren.5 The effect of price on cigarette consumptionhas been demonstrated in numerous studies using awide variety of data and methods. These studies predictthat a 10% increase in price will reduce overall cigaretteconsumption by 3%-5%.5 To generate funds for tobaccocontrol and reduce smoking initiation among adoles-cents, the American Cancer Society has joined withother leading health organizations to issue the TobaccoTax Challenge encouraging governors to enact an above-
WhenSmokersQuit
When smokers quit, their bodies show immediate and long-lasting improvements, including lower blood pressure andreduced risk of lung cancer. The American Cancer Societyprovides valuable resources that can help smokers quit.

Cancer Prevention & Early Detection Facts & Figures 2005 23
average sales tax on cigarettes.5,152 State cigarette excisetaxes per pack range from 3 cents in Kentucky to $2.46 inRhode Island (Table 2B).153 In the past 3 years, 36 states,including the tobacco-growing state of Virginia and the
District of Columbia, have increased their cigarette taxes(Figure 2F). Only 16 states have laws requiring that aportion of the excise tax be dedicated to tobacco controlor cancer programs.5,154
Source: Burns et al. Insurance coverage of smoking cessation treatment for state health employees. AJPH. 2004;94(8):1338-1340.
Figure 2D. Insurance Coverage of Smoking Cessation Treatments
AL
AZAR
CA CO
CT
DE
FL
GA
ID
IL IN
IA
KS
KY
LA
ME
MD
MA
MI
MN
MS
MO
MT
NENV
NH
NJ
NM
NY
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WIWY
DC
HI
AK
Required coverage of smoking cessation treatments for all or some state employees, including some form of counseling and some type of drug therapy.
Required coverage of smoking cessation treatments for some state employees, including some form of counseling or some type of drug therapy.
Coverage of smoking cessation treatments are not required for any state employee.
State Employees, 2003
Did not participate in the survey.
Source: Centers for Disease Control and Prevention. State Medicaid coverage for tobacco-dependence treatments – United States, 1994-2002. MMWR Morb Mortal Wkly Rep. 2004;53(03):54-57. Post publication update provided by National Government Relations Department, unpublished data.
AL
AZAR
CA CO
CT
DE
FL
GA
ID
IL IN
IA
KS
KY
LA
ME
MD
MA
MI
MN
MS
MO
MT
NENV
NH
NJ
NM
NY
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WIWY
DC
HI
AK
Provides full coverage for smoking cessation to all Medicaid beneficiaries, including some form of counseling and some type of drug therapy.
Provides partial coverage for smoking cessation to all Medicaid beneficiaries, including some form of counseling and some type of drug therapy.
There are no state requirements to cover Medicaid beneficiaries for smoking cessation treatments.
Medicaid Recipients, 2004

24 Cancer Prevention & Early Detection Facts & Figures 2005
Source: Campaign for Tobacco-Free Kids, et al. A broken promise to our children: the 1998 state tobacco settlement six years later. 2004.
Figure 2E. Funding for Tobacco Prevention, by State, 2005
AL
AZAR
CA CO
CT
DE
FL
GA
ID
IL IN
IA
KS
KY
LA
ME
MD
MA
MI
MN
MS
MO
MT
NENV
NH
NJ
NM
NY
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WIWY
DC
HI
AK
100% or more
50% to 99%
25% to 49%
Less than 25%
Percent (%) of Centers for Disease Control and Prevention minimum recommended fundinglevel committed by state for tobacco control
Figure 2F. Tobacco Excise Tax, by State, 2004*
AL
AZAR
CA CO
CT
DE
FL
GA
ID
IL IN
IA
KS
KY
LA
ME
MD
MA
MI
MN
MS
MO
MT
NENV
NH
NJ
NM
NY
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WIWY
DC
HI
AK
Equal to or above the national average of 79 cents per pack
Below the national average in the range of 35 to 78 centsper pack
Far below the national average up to 34 cents per pack
*Data current as of October 2004.
Source: National Government Relations Department, American Cancer Society, 2004

Cancer Prevention & Early Detection Facts & Figures 2005 25
Overweight and Obesity, PhysicalInactivity, and Nutrition Among AdultsFor the majority of Americans who do not use tobacco,improving diet, increasing physical activity, and main-taining a healthy weight are the most importantapproaches to reducing the risk of developing cancer.While individual choices are important factors thatinfluence dietary and physical activity habits, thesechoices are themselves influenced by the social context.America produces twice as many calories each year asare needed to maintain the health of the population.Large portion sizes and calorie-dense foods are usedextensively to market foods in restaurants and super-markets. (Calorie-dense foods are those in which fatsand sugars make up much of their caloric content perunit serving.) Changes in urban design and land use havereduced opportunities for physical activity. Scientificevidence suggests that about one-third of the cancerdeaths that occur in the US each year are due to nutri-tion and physical activity factors, including obesity.2,98
Because of the linkage between nutrition, physical activ-ity, and cancer, the American Cancer Society in 2002published updated guidelines for nutrition and physicalactivity.156 These guidelines also include explicit recom-mendations on how communities can play an essentialrole in facilitating healthy dietary choices, and howschools, worksites, and neighborhoods can increaseopportunities for physical activity (see sidebar on page26). As a first step in demonstrating the Society’s com-mitment to these guidelines, it has implemented anActive for LifeSM worksite wellness program that encour-ages Society employees to adopt healthy nutrition andphysically active lifestyle behaviors aimed at reducingtheir cancer risk.
In addition to their effects on overweight and obesity,nutrition and physical activity directly affect the risk ofdeveloping or dying from certain cancers. Physical activ-ity decreases the risk of breast, colon, and, possibly,endometrial and prostate cancers.157 Eating a diet highin vegetables and fruits is associated with lower risk of
Success StoriesThe state of Virginia, home of the world’s largest cigarette factory and the national headquartersfor Phillip Morris, passed tobacco legislation that increased the state excise tax on cigarettes by 20cents in 2004 and an additional 10 cents in 2005. Revenue generated from excise taxes on cigaretteswill be directed to the newly established Virginia Health Care Fund. In addition, the tax plan imposesa new 10% tax at the wholesale level on other tobacco products, including cigars and smokelesstobacco, beginning in 2005.8
The Washington State Tobacco Control Program delivers comprehensive tobacco controlthroughout Washington. By working through local health agencies, American Indian tribes, schools,and community-based organizations, the program delivers integrated antitobacco activities to allWashington residents.120 The program is funded from a variety of sources; its budget in 2004 was at78.6% of the CDC’s minimum recommendation, ranking Washington as eighth among the stateswith the most funding for tobacco prevention programs. In less than 3 years, the Washington StateDepartment of Health and its partners have achieved several milestones in reducing tobacco use:120
• Reduced adult smoking prevalence among adults: from 22.4% in 1999 to 19.5% in 2003.
• Protected the health of nonsmokers through smoke-free policies: 74% of Washington residentswork in smoke-free workplaces (compared to 69% nationally).
• Changed the social acceptance and norms toward smoking: 69% of adults report having smoke-free policies in their homes vs. 61% nationally.155
Further information about the Washington State Tobacco Control Program can be found athttp://www.doh.wa.gov/Tobacco/default.htm

26 Cancer Prevention & Early Detection Facts & Figures 2005
cancers of the mouth and pharynx, esophagus, lung,stomach, colon, and rectum.158
ObesityObesity is the nation’s fastest growng health problem.Overall, nearly two-thirds (65%) of Americans are over-weight or obese. Of these, about 44.3 million adults(30%) are obese.160,161 Obesity increases the risk of devel-oping or dying from multiple diseases, including heartdisease, diabetes, and many types of cancer.4
US medical expenditures associated with the treatmentof overweight and obesity totaled $92.6 billion in 2002;Medicaid and Medicare programs together paid approx-imately half of these medical costs.159
Obesity and CancerThe American Cancer Society was one of the firstnational organizations to call attention to the relation-ship between obesity and cancer in a special section ofCancer Facts & Figures 2000.162 In 2003, the AmericanCancer Society released the most comprehensive studyto date on the relationship between excess body weightand cancer mortality, using data from the CancerPrevention Study II.163 Body mass index was significantlyassociated with higher death rates from 11 types ofcancer in men and 12 types of cancer in women (Figure2G).163 Based on the observed associations, theAmerican Cancer Society study estimated that currentpatterns of overweight and obesity in the US couldaccount for 1 in 7 cancer deaths in men and 1 in 5 inwomen.163
Prevalence of Overweight and ObesityObesity has reached epidemic proportions in the US.The percentage of adults aged 20-74 who are obese (bodymass index (BMI) greater or equal to 30 kg/m2) rosefrom 14.5% in 1974 to 30.4% in 2002, with the largestincreases occurring during the 1990s.160,164 Similartrends were observed among men and women (Figure2H). Overall, 65.1% of US adults aged 20 and older wereoverweight or obese.160
In 2003, Mississippi, Alabama, Kentucky, North Dakota,Arkansas, Michigan, West Virginia, Indiana, Texas, Iowa,Louisiana, and North Carolina were the 12 states inwhich more than two-thirds of adults were overweight or
American Cancer Society Guidelines onNutrition and Physical Activity for CancerPreventionRecommendations for Individuals1 Eat a variety of healthful foods, with an emphasis on
plant sources.
• Eat 5 or more servings of a variety of vegetables and fruitseach day.
• Choose whole grains in preference to processed (refined)grains and sugars.
• Limit your consumption of red meats, especially high-fatand processed meats.
• Choose foods that maintain a healthful weight.
2. Adopt a physically active lifestyle.
• Adults: Engage in at least moderate activity for 30 minutesor more on 5 or more days of the week; 45 minutes ormore of moderate to vigorous activity on 5 or more daysper week may further enhance reductions in the risk ofbreast and colon cancer.
• Children and adolescents: Engage in at least 60 minutesper day of moderate to vigorous physical activity at least 5days per week.
3. Maintain a healthful weight throughout life.
• Balance caloric intake with physical activity.
• Lose weight if currently overweight or obese.
4. If you drink alcoholic beverages, limit consumption.
Recommendation for Community ActionPublic, private, and community organizations should workto create social and physical environments that support theadoption and maintenance of healthful nutrition andphysical activity behaviors.
• Increase access to healthful foods in schools, worksites,and communities.
• Provide safe, enjoyable, and accessible environments forphysical activity in schools and for transportation andrecreation in communities.

Cancer Prevention & Early Detection Facts & Figures 2005 27
obese (Table 2C). Figure 2I illus-trates that the prevalence ofoverweight and obesity variesby region, with the lowest ratesseen in some Western statesand the highest rates in theSoutheast. Some states showlittle variation in overweight-obesity prevalence by county,while for others the variation is considerable. In Maine, for example, counties with the highest prevalence ofoverweight-obesity are locatedin the northern and southernregions of the state.
Why Is ObesityIncreasing?The sudden increase in obesityhas occurred because of socialchanges that have increasedcaloric consumption anddecreased energy expenditurein the population.166 For mostAmericans, both excessivecaloric intake and inadequatephysical activity are importantfactors. Food is inexpensive andreadily available; calorie-densefoods are cheaper, more widelyavailable, and more aggressivelymarketed than healthy foods(such as vegetables and fruits).Large portion sizes are used toattract customers in restau-rants and fast-food establish-ments, and vending machinesthat dispense calorie-dense
Figure 2G. Cancer Mortality by Body Mass Index for US Men and Women in the Cancer Prevention Study II, 1982-1998
Typ
e o
f ca
nce
r (h
igh
est
BM
I cat
ego
ry)
For each relative risk, the comparison was between men and women in the highest body mass index (BMI) category (indicated in parentheses) and men and women in the reference category (body mass index, 18.5 to 24.9). Asterisks indicate relative risks for men and women who never smoked. Results of the linear test for trend were significant (P0.05) for all cancer sites.
Source: Calle EE et al. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of US adults. N Engl J Med. 2003;348:1625-1638 ©2003 Massachusetts Medical Society. All rights reserved.
Relative risk of death (95% confidence interval)
Men
Typ
e o
f ca
nce
r (h
igh
est
BM
I cat
ego
ry)
Relative risk of death (95% confidence interval)
Women
Multiple myeloma (35)
Colon and rectum (40)
Ovary (35)
Liver (35)
All cancers (40)
Non-Hodgkin lymphoma (35)
Breast (40)
Gallbladder (30)
All other cancers (40)
Esophagus (30)
Pancreas (40)
Cervix (35)
Kidney (40)
Uterus (40)
Prostate (35)
Non-Hodgkin lymphoma (35)
All cancers (40)
All other cancers (30)
Kidney (35)
Multiple myeloma (35)
Gallbladder (30)
Colon and rectum (35)
Esophagus (30)
Stomach (35)
Pancreas (35)
Liver (35)
1.34•1.49•
1.52•1.68*
•1.70•
1.71•1.76•1.84•
1.91*•
1.94•
2.61*•
4.52•
0 1 2 3 4 5 6 7
0 1 2 3 4 5 6 7 8 9 10 11
1.44•
1.46•
1.51•1.68•1.88*
•1.95•2.12•
2.13•2.51*
•2.64*
•2.76•
3.20•
4.75•
6.25•
What is relative risk? What is the confidence interval?A relative risk compares the risk of disease among people with a particular exposure to the risk amongpeople without that exposure. If the relative risk is above 1.0, then risk is higher among exposed than unex-posed persons. If the relative risk is below 1.0, then risk is lower among exposed than unexposed persons.However, while relative risks are useful for comparisons, they do not provide information about the absoluteamount of additional risk experienced by the exposed group.
A confidence interval is a statistical estimate of the range in which the true value is likely to fall. A 90%confidence interval is one that will contain the true value in 90 out of 100 samples surveyed. Similarly, a95% confidence interval will contain the true value in 95 out of 100 samples.

foods are ubiquitous at worksites, schools, and hotels.Urban development patterns increase reliance on carsand discourage walking. Opportunities for physicalactivity as part of daily life have been reduced or elimi-nated in most schools, workplaces, and communities.167
Prevalence and Trends in Physical ActivityThe measure of physical activity that has been routinelytracked in population surveillance in the US is leisure-time physical activity. Over the past decade, leisure-timephysical activity has changed little among adults.58,168
Table 2C shows that nationally, 24.3% of US adults reportno leisure-time physical activity, 46.1% report engagingin moderate levels of activity, and 25.8% report vigorouslevels of physical activity. Across the 50 states and DC,the proportion of adults engaging in physical activityvaries greatly. Generally, states with a high percentage ofpeople reporting no leisure-time physical activity have ahigher prevalence of overweight and obesity.
Leisure-time physical activity does not reflect physicalactivity at work. Studies show that individuals who arevery active at work are less likely to be overweight andmay be less likely to participate in leisure-time physicalactivity.169 Surveys that ignore occupational activity mayunderestimate activity for some population groups thatreport little or no leisure-time activity. For example,based on analysis of the 2003 Behavioral Risk FactorSurveillance System, 35% of adults reported being phys-
28 Cancer Prevention & Early Detection Facts & Figures 2005
ically active in their job (i.e., by doing either hard labor orwalking activities) while also being active during theirleisure time. In contrast, 41% of adults reported beingphysically active in their job but report being sedentaryduring their leisure time (unpublished data, SurveillanceResearch, American Cancer Society).
Figure 2H. Adult Obesity*, by Gender, Ages 20-74, 1960-2002
Perc
ent
American Cancer Society, Surveillance Research
*Body mass index of 30 kg/m2 or greater. †Obesity estimates for adults 20 years and older.
Source: National Health Examination Survey, 1960-1962, National Health and Nutrition Examination Survey, 1971-1974, 1976-1980, 1988-1994, 1999-2002, National Center for Health Statistics, Centers for Disease Control and Prevention. Hedley, et al. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. JAMA. 2004;291(23):2847-2850.
1960-1962
0
5
10
15
20
25
30
35
40
WomenMenAll adults
1971-19741976-19801988-1994
1999-2002†
30.4
23.3
10.712.1
12.7
20.6
27.6
13.414.5
15.015.8
16.617.0
33.2
25.9
Defining Body Mass Index (BMI)Different measures are used to determine whether a personis considered normal weight, overweight, or obese, takingheight into account. A common scale is the body mass index(BMI), or ratio of weight (in kilograms) to height (in meters,squared). For adults aged 20 years and older, overweight isdefined as a BMI of 25.0-29.9 kg/m2, and obesity is definedas a BMI of 30.0 kg/m2 or greater. Although BMI may over-estimate body fat in athletes and others who have a muscu-lar build, or underestimate body fat in older persons whohave lost muscle mass,165 it is a generally reliable indicator oftotal body fat.
The table below relates BMI to pounds and inches ratherthan kilograms and meters. BMI corresponds to an individ-ual’s height (in the left column) and weight category (inpounds). An adult aged 20 or older is considered overweightor obese if his or her weight falls within the correspondingarea of the table. For example, a 5'4" woman is consideredoverweight if she weighs between 145 and 173 pounds. Sheis considered obese if she weighs 174 pounds or more. A5'10" man is considered overweight if he weighs between174 and 206 pounds and obese if he weighs 207 pounds ormore.
Height Body weight (pounds)(feet, inches) Overweight* Obese†
6’4” 205 246
6’3” 200 240
6’2” 194 233
6’1” 189 227
6’0” 184 221
5’11” 179 215
5’10” 174 207
5’9” 169 203
5’8” 164 197
5’7” 159 191
5’6” 155 186
5’5” 150 180
5’4” 145 174
5’3” 141 169
5’2” 136 164
5’1” 132 158
5’0” 128 153
4’11” 124 148
4’10” 119 143
*Overweight defined as BMI of 25 to 29.9 kg/m2.†Obesity defined as BMI of 30 kg/m2 or greater.

Cancer Prevention & Early Detection Facts & Figures 2005 29
Table 2C. Overweight, Obesity, and Related Factors, Adults 18 and Older, by State, 2003% % % % % %
Clinically Clinically % No leisure- % % Eating five Eating three Eating two overweight obese Overweight time Vigorous Moderate fruits and or more or more
(25-29.9 (30 kg/m2 (25 kg/m2 State physical physical physical vegetables vegetables fruits kg/m2) or greater) or greater) rank* activity activity† activity‡ a day a day a day
Alabama 34.86 28.45 63.31 50 29.95 21.29 40.31 22.36 12.16 10.86Alaska 37.08 23.61 60.69 35 19.10 34.62 58.11 22.59 6.44 15.70Arizona 36.97 20.22 57.19 13 21.06 28.87 49.64 22.85 8.27 13.56Arkansas 36.88 25.16 62.04 47 29.21 23.37 45.40 20.78 13.57 11.58California 36.20 23.20 59.39 25 22.34 28.64 46.68 26.89 8.40 24.21
Colorado 35.38 16.03 51.40 2 16.87 32.99 55.01 24.16 9.25 19.40Connecticut 35.71 19.14 54.85 6 20.98 30.61 51.64 29.81 8.57 20.74Delaware 36.27 24.00 60.26 29 26.55 23.30 43.68 22.01 10.14 10.53Dist. of Columbia 31.86 20.56 52.42 3 22.78 32.72 52.08 29.46 10.34 19.37Florida 38.77 19.97 58.74 21 27.88 21.46 41.21 23.35 9.47 14.25
Georgia 35.31 25.22 60.53 33 24.56 24.98 42.40 22.84 13.10 11.07Hawaii 33.58 16.46 50.04 1 18.31 26.35 49.86 27.60 10.26 7.47Idaho 37.17 21.84 59.01 22 18.68 31.85 55.86 20.35 6.52 15.78Illinois 37.41 23.69 61.10 40 25.69 23.48 43.73 23.04 7.68 16.07Indiana 35.73 25.98 61.71 44 26.20 25.31 46.83 22.03 8.41 14.48
Iowa 37.63 23.97 61.60 42 22.70 20.96 43.59 17.06 6.29 11.34Kansas 37.81 22.70 60.52 32 25.95 22.82 43.85 18.80 6.00 8.40Kentucky 37.45 25.64 63.09 49 30.55 16.40 33.84 18.21 14.03 3.44Louisiana 36.38 24.82 61.20 41 30.59 21.45 40.22 16.36 11.72 5.37Maine 38.26 19.86 58.12 17 20.65 29.11 52.98 26.87 10.33 17.57
Maryland 37.11 22.02 59.13 23 21.29 28.98 49.33 28.84 12.15 19.67Massachusetts 36.22 16.87 53.09 4 21.75 31.06 52.69 28.99 8.69 19.57Michigan 36.61 25.17 61.78 46 21.77 26.60 47.44 20.04 5.25 16.35Minnesota 37.98 22.96 60.93 38 15.04 26.37 49.03 24.25 5.94 18.44Mississippi 36.77 28.18 64.95 51 30.36 20.27 40.34 17.81 11.21 8.31
Missouri 35.66 23.65 59.31 24 24.12 22.61 45.21 20.06 8.54 11.58Montana 38.22 18.83 57.04 11 20.19 33.30 58.61 22.03 6.04 15.88Nebraska 37.01 23.89 60.90 37 20.69 21.67 44.58 17.75 5.48 9.74Nevada 37.31 21.19 58.51 19 24.74 30.34 50.82 20.35 4.74 16.64New Hampshire 36.68 20.28 56.97 10 19.99 31.02 54.71 28.44 10.13 18.96
New Jersey 37.18 20.11 57.29 15 26.93 25.39 44.78 26.58 7.70 16.99New Mexico 36.38 20.27 56.65 9 22.92 28.60 51.35 22.36 8.01 14.89New York 35.38 20.99 56.37 8 27.05 24.56 44.54 25.73 7.03 19.47North Carolina 37.00 24.08 61.08 39 25.04 19.33 37.74 23.17 14.99 7.35North Dakota 39.15 23.85 63.00 48 23.78 26.84 49.39 21.40 5.98 17.13
Ohio 35.95 24.90 60.85 36 26.50 26.04 46.94 22.59 7.10 15.47Oklahoma 36.16 24.43 60.58 34 30.43 19.59 39.98 15.42 8.52 3.93Oregon 36.80 21.51 58.31 18 18.88 30.54 53.92 24.05 8.88 18.60Pennsylvania 36.43 23.74 60.16 27 22.58 26.31 49.25 24.68 6.89 18.80Rhode Island 38.63 18.47 57.09 12 23.34 29.56 50.30 27.00 8.29 17.56
South Carolina 35.75 24.53 60.28 30 23.27 25.87 46.22 22.19 12.51 14.09South Dakota 37.31 22.86 60.17 28 21.66 22.04 46.61 19.03 3.95 12.62Tennessee 35.43 25.06 60.50 31 29.76 20.03 37.64 22.21 15.58 5.77Texas 37.03 24.59 61.62 43 27.58 26.09 44.69 22.51 11.10 15.55Utah 33.81 20.87 54.68 5 17.34 35.55 57.07 19.40 7.19 16.49
Vermont 35.96 19.60 55.56 7 18.71 32.31 55.87 32.49 10.69 21.93Virginia 35.96 21.74 57.69 16 22.06 28.10 49.43 25.79 11.69 16.68Washington 36.81 21.75 58.56 20 17.73 31.26 54.41 23.26 8.60 17.91West Virginia 34.03 27.69 61.72 45 28.01 19.14 42.73 18.73 11.02 7.06Wisconsin 39.11 20.96 60.08 26 18.81 30.31 54.80 21.49 6.14 18.19Wyoming 37.12 20.12 57.24 14 21.11 32.11 55.41 22.07 7.37 14.78
United States§ 36.57 22.84 59.41 24.34 25.79 46.12 23.55 9.14 15.97Range 31.86-39.15 16.03-28.45 50.04-64.95 15.04-30.59 16.40-35.55 33.84-58.61 15.42-32.49 3.95-15.58 3.44-24.21
*Rank based on % overweight (25kg/m2 or greater). †Any activity that caused large increases in breathing or heart rate at least 20 minutes 3 or more times per week (such asrunning, aerobics, or heavy yardwork). ‡Any activity that meets the criteria for vigorous physical activity (see previous definition) OR activity that caused small increases in breath-ing or heart rate at least 30 minutes 5 or more times a week (such as brisk walking, bicycling, vacuuming, or gardening). §See Statistical Notes on page 47 for definition.
Source: Behavioral Risk Factor Surveillance System Public Use Data Tape 2003, National Center for Chronic Disease Prevention and Health Promotion, Centers for DiseaseControl and Prevention, 2004.
American Cancer Society, Surveillance Research

Recent surveys have begun to assess physical activity ina broader context. For example, in 2001, the BehavioralRisk Factor Surveillance System revised its physicalactivity questions to include leisure-time activities,household activities, and transportation-related physi-cal activities; previous questionnaires included leisure-time activities only. As a result, the percentage of thepopulation meeting recommended physical activity lev-els increased from 26.2% in 2000 to 45.4% in 2001.However, the percentage of adults reporting no leisure-time physical activity declined only slightly, from 27.4%in 2000 to 26.0% in 2001.170 The American CancerSociety Guidelines on Diet, Nutrition, and CancerPrevention recommend that individuals engage in atleast 30 minutes or more of moderate physical activityon 5 or more days of the week.156
Benefits of an Active lifestyleRegular physical activity substantially reduces the risk ofdying of coronary heart disease, the nation’s leadingcause of death, and decreases the risk for stroke, colon
30 Cancer Prevention & Early Detection Facts & Figures 2005
cancer, breast cancer, diabetes, and high blood pressure.Physical activity also helps to control weight (therebypotentially decreasing the risk of the many cancersrelated to excess weight); contributes to healthy bones,muscles, and joints; reduces falls among older adults;helps to relieve the pain of arthritis; reduces symptomsof anxiety and depression; and is associated with fewerhospitalizations, physician visits, and medica-tions.4,58,157,171 Moreover, physical activity does not needto be strenuous to be beneficial; people of all ages bene-fit from participating in regular, moderate physical activ-ity, such as 30 minutes of brisk walking 5 or more timesa week. Participating in moderate-intensity physicalactivity is a vital component of a healthy lifestyle forpeople of all ages and abilities. There is no demographicor social group that could not benefit from becomingmore active.58
Although there are no data to directly estimate trends intotal physical activity in US adults in the last severaldecades, a number of social, environmental, and eco-nomic changes are thought to have contributed to
Figure 2I. Prevalence of Overweight Among US Adults by County, 1999-2002
60.50-78.43
58.50-60.49
56.50-58.49
54.50-56.49
43.80-54.49
Percentage
Source: Behavioral Risk Factor Surveillance System Public Use Data Tapes 1999, 2000, 2001, 2002, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 2000, 2001, 2002, 2003.
American Cancer Society, Surveillance Research

reduced levels of physical activity. The number of walk-ing excursions decreased by 42% for the averageAmerican adult between 1975 and 1995.172 More andmore communities are structured for automobile traveland do not provide sidewalks, stores, or schools withinwalking distance of homes.173 Physical activity has beenengineered out of many aspects of daily life. Further-more, workplace activities have shifted from manuallabor to white-collar jobs.172
Strategies to Prevent Obesity and PromoteHealthy LifestylesA 2001 Surgeon General’s Report recognized the obesityepidemic as a serious public health problem and calledfor collaborative efforts among governmental and pri-vate health organizations, the food industry, employers,the media, and communities to address the issue.6 In2003, a number of National Institute of Health (NIH)agencies formed a multi-disciplinary Obesity ResearchTask Force to coordinate research on obesity. The TaskForce recently published a strategic research plan whichfocuses research efforts on defining the causes of theobesity problem more precisely, identifying interven-tions that will help people maintain a healthy bodyweight, and improving the treatment of obesity. Suchresearch could include studies of biological, psychologi-cal, and social factors that promote caloric imbalance,identification of barriers to behavioral change, and thedevelopment of effective and economical interventionsand treatments.174 Other government organizations(such as the CDC and state health departments) and
Cancer Prevention & Early Detection Facts & Figures 2005 31
nonprofit organizations have formed coalitions todevelop and implement public health strategies toaddress the epidemic of overweight and obesity.6 Thesidebar on page 32 describes some approaches that havebeen proposed.
Moderate Physical Activity Examples*
Washing and waxing a car Less Vigorous,for 45-60 minutes More Time
Washing windows or floors for 45-60 minutes
Playing volleyball for 45 minutes
Playing touch football for 30-45 minutes
Gardening for 30-45 minutes
Wheeling self in wheelchair for 30-40 minutes
Walking 13/4 miles in 35 minutes (20 minutes per mile)
Basketball (shooting baskets) for 30 minutes
Bicycling 5 miles in 30 minutes
Dancing fast (social) for 30 minutes
Pushing a stroller 11/2 miles in 30 minutes
Raking leaves for 30 minutes
Walking 2 miles in 30 minutes (15 minutes per mile)
Water aerobics for 30 minutes
Swimming laps for 20 minutes
Wheelchair basketball for 20 minutes
Basketball (playing a game) for 15-20 minutes
Bicycling 4 miles in 15 minutes
Jumping rope for 15 minutes
Running 11/2 miles in 15 minutes (10 minutes per mile)
Shoveling snow for 15 minutes More Vigorous,Stairwalking for 15 minutes Less Time
*The amount of physical activity is influenced by its duration, intensity,and frequency. The same amount of activity can be obtained in longersessions of moderately intense activities (such as brisk walking) as inshorter sessions of more strenuous activities (such as running).
Adapted from: Chronic Disease Notes & Reports, a publication of theCenters for Disease Control and Prevention.171
To achieve the American Cancer Society physical activityguidelines, adults may choose a variety of activities. Someexamples from the table above include:
• Bicycle 5 miles in 30 minutes
• Walk 2 miles in 30 minutes or run 11/2 miles in 15 minutes
• Garden for 30 minutes
• Play volleyball for 45 minutes

32 Cancer Prevention & Early Detection Facts & Figures 2005
One way to enhance efforts to increase physical activityand reduce obesity is for communities to increase accessto safe and convenient physical activity. Such initiativesmight include:175
• Modifying the design of new residential communitiesto allow residents to walk or bike to shops, schools,and other services (mixed-use development).
• Developing worksite programs that encourage physi-cal activity, especially for people with sedentary jobs.
Based on a systematic review on the effectiveness ofcommunity interventions to increase physical activity,the Task Force on Community Preventive Servicesstrongly recommends the following interventions: com-munity-wide campaigns, use of signs near stairs toencourage people to use them, social support interven-tion (i.e., social networks that provide supportive rela-tionships for physical activity behavior change, such assetting up walking groups among friends), and environ-mental and policy approaches to create and improveaccess to places for physical activity in the communityand worksites.171
Vegetable and Fruit ConsumptionThe International Agency for Research on Cancer(IARC) recently published a report documenting the evi-dence on the preventive effect of vegetable and fruit con-sumption on cancer. It found the most conclusiveevidence for cancers of the mouth and pharynx, esopha-gus, larynx, lung, stomach, kidney, colon and rectum,ovary (vegetables only), and bladder (fruit only).158 Thespecific protective factors in vegetable and fruit con-sumption have not been identified with certainty, and itis possible that their consumption may be a marker forsome other associated dietary or lifestyle factor. TheIARC review concluded that the evidence supported the current recommendations of many organizations(including the American Cancer Society) to promoteconsumption of vegetables and fruits for the reductionof cancer risk.158
Since its inception in 1991, the national 5 A Day forBetter Health program has become one of the mostwidely recognized health promotion programs in theworld. As the largest public/private partnership fornutrition education, the 5 A Day program’s strength isthe combined efforts of the National Cancer Institute(NCI), the Produce for Better Health Foundation, theAmerican Cancer Society, the Centers for Disease
Approaches to Improving PhysicalActivity and Nutrition for Adults 6,50
• Encourage restaurants to provide nutrition information onmenus (calories, fat, transfat, sugars, etc.).
• Invest in community design that supports development ofsidewalks, bike lanes, and access to parks and greenspace.
• Implement a large-scale marketing campaign, targetingconsumers and decision-makers, to increase awareness ofthe lifestyle/cancer connection and to motivate people tomake their worksites, schools, and communities more“health friendly.”
• Develop and promote “communities of excellence” pro-grams in nutrition and physical activity that exemplify pol-icy and environmental changes within worksites, schools,and communities that increase access to healthy foodsand opportunities for physical activity.
• Increase federal funding so states can implement compre-hensive nutrition and physical activity plans.
• Encourage collaboration among government, nonprofit,and private sectors to develop research and interventionprograms.
• Increase resources from governmental and nongovern-mental sources to facilitate a strategic and action-orientedplan to address the obesity problem.

Cancer Prevention & Early Detection Facts & Figures 2005 33
Control and Prevention, the United States Departmentof Agriculture, the United Fresh Fruit and VegetableAssociation, the Produce Marketing Association, andthe National Alliance for Nutrition and Activity.
This program seeks to increase the number of individu-als consuming 5 to 9 servings of vegetables and fruitsdaily. A recent evaluation showed that awareness of the5 A Day program message has increased amongadults,176 an increase that has coincided with a slow butsteady increase in vegetable and fruit consumption dur-ing the period 1994 to 1998.176 The 5 A Day program iscontinuing an initiative to increase the availability offruits and vegetables in schools by increasing the num-ber of salad bars in school lunch programs.
Two campaigns for adults initiated in 2003 are targetedat men, the Men’s 9 A Day campaign and the African-American Men’s 9 A Day campaign. Media campaignshave included radio spots on ABC’s Urban AdvantageNetwork, reaching more than 225 urban stations, and anInternet site featuring upbeat messages and tips for
changing dietary habits, all addressing AfricanAmerican men. A new NCI brochure, Men Eat 9 A Day, isdistributed by NCI’s partners, including the NationalAssociation for the Advancement of Colored People(NAACP) and the National Medical Association (NMA).Through the National Newspaper Publishers Associa-tion, NCI collaborates with African American-ownednewspapers across the country on a column, Eat Better,Live Better.177 More information can be found atwww.5aday.gov.
Even so, consumption of vegetables and fruits remainsmuch lower than recommended levels. Only 23.5% ofAmericans surveyed in the 2003 Behavioral Risk FactorSurveillance System reported eating 5 or more servingsof vegetables and fruits a day. This ranged from 15.4% inOklahoma to 32.5% in Vermont (Table 2C). In general,the proportion of adults eating 3 or more servings ofvegetables per day is even lower than the proportion ofadults consuming 2 or more fruit servings per day (Table2C).
Success StoriesExamples of community programs to improvephysical activity and nutritionThis section highlights five community programs designed toimprove nutrition and physical activity.
The statewide Colorado Physical Activity andNutrition (COPAN) programThe Colorado Physical Activity and Nutrition State Plan 2010,known as COPAN, was jointly prepared by the ColoradoCoalition on Physical Activity and Nutrition and the ColoradoDepartment of Public Health and Environment. The planincludes specific steps the state intends to take to address theobesity epidemic. One component of the plan is calledColorado on the MoveTM, a statewide initiative that worksthrough schools and worksites and with communities toencourage residents to increase walking by 2,000 steps per day(about a mile). The program offers pedometers to support par-ticipants in counting their steps and increasing their daily activ-ity levels. More than 100,000 pedometers have beendistributed in Colorado, and an initial evaluation indicates thatmost participants have been able to add 2,000 steps to theirday’s activities. The Colorado 5 A Day for Better Health is thenutritional component of the statewide program whichemphasizes consumption of 5 or more servings of fruits andvegetables daily. In an evaluation study, it was documentedthat from 1994 to 2000, the percentage of Colorado adults
who consumed at least 5 servings of fruits and vegetables on adaily basis increased from 21.6% to 23.4%, and the averagenumber of daily servings increased from 3.7 to 3.9 servings perday.178 Because of the modest observed increases in behaviorsachieved by this program, future efforts will involve identifyingbetter strategies leading to wider program impacts.
The Seattle 5 A Day programThis is a tested intervention designed for worksites to increaseemployees’ vegetable and fruit consumption using bothenvironmental approaches (in the cafeteria, and more broadly,at work) and individual behavioral strategies. At the worksite,an employee advisory board develops activities to recruitemployees for participation in the program. Examples of activi-ties include messages to raise awareness about eating vegeta-bles and fruits; skill-building activities for employees; changesin the worksite cafeteria, including point-of-purchase displays,signs identifying foods as 5 A Day foods, and spotlights onhealthy eating; and, in some instances, incentives for eatingmore vegetables and fruits. Messages are delivered throughposters, newsletters, table tents, and a self-help manual. Anoutcome evaluation study documented that the interventionproduced both an increase in employees’ use of materials andactivities and increases in consumption of vegetables andfruits.179
continued on page 34

34 Cancer Prevention & Early Detection Facts & Figures 2005
Success Stories, continued
The WISEWOMAN programThe Well-Integrated Screening and Evaluation for WomenAcross the Nation (WISEWOMAN) program is a CDC-spon-sored program currently being implemented in 15 communitiesacross the US. WISEWOMAN programs operate at the locallevel through community partnerships which help strengthenthe program by pooling resources and sharing lessons learned.Specifically, the program targets economically disadvantagedwomen who are particularly vulnerable to obesity, smoking,and other risk factors for chronic disease. The mission is toprovide low-income and uninsured women, aged 40-64, withthe knowledge, skills, and opportunities to improve their diet,physical activity, and other lifestyle behaviors to prevent, delay,and control chronic diseases. The program offers these womena comprehensive approach to preventive services (screening forchronic risk factors such as smoking and overweight) andpromotes behavioral change through education, counseling,and culturally appropriate activities that foster healthylifestyles.180 An evaluation study of the MassachusettsWISEWOMAN project documented significant increases in thedaily consumption of vegetables and fruits, as well as in partic-ipation in moderate levels of physical activity at least 3 times aweek for 30 minutes or more per day.181
Body & Soul: A Celebration of Healthy LivingThis celebration of healthy living is a joint program of theAmerican Cancer Society, the NCI, and the CDC. The programworks through faith-based communities to encourage AfricanAmericans to eat at least 5 servings of vegetables and fruitseach day. The program includes pastor support and involve-ment, church activities, and policy and environmental changeswithin the church. A randomized effectiveness trial conductedamong approximately 1,000 members from 15 AfricanAmerican churches demonstrated that at the 6-month followup, participants reported increased vegetable and fruit con-sumption and greater motivation to eat those foods, as well assignificant decreases in fat consumption.182
Signs that encourage people to use the stairsA recent review of intervention studies to evaluate the effec-tiveness of signs encouraging the use of nearby stairs showedthat this intervention significantly increased stair usage. Placedby elevators and escalators, the signs encourage people to usenearby stairs for health benefits or weight loss by describing thebenefits of taking the stairs and reminding people in elevatorsthat the stairs are an opportunity to be more active. A versatileintervention, it is also effective in railway, subway, and busstations; shopping malls; and university libraries. In one study,obese people used the stairs more often if the signs linked stairuse to weight loss rather than to health benefits.171

Cancer Prevention & Early Detection Facts & Figures 2005 35
Cancer Screening
Aside from tobacco avoidance and maintaining ahealthy weight, following recommendations from theAmerican Cancer Society or US Preventive Services TaskForce for cancer screening is the most important thingpeople can do to reduce their chances of dying fromcancer. Screening can identify persons who may havecancer or pre-cancerous tissue changes that warrant fur-ther evaluation. It can also detect cancers earlier in theirdevelopment, which often can improve the effectivenessof treatment and prevent death. Screening has beenshown to reduce mortality from cancers of the breast,cervix, and colon and rectum. There are also othercancers for which screening may be associated withlower mortality, but the evidence is less certain.183 Seepage 36 for the American Cancer Society’s screeningguidelines for the early detection of cancer in asympto-matic people.
Breast Cancer ScreeningBreast cancer screening has been shown to reduce breastcancer mortality. Currently, 63% of breast cancers arediagnosed at a localized stage, for which the 5-year sur-vival rate is 97.5%.1 The relatively high rates of earlydetection of breast cancer can be attributed to use ofmammography screening, as well as to high awareness ofbreast cancer symptoms in the population. However,African American, Hispanic/Latina, and AmericanIndian/Alaska Native women are more likely to be diag-nosed at regional and distant stages than whites andAsian Americans/Pacific Islanders.1
National breast cancer screening data are available from2 different sources: the National Health Interview Survey(NHIS) and the Behavioral Risk Factor SurveillanceSystem (BRFSS), both of which measure screeningwithin the past year and the past 2 years. According tothe NHIS, the percentage of women aged 40 and olderwho reported having had a mammogram within the past2 years (following the US Preventive Services Task Forcerecommendations) increased from 29% in 1987 to 70% in2000.184 While the difference between non-Hispanicwhite and African American women narrowed duringthat time, there was less progress in closing the gap forother racial and ethnic groups.184 In 2000, the prevalenceof mammography use in the past 2 years among whitewomen 40 and older was 72.1 %, 68.2% among AfricanAmericans, 62.6% among Hispanics/Latinas, 52.4%among American Indians/Alaska Natives, and 57.0%among Asian Americans (Table 3A).
Table 3A. Mammography, Women 40 andOlder, US, 2000
% % Mammogram Mammogram
within the past within the Characteristic 2 years* past year*
Race/EthnicityWhite (non-Hispanic) 72.1 56.9African American (non-Hispanic) 68.2 52.8Hispanic/Latina 62.6 48.0American Indian and Alaska Native 52.4 36.6Asian American† 57.0 47.8
Education (years)11 or fewer 56.8 41.712 68.9 54.713 to 15 73.3 58.216 or more 80.1 65.1
Health insurance coverageYes 73.6 58.3No 39.5 27.9
Immigration
Born in US 71.6 56.2
In US fewer than 10 years 41.4 33.7In US 10 years or more 65.0 50.9
Total 70.3 55.3
*Percentages are age-adjusted to 2000 US standard population. SeeStatistical Notes on page 47 for more information. †Does not includeNative Hawaiians and other Pacific Islanders.
Source: National Health Interview Survey Public Use Data File 2000,National Center for Health Statistics, Centers for Disease Control andPrevention, 2002.
American Cancer Society, Surveillance Research

36 Cancer Prevention & Early Detection Facts & Figures 2005
Screening GuidelinesFor the Early Detection of Cancer in Asymptomatic PeopleSite Recommendation
Breast • Yearly mammograms are recommended starting at age 40. The age at which screening should be stopped shouldbe individualized by considering the potential risks and benefits of screening in the context of overall healthstatus and longevity.
• Clinical breast exam should be part of a periodic health exam, about every 3 years for women in their 20s and30s, and every year for women 40 and older.
• Women should know how their breasts normally feel and report any breast change promptly to their health careproviders. Breast self-exam is an option for women starting in their 20s.
• Women at increased risk (e.g., family history, genetic tendency, past breast cancer) should talk with their doc-tors about the benefits and limitations of starting mammography screening earlier, having additional tests (i.e.,breast ultrasound and MRI), or having more frequent exams.
Colon & Beginning at age 50, men and women should begin screening with 1 of the examination schedules below: rectum • A fecal occult blood test (FOBT) or fecal immunochemical test (FIT) every year
• A flexible sigmoidoscopy (FSIG) every 5 years• Annual FOBT or FIT and flexible sigmoidoscopy every 5 years*• A double-contrast barium enema every 5 years• A colonoscopy every 10 years*Combined testing is preferred over either annual FOBT or FIT, or FSIG every 5 years, alone. People who are at moderate or highrisk for colorectal cancer should talk with a doctor about a different testing schedule.
Prostate The PSA test and the digital rectal examination should be offered annually, beginning at age 50, to men who havea life expectancy of at least 10 years. Men at high risk (African American men and men with a strong family historyof 1 or more first-degree relatives diagnosed with prostate cancer at an early age) should begin testing at age 45.For both men at average risk and high risk, information should be provided about what is known and what isuncertain about the benefits and limitations of early detection and treatment of prostate cancer so that they canmake an informed decision about testing.
Uterus Cervix: Screening should begin approximately 3 years after a woman begins having vaginal intercourse, but nolater than 21 years of age. Screening should be done every year with regular Pap tests or every 2 years using liquid-based tests. At or after age 30, women who have had 3 normal test results in a row may get screened every 2 to 3years. Alternatively, cervical cancer screening with HPV DNA testing and conventional or liquid-based cytologycould be performed every 3 years. However, doctors may suggest a woman get screened more often if she hascertain risk factors, such as HIV infection or a weak immune system. Women 70 years and older who have had 3or more consecutive normal Pap tests in the last 10 years may choose to stop cervical cancer screening. Screeningafter total hysterectomy (with removal of the cervix) is not necessary unless the surgery was done as a treatmentfor cervical cancer.Endometrium: The American Cancer Society recommends that at the time of menopause all women should beinformed about the risks and symptoms of endometrial cancer, and strongly encouraged to report any unexpectedbleeding or spotting to their physicians. Annual screening for endometrial cancer with endometrial biopsy begin-ning at age 35 should be offered to women with or at risk for hereditary nonpolyposis colon cancer (HNPCC).
Cancer- For individuals undergoing periodic health examinations, a cancer-related checkup should include health related counseling, and, depending on a person’s age and gender, might include examinations for cancers of the thyroid, checkup oral cavity, skin, lymph nodes, testes, and ovaries, as well as for some nonmalignant diseases.
American Cancer Society guidelines for early cancer detection are assessed annually in order to identify whether there is new scientific evidence sufficient to war-rant a reevaluation of current recommendations. If evidence is sufficiently compelling to consider a change or clarification in a current guideline or the develop-ment of a new guideline, a formal procedure is initiated. Guidelines are formally evaluated every 5 years regardless of whether new evidence suggests a change inthe existing recommendations. There are 9 steps in this procedure, and these “guidelines for guideline development” were formally established to provide a spe-cific methodology for science and expert judgment to form the underpinnings of specific statements and recommendations from the Society. These proceduresconstitute a deliberate process to ensure that all Society recommendations have the same methodological and evidence-based process at their core. This processalso employs a system for rating strength and consistency of evidence that is similar to that employed by the Agency for Health Care Research and Quality(AHCRQ) and the US Preventive Services Task Force (USPSTF).
©2005, American Cancer Society, Inc.

The lowest prevalence of mammography use in the pasttwo years occurred among women who lack healthinsurance (39.5%) and immigrant women who have livedin the US for fewer than 10 years (41.4%) (Table 3A). The2000 NHIS survey found that only 55.3% of womenreported having a mammogram within the past year,consistent with the American Cancer Society’s cancerscreening recommendations.
According to Behavioral Risk Factor Surveillance Systemdata for states collected in 2002 (Table 3B), the percent-age of women 40 and older who reported having a mam-mogram in the last year (as recommended by theAmerican Cancer Society) ranged from 51.1 % in Utah to71.6 % in Delaware. Interestingly, Utah is also the onlystate for which state law does not take steps to ensurethat mammography screening is covered by privateinsurers.185 For a recent mammogram and clinical breastexam, the percentages were 3 to 12 percentage pointslower than for a recent mammogram, ranging from43.7% in Utah to 64.3% in Massachusetts. Having a usualsource of care is an indicator of access to preventivehealth care services and is related in part to health carecoverage. In almost all states, women who lack a usualsource of care or are uninsured have a much lower prev-alence of breast cancer screening than the generalpopulation.
Cervical Cancer ScreeningCervical cancer incidence and mortality rates havedecreased markedly in the past several decades, withmost of the reduction attributed to the Pap test, whichdetects cervical cancer and pre-cancerous lesions.186
Cervical cancer is one of the most successfully treatablecancers when detected at an early stage.186
In 1987, approximately three-quarters (73%) of womenaged 25 and older had a Pap test within the past 3 yearsand by 2000, the proportion had increased to 82%,according to National Health Interview Survey data.184
The lowest prevalence of cervical cancer screeningamong women aged 18 and older in 2000 occurred inwomen with no health insurance (64.1%) and in recentimmigrants (59.3 %). The prevalence of cervical cancerscreening varied by race and ethnicity: Asian American(68.2%), American Indian/Alaska Native (78.4%),Hispanic/Latina (77.9%), African American (85.5%), andnon-Hispanic white (83.9%) (Table 3C). Across the statessurveyed by the Behavioral Risk Factor SurveillanceSystem in 2002 (Table 3D), the recent Pap test percent-age among women aged 18 and older was 86.2 %, rangingfrom 80.1% in Utah to 91.7% in Maryland.
Cancer Prevention & Early Detection Facts & Figures 2005 37
Programs to Increase the Rate of Breast andCervical Cancer Screening• The Centers for Disease Control and Prevention’s
National Breast and Cervical Cancer Early DetectionProgram (NBCCEDP) helps low-income, uninsured,and underserved women gain access to screeningexams for the early detection of breast and cervicalcancers.187 Since about 15% of the US population iswithout health insurance, the NBCCEDP programlikely contributed to the 18% increase in mammogra-phy use among women older than age 50 since theprogram’s inception in 1991. To date, about 50% of thewomen screened in the program have been fromracial/ethnic minority groups. More than 4 millionscreening tests have been provided, leading to thediagnosis of about 14,446 breast cancers, 55,210 pre-cancerous cervical lesions, and 1,020 cases of invasivecervical cancer.187 The Centers for Disease Control andPrevention estimates that the program is currentlyreaching approximately 20% of eligible women. TheAmerican Cancer Society has advocated for additionalfunding so that more eligible women can benefit. Thepassage of the Breast and Cervical Cancer Preventionand Treatment Act, effective October 1, 2000, gavestates the option to provide medical assistance andfollow-up treatment through the Medicaid program toeligible women who were screened in the NBCCEDP.As of December 2004, 49 states and the District ofColumbia have elected to provide this coverage.187
Currently, the Society is working to increase federalfunding for the screening program, as well as to ensurethat state dollars supporting the treatment programare protected.
• The Medicare program now covers annual mammo-grams for women aged 65 and older. Research andrecent efforts to raise awareness about the Medicaremammography benefit and other screening optionsled to the implementation of a program in whichpersonalized letters were mailed to eligible women.The letters included information about breast cancerrisk for women in their age group and a facility guideto where they could obtain low-cost screening mam-mograms in their communities. An evaluation of thisprogram showed a significant two-fold increase in therate of mammography use among the group of womenwho received the letter compared to those who didnot.188

38 Cancer Prevention & Early Detection Facts & Figures 2005
Table 3B. Mammography and Clinical Breast Exam, Women 40 and Older, by State, 2002% Recent mammogram* % Recent mammogram and clinical breast exam†
No usual No usual source of No source of No
40 years 40 to 64 65 years medical health 40 years 40 to 64 65 years medical health and older years and older care‡ insurance§ and older years and older care‡ insurance§
Alabama 65.3 64.9 66.4 40.4 40.8 57.1 58.9 53.3 35.1 36.2Alaska 53.9 51.3 66.8 28.0 35.3 50.6 48.9 59.7 26.2 34.0Arizona 63.8 60.1 71.2 36.8 30.2 56.4 56.0 57.0 27.6 25.4Arkansas 53.5 52.7 54.9 19.7 30.9 46.6 47.8 44.3 16.8 28.0California|| 60.7 59.1 64.6 35.7 39.7 48.5 49.7 45.8 28.4 28.3
Colorado 59.8 59.4 61.0 32.8 25.9 53.4 55.3 47.9 21.8 21.1Connecticut 68.7 69.0 68.1 43.9 46.8 61.9 63.9 58.0 35.6 41.9Delaware 71.6 71.5 72.0 45.9 39.8 64.2 64.8 62.8 40.2 35.3Dist. of Columbia 68.7 68.8 68.5 39.5 ¶ 61.9 63.7 58.4 37.5 ¶
Florida 66.7 65.1 69.5 44.2 41.6 60.0 60.3 59.5 40.3 39.1
Georgia 59.9 59.4 61.4 30.3 32.5 53.3 54.0 51.5 26.9 28.4Hawaii 56.3 55.1 59.1 36.1 26.7 50.3 50.2 50.6 32.5 24.8Idaho 51.4 50.4 53.7 29.9 27.8 46.4 47.0 45.0 28.5 25.0Illinois 60.2 59.6 61.6 28.8 37.8 51.9 53.5 48.5 18.1 28.1Indiana 57.1 57.8 55.7 24.0 36.3 50.0 53.2 43.0 21.3 32.5
Iowa 64.9 66.0 63.0 40.4 38.9 60.3 63.1 54.9 36.6 35.0Kansas 63.2 60.8 68.0 34.3 29.7 57.5 57.3 58.0 30.1 29.0Kentucky 61.7 61.8 61.5 40.9 34.5 57.2 58.1 55.2 36.4 32.0Louisiana 64.9 64.1 66.7 46.2 43.6 56.8 57.3 55.5 40.4 38.0Maine 67.4 65.7 70.9 ¶ 37.3 59.4 60.0 58.0 ¶ 29.1
Maryland 67.1 67.4 66.3 33.0 49.0 61.2 62.3 58.4 27.2 43.6Massachusetts 70.2 70.2 70.2 34.5 41.9 64.3 64.8 63.2 31.2 42.3Michigan 61.8 60.4 65.1 34.0 41.2 54.8 55.5 53.2 29.9 32.1Minnesota 64.9 63.4 68.3 41.8 ¶ 59.9 59.6 60.7 37.8 ¶
Mississippi 52.9 52.0 54.8 31.5 30.8 46.8 47.3 45.6 26.7 27.2
Missouri 59.0 58.8 59.3 25.8 29.6 51.5 54.3 45.5 17.9 22.9Montana 57.1 56.0 59.6 38.3 23.2 51.6 51.6 51.6 33.9 21.1Nebraska 59.5 61.1 56.5 25.9 31.1 55.4 58.5 49.4 20.2 28.5Nevada 57.7 55.9 62.6 33.6 42.2 47.0 46.7 47.7 26.5 32.8New Hampshire 66.7 66.8 66.4 31.1 33.4 60.7 61.8 58.1 28.8 29.4
New Jersey 64.2 64.2 64.1 33.6 45.2 58.2 60.3 54.1 29.7 39.4New Mexico 51.3 50.0 54.8 26.2 23.5 46.1 45.7 47.1 22.7 20.8New York 63.7 63.0 65.1 35.0 42.7 55.2 55.9 53.6 30.4 34.4North Carolina 67.6 66.2 70.9 44.0 44.2 62.5 62.1 63.3 39.9 40.2North Dakota 61.8 60.1 64.8 33.7 31.7 55.5 56.3 53.9 30.3 33.1
Ohio 61.7 60.2 64.8 42.4 40.0 54.8 55.5 53.4 39.3 37.3Oklahoma 54.9 54.7 55.4 31.5 32.0 47.8 49.3 44.6 24.1 25.5Oregon 57.8 54.4 65.7 27.1 25.5 49.6 48.7 51.7 24.2 23.1Pennsylvania 62.0 61.8 62.5 30.2 38.0 54.5 56.3 51.3 26.0 33.3Rhode Island 71.5 70.6 73.0 37.4 57.3 64.0 65.4 61.5 30.7 47.3
South Carolina 58.3 55.5 64.9 33.2 34.8 51.0 49.8 53.7 28.1 29.0South Dakota 63.4 62.9 64.3 39.2 48.8 58.8 59.7 57.1 36.5 45.7Tennessee 63.9 64.1 63.3 29.3 38.3 58.7 60.5 54.7 23.0 38.1Texas 52.4 51.6 54.3 21.9 28.1 45.6 46.6 42.9 15.5 24.2Utah 51.1 51.1 51.0 28.2 31.0 43.7 46.3 36.9 19.3 25.5
Vermont 62.8 61.0 67.1 32.9 36.8 57.0 57.1 56.8 30.3 34.1Virginia 59.1 57.8 62.3 33.0 32.9 51.8 51.7 52.0 27.2 28.3Washington 58.6 56.3 64.3 22.0 34.1 52.6 52.5 52.9 21.3 31.9West Virginia 60.5 61.9 57.9 39.9 38.7 52.1 55.3 45.8 35.1 35.0Wisconsin 64.5 63.5 66.8 24.6 44.8 57.8 58.2 57.1 22.3 39.3Wyoming 52.8 52.3 53.9 34.1 32.2 44.5 46.3 39.8 28.5 30.3
United States# 61.5 60.5 63.8 33.7 36.6 54.1 54.9 52.3 28.3 31.4Range 51.1-71.6 50.0-71.5 51.0-73.0 19.7-46.2 23.2-57.3 43.7-64.3 45.7-65.4 36.9-63.3 15.5-40.4 20.8-47.3
*A mammogram within the past year. †Both a mammogram and clinical breast exam within the past year. ‡Women 40 and older who reported that they did not have apersonal doctor or health care provider. §Women aged 40 to 64 who reported they they did not have any kind of health care coverage, including health insurance, prepaidplans such as HMOs, or government plans such as Medicare. ||Questions for mammogram and clinical breast exam differed and may not be comparable to the state per-centages in this table. ¶Sample size is insufficient to provide a stable estimate. #See Statistical Notes on page 47 for definition.
Source: Behavioral Risk Factor Surveillance System Public Use Data Tape 2002, National Center for Chronic Disease Prevention and Health Promotion, Centers for DiseaseControl and Prevention, 2003.
American Cancer Society, Surveillance Research

Cancer Prevention & Early Detection Facts & Figures 2005 39
Colorectal Cancer ScreeningColorectal cancer screening reduces death from colo-rectal cancer. It is also one of the few cancers that can beprevented through screening because adenomatouspolyps, from which colon cancers often develop, can beidentified and removed during screening. Several avail-able screening options (i.e., the fecal occult blood home-test kit, endoscopy procedures such as the flexiblesigmoidoscopy or colonoscopy, and radiological imagingwith double-contrast barium enema) can be effective indetecting the disease.183,189
Early diagnosis and treatment of colorectal cancerresults in a survival rate of 90%. However, only 39% ofcases are diagnosed at this early stage.1 Despite the avail-ability of different screening methods and their life-
saving potential, colorectal cancer screening is notwidely used.190,191 From 1987 to 2000, the use of a colo-rectal cancer screening test (either a fecal occult bloodtest [FOBT] within the last year or a colorectal endo-scopic procedure within the last 3 years) among USadults aged 50 and older increased by 12% (from 27% in1987 to 39% in 2000) based on National Health InterviewSurvey data.184 Data from the CDC’s Behavioral RiskFactor Surveillance System showed little increase incolorectal cancer screening from 1997 to 2001.192
Colorectal cancer screening rates among US adults aged50 and older in 2000 varied by gender, race, education,health insurance coverage, and immigration status. Theywere lowest among those without health insurance (13%for FOBT within the past year and 14.4% for endoscopywithin the past 5 years); among those with less than ahigh school education (12.1% for FOBT and 22.0% forendoscopy); among Hispanics/Latinos (9.8% for FOBTand 21.8% for endoscopy); and among recent immigrants(3.3% for FOBT and 14.3% for endoscopy) (Table 3E).
Across the states surveyed in 2002 by the Behavioral RiskFactor Surveillance System (Table 3F), the recent fecaloccult blood test percentages for adults aged 50 andolder ranged from 12.2% in Utah to 33.4% in Maine.Percentages for adults 50 and older who had a recent(within the preceding 5 years) sigmoidoscopy or colon-oscopy ranged from 30.1% in Wyoming to 54.9% inMinnesota. In general, adults aged 65 and older weremore likely to have had a colorectal cancer screening testcompared to those between the ages of 50 and 64. Theprevalence of colorectal cancer screening was even lowerfor adults 50 and older who lacked a usual source of careor who were uninsured (Table 3F). An American CancerSociety study also showed that lack of access to a usualsource of care, as well as other socioeconomic factors,such as low educational attainment and lack of healthinsurance, were associated with under-utilization ofcolorectal cancer screening.191
Lack of coverage for the full range of colorectal cancerscreening tests may contribute to low utilization of thesetests, and it is difficult to determine the extent to whichinsurers cover these screening tests in accordance withAmerican Cancer Society guidelines. Plans often con-sider such information proprietary, and there can be alack of clarity about which specific tests are covered,whether coverage is available for true screening or lim-ited to diagnostic testing, or whether the full range oftests is available to people at average risk or limited tothose at high risk. Limited data currently available
Table 3C. Pap Test*, Women 18 and Older, US,2000Characteristic %†
Age (years)18-20 59.921-29 86.830-39 89.840-49 86.850-59 87.860-64 82.565-85 68.4
Race/EthnicityWhite (non-Hispanic) 83.9African American (non-Hispanic) 85.5Hispanic/Latina 77.9American Indian and Alaska Native 78.4Asian American‡ 68.2
Education (years)§11 or fewer 74.312 82.513-15 86.216 or more 90.1
Health insurance coverageYes 85.2No 64.1
ImmigrationBorn in US 84.1In US fewer than 10 years 59.3In US 10 years or more 79.2
Total 82.3
*A Pap test within the past 3 years for women with intact uteri.†Percentages are age-adjusted to 2000 US standard population. SeeStatistical Notes on page 47 for more information. ‡Does not includeNative Hawaiians and other Pacific Islanders. §Women aged 25 andolder.
Source: National Health Interview Survey Public Use Data File, 2000,National Center for Health Statistics, Centers for Disease Control andPrevention, 2002.
American Cancer Society, Surveillance Research

40 Cancer Prevention & Early Detection Facts & Figures 2005
Table 3D. Pap Test, Women 18 and Older, by State, 2002% Recent Pap test*
No usual source No health 18 years and older 18 to 64 years 65 years and older of medical care† insurance‡
Alabama 88.2 89.8 77.1 78.2 81.0Alaska 90.0 90.6 79.4 83.5 79.5Arizona 88.2 88.9 83.7 73.1 76.6Arkansas 83.0 86.0 64.3 62.1 75.1California§ 84.4 84.6 82.3 71.4 75.4
Colorado 88.7 90.3 73.9 79.4 79.0Connecticut 88.4 90.6 76.2 79.0 77.4Delaware 87.1 93.3 74.8 || ||
Dist. of Columbia 89.4 91.5 73.7 78.2 85.1Florida 86.0 88.0 77.0 75.9 76.8
Georgia 89.3 91.0 70.3 76.3 85.0Hawaii 85.6 88.1 71.3 73.8 70.9Idaho 83.5 86.1 63.0 70.3 73.6Illinois 84.2 86.4 72.0 74.5 76.8Indiana 85.0 87.2 70.9 64.6 73.7
Iowa 87.8 90.4 75.4 76.7 77.8Kansas 87.8 89.6 77.5 79.3 83.2Kentucky 84.3 85.4 76.4 73.5 74.3Louisiana 88.6 90.1 74.8 82.9 83.1Maine 91.5 93.4 80.7 72.3 83.7
Maryland 91.7 93.9 76.4 79.9 86.9Massachusetts 88.1 90.6 73.4 70.5 77.2Michigan 87.6 89.4 75.3 78.7 83.0Minnesota 89.7 90.9 81.5 81.0 78.0Mississippi 83.9 86.9 61.2 79.3 79.7
Missouri 84.2 87.8 65.3 67.1 76.4Montana 84.8 85.7 78.7 73.0 74.5Nebraska 86.3 88.9 71.7 81.1 84.5Nevada 82.9 84.9 66.7 72.2 77.1New Hampshire 90.2 92.0 78.3 76.0 84.2
New Jersey 85.3 88.1 70.5 70.3 74.1New Mexico 84.0 86.2 68.0 73.3 74.1New York 84.8 87.0 72.4 70.0 67.3North Carolina 89.9 91.6 79.5 78.0 84.4North Dakota 86.6 88.1 78.8 79.5 69.0
Ohio 86.4 88.5 73.8 73.7 75.2Oklahoma 83.0 85.4 64.9 69.8 76.6Oregon 85.5 87.2 72.9 77.2 77.4Pennsylvania 85.1 88.4 68.5 72.5 77.9Rhode Island 89.8 92.5 74.7 73.0 78.5
South Carolina 87.9 88.0 87.5 75.0 78.5South Dakota 86.3 89.1 71.8 78.2 81.9Tennessee 88.7 91.2 71.2 83.6 87.6Texas 83.7 85.2 70.1 71.8 78.3Utah 80.1 81.6 61.5 69.3 65.4
Vermont 89.1 91.2 76.5 77.8 79.5Virginia 89.2 90.4 79.7 76.8 76.4Washington 87.1 88.5 76.2 71.7 76.1West Virginia 85.2 88.8 67.5 78.0 82.2Wisconsin 87.9 90.1 74.6 71.1 71.5Wyoming 84.7 87.0 67.8 72.9 77.8
United States¶ 86.2 88.0 74.4 73.8 77.3Range 80.1-91.7 81.6-93.9 61.2-87.5 62.1-83.6 65.4-87.6
*A Pap test within the preceding 3 years for women with intact uteri. †Women 18 and older who reported that they did not have a personal doctor or health careprovider. ‡Women aged 18 to 64 who reported that they did not have any kind of health care coverage, including health insurance, prepaid plans such as HMOs, orgovernment plans such as Medicare. §Questions for Pap test differed and may not be comparable to the state percentages in this table. ||Sample size is insufficientto provide a stable estimate. ¶See Statistical Notes on page 47 for definition.
Source: Behavioral Risk Factor Surveillance System Public Use Data Tape 2002, National Center for Chronic Disease Prevention and Health Promotion, Centers forDisease Control and Prevention, 2003.
American Cancer Society, Surveillance Research

Cancer Prevention & Early Detection Facts & Figures 2005 41
suggest that many plans do not cover the full range ofscreening tests and that many do not cover screeningcolonoscopy for people at average risk.193,194 In addition,very few health plans have all 3 essential colorectalcancer screening delivery components – coverage,guidelines, and tracking systems – in place.194
Improving insurance coverage for colorectal cancerscreening tests is a priority for the American CancerSociety, which has advocated for states to pass legis-lation to ensure that private health insurance planscover the full range of screening methods available forcolorectal cancer screening. To date, 16 states and theDistrict of Columbia have passed such legislation (Figure3A).8 The Society has also advocated at the federal levelfor full coverage of colorectal cancer screening tests.Since 2001, Medicare has covered all Society-recommended colorectal cancer screening options. Inaddition, the Society has worked with the Office ofPersonnel Management to increase the proportion ofhealth plans offered to federal employees that cover thefull range of tests.
As part of its efforts to encourage coverage of the fullrange of colorectal cancer screening options, the Societyworked with an economic consulting firm to estimatethe short-term costs of adding screening colonoscopy toa health plan’s list of options, compared with FOBT andflexible sigmoidoscopy. The data indicate that colonos-copy done once every 10 years is actually less costly interms of per-member, per-month costs than flexiblesigmoidoscopy every 5 years combined with an annualFOBT.195
The Society also took a leading role in securing a pre-ventive care coverage benefit that will help promotescreening under the Medicare Prescription Drug,Improvement, and Modernization Act of 2003.Beginning in 2005, all new Medicare beneficiaries areeligible for an initial preventive physical exam (known asthe “Welcome to Medicare” physical exam) availablewithin 6 months of enrolling in Medicare, during whichphysicians can refer patients for needed screeningbenefits, such as colorectal cancer screenings.8
Also of note are recent strategies by the federal govern-ment (e.g., the Centers for Disease Control and Preven-tion [CDC] Screen for Life awareness campaigns), privatenonprofit organizations (e.g., the National ColorectalCancer Roundtable), and the collaboration between theAd Council and the American Cancer Society (e.g., PolypMan®, see page 43) that aim to raise awareness of colo-rectal cancer screening and to remove existing obstaclesto early detection.
• The Centers for Disease Control and Prevention’s colo-rectal cancer prevention and control initiative helpseducate the public and health care providers about theimportance of colorectal cancer screening.196 In addi-tion, the CDC conducts research on nationwide capac-ity for colorectal cancer screening and strategies toincrease use of colorectal cancer screening rates andworks with its national partners (including theAmerican Cancer Society) to raise colorectal cancerawareness.
• The National Colorectal Cancer Roundtable (NCCRT)is a national coalition of public, private, and voluntaryorganizations, co-founded by the American CancerSociety and the CDC, whose mission is to advancecolorectal cancer control efforts by improving com-munication, coordination, and collaboration amonghealth agencies, medical-professional organizations,and the public. The ultimate goal of this multi-
Table 3E. Colorectal Cancer Screening, Adults50 and Older, US, 2000
Fecal occult blood test* Endoscopy†
Characteristic %‡ %‡
GenderMale 17.1 33.5Female 17.6 27.0
Race/EthnicityWhite (non-Hispanic) 18.3 31.3African American (non-Hispanic) 14.9 27.0Hispanic/Latino 9.8 21.8American Indian and Alaska Native§ 14.0 25.2Asian American|| 14.5 19.2
Education (years)11 or fewer 12.1 22.012 16.4 28.113 to 15 19.4 31.916 or more 23.0 40.4
Health insurance coverageYes 17.9 31.0No 13.0 14.4
ImmigrationBorn in US 18.1 30.9In US fewer than 10 years 3.3 14.3In US 10 years or more 12.7 23.8
Total 17.3 30.0
*A fecal occult blood test within the past year. †An endoscopy (testsinclude sigmoidoscopy, colonoscopy, or proctoscopy) within the past 5years. ‡Percentages are age-adjusted to the 2000 US standard popula-tion. See Statistical Notes on page 47 for more information. §Estimatesshould be interpreted with caution because of the small sample sizes.||Does not include Native Hawaiians and other Pacific Islanders.
Source: National Health Interview Survey Public Use Data File, 2000,National Center for Health Statistics, Centers for Disease Control andPrevention, 2002.
American Cancer Society, Surveillance Research

42 Cancer Prevention & Early Detection Facts & Figures 2005
Table 3F. Colorectal Cancer Screening, Adults 50 and Older, by State, 2002% Recent fecal occult blood stool test* % Recent sigmoidoscopy or colonoscopy†
No usual No usual50 years 65 years source of No 50 years 65 years source of No
and 50 to 64 and medical health and 50 to 64 and medical health older years older care‡ insurance§ older years older care‡ insurance§
Alabama 18.4 16.2 21.2 6.5 5.2 39.8 36.3 44.5 20.7 23.9Alaska 18.9 19.8 16.2 14.0 16.2 40.0 32.6 59.9 25.2 11.8Arizona 27.1 24.8 30.0 11.2 9.7 42.0 35.8 49.8 25.2 11.3Arkansas 15.9 12.4 20.1 7.3 11.1 32.6 26.7 39.8 19.7 9.8California 19.9 16.6 24.6 8.1 2.8 40.4 33.9 49.4 20.5 14.2
Colorado 25.7 23.7 29.2 11.8 9.6 37.9 33.1 45.8 13.1 9.2Connecticut 27.2 24.8 30.0 14.0 15.8 49.0 45.0 53.8 24.9 30.6Delaware 23.3 20.0 27.4 14.6 18.7 51.7 48.7 55.5 24.9 16.5Dist. of Columbia 29.1 24.8 34.6 24.1 || 53.8 47.6 62.1 27.6 ||
Florida 25.4 18.3 32.4 11.7 8.4 44.4 36.3 52.2 22.8 18.8
Georgia 21.1 20.0 22.9 11.6 7.5 40.8 36.2 48.2 21.7 19.3Hawaii 24.4 22.2 27.0 11.3 12.5 33.2 27.9 39.6 15.8 13.4Idaho 17.2 15.4 19.6 9.3 6.9 36.0 31.3 42.5 20.9 13.6Illinois 18.4 16.6 20.7 4.7 5.6 37.0 33.3 42.0 9.1 21.1Indiana 17.3 15.7 19.4 8.4 10.6 33.6 30.1 38.2 16.7 17.0
Iowa 24.7 22.5 27.1 6.4 7.1 39.2 32.0 47.0 18.5 12.5Kansas 24.5 19.3 30.6 10.3 15.4 38.5 33.1 44.8 17.6 19.4Kentucky 20.8 19.7 22.5 16.6 13.4 37.4 33.1 43.5 22.0 15.6Louisiana 19.8 16.7 24.2 13.1 12.8 34.0 28.6 41.5 24.0 20.2Maine 33.4 30.3 37.3 22.4 18.2 40.9 33.9 49.6 4.7 18.3
Maryland 30.1 25.3 37.1 14.9 22.5 46.7 41.6 54.1 22.0 17.0Massachusetts 29.1 27.0 31.5 8.0 18.3 46.7 41.1 53.1 17.0 25.0Michigan 23.9 21.8 26.8 12.6 11.7 44.7 38.8 52.8 20.5 28.0Minnesota 23.6 20.5 27.8 11.6 || 54.9 48.8 63.0 32.5 ||
Mississippi 17.5 15.6 20.0 8.7 4.2 34.5 28.1 43.0 17.1 9.7
Missouri 21.1 19.9 22.6 12.7 16.6 36.2 32.9 40.4 24.7 26.3Montana 18.7 17.8 19.8 9.0 9.1 38.7 31.2 48.5 21.0 16.1Nebraska 22.1 18.6 26.0 9.5 8.1 35.0 31.2 39.4 18.3 22.2Nevada 18.9 15.1 24.8 7.2 4.4 33.1 24.5 46.2 16.9 11.2New Hampshire 30.2 27.5 34.0 15.6 14.5 42.3 38.7 47.3 18.6 18.3
New Jersey 19.9 15.4 25.9 5.9 7.0 41.2 33.9 50.6 19.9 14.7New Mexico 16.8 14.8 19.8 6.1 6.2 35.0 29.4 43.0 15.2 14.1New York 21.0 18.8 23.7 8.6 9.0 44.6 39.5 50.9 21.1 24.7North Carolina 29.4 28.3 30.9 11.8 17.7 40.8 37.5 45.6 17.9 18.9North Dakota 16.2 12.5 20.2 9.0 5.3 39.9 29.6 51.3 20.6 15.7
Ohio 22.3 19.4 25.9 10.8 18.6 37.7 34.1 42.1 24.9 25.3Oklahoma 17.5 15.7 19.7 7.2 8.9 30.2 24.5 37.2 15.1 13.4Oregon 21.6 17.6 27.1 5.8 5.9 38.9 32.2 48.0 17.2 20.4Pennsylvania 20.0 16.2 24.1 9.6 11.5 39.0 33.6 44.8 15.7 14.7Rhode Island 28.1 25.1 31.2 12.4 16.4 47.8 42.1 54.0 25.4 18.7
South Carolina 20.4 16.1 26.5 7.3 10.0 40.6 33.2 51.1 25.5 27.0South Dakota 20.7 19.1 22.3 13.7 8.0 34.4 27.1 42.3 25.1 18.0Tennessee 23.6 20.3 28.2 16.7 9.7 39.6 35.5 45.3 18.4 18.6Texas 16.4 14.7 18.9 6.7 4.2 36.2 29.7 45.7 12.4 16.7Utah 12.2 10.6 14.4 7.3 5.0 39.9 34.2 47.6 18.1 29.3
Vermont 30.3 26.7 35.5 8.8 14.4 44.8 39.6 52.0 16.5 21.9Virginia 19.6 18.1 21.8 7.1 12.4 41.3 37.9 46.3 22.9 19.1Washington 26.1 25.0 27.5 7.0 6.4 43.0 37.6 51.1 19.9 12.0West Virginia 18.8 16.5 21.8 12.9 10.3 31.5 27.3 36.7 20.4 16.3Wisconsin 22.2 20.9 24.0 6.8 13.0 46.8 41.1 54.0 17.8 27.9Wyoming 12.5 10.6 15.4 6.8 2.8 30.1 24.0 39.2 15.6 12.3
United States¶ 21.8 18.9 25.4 9.4 9.0 40.5 35.0 47.7 19.5 18.5Range 12.2-33.4 10.6-30.3 14.4-37.3 4.7-24.1 2.8-22.5 30.1-54.9 24.0-48.8 36.7-63.0 4.7-32.5 9.2-30.6
*A fecal occult blood test within the last year. †A sigmoidoscopy or colonoscopy within the preceding 5 years. ‡Adults 50 and older who reported that they did not have apersonal doctor or health care provider. §Adults 50 to 64 who reported that they did not have any kind of health care coverage, including health insurance, prepaid plans such as HMOs, or government plans such as Medicare. ||Sample size is insufficient to provide a stable estimate. ¶See Statistical Notes on page 47 for definition. Note: The colorectal cancer screening prevalence estimates do not distinguish between examinations for screening or for diagnosis.
Source: Behavioral Risk Factor Surveillance System Public Use Data Tape 2002, National Center for Disease Prevention and Health Promotion, Centers for Disease Controland Prevention, 2003.
American Cancer Society, Surveillance Research

organization collaboration is to increase the use ofproven colorectal cancer screening tests among theentire population for whom screening is appropriate.
• The American Cancer Society collaborated with theAd Council to launch the Polyp Man colorectal cancerprevention and detection campaign in 2002. Thisnationwide media campaign used television, radio,print, and Internet public service announcements toincrease the general public’s awareness of colon cancerscreening. Since its inception, the Polyp Man cam-paign has received more than $85 million in donatedmedia. In 2003 alone, the campaign garnered close to$43 million in television, radio, print, Internet, andoutdoor placement. This dollar value is a 53% increaseover 2002. The campaign ranked in the top 10 of the 50active Ad Council campaigns in 2003 for overall mediaplacement. The Polyp Man campaign also launchednew ads in 2003 that emphasize reaching the AfricanAmerican community – a population at high risk forcolorectal cancer – with lifesaving prevention andearly detection messages.
• The American Cancer Society has also launched anaggressive outreach effort targeting physicians and
Cancer Prevention & Early Detection Facts & Figures 2005 43
other health care providers and geared to educatingthem about their important role in getting patientsscreened for colorectal cancer. This health care provideroutreach will include advertisements in medical jour-nals, a direct email campaign, physician office detailing(in select markets), and working with health plans toreach their contracted providers. A variety of tools havebeen developed and will be available from the Society toassist physicians in their efforts to increase screening intheir practices.
*The New York Health Plan Association, which serves 6 million New Yorkers, covers the full range of colorectal cancer screening tests, as part of a voluntary collaboration with the American Cancer Society.
Sources: Health Policy Tracking Service & Individual state bill tracking services.
Figure 3A. Colorectal Cancer Screening Coverage Legislation, by State, 2004
AL
AZAR
CA CO
CT
DE
FL
GA
ID
IL IN
IA
KS
KY
LA
ME
MD
MA
MI
MN
MS
MO
MT
NENV
NH
NJ
NM
NY*
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WIWY
DC
HI
AK
Screening law ensures coverage for the full range of tests.
Screening law requires insurers to cover some tests, but not the full range. or Statewide insurer agreements are in place to cover the full range of tests.
Screening law requires insurers to offer coverage, but does not ensure coverage. or There are no state requirements for coverage.
American Cancer Society National Government Relations Department Policy Research, Updated December 2004.

44 Cancer Prevention & Early Detection Facts & Figures 2005
Finally, in order to help more of the medically under-served community gain access to colorectal cancerscreening, the Society is working on legislation thatwould authorize a CDC pilot program for colorectalcancer community screening and treatment designed totarget medically underserved populations.
Prostate Cancer ScreeningAmong US men, cancer of the prostate is the most com-mon type of cancer (other than skin cancer) and thesecond leading cause of cancer death. At present, there isnot a consensus among national organizations regardingthe value of prostate cancer screening. Both theAmerican Cancer Society and the American UrologicalAssociation recommend that, pending the outcome ofprospective randomized trials on the value of prostatecancer screening, shared decision-making with one’sphysician about testing for early prostate cancer detec-tion is appropriate.183,197
The American Cancer Society recommends that aprostate-specific antigen (PSA) test and digital rectalexam (DRE) be offered annually to men 50 and older, andthat prior to testing, they should be informed about thebenefits and limitations of testing for early prostatecancer detection. Men at high risk, including men of
African descent and men with a first-degree relativediagnosed with prostate cancer at a young age, shouldbegin screening at age 45. They should also be informedabout the benefits and limitations of testing.
The 2000 National Health Interview Survey was the firstnational survey to include detailed PSA testing ques-tions, including whether the advantages and disadvan-tages of the test were discussed prior to testing. Theresults from this national survey showed that the preva-lence of PSA screening within the past year was 41% inmen aged 50 and older and that the least likely to havethis test were men who had no usual source of care orhealth insurance.184 Among screened men, 66.5% of menaged 74 and older and 67% of men aged 50 to 74 reportedhaving a discussion about the advantages and disadvan-tages of the test with their doctor before PSA testing.198
The same detailed questions on PSA testing are notavailable on the Behavioral Risk Factor SurveillanceSystem. Across states (Table 3G), the recent PSA testpercentages in 2002 for men aged 50 and older rangedfrom 37.4% in Hawaii to 63.9% in Rhode Island. Menaged 65 and older were significantly more likely to havereceived a PSA test within the past year than men aged50 to 64 in approximately three-quarters of the states.
The recent digital rectal exam (DRE) percent-ages in 2002 for men aged 50 and older rangedfrom 33.8% in Hawaii to 69.2% in RhodeIsland. Unlike the PSA percentages, there waslittle variability in these proportions by age.Only one-third of the states showed that menaged 65 and older had higher percentages of aDRE within the past year than men aged 50 to64. Across all states, men aged 50 and olderwho lack a usual source of care and uninsuredmen aged 50-64 were significantly less likely tohave had a recent PSA or DRE.
Barriers and Opportunities toImprove Cancer ScreeningHealth insurance coverage is an importantdeterminant of access to health care, and stud-ies document that people who lack health careinsurance have reduced access to preventivecare and are less likely to get timely cancerscreening examinations.199 For people aged 65and older, health insurance coverage is nearlyuniversal because of the Medicare program.200
However, during 1994-2001, among thoseyounger than 65, 16%-17% had no health

Cancer Prevention & Early Detection Facts & Figures 2005 45
Table 3G. Prostate Cancer Screening, Men 50 and Older, by State, 2002% Recent prostate-specific antigen test* % Recent digital rectal exam†
No usual No usual50 years 65 years source of No 50 years 65 years source of No
and 50 to 64 and medical health and 50 to 64 and medical health older years older care‡ insurance§ older years older care‡ insurance§
Alabama 57.3 53.7 63.6 || || 54.5 51.2 60.4 || ||
Alaska 50.6 49.7 53.6 39.2 || 53.4 52.2 57.6 42.3 27.4Arizona 58.6 52.9 66.9 24.3 || 55.0 52.5 58.7 28.0 ||
Arkansas 52.2 47.9 58.8 29.6 39.1 47.9 43.1 54.8 23.0 38.1California 53.4 46.9 66.0 27.6 || 52.1 48.2 59.4 19.8 ||
Colorado 53.7 50.4 61.2 22.7 || 53.1 51.1 57.8 24.6 ||
Connecticut 53.3 48.7 60.7 18.0 || 58.0 55.2 62.7 20.5 ||
Delaware 63.2 60.8 67.4 || || 60.4 58.7 63.1 || ||
Dist. of Columbia 57.6 52.7 66.1 || || 59.7 53.1 72.4 || ||
Florida 60.3 55.2 66.3 27.0 29.1 54.3 50.7 58.6 27.7 27.0
Georgia 54.8 51.3 62.1 25.7 22.1 50.8 46.5 59.5 26.0 17.5Hawaii 37.4 31.5 45.8 14.2 14.6 33.0 30.4 36.7 15.6 19.2Idaho 50.2 44.5 60.6 24.0 24.2 49.1 46.0 54.4 24.2 21.0Illinois 47.9 43.4 56.1 11.4 || 47.2 44.2 52.6 13.9 ||
Indiana 49.3 46.6 54.0 25.4 30.0 47.7 46.8 49.1 25.1 26.8
Iowa 56.9 51.4 64.6 || || 55.0 53.9 56.5 || ||
Kansas 59.1 53.4 68.3 35.7 || 54.0 51.3 58.3 26.2 ||
Kentucky 51.7 48.6 57.1 33.5 28.8 46.3 44.8 49.0 33.3 26.4Louisiana 57.7 54.2 64.0 37.8 37.0 52.1 49.9 55.9 36.5 39.8Maine 53.4 46.4 64.9 || || 63.0 59.9 68.1 || ||
Maryland 58.7 54.1 67.0 21.8 || 57.4 52.5 66.4 21.9 ||
Massachusetts 55.4 55.0 56.1 21.4 28.2 60.9 63.2 57.1 24.2 37.7Michigan 54.3 49.5 62.8 21.2 37.0 53.4 48.5 62.4 20.0 27.6Minnesota 53.4 45.5 67.0 26.5 || 58.0 52.9 66.6 33.3 ||
Mississippi 51.5 47.5 58.3 22.3 23.7 46.8 45.1 49.9 25.8 25.3
Missouri 58.2 56.6 60.9 37.9 39.2 56.8 56.6 57.0 34.7 44.1Montana 51.7 47.6 59.0 27.3 29.5 51.2 48.8 55.2 29.8 37.1Nebraska 50.9 49.6 52.8 29.1 || 42.4 40.0 45.9 19.9 ||
Nevada 55.0 50.1 63.7 26.8 19.9 43.2 35.9 55.9 22.9 18.9New Hampshire 56.9 53.6 63.0 35.5 33.3 63.7 61.3 68.2 27.8 32.4
New Jersey 52.5 48.0 60.5 22.4 56.6 51.1 47.4 57.7 21.1 47.5New Mexico 48.1 40.8 60.5 15.5 11.4 49.0 42.1 60.8 19.0 17.6New York 54.9 48.8 65.6 31.3 || 56.6 53.5 62.0 25.3 ||
North Carolina 53.3 49.1 61.4 25.4 39.4 53.5 51.0 58.2 23.0 38.9North Dakota 46.6 39.4 58.2 20.1 || 46.5 38.9 58.6 21.9 ||
Ohio 52.2 47.0 60.7 22.9 || 47.2 44.0 52.2 22.5 ||
Oklahoma 50.9 45.5 59.7 31.3 26.5 45.0 40.2 52.9 20.6 22.0Oregon 42.0 36.6 51.4 10.5 || 43.4 40.8 47.9 20.5 ||
Pennsylvania 54.8 48.4 64.0 27.5 34.3 51.1 46.4 58.0 26.8 30.4Rhode Island 63.9 61.8 66.9 26.7 || 68.6 64.5 74.6 27.6 ||
South Carolina 58.4 53.9 66.9 31.7 41.5 52.7 47.6 62.0 26.5 23.9South Dakota 54.5 50.5 60.4 24.5 26.4 48.6 45.5 53.1 22.3 21.0Tennessee 55.9 51.2 64.8 31.3 || 49.3 49.4 49.3 22.5 ||
Texas 50.2 46.2 57.8 20.8 16.9 46.9 43.1 54.1 15.7 16.3Utah 47.0 40.5 58.4 25.4 || 48.4 45.5 53.3 24.6 ||
Vermont 54.1 51.0 60.0 19.9 || 57.9 55.4 62.5 19.3 35.3Virginia 52.8 52.3 53.5 31.6 || 52.6 54.0 50.0 24.4 33.6Washington 45.6 43.3 49.8 18.6 12.2 49.5 49.7 49.2 19.0 9.1West Virginia 54.1 50.2 60.4 29.2 49.0 44.6 55.9 26.7 ||
Wisconsin 54.2 49.5 62.4 23.2 27.1 59.8 56.7 64.8 26.8 24.9Wyoming 61.3 54.7 73.6 38.3 22.8 42.9 35.5 56.9 21.8 13.6
United States¶ 53.7 49.0 61.8 25.5 28.2 52.0 48.9 57.2 23.1 26.4Range 37.4-63.9 31.5-61.8 45.8-73.6 10.5-39.2 11.4-56.6 33.0-68.6 30.4-64.5 36.7-74.6 13.9-42.3 9.1-47.5
*A prostate-specific antigen test within the last year for men 50 and older who reported they were not told by a doctor, nurse, or other health professional that they hadprostate cancer. †A digital rectal exam within the last year for men 50 and older who reported they were not told by a doctor, nurse, or other health professional that theyhad prostate cancer. ‡Men 50 and older who reported that they did not have a personal doctor or health care provider. §Men 50 to 64 who reported that they did not haveany kind of health care coverage, including health insurance, prepaid plans such as HMOs, or government plans such as Medicare. ||Sample size is insufficient to provide astable estimate. ¶See Statistical Notes on page 47 for definition.
Source: Behavioral Risk Factor Surveillance System Public Use Data Tape 2002, National Center for Disease Prevention and Health Promotion, Centers for Disease Controland Prevention, 2003.
American Cancer Society, Surveillance Research

46 Cancer Prevention & Early Detection Facts & Figures 2005
insurance coverage, 9%-11% had Medicaid coverage, and70%-73% had private insurance.116 The uninsured weremore likely to be at or below the poverty level, beHispanic/Latino or African American, and report feweryears of education.199 Changes in employment status canalso affect health care coverage.200 Despite recent effortsto expand coverage incrementally, the number of unin-sured Americans has continued to grow, reaching 45million in 2003, up 3.8 million from 2001. Millions moreface erosion of their coverage, higher deductibles, andperiods without insurance.201 According to a recentreport, higher-wage workers are more likely than theirlower-paid counterparts to have health insurance andhealth-related benefits, such as paid sick leave, and touse preventive care services. Low-wage workers, mean-while, are much more likely to forgo needed health carebecause of cost and are more likely to report problemspaying medical bills.202 Many studies consistently docu-ment that uninsured persons are more likely to delay orforgo preventive health care, including cancer screen-ing.7,203
Clinicians and the health care system play a major role inenabling patient participation in cancer screening andensuring quality services. Research on barriers related tocancer screening shows that multiple factors, such aspublic policy, organizational systems and practicesettings, clinicians, and patients, influence cancerscreening and that a diverse set of intervention strategiestargeted at each of these factors can improve cancerscreening rates.7,204 Studies also have shown that peoplewho received a clinician’s recommendation for cancerscreening are more likely to be screened than those whodid not receive a recommendation.7
To maximize the potential impact of interventions forimproving cancer screening, a diverse set of strategiesshould be implemented. These include centralized oroffice-based systems (including computer-basedreminder systems) to assist clinicians in counselingage/risk-eligible patients about screening, and organi-zational support systems to help manage referrals andfollow up of cancer screening tests.7,205 In addition,multiple interventions directed at patients (strategies toraise awareness about the importance of cancer screen-ing), physicians (strategies to assist them in their cancerscreening counseling and follow up), and health caresystems (strategies to ensure that high-quality andtimely cancer screening is delivered to beneficiaries in ahealth care plan) may provide the best approach toimproving rates of cancer screening.206,207 In addition,multi-partner efforts between the American CancerSociety and government agencies are underway toimplement interventions, integrate screening intoroutine care, and address health disparities. Visitwww.cdc.gov/nccdphp/aag/aag_reach.htm for moreinformation.
The American Cancer Society continues to monitor,analyze, and advocate for state and federal policy initia-tives to promote and increase cancer screenings amongthe uninsured. Delaware, for example, established a $1.5million annual allocation this year specifically for colo-rectal cancer screening for the uninsured. As more statesdevelop innovative models to provide screenings andtreatment for the uninsured, the American CancerSociety will play a larger role in advocating for and help-ing to replicate those programs.

Cancer Prevention & Early Detection Facts & Figures 2005 47
Statistical Notes
Sample SurveysIn measuring the prevalence of certain behaviors in apopulation, it is usually costly and unfeasible to surveyevery person. Hence, most population-based surveysare conducted by choosing a randomly selected sampleof people to estimate the true prevalence in a popula-tion. Such surveys are considered to have high externalvalidity, and, therefore, results are considered applicableto the entire population that the sample represents. Allof the adult and youth statistics presented in this publi-cation have been weighted and are estimates of the trueprevalence in the population. The population-based sur-vey methodology introduces sampling error to the esti-mated prevalence since a true prevalence is notcalculated. In addition, a standard error is associatedwith the estimated prevalence and can be used to calcu-late the confidence interval. (See Other StatisticalTerms, below.)
Prevalence: The percentage of people exhibiting thebehavior out of the total number in the defined popula-tion. For example, in 2002, 66.7% of Floridian womenaged 40 and older had a mammogram within the pastyear. The percentage of people exhibiting the behavior is66.7%, and the defined population is women aged 40 andolder living in Florida in 2002.
Population: A group of people defined by the survey. Forexample, the BRFSS data target adults 18 and older, andthe YRBSS data target students in grades 9 through 12 atpublic and private high schools.
Population-based surveys: A survey conducted to esti-mate the prevalence of a disease, risk factor, or othercharacteristic in an entire population in a city, state, ornation. For example, the BRFSS is designed to representall residents in a given state, and the YRBSS is designedto represent all high school students in the nation, astate, or a city.
Sample: A smaller group of people chosen from the pop-ulation defined by the survey. The sample is chosenbased on the age, race, ethnic, and gender demographicsof the city, state, or nation. At times, population-basedsurveys will oversample a particular age, race, ethnic, orgender group. This oversampling provides enoughresponses to make valid estimates for a particular popu-lation of interest.
Weighted data: Data that are representative of an entirecity, state, or nation. Once the sample of the population
has completed the survey, statistical analyses are con-ducted to extrapolate the surveyed group’s responses tothe entire population (city, state, or nation). For example,BRFSS data in this publication is representative of allnoninstitutionalized, civilian adults with telephones.The YRBSS data in this publication are representative ofall public and private high school students in grades 9through 12.
Standard error: A measure of variability around theestimated prevalence. A small value indicates a moreprecise prevalence estimate, whereas a larger value indi-cates a less precise prevalence estimate. The size of thismeasure is dependent upon the size of the sample.
Data quality: The sources of data used for this reportare from government-sponsored national and state sys-tems of behavioral surveillance. These systems employsystematic, standardized techniques for sampling anduse the latest advances in survey research methodologyto survey targeted population groups on an ongoingbasis, in order to monitor a variety of characteristics (e.g.,behaviors). The design and administration of thesesurveillance systems can provide sources of good-qualitydata from which to derive population estimates ofspecific behaviors in a targeted population. However,factors such as cost, feasibility, and practical aspects ofmonitoring behaviors in the population may play a rolein data quality. Therefore, the data reported in thisreport are subject to 3 limitations. First, with regard totelephone-based surveys such as the BRFSS, the partici-pants are those from households with a telephone.Second, both in-person and telephone surveys havevarying proportions of individuals who do not partici-pate for a variety of reasons (e.g., cannot be reached dur-ing the time of data collection or refused to participateonce reached). Third, survey measures in general arebased on self-reported data which may be subject torecall bias and cannot be easily validated.
Other Statistical TermsAge-adjusted prevalence: A statistical method used to adjust prevalence estimates to allow for valid com-parisons between populations with different agecompositions.
Confidence interval (CI): A range of possible values forthe estimated prevalence. A 90% confidence interval isone that will contain the true value in 90 out of 100samples surveyed. Similarly, a 95% confidence interval

48 Cancer Prevention & Early Detection Facts & Figures 2005
Behavioral Risk Factor Surveillance System (BRFSS).The BRFSS is a survey of the Centers for Disease Controland Prevention (CDC), National Center for ChronicDisease Prevention and Health Promotion (NCCDPHP),and the US states and territories. It is designed toprovide state prevalence estimates on behavioral riskfactors such as cigarette smoking, physical activity, andcancer screening. Data are gathered through monthly,
will contain the true value in 95out of 100 samples surveyed. A95% confidence interval iscommonly reported, and theaccompanying table reports theconfidence interval ranges forthe survey data.
Example: The confidence inter-val range for current cigarettesmoking among adults isbetween 1.0% and 2.8%. The nar-rowest confidence interval isaround the percentage forPennsylvania (24.6%±1.0%) or(23.6, 25.6), and the percentagefor Alaska has the widest rangeof possible values (29.4%±2.8%)or (26.6, 32.2).
Correlation: Correlation quan-tifies the extent to which twoindependent quantities (variableX and Y) “go together.” Whenhigh values of X are associatedwith high values of Y, a positivecorrelation is said to exist. When high values of X areassociated with low values of Y, a negative correlation issaid to exist. The strength of a correlation between 2variables, X and Y, is evaluated by using a statisticalmeasure called the correlation coefficient. The p-valuemeasures the likelihood that the observed associationoccurred by chance alone; p-values less than 0.05 areconsidered statistically significant (but unlikely that theassociation occurred by chance).
Range: The lowest and highest values of a group ofprevalence estimates.
US definition for state tables: The state-based BRFSSdata were aggregated to represent the US. Thus, themedian BRFSS values for all US states/territories pub-lished by the CDC will differ from these. Due to the dif-ferences in sampling methodology and survey methods,this percentage may not be the same as the percentagereported by the NHIS.
Confidence Interval (CI) Ranges for Percentages Listed in Tables, by StateTable Description 95% CI Range
1A Current cigarette smoking, high school students, total ± 1.8% to 6.2%
1B At risk for becoming overweight, high school students, total ± 0.7% to 2.4%Overweight, high school students, total ± 1.4% to 3.5%Moderate physical activity, high school students, total ± 1.6% to 3.9%Vigorous physical activity, high school students, total ± 1.9% to 4.9%Five or more fruits and vegetables a day, high school students, total ± 1.6% to 3.4%
2B Current cigarette smoking, adults 18 and older ± 0.7% to 2.5%Current cigarette smoking, men 18 and older ± 1.2% to 4.2%Current cigarette smoking, women 18 and older ± 0.9% to 3.0%
2C Clinical overweight, adults 18 and older ± 0.9% to 2.7%Clinical obese, adults 18 and older ± 0.8% to 2.4%No leisure-time physical activity, adults 18 and older ± 0.7% to 2.5%Moderate physical activity, adults 18 and older ± 0.9% to 2.9%Vigorous physical activity, adults 18 and older ± 0.9% to 2.8%Five or more fruits and vegetables a day, adults 18 and older ± 0.8% to 2.5%
3B Recent mammogram, women 40 and older ± 1.7% to 5.3%Recent mammogram, women 65 and older ± 2.7% to 11.2%
3D Recent Pap test, women 18 and older ± 1.3% to 3.4%Recent Pap test, women 65 and older ± 3.6% to 12.0%
3F Recent fecal occult blood test, adults 50 and older ± 1.3% to 4.6%Recent sigmoidoscopy or colonoscopy, adults 50 and older ± 1.6% to 5.1%
3G Recent prostate-specific antigen test, men 50 and older ± 2.7% to 7.6%Recent digital rectal examination, men 50 and older ± 2.7% to 7.3%
Survey Sources
The statistics reported in this publication are compiledfrom several different publicly available surveys designedto provide prevalence estimates of health-related behav-iors and practices for a city, state, or nation. The surveydesign varies; some surveys provide prevalence esti-mates on a national level, whereas some surveys provideestimates on a state level. A brief description of eachsurvey follows:

Cancer Prevention & Early Detection Facts & Figures 2005 49
computer-assisted telephone interviews with adultsaged 18 and older, living in households in a state or USterritory. The BRFSS is an annual survey, and all 50states, the District of Columbia, and Puerto Rico haveparticipated since 1996. The methods are generallycomparable from state to state and from year to year,which allows states to monitor the effects of interven-tions over time. Prevalence estimates from BRFSS aresubject to several limitations. For example, the preva-lence estimates are only applicable to adults living inhouseholds with a residential telephone line. Although95% of US households have telephones, the coverageranges from 87% to 98% in the states and varies by state.For more information, visit the BRFSS Web site atwww.cdc.gov/brfss.
National Health and Nutrition Examination Survey(NHANES). The NHANES is a survey of the Centers forDisease Control and Prevention (CDC), National Centerfor Health Statistics (NCHS). The survey is designed toprovide national prevalence estimates on the health andnutritional status of US adults and children, such asprevalence of major diseases, nutritional disorders, andpotential risk factors. Data are gathered through in-person interviews and direct physical exams in mobileexamination centers. Questions regarding diet andhealth are asked in the interview; the physical exam con-sists of medical and dental exams, physiological meas-urements, and laboratory tests. Three cycles of NHANESwere conducted between 1971 and 1994; the most recentand third cycle (NHANES III) was conducted from 1988to 1994. Beginning in 1999, NHANES was implementedas a continuous, annual survey. For more information,visit the NHANES Web site at www.cdc.gov/nchs/nhanes.htm.
National Health Interview Survey (NHIS). The NHISis a survey of the Centers for Disease Control andPrevention (CDC), National Center for Health Statistics(NCHS). The survey is designed to provide nationalprevalence estimates on personal, socioeconomic,demographic, and health characteristics, such as ciga-rette smoking and physical activity, of US adults. Dataare gathered through a computer-assisted personalinterview of adults aged 18 and older living in house-holds in the US. The NHIS is an annual survey and hasbeen conducted by NCHS since 1957. For more informa-tion, visit the NHIS Web site at www.cdc.gov/nchs/nhis.htm.
National Youth Tobacco Survey (NYTS). The NYTS isa survey of the Centers for Disease Control and Preven-tion (CDC) Foundation funded by the American LegacyFoundation. The survey is designed to provide nationaldata for public and private students in grades 6 through12. It allows for the design, implementation, and evalua-tion of a comprehensive tobacco control program withmore detailed tobacco-related questions than theYRBSS, including those on nontraditional tobaccoproducts such as bidis, secondhand smoke exposure,smoking cessation, and school curriculum. Data aregathered through a self-administered questionnairecompleted during a required subject or class period. TheNYTS was first conducted in fall 1999, again in spring2000, and will be conducted every other year.
Youth Risk Behavior Surveillance System (YRBSS).The YRBSS is a survey of the Centers for Disease Controland Prevention (CDC), National Center for ChronicDisease Prevention and Health Promotion (NCCDPHP).The survey is designed to provide national, state, andlocal prevalence estimates on health risk behaviors, suchas tobacco use, unhealthy dietary behaviors, physicalinactivity, and others, among youth and young adultswho attend public and private high schools. Differentstatistical methods are used to choose the representativesample for the national, state, and local prevalence esti-mates. (See Statistical Notes, page 47.) Data are gatheredthrough a self-administered questionnaire completedduring a required subject or class period. The YRBSS is abiennial survey that began in 1991. The state and localsurveys are of variable data quality, and caution shouldbe used in comparing data among them. Data fromstates and local areas with an overall response rate of60% and appropriate documentation are consideredweighted and are generalized to all public and privatehigh school students in grades 9 through 12 in therespective jurisdiction. However, data from states andlocal areas without an overall response rate of 60% andthose with inadequate documentation, are reportedunweighted and are only applicable to students partici-pating in the survey. Beginning with the 2003 survey,state data that does not meet the weighting require-ments described above will no longer be made publiclyavailable through the CDC. For more information, visitthe YRBSS Web site at www.cdc.gov/HealthyYouth/yrbs/index.htm.

50 Cancer Prevention & Early Detection Facts & Figures 2005
References1. American Cancer Society. Cancer Facts & Figures 2005. Atlanta(GA): American Cancer Society; 2005.
2. McGinnis JM, Foege WH. Actual causes of death in the UnitedStates. JAMA. 1993;270:2207-2212.
3. Mokdad AH, Marks JS, Stroup DF, Geloerding JL. Actual causes ofdeath in the US, 2000. JAMA. 2004; 291:1238-1245. Erratum: JAMA.2005; 293-294.
4. Eyre H, Kahn R, Robertson R, Committee AAACW. Preventingcancer, cardiovascular disease, and diabetes: a common agenda for theAmerican Cancer Society, the American Diabetes Association, andthe American Heart Association. CA Cancer J Clin. 2004;54(4):190-207.
5. US Department of Health and Human Services. Reducing TobaccoUse: A Report of the Surgeon General. Atlanta (GA): US Department ofHealth and Human Services, Centers for Disease Control andPrevention, National Center for Chronic Disease Prevention andHealth Promotion, Office on Smoking and Health; 2000.
6. US Department of Health and Human Services. The SurgeonGeneral’s Call to Action to Prevent and Decrease Overweight andObesity. Washington (DC): US Department of Health and HumanServices; 2001.
7. Curry SJ, Byers T, Hewitt M, eds. Fulfilling the Potential of CancerPrevention and Early Detection. Washington (DC): The NationalAcademies Press; 2003.
8. American Cancer Society. How Do You Measure Up? A ProgressReport on State Legislative Activity to Reduce Cancer Incidence andMortality. Atlanta (GA): American Cancer Society; 2004.
9. Centers for Disease Control and Prevention. Healthy Youth: AnInvestment in Our Nation’s Future 2003. Atlanta (GA): Centers forDisease Control and Prevention, National Center for Chronic DiseasePrevention and Health Promotion; 2003.
10. Serdula MK, Ivery D, Coates RJ, Freedman DS, Williamson DF,Byers T. Do obese children become obese adults? A review of the liter-ature. Prev Med. 1993;22:167-177.
11. Centers for Disease Control and Prevention. Guidelines for schooland community programs to promote lifelong physical activity amongyoung people. MMWR Morb Mortal Wkly Rep. 1997;46 (RR-6).
12. US Department of Health and Human Services. PreventingTobacco Use Among Young People: A Report of the Surgeon General.Atlanta (GA): US Department of Health and Human Services, Centersfor Disease Control and Prevention, National Center for ChronicDisease Prevention and Health Promotion, Office on Smoking andHealth; 1994.
13. US Department of Health and Human Services. Promoting BetterHealth for Young People Through Physical Activity and Sports.Washington (DC): US Department of Health and Human Services andUS Department of Education; 2000.
14. Centers for Disease Control and Prevention. Youth Risk BehaviorSurveillance – United States, 2003. MMWR Morb Mortal Wkly Rep.2004;53(SS-2).
15. Centers for Disease Control and Prevention. Cigarette use amonghigh school students – United States, 1991-2003. MMWR Morb MortalWkly Rep. 2004;53(23):499-502.
16. Federal Trade Commission. Federal Trade Commission CigaretteReport for 2001. Washington (DC): Federal Trade Commission; 2003.
17. Federal Trade Commission. Federal Trade Commission CigaretteReport for 2002. Washington, DC: Federal Trade Commission; 2004.
18. ImpacTeen. Higher Cigarette Prices Keep Kids from Starting toSmoke. ImpacTeen and YES! for Bridging the Gap: Research InformingPractice for Healthy Youth Behavior. Available at: http://www.uic.edu/orgs/impacteen/generalarea_PDFs/4-20%20IT-YES%20Releasepaper2.pdf. Accessed November 12, 2003.
19. Farrelly MC, Nimsch CT, James J. State Cigarette Excise Taxes:Implications for Revenue and Tax Evasion. Research Triangle Park(NC): RTI International, Health, Social, and Economics Research;2003.
20. Farrelly MC, Healton CG, Davis KC, Messeri P, Hersey JC, HavilandML. Getting to the truth: evaluating national tobacco countermarket-ing campaigns. Am J Public Health. 2002;92:901-907.
21. Centers for Disease Control and Prevention. Youth TobaccoSurveillance – United States, 2000. MMWR Morb Mortal Wkly Rep.2001;50 (SS-4).
22. Mowery P, Farrelly M, Haviland L, Gable J, Wells H. Progression toestablished smoking among US youths. Am J Public Health.2004;94(2):331-337.
23. Halpern-Felsher B, Biehl M, Kropp R, Rubinstein M. Perceivedrisks and benefits of smoking: differences among adolescents withdifferent smoking experiences and intentions. Prev Med. 2004;39:559-567.
24. DiFranza J, Savageau J, Fletcher K, et al. Measuring the loss ofautonomy over nicotine use in adolescents. Arch Pediatr Adolesc Med.2002;156:397-403.
25. O’Loughlin J, DiFranza J, Tyndale R, et al. Nicotine-dependencesymptoms are associated with smoking frequency in adolescents. AmJ Prev Med. 2003;25(3):219-225.
26. Biener L, Siegel M. Tobacco marketing and adolescent smoking:more support for a causal inference. Am J Public Health. 2000;90(3):407-411.
27. Centers for Disease Control and Prevention. School Health Policiesand Programs Study 2000, State Level Summaries, Health Education(Table 1.4). Centers for Disease Control and Prevention. Available at:http://www.cdc.gov/nccdphp/dash/shpps/summaries/health_ed/index.htm. Accessed October 13, 2003.
28. Centers for Disease Control and Prevention. Guidelines for schoolhealth programs to prevent tobacco use and addiction. MMWR MorbMortal Wkly Rep. 1994;43 (RR-2).
29. Siegel M, Biener L. The impact of an antismoking media campaignon progression to established smoking: results of a longitudinal study.Am J Public Health. 2000;90(3):380-386.
30. Siegel M. The effectiveness of state-level tobacco control interven-tions: a review of program implementation and behavioral outcomes.Ann Rev Public Health. 2002;23:45-71.
31. Hamilton W, Norton GD, Weintraub J. Independent Evaluation ofthe Massachusetts Tobacco Control Program. Cambridge (MA): AbtAssociates, Inc; 2003.
32. Campaign for Tobacco-Free Kids. Trends in state tobacco preven-tion spending versus tobacco revenues. National Center for Tobacco-Free Kids. December 18, 2003. Available at: http://www.tobaccofreekids.org/research/factsheets/index.php?CategoryID=7.Accessed August, 2004.
33. Centers for Disease Control and Prevention. Effect of ending anantitobacco youth campaign on adolescents’ susceptibility to ciga-rette smoking - Minnesota, 2002-2003. MMWR Morb Mortal Wkly Rep.2004;53(14):301-304.

Cancer Prevention & Early Detection Facts & Figures 2005 51
34. McDonald P, Colwell B, Backinger CL, Husten C, Maule CO. Betterpractices for youth tobacco cessation: evidence of review panel. Am JHealth Behav. 2003;27:S144-S158.
35. Centers for Disease Control and Prevention. Trends in cigarettesmoking among high school students – United States, 1991-2001.MMWR Morb Mortal Wkly Rep. 2002;51(19):409-412.
36. Garrison M, Christakis D, Ebel B, Wiehe S, Rivera F. Smoking ces-sation intervention in youth. Evidence based effectiveness not demon-strated. Am J Prev Med. 2003;25:363-367.
37. Killen J, Robinson T, Ammerman S, et al. Randomized clinical trialof the efficacy of bupropion combined with nicotine patch in thetreatment of adolescent smokers. J Consult Clin Psychol. 2004;72(4):729-735.
38. Sargent J, DiFranza J. Tobacco control for clinicians who treat ado-lescents. CA Cancer J Clin. 2003;53:102-123.
39. Backinger CL, McDonald P, Ossip-Klein DJ, et al. Improving thefuture of youth smoking cessation. Am J Health Behav. 2003;27:S170-S184.
40. Centers for Disease Control and Prevention. Tobacco use amongmiddle and high school students - United States, 2002. MMWR MorbMortal Wkly Rep. 2003;52(45):1096-1098.
41. Gilpin E, Pierce J. Concurrent use of tobacco products by Californiaadolescents. Prev Med. 2003;36:575-584.
42. Pateman B, Irvin L, Shoji L, Serna K. Building school health pro-grams through public health initiatives: the first three years of theHealthy Hawaii Initiative partnership for school health. Centers forDisease Control and Prevention. Available at: http://www.cdc.gov/pcd/issues/2004/jan/pateman.htm. Accessed January 20,2004.
43. Schroeder S. Tobacco control in the wake of the 1998 MasterSettlement Agreement. N Engl J Med. 2004;350(3):293-301.
44. American Academy of Pediatrics. Prevention of pediatric over-weight and obesity. Pediatr. 2003;112:424-430.
45. National Institutes of Health. Clinical Guidelines on theIdentification, Evaluation, and Treatment of Overweight and Obesity inAdults. Bethesda (MD): National Institutes of Health, National Heart,Lung, and Blood Institute; 1998.
46. Jeffreys M, Smith G, Martin R, Frankel S, Gunnell D. Childhoodbody mass index and later cancer risk: a 50-year follow-up of the BoydOrr Study. Int J Cancer. 2004;112:348-351.
47. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence andtrends in overweight among US children and adolescents, 1999-2000.JAMA. 2002;288:1728-1732.
48. Schmidt CW. Obesity: a weighty issue for children. Environ HealthPerspect. 2003;111:A700-A707.
49. Schwartz RP. Soft drinks taste good, but the calories count. JPediatr. 2003;142:599-601.
50. Koplan J, Liverman C, Kraak V. Preventing Childhood Obesity:Health in the Balance. Washington, D.C.: National Academy ofSciences, Institute of Medicine, Board on Health Promotion andDisease Prevention, Food and Nutrition Board, Committee onPrevention of Obesity in Children and Youth; 2004.
51. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. CDC growthcharts: United States (Advance Data no. 314). Hyattsville (MD):National Center for Health Statistics; 2000.
52. Dietz W, Gortmaker S. Do we fatten our children at the televisionset? Pediatr. 1985;75:807-812.
53. Strasburger VC. Children, adolescents, and television. Pediatr Rev.1992;13:144-151.
54. Lowry R, Wechsler H, Galuska DA, Fluton JE, Kann L. Televisionviewing and its associations with overweight, sedentary lifestyle, andinsufficient consumption of fruits and vegetables among US highschool students: differences by race, ethnicity, and gender. J SchHealth. 2002;72:413-421.
55. Andersen RE, Crespo CJ, Bartlett SJ, Cheskin LJ, Pratt M.Relationship of physical activity and television watching with bodyweight and level of fatness among children: results from the ThirdNational Health and Nutrition Examination Survey. JAMA.1998;279:938-942.
56. Boynton-Jarrett R, Thomas T, Peterson K, Wiecha J, AM S,Gortmaker S. Impact of television viewing patterns on fruit andvegetable consumption among adolescents. Pediatr. 2003;112(6):1321-1326.
57. Pate R, Baranowski T, Dowda M, Trost SG. Tracking of physicalactivity in young children. Epidemiology. 1996;28:92-96.
58. US Department of Health and Human Services. Physical Activityand Health: A Report of the Surgeon General. Atlanta (GA): USDepartment of Health and Human Services, Centers for DiseaseControl and Prevention, National Center for Chronic DiseasePrevention and Health Promotion; 1996.
59. Gordon-Larsen P, Nelson M, Popkin B. Longitudinal physical activ-ity and sedentary behavior trends: adolescence to adulthood. Am JPrev Med. 2004;27(4):277-283.
60. Kim S, Glynn N, Kriska A, et al. Decline in physical activity in blackgirls and white girls during adolescence. N Engl J Med. 2002;347:709-715.
61. Pate RR, Freedson PS, Sallis JF, et al. Compliance with physicalactivity guidelines: prevalence in a population of children and youth.Ann Epidemiol. 2002;12:303-308.
62. American Academy of Pediatrics. Organized sports for childrenand preadolescents. Pediatr. 2001;107:1459-1462.
63. Jackson RJ. The impact of the built environment on health: anemerging field. Am J Public Health. 2003;93:1382-1384.
64. Geller AL. Smart growth: a prescription for livable cities. Am JPublic Health. 2003;93:1410-1415.
65. Tompkins N, Zizzi S, Zedosky L, Wright J, Vitullo E. School-basedopportunities for physical activity in West Virginia public schools.Prev Med. 2004;39:834-840.
66. Evenson K, Huston S, McMillen B, Bors P, Ward D. Statewideprevalence and correlates of walking and bicycling to school. ArchPediatr Adolesc Med. 2003;157:887-892.
67. Centers for Disease Control and Prevention. Barriers to childrenwalking and biking to school. MMWR Morb Mortal Wkly Rep.2002;51:701-704.
68. Molnar B, Gortmaker S, Bull F, Buka S. Unsafe to play?Neighborhood disorder and lack of safety predict reduced physicalactivity among urban children and adolesceents. Am J HealthPromotion. 2004;18(5):378-386.
69. Handy S, Boarnet M, Ewing R, Killingsworth R. How the built envi-ronment affects physical activity: views from urban planning. Am JPrev Med. 2002;23 (suppl 2):64-73.
70. Jones S, Brener N, McManus T. Prevalence of school policies, pro-grams, and facilities that promote a healthy physical school environ-ment. Am J Public Health. 2003;93(9):1570-1575.
71. Sallis J, Conway T, Prochaska J, McKenzie T, Marshall S, Brown M.The association of school environments with youth physical activity.Am J Public Health. 2001;91(4):618-620.
72. Centers for Disease Control and Prevention. Participation in highschool physical education – United States, 1991-2003. MMWR MorbMortal Wkly Rep. 2004;53(36):844-847.

52 Cancer Prevention & Early Detection Facts & Figures 2005
73. Datar A, Sturm R. Physical education in elementary school andbody mass index: evidence from the early childhood longitudinalstudy. Am J Public Health. 2004;94(9):1501-1506.
74. Centers for Disease Control and Prevention. Physical activity levelsamong children aged 9-13 years – United States, 2002. MMWR MorbMortal Wkly Rep. 2003;52:785-788.
75. Centers for Disease Control and Prevention. KidsWalk-to-SchoolWeb site. Centers for Disease Control and Prevention, National Centerfor Chronic Disease Prevention and Health Promotion. Available at:http://www.cdc.gov/nccdphp/dnpa/kidswalk/index.htm. AccessedNovember 13, 2003.
76. Bayne-Smith M, Fardy P, Azzollini A, Magel J, Schmitz K, Agin D.Improvements in heart health behaviors and reduction in coronaryartery disease risk factors in urban teenage girls through a school-based intervention: the PATH program. Am J Public Health.2004;94(9):1538-1543.
77. Kranz S, Siega-Riz A, Herring A. Changes in diet quality ofAmerican preschoolers between 1977 and 1998. Am J Public Health.2004;94(9):1525-1530.
78. Lin B, Guthrie J, Frazao E. American children’s diets not makingthe grade. Food Review. 2001;24:8-17.
79. Cavadini C, Siega-Riz A, Popkin B. US adolescent food intaketrends from 1965 to 1996. Arch Dis Child. 2000;83:18-24.
80. Bull NL. Dietary habits, food consumption, and nutrient intakeduring adolescence. J Adolesc Health. 1992;13:384-388.
81. Bowman SA, Gortmaker SL, Ebbeling CB, Pereira MA, Ludwig DS.Effects of fast-food consumption on energy intake and diet qualityamong children in a national household survey. Pediatr. 2004;113:112-118.
82. Ebbeling C, Sinclair K, Pereira M, Garcia-Lago E, Feldman H,Ludwig D. Compensation for energy intake from fast food amongoverweight and lean adolescents. JAMA. 2004;291(23):2828-2833.
83. American Cancer Society 2001 Advisory Committee on Diet,Nutrition, and Cancer Prevention. Guidelines on diet, nutrition, andcancer prevention: reducing the risk of cancer with healthy foodchoices and physical activity. CA Cancer J Clin. 2001;52:92-119.
84. Brown K, Akintobi T, Pitt S, et al. California school board members’perceptions and factors influencing school nutrition policy. J SchoolHealth. 2004;74(2):52-58.
85. Cullen K, Zakeri I. Fruits, vegetables, milk, and sweetened bever-age consumption and access to a la carte/snack bar meals at school.Am J Public Health. 2004;94(3):463-467.
86. Kubik M, Lytle L, Hannan P, Perry C, Story M. The association ofthe school food environment with dietary behaviors of young adoles-cents. Am J Public Health. 2003;93(7):1168-1173.
87. American Academy of Pediatrics. Soft drinks in schools. Pediatr.2004;113:152-154.
88. Ludwig D, Peterson K, Gortmaker S. Relation between consump-tion of sugar-sweetened drinks and childhood obesity: a prospective,observational analysis. The Lancet. 2001;357:505-508.
89. Phillips S, Bandini L, Naumova E, et al. Energy-dense snack foodintake in adolescence: longitudinal relationship to weight and fatness.Obesity Research. 2004;12(3):461-472.
90. Troiano R, Briefel R, Carroll M, Bialostosky K. Energy and fatintakes of children and adolescents in the United States: data from theNational Health and Nutrition Examination Surveys. Am J Clin Nutr.2000;72:1343S-1353S.
91. James J, Thomas P, Cavan D, Kerr D. Preventing childhood obesityby reducing consumption of carbonated drinks: cluster randomizedcontrolled trial. BMJ. 2004.
92. United States General Accounting Office. Public Education:Commerical Activities in Schools. Washington, DC: United StatesGeneral Accounting Office, Health, Education, and Human ServicesDivision; 2000. GAO/HEHS-00-156.
93. French S, Story M, Neumark-Sztainer D, Fulkerson J, Hannan P.Fast food restaurant use among adolescents: associations with nutri-ent intake, food choices and behavioral and psychosocial variables. IntJ Obesity. 2001;25:1823-1833.
94. Giammattei J, Blix G, Marshak H, Wollitzer A, Pettitt D. Televisionwatching and soft drink consumption: associations with obesity in 11-to 13-year-old schoolchildren. Arch Pediatr Adolesc Med. 2003;157:882-886.
95. Kotz K, Story M. Food advertisements during children’s Saturdaymorning television programming: are they consistent with dietary rec-ommendations? J Am Diet Assoc. 1994;94(11):1296-1300.
96. Buzby J, Guthrie J, Kantor L. Evaluation of the USDA Fruit andVegetable Pilot Program: Report to Congress: Food Assistance andNutrition Research Program, Food and Rural Economics Division,Economic Research Service, US Department of Agriculture; 2003.
97. French S, Story M, Fulkerson J, Hannan P. An environmental inter-vention to promote lower-fat food choices in secondary schools: out-comes of the TACOS study. Am J Public Health. 2004;94(9):1507-1512.
98. Harvard Center for Cancer Prevention. Harvard report on cancerprevention volume 1: causes of human cancer. Cancer Causes Control.1996;7:S55.
99. Gallagher RP, McLean DI, Yang CP. Suntan, sunburn, pigmentationfactors and the frequency of acquired melanocytic nevi in children.Similarities to melanoma: the Vancouver mole study. Arch Dermatol.1990;126:770-776.
100. Weinstock MA, Colditz GA, Willett WC, Stampfer MJ.Nonfamilial cutaneous melanoma incidence in women associatedwith sun exposure before 20 years of age. Pediatrics. 1989;84:199-204.
101. Gallagher RP, Hill GB, Bajdik DR, Heenan PJ. Does intermittentsun exposure cause basal cell carcinoma? A case-control study inWestern Australia. Int J Cancer. 1995;131:157-163.
102. Centers for Disease Control and Prevention. Sun-protectionbehaviors used by adults for their children – United States, 1997.MMWR Morb Mortal Wkly Rep. 1998;47:480-482.
103. Buller DB, Borland R. Public education projects in skin cancerprevention: child care, school, and college-based. Clin Dermatol.1998;16:447-459.
104. Cokkinides VE, Davis KJ, Weinstock M, et al. Sun exposure andsun-protection behaviors and attitudes among US youth, 11 to 18years of age. Prev Med. 2001;33:141-151.
105. Centers for Disease Control and Prevention. Youth Risk BehaviorSurvey Results, United States, High School Survey Codebook. Centersfor Disease Control and Prevention, National Center for ChronicDisease Prevention and Health Promotion. Available at:http://www.cdc.gov/nccdphp/dash/yrbs/data/2001/yrbs2001.pdf.Accessed July 20, 2002.
106. Davis KJ, Cokkinides VE, Weinstock MA, O’Connell MC, WingoPA. Summer sunburn and sun exposure among youth ages 11 to 18:national prevalence and associated factors. Pediatr. 2002;110:27-35.
107. Weinstock MA. Don’t drop the Slop! PhotodermatolPhotoimmunol Photomed. 2001;17:238-239.
108. International Agency for Research on Cancer. IARC Handbooks ofCancer Prevention. Volume 5: Sunscreens. Lyon, France: IARC Press;2001.

Cancer Prevention & Early Detection Facts & Figures 2005 53
109. Centers for Disease Control and Prevention. Guidelines for schoolprograms to prevent skin cancers. MMWR Morb Mortal Wkly Rep.2002;51 (RR-4).
110. Centers for Disease Control and Prevention. Survey of knowledgeof and awareness about melanoma – United States. MMWR MorbMortal Wkly Rep. 1996;45:346-349.
111. Centers for Disease Control and Prevention. Annual smoking-attributable mortality and years of potential life lost, and economiccosts – United States, 1995-1999. MMWR Morb Mortal Wkly Rep.2002;51:300-303.
112. US Department of Health and Human Services. The HealthConsequences of Smoking: A Report from the Surgeon General.Washington, DC: US Department of Health and Human Services,Centers for Disease Control and Prevention, National Center forChronic Disease Prevention and Health Promotion, Office of Smokingand Health; 2004.
113. IARC Tobacco Smoke and Involuntary Smoking. IARCMonographs on the Evaluation of the Carcinogenic Risk of Chemicals toHumans. Lyon: International Agency for Research on Cancer.; 2004.
114. National Center for Health Statistics. Health, United States, 1998,with Socioeconomic Status and Health Chartbook. Hyattsville (MD):National Center for Health Statistics; 2001.
115. Centers for Disease Control and Prevention. Cigarette smokingamong adults – United States, 2002. MMWR Morb Mortal Wkly Rep.2004;53(20):427-431.
116. National Center for Health Statistics. Health, United States, 2003with Chartbook on Trends in the Health of Americans. Hyattsville(MD): National Center for Health Statistics, Centers for DiseaseControl and Prevention; 2003.
117. Centers for Disease Control and Prevention. Best Practices forComprehensive Tobacco Control Programs – August 1999. Atlanta(GA): US Department of Health and Human Services, Centers forDisease Control and Prevention, National Center for Chronic DiseasePrevention and Health Promotion, Office of Smoking and Health;1999.
118. Stillman F, Hartman A, Graubard B, Gilpin E, Murray D, Gibson J.Evaluation of the American Stop Smoking Intervention Study(ASSIST): A Report of Outcomes. J Natl Cancer Inst. 2003;95(22):1681-1691.
119. Jemal A, Cokkinides V, Shafey O, Thun M. Lung cancer trends inyoung adults: an early indicator of progress in tobacco control. CancerCauses Control. 2003;14(6):579-585.
120. Washington State Department of Health. Tobacco Preventionand Control Program: Progress Report. Executive Summary. Availableat: http://www.doh.wa.gov/Tobacco/program/reports.htm. AccessedJuly 29, 2004. Olympia, Washington: State Department of Health; 2003.
121. Fichtenberg C, Glantz S. Effect of smoke-free workplaces onsmoking behaviour: systematic review. British Medical Journal.2002;325:1-7.
122. Rohrbach L, Howard-Pitney B, Unger J, et al. Independent evalua-tion of the California tobacco control program: relationships betweenprogram exposure and outcomes, 1996-1998. Am J Pub Health Aff(Millwood). 2002;92(6):975-983.
123. California Department of Health Services. California TobaccoControl Update. Available at: http://www.dhs.ca.gov/ps/cdic/ccb/tcs/documents/CTCUpdate.pdf. Accessed July 29, 2004.Sacramento, CA: California Department of Health Services, TobaccoControl Section; 2000.
124. Centers for Disease Control and Prevention. Tobacco use amongadults – Arizona, 1996 and 1999. MMWR Morb Mortal Wkly Rep.2001;50(20):402-406.
125. Centers for Disease Control and Prevention. Declines in LungCancer Rates - California, 1988-1997. MMWR Morb Mortal Wkly Rep.2000;49(7):1066-1069.
126. Centers for Disease Control and Prevention. Decline in cigaretteconsumption following implementation of a comprehensive tobaccoprevention and education program – Oregon, 1996-1998. MMWRMorb Mortal Wkly Rep. 1999;48(7):140-141.
127. Barnoya J, Glantz S. Association of the California tobacco controlprograms with declines in lung cancer incidence. Cancer CausesControl. 2004;15:689-695.
128. California Department of Health Services. Toward a Tobacco FreeCalifornia, 2003-2005: The Myth of Victory. Sacramento, CA: CaliforniaDepartment of Health Services, Tobacco Control Section, theUniversity of California Tobacco Related Disease Research Program,and the Tobacco Education and Research Oversight Committee(TEROC); 2003.
129. American Nonsmokers’ Rights Foundation. How ManySmokefree Laws? American Nonsmokers’ Rights Foundation.Available at: http://www.no-smoke.org/mediaordlist.pdf. AccessedJanuary, 2005.
130. American Nonsmokers’ Rights Foundation. Summary of UnitedStates Population Protected by 100% Smokefree Laws. AmericanNonsmokers’ Rights Foundation. Available at: http://www.no-smoke.org/SummaryUSPopList.pdf. Accessed October 6, 2004.
131. Scollo M, Lal A, Hyland A, Glantz S. Review of the Quality ofStudies on the Economic Effects of Smoke-Free Policies on theHospitality Industry. Tobacco Control. 2003;12:13-20.
132. Goldstein A, Sobel R. Environmental Tobacco Smoke RegulationsHave Not Hurt Restaurant Sales in North Carolina. N C Med J.1998;59(5): 284-287.
133. Hyland A, Cummings K. Restaurant Employment Before andAfter the New York City Smoke-Free Air Act. J Public Health ManagePract. 1999;5(1):22-27.
134. Hyland A, Tuk J. Restaurant Employment Boom in New York City.Tobacco Control. 2001;10:199.
135. Hyland A, Cummings K, Nauenberg E. Analysis of Taxable SalesReceipts: Was New York City’s Smoke-Free Air Act Bad for RestaurantBusiness? J Public Health Manage Pract. 1999;5(1):14-21.
136. New York City Department of Finance, New York CityDepartment of Health and Mental Hygiene, New York CityDepartment of Small Business Services, New York City EconomicDevelopment Corporation. The State of Smoke-free New York City: AOne Year Review. New York City March 2004.
137. State of Delaware, Office of the Governor. Delaware’s SmokingRate Decreased by 11 Percent in 2003. Available at: www.state.de.us/governor/news/2004/07july/070204%20%20smoking%20study.shtml.Accessed October 6, 2004.
138. Repace J. Respirable particles and carcinogens in the air ofDelaware hospitality venues before and after a smoking ban. J OccupEnviron Med. 2004;46(9):887-905.
139. Glantz S, Charlesworth A. Tourism and Hotel Revenues Beforeand After Passage of Smoke-Free Restaurant Ordinances. JAMA.1999;281(20):1911-1918.
140. Sciacca J, Ratliff M. Prohibiting Smoking in Restaurants: Effectson Restaurant Sales. Am J Health Promotion. 1998;12(3):176-184.

54 Cancer Prevention & Early Detection Facts & Figures 2005
141. Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation tosmoking: 50 years’ observation of male British doctors. BMJ.2004;328:1519-1527.
142. Fiore MC. The tobacco use and dependence clinical practiceguideline panel, staff, and consortium representatives: a clinical prac-tice guideline for treating tobacco use and dependence. A US PublicHealth Service report. JAMA. 2000;293:3244-3254.
143. Fiore M, Croyle R, Curry S, Cutler C, Davis R, . Preventing 3 mil-lion premature deaths and helping 5 million smokers quit: a nationalaction plan for tobacco cessation. Am J Public Health. 2004;94(2):205-210.
144. Cokkinides V, Ward E, Jemal A, Thun M. Underuse of tobacco ces-sation treatments: Results from the 2000 National Health InterviewSurvey. Am J Prev Med (in press.). 2005.
145. Alesci N, Boyle R, Davidson G, Solberg L, S. M. Does a health planeffort to increase smokers’ awareness of cessation medication cover-age increase utilization and cessation? Am J Health Promotion.2004;18(5):366-369.
146. Solberg L, Quinn V, Stevens V, et al. Tobacco control efforts inmanaged care: what do the doctors think? Am J Managed Care.2004;10(3):193-198.
147. Burns M, Bosworth T, Fiore M. Insurance coverage of smokingcessation treatment for state health employees. Am J Public Health.2004;94(8):1338-1340.
148. Centers for Disease Control and Prevention. State MedicaidCoverage for Tobacco Dependence Treatments, US. MMWR MorbMortal Wkly Rep. 2004;53(3):54-57.
149. McAfee T, Sofian N, Wilson J, Hindmarsh M. The role of tobaccointervention in population-based health care. Am J Prev Med.1998;14:46-52.
150. Center for Tobacco Cessation. State Snapshot: Tobacco CessationStatus and Activity. Available at: http://www.ctcinfo.org/. AccessedOctober 5, 2004.
151. Campaign for Tobacco-Free Kids. State Tobacco Settlement:Special Reports. Washington (DC): National Center for Tobacco-FreeKids – Available at: http://www.tobaccofreekids.org/reports/settlements/. Accessed December 2, 2004.
152. American Medical Association. Tobacco Tax Challenge.Smokeless States National Tobacco Policy Initiative. Chicago (IL):American Medical Association; 2003.
153. American Cancer Society. unpublished information as of October2004. Washington (DC): American Cancer Society, NationalGovernment Relations Department; 2004.
154. National Cancer Institute. Tobacco Product Excise Taxes (Apr2003). Bethesda (MD): National Cancer Institute, State CancerLegislative Database Program; 2003.
155. Centers for Disease Control and Prevention. Tobacco ControlState Highlights 2004: Sustaining State Funding for Tobacco ControlPrograms. Atlanta (GA): US Department of Health and HumanServices, Centers for Disease Control and Prevention, National Centerfor Chronic Disease Prevention and Health Promotion, Office onSmoking and Health; 2004.
156. American Cancer Society. 2001 Advisory Committee on Diet,Nutrition, and Cancer Prevention – Guidelines on diet, nutrition, andcancer prevention: reducing the risk of cancer with healthy foodchoices and physical activity. CA Cancer J Clin. 2001;52:92-119.
157. International Agency for Research on Cancer. IARC Handbooks ofCancer Prevention. Volume 6: Weight Control and Physical Activity.Lyon, France: IARC Press; 2001.
158. International Agency for Research on Cancer. IARC Handbooks ofCancer Prevention. Volume 8: Fruits and Vegetables. Lyon, France:IARC Press; 2003.
159. Finkelstein E, Fiebelkorn I, Wang G. National medical spendingattributable to overweight and obesity: How much, and who’s paying?Health Affairs. 2003;3(1):219-226.
160. Hedley A, Odgen C, Johnson C, Carroll M, Curtin L, Flegal K.Prevalence of Overweight and Obesity Among US Children,Adolescents and Adults, 1999-2002. JAMA. 2004;291(23):2847-2850.
161. Mokdad A, Ford E, Bowman B, et al. Prevalence of Obesity,Diabetes, and Obesity-Related Health Risk Factors, 2001. JAMA.2003;289(1):76-79.
162. American Cancer Society. Special Section on Obesity in CancerFacts & Figures 2000. Atlanta (GA): American Cancer Society; 2000.
163. Calle E, Rodriguez C, Walker-Thurmond K, Thun M. Overweight,obesity, and mortality from cancer in a prospectively studied cohort ofUS adults. N Engl J Med. 2003;348:1625-1638.
164. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence andtrends in obesity among US adults, 1999-2000. JAMA. 2002;288:1723-1727.
165. NHLBI. National Heart, Lung, and Blood Institute, NationalInstitute of Health, Classification of Overweight and Obesity by BMI,Waist Circumference, and Associated Disease Risks. Available at:http://www.nhlbi.nih.gov/health/public/heart/obesity/lose_wt/bmi_dis.htm. Accessed October 20, 2004.
166. Koplan JP, Dietz WH. Caloric imbalance and public health policy.JAMA. 1999;282:1579-1581.
167. Hill JO, Wyatt HR, Reed GW, Peters JC. Obesity and the environ-ment: where do we go from here? Science. 2003;299:853-855.
168. Centers for Disease Control and Prevention. Prevalence of NoLeisure-Time Physical Activity – 35 States and the District ofColumbia, 1988-2002. MMWR Morb Mortal Wkly Rep. 2003;53(4):82-86.
169. King G, Fitzhugh E, Bassett D, et al. Relationship of leisure-timephysical activity and occupational activity to the prevalence of obe-sity. Int J Obes Related Metab Disord. 2001;25(5):606-612.
170. Centers for Disease Control and Prevention. Prevalence of physi-cal activity including lifestyle activities among adults, United States,2000-2001. MMWR Morb Mortal Wkly Rep. 2003;52:764-769.
171. Task Force on Community Preventive Services. Increasing physi-cal activity – a report on recommendations of the Task Force onCommunity Preventive Services. MMWR Morb Mortal Wkly Rep.2001;50 (RR-18).
172. Killingsworth RE, Lamming J. Development and Public Health.Urban Land. 2001;XX:12-17.
173. Frank L. Economic determinants of urban form: resulting trade-offs between active and sedentary forms of travel. Am J Prev Med.2004;27(3 Suppl):146-153.
174. National Institutes of Health and Centers for Disease Control andPrevention. The Strategic Plan for NIH Obesity Research – A Report ofthe NIH Obesity Task Force. Available at http://obesityresearch.nih.gov/About/strategic-plan.htm Accessed on July 15, 2004.Bethesda, Maryland: US Department of Health and Human Services,National Institutes of Health; 2004.

Cancer Prevention & Early Detection Facts & Figures 2005 55
175. Killingsworth RE. Health promoting community design: a newparadigm to promote healthy and active communities. Am J HealthPromotion. 2003;17:169-170.
176. National Cancer Institute. 5-A-Day for Better Health Program,.Division of Cancer Control and Population Sciences, National CancerInstitute. Available at: http://dccps.nci.nih.gov/5ad_2_evi.html; (foradditional information accessed www.5aday.com). Accessed October30, 2004.
177. National Cancer Institute. National 5 A Day Partnership. Divisionof Cancer Control and Population Sciences, National Cancer Institute.Available at: www.who.int/dietphysicalactivity/media/en/gs_fv_report.pdf. Accessed November 3, 2004.
178. Colorado Physical Activity and Nutrition Coalition. COPAN – TheColorado Physical Activity and Nutrition State Plan 2010. Available at: http://www.cdphe.state.co.us/pp/COPAN/COPAN_2010.pdf Accessed September 23 2004; http://www.cdphe.state.co.us/pp/COPAN/5ADAY.html. Accessed September 232004. Denver, CO: Colorado Department of Public Health andEnvironment; 2003.
179. Beresford SA, Shannon J, McLerran D, Thompson B. Seattle 5-a-day work-site project: process evaluation. Health Educ Behav.2000;27:213-222.
180. Will J, Farris R, Sanders C, Stockmyer C, Finkelstein E. Healthpromotion interventions for disadvantaged women: overview of theWISEWOMAN projects. J Womens Health. 2004;13(5):484-502.
181. Stoddard A, Palombo R, Troped P, Sorensen G, Will J.Cardiovascular Disease Risk Reduction: The Massachusetts WISE-WOMAN project. J Womens Health. 2004;13(5):539-546.
182. Resnicow K, Kramish CA, Carr C, et al. Body and Soul: a dietaryintervention conducted through African-American churches. Am JPrev Med. 2004;27(2):97-105.
183. Smith RA, Eschenbach A, Wender R, et al. American CancerSociety guidelines for the early detection of cancer: update of earlydetection guidelines for prostate, colorectal, and endometrial cancers.also: update 2001-testing for early lung cancer detection. CA Cancer JClin. 2001;51:38-75.
184. Swan J, Breen N, Coates RJ, Rimer BK, Lee NC. Progress in cancerscreening practices in the United States. Results from the 2000National Health Interview Survey. Cancer. 2003;97:1528-1540.
185. Centers for Disease Control and Prevention. State laws relating tobreast cancer: legislative summary January 1949-May 2000, Division ofCancer Control and Prevention. Available at: www.cdc.gov/cancer/nbccedp/bccpdfs/BCLaws.PDF.
186. Schiffman MH, Brinton LA, Devesa SS, Fraumeni J, Joseph F.Cervical Cancer. In: Schottenfeld D, Fraumeni J, Joseph F., eds. CancerEpidemiol Prev. New York (NY): Oxford University Press; 1996.
187. Centers for Disease Control and Prevention. The National Breastand Cervical Cancer Early Detection Program – Reducing MortalityThrough Screening – 2004/2005 Factsheet. National Center forChronic Disease Prevention and Health Promotion, Centers forDisease Control and Prevention. Available at: http://www.cdc.gov/cancer/nbccedp/nbcam.htm. Accessed September 30, 2004.
188. Fox S, Stein J, Sockloskie R, Ory M. Targeted mailed materials andthe Medicare beneficiary: increasing mammogram screening amongthe elderly. Am J Public Health. 2001;91(1):55-61.
189. Pignone M, Rich M, Teutsch S, Berg AO, Lohr KN. Screening forcolorectal cancer in adults at average risk: a summary of the evidencefor the US Preventive Services Task Force. Ann Internal Med.2002;137:132-141.
190. Chao A, Connell C, Cokkinides V, Jacobs E, Calle E, Thun M.Underuse of Screening Sigmoidoscopy and Colonoscopy in a LargeCohort of US Adults. Am J Public Health. 2004;94:1775-1781.
191. Cokkinides VE, Chao A, Smith RA, Vernon SW, Thun MJ.Correlates of underutilization of colorectal cancer screening amongUS adults, age 50 years and older. Prev Med. 2003;36:85-96.
192. Centers for Disease Control and Prevention. Colorectal cancertest use among persons aged >= 50 years – United States, 2001.MMWR Morb Mortal Wkly Rep. 2003;52:193-196.
193. Klabunde C, Frame P, Meadow A, Jones E, Nadel M, Vernon S. Anational survey of primary care physicians’ colorectal cancer screen-ing recommendations and practices. Prev Med. 2003;36(3):352-362.
194. Klabunde C, Riley G, Mandelson M, Frame P, Brown M. Healthplan policies and programs for colorectal cancer screening: a nationalprofile. Am J Managed Care. 2004;10(4):273-279.
195. The Lewin Group. Short-Term Cost-Impact Analysis of ColorectalCancer Screening: Commissioned by the American Cancer Society;March 13, 2003.
196. Centers for Disease Control and Prevention. Screen for Life:National Colorectal Cancer Action Campaign. National Center forChronic Disease Prevention and Health Promotion, Centers forDisease Control and Prevention. Available at: http://www.cdc.gov/cancer/screenforlife/spotlight.htm. Accessed September 30,2003.
197. American Urological Association. Prostate-specific antigen(PSA) best practice policy. American Urological Association (AUA).Oncology (Huntingt). 2000;14:267-272, 277-278, 280 passim.
198. Lu-Yao G, Stukel T, Yao S. Prostate-specific antigen screening inelderly men. J Natl Cancer Inst. 2003;95:1792-1796.
199. Institute of Medicine. Care without Coverage: Too Little, Too Late(report brief). Institute of Medicine, National Academy Press.Available at: http://books.nap.edu/html/care_without/reportbrief.pdf. Accessed September 17, 2002.
200. Schoenborn CA, Adams PF, Schiller JS. Summary HealthStatistics for the US Population: National Health Interview Survey,2000. Vital Health Stat. 2003;10 (214):1-83.
201. Kaiser Commission on Medicaid and the Uninsured. TheUninsured and their Access to Health Care ( fact sheet). Washington(DC): The Henry J. Kaiser Family Foundation; 2004.
202. Collins S, Davis K, Doty M, Ho A. Wages, Health Benefits, andWorkers’ Health. New York, NY: The Commonwealth Fund; 2004.
203. Ayanian J, Weissman J, Schneider E, Ginsburg J, Zaslavsky A.Unmet health needs of uninsured adults in the United States. JAMA.2000;284:2061-2069.
204. Meissner H, Smith R, Rimer B, et al. Promoting Cancer Screening:Learning from Experience. Cancer. 2004;101:1107-1117.
205. Rakowski W, Lipkus IM, Clark MA, et al. Reminder letter, tailoredstepped-care, and self-choice comparison for repeat mammography.Am J Prev Med. 2003;25:308-314.
206. Breen N, Wagener DK, Brown ML, Davis WW, Ballard-Barbash R.Progress in cancer screening over a decade: results of cancer screeningfrom the 1987, 1992, and 1998 National Health Interview Surveys. JNatl Cancer Inst. 2001;93:1704-1713.
207. Rimer BK, Conaway M, Lyna P, et al. The impact of tailored inter-ventions on a community health center population. Patient EducCouns. 1999;37:125-140.

56 Cancer Prevention & Early Detection Facts & Figures 2005
List of Tables and FiguresTables1A. Tobacco Use, High School Students, by State and City, 2003 41B. Overweight and Related Factors, High School Students, by State and City, 2003 92A. Current Cigarette Use, Adults 18 and Older, United States, 2002 182B. Tobacco Use, Adults 18 and Older, 2003, and Comprehensive Tobacco Control Measures,
by State, 2001, 2004, and 2005 192C. Overweight, Obesity, and Related Factors, Adults 18 and Older, by State, 2003 293A. Mammography, Women 40 and Older, US, 2000 353B. Mammography and Clinical Breast Exam, Women 40 and Older, by State, 2002 383C. Pap Test, Women 18 and Older, US, 2000 393D. Pap Test, Women 18 and Older, by State, 2002 403E. Colorectal Cancer Screening, Adults 50 and Older, US, 2000 413F. Colorectal Cancer Screening, Adults 50 and Older, by State, 2002 423G. Prostate Cancer Screening, Men 50 and Older, by State, 2002 45
Figures1A. Current Cigarette Smoking Among 12th Graders, by Race/Ethnicity, 1977-2003 31B. Current Cigarette Smoking Among High School Students, by Race/Ethnicity and Gender, 1991-2003 51C. Progression to Established Smoking of US Youth by Age, 1999-2000 61D. Overweight Children and Adolescents, by Age Group, 1971-2002 81E. Combined Youth Overweight Versus Three or More Hours of Television Watching, by State, 2003 101F. Policies for Required Sun Safety or Skin Cancer Prevention in Schools, by State, 2000 162A. Annual Number of Cancer Deaths Attributable to Smoking, Males and Females, by Site, US, 1995-1999 172B. Current Cigarette Smoking by Education, Adults 25 and Older, 1974-2002 182C. Smokefree Legislation at the State, County, and City Level 212D. Insurance Coverage of Smoking Cessation Treatments, State Employees, 2003, and
Medicaid Recipients, 2004 232E. Funding for Tobacco Prevention, by State, 2005 242F. Tobacco Excise Tax, by State, 2004 242G. Cancer Mortality by Body Mass Index for US Men and Women in the Cancer Prevention Study II,
1982-1998 272H. Adult Obesity, by Gender, Ages 20-74, 1960-2002 282I. Prevalence of Overweight Among US Adults by County, 1999-2002 303A. Colorectal Cancer Screening Coverage Legislation, by State, 2004 43

California Division, Inc.1710 Webster StreetOakland, CA 94612(510) 893-7900 (O)(510) 835-8656 (F)
Eastern Division, Inc.(LI, NJ, NYC, NYS, Queens,Westchester)6725 Lyons StreetEast Syracuse, NY 13057(315) 437-7025 (O)(315) 437-0540 (F)
Florida Division, Inc.(including Puerto Rico operations)3709 West Jetton AvenueTampa, FL 33629-5146(813) 253-0541 (O)(813) 254-5857 (F)
Puerto RicoCalle Alverio #577Esquina Sargento MedinaHato Rey, PR 00918(787) 764-2295 (O)(787) 764-0553 (F)
Great Lakes Division, Inc.(MI, IN)1755 Abbey RoadEast Lansing, MI 48823-1907(517) 332-2222 (O)(517) 664-1498 (F)
Great West Division, Inc.(AK, AZ, CO, ID, MT, ND, NM, NV, OR, UT, WA, WY)2120 First Avenue NorthSeattle, WA 98109-1140(206) 283-1152 (O)(206) 285-3469 (F)
Heartland Division, Inc.(KS, MO, NE, OK)1100 Pennsylvania AvenueKansas City, MO 64105(816) 842-7111 (O)(816) 842-8828 (F)
Illinois Division, Inc.225 N. Michigan AvenueSuite 1200Chicago, IL 60601(312) 641-6150 (O)(312) 641-3533 (F)
Mid-South Division, Inc.(AL, AR, KY, LA, MS, TN)1100 Ireland WaySuite 300Birmingham, AL 35205-7014(205) 930-8860 (O)(205) 930-8877 (F)
Midwest Division, Inc.(IA, MN, SD, WI)8364 Hickman RoadSuite DDes Moines, IA 50325(515) 253-0147 (O)(515) 253-0806 (F)
Chartered Divisions of the American Cancer Society, Inc.
New England Division, Inc.(CT, ME, MA, NH, RI, VT)30 Speen StreetFramingham, MA 01701-9376(508) 270-4600 (O)(508) 270-4699 (F)
Ohio Division, Inc.5555 Frantz RoadDublin, OH 43017(614) 889-9565 (O)(614) 889-6578 (F)
Pennsylvania Division, Inc.(PA, Phil)Route 422 and Sipe AvenueHershey, PA 17033-0897(717) 533-6144 (O)(717) 534-1075 (F)
South Atlantic Division, Inc.(DC, DE, GA, MD, NC, SC, VA, WV)2200 Lake BoulevardAtlanta, GA 30319(404) 816-7800 (O)(404) 816-9443 (F)
Texas Division, Inc.(including Hawaii Pacific operations)2433 Ridgepoint DriveAustin, TX 78754(512) 919-1800 (O)(512) 919-1844 (F)
Hawaii Pacific, Inc. 2370 Nuuanu AvenueHonolulu, HI 96817(808) 595-7500 (O)(808) 595-7502 (F)
AcknowledgmentsThe production of this report would not have been possible without the efforts of: Kim Andrews; Rachel Ballard-Barbash, MD; Michelle Boone; Durado Brooks, MD, MPH; Jeanne Calle, PhD; Jessica Corsi; Rebecca Cowens-Alvarado,MPH; Sherryn Craig; Mary Doroshenk; Colleen Doyle, MS, RD; Thomas J Glynn, PhD; Yongping Hao, PhD; MaggieHopkins; Corinne Husten, MD, MPH; Wendi Klevan; Marji McCullough, ScD, RD; Heidi Michels-Blank, PhD, DebbieSaslow, PhD; Christy Schmidt; Susan Summers; Robert Smith, PhD; Michael J. Thun, MD, MS; Janet Weaver; Jerome WYates, MD, MPH; Harriet Zoller.
Cancer Prevention & Early Detection Facts & Figures is an annual publication of the American Cancer Society, Atlanta,Georgia.

©2005, American Cancer Society, Inc.No. 8600.05
1.800.ACS.2345www.cancer.org
Hope.Progress.Answers.®
The American Cancer Society is the nationwide community-based voluntary health organization dedicated to eliminating cancer as a major health problem by preventing cancer, saving lives, and diminishing suffering from cancer, through research, education, advocacy, and service.
No matter who you are, we can help. Contact us anytime, day or night, forinformation and support.