Neonatal oral tumors: congenital epulis and epignathus
3
Neonatal oral tumors: congenital epulis and epignathus Basant Kumar ⁎ , Shyam B. Sharma Department of Pediatric Surgery, Sir Padampat Mother and Child Health Institute (Jaykaylon Hospital), SMS Medical College, Jaipur 302004, Rajasthan, India Received 25 February 2008; revised 21 March 2008; accepted 25 March 2008 Key words: Congenital epulis; Oropharyngeal teratoma; Epignathus Abstract Oroparyngeal tumors in neonates protruding from the mouth are extremely rare. They have the potential to cause respiratory distress, or even death of the child during the perinatal period owing to airway obstruction and may need a multidisciplinary team approach at the time of birth. Congenital epulis and epignathus are the 2 rare lesions usually presenting like this and clinical manifestations depend on their position and size. They have an excellent prognosis, if treated properly. This paper will discuss our experience with these 2 lesions and review the literature. © 2008 Elsevier Inc. All rights reserved. Congenital oral tumors protruding from the mouth of the newborn are rare [1]. These lesions have the potential to cause the death of the child from asphyxia during the perinatal and postnatal period due to respiratory obstruction and may need urgent surgical intervention [1,2]. Congenital epulis or granular cell tumor and epignathus or orophar- yngeal teratoma are the 2 rare lesions presenting like this and very few centers have experience with both these lesions [1] (Figs. 1 and 2). Large lesions can be diagnosed antenatally and one needs to plan a unique strategy for peripartum management [2]. This article aimed to report and discuss our experience with the management of both these lesions and review the literature. 1. Case 1 A 30-hours-old, full-term, vaginally delivered, female neonate weighing 2.5 kg was presented with a mass in her oral cavity with recurrent respiratory distress and inability to feed since birth. On examination, a pedunculated, smooth, fleshy, skin covered mass of about 11 × 4 cm in size was present in oral cavity arising from the nasopharyx in the region of basisphenoid (Rathke's pouch). The palate was normal. The mass was mobile and filling almost the whole oral cavity causing intermittent respiratory distress. The mass was pulled out by a stay suture to eliminate distress and a computed tomography scan of the head and neck was done. Computed tomography scan showed bony attachment of the mass but no intracranial extension or bony defect. Measure- ment of serum alpha-fetoprotein (AFP) was not done preoperatively. After a nasotracheal intubation, the mass was simply excised from the base by the use of cautery. After hemostasis, raw area was left as such. The postoperative period was uneventful. Histopathology of the resected specimen showed well-differentiated mature teratoma con- taining skin, fat, bony tissues, cartilages, and various tissues ⁎ Corresponding author. Resident Doctors' Hostel, JLN Marg, SMS Medical College, Jaipur, Rajasthan 302004, India. Tel.: +91 9929796737 (mobile). E-mail addresses: [email protected], [email protected] (B. Kumar). www.elsevier.com/locate/jpedsurg 0022-3468/$ – see front matter © 2008 Elsevier Inc. All rights reserved. doi:10.1016/j.jpedsurg.2008.03.055 Journal of Pediatric Surgery (2008) 43, E9–E11
-
Upload
basant-kumar -
Category
Documents
-
view
214 -
download
1
Transcript of Neonatal oral tumors: congenital epulis and epignathus

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2008) 43, E9–E11
Neonatal oral tumors: congenital epulis and epignathusBasant Kumar ⁎, Shyam B. Sharma
Department of Pediatric Surgery, Sir Padampat Mother and Child Health Institute (Jaykaylon Hospital),SMS Medical College, Jaipur 302004, Rajasthan, India
Received 25 February 2008; revised 21 March 2008; accepted 25 March 2008
M(m
(B
0d
Key words:Congenital epulis;Oropharyngeal teratoma;Epignathus
Abstract Oroparyngeal tumors in neonates protruding from the mouth are extremely rare. They have thepotential to cause respiratory distress, or even death of the child during the perinatal period owing toairway obstruction and may need a multidisciplinary team approach at the time of birth. Congenitalepulis and epignathus are the 2 rare lesions usually presenting like this and clinical manifestationsdepend on their position and size. They have an excellent prognosis, if treated properly. This paper willdiscuss our experience with these 2 lesions and review the literature.© 2008 Elsevier Inc. All rights reserved.
Congenital oral tumors protruding from the mouth of thenewborn are rare [1]. These lesions have the potential tocause the death of the child from asphyxia during theperinatal and postnatal period due to respiratory obstructionand may need urgent surgical intervention [1,2]. Congenitalepulis or granular cell tumor and epignathus or orophar-yngeal teratoma are the 2 rare lesions presenting like this andvery few centers have experience with both these lesions [1](Figs. 1 and 2). Large lesions can be diagnosed antenatallyand one needs to plan a unique strategy for peripartummanagement [2]. This article aimed to report and discuss ourexperience with the management of both these lesions andreview the literature.
⁎ Corresponding author. Resident Doctors' Hostel, JLN Marg, SMSedical College, Jaipur, Rajasthan 302004, India. Tel.: +91 9929796737obile).E-mail addresses: [email protected], [email protected]
. Kumar).
022-3468/$ – see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2008.03.055
1. Case 1
A 30-hours-old, full-term, vaginally delivered, femaleneonate weighing 2.5 kg was presented with a mass in heroral cavity with recurrent respiratory distress and inability tofeed since birth. On examination, a pedunculated, smooth,fleshy, skin covered mass of about 11 × 4 cm in size waspresent in oral cavity arising from the nasopharyx in theregion of basisphenoid (Rathke's pouch). The palate wasnormal. The mass was mobile and filling almost the wholeoral cavity causing intermittent respiratory distress. The masswas pulled out by a stay suture to eliminate distress and acomputed tomography scan of the head and neck was done.Computed tomography scan showed bony attachment of themass but no intracranial extension or bony defect. Measure-ment of serum alpha-fetoprotein (AFP) was not donepreoperatively. After a nasotracheal intubation, the masswas simply excised from the base by the use of cautery. Afterhemostasis, raw area was left as such. The postoperativeperiod was uneventful. Histopathology of the resectedspecimen showed well-differentiated mature teratoma con-taining skin, fat, bony tissues, cartilages, and various tissues

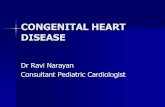
Fig. 1 Epignathus protruding from the mouth, pedunculated, andmobile causing recurrent airway obstruction since birth.
E10 B. Kumar, S.B. Sharma
resembling tissues of the alimentary tract and brain. Thechild was doing well without recurrence in our follow-upperiod of 1 year.
2. Case 2
A 2-day-old, full-term, vaginally delivered male neonateweighing 2.75 kg was admitted with complaints of a mass inthe oral cavity with feeding difficulties. There was norespiratory distress but the child had problems sucking. Onexamination, a firm, smooth, nontender mass measuring 4 ×3 cm was present arising from the left upper alveolar marginwith a broad base. The palate was normal. Near total excisionof the mass was done by the use of cautery after nasotrachealintubation. The postoperative period was uneventful.Histopathology of the resected specimen showed mucosawith underlying sheets of large granular cells with centrallyplaced round nuclei, consistent with a congenital epulis.After 1.5 years, the child was doing well without recurrenceand without any problem in dentition.
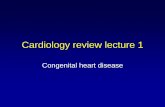
ig. 2 Congenital epulis presenting as oral mass with difficultysucking.
3. Discussion
Congenital epulis and epignathus or oropharyngealteratoma are both extremely rare intraoral tumors of thenewborn and are much more common in females [1,3,4]. Theetiology is unknown and there is still controversy regardingthe exact cell of origin in cases of epulis, but epignathi arethought to arise from pleuripotential cells in the region of
Rathke's pouch that grow in a disorganized manner andcontain well-differentiated cell lines derived from all 3 germcell layers [1,4]. Congenital oral tumors are commonlyrecognized at birth or just after birth except in instanceswhere the tumor is very small and causing no obvioussymptoms. The clinical manifestations depend on the sizeand location of the lesions and include dyspnea, suffocation,cyanosis, cough, difficulty in sucking and swallowing, and,occasionally, vomiting [4]. With advancement in imaging,oropharyngeal lesions may be diagnosed before birth. Inmany of these cases especially with epignathus, the neonatesdied owing to respiratory distress secondary to airwayobstruction at the time of birth. A multidisciplinary teamapproach is needed during birth in a tertiary level center tomaximize the chances of a good outcome for the child [2].
Oropharyngeal teratoma or epignathus constitutes lessthan 2% cases of congenital teratoma and successful excisionof only 8 cases of true epignathi has been reported (excludinghairy polyps or dermoids) [2,4,5]. Ewing (1940) classifiedoropharyngeal teratoma into dermoids, teratomata andteratoids, and epignathi [cited in 6]. Dermoids or hairypolyps are the most common and tend to affect adults. Morethan 100 cases of hairy polyps have been reported in theliterature, whereas true epignathi are very rare [4]. Giantepignathi are highly organized teratomas containing recog-nizable organs and are regarded as parasitic fetuses [4,6].Approximately 60% of epignathi originate in the nasophar-ynx, predominantly in females and frequently associatedwith cleft palate which may be severe [4,6]. Intracranialextension may occur, but only 1 case with intracranialteratoma associated with true epignathus has been reported[4]. Approximately 6% of patients with epignathus haveassociated anomalies, including other facial abnormalities,branchial cleft cysts, and congenital heart disease [2].
The treatment of both these tumors depends on the extentand site of origin. Preoperative tissue diagnosis between
Fin

E11Neonatal oral tumors: congenital epulis and epignathus
these 2 entities is not necessary as surgical excision is thetreatment of choice in both [1]. A plain radiograph to checkthe calcification of mass and a CT scan are recommended forevaluation of any bony defect or intracranial extension ofmass [6]. Emergency surgery should not be contemplated inpatients with stabilized airway, and radical disfiguringsurgery, which would result in impairment of speech anddeglutition, is contraindicated in the neonates [2,6]. If thechild is in respiratory distress, and the airway cannot besecured by endotracheal intubation, then an emergenttracheostomy should be done. An elective procedureremoving as much as possible of the tumor may be plannedlater. Heroic emergency surgery of the tumor should not becontemplated as profuse hemorrhage may be lethal [6].Surgical excision at the tumor base through oral approach ispreferred after excluding intracranial extension and ence-phalocele [4]. Elevated levels of serum AFP have also beenreported in epignathi [5].
Epulis is also known as congenital gingival granular celltumor of newborn or Neumann's tumor [3]. It can bemultiple and may occur in the mandible, maxilla, or tongue,but usually arises from the anterior part of the maxillaryalveolar ridge and may or may not be associated with othercongenital anomalies [3,7]. Epulis is seen only in thenewborn and is thought to be a different entity from othergranular cell tumors [3]. Radical excision is not needed.Local recurrences, malocclusion of the jaws, and damage tofuture dentition have not been reported [3].
In both of our cases, lesions are relatively small and havefewer symptoms. Our patient with the epignathus presented
with respiratory distress but was managed easily as the masswas freely mobile and had a narrow base. Althoughmalignancy has not been reported in epignathus, malignanttransformation of residual elements is reported and monitor-ing of serum AFP is recommended [5,6]. We did not performserum AFP level preoperatively. Serum AFP level was lessthan 2 ng/mL after 10 months and there was no evidence oflocal recurrence. Congenital epulis has a marked femalepreponderance of 8:1 [3], but our patient was male. Theprognoses of both these lesions are excellent and a carefulpre- and postoperative management is necessary for anuneventful recovery.
References
[1] Chattopadhyay A, Patra R, Kumar V. Oral tumors in newborn. Indian JPediatr 2003;70(7):587-8.
[2] Levine AB, Alvarez M, Wedgwood J, et al. Contemporary managementof a potentially lethal fetal anomaly: a successful perinatal approach toepignathus. Obstet Gynecol 1990;76:962-6.
[3] Lapid O, Shaco-Levy R, Krieger Y, Kachko L, Sagi A. Congenitalepulis. Pediatrics 2001;107(2):E-22.
[4] Maeda K, Yamamoto T, Yoshimura H, et al. Epignathus: a report of twoneonatal cases. J Pediatr Surg 1989;24(4):395-7.
[5] Antonio G, Oliveira F, Carvalho MH, et al. Epignathus: report of a casewith successful outcome. J Pediatr Surg 1988;33(3):520-1.
[6] Valente A, Grant C, Orr JD, et al. Neonatal tonsillar teratoma. J PediatrSurg 1988;23(4):364-6.
[7] Tandon P, Malik R, Tandon R. Congenital epulis of the newborn: acase report with review of literature. Indian J Pathol Microbiol 2007;50(3):593-4.