My Global Medical Brigades Experience
33
REFLECTION A BY: OLIVIA NIEPSUJ MY GLOBAL BRIGADES EXPERIENCE IN GHANA
Transcript of My Global Medical Brigades Experience

R E F L E C T I O N A
B Y : O L I V I A N I E P S U J
MY GLOBAL BRIGADES EXPERIENCE IN GHANA


How did I serve Techiman?
Medical Care
During four clinic days, we provided medical care to over nine hundred community members—people who
truly needed it. We did this through triage, filling prescriptions, and providing free physician access.

Ph
arm
acy
After patients were seen by a doctor, we filled prescriptions—most frequently for
pain killers and anti-malarials.

How did I serve Techiman?
Education
We educated community members on the importance of clean water, malaria prevention, good hygiene,
healthy eating, and exercise.
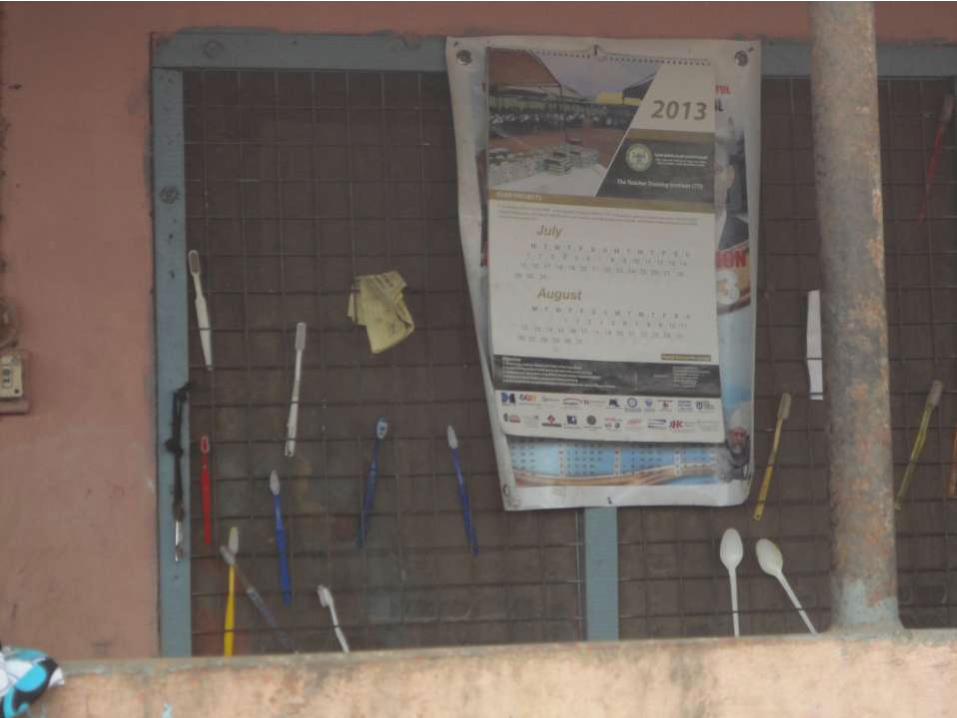

In addition to talking with community members about brushing
teeth, wearing shoes, and bathing regularly, we also provided them with toothbrushes and toothpaste so they could begin some of the good habits
we were encouraging.
Hy
gien
e

The nutrient most eaten in the community is starch. While, as the community members mentioned
during “Public Health”, the nutrient is filling, it is also lacks many
vitamins and minerals. We educated community members on the health
problems such a diet causes and encouraged them to eat “colorful
fruits and vegetables”.
Nu
trition

We stood up and stretched with the community members, teaching them a few exercises to help alleviate pains
associated with farming.
Many were prescribed short-term pain killers, but teaching stretches was a more long-term solution to their back, neck, and hip pains.
Ex
ercise

How did I serve Techiman?
Building Community
Through Global Brigades, we were able to build community and create relationships that aided in the
success of the brigade and, ultimately, the health of the people.

How did I serve Techiman?
Connection
The door-to-doors really allowed me to connect with the community members, making me feel like “their
ills are my ills”—a reason for service illustrated by Adam Davis in What We Don’t Talk About When We
Don’t Talk About Service. Through talking and listening about their lives, we were able to not only
create an environment where providing good healthcare was possible, but where building
friendships and community came easily.

What issues were observed in Techiman?
Water
The first problem with water in Techiman is that people are not getting enough of it. There is no local
source of water—community members have to walk to the next town over to pay for filling up their large
gallon containers that they then carry back to their village.
Secondly, the water is not clean. Without the use of Aqua tabs and boiling, their water is discolored and contains many parasites and bacteria that have the
potential to cause serious disease.

What issues were observed in Techiman?
Poor Healthcare
The people of Techiman had virtually no access to a health clinic, let alone a free health clinic. Additionally,
chronic conditions such as diabetes or hypertension are rarely treated properly because of high cost of
treatment/medication and poor access to a pharmacy.

What issues were observed in Techiman?
Malaria
The primary cause of sickness in Techiman? Malaria. We were able to provide anti-malarials; however, the disease inevitably returns unless precautions such as sleeping under mosquito nets and avoiding standing
water are taken.
Even so, if someone does get Malaria, due to inability to get to an affordable health clinic make the disease
life-threatening.

What issues were observed in Techiman?
Education
Most children only finish school through what we would consider a middle school level. Much of the
problem stems from there being no higher-education facility in the community and the need for children to
work to help support the family.

What issues were observed in Techiman?
Misconceptions About Healthcare
Most community members had no clue of the poor nutritional value of dishes such as Foofoo, thinking that starches, since they are filling, are nutritious
enough—even teasing us at door-to-doors for eating so many “green things”.
Many women do not have access to educational materials about menstruation and pregnancy. One
pregnant woman came to the gynecologist asking how to stop having children—illustrating the need for better
access to educational materials.

What issues were observed in Techiman?
Money
Although we encouraged community members to eat a variety of fruits and vegetables and brush their teeth, money is an enormous barrier. If people can barely
afford clean water, shoes, and healthcare, it is unlikely that they will splurge on toothpaste and more
expensive vegetables.
Many of my experiences in Ghana left me truly surprised, but I was perhaps most taken aback by the first day of door-to-door when one of the community members
asked me and my fellow brigaders if we were “commanded to volunteer”. At the time we all answered “no”. After reading What We Don’t Talk About When We
Don’t Talk About Service by Adam Davis, I was forced to reconsider my answer to the question. In his essay, Davis states “It has become so clear that Service Is
Good (SIG) that we can demand service activity” (Davis). In this experience, no one directly commanded that I go; however, volunteer work has almost become
demanded by many institutions. My intent for going to Ghana was to help people who were not as fortunate as I—to bridge, even a little bit, the inequality gap. However, I would be lying if I said I didn’t also go to prepare my resume for
medical schools—where volunteering is almost a requirement.
My overall experience in Ghana was life changing largely do to the fact that it reinforced my passion for not only the healthcare field, but also the inequality in
healthcare—another concept that Davis mentions in his essay. I went on the brigade knowing that I would see a tremendous discrepancy between our access to
healthcare versus the access the community members have. After all, we have doctors on almost every city block, whereas the clinic nearest Techiman is a few miles walking. I thought that by going on this brigade, I would be helping close
that gap, if even just a little. As the week went by, I felt like my goals were getting further and further away. Yes, we were treating children of malaria and parasites. Yes, we were giving overworked people analgesics for their pain. But how long are
the effects of our brigade going to resonate? A few days while the medication lasts? Until the next brigade comes in a few months?
After this brigade, I feel angry. My anger at the unequal distribution of medical care narrowed in then from this global inequality to unequal access in Chicago.
Recently, hospitals near the south side of Chicago—increasingly called “Chiraque”—have been closing down trauma centers due to the large influx of
uninsured gunshot victims—of which many are children. As a result, ambulances are forced to drive several miles to the north side of Chicago where the closest
hospitals authorized to take these victims are located—Rush or Northwestern. The chances of survival, as a result, are at best slim. I cannot possibly put into words my frustration at the medical system for not providing health care for those who
need it most. Davis emphasizes “We cherish inequality […] schools, jobs, cars, clothes, teeth, bellies, eyes. Look anywhere at all and you’ll see signs, indisputable signs, of inequality”(Davis). Yes, of course inequality exists. However, healthcare
ought be the exception. Regardless of social status, wealth, race, gender, age, access to healthcare is a human right, not a privilege. My experiences in Ghana
have further solidified this belief.