Molecular Microbiological Profile of Chronic …United States) associated with otitis media and its...
9
Molecular Microbiological Profile of Chronic Suppurative Otitis Media Michel Neeff, a Kristi Biswas, a Michael Hoggard, b Michael W. Taylor, b Richard Douglas a School of Medicine, The University of Auckland, Auckland, New Zealand a ; School of Biological Sciences, The University of Auckland, Auckland, New Zealand b Chronic suppurative otitis media (CSOM) presents with purulent otorrhea (ear discharge), is characterized by chronic inflam- mation of the middle ear and mastoid cavity, and contributes to a significant disease burden worldwide. Current antibiotic ther- apy is guided by swab culture results. In the absence of detailed molecular microbiology studies of CSOM patients, our current understanding of the microbiota of CSOM (and indeed of the healthy ear) remains incomplete. In this prospective study, 24 pa- tients with CSOM were recruited, along with 22 healthy controls. Culture-based techniques and 16S rRNA gene amplicon se- quencing were used to profile the bacterial community for each patient. Comparisons between patients with and without cho- lesteatoma in the middle ear and mastoid cavity were also made. A major finding was that the middle ear of many healthy controls was not sterile, which is contradictory to the results of previous studies. However, sequencing data showed that Staphy- lococcus aureus, along with a range of other Gram-positive and Gram-negative organisms, were present in all subgroups of CSOM and healthy controls. Large interpatient variability in the microbiota was observed within each subgroup of CSOM and controls, and there was no bacterial community “signature” which was characteristic of either health or disease. Comparisons of the culture results with the molecular data show that culture-based techniques underestimate the diversity of bacteria found within the ear. This study reports the first detailed examination of bacterial profiles of the ear in healthy controls and patients with CSOM. C hronic suppurative otitis media (CSOM) is one of the most common childhood diseases worldwide (1). It carries a signif- icant disease burden, estimated at 2 million disability-adjusted life years (2, 3). CSOM is characterized by chronic ear discharge through a perforated tympanic membrane for more than 6 weeks to 3 months (2, 4, 5). Its prevalence is related to poor socioeco- nomic conditions, and it is relatively uncommon in developed countries. Estimates suggest that between 65 and 300 million cases occur worldwide, with 60% of these cases suffering significant hearing impairment (3, 6, 7). Globally, 28,000 deaths per year due to complications of CSOM have been reported (2). There is an enormous financial burden (around $5 billion per annum in the United States) associated with otitis media and its sequelae, in- cluding chronic suppurative otitis media (8, 9). CSOM often begins as an acute infection of the middle ear, acute otitis media (AOM), which occurs in up to 80% of children by the age of 3 (8, 10). While most cases resolve spontaneously, a small minority of patients progress to a chronic phase character- ized by chronic purulent ear discharge through a perforated tym- panic membrane with associated inflammation of the mastoid and middle ear mucosa and hearing loss. CSOM can occur with or without cholesteatoma (epithelial inclusion cyst), but the pres- ence of cholesteatoma does not necessarily alter the clinical symp- toms. Intracranial complications such as brain abscess and men- ingitis contribute to the morbidity and occasional mortality of this condition (2, 3). The pathogenesis of CSOM remains poorly understood. Com- plex interactions between the environment, microbes, and host are thought to lead to the development of this multifactorial dis- ease (3, 10, 11). Topical and oral antibiotics are prescribed to patients based on bacterial culture results when available, but the clinical benefit of antibiotic therapy is not always clear (3). Surgery may prevent local, regional, or systemic complications, but some patients may continue to have ear discharge postoperatively (12). Research into the putative microbial causes of CSOM has so far been reliant on culture-based techniques. In these studies, Staph- ylococcus aureus and Pseudomonas aeruginosa were the most com- monly isolated bacteria, with methicillin-resistant S. aureus (MRSA) isolated in some cases (10, 13–21). However, there are treatment failures even when these specific organisms are tar- geted. It has previously been assumed that a healthy individual’s ear is sterile (22, 23). Infections in the middle ear are thought to occur when pathogens enter the middle ear through the external ear canal or Eustachian tube. Other theories to explain the persistent nature of this disease and repeated infection include toxin produc- tion by P. aeruginosa (24), microbes embedding within the dead/ damaged tissue (cholesteatoma) (16, 18), formation of biofilms (25, 26), recurrent bacterial infection from the nasopharynx not covered by the antibiotics prescribed (21), or development of an- tibiotic resistance (20, 27). Fluorescence in situ hybridization (FISH) has previously shown S. aureus biofilms to be present within the tissue of CSOM patients (28). Biofilm has also been demonstrated on the middle ear mucosa of children with chronic otitis media (23) and in middle ear effusions from children with recurrent AOM (29, 30), which is a likely risk factor for CSOM. Received 17 May 2016 Returned for modification 7 June 2016 Accepted 26 July 2016 Accepted manuscript posted online 3 August 2016 Citation Neeff M, Biswas K, Hoggard M, Taylor MW, Douglas R. 2016. Molecular microbiological profile of chronic suppurative otitis media. J Clin Microbiol 54:2538 –2546. doi:10.1128/JCM.01068-16. Editor: E. Munson, Wheaton Franciscan Laboratory Address correspondence to Richard Douglas, [email protected]. Supplemental material for this article may be found at http://dx.doi.org/10.1128 /JCM.01068-16. Copyright © 2016, American Society for Microbiology. All Rights Reserved. crossmark 2538 jcm.asm.org October 2016 Volume 54 Number 10 Journal of Clinical Microbiology on October 16, 2020 by guest http://jcm.asm.org/ Downloaded from
Transcript of Molecular Microbiological Profile of Chronic …United States) associated with otitis media and its...

Molecular Microbiological Profile of Chronic Suppurative Otitis Media
Michel Neeff,a Kristi Biswas,a Michael Hoggard,b Michael W. Taylor,b Richard Douglasa
School of Medicine, The University of Auckland, Auckland, New Zealanda; School of Biological Sciences, The University of Auckland, Auckland, New Zealandb
Chronic suppurative otitis media (CSOM) presents with purulent otorrhea (ear discharge), is characterized by chronic inflam-mation of the middle ear and mastoid cavity, and contributes to a significant disease burden worldwide. Current antibiotic ther-apy is guided by swab culture results. In the absence of detailed molecular microbiology studies of CSOM patients, our currentunderstanding of the microbiota of CSOM (and indeed of the healthy ear) remains incomplete. In this prospective study, 24 pa-tients with CSOM were recruited, along with 22 healthy controls. Culture-based techniques and 16S rRNA gene amplicon se-quencing were used to profile the bacterial community for each patient. Comparisons between patients with and without cho-lesteatoma in the middle ear and mastoid cavity were also made. A major finding was that the middle ear of many healthycontrols was not sterile, which is contradictory to the results of previous studies. However, sequencing data showed that Staphy-lococcus aureus, along with a range of other Gram-positive and Gram-negative organisms, were present in all subgroups ofCSOM and healthy controls. Large interpatient variability in the microbiota was observed within each subgroup of CSOM andcontrols, and there was no bacterial community “signature” which was characteristic of either health or disease. Comparisons ofthe culture results with the molecular data show that culture-based techniques underestimate the diversity of bacteria foundwithin the ear. This study reports the first detailed examination of bacterial profiles of the ear in healthy controls and patientswith CSOM.
Chronic suppurative otitis media (CSOM) is one of the mostcommon childhood diseases worldwide (1). It carries a signif-
icant disease burden, estimated at 2 million disability-adjusted lifeyears (2, 3). CSOM is characterized by chronic ear dischargethrough a perforated tympanic membrane for more than 6 weeksto 3 months (2, 4, 5). Its prevalence is related to poor socioeco-nomic conditions, and it is relatively uncommon in developedcountries. Estimates suggest that between 65 and 300 million casesoccur worldwide, with 60% of these cases suffering significanthearing impairment (3, 6, 7). Globally, 28,000 deaths per year dueto complications of CSOM have been reported (2). There is anenormous financial burden (around $5 billion per annum in theUnited States) associated with otitis media and its sequelae, in-cluding chronic suppurative otitis media (8, 9).
CSOM often begins as an acute infection of the middle ear,acute otitis media (AOM), which occurs in up to 80% of childrenby the age of 3 (8, 10). While most cases resolve spontaneously, asmall minority of patients progress to a chronic phase character-ized by chronic purulent ear discharge through a perforated tym-panic membrane with associated inflammation of the mastoidand middle ear mucosa and hearing loss. CSOM can occur with orwithout cholesteatoma (epithelial inclusion cyst), but the pres-ence of cholesteatoma does not necessarily alter the clinical symp-toms. Intracranial complications such as brain abscess and men-ingitis contribute to the morbidity and occasional mortality of thiscondition (2, 3).
The pathogenesis of CSOM remains poorly understood. Com-plex interactions between the environment, microbes, and hostare thought to lead to the development of this multifactorial dis-ease (3, 10, 11). Topical and oral antibiotics are prescribed topatients based on bacterial culture results when available, but theclinical benefit of antibiotic therapy is not always clear (3). Surgerymay prevent local, regional, or systemic complications, but somepatients may continue to have ear discharge postoperatively (12).Research into the putative microbial causes of CSOM has so far
been reliant on culture-based techniques. In these studies, Staph-ylococcus aureus and Pseudomonas aeruginosa were the most com-monly isolated bacteria, with methicillin-resistant S. aureus(MRSA) isolated in some cases (10, 13–21). However, there aretreatment failures even when these specific organisms are tar-geted.
It has previously been assumed that a healthy individual’s ear issterile (22, 23). Infections in the middle ear are thought to occurwhen pathogens enter the middle ear through the external earcanal or Eustachian tube. Other theories to explain the persistentnature of this disease and repeated infection include toxin produc-tion by P. aeruginosa (24), microbes embedding within the dead/damaged tissue (cholesteatoma) (16, 18), formation of biofilms(25, 26), recurrent bacterial infection from the nasopharynx notcovered by the antibiotics prescribed (21), or development of an-tibiotic resistance (20, 27). Fluorescence in situ hybridization(FISH) has previously shown S. aureus biofilms to be presentwithin the tissue of CSOM patients (28). Biofilm has also beendemonstrated on the middle ear mucosa of children with chronicotitis media (23) and in middle ear effusions from children withrecurrent AOM (29, 30), which is a likely risk factor for CSOM.
Received 17 May 2016 Returned for modification 7 June 2016Accepted 26 July 2016
Accepted manuscript posted online 3 August 2016
Citation Neeff M, Biswas K, Hoggard M, Taylor MW, Douglas R. 2016. Molecularmicrobiological profile of chronic suppurative otitis media. J Clin Microbiol54:2538 –2546. doi:10.1128/JCM.01068-16.
Editor: E. Munson, Wheaton Franciscan Laboratory
Address correspondence to Richard Douglas, [email protected].
Supplemental material for this article may be found at http://dx.doi.org/10.1128/JCM.01068-16.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
crossmark
2538 jcm.asm.org October 2016 Volume 54 Number 10Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

These evade the host immune response and antibiotic therapy bygrowing in a protective biofilm matrix.
The aim of this study was to characterize the bacterial commu-nities within the middle ears and mastoids of patients with andwithout CSOM. Bacterial community profiles obtained using cul-ture and molecular-based techniques were compared, with thelatter in particular providing novel insights into the microbiota ofCSOM patients. While previous studies have described the micro-biota of otitis media with effusion (31, 32), there is limited infor-mation on the microbiota associated with CSOM (33).
MATERIALS AND METHODSPatient information. This was a prospective study of 24 patients under-going mastoid surgery for CSOM and 22 patients with healthy middle earsundergoing either cochlear implantation (CI) or benign brain tumor (ves-tibular schwannoma) (T) removal via the mastoid and middle ear. Noneof the study patients received antibiotics within the 2 months precedingsurgery, but all patients (subjects and controls) received intravenous ce-fazolin on induction as part of the institutional perioperative protocol.The CSOM patients were subdivided based on the presence or absence ofcholesteatoma. Patients undergoing surgery for CSOM were also catego-rized according to the extent of surgery (canal wall up [CWU] or canalwall down [CWD] procedure). Patients with cholesteatoma were gradedby disease severity (34), but there is no such disease severity scale currentlyavailable for CSOM without cholesteatoma. Patients with anatomicaltemporal bone abnormalities or immune deficiencies were excluded.
The study was approved by the New Zealand Health and DisabilityEthics Committee (NTX/12/03/024).
Mastoid surgery was performed under general anesthesia and sterileconditions. The ear canal was left intact in more limited disease (CWU)but taken down and the mastoid air cell system externalized (canal walldown,) in more extensive disease. Assessment of disease severity wasbased on clinical and imaging findings that were evaluated by an oto-laryngologist (M.N.). Intraoperatively, tissue samples and two sterile ray-on-tipped swab (Copan 170KS01) samples were taken from the mastoidand middle ear. Collected swab samples were placed immediately on iceand then frozen (�20°C) within 2 h of surgery.
Conventional microbiology swab samples were also collected duringsurgery and sent to a hospital laboratory for bacterial culture analysis.Swab samples were inoculated on the following culture media (Fort Rich-ard Laboratories Ltd., New Zealand): Columbia sheep blood, supple-mented chocolate with bacitracin, MacConkey, colistin-nalidixic acid,and Sabouraud dextrose agars. The former two were incubated at 37°C inambient air supplemented with 5% CO2, while the latter three were incu-bated at 37°C in ambient air. Swab samples collected from patients withchronic infections were also plated on brain heart infusion medium andincubated anaerobically. Significant bacterial species were identified usingthe Vitek MS system (bioMérieux) and antibiotic sensitivity testing wasperformed on the Vitek 2 system (bioMérieux) or by using disc diffusioncriteria as appropriate and interpreted using the Clinical and LaboratoryStandards Institute guidelines (35). Samples that led to cultivation of asingle colony or more were considered to be positive.
DNA extraction. Swab samples were thawed on ice and placed into asterile Lysing Matrix E tube (MP Biomedicals, Australia). Genomic DNAwas extracted from the paired swabs using the AllPrep DNA/RNA isola-tion kit (Qiagen), as described previously (36). A negative extraction con-trol to test for contamination originating from the DNA isolation kit wascarried out in triplicate using 200 �l of sterile water. In no case did theseextraction controls yield measurable DNA, and subsequent PCRs includ-ing this DNA were invariably negative.
16S rRNA gene sequencing and bioinformatics. A nested PCR ap-proach was used to amplify the bacterial 16S rRNA genes from genomicDNA due to difficulties in obtaining PCR products from most samplesafter 35 cycles of amplification. Primers 616V (37) and 1492R (38) wereused to amplify nearly the full length (targeting Escherichia coli positions 8
to 1513) of the bacterial 16S rRNA gene, as described previously (39).After 12 initial PCR cycles, 1 �l from the first PCR was used as the templatefor the second PCR amplification. In this second reaction, the V3 to V4region of the bacterial 16S rRNA gene was amplified (35 cycles) usingprimers 341F and 806R (read length of 465 bp) (40). The PCR mixtureincluded the following: genomic DNA template (�100 ng), equimolarconcentrations (0.2 �M) of each primer, deoxynucleoside triphosphates(dNTPs) (0.2 mM), HotStar PCR buffer (1�), MgCl2 (2 mM), 0.5 UHotStar DNA polymerase (Qiagen), and PCR-grade water to a final vol-ume of 25 �l. PCRs were conducted under the following conditions:95°C for 15 min, followed by 35 cycles of 95°C for 30 s, 55°C for 30 s, and70°C for 40 s, with a final step of 3 min at 70°C. Duplicate PCRs wereconducted for each sample. Negative and positive controls were runfor all PCRs. In addition, 1 �l of the initial PCR negative control wasused as a template in the second PCR to ensure that the final PCRproducts obtained were not due to contamination. Study samples thatproduced no amplification product after the nested PCR amplification(47 cycles in total) were considered to be negative. Amplicons werepurified using Agencourt AMPure beads (Beckman Coulter Inc.) andthen subjected to both quality (Agilent Bioanalyzer DNA high-sensi-tivity [HS] assays) and quantity (Qubit double-stranded DNA(dsDNA) HS assay kit) checks.
Sequencing on an Illumina MiSeq (2 � 300 bp, paired-end reads) wasperformed at a commercial sequencing provider (Macrogen, South Ko-rea). Raw sequences were analyzed using a combination of the UPARSEand QIIME software packages (41, 42). In brief, raw sequences weremerged, trimmed, and quality checked using UPARSE. Unique sequenceswere clustered in UPARSE into operational taxonomic units (OTUs) at athreshold of 97% 16S rRNA gene sequence similarity. Chimera checkswere performed by checking the sequences against a chimera database(SILVA gold chimera reference database). Taxonomic assignment of thesequences was subsequently performed in QIIME using RDP Classifier 2.2and the SILVA 16S rRNA gene database (version 119) as the reference(43). Sequences were aligned using PyNAST (44), and a phylogenetic treewas generated via FastTree 2.1.3 (45). Samples were rarefied to an evensequencing depth of 1,168 sequences per sample. Alpha and beta diversityanalyses (including UniFrac [46]) were conducted in QIIME.
Statistical analysis. The software programs Prism 6 and PRIMER6were used to statistically analyze the data sets. Permutational analysis ofvariance (PERMANOVA) was performed in PRIMER6 (version 6.1.13)using Jaccard, Bray-Curtis, and weighted and unweighted UniFrac dis-tances. Multidimensional scaling plots were constructed from theweighted UniFrac distance matrix in PRIMER6. Kruskal-Wallis tests wereperformed with Dunn’s multiple comparison corrections to measure sig-nificant differences (P � 0.05) between variables.
Accession number. Raw sequences were uploaded to the NCBI Se-quence Read Archive, and the accession numbers can be found via Bio-Project record number PRJNA320336.
RESULTSClinical characteristics of the cohort. A total of 24 patients withCSOM were recruited, along with 22 healthy controls. Most pa-tients with cholesteatoma had extensive middle ear and mastoiddisease (grades 3 to 5). The patients’ demographic information ispresented in Table 1.
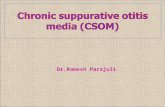
Culture-based description of the bacterial communities.Swab samples collected from the control (CI and T) and noncho-lesteatoma patients with the CWU procedure led to no microbialgrowth on culture plates. In contrast, patients with cholesteatoma(CWU and CWD procedures) had positive growth for both mid-dle ear (40 to 60%) and mastoid (20 to 50%) samples (Fig. 1A).None of the negative controls produced any amplification prod-ucts after the nested PCR amplification process and were consid-ered to be negative. A range of organisms were identified as Gram-
Microbiota of Chronic Suppurative Otitis Media
October 2016 Volume 54 Number 10 jcm.asm.org 2539Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

positive or anaerobic and included Corynebacterium jeikeium andShewanella algae. In addition, noncholesteatoma patients under-going a CWD procedure had higher rates of positive cultures fromthe middle ear (80%) than from the mastoid (20%) swab samples.Microbes identified in these patients included Klebsiella oxytoca,P. aeruginosa, C. jeikeium, Aspergillus flavus, and methicillin-resis-tant S. aureus.
Molecular characterization of the bacterial communities.16S rRNA gene sequences could be obtained from middle ear andmastoid samples of 50 to 80% of cholesteatoma patients, 35 to80% of noncholesteatoma patients, 43% of control CI patients,and 14% of control T patients (Fig. 1B). The success in obtainingamplifiable DNA was not consistent between sample sites (middleear and mastoid) for each patient. The number of sequences per
TABLE 1 Patient demographics
Group Surgerya Patientb Sexc Aged Sidee Stagef Ethnicity
Controls Cochlear implant C_CI_1 F 12 L EuropeanC_CI_2 M 18 m L EuropeanC_CI_3 F 5 R ChineseC_CI_4 F 4 L EuropeanC_CI_5 M 4 L AfricanC_CI_6 F 14 L EuropeanC_CI_7 F 14 R IndonesianC_CI_8 M 70 L EuropeanC_CI_9 F 85 R EuropeanC_CI_10 M 15 R MaoriC_CI_11 M 10 R EuropeanC_CI_12 F 7 m R PolynesianC_CI_13 M 6 R MaoriC_CI_14 M 53 R EuropeanC_CI_15 F 6 m R Chinese
Tumor C_T_1 M 65 L EuropeanC_T_2 M 52 R EuropeanC_T_3 M 72 R IndianC_T_4 M 57 L EuropeanC_T_5 M 61 R EuropeanC_T_6 M 36 L VietnameseC_T_7 M 63 R European
Cholesteatoma CWD CWD_Ch_1 F 71 L 4 EuropeanCWD_Ch_2 M 74 R 2 ChineseCWD_Ch_3 M 45 R 4 IndianCWD_Ch_4 M 4 R 4 IndianCWD_Ch_5 M 12 R 4 PolynesianCWD_Ch_6 F 55 L 4 Maori
CWU CWU_Ch_1 M 6 R 4 PolynesianCWU_Ch_2 M 19 R 3 ChineseCWU_Ch_3 M 5 R 2 MaoriCWU_Ch_4 F 66 R 2 EuropeanCWU_Ch_5 F 7 R 4 EuropeanCWU_Ch_6 M 29 L 4 PolynesianCWU_Ch_7 F 7 L 2 EuropeanCWU_Ch_8 M 40 R 4 EuropeanCWU_Ch_9 M 7 L 2 EuropeanCWU_Ch_10 M 17 R 1 Polynesian
No cholesteatoma CWD CWD_NC_1 F 75 R EuropeanCWD_NC_2 M 30 R EuropeanCWD_NC_3 M 46 R MaoriCWD_NC_4 M 52 L EuropeanCWD_NC_5 F 73 R Maori
CWU CWU_NC_1 M 7 R IndianCWU_NC_2 F 44 L PolynesianCWU_NC_3 M 1 L Maori
a CWD, canal wall up; CWD, canal wall down.b CI, cochlear implant; T, tumor; Ch, cholesteatoma; NC, no cholesteatoma.c F, female; M, male.d Age in years or months (m).e L, left; R, right.f Stage: 1 to 6 (6 represents the most extensive disease).
Neeff et al.
2540 jcm.asm.org October 2016 Volume 54 Number 10Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

sample varied between 1,168 and 86,952. The total numbers ofOTUs obtained after quality trimming of the sequences across allmastoid (n � 21) and middle ear (n � 25) samples were 156 and163, respectively. Noncholesteatoma patients had the lowest bac-terial diversity compared with the cholesteatoma and controlgroups, as measured by the number of observed species and Shan-non and Simpson indices (see Fig. S1 in the supplemental mate-rial). However, these observed differences were not significant(Kruskal-Wallis test).
Interpatient differences explained the majority of the variationin bacterial composition observed in the data set of CSOM pa-tients (R2 � 34.4%, P � 0.002). Interestingly, such high variationwas not observed in the control group. In addition, no significantdifferences were measured between the sampling site (mastoidversus middle ear) or disease status or subgroupings or age.
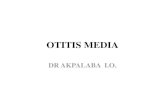
The microbiota of the healthy ear was composed of a range ofbacteria, including members of the genera Novosphingobium,Staphylococcus, Streptococcus, Escherichia-Shigella, and Burkhold-eria (Fig. 2). The bacterial compositions of CSOM were also vari-able between patients and included members of the genera Hae-mophilus, Staphylococcus, Alloiococcus, and Streptococcus. Thegenus Pseudomonas was found in a minor proportion (4/46) ofsamples and with variable relative abundance ranging from 0.01 to99%. Staphylococcus, another commonly cultured organism fromear discharge, was detected in 39% (18/46) of the samples, includ-ing healthy controls, with relative abundance ranging from 0.01 to99%. Propionibacterium was found in the middle ears and mas-toids of both control and CSOM patients (�11% relative se-
quence abundance). In addition, Alloiococcus and Haemophiluswere detected largely in cholesteatoma patients (Fig. 3).
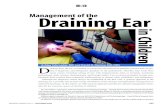
All samples from this study with sequence information wereplotted on a multidimensional scaling (MDS) plot using weightedUniFrac distances to visualize clustering of sample types (Fig. 4).However, no clustering was observed based on disease status (withand without CSOM) or sampling site (mastoid versus middle ear)or the CWU or CWD procedure.
DISCUSSION
Our current understanding of the microbiology of the middle earand mastoid mucosa in healthy and diseased states has beenlargely derived from bacterial cultivation studies. These results areinevitably skewed due to the failure of some bacteria to grow instandard culture media (47). In contrast, cultivation-independentmolecular techniques are able to provide a more accurate assess-ment of the microbial communities growing on the mucosa. Here,we applied molecular techniques to determine the microbiota inboth patients with CSOM and those with healthy middle ear mu-cosa, and our findings are very different from those of previousculture-based studies.
Molecular evidence that the healthy middle ear is not sterile.It has been a long-held belief that the middle ear of a healthyindividual is sterile (22, 23). In contrast, the results from this studyshow a diverse bacterial community being detected in 45% ofhealthy mastoids and middle ears. Notably, our cultivation-baseddata, which are targeted toward suspected pathogens, detected nobacteria in either the middle ears or mastoids of healthy individ-
FIG 1 Relative proportion of samples that had positive results for bacteria from either culture (A) or molecular techniques (B). Middle ear (black) and mastoid(gray) samples are shown in the graphs. Samples were grouped into control with cochlear implant (CI) or tumor (T) surgeries, cholesteatoma (Ch) with canal wallup (CWU) or canal wall down (CWD) procedures, and noncholesteatoma (NC) with CWU or CWD.
Microbiota of Chronic Suppurative Otitis Media
October 2016 Volume 54 Number 10 jcm.asm.org 2541Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

uals. Only with the application of cultivation-independent, mo-lecular biology techniques were bacteria detected in these patients.Even then, a highly permissive PCR protocol (comprising �45PCR cycles) was required, suggesting that bacterial loads on themucosa of healthy individuals are low. In addition, the swab sam-ples contained traces of blood, which could have potentially in-hibited PCRs in some samples. Future studies should focus onconfirming the findings from this study by using alternative ap-proaches such as FISH.
CSOM is thought to result from bacteria ascending from thenasopharynx via the Eustachian tube (48) or invading from theexternal auditory meatus (ear canal) through a perforation ofthe tympanic membrane. This ultimately causes irreversible mu-cosal changes that produce chronic otorrhea (ear discharge) andlead to hearing loss. However, our demonstration that manyhealthy middle ears do in fact contain bacteria demands consid-eration of a potential new concept for initiation of CSOM. Infec-tions within the middle ear and mastoid may need to be viewed asa consequence of a disturbance to the normal balance of commen-sal bacteria (i.e., dysbiosis), at least in some individuals. Undersuch a model, pathogenesis would likely still involve invasion ofbacteria from the nasopharynx or ear canal, but after a perturba-tion of the resident bacterial community rather than invasion of apreviously sterile space.
Alternatively, or in addition to the above, CSOM may arisefrom middle ear or mastoid commensal bacteria alone, withoutcontributions from adjacent anatomical sites. Indeed, potentialpathogens, such as Staphylococcus, Pseudomonas, Streptococcus,and Moraxella, which have been implicated in ear disease usingcultivation techniques, were also detected among healthy con-trols, supporting the notion of the resident microbiota as a poten-
tial source of infection from within. Perturbations to the com-mensal microbiota could conceivably occur due to, for example,excessive antibiotic usage and/or compromised immunity.
At other mucosal sites, commensal organisms play importantroles in defense against opportunistic bacterial invasion. In thegut, for example, communication and regulation between bacteriacan have positive or negative effects on bacterial growth. Suchinteractions appear to be mediated through signaling moleculesreleased by bacteria and reabsorbed by the host cell (49, 50). It ispossible, but remains to be demonstrated, that similar interac-tions occur in the middle ear.
Disease status and interpersonal differences account formuch of the variation in the microbiota of the middle ear andmastoid. The majority of the variation in the bacterial communi-ties of CSOM patients was accounted for by interpersonal differ-ences. As this observation was not seen for controls, it furthersupports the suggestion that the bacterial communities of CSOMpatients are disrupted, leading to an imbalance in communitystructure. Such observations have been reported previously in thegut (51) and paranasal sinuses (52, 53). Interestingly, sample site(mastoid versus middle ear) within an individual had no influenceon bacterial community variation, suggesting that similar com-munities were found at both sites. Substantial interpatient varia-tion has been observed in a number of human sinus, gut, and skinmicrobiomes (35, 54, 55). Ethnicity has been shown to contributeto some of this variation (56). Due to the small patient numbers inthis study, no such associations were observed in this study (Table1). It is possible that with a larger study (more patients), ethnicitysignatures might become more apparent.
Identification of prominent CSOM microbiota. The diversityof pathogens/bacteria identified in swab samples by hospital cul-
FIG 2 16S rRNA gene-based bacterial community compositions of the middle ears (A) and mastoids (B) of CSOM subjects and healthy individuals. CSOMpatients have been grouped into cholesteatoma (Ch) and noncholesteatoma (NC) patients. Types of surgery (canal wall up [CWU] or canal wall down [CWD])are also indicated on the graph. Bacterial community sequence data are displayed at the genus level, with data for each taxon expressed as a proportion of sequencereads for a given sample. CI, cochlear implant; T, tumor.
Neeff et al.
2542 jcm.asm.org October 2016 Volume 54 Number 10Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

tivation techniques is typically an underestimate. Routine diag-nostic hospital laboratories will normally selectively culture forknown pathogens; therefore, other cultivable organisms may beoverlooked. Notwithstanding this caveat, given that much of the
human microbiota is uncultivable or extremely hard to grow (47),molecular tools are able to offer better insights into the bacterialcommunity composition of a given sample. Based on the results ofthis study, we did not observe a specific microbial profile typical of
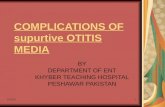
FIG 3 Relative sequence abundance of six prominent ear bacterial genera. These include Alloiococcus (A), Haemophilus (B), Staphylococcus (C), Pseudomonas (D),Moraxella (E), and Propionibacterium (F). The data shown represent the middle ears (Mid) and mastoids (Mast) of control, noncholesteatoma (NC), and cholestea-toma (Chol) patients. An asterisk represents a significantly different (P � 0.05) group compared with the 5 other groups in this study. Error bars are standard deviations.
Microbiota of Chronic Suppurative Otitis Media
October 2016 Volume 54 Number 10 jcm.asm.org 2543Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

CSOM. Putative pathogens such as Staphylococcus, Pseudomonas,and Haemophilus were also observed in healthy control microbi-ota. The next step for this research is to elucidate the influence ofthe microbiota on the host.
We demonstrated the presence of Propionibacterium in normalmastoid and middle ear mucosa. The relative sequence abundanceof Propionibacterium was significantly higher in controls than inpatients with CSOM. Members of the genus Propionibacterium arepart of the normal microbiota of the skin, mouth, and gut (57–60). They are believed to play a role in stabilizing the normalmicrobiota by occupying niches which then cannot be invaded bypathogens (58, 59). Moraxella is a known pathogen of the humanrespiratory tract, typically causing pneumonias in adults and acuteotitis media in children (48). It is not a classic pathogen reportedin CSOM. The occurrence of Moraxella was variable betweengroups, but it was mostly found in control and noncholesteatomapatients at relatively low abundance. Our findings thus support itbeing part of the commensal microbiota in normal middle earsand mastoids but not a significant player in CSOM.
There has been debate about whether members of the bacterialgenus Alloiococcus play a role in the pathogenesis of otitis media inchildren or if they are part of the commensal microbiota (61, 62).Using molecular techniques, we found higher relative abundancein CSOM patients with cholesteatoma than in controls or othersubject groups. To better understand the potential role of Alloio-coccus in CSOM, further study into host interaction and coloniza-tion of adjacent sites in normal and diseased patients will be nec-essary. Of note, Staphylococcus was identified in the microbiota ofmany patients in our study, but was Pseudomonas detected in rel-atively few patients. These results contrast with those of many
culture-based studies in which P. aeruginosa and S. aureus werethe dominant bacteria (10, 13�16, 18). Differences in the capa-bilities of certain species to grow in culture media may account formuch of the disparity between culture-based and molecular tech-niques (47). The preliminary findings of this small study will needto be further validated in the future with larger cohort sizes.
Clinical implications. In light of our findings, the importanceof Pseudomonas as a pathogen in CSOM requires further investi-gation. Patients in this study would not have benefited from anti-biotics targeting Pseudomonas in CSOM. This is clinically impor-tant, as overuse of antipseudomonal antibiotics can promotebacterial resistance (10, 17, 27). More generally, the use of broad-spectrum antibiotics may have an unfavorable effect on commen-sal bacterial communities, potentially affording pathogens a com-petitive advantage by eliminating competing commensal bacteria.Antibiotics administered early in life may alter the biomass andcomposition of the normal microbiota and reduce the exposure ofpotential pathogens to the immune system. In studies on gut mi-crobiota, these mechanisms have been reported to result in dys-biosis (63). It is possible that antibiotic use for CSOM early in lifemay cause dysbiosis and may have a detrimental effect on a pa-tient’s long-term ear health. Further studies are needed to exam-ine the effect of antibiotics on the middle ear microbiota in healthand disease.
In conclusion, the healthy middle ear and mastoid mucosa aredependent on normal Eustachian tube function and mucosal im-munity and an absence of allergy and infection (3). In humanbeings, commensal bacteria have been shown to coexist to main-tain a healthy environment in a variety of body sites, and this studysuggests that a bacterial community is often present in the normal
FIG 4 Nonmetric multidimensional scaling plots based on weighted UniFrac values of the bacterial communities. Only paired mastoid and middle ear samplesfrom patients were chosen for this analysis. Bacterial communities were grouped based on sample type (mastoid versus middle ear) (A), study subgroups(cholesteatoma [CWU and CWD], noncholesteatoma, and controls) (B), and patients (C).
Neeff et al.
2544 jcm.asm.org October 2016 Volume 54 Number 10Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

human middle ear and mastoid. There is a disparity between cul-ture and molecular assessment of the middle ear and mastoid,which may lead to inappropriate prescribing of antibiotics. Theuse of molecular techniques to describe the microbiota shouldfurther refine our understanding of the role of the middle ear andmastoid microbiota in the pathogenesis of chronic inflammatoryear diseases.
ACKNOWLEDGMENTS
We thank all of the participants of this study.The research reported here was funded by an A trust research grant
(Auckland District Health Board).
FUNDING INFORMATIONThis work, including the efforts of Michel Neeff, Kristi Biswas, Michael W.Taylor, and Richard Douglas, was funded by Auckland District HealthBoard (A5469).
REFERENCES1. Li MG, Hotez PJ, Vrabec JT, Donovan DT. 2015. Is chronic suppurative
otitis media a neglected tropical disease? PLoS Negl Trop Dis 9:e0003485.http://dx.doi.org/10.1371/journal.pntd.0003485.
2. Acuin J, World Health Organization Department of Child and HealthAdolescent Health and Development and the Team for Prevention ofBlindness and Deafness of the World Health Organization Blindness.2004. Chronic suppurative otitis media: burden of illness and manage-ment options. World Health Organization, Geneva, Switzerland.
3. Acuin J. 2007. Chronic suppurative otitis media. BMJ Clin Evid 2007:0507.
4. Verhoeff M, van der Veen EL, Rovers MM, Sanders EAM, Schilder AGM.2006. Chronic suppurative otitis media: a review. Int J Pediatr Otorhinolar-yngol 70:1–12. http://dx.doi.org/10.1016/j.ijporl.2005.08.021.
5. Lasisi AO, Olaniyan FA, Muibi SA, Azeez IA, Abdulwasiu KG, Lasisi TJ,Imam ZO, Yekinni TO, Olayemi O. 2007. Clinical and demographic riskfactors associated with chronic suppurative otitis media. Int J PediatricOtorhinolaryngol 71:1549 –1554. http://dx.doi.org/10.1016/j.ijporl.2007.06.005.
6. Monasta L, Ronfani L, Marchetti F, Montico M, Vecchi Brumatti L,Bavcar A, Grasso D, Barbiero C, Tamburlini G. 2012. Burden of diseasecaused by otitis media: systematic review and global estimates. PLoS One7:e36226. http://dx.doi.org/10.1371/journal.pone.0036226.
7. Morris P. 2012. Chronic suppurative otitis media. BMJ Clin Evid 2012:0507.
8. Coticchia JM, Chen M, Sachdeva L, Mutchnick S. 2013. New paradigmsin the pathogenesis of otitis media in children. Front Pediatr 1:52. http://dx.doi.org/10.3389/fped.2013.00052.
9. Taylor PS, Faeth I, Marks MK, Del Mar CB, Skull SA, Pezzullo ML,Havyatt SM, Coates HL. 2009. Cost of treating otitis media in Australia.Expert Rev Pharmacoecon Outcomes Res 9:133–141. http://dx.doi.org/10.1586/erp.09.6.
10. Mittal R, Lisi CV, Gerring R, Mittal J, Mathee K, Narasimhan G, AzadRK, Yao Q, Grati M, Yan D, Eshraghi AA, Angeli SI, Telischi FF, LiuXZ. 2015. Current concepts in the pathogenesis and treatment of chronicsuppurative otitis media. J Med Microbiol 64:1103–1116. http://dx.doi.org/10.1099/jmm.0.000155.
11. Levi J, O’Reilly RC, Isaacson GC, Armsby C. 2016. Chronic suppurativeotitis media (CSOM): Pathogenesis, clinical manifestations, and diagno-sis. www.uptodate.com.
12. O’Leary S, Veldman JE. 2002. Revision surgery for chronic otitis media:recurrent-residual disease and hearing. J Laryngol Otol 116:996 –1000.
13. Attallah MS. 2000. Microbiology of chronic suppurative otitis media withcholesteatoma. Saudi Med J 21:924 –927.
14. Juyal D, Negi V, Pal S, Adekhandi S, Sharma M, Sharma N, Prakash R.2013. Microbiology of chronic suppurative otitis media in a tertiary caresetup of Uttarakhand state, India. North Am J Med Sci 5:282. http://dx.doi.org/10.4103/1947-2714.110436.
15. Shrestha BL, Amatya R, Shrestha I, Ghosh I. 2012. microbiologicalprofile of chronic suppurative otitis media. Nepalese J ENT Head NeckSurg 2:6 –7.
16. Ahn JH, Kim M-N, Suk YA, Moon BJ. 2012. Preoperative, intraopera-
tive, and postoperative results of bacterial culture from patients withchronic suppurative otitis media. Otol Neurotol 33:54 –59. http://dx.doi.org/10.1097/MAO.0b013e31823dbc70.
17. Lee SK, Park DC, Kim MG, Boo SH, Choi YJ, Byun JY, Park MS, YeoSG. 2012. Rate of isolation and trends of antimicrobial resistance of mul-tidrug resistant Pseudomonas aeruginosa from otorrhea in chronic suppu-rative otitis media. Clin Exp Otorhinolaryngol 5:17. http://dx.doi.org/10.3342/ceo.2012.5.1.17.
18. Albert RRA, Job A, Kuruvilla G, Joseph R, Brahmadathan KN, John A.2005. Outcome of bacterial culture from mastoid granulations: is it rele-vant in chronic ear disease? J Laryngol Otol 119:774 –778.
19. Macfadyen C, Gamble C, Garner P, Macharia I, Mackenzie I, Mugwe P,Oburra H, Otwombe K, Taylor S, Williamson P. 2005. Topical quino-lone vs. antiseptic for treating chronic suppurative otitis media: a random-ized controlled trial. Trop Med Int Health 10:190 –197. http://dx.doi.org/10.1111/j.1365-3156.2004.01368.x.
20. Yang JA, Kim JY, Yoon YK, Kim S, Park DW, Sohn JW, Sim HS, KimMJ. 2008. Epidemiological and genetic characterization of methicillin-resistant Staphylococcus aureus isolates from the ear discharge of outpa-tients with chronic otitis media. J Korean Med Sci 23:762. http://dx.doi.org/10.3346/jkms.2008.23.5.762.
21. Chang J, Lee S-H, Choi J, Im GJ, Jung HH. 2011. Nasopharynx as amicrobiologic reservoir in chronic suppurative otitis media: preliminarystudy. Clin Exp Otorhinolaryngol 4:122. http://dx.doi.org/10.3342/ceo.2011.4.3.122.
22. Westerberg BD, Kozak FK, Thomas EE, Blondel-Hill E, BrunsteinJD, Patrick DM. 2009. Is the healthy middle ear a normally sterile site?Otol Neurotol 30:174 –177. http://dx.doi.org/10.1097/MAO.0b013e31819225a0.
23. Hall-Stoodley L, Hu FZ, Gieseke A, Nistico L, Nguyen D, Hayes J,Forbes M, Greenberg DP, Dice B, Burrows A. 2006. Direct detection ofbacterial biofilms on the middle-ear mucosa of children with chronic otitismedia. JAMA 296:202–211. http://dx.doi.org/10.1001/jama.296.2.202.
24. Baron S, Iglewski BH. 1996. Pseudomonas. In Baron S (ed), Medicalmicrobiology, 4th ed. The University of Texas Medical Branch at Galves-ton, Galveston, TX.
25. Byrd MS, Pang B, Hong W, Waligora EA, Juneau RA, Armbruster CE,Weimer KED, Murrah K, Mann EE, Lu H, Sprinkle A, Parsek MR, KockND, Wozniak DJ, Swords WE. 2011. Direct evaluation of Pseudomonasaeruginosa biofilm mediators in a chronic Infection model. Infect Immun79:3087–3095. http://dx.doi.org/10.1128/IAI.00057-11.
26. Dohar JE, Hebda PA, Veeh R, Awad M, Costerton JW, Hayes J, EhrlichGD. 2005. Mucosal biofilm formation on middle-ear mucosa in a nonhu-man primate model of chronic suppurative otitis media. Laryngoscope115:1469 –1472. http://dx.doi.org/10.1097/01.mlg.0000172036.82897.d4.
27. Lee SK, Lee MS, Jung SY, Byun JY, Park MS, Yeo SG. 2010. Antimi-crobial resistance of Pseudomonas aeruginosa from otorrhea of chronicsuppurative otitis media patients. Otolaryngol Head Neck Surg 143:500 –505. http://dx.doi.org/10.1016/j.otohns.2010.06.906.
28. Homøe P, Bjarnsholt T, Wessman M, Sørensen HCF, Johansen HK.2009. Morphological evidence of biofilm formation in Greenlanders withchronic suppurative otitis media. Eur Arch Otorhinolaryngol 266:1533–1538. http://dx.doi.org/10.1007/s00405-009-0940-9.
29. Thornton RB, Rigby PJ, Wiertsema SP, Filion P, Langlands J, CoatesHL, Vijayasekaran S, Keil AD, Richmond PC. 2011. Multi-species bac-terial biofilm and intracellular infection in otitis media. BMC Pediatr 11:94. http://dx.doi.org/10.1186/1471-2431-11-94.
30. Thornton RB, Wiertsema SP, Kirkham L-AS, Rigby PJ, Vijayasekaran S,Coates HL, Richmond PC. 2013. Neutrophil extracellular traps and bac-terial biofilms in middle ear effusion of children with recurrent acute otitismedia—a potential treatment target. PLoS One 8:e53837. http://dx.doi.org/10.1371/journal.pone.0053837.
31. Liu CM, Cosetti MK, Aziz M, Buchhagen JL, Contente-Cuomo TL,Price LB, Keim PS, Lalwani AK. 2011. The otologic microbiome: a studyof the bacterial microbiota in a pediatric patient with chronic serous otitismedia using 16S rRNA gene-based pyrosequencing. Arch OtolaryngolHead Neck Surg 137:664 – 668. http://dx.doi.org/10.1001/archoto.2011.116.
32. Jervis-Bardy J, Rogers GB, Morris PS, Smith-Vaughan HC, NosworthyE, Leong LEX, Smith RJ, Weyrich LS, De Haan J, Carney AS, Leach AJ,O’Leary S, Marsh RL. 2015. The microbiome of otitis media with effusionin Indigenous Australian children. Int J Pediatr Otorhinolaryngol 79:1548 –1555. http://dx.doi.org/10.1016/j.ijporl.2015.07.013.
Microbiota of Chronic Suppurative Otitis Media
October 2016 Volume 54 Number 10 jcm.asm.org 2545Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

33. Liu C, Cosetti M, Price L, Keim P, Lalwani A. 2010. Pyrosequencing-based analysis of the middle ear microbiota. Otolaryngol Head Neck Surg143:P102–P102. http://dx.doi.org/10.1016/j.otohns.2010.06.177.
34. Bluestone CD, Klein JO. 2007. Otitis media in infants and children, 4thed. BC Decker, Inc., Hamilton, ON, Canada.
35. Clinical and Laboratory Standards Institute. 2014. Performance stan-dards for antimicrobial susceptibility testing; 24th informational supple-ment. Clinical and Laboratory Standards Institute, Wayne PA.
36. Biswas K, Hoggard M, Jain R, Taylor MW, Douglas RG. 2015. The nasalmicrobiota in health and disease: variation within and between subjects.Front Microbiol 9:134. http://dx.doi.org/10.3389/fmicb.2015.00134.
37. Spring S, Lins U, Amann R, Schleifer KH, Ferreira LC, Esquivel DM,Farina M. 1998. Phylogenetic affiliation and ultrastructure of unculturedmagnetic bacteria with unusually large magnetosomes. Arch Microbiol169:136 –147. http://dx.doi.org/10.1007/s002030050553.
38. Polz MF, Cavanaugh CM. 1998. Bias in template-to-product ratios inmultitemplate PCR. Appl Environ Microbiol 64:3724 –3730.
39. Kim RJT, Biswas K, Hoggard M, Taylor MW, Douglas RG. 2015. Pairedanalysis of the microbiota of surface mucus and whole-tissue specimens inpatients with chronic rhinosinusitis. Int Forum Allergy Rhinol 5:877– 883.http://dx.doi.org/10.1002/alr.21600.
40. Herlemann DP, Labrenz M, Jürgens K, Bertilsson S, Waniek JJ, Ander-sson AF. 2011. Transitions in bacterial communities along the 2000 kmsalinity gradient of the Baltic Sea. ISME J 5:1571–1579. http://dx.doi.org/10.1038/ismej.2011.41.
41. Edgar RC. 2013. UPARSE: highly accurate OTU sequences from micro-bial amplicon reads. Nat Methods 10:996 –998. http://dx.doi.org/10.1038/nmeth.2604.
42. Caporaso JG, Kuczynski J, Stombaugh J, Bittinger K, Bushman FD,Costello EK, Fierer N, Peña AG, Goodrich JK, Gordon JI, Huttley GA,Kelley ST, Knights D, Koenig JE, Ley RE, Lozupone CA, McDonald D,Muegge BD, Pirrung M, Reeder J, Sevinsky JR, Turnbaugh PJ, WaltersWA, Widmann J, Yatsunenko T, Zaneveld J, Knight R. 2010. QIIMEallows analysis of high-throughput community sequencing data. NatMethods 7:335–336. http://dx.doi.org/10.1038/nmeth.f.303.
43. Wang Q, Garrity GM, Tiedje JM, Cole JR. 2007. Naive Bayesian classifierfor rapid assignment of rRNA sequences into the new bacterial taxonomy.Appl Environ Microbiol 73:5261–5267. http://dx.doi.org/10.1128/AEM.00062-07.
44. Caporaso JG, Bittinger K, Bushman FD, DeSantis TZ, Andersen GL,Knight R. 2010. PyNAST: a flexible tool for aligning sequences to a tem-plate alignment. Bioinformatics 26:266 –267. http://dx.doi.org/10.1093/bioinformatics/btp636.
45. Price MN, Dehal PS, Arkin AP. 2010. FastTree 2 approximately maxi-mum-likelihood trees for large alignments. PLoS One 5:e9490. http://dx.doi.org/10.1371/journal.pone.0009490.
46. Lozupone C, Knight R. 2005. UniFrac: a new phylogenetic method forcomparing microbial communities. Appl Environ Microbiol 71:8228 –8235. http://dx.doi.org/10.1128/AEM.71.12.8228-8235.2005.
47. Stewart EJ. 2012. Growing unculturable bacteria. J Bacteriol 194:4151–4160. http://dx.doi.org/10.1128/JB.00345-12.
48. Murphy TF, Parameswaran GI. 2009. Moraxella catarrhalis, a humanrespiratory tract pathogen. Clin Infect Dis 49:124 –131. http://dx.doi.org/10.1086/599375.
49. Vogt SL, Peña-Díaz J, Finlay BB. 2015. Chemical communication in thegut: effects of microbiota-generated metabolites on gastrointestinal bac-
terial pathogens. Anaerobe 34:106 –115. http://dx.doi.org/10.1016/j.anaerobe.2015.05.002.
50. Thompson JA, Oliveira RA, Xavier KB. 2016. Chemical conversations inthe gut microbiota. Gut Microbes 7:163–170. http://dx.doi.org/10.1080/19490976.2016.1145374.
51. Guinane CM, Cotter PD. 2013. Role of the gut microbiota in health andchronic gastrointestinal disease: understanding a hidden metabolic organ.Ther Adv Gastroenterol 6:295–308. http://dx.doi.org/10.1177/1756283X13482996.
52. Stressmann FA, Rogers GB, Chan SW, Howarth PH, Harries PG, BruceKD, Salib RJ. 2011. Characterization of bacterial community diversity inchronic rhinosinusitis infections using novel culture-independent tech-niques. Am J Rhinol Allergy 25:e133– e140.
53. Feazel LM, Robertson CE, Ramakrishnan VR, Frank DN. 2012. Micro-biome complexity and Staphylococcus aureus in chronic rhinosinusitis.Laryngoscope 122:467– 472. http://dx.doi.org/10.1002/lary.22398.
54. Turnbaugh PJ, Hamady M, Yatsunenko T, Cantarel BL, Duncan A, LeyRE, Sogin ML, Jones WJ, Roe BA, Affourtit JP, Egholm M, Henrissat B,Heath AC, Knight R, Gordon JI. 2009. A core gut microbiome in obeseand lean twins. Nature 457:480 – 484. http://dx.doi.org/10.1038/nature07540.
55. Grice EA, Kong HH, Renaud G, Young AC, NISC Comparative Se-quencing Program, Bouffard GG, Blakesley RW, Wolfsberg TG, TurnerML, Segre JA. 2008. A diversity profile of the human skin microbiota.Genome Res 18:1043–1050. http://dx.doi.org/10.1101/gr.075549.107.
56. The Human Microbiome Project Consortium. 2012. A framework forhuman microbiome research. Nature 486:215–221. http://dx.doi.org/10.1038/nature11209.
57. Grice EA, Kong HH, Conlan S, Deming CB, Davis J, Young AC, NISCComparative Sequencing Program, Bouffard GG, Blakesley RW, Mur-ray PR, Green ED, Turner ML, Segre JA. 2009. Topographical andtemporal diversity of the human skin microbiome. Science 324:1190 –1192. http://dx.doi.org/10.1126/science.1171700.
58. McDowell A, Barnard E, Nagy I, Gao A, Tomida S, Li H, Eady A, CoveJ, Nord CE, Patrick S. 2012. An expanded multilocus sequence typingscheme for Propionibacterium acnes: Investigation of ‘pathogenic,’ ‘com-mensal’ and antibiotic resistant strains. PLoS One 7:e41480 –14. http://dx.doi.org/10.1371/journal.pone.0041480.
59. Bojar RA, Holland KT. 2004. Acne and Propionibacterium acnes. ClinDermatol 22:375–379. http://dx.doi.org/10.1016/j.clindermatol.2004.03.005.
60. Marsh RL, Binks MJ, Beissbarth J, Christensen P, Morris PS, Leach AJ,Smith-Vaughan HC. 2012. Quantitative PCR of ear discharge from In-digenous Australian children with acute otitis media with perforation sup-ports a role for Alloiococcus otitidis as a secondary pathogen. BMC EarNose Throat Disord 12:11. http://dx.doi.org/10.1186/1472-6815-12-11.
61. Harimaya A, Takada R, Somekawa Y, Fujii N, Himi T. 2006. Highfrequency of Alloiococcus otitidis in the nasopharynx and in the middle earcavity of otitis-prone children. Int J Pediatr Otorhinolaryngol 70:1009 –1014. http://dx.doi.org/10.1016/j.ijporl.2005.10.012.
62. Tano K, Essen von R, Eriksson PO, Sjöstedt A. 2008. Alloiococcusotitidis– otitis media pathogen or normal bacterial flora? APMIS 116:785–790. http://dx.doi.org/10.1111/j.1600-0463.2008.01003.x.
63. Principi N, Esposito S. 2016. Antibiotic administration and the develop-ment of obesity in children. Int J Antimicrob Agents 47:171–177. http://dx.doi.org/10.1016/j.ijantimicag.2015.12.017.
Neeff et al.
2546 jcm.asm.org October 2016 Volume 54 Number 10Journal of Clinical Microbiology
on October 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from