Management of the Draining Earpedclerk.bsd.uchicago.edu/sites/pedclerk.uchicago... · Chronic...
12
PEDIATRIC ANNALS 33:12 | DECEMBER 2004 843 D rainage from the ear, or otorrhea, is commonly encountered in pediatric practice and can pre- sent a diagnostic and therapeutic quandary to the pediatrician. Otorrhea may result from many causes, including soiling of ears with tympanostomy tubes or tympanic membrane perforations, otitis externa, cholesteatoma, and foreign bodies. Less common etiologies include cere- brospinal fluid otorrhea from congenital malformations or trauma, otitic candidiasis, and malignancy. Although the diagnosis cannot always be established at the first visit, a general approach to the draining ear is possible that permits timely elucidation of the etiology and appropriate management or referral if necessary. In this article, we offer such an approach and discuss rational management strate- gies for the common causes of otorrhea in children. Management of the Dr. Schroeder is a physician with the Department of Otolaryngology – Head & Neck Surgery, Portsmouth Naval Med- ical Center, Portsmouth,VA, and a commander in the United States Navy. Dr. Darrow is associate professor of otolaryn- gology and pediatrics, Eastern Virginia Medical School, and attending otolaryngologist, Children’s Hospital of The King’s Daughters, both in Norfolk, VA. Address reprint requests to: David H. Darrow, MD, DDS, Department of Otolaryngology – Head & Neck Surgery, East- ern Virginia Medical School, 825 Fairfax Avenue, Norfolk,VA 23507. Dr. Darrow is on the Speakers’ Bureau with Alcon Laboratories. Dr. Schroeder has no industry relationships to disclose. Ashley Schroeder, MD and David H. Darrow, MD, DDS Draining Ear in Children
Transcript of Management of the Draining Earpedclerk.bsd.uchicago.edu/sites/pedclerk.uchicago... · Chronic...

PEDIATRIC ANNALS 33:12 | DECEMBER 2004 843
Drainage from the ear, or otorrhea, is commonly encountered in pediatric practice and can pre-
sent a diagnostic and therapeutic quandary to the pediatrician. Otorrhea may result from
many causes, including soiling of ears with tympanostomy tubes or tympanic membrane
perforations, otitis externa, cholesteatoma, and foreign bodies. Less common etiologies include cere-
brospinal fluid otorrhea from congenital malformations or trauma, otitic candidiasis, and malignancy.
Although the diagnosis cannot always be established at the first visit, a general approach to the
draining ear is possible that permits timely elucidation of the etiology and appropriate management or
referral if necessary. In this article, we offer such an approach and discuss rational management strate-
gies for the common causes of otorrhea in children.
Management of the
Dr. Schroeder is a physician with the Department of Otolaryngology – Head & Neck Surgery, Portsmouth Naval Med-ical Center, Portsmouth, VA, and a commander in the United States Navy. Dr. Darrow is associate professor of otolaryn-gology and pediatrics, Eastern Virginia Medical School, and attending otolaryngologist, Children’s Hospital of The King’sDaughters, both in Norfolk,VA.
Address reprint requests to: David H. Darrow, MD, DDS, Department of Otolaryngology – Head & Neck Surgery, East-ern Virginia Medical School, 825 Fairfax Avenue, Norfolk,VA 23507.
Dr. Darrow is on the Speakers’ Bureau with Alcon Laboratories. Dr. Schroeder has no industry relationships to disclose.
Ashley Schroeder, MD and David H. Darrow, MD, DDS
Draining Earin Children

844 PEDIATRIC ANNALS 33:12 | DECEMBER 2004
APPROACH TO THE DRAINING EARWhen evaluating a child with otor-
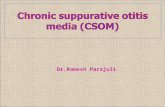
rhea, a thorough history of the chiefcomplaint and past otologic events oftensuggests an etiology (Sidebar 1, seepage 846). Bilateral drainage occursmost commonly with tympanostomytubes or tympanic membrane perfora-tions (Figure 1, see page xxx) but mayalso occur in unusual cases of otitisexterna (swimmer’s ear). A history ofswimming or upper respiratory infectionpreceding the onset of otorrhea is com-mon with tubes or tympanic membraneperforation. Bilateral cholesteatoma is a
rare occurrence. Long-standing drainageusually suggests a chronic middle earprocess such as cholesteatoma or granu-lation tissue.
Chronic drainage also may resultwhen common infectious agents areinadequately treated topically or sys-temically; when yeast, fungi, ormycobacteria are present; or when thepatient is unable to mount an appropri-ate immune response. Bloody drainageusually suggests the presence of granu-lation tissue or trauma to the ear canal,although severe otitis media also mayoccasionally be associated with thisfinding. Pain on palpation of the auriclemost commonly is associated with otitisexterna but may be present when pro-longed drainage of any kind has causedirritation of the external ear. Deep painmay be associated with complications ofotitis media.
CAUSES OF OTORRHEA Tympanostomy Tube Otorrhea
Tympanostomy tube otorrhea is themost common type of otorrhea encoun-tered, occurring at least once in up to75% of patients within the first 12
months after tubes are inserted.1 In arecent meta-analysis of patients whounderwent tube insertion, otorrhea wascharacterized as early (less than 2 weeksafter placement) in 16% and late in26%, and recurrent in 7.4% and chronicin 4%.2 Early tube otorrhea most com-monly is associated with mucoid orpurulent effusions at surgery and far lesscommonly with serous or absent effu-sion.3 It is more likely related to middleear conditions at surgery than to sterilepreparation of the ear canal.4-6
Post-tympanostomy tube otorrheamay be reduced by the use of antibioticeardrops at the time of tube placementand by saline irrigation of the middle earthrough the myringotomy at surgery.7,8
Bacterial biofilms have been implicatedas a possible etiology in cases of recur-rent and chronic otorrhea.9
Usually seen during episodes ofacute upper respiratory infection, tubeotorrhea is precipitated by the usual oti-tis media organisms (Streptococcuspneumoniae, Haemophilus influenzae,Moraxella catarrhalis). However, with-in hours to days, Pseudomonas aerugi-nosa may become the predominantorganism.10 In children older than 3,middle ear organisms are cultured lesscommonly and Staphylococcus aureusis found more frequently.11,12 In thesummer, when otorrhea may be associ-ated with infection from externalsources, involvement of nasopharyngealpathogens is even less likely.11
In most cases, tube otorrhea is pain-less and resolves spontaneously within afew days. In children 6 or younger treat-ed with oral placebo and daily suction-ing of the tube, about one-third resolvedby day 4.13 In more persistent or symp-tomatic cases, topical or systemicantimicrobial therapy may be indicated.
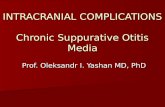
When the drainage is bloody or failsto clear after ototopical therapy, granu-lation tissue often is present at the edgeof the tube (Figure 2). This occurs in 5%Figure 1. External crusting frequently is associated with draining ears.
EDUCATIONAL OBJECTIVES
1. Describe the differentialdiagnosis of and initialmanagement of the draining earin children.
2. List the indications for, andefficacy of, topical, oral, andintravenous therapy of otorrheain children.
3. Discuss those situations inwhich a child with otorrheashould be referred to anotolaryngologist.

PEDIATRIC ANNALS 33:12 | DECEMBER 2004 845
to 14% of patients whose tubes havebeen in less than 3 years, and the risk ofdeveloping granulation increases withtube longevity.14 Although granulationusually is present on the lateral surfaceof the eardrum, the tissue may alsooccupy the middle ear or even the lumenof the tube, rendering it ineffective.
The risk of otorrhea due to waterexposure in patients with tubes has beenaddressed in a number of studies.15-19 Invitro models of tubes exposed to watersuggest that pressures of 12.8 to 13.3 cmH20 (equivalent to approximately 6 feetof depth below the surface) are requiredto push most types of water through thelumen of a standard tube.19 Most authorsof in vivo studies have concluded thatpatients who swim on the surface and donot make deep dives have no increasedrisk of otorrhea with water exposure.15-21
Factors that may increase the risk ofotorrhea due to water exposure includelarge lumen tubes or tympanic mem-brane perforations, soapy water (whichdecreases surface tension), lake water orwater known to be contaminated, andswimming at depths below 2 to 6feet.15,18-20 When these factors are pre-sent, the ear should be protected usingcommercially available ear plugs. Mold-able putty plugs must be gently placedin the ear so as to avoid fragmenting thematerial deep in the ear canal. Duringperiods of brief water exposure, cottoncoated with petroleum jelly may provideadequate protection.
For those uncommon patients whoare highly susceptible to otorrhea, limit-ed water exposure or use of water pre-cautions may be recommended. Oto-topical medications may be used afterswimming, although these medicationsoccasionally may cause discomfortwhen used in a dry middle ear.
Otitis ExternaOtitis externa is an infection of the
external auditory canal most commonly
preceded by mechanical or chemicaldamage to the normal protective barriercreated by the skin and cerumen. Theloss of protective films and secretionsleads to elevated pH and an environmentin which infecting organisms thrive. P.aeruginosa and S. aureus are the mostcommon infecting organisms, althoughcultures from the canal may demonstrateEscherichia coli, streptococci,Aspergilli, or Candida albicans. Chronicor recurrent external otitis may resultfrom fungal infection or from skin con-ditions such as eczema, seborrhea, orpsoriasis. In cases of eczematous der-matitis of the ear canal, moist vesicle andpustules are seen acutely and crusts andscales form in ears affected chronically.
Although otorrhea is often present,the hallmarks of external ear infectionsare severe pain and a sense of fullness inthe affected ear. When the ear canal ispatent, cheesy debris due to desquama-tion may be found along the canal walls.
In severe cases, the tympanic membranemay be obscured and associated postau-ricular swelling may be confused withmastoiditis. However, association withswimming or canal trauma, the absenceof high fever, and pain with movementof the auricle are more typical of otitisexterna. Equivocal cases should bereferred for otolaryngologic evaluation.
Chronic Suppurative Otitis Media(Without Cholesteatoma)
Chronic suppurative otitis media(CSOM) is characterized by otorrheathrough a perforation of the tympanicmembrane. This disorder begins as amucosal disease of the middle ear andmastoid due to soiling of the middle ear.Suppurative otitis is considered chronicafter 6 weeks, when scarring, osteitis,and bone destruction may be present.22-
24 In most cases, the drainage is pain-less; however, in the presence of boneinvolvement, otorrhea may be associat-
Figure 2. Granulation tissue and debris surround a retained tympanostomy tube.

846 PEDIATRIC ANNALS 33:12 | DECEMBER 2004
ed with deep pain and a foul smell.Advanced cases may involve intracra-nial complications.
The offending organisms in CSOMare much the same as seen in otitisexterna, with P. aeruginosa being themost common isolate. However, manycultures demonstrate polymicrobialinfections including gram-negativebacilli, Staphylococcus aureus, andanaerobes.22,23,25 The presence of middleear granulation may also suggest infec-tion by mycobacteria.26 Other uncom-mon causes of CSOM include tubercu-losis, syphilis, histiocytosis, and rhab-domyosarcomas.24
Recent reports suggest that medicalmanagement of CSOM is successful in75% to 89% of patients.22,23,25,27 A 10- to14-day course of systemic antibiotictherapy is recommended, accompaniedby daily aural toilet using the otologicmicroscope. However, in studies byKenna and colleagues, among childrenwho failed medical management, 36%to 50% had occult cholesteatoma at thetime of surgery.22,27 These data suggestthat the success rate of medical manage-ment in patients with true CSOM isactually higher. However, CSOM andcholesteatoma may simply representtwo points on the spectrum of ear dis-ease and, in refractory cases, the patientshould be examined meticulously by anotolaryngologist for abnormal tissuewithin or extruding from the middle ear.
Computer tomography scanning may beuseful in evaluating the extent of the softtissue disease and biopsy of this tissuethrough the perforation can occasionallybe performed in the office setting if nec-essary for diagnosis. Once the diagnosisis established, tympanomastoidectomyis often necessary for complete removalof the cholesteatoma or soft tissue andimprove ventilation.
Granular MyringitisGranular myringitis is characterized
by clear or purulent otorrhea associatedwith flat granulations on the surface of athickened but intact tympanic mem-brane. This disorder may be seen inpatients with otitis externa, or may pre-sent separately. Frequently, the etiologycannot be established. Treatment con-sists of debridement of the ear and treat-ment of the granulations with caustic orantiseptic agents, such as silver nitrate,trichloroacetic acid, gentian violet, orsteroid preparations.
Acute Otitis MediaNot infrequently, acute otitis media
presents with an acute perforation andotorrhea. The diagnosis can usually bemade based on a history of fever andsymptoms of upper respiratory infectionassociated with severe otalgia that sud-denly resolved when the ear begandraining purulent material. The perfora-tion is usually quite small and generally
closes within a few days. As a result,ototopical medications are generally farless effective in managing such infec-tions than are systemic agents. Patientsshould be reevaluated once the drainagehas ceased to be certain that the perfora-tion heals and the middle ear effusionclears spontaneously.
CholesteatomaCholesteatoma, more properly
termed “aural keratoma,” is the growthof squamous epithelium in the middleear space. This condition is frequentlyassociated with otorrhea, but thedrainage is often mild, resulting in inad-equate therapy and delayed referral. Themass consists of a matrix of differentiat-ed squamous epithelium that grows byaccumulation of desquamated material.A layer of granulation tissue surround-ing the keratoma elaborates enzymesthat cause the bony destruction seen inears with this disease.
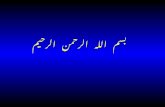
Aural keratoma generally is classifiedas either congenital or acquired. Con-genital keratomas are thought to arisefrom epithelial rests within the middleear. They are most frequently encoun-tered as a white pearl in the anterosupe-rior quadrant behind an intact tympanicmembrane. Destruction of the eardrumand otorrhea generally occur only inadvanced stages after the keratoma hasgrown considerably. Acquired keratomamay result from deep, chronic retrac-tions of the tympanic membrane, usuallyin the region of the pars flaccida (“pri-mary acquired keratoma”), or fromchronic perforation of the tympanicmembrane resulting in ingrowth of squa-mous tissue (“secondary acquired ker-atoma”) (Figure 3, see page 847).Acquired keratoma is also a rare butpotentially serious consequence of tym-panostomy tube placement, followingwhich the eardrum may be weak or per-forated at the site of the extruded tube.28
Acquired keratomas are identified as a
SIDEBAR 1.
Questions to Determine the Etiology of Otorrhea
1. Is the drainage unilateral or bilateral?
2. How long has the drainage been present?
3. Has there been any bloody drainage?
4. Does the ear hurt? If so, is the pain deep or confined to the external ear?
5. Is there a history of tympanostomy tubes or tympanic membrane
perforation?
6. Does the child have any known immune deficiencies?

PEDIATRIC ANNALS 33:12 | DECEMBER 2004 847
collection of pearly white squamousdebris associated with an irregular orperforated tympanic membrane, often ina superior location. The process is fre-quently obscured by a layer of purulentdrainage or granulation tissue, as the ker-atomatous debris serves as an excellentculture medium for bacteria.
Treatment of the associated bacterialinfection with ototopical medicationoften simplifies the diagnosis. Manypatients have hearing loss on audiomet-ric screening, especially in the presenceof a large perforation or ossicular ero-sion. Some patients have remarkablygood hearing, however, due to conduc-tion of sound through the cholesteatomato the oval window.
Once the diagnosis of keratoma issuspected, referral to the otolaryngolo-gist is imperative. Delayed referral maylead to complications including facialnerve paralysis, semicircular canal ero-sion with labyrinthine fistula, ossicularerosion, periosteal abscess, lateral sinusthrombosis, and intracranial abscess.Computed tomography is necessary todefine the extent and to plan the surgicalremoval of the disease. Tympanoplastywith or without mastoidectomy is usual-ly necessary, including repair of thedamaged eardrum.
Foreign BodyAlthough even foreign bodies of long
duration are often asymptomatic, theyoccasionally present with unilateral otal-gia and otorrhea, much like otitis exter-na. Parents are usually unaware that thedrainage is associated with a foreignbody, and the object is often apparentonly after thorough debridement.
Once a foreign body is identified, thefirst attempt at removal is usually thebest, and may be the last before a trip tothe operating room or conscious seda-tion is necessary. Irrigation is to beavoided in most cases, since this maypush the foreign body deeper and the
child may become increasingly anxious.Some objects, such as beans, mayexpand in the presence of moisture mak-ing removal even more difficult. Refer-ral to an otolaryngologist should be con-sidered since removal may be difficultand complete inspection of the canaland tympanic membrane are necessary.If removal is undertaken, the shape, tex-ture, and orientation of the object mustbe studied. A wide variety of instru-ments should be available, including:alligator forceps for objects with edges;Hartmann forceps and wax loops forround objects; and Rosen and rightangle picks for soft foreign bodies andthose with holes. A Baron suction tip isvery useful to debride blood and to aidwith the extraction. After removal, it isusually wise to prescribe a topicalantibiotic-steroid mixture for anydrainage and to reduce the inflammation
created by the foreign body and theextraction procedure.
Cerebrospinal Fluid Otorrhea andPerilymphatic Fistula
Clear discharge from the ear is rarebut may suggest the presence of a leakof cerebrospinal fluid (CSF) or peri-lymph. These disorders result from aviolation of the normal bony contours ofthe ear due to trauma, congenital mal-formation, or erosive processes. In mostcases, patients complain of aural full-ness, and examination reveals fluid inthe ear canal that reaccumulates whenevacuated. Occasionally, such patientspresent with dizziness, hearing loss, orrecurrent bouts of meningitis.
Diagnosis of a CSF or perilymphleak is made by sampling the fluid andby imaging studies. A fluid sample witha glucose concentration of approximate-
Figure 3. The posterosuperior quadrant and pars flaccida are the most common locations for acquiredcholesteatoma.

848 PEDIATRIC ANNALS 33:12 | DECEMBER 2004
ly 60% of the serum value and a proteinconcentration of less than 200 mg/dL ismost likely CSF or perilymph. �2 trans-ferrin has also been described as a mark-er for perilymph;29,30 however, someinvestigators have questioned the relia-bility of this test.31,32 The location of aCSF leak may be established using com-puterized tomography with intrathecalcontrast or nuclear scans with intrathe-
cal radionuclides. CSF leaks may healspontaneously, or may require explo-ration through a variety of approaches,depending on the cause and location ofthe leak.
MICROBIOLOGY OF OTORRHEAWhile most pediatricians are familiar
with the conditions favoring infectionby otitis media organisms, the presenceof Pseudomonas in the ear is often lesswell understood. Pseudomonas is anaerobic, motile gram-negative rod com-monly found in moist environmentssuch as water, sewage, and soil. In theear, P. aeruginosa is rarely culturableunless there is infection present.33,34
Patients who develop otorrhea due toPseudomonas tend to retain moisture inthe ear canal due to stenosis or excessivecerumen, and the prevalence ofPseudomonas in the external canal isknown to increase with increasing waterexposure.33 Other sources of moisture inthe ear canal that may be associated withPseudomonas infection include humidair, perspiration from wearing tightly fit-ted hearing aid molds or hearing protec-
tors, and drainage from the middle eardue to otitis media. Trauma to the canalskin can also lead to Pseudomonasinfection, most likely due to interruptionof the protective layers of cerumen andskin and to local pH changes. Based onbiochemical and growth characteristics,strains isolated from patients with otitisexterna more closely resemble those ofPseudomonas in its natural water habitat
than those associated with other infec-tions in humans.35
In cases of tympanostomy tube otor-rhea, drainage is most often precipitatedby upper respiratory colonization orinfection by one of the usual otitis mediaorganisms (S. pneumoniae, H. influen-zae, or M. catarrhalis), particularly dur-ing the colder months of the year. How-ever, within hours to days, increasedmoisture in the ear canal allowsPseudomonas to multiply and becomethe predominant organism.10,36 Duringsummer months, otorrhea in the pres-ence of tubes often starts as aPseudomonas or Staphylococcus infec-tion resulting from contamination fromexternal sources.11,37 In about 10% ofcases, at least one organism from eachof these two groups may be isolated.37
Other organisms, including Staphylo-coccus epidermidis, Neisseria sp., diph-theroids, enterococcus, Proteus mira-bilis, and Enterobacter cloacae, havebeen demonstrated in more 60% ofcases.36,38 Anaerobes may also play arole in otorrhea, as suggested by onestudy in which these organisms were
cultured from 49% of cases.36 Chronicotorrhea may also result from oppor-tunistic infections by Aspergillus andCandida species.
In otitis externa, P. aeruginosa is themost common infecting organism(61%), although cultures from the earcanal often demonstrate a polymicro-bial infection (44%).39 Chronic orrecurrent external otitis may result fromfungal infections; from skin conditionssuch as eczema, seborrhea, or psoriasis;or from poor aural hygiene or trauma instenotic ear canals. In chronic suppura-tive otitis media (CSOM), the organ-isms are similar to those in otitis exter-na, with Pseudomonas being the mostcommon isolate (37% to 84%).40,41
However, most cultures (5% to 58%)demonstrate polymicrobial infections,including gram-negative bacilli, S.aureus, and anaerobes.22,23,25,40,41 Un-common causes of CSOM includetuberculosis and syphilis, as well asnoninfectious causes such as histiocyto-sis and rhabdomyosarcoma.
TREATMENT OF THE DRAINING EAR
The Initial VisitDebridement of the ear canal is
unquestionably the most critical step inthe diagnosis and management of otor-rhea. In the presence of significant canalswelling or otorrhea, determination ofthe cause of the drainage is not possible,and the treating physician may be uncer-tain whether to treat the patient for otitismedia or otitis externa. Furthermore,removal of the drainage is necessary sothat applied ototopical medication canreach the target pathology.
Before debridement, the ear canalmust be visualized adequately, to mini-mize canal wall trauma and optimizeexamination of the tympanic membrane.This is best accomplished using a head-light, which keeps the examiner’s handsfree for retraction of the auricle and
Debridement of the ear canal is unquestionably the most critical step in thediagnosis and management of otorrhea.

PEDIATRIC ANNALS 33:12 | DECEMBER 2004 849
instrumentation of the ear. Headlightsserve a similar role in examination ofthe nose and throat and are an invaluableaddition to any pediatric practice.
Debridement of the canal is per-formed using swabs or a small suctiondevice. Suction is generally quicker,more effective, and less traumatic to thecanal wall, but the noise may be fright-ening to some patients, and the neces-sary equipment is not available in mostpediatric practices. Cotton-tipped appli-cators, self-made cotton swabs, or smallcalcium alginate swabs, on the otherhand, clear the majority of the drainagewith less trauma to the canal walls.However, debridement using this tech-nique is often insufficient to afford anadequate view of the tympanic mem-brane. Irrigation of the canal with roomtemperature saline for this purposeshould be performed with extreme cau-tion due to the potential for vertigo fromcaloric stimulation, particularly inpatients with tubes or perforations.
Once the source of the otorrhea has
been established, topical antibiotic ther-apy is usually indicated. Selection of anappropriate ototopical and duration oftherapy is addressed later in this article.If adequate visualization of the ear canaland tympanic membrane are not possi-ble due to poor patient cooperation, atrial of ototopical medication is still rea-sonable prior to considering referral toan otolaryngologist. In the presence oftympanic membrane perforation or tym-panostomy tubes, oral antibiotics arerarely indicated; otorrhea concentrationsof antibiotics administered through theeardrum are 100 to 1,000 times greaterthan those achieved with systemic ther-apy and likely exceed the and likelyexceed the MIC90 (the minimum con-centration at which 90% of tested strainsare inhibited) for a longer time.42 Thetopical route also reduces the potentialfor alterations in bacterial flora at othersites and the likelihood of inducing bac-terial resistance. Parents should beinstructed to debride the ear with twist-ed tissue paper or cotton prior to admin-
istering drops and to let each drop settlethrough the canal before the next isgiven. Tragal pressure applied after-wards ensures that the medication reach-es the middle ear space.43
Figure 4. Otowicks may be used to expand theswollen ear canal and to keep the canal skin incontact with topically applied medications
TABLE.
Ototopic Antibiotic Preparations
Brand Name Antimicrobral Solvent/Antiseptic SteroidChloromycetin otic Chloramphenicol Propylene glycol None
Ciloxan ophthalmic solution Ciprofloxacin Benzalkonium chloride None
Cipro HC otic Ciprofloxacin Polyvinyl alcohol Hydrocortisone
Ciprodex otic Ciprofloxacin Polyvinyl alcohol Dexamethasone
Colymycin S otic Neomycin, polymyxin B Aqueous Hydrocortisone
Cortisporin otic solution Neomycin, polymyxin B Propylene glycol, HCl Hydrocortisone
Cortisporin otic suspension Neomycin, polymyxin B Propylene glycol, alcohol Hydrocortisone
Floxin otic Ofloxacin Benzalkonium chloride None
Lidex solution None Propylene glycol, alcohol Fluocinonide
Lotrimin solution Clotrimazole Polyethylene glycol None
Otocort suspension Neomycin, polymyxin B Propylene glycol, alcohol Hydrocortisone
Pediotic suspension Neomycin, polymyxin B Propylene glycol, alcohol Hydrocortisone
Tobradex ophthalmic solution Tobramycin Benzalkonium chloride Dexamethasone
Vosol HC solution None Acetic acid, propylene glycol Hydrocortisone

850 PEDIATRIC ANNALS 33:12 | DECEMBER 2004
When swelling obscures the tympan-ic membrane or pain is severe, place-ment of an expandable methylcelluloseotowick or sponge maximizes exposureof the canal walls to ototopical medica-tion and reduces drainage through thetube or perforation if one is present (Fig-ure 4, see page 849). After 2 to 4 days,the wick is removed and the drops maythen be delivered directly to the external
canal, as edema most likely will havesubsided. The swelling should be re-duced sufficiently within several days tocomplete the examination of the ear.Narcotic analgesics may be necessaryfor pain management during the firstfew days of treatment.
Ototopic therapyTreatments for otorrhea during the
past four centuries have included redlead, tree resin, frankincense, goosegrease, cream from cow’s milk, vermil-ion, cumin, ass ear, olive oil, and hatetoil.44 By the first half of the 20th century,medical science had evolved such thatastringents and antiseptics were the pre-ferred therapeutic modalities; for manyphysicians, these agents remain the treat-ment of choice.44 However, the advent ofantibiotics some 60 years ago brought ashift in therapy toward the use of ototopi-cal antibiotic preparations. Though thereare many ototopical medications avail-able for use, each has its own identity andindications (Table, see page 849).
The earliest ototopical antibioticpreparations included sulfathiazoleascorbate and sodium penicillin-sul-fathiazole.44 Chloramphenicol, strepto-mycin, erythromycin, and aminoglyco-sides later became available in a varietyof powders and solutions. In the 1960s,an ototopical containing neomycin (anaminoglycoside), polymyxin B (apolypeptide antibiotic), and hydrocorti-
sone emerged as the preferred therapyfor otorrhea. However, cases ofneomycin allergy began to appear, pre-senting as erythema and swelling of theauricle with peeling of the skin. In addi-tion, data from animal studies beginningin the late 1960s suggested all of thesemedications, as well as their carriers andsolvents, have inflammatory and ototox-ic potential.45-47 Toxic effects includedinner and outer hair cell destruction,squamous metaplasia and growth intothe middle ear, cholesteatoma, hearingloss, damage to the stria vascularis,adhesion formation, and mucosalinflammation.
Nevertheless, few reports in humansubjects subsequently confirmed theseeffects, perhaps owing to greater thick-ness of the human round window mem-brane, especially in the setting ofinflammation.48-52 As of the 1990s, com-bination preparations were still themost commonly used, although somephysicians continued off-label use ofophthalmic aminoglycoside medica-
tions.53,54 However, a 2004 consensuspanel of the American Academy of Oto-laryngology – Head and Neck Surgeryconcluded that “when possible, topicalantibiotic preparations free of potentialototoxicity should be used in preferenceto ototopical preparations that have thepotential for otologic injury if the mid-dle ear or mastoid are open,” and that “ifused, potentially ototoxic antibioticpreparation should be used only ininfected ears.”55
During the past decade, ototopicalpreparations containing fluoroquinoloneantibiotics have appeared on the market.Ofloxacin was the first such ototopicalavailable. Ciprofloxacin, which hadbeen used off-label in ophthalmic formfor several years, later became availablefor otic use in a combination preparationwith hydrocortisone and is now avail-able in combination with dexametha-sone. Only ciprofloxacin is availablewith steroid medication, which often isrequired to control granulation tissueinvolving the tympanic membrane andmiddle ear. Steroids also seem toimprove the efficacy of ciprofloxacin inthe treatment of acute otitis media andotorrhea through tympanostomy tubes.56
In studies of possible inner ear effects ofthese medications, neither ciprofloxacinnor ofloxacin has demonstrated ototoxicpotential.57-63
Both preparations are dosed twiceper day, compared with three times perday for the neomycin–polymyxinB–hydrocortisone combination. Howev-er, both are also more costly and may bedifficult to find on the formularies ofsome third-party payors.
Sensitivity studies of aural pathogenstreated topically must be interpretedwith caution, as traditional susceptibili-ty breakpoints are established only forsystemically administered medications.In studies of acute tympanostomy tubeotorrhea, ototopic agents demonstratedequal or greater clinical efficacy, superi-
Treatments for otorrhea during the pastfour centuries have included red lead, treeresin, frankincense, goose grease, cream,vermilion, cumin, olive oil, and hatet oil.

PEDIATRIC ANNALS 33:12 | DECEMBER 2004 851
or eradication of pathogens, and feweradverse effects when compared withoral antimicrobials.58,64 However,although both ofloxacin and cipro-floxacin–dexamethasone have FDAapproval for use in infections by “otitismedia” organisms, ciprofloxacin hasdemonstrated efficacy superior or equalto that of ofloxacin among isolates frompatients with chronic otitis and sinusi-tis,65 as well as among isolates of S.pneumoniae, H. influenzae, and M.catarrhalis from all sources.66-70 An invivo study of ototopical therapy inpatients with acute otitis media throughtympanostomy tubes also foundciprofloxacin–dexamethasone moreeffective than ofloxacin.71
Aural isolates of P. aeruginosa havedemonstrated little resistance to antibi-otics in common ototopical preparations.In vitro susceptibility rates for polymyx-in B, gentamicin, colistin, norfloxacin,ciprofloxacin, and ofloxacin in moststudies are greater than 95%,58,65,72-74
although one study found 13% resis-tance to ofloxacin.65 Both ofloxacinand ciprofloxacin have demonstratedhigh efficacy in vitro and in vivo in themanagement of otorrhea due to P.aeruginosa and S. aureus.57-59,64,72-76
However, recent literature suggests theemergence of strains of P. aeruginosathat are resistant to the fluoro-quinolones, as well as an increasingprevalence of methicillin-resistant S.aureus, which also may be fluoro-quinolone-resistant.77-80 Neo-mycin andchloramphenicol demonstrate poor effi-cacy, with susceptibility rates of just17.8% and 13.4%, respectively.72,73
Cases in which fungal elements areseen or yeast or fungus are identified byculture may be treated with topical anti-fungal agents such as clotrimazoledematologic solution.10 Such therapymay be administered in alternatingdoses with a topical antibiotic if a mixedinfection is present.
Granulation tissue is a commoncause of drainage from the ear and maybe found in about 15% of ears withtympanostomy tube otorrhea.81 Oto-topical antibiotics combined withsteroids are more effective at clearinggranulation tissue than are ototopicalantibiotics alone.81 A 7-day to 14-daycourse of medication is recommended;however, the ear should be reassessedfor residual granulation after therapy. Iftissue persists, additional medicationmay be useful. Alternatively, the oto-laryngologist may be able to salvagethe tube by removing the granulationpolyp in the office setting. When allother measures have failed, the tubeshould be removed or replaced.Steroid-containing ototopicals are alsouseful in the treatment of dermatologicconditions of the ear canal such aseczema; in such cases, solutions con-taining steroid only (ie, fluocinonide)also should be considered.
Systemic Antibiotic TherapySystemic therapy is rarely necessary
to treat otorrhea; most cases can be ade-quately treated with debridement andtopical therapy alone. In patients withsevere cellulitis possibly due to gram-positive organisms, and in those casesassociated with upper respiratory infec-tion of long duration in which bacterialetiology is likely, additional systemictherapy may be considered and shouldbe directed by cultures of the ear canal.Patients with refractory chronic suppu-rative otitis of more than 6 weeks’ dura-tion are also candidates for outpatient orinpatient parenteral therapy combinedwith daily aural toilet.
Pediatricians are quite familiar withthe oral and intravenous antimicrobialsindicated when otitis media organismsare identified. (See the article by Dr.Rosenfeld on page 833). In studiesinvestigating sensitivities of P. aerugi-nosa to common intravenous agents,
ceftazidime, piperacillin, and tobra-mycin had the best susceptibility pro-files for Pseudomonas; ticarcillin andgentamicin also were effective.73,82
Aural isolates of S. aureus are exquis-itely sensitive to ciprofloxacin, oflox-acin, and trimethoprim–sulfamethoxa-zole, less so to gentamicin and chloram-phenicol, and resistant to polymyxinB.65,73,74 When culture results are notavailable, agents such as azlocillin,mezlocillin and ticarcillin/ sulbactamprovide good coverage for both middleear and external ear pathogens. Systemicuse of cipro-floxacin may be consideredfor older children but at this timeremains unapproved for young childrendue to the theoretical risk of bone or car-tilage toxicity.83
Intravenous azlocillin, mezlocillin,and ticarcillin–clavulanic acid havedemonstrated efficacy in the treatmentof chronic suppurative otitis.22,23,25,27
Some investigators have recommendedcontinued oral antibiotics as prophylax-is following intravenous therapy; how-ever, Fliss et al.23 found no statisticallysignificant difference in recurrence ratewith the use of amoxicillin prophylaxis.
Follow-up for Draining EarsOnce the otorrhea has cleared, exam-
ination of the ear canal and tympanicmembrane should be completed.Retained tympanostomy tubes andeardrum perforations occasionallydevelop granulation tissue peripherallyor in the lumen that responds to topical-ly administered steroid-containing pre-parations if one was not chosen as initialtherapy. Tubes also may become occlud-ed with inspissated debris and mayrequire disimpaction manually or withhydrogen peroxide drops. When no tubeor perforation is appreciated and the his-tory does not suggest otitis externa, thepediatrician should examine theeardrum carefully for retraction pocketsor squamous debris suggestive of

852 PEDIATRIC ANNALS 33:12 | DECEMBER 2004
cholesteatoma. Timely otolaryngologicreferral should be made when otorrheais refractory to therapy or an etiologycannot be established.
SUMMARYThere are a variety of causes of otor-
rhea in children. The most importantfactor in reaching the proper diagnosisand providing relief of the problem isaural toilet. Once adequate debridementhas been performed, the diagnosis isusually clearer, and treatment with oto-topicals is significantly more effective.
Most cases of otorrhea are due toinfection or granulation tissue and canbe managed initially with appropriatelyselected ototopical medication, therebyavoiding the risks and side effects ofsystemic therapy and the need for refer-ral to a specialist. However, otorrhea inchildren that is refractory to medicaltherapy may be due to retained tympa-nostomy tubes or insidious pathologysuch as cholesteatoma or malignancy. Insuch cases, prompt referral to the oto-laryngologist can facilitate accuratediagnosis and successful management.
REFERENCES1. Ah-Tye C, Paradise JL, Colborn DK. Otor-
rhea in young children after tympanostomy-tube placement for persistent middle-ear effu-sion: prevalence, incidence, and duration.Pediatrics. 2001;107(6):1251-1258.
2. Rosenfeld RM. Surgical prevention of otitismedia. Vaccine. 2001;19(Suppl 1):S134-S139.
3. Balkany TH, Barkin RM, Suzuki BH, WatsonWJ. A prospective study of infection follow-ing tympanostomy and tube insertion. Am JOtol. 1983;4(4):288-291.
4. Kinsella JB, Fenton J, Donnelly MJ,McShane DP. Tympanostomy tubes and earlypost-operative otorrhea. Int J Pediatr Otorhi-nolaryngol. 1994;30(2):111-114.
5. Giebink GS, Daly K, Buran DJ, Satz M, AyreT. Predictors for postoperative otorrhea fol-lowing tympanostomy tube insertion. ArchOtolaryngol Head Neck Surg. 1992;118(5):491-494.
6. Scott BA, Strunk CL. Posttympanostomyotorrhea: the efficacy of canal preparation.Laryngoscope. 1992; 102(10):1003-1007.
7. Garcia P, Gates GA, Schechtman KB. Doestopical antibiotic prophylaxis reduce post-
tympanostomy tube otorrhea? Ann Otol Rhi-nol Laryngol. 1994;103(1):54-58.
8. Gross RD, Burgess LP, Holtel MR, et al.:Saline irrigation in the prevention of otorrheaafter tympanostomy tube placement. Laryn-goscope. 2000;110(2 pt 1):246-249.
9. Post JC. Direct evidence of bacterial biofilmsin otitis media. Laryngoscope. 2001;111(12):2083-2094.
10. Poole MD. Treatment of otorrhea associatedwith tubes or perforations. Ear Nose Throat J.1993;72(3):225-226.
11. Mandel EM, Casselbrant ML, Kurs-Lasky M.Acute otorrhea: bacteriology of a commoncomplication of tympanostomy tubes. AnnOtol Rhinol Laryngol. 1994;103(9):713-718.
12. Schneider ML. Bacteriology of otorrhea fromtympanostomy tubes. Arch Otolaryngol HeadNeck Surg. 1989;115(10):1225-1226.
13. Ruohola A, Heikkinen T, Meurman O, et al.Antibiotic treatment of acute otorrheathrough tympanostomy tube: randomizeddouble-blind placebo-controlled study withdaily follow-up. Pediatrics 2003; 111(5 pt1):1061-1067.
14. Roland PS. The formation and managementof middle ear granulation tissue in chronic eardisease. Ear Nose Throat J. 2004;83(1Suppl):5-8.
15. Salata JA, Derkay CS. Water precautions inchildren with tympanostomy tubes. Arch Oto-laryngol Head Neck Surg. 1996;122(3):276-280.
16. Jaffe BF. Are water and tympanostomy tubescompatible? Laryngoscope. 1981; 91(4):563-564.
17. Lounsbury BF. Swimming unprotected withlong-shafted middle ear ventilation tubes.Laryngoscope. 1985;95(3):340-343.
18. Becker GD, Eckberg TJ, Goldware RR.Swimming and tympanostomy tubes: aprospective study. Laryngoscope. 1987;97(6):740-741.
19. Marks MJ, Mills RP. Swimming and grom-mets. J R Soc Med 1983; 76(1):23-26.
20. Golz A, Ghersin T, Joachims HZ, et al. Pro-phylactic treatment after ventilation tubeinsertion: comparison of various methods.Otolaryngol Head Neck Surg. 1998;119(1):117-120.
21. Lee D, Youk A, Goldstein NA. A meta-analy-sis of swimming and water precautions.Laryngoscope. 1999;109(4):536-540.
22. Kenna MA, Bluestone CD, Reilly JS, LuskRP. Medical management of chronic suppura-tive otitis media without cholesteatoma inchildren. Laryngoscope. 1986;96(2):146-151.
23. Fliss DM, Dagan R, Houri Z, Lieberman A.Medical management of chronic suppurativeotitis media without cholesteatoma in chil-dren. J Pediatr. 1990;116(6):991-996.
24. Kimmelman CP. Office management of thedraining ear. Otol Clin N Am. 1992;25(4):739-744.
25. Dagan R, Fliss DM, Einhorn M, Kraus M,Leiberman A. Outpatient management ofchronic suppurative otitis media withoutcholesteatoma in children. Pediatr Infect DisJ. 1992;11(7):542-546.
26. Ma KH, Tang PS, Chan KW. Aural tuberculo-sis. Am J Otol. 1990;11(3):174-177.
27. Kenna MA, Rosane BA, Bluestone CD. Med-ical management of chronic suppurative otitismedia without cholesteatoma in children –update 1992. Am J Otol. 1993;14(5):469-473.
28. Golz A, Goldenberg D, Netzer A, et al.Cholesteatomas associated with ventilationtube insertion. Arch Otolaryngol Head NeckSurg. 1999;125(7):754-757.
29. Skedros DG, Cass SP, Hirsch BE, Kelly RH.Beta-2 transferrin assay in clinical manage-ment of cerebral spinal fluid and perilym-phatic fluid leaks. J Otolaryngol. 1993;22(5):341-344.
30. Weber PC, Kelly RH, Bluestone CD,Bassiouny M. Beta 2-transferrin confirmsperilymphatic fistula in children. OtolaryngolHead Neck Surg. 1994;110(4):381-385.
31. Levenson MJ, Desloge RB, Parisier SC. Beta-2 transferrin: Limitations of use as a clinicalmarker for perilymph. Laryngoscope. 1996;106(2 pt 1):159-161.
32. Buchman CA, Luxford WM, Hirsch BE,Fucci MJ, Kelly RH. Beta-2 transferrin assayin the identification of perilymph. Am J Otol.1999;20(2):174-178.
33. Salit IE, Miller B, Wigmore M, Smith JA.Bacterial flora of the external canal in diabet-ics and non-diabetics. Laryngoscope.1982;92(6 pt 1):672-673.
34. Stroman DW, Roland PS, Dohar J, Burt W.Microbiology of normal external auditorycanal. Laryngoscope. 2001;111(11 pt 1):2054-2059.
35. Sundstrom J, Jacobson K, Munck-Wikland E,Ringertz S. Pseudomonas aeruginosa in otitisexterna: a particular variety of the bacteria?Arch Otolaryngol Head Neck Surg.1996;122(8):833-836.
36. Brook I, Yocum P, Shah K. Aerobic andanaerobic bacteriology of otorrhea associatedwith tympanostomy tubes in children. ActaOtolaryngol. 1998;118(2):206-210.
37. Dohar J. Microbiology of otorrhea in childrenwith tympanostomy tubes: implications fortherapy. Int J Pediatr Otorhinolaryngol.2003;67(12):1317-1323.
38. Schneider ML. Bacteriology of otorrhea fromtympanostomy tubes. Arch Otolaryngol HeadNeck Surg. 1989;115(10):1225-1226.
39. Clark WB, Brook I, Bianki D, Thompson DH.Microbiology of otitis externa. OtolaryngolHead Neck Surg. 1997;116(1):23-25.
40. Fliss DM, Dagan R, Meidan N, Leiberman A.Aerobic bacteriology of chronic suppurativeotitis media without cholesteatoma in chil-dren. Ann Otol Rhinol Laryngol. 1992;101(10):866-869.

PEDIATRIC ANNALS 33:12 | DECEMBER 2004 853
41. Arguedas A, Loaiza C, Herrera JF, Mohs E.Antimicrobial therapy for children withchronic suppurative otitis media withoutcholesteatoma. Ped Infect Dis J. 1994;13(10):878-881.
42. Ohyama M, Furuta S, Ueno K, et al.Ofloxacin otic solution in patients with otitismedia: an analysis of drug concentrations.Arch Otolaryngol Head Neck Surg. 1999;125(3):337-340.
43. Hebert RL 2nd, Vick ML, King GE, Bent JP3rd. Tympanostomy tubes and otic suspen-sions: do they reach the middle ear space?Otolaryngol Head Neck Surg. 2000;122(3):330-3.
44. Myer CM 3rd. Historical perspective on theuse of otic antimicrobial agents. PediatrInfect Dis J. 2001;20(1):98-101.
45. Wright CG, Meyerhoff WL. Ototoxicity ofotic drops applied to the middle ear in thechinchilla. Am J Otolaryngol. 1984;5(3):166-176.
46. Wright CG, Meyerhoff WL, Burns DK. Mid-dle ear cholesteatoma: an animal model. Am JOtolaryngol. 1985;6(5):327-341.
47. Vernon J, Brummett R, Walsh T. The ototox-ic potential of propylene glycol in guineapigs. Arch Otolaryngol. 1978;104(12):726-729.
48. Pickett BP, Shinn JB, Smith MF. Ear dropototoxicity: Reality or myth? Am J Otol.1997;18(6):782-791.
49. Linder TE, Zwicky S, Brandle P. Ototoxicityof ear drops: a clinical perspective. Am J Otol.1995;16(5):653-657.
50. Podoshin L, Fradis M, Ben David J. Ototoxi-city of ear drops in patients suffering fromchronic otitis media. J Laryngol Otol.1989;103(1):46-50.
51. Roland PS. Clinical ototoxicity of topicalantibiotic drops. Otolaryngol Head NeckSurg. 1994;110(6):598-602.
52. Lundy LB, Graham MD. Ototoxicity and oto-topical medications: a survey of otolaryngol-ogists. Am J Otol. 1993;14(2):141-146.
53. Charnock DR. Early postoperative otorrheaafter tympanostomy tube placement: a com-parison of topical ophthalmic and otic drops.Ear Nose Throat J. 1997;76(12):870-871.
54. Hoffman RA, Goldofsky E. Topical ophthal-mologics in otology. Ear Nose Throat J.1991;70(4):205-210.
55. Roland PS, Stewart MG, Hannley M, et al.Consensus panel on role of potentially oto-toxic antibiotics for topical middle ear use:Introduction, methodology, and recommenda-tions. Otolaryngol Head Neck Surg.2004;130(3 Suppl):S51-S56
56. Roland PS, Anon JB, Moe RD, et al. Topicalciprofloxacin/dexamethasone is superior tociprofloxacin alone in pediatric patients withacute otitis media and otorrhea through tym-panostomy tubes. Laryngoscope. 2003;
113(12):2116-122. 57. Simpson KL, Markham A. Ofloxacin otic solu-
tion: A review of its use in the management ofear infections. Drugs. 1999;58(3): 509-531.
58. Goldblatt EL, Dohar J, Nozza, et al. Topicalofloxacin versus systemic amoxicillin/clavu-lanate in purulent otorrhea in children withtympanostomy tubes. Int J Pediatr Otorhino-laryngol. 1998;46(1-2):91-101.
59. Tong MC, Woo JK, van Hasselt CA. A dou-ble-blind comparative study of ofloxacin oticdrops versus neomycin-polymyxin B-hydro-cortisone otic drops in the medical manage-ment of chronic suppurative otitis media. JLaryngol Otol. 1996;110(4):309-314.
60. Brownlee RE, Hulka GF, Prazma J, PillsburyHC 3rd. Ciprofloxacin: use as a topical oticpreparation. Arch Otolaryngol Head NeckSurg. 1992;118(4):392-396.
61. Barlow DW, Duckert LG, Kreig S, Gates GA.Ototoxicity of topical otomicrobial agents.Acta Otolaryngol. 1995;115(2):231-235.
62. Claes J, Govaerts PJ, Van de Heyning PH,Peeters S. Lack of ciprofloxacin ototoxicityafter repeated ototopical application. Antimi-crob Agents Chemother. 1991;35(5):1014-1016.
63. Dohar JE, Alper CM, Rose EA, et al. Treat-ment of chronic suppurative otitis media withtopical ciprofloxacin. Ann Otol Rhinol Laryn-gol. 1998;107(10 pt 1):865-871.
64. Klein JO. In vitro and in vivo antimicrobialactivity of topical ofloxacin and other oto-topical agents. Pediatr Infect Dis J.2001;20(1):102-103.
65. Gaillot O, Berche P. In vitro susceptibility tociprofloxacin of bacterial strains isolatedfrom chronic otitis media and chronic sinusi-tis. Drugs 1995;49(suppl 2):200-202.
66. Jacobs MR, Bajaksouzian S, Zilles A, et al.Susceptibilities of Streptococcus pneumoniaeand Haemophilus influenzae to 10 oralantimicrobial agents based on pharmacody-namic parameters: 1997 U.S. surveillancestudy. Antimicrob Agents Chemother.1999;43(8):1901-1908.
67. Thornsberry C, Ogilvie PT, Holley HP, SahmDF. Survey of Streptococcus pneumoniae,Haemophilus influenzae, and Moraxellacatarrhalis isolates to 26 antimicrobial agents:a prospective U.S. study. Antimicrob AgentsChemother. 1999;43(11):2612-2623.
68. Fremaux A, Sissia G, Geslin P. In-vitro bacte-riostatic activity of levofloxacin and threeother fluoroquinolones against penicillin-sus-ceptible and penicillin-resistant Streptococ-cus pneumoniae. J Antimicrob Chemother.1999; 43(Suppl C):9-14.
69. Thomson KS, Chartrand SA, Sanders CC,Block SL. In-vitro activity of levofloxacinagainst Streptococcus pneumoniae with vari-ous levels of penicillin resistance. J Antimi-crob Chemother. 1999;43(Suppl C):15-19.
70. Kitzis MD, Goldstein FW, Miegi M, Acar JF.In-vitro activity of levofloxacin, a new fluoro-quinolone: evaluation against Haemophilusinfluenzae and Moraxella catarrhalis. JAntimicrob Chemother. 1999;43(Suppl C):21-26.
71. Roland PS, Kreisler LS, Reese B, et al. Topi-cal ciprofloxacin/dexamethasone otic suspen-sion is superior to ofloxacin otic solution inthe treatment of children with acute otitismedia with otorrhea through tympanostomytubes. Pediatrics. 2004;113(1 pt 1):e40-e46.
72. Dohar JE, Kenna MA, Wadowsky RM. Invitro susceptibility of aural isolates ofPseudomonas aeruginosa to commonly usedototopical antibiotics. Am J Otol. 1996;17(2):207-209.
73. Indudharan R, Haq JA, Aiyar S. Antibiotics inchronic suppurative otitis media: a bacterio-logic study. Ann Otol Rhinol Laryngol.1999;108(5):440-444.
74. Dohar JE, Garner ET, Nielsen RW, Biel MA,Seidlin M. Topical ofloxacin treatment ofotorrhea in children with tympanostomytubes. Arch Otolaryngol Head Neck Surg.1999;125(5):537-545.
75. Zipfel TE, Wood WE, Street DF, et al. Theeffect of topical ciprofloxacin on postopera-tive otorrhea after tympanostomy tube inser-tion. Am J Otol. 1999;20(4):416-420.
76. Wintermeyer SM, Hart MC, Nahata MC.Efficacy of ototopical ciprofloxacin inpatients with otorrhea. Otolaryngol HeadNeck Surg. 1997;116(4):450-453.
77. Matsumoto Y, Suzuki Y, Ishii Y, et al. Antimi-crobial activity of ofloxacin against recentclinical isolates from otitis media and otitisexterna. Jpn J Antibiot. 1998;51(9):561-575.
78. Jang CH, Park SY. Emergence ofciprofloxacin-resistant pseudomonas inchronic suppurative otitis media. Clin Oto-laryngol. 2004;29(4):321-323.
79. Hwang JH, Tsai HY, Liu TC. Community-acquired methicillin-resistant Staphylococcusaureus infections in discharging ears. ActaOtolaryngol. 2002;122(8):827-830.
80. Hwang JH, Chu CK, Liu TC. Changes in bac-teriology of discharging ears. J LaryngolOtol. 2002;116(9):686-689.
81. Roland PS, Dohar JE, Lanier BJ, et al. Topi-cal ciprofloxacin/dexamethasone otic suspen-sion is superior to ofloxacin otic solution inthe treatment of granulation tissue in childrenwith acute otitis media with otorrhea throughtympanostomy tubes. Otolaryngol Head NeckSurg. 2004;130(6):736-741.
82. Dohar JE, Kenna MA, Wadowsky RM. Ther-apeutic implications in the treatment of auralPseudomonas infections based on in vitrosusceptibility patterns. Arch OtolaryngolHead Neck Surg. 1995;121(9):1022-1025.
83. Package information. Cipro® (ciprofloxacin).West Haven, CT; Miles, Inc.; 1993.