Module 9 Mobility

of 174
-
Upload
aura-palacios -
Category
Documents
-
view
236 -
download
0
Transcript of Module 9 Mobility
-
7/27/2019 Module 9 Mobility
1/174
9. Mobility and the Lower Extremity pg. 1 of 174www.ebrsr.com
9. Mobility and the Lower ExtremityNorine Foley MSc, Shelialah Pereira MSc, PT, Robert Teasell MD, Sanjit Bhogal MSc.
Key Points
The restorative (Bobath) approach is associated with similar gains infunction, but longer lengths of hospital stay, compared with other
therapeutic approaches.
Augmented physical therapy may improve gait post-stroke, although
the results are not maintained over time.
Task-specific gait training improves gait post-stroke.
Virtual reality devices may enhance gait performance.
Balance training, using specific devices or exercises, post stroke is
beneficial.
Rhythmic sensory auditory stimulation improves gait post-stroke.
Robotic devices may not offer additional benefit compared with
conventional therapy.
It is uncertain whether partial body weight support and treadmill
training results in improved gait training.
Strength training is beneficial for hemiparetic stroke patients.
Cardiovascular training improves physical fitness post stroke.
Encouraging self-propelling a wheelchair by hemiplegic stroke
patients does not have an impact on functional outcomes.
The use of canes is associated with improved mobility post stroke.
Electrical stimulation combined with gait training improves hemiplegic
gait. EMG/Biofeedback treatment improves gait retraining.
Ankle foot orthoses appear to improve gait, particularly in association
with posterior tibial nerve deinnervation.
A variety of drugs may help to improve functional outcome following
stroke including levadopa, Selegiline, L-threo-3,4-
The Evidence-BasedReview of Stroke
Rehabilitation (EBRSR
reviews currentpractices in stroke
rehabilitation.
Contacts:
Dr. Robert Teasell
801 CommissionersRoad East
London, Ontario,
Canada
N6C 5J1
Phone:519.685.4000
Web:www.ebrsr.com
Email:
Robert.teasell@sjhc.
ndon.on.ca
-
7/27/2019 Module 9 Mobility
2/174
9. Mobility and the Lower Extremity pg. 2 of 174www.ebrsr.com
dihydroxyphenylserine (L-DOPS), Almitrine + Raubasine , Citicoline
and Citalopram.
It is unclear whether amphetamines and levadopa improve motor
recovery and/or functional outcome.
A tilt table or night splint can prevent ankle contracture early poststroke.
Electrical stimulation and therapeutic ultrasound can reduce ankle
plantarflexion spasticity.
Treatment with Botulinum toxin reduces lower-limb spasticity, but
has not convincingly been shown to improve function.
Oral pharmacological agents can be effectively used in the
management of spasticity, although some are associated withsignificant side effects.
Intrathecal Baclofen can reduce spasticity in chronic stroke.
Last updated October 2012,
We gratefully acknowledge the contribution of Dr. Lucie Brosseau
and Dr. Janice Eng
-
7/27/2019 Module 9 Mobility
3/174
9. Mobility and the Lower Extremity pg. 3 of 174www.ebrsr.com
Table of Contents9.1 Approaches to Therapy ............................................................................. 4
9.1.1 The Compensatory Approach.................................................................. 49.1.2 The Restorative Approach ..................................................................... 4
9.2 Intensity of Training ............................................................................... 129.3 Balance Retraining and Falls Prevention ..................................................... 18
9.3.1 Balance Retraining ............................................................................ 189.3.2 Falls Prevention................................................................................ 30
9.4 Gait Retraining ...................................................................................... 329.4.1 Repetitive Task Training...................................................................... 329.4.2 Treadmill Training ............................................................................. 409.4.3 Treadmill Training with Body Weight Support ............................................. 469.4.4 Virtual Reality Training........................................................................ 559.4.5 Feedback ....................................................................................... 579.4.6 EMG / Biofeedback............................................................................ 639.4.7 Bilateral Leg Training ......................................................................... 669.4.8 Mental Practice ................................................................................ 67
9.5 Strength Training ................................................................................... 689.5.1 Weakness Post-Stroke....................................................................... 689.5.2 Relationship Between Strength and Functional Activities Post Stroke................ 699.5.3 Strength Training
.......................................................................................................... 699.6 Cardiovascular Conditioning and Aerobic Exercises ..................................... 779.7 Assistive Devices for the Lower Extremity ................................................... 87
9.7.1 Wheelchair...................................................................................... 879.7.2 Canes ........................................................................................... 889.7.3 Ankle Foot Orthoses .......................................................................... 909.7.4 Electromechanical-assisted Training Devices ............................................. 94
9.8 Electrical Stimulation ........................................................................... 1029.8.1 Transcutaneous Electrical Nerve Stimulation (TENS).................................. 1029.8.2 Functional Electrical Stimulation .......................................................... 105
9.9 Medications Used in Motor Recovery Following Stroke ................................ 1159.9.1 Noradrenergic Agents....................................................................... 1159.9.2 Dopaminergic Agents ....................................................................... 1229.9.3 Serotonergic Agents ........................................................................ 1239.9.4 Other Drugs .................................................................................. 1259.9.5 A Summary of the Drugs Used in the Motor Recovery Following Stroke............ 128
9.9 Spasticity and Contractures in Lower Extremities ....................................... 1289.9.1 The Prevention of Contracture............................................................. 1289.9.2 Injection of Botulinum Toxin (BTx) ........................................................ 1299.9.3 Nerve Blocking in the Lower Extremity ................................................... 1369.9.4 Antispastic Medications Post Stroke ...................................................... 1389.9.5 Intrathecal Drug Therapy for Post Stroke Spasticity.................................... 1409.9.6 Electrical Stimulation for Post Stroke Spasticity......................................... 1429.9.7 Therapeutic Ultrasound for Post Stroke Spasticity ..................................... 1459.9.8 Physical Therapy to Reduce Spasticity................................................... 146
9.10 Summary .......................................................................................... 148References.............................................................................................. 151
-
7/27/2019 Module 9 Mobility
4/174
9. Mobility and the Lower Extremity pg. 4 of 174www.ebrsr.com
9. The Lower Extremity
9.1 Approaches to Therapy
There are two basic approaches torehabilitating sensorimotor disordersin spastic hemiplegia or hemiparesiswith or without sensory or perceptualdisorders. These two approaches are:(1) the compensatory or (2) therestorative approach also referred tothe remediation approach. Althoughnot exclusive of each other, they doreflect differing philosophies.
9.1.1 The Compensatory Approach
The goal of the compensatoryapproach towards treatment is notnecessarily on improving motorrecovery or reducing impairments butrather on teaching patients a newskill, even if it only involvespragmatically using the non-involvedside (Gresham et al. 1995). The aimis to teach an adaptive approach,one-handed if necessary, with a
focus on improving activities ofdaily living. Furthermore,Gresham et al. (1995) noted thatthere is a paucity of evidenceindicating whether such anapproach is effective. There isanecdotal evidence that thecompensatory approach maysuppress neurological recovery(Bobath 1978, 1980), a conceptsupported by evidence that theforced-use approach can enhance
motor control in selected patients(Taub et al. 1993, Wolf et al.1989).
9.1.2 The Restorative Approach
The restorative approach focuses ontraditional physical therapy exercisesand neuromuscular facilitation, whichinvolves sensorimotor stimulation,
exercises and resistance training,designed to enhance motor recoveryand maximize brain recovery of theneurological impairment (Gresham etal. 1995). Research utilizing newtechnology such as functional MRI hascertainly demonstrated the potentialof the central nervous system to atleast partially recover in response tospecific training and stimulation.
There are several restorative
approaches used in strokerehabilitation. The key ones are listedbelow (Table 9.1). Although each onehas its own proponents, unfortunately,there is little evidence that suggestsany one of these approaches issuperior to another (Ashburn et al.1993, Ernst 1990, Partridge &Deweedt 1995, Duncan 1997,
Table 9.1 Restorative Techniques of Stroke Rehab
(adapted from Zorowitz 1999)
Author/Type Theory
Bobath (NDT) Suppress synergistic movementFacilitate normal movement
Knott, Voss (PNF) Suppress normal movementFacilitate defined massmovement
Brunnstrom Facilitate synergistic movement
Rood Modify movement withcutaneous sensory stimulation
Forced-Use Overcome learned non-use
Motor Learning Active practice of context-specificmotor tasks with feedback
-
7/27/2019 Module 9 Mobility
5/174
9. Mobility and the Lower Extremity pg. 5 of 174www.ebrsr.com
Pomerory & Tallis 2000a, Van Peppenet al. 2003). A Cochrane review(Pollack et al. 1999) also concludedthat there was insufficient evidencethat one therapy approach wassuperior to another. Eleven trials were
included in the analysis, whichevaluated both the neurophysiologicalapproach and the motor learningapproach. The authors identifiedseveral potential factors, which mayhave contributed to the null findings:i) an inability to identify all relevanttrials due to lack of consistentterminology, ii) The poormethodological quality of many of the11 trials, iii) the heterogeneity ofinterventions, outcome assessments
and patient characteristics, and iv)poor descriptions and classification ofthe interventions provided.
A recent review authored by Paci(2003) evaluated 15 trials, which hadassessed the effectiveness of theBobath approach and concluded thatthere was insufficient evidence thatthis approach was superior to others.Paci also noted that the
methodological shortcomings of thestudies included in the review do notallow for a conclusion of non-efficacy.
A Cochrane review authored byPollock et al. (2007) examining theefficacy of various treatmentapproaches for lower limbrehabilitation also concluded thatusing a mix of components from
different therapy approaches is moreeffective than no treatment or placebocontrol, and that no one therapyapproach is superior to another.
Most recently, Kollen et al. (2009)conducted a systematic reviewevaluating the Bobath approachcompared with other therapyapproaches in terms of sensorimotorcontrol of upper and lower limb,dexterity, mobility, activities of daily
living, health-related quality of life,and cost-effectiveness using data from16 RCTs. Only limited evidence wasfound for balance control in favor ofBobath. The authors concluded thatoverall, the Bobath Concept is notsuperior to other approaches. Basedon best evidence synthesis, noevidence is available for thesuperiority of any approach. Theauthors also noted the methodological
shortcomings of many of the studiesreviewed.
Table 9.2 Bobath vs. Other Approaches
Author , YearCountry
PEDro Score
Methods Outcomes
Richards et al.1993Canada6 (Single-blind
RCT)
27 patients randomized to receive one of threetherapies: 1) Early intensive therapyincorporating the use of a tilt table, resistedexercises and treadmill, beginning ~8 days
post stroke, for 1.7 hrs/day x 5 weeks(experimental); 2) Early conventional therapyincluded traditional approach with therapybeginning ~9 days post stroke, for 1.8 hrs/dayx 5 wks (control 1); or 3) Conventionaltherapy beginning 13 days post stroke, 0.72hrs x 5 wks (control 2).
At week 6, gait speed in the 2 controlgroups was similar and lower than theexperimental group. By months 3 and 6,the gait speed between all groups was
similar.
Gelber et al.1995
20 patients with pure motor hemiparesisfollowing a stroke within the previous month
There were no significant differencesbetween the groups at any of the testing
-
7/27/2019 Module 9 Mobility
6/174
9. Mobility and the Lower Extremity pg. 6 of 174www.ebrsr.com
USA5 (RCT)
were randomized to neurodevelopmentaltechnique (NDT) (Bobath) or traditionalfunctional retraining (TRF) treatmentapproaches for the period of inpatientrehabilitation. FIM, gait velocity and stridelength were evaluated at admission, discharge,6 and 12 months.
intervals, other than a difference in gaitvelocity at discharge, which favoured theNDT approach. Length of hospital staywas similar for both groups.
Wagenaar etal. 1990NetherlandsNo Score
7 patients alternated between 2 therapyapproaches 5-9 days post stroke: 1)Brunnstrom approach and 2) Bobath (Neuro-developmental treatment-NDT). Therapieswere provided for 30 min/session for 21weeks. Starting order was randomized. BarthelIndex and gait parameters were assessed.
The only significant difference foundbetween the groups at the end of thetreatment period was for comfortablewalking speed (favouring the Brunnstrommethod).
Patel et al.1998UKNo Score
184 stroke patients with moderate disabilityreceived treatment on a rehabilitation unit thatwas either impairment focused (andtheoretically driven) or disability focused,aimed at restoration of normal function
(Bobath).
Both one week and discharge BarthelIndex scores were similar between thetwo groups. LOS was shorter for patientswho received treatment on the disability-focused rehabilitation unit, 53.7 vs. 72.3
days.Langhammeret al. 2000,2003Norway8 (RCT)
A double blind trial of 61 stroke patientsrandomized to receive therapy based onBobath concept (represents a theoreticalframework in a reflex-hierarchical theory) or toreceive a Motor Relearning Programme (basedon system theory and task oriented) (MRP). Allpatients received physiotherapy 5 days weeklywith a minimum of 40 minutes duration aslong as they were hospitalized and the samecomprehensive multidisciplinary treatment forstroke patients from doctors, nurses,occupational therapist and speech therapist
according to recommendation for stroke unitsin Norway.
Length of stay was significantly shorter inMRP group compared to Bobath group, 21vs. 34 days.
Mudie et al.2002Australia8 (RCT)
40 patients with recent stroke and who borethe majority of their weight consistently to oneside while sitting were randomized to one of 4groups: task specific reach, Bobath method,balance performance monitor (BPM) feedbacktraining and control. Patients were measuredon weight distribution measurements usingBPM daily before treatment session, 2 weeksafter cessation of treatment and 12 weekspost-study.
Bobath method was most effective forretraining sitting symmetry after stroke inthe short term. The BPM and the non-training control group also demonstratedsignificant improvement. After 12 weeks83% of BMP group, 38% of task-specificgroup, 29% of Bobath group and 0% ofcontrols were found to be distributingweight to both sides.
Pollock et al.2002UK5 (RCT)
Inpatients with diagnosis of stroke, havingachieved one minute of independent sittingbalance but not yet achieved 10 independentsteps, were randomized to a four-week regimeof independent practice aimed at improvingaspects of balance, (motor learning) inaddition to standard physiotherapy treatmentbased on the Bobath Approach (n=9) or toroutine care using the Bobath approach
Nineteen subjects were randomized to thecontrol group; nine to the interventiongroup. There were no clinically significantdifferences in measured outcomebetween the groups.
-
7/27/2019 Module 9 Mobility
7/174
9. Mobility and the Lower Extremity pg. 7 of 174www.ebrsr.com
(n=19). Treatment was provided 5 days/weekfor 4 weeks. Proportion of patients achieving'normal' symmetry of weight distributionduring sitting, standing, rising to stand, sittingdown, and reaching were assessed.
Van Vliet et al.2005
UK7 (RCT)
120 patients admitted to a strokerehabilitation ward were randomized to two
rehabilitation approaches Bobath based (BB)or movement science based (MSB). RivermeadMotor Assessment (RMA) and MotorAssessment Scale (MAS) scores were assessedat 1,3 and 6 months.
There were no significant differencesbetween the two groups. Scores on the
subsections of both RAM and MASassociated with lower extremity functionwere similar.
Wang et al.2005Taiwan7 (RCT)
21 patients with hemiplegia and spasticity and23 patients with partial recovery wererandomized to 20 sessions of physical therapyin four weeks, using either a Bobath ororthopaedic approach. Assessments wereconducted before and after treatment andincluded Stroke Impairment Assessment Set
(SIAS), Motor Assessment Scale (MAS), BergBalance Scale (BBS) and Stroke Impact Scale(SIS).
Patients with spasticity showed greaterimprovement in SIAS (tone control), MASscores and SIS scores using the Bobathapproach compared to the orthopaedicapproach. Patients with partial recoveryusing the Bobath approach had higherchange scores on MAS, BBS and SIS
scores.
Hafsteinsdottiret al. 2005TheNetherlandsNo Score
A controlled, multi-site cluster trial. 225patients in 6 hospitals received rehabilitationon units using the NDT approach and 101patients on 6 wards received rehabilitation onunits using a conventional (non-NDT)approach. The primary outcome was a pooroutcome (Barthel Index scores < 12 or death)at one-year. Quality of life (QoL) was alsoassessed.
There were no differences in theproportion of patients experiencing a pooroutcome. The adjusted odds ratioassociated with the NDT approach was1.7 (0.8, 3.5). There were no differencesin median QoL scores between the groupsat 12 months.
Lennon et al.2006UKNo Score
9 stroke patients received additional outpatienttherapy, based on the Bobath system,following inpatient rehabilitation. The followingoutcomes were assessed at the beginning andend of, outpatient therapy: Motor AssessmentScale (MAS), Sodring Motor Evaluation Scale(SMAS), Modified Ashworth Scale, the steptest, 10 m walk test, the Barthel Index (BI)and London Handicap Score (LHS). Gaitkinematics and kinetics were also assessed.
In terms of gait kinematics/kinetics, therewas improvement in only 2 parameterspeak dorsiflexion and hip flexormovement. There were improvements inall of the other outcomes with theexception of Modified Ashworth scoresand LHS.
Brock et al.2011Australia
7 (RCT)
26 patients who were able to walk withsupervision indoors and from 4-20 weeks poststroke were randomized to receive 6x 1 hour
physical therapy sessions over a two-weekperiod using structured task practice or theBobath approach in addition to task practice.The primary outcome was a modification of thesix-minute walk test.
There was no significant difference inimprovement between the two groups atthe end of the intervention (TP: 102.6 to
192.5 vs.TP+Bobath: 78.5 to 119.5 m,p=0.07). However, patients in theTP+Bobath group significantly increasedtheir walking speed (26.2 vs. 9.9 m/min,p=0.01). There were no significantdifferences on Berg Balance Scoresbetween groups (47 vs. 47).
-
7/27/2019 Module 9 Mobility
8/174
9. Mobility and the Lower Extremity pg. 8 of 174www.ebrsr.com
Table 9.3 Summary of RCTs Evaluating the Bobath Therapy Approach (Arranged inDescending order of Methodological Quality)
AuthorPEDro Score
N Intervention Main Outcome(s)Result
Langhammer andStanghelle 2000,20038 (RCT)
61 Motor RelearningProgramme (MRP) vs.
Bobath
Hospital stays (+ Bobath)Motor Assessment Scale
(+ MRP)(- at 1 and 4 yrs F/U)
Sodring Motor Evaluation Scale (+ MRP)(- at 1 and 4 yrs F/U)Life Quality Test (-)
Mudie et al. 20028 (RCT)
40 task specific reach vs.Bobath vs. Balance
Performance Monitor (BPM)feedback training) vs. no
specific treatment
Sitting balance (+ Bobath, short-term)Sitting balance (- long term)
Brock et al. 20117 (RCT)
26 task practice vs. Bobath +addition of task practice.
Six-minute walk test (-)
Van Vliet et al. 20057 (RCT)
120 Motor RelearningProgramme (MRP) vs.
Bobath
Rivermead Motor Assessment(-)
Motor Assessment Scale (-)
Wang et al. 20057 (RCT)
21 Bobath vs. orthopedicapproach
Motor Assessment Scale(+ Bobath)
Stroke Impact Scale(+ Bobath)
Richards et al 19936 (RCT)
27 Bobath vs. Mixed vs.Conventional
Balance (-)Gait velocity (-)
Gelber et al. 19955 (RCT)
20 Bobath vs. Traditionaltechniques
FIM (-)LOS (-)
Pollock et al. 20025 (RCT)
28 Bobath vs. mixedtechniques
Proportion of patients achieving 'normal'symmetry of weight distribution during
various tasks (-)
Table 9.4 Motor Learning Approach vs. Other Approaches
Author , YearCountry
PEDro Score
Methods Outcomes
Dean et al.1997Australia7 (RCT)
20 patients at least 1 year after stroke wererandomized into an experimental or controlgroup providing 10 treatment sessions over 2weeks. The experimental group participated ina standardized training program involvingpractice of reaching beyond arm's length(motor learning approach). The control groupreceived sham training involving completion ofcognitive-manipulative tasks within arm'slength. Performance of reaching in sitting wasmeasured before and after training usingelectromyography, videotaping, and two force
After training, experimental subjects wereable to reach faster and further, increaseload through the affected foot, andincrease activation of affected leg musclescompared with the control group. Neithergroup improved in walking.
-
7/27/2019 Module 9 Mobility
9/174
9. Mobility and the Lower Extremity pg. 9 of 174www.ebrsr.com
plates. Variables tested were movement time,distance reached, vertical ground reactionforces through the feet, and muscle activity.Subjects were also tested on sit-to-stand,walking, and cognitive tasks.
Dean et al.2000
Canada5 (RCT)
12 chronic stroke subjects were randomlyassigned to the experimental or the control
group. Both experimental and control groupsparticipated in exercise classes three times aweek for 4 weeks. The exercise class for theexperimental group focused on strengtheningthe affected lower limb and practicingfunctional tasks involving the lower limbs(motor learning approach), while the controlgroup practiced upper-limb tasks. Lower-limbfunction was evaluated by measuring walkingspeed and endurance, peak vertical groundreaction force through the affected foot duringsit-to-stand, and the step test. Patients were
evaluated pre-test, post test and at 2 monthsfollow up.
At 2 months, the experimental group hadincreased the distance walked in 6
minutes significantly greater compared tothe control group. There were alsosignificantly greater improvementsfavouring the experimental group inwalking speed, the step test and the sit-to-stand test.
Langhammeret al. 2000,2003Norway8 (RCT)
A double blind trial of 61 stroke patientsrandomized to receive therapy based onBobath concept (represents a theoreticalframework in a reflex-hierarchical theory) or toreceive a Motor Relearning Programme (basedon system theory and task oriented) (MRP). Allpatients received physiotherapy 5 days weeklywith a minimum of 40 minutes duration aslong as they were hospitalized and the samecomprehensive multidisciplinary treatment forstroke patients from doctors, nurses,
occupational therapist and speech therapistaccording to recommendation for stroke unitsin Norway.
Length of stay was significantly shorter inMRP group compared to Bobath group, 21vs. 34 days.
Van Vliet et al.2005UK7 (RCT)
120 patients admitted to a strokerehabilitation ward were randomized to tworehabilitation approaches Bobath based (BB)or movement science base (MSB). RivermeadMotor Assessment (RMA) and MotorAssessment Scale (MAS) scores were assessedat 1,3 and 6 months.
There were no significant differencesbetween the two groups. Scores on thesubsections of both RAM and MASassociated with lower extremity functionwere similar.
Chan et al.2006
Hong Kong7 (RCT)
52 stroke outpatients (
-
7/27/2019 Module 9 Mobility
10/174
9. Mobility and the Lower Extremity pg. 10 of 174www.ebrsr.com
Table 9.5 Summary of RCTs Evaluating the Motor Learning Therapy Approach (Arrangedin Descending Order of Methodological Quality)
AuthorPEDro Score
N Intervention Main Outcome(s)Result
Langhammer and
Stanghelle 2000,20038 (RCT)
61 Motor Relearning
Programme (MRP) vs.Bobath
Hospital stays (+ Bobath)
Motor Assessment Scale(+ MRP)(- at 1 and 4 yrs F/U)
Sodring Motor Evaluation Scale (+ MRP)(- at 1 and 4 yrs F/U)Life Quality Test (-)
Salbach et al. 20048 (RCT)
91 Motor relearning (lower) vs.motor learning upper
extremity-control)
Gait velocity (-)
Van Vliet et al. 20057 (RCT)
120 Motor RelearningProgramme (MRP) vs.
Bobath
Rivermead Motor Assessment(-)
Motor Assessment Scale (-)
Chan et al. 2004Hong Kong7 (RCT)
52 Motor Relearning vs.conventional therapy
Berg Balance Scale (+)Timed Up & Go Test (-)
FIM-motor (+)Modified Lawson Instrumental Activities of
Daily Living Test (+) Community IntegrationQuestionnaire (+)
Dean et al. 19977 (RCT)
20 Motor relearning vs. placebo Improved reach (+ MR)
Dean et al. 20005 (RCT)
12 Motor relearning vs. placebo Measures of gait (+ MR)
Table 9.6 Mixed Approach vs. Other
Author , YearCountry
PEDro Score
Methods Outcomes
Stern et al.1970USA4 (RCT)
62 hemiplegic stroke rehabilitation in-patientswere randomized to receive either a specialtherapeutic exercise program given 5days/week during hospitalization or a passiveexercise program.
There were no significant changes frominitial scores to discharge between thetwo groups in Motility Index, torquedynamometry measurements of kneeflexors/extensors or Kenny Institute ofRehabilitation ADL scale.
Pollock et al.2002UK5 (RCT)
Inpatients with diagnosis of stroke, havingachieved one minute of independent sittingbalance but not yet achieved 10 independentsteps, were randomized to a four-week regimeof independent practice aimed at improvingaspects of balance, (motor learning) inaddition to standard physiotherapy treatmentbased on the Bobath Approach (n=9) or toroutine care using the Bobath approach(n=19). Treatment was provided 5 days/weekfor 4 weeks. Proportion of patients achieving'normal' symmetry of weight distribution
Nineteen subjects were randomized to thecontrol group; nine to the interventiongroup. There were no clinically significantdifferences in measured outcomebetween the groups.
-
7/27/2019 Module 9 Mobility
11/174
9. Mobility and the Lower Extremity pg. 11 of 174www.ebrsr.com
during sitting, standing, rising to stand, sittingdown, and reaching were assessed.
Table 9.7 Summary of RCTs Evaluating a Mixed Approach
Author
PEDro Score
N Intervention Main Outcome(s)
ResultPollock et al. 20025 (RCT)
28 Bobath vs. mixedtechniques
Proportion of patients achieving 'normal'symmetry of weight distribution during
various tasks (-)
Stern et al. 19704 (RCT)
62 Mixed vs.neurophysiological
ADL (-)
Discussion
The evidence for the restorativeapproach is almost exclusivelyempirical and evidence supporting its
usage is limited. Miller et al. (1998)noted that although there is evidenceto demonstrate a short-term benefit offacilitation techniques, part of therestorative approach, there is a lack ofevidence that would suggestfunctional clinical outcomes areimproved. Two recent studies,Langhammer and Stranghelle (2000)and Patel et al. (1998), have shownthat the restorative approach
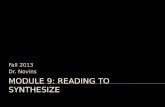
increases length of hospital rehab staywithout improving outcomes (Figure9.1). Langhammer and Stranghelle(2000) (PEDro = 8) conducted an RCTcomparing the Bobath approach(remedial type of therapy) and theMotor Relearning Programme (MRP),in which, the MRP resulted in shorterhospital stays and improved motorfunction. Despite an improvement infunctional mobility and ADLperformance, Lennon et al. (2006)
reported that normal movementpatterns were not restored followingtherapy using the Bobath principles.In the case of Patel et al. (1998), anon-randomized comparative study(unrated), there was a suggestion thatthe restorative approach actuallyincreases the number of patients who
are institutionalized. Results from thetwo more recent studies, of equalmethodological quality, comparing twocompensatory therapy approaches toa restorative (Bobath) approach were
conflicting (Van Vliet et al. 2005,Wang et al. 2005). Treatment timeswere similar in both studies (15-20sessions each), as was the time fromstroke onset to randomization (2- 3weeks). Patient characteristicsappeared to be similar. Although thepatients in the Hafsteinsdottir et al.(2005) study were not randomized theauthors controlled for a number ofcovariates in their analysis including
age, living situation education,modified Rankin scale scores, BarthelIndex, MMSE and depression. In thismulti-centered trial the sample sizewas also larger than any previous RCTconducted to date. While the authorsacknowledge the potential for biasusing a non-randomized design theyalso noted that randomization isimpractical in a clinical setting wheremost institutions use one treatmentapproach exclusively. This study was
also the first to assess quality of lifeassociated with different treatmentapproaches. Chan et al. (2006)reported greater improvement in aseries of performance-based tasksassociated with the motor relearningapproach compared to a conventionalapproach. These authors included
-
7/27/2019 Module 9 Mobility
12/174
9. Mobility and the Lower Extremity pg. 12 of 174www.ebrsr.com
both sequential and function-basedcomponents into their protocol, which
the authors believed was, responsible,in part, for the superior outcomes.
Lennon et al. (2006) suggested thatcurrent evidence reveals no realdifferences between therapyapproaches; a finding that may be
explained, in part, by the fact thatthey all share common treatmentcomponents.
Figure 9.1 Bobath or motor relearning programme? A comparison of two
different approach of physiotherapy in stroke rehabilitation: a randomized
controlled study. (Langhammer et al. 2000)
21
34
0 5 10 15 20 25 30 35
Length of Stay (days)
MRP
Bobath
LOS for Physiotherapy using the Motor Relearning Programme (MRP) vs.
Bobath
p=.008
61 stroke patients participating in a double blind trial were randomly assigned to
receive either therapy based on Bobath concept (represents a theoretical
framework in a reflex-hierarchical theory) or a Motor Relearning Programme
based on s stem theor and task oriented MRP .
Length of stay was significantly shorter in the MRP group compared to Bobath
group, 21 vs. 34 days.
Conclusions Regarding Restorativeand Compensatory Approaches
There is strong (Level 1a) evidence thatthe Bobath approach is not superior toother therapy approaches.
There is con flic ting (Level 4) evidencethat the Motor Learning Approach is
superior to the Bobath approach forachieving improvements in functionaloutcome. There is moderate (Level 1b)evidence that a Motor LearningApproach reduces length o f hospitalstay.
There is strong (Level 1a) evidence thatthe Motor Learning Approach issuperior to placebo and moderate
(Level 1b) evidence that it is superior toa conventional phys iotherapy approachfor achieving improvements infunctional outcome.
The restorative (Bobath) approachresults in longer lengths of s tay andoffers no advantage over othertherapy approaches.
9.2 Intensity of Training
The role of intensity in therehabilitation of the lower limb hasbeen the subject of debate. Whileseveral meta-analyses investigatingthe benefit of augmented physicaltherapy have been published, most of
-
7/27/2019 Module 9 Mobility
13/174
9. Mobility and the Lower Extremity pg. 13 of 174www.ebrsr.com
these included studies whichevaluated the outcomes such asimprovement in ADL function andwere not specific to measures of gaitor mobility. For example, the resultsof a meta-analysis of seven
randomized controlled trials examiningthe effects of differing intensities ofphysical therapy showed significantimprovements in activities of dailyliving (ADL) function and reduction ofimpairments with higher intensities oftreatment (Langhorne et al. 1996).Another meta-analysis of nine studies(eight RCTs and one non-randomizedexperiment) looking at the effects ofintensity of stroke rehabilitation founda small but statistically significant
intensity-effect on ADL and functionaloutcome parameters (Kwakkel et al.1997). However, Cifu and Stewart(1999) found only 3 moderate qualitystudies and one meta-analysis lookingat the intensity of rehabilitationservices and functional outcome.These authors concluded that theintensity of rehabilitation services wasonly weakly associated with improvedfunctional outcomes after stroke.
Kwakkel et al. (2004) conducted afurther meta-analysis, evaluating thebenefit of augmented physicaltherapy, including 20 studies whichhad assessed many interventions:occupational (upper extremity),physiotherapy (lower extremity),leisure therapy, home care andsensorimotor training. After adjustingfor differences in treatment intensitycontrasts, augmented therapy was
associated with statistically significanttreatment effects for the outcomes ofADL and walking speed, although notfor upper extremity therapy, assessedusing the Action Research Arm test.Augmented therapy was found to be
more effective when initiated withinsix months of the stroke.
The term, intensity, most frequentlyrefers to the frequency of repetitionswithin a given period of time, althoughmore correctly, is defined as theamount of mechanical output ofphysical activity. However, suchmeasurement is not usually possiblewithin a clinical setting. Therefore,establishing a dose-response
relationship is problematic in strokerehabilitation. Many factors precludethe routine recommendation ofstandard amounts of therapy time anindividual patient should receive.Therefore, it is extremely difficult toknow how much additional therapywould confer benefit. Nevertheless,Kwakkel (2006) noted that anassociation between effect size andadditional treatment time has been
demonstrated. Bode et al. (2004)reported that intensive practice offunction-focused physiotherapypredicted greater than expected gainsin mobility among 198 stroke patients.
Nine studies were identified whichevaluated intensity of physical therapyinterventions of assessments of gait(Table 9.8).
Table 9.8 Intensity of Lower Extremity Training
Author, YearCountry
PEDro Score
Methods Outcomes
Wade et al.1992UK6 (Crossover
94 stroke patients with reducedmobility 1 year following stroke wererandomized to one of 2 home therapygroups: 1) patients who received
Immediately following treatment, both groupsdemonstrated a significant improvement in gaitspeed. At 3 months, the early therapy groupshowed a significant improvement in gait speed
-
7/27/2019 Module 9 Mobility
14/174
9. Mobility and the Lower Extremity pg. 14 of 174www.ebrsr.com
RCT) physiotherapy immediately uponentry into the study, continuing for 3months followed by no therapy for 3months or 2) received no therapy for3 months followed by therapy for 3months. Treatment emphasized self-management.
compared to the no treatment group (-3.9 vs.6.4 sec to walk 10 m). Between 3 and 6 monthsthe group given delayed therapy showedimprovement and the previously treated groupdeclined (differences of 6.5 v -3.9 s to walk 10m). A 9% decrease in time taken to walk 10 mwas associated with treatment and a 12% (2%
to 19%) increase when patients wereuntreated.
Richards et al.1993Canada6 (Single-blindRCT)
27 patients randomized to receiveone of three therapies: 1) Earlyintensive therapy incorporating theuse of a tilt table, resisted exercisesand treadmill, beginning ~8 days poststroke, for 1.7 hrs/day x 5 weeks(experimental); 2) Early conventionaltherapy included traditional approachwith therapy beginning ~9 days poststroke, for 1.8 hrs/day x 5 wks
(control 1); or 3) Conventionaltherapy beginning 13 days poststroke, 0.72 hrs x 5 wks (control 2).
At week 6, gait speed in the 2 control groupswas similar and lower than the experimentalgroup. By months 3 and 6, the gait speedbetween all groups was similar.
Kwakkel et al.1999Netherlands8 (RCT)
101 patients were randomized 14days following stroke to receive oneof 3 therapies: 1) arm training, 2)leg training or 3) basic rehabilitationonly. Leg and arm treatments wereapplied for 30 min 5 days/week x 20weeks. All patients received basicrehabilitation.
Patients in the leg-training group (n=31) hadhigher median scores compared to the controlgroup (n=37) for ADL ability (19 vs. 16),walking ability, assessed by the FunctionalAmbulation Categories (4 vs. 3), and dexterity(2 vs.0).
Partridge etal. 2000
UK8 (RCT)
114 patients randomized to receiveeither 30 minutes or 60 minutes of
physiotherapy daily for an unspecifiedperiod of time.
No differences in Profiles of Recovery Scalescores, sit to stand or timed walk were noted
between the groups at 6 weeks or at 6 months.
Green et al.2002UK8 (RCT)
170 stroke patients > 50 Years withmobility problems one year followingstroke were randomized to receivecommunity physiotherapy treatmentor to a no treatment control group.Patients in the treatment group wereseen for a maximum of 13 weeks.
There was a difference in Rivermead mobilityindex (RMI) scores at 3 months, after adjustingfor differences in baseline gait speed. However,there were no longer differences in RMI scoresbetween the groups at 6 or 9 months.Treatment had no effect on patients' dailyactivity, social activity, anxiety, depression, andnumber of falls, or on emotional stress ofcarers.
Kwakkel et al.
2002Netherlands8 (RCT)
Follow-up study to Kwakkel et al.
1999. Evaluations of the lowerextremity included Barthel Index (BI),Functional Ambulation Categories(FAC), and comfortable walkingspeed, and were assessed at 6, 9,and 12 months after stroke.
There were no significant between group
differences on any of the outcome measuresassociated with ADL or lower mobility functionat 6, 9 or 12 months.
Kwakkel &Wagenaar etal. 2002
Additional analysis from Kwakkel et al1999.
Longer durations of rehabilitation sessions wereassociated with a trend towards improvement incomfortable walking speed compared with
-
7/27/2019 Module 9 Mobility
15/174
9. Mobility and the Lower Extremity pg. 15 of 174www.ebrsr.com
longer duration of rehabilitation sessions for theupper extremity and the control condition.However the benefits were limited to the periodof the intervention.
GAPS2004UK
7 (RCT)
A multisite (3 centre) single-blindrandomized controlled trial (RCT)comparing the effects of augmented
physiotherapy with normalphysiotherapy on the recovery ofmobility after stroke. 70 strokepatients admitted to hospital, able totolerate and benefit from mobilityrehabilitation were randomized toreceive twice the amount ofphysiotherapy compared to thecontrol group. Primary outcomes weremobility milestones (ability to stand,step and walk), Rivermead MobilityIndex (RMI) and walking speed.
The augmented therapy group received moredirect time with therapists (62 vs. 35 min/day)and were more active (8.0% versus 4.8% time
standing or walking) than normal therapycontrols. There were trends favouring theaugmented group in the outcomes ofachievement to independent walking earlier,and higher RMI scores at three months.However, there was no significant difference inany other outcome.
Jette et al.2005USANo Score
Retrospective analysis of 4,988patients (993 with stroke), evaluatingLOS and functional improvement.
Higher intensity of therapy was associated withshorter lengths of stay. Patients receiving < 1hour of therapy/day dad an average LOS of21.4 (19.7-23.3) days, compared to those whoreceived 1-1.5 hour/day (16.9;15.7-18.1) daysor >1.5 hours/day (15.5;14.2-16.9) days. Theodds of improving both independence inmobility and functional independence wereassociated with increasing intensity of therapy.
Langhammeret al. 2007Norway6 (RCT)
75 stroke patients discharged fromacute inpatient rehabilitation wererandomized to receive an intensiveoutpatient exercise program
emphasizing strength, balance andendurance or to a control group ofregular exercise. Patients in theintensive group receivedphysiotherapy during four periodswith a minimum of 20 hours everythird month. Treatment was carriedout in home, at clinics or duringinpatient rehabilitation. Subjects inthe control group received follow-uptreatment or rehabilitation only asrequired. Motor Assessment Scale
(MAS, BI and grip strength measuredwith a vogorimeter (bars) wereassessed at discharge from the acuteward and at 3, 6, 12 months.
There were no differences between groups atany of the testing intervals. The meandifferences from acute discharge to one yearwere: Intensive Group Regular Group
MAS +2.5 +7.4BI +5.3 +11.9Grip strength 0.23 0.19(paretic hand)
Langhammeret al. 2009Norway8 (RCT)
Additional results from 2007 studyreported. The main outcome wasInstrumental Activities of Daily Living(IADL), motor function, gaitperformance, balance, grip strength,
Patients in both groups improved over time. Theonly significant difference between the groupswas one component of the IADL scale, favouringthe control group (ability to use the telephoneindependently).
-
7/27/2019 Module 9 Mobility
16/174
9. Mobility and the Lower Extremity pg. 16 of 174www.ebrsr.com
and muscle tone. Additional outcomemeasures included Motor AssessmentScale, 6-Minute Walk Test, BergBalance Scale, Timed Up-and-GoTest, grip strength, Modified AshworthScale, and pulse monitoring. Thepatients were tested on admission, at
discharge, and after 3, 6, and 12months post stroke.
Moore et al.2010USA5 (RCT)
20 chronic stroke subjects completeda randomized crossover trialevaluating additional gait trainingafter reaching a plateau. After the last4 weeks of outpatient physicaltherapy (PT) subjects either received4 weeks of intensive Locomotortraining (LT) using a treadmill withbody-weight support or continuedwith their conventional treatment. At
the end of that 4-week period,subjects were crossed over andreceived an additional 4 weeks oftreatment. Outcome measuresincluded clinical and physiological(metabolic) measures of walkingoverground and on a treadmill, andmeasures of daily stepping activity inthe home and community, includingduring clinical PT and subsequent LTsessions.
Average daily stepping increased significantlyfollowing LT treatment (4,207 vs, 5,560step/day p
-
7/27/2019 Module 9 Mobility
17/174
9. Mobility and the Lower Extremity pg. 17 of 174www.ebrsr.com
two evaluated treatments in thechronic stage. Langhammer et al.(2007/2009) studied patientsfollowing inpatient rehab for one yearpost stroke. Of the studies evaluatingearlier interventions, gait speed was
evaluated in two (Richards et al. 1993,GAPS, 2004). The results wereconflicting for assessments performedwithin three months, while at sixmonths both reported no significantdifferences between treatment andcontrol conditions. Only a single RCTexamined the effect of enhancedtraining for chronic stroke patientsand reported a benefit with respect toimprovement in gait speed (Wade etal. 1992). Four RCTs evaluated less
specific measures of gait and mobility.Two of the trials were negative(Partridge et al. 2000, GAPS 2004),while two were equivocal anddemonstrated early benefits (withinthree months), but which were notmaintained at six months. The studywith the longest intervention period (1year)(Langhammer et al. 2007/2009)failed to identify significantly greatergains on a variety of outcome
measures between subjects whoreceived intensive physical therapyand those who participated in the self-
directed program. This result was notconsistent with the authorshypothesis or from their previouswork. The authors suggested that highcompliance in both groups may havebeen triggered by frequent
assessments and interest by researchstaff. Nevertheless, both intensive andinformal exercise programs wereassociated with improvement up toone year following stroke.
In a retrospective analysis of 993stroke patients receiving rehabilitationin a skilled nursing facility, Jette et al.(2005) reported that patients whoreceived less than one hour of therapyper day (combined OT/PT/ SLP) had
longer lengths of stay compared topatients who received 1-1.5 hours perday (21.4 vs. 15-17 days). Howeverthere was no difference in LOSbetween patients receiving 1-1.5hours per day and those receivingmore than 1.5 hours. Although agreater level of therapy intensity wasassociated with shortened LOS, thetotal daily therapy time would beconsidered very modest and likely not
representative of most inpatientrehabilitation programs.
Table 9.9 Summary of RCTs Evaluating Intensity of Therapy on Assessments of Gait andMobility
Author PEDroScore
N Timing of InterventionFrom Stroke Onset
Outcome Assessed Result
Wade et al. 1992 6 94 > 1 year Gait speed +
Richards et al.1993
6 27 < 30 days Gait speed + (6 weeks)- (3 & 6 months)
Kwakkel et al. 1999& 2002
8 101 1 week Walking ability(FunctionalAmbulationCategories)
+ (6 weeks)+ (12 weeks)+ (20 weeks)- (26 weeks)- (52 weeks)
Partridge et al.2000
8 114 Unclear (assumed tobe early)
Profiles of RecoveryTimed walk
- (6 weeks)- (6 months)
Green et al. 2002 8 170 > 1 year * RMI + (3 months)- (6 & 9 months)
Langhammer et al. 8 75 Following d/c from MAS -
-
7/27/2019 Module 9 Mobility
18/174
9. Mobility and the Lower Extremity pg. 18 of 174www.ebrsr.com
2007/2009 inpatient rehab IADL6 min walk test
- (at 1 year)-
GAPS 2004 7 70 < 30 days Walking speed* RMI
- (
-
7/27/2019 Module 9 Mobility
19/174
9. Mobility and the Lower Extremity pg. 19 of 174www.ebrsr.com
Lubetzky-Vilnai & Kartin (2010)conducted a narrative, systematicreview, including the results from 22studies (9 RCTs) examining theeffectiveness of balance trainingprograms following stroke. The
authors noted variations in the dosageand type of interventions assessed,the chronicity of stroke among
participants, the length of theprograms and the length of follow-up.Regardless, they reported that therewas evidence to support the use ofindividual balance training in the acutestage of stroke and either group or
individual sessions among patients inthe sub acute or chronic stages ofstroke.
Table 9.10 RCTs Included in Two Systematic Reviews of Biofeedback Training
Barclay-Goddard et al. 2004(Cochrane Review)
Van Peppen et al. (2006)
Chen et al. 2002Geiger et al. 2001Lee et al. 1996Sackley et al. 1997Shumway-Cook et al. 1988
Walker et al. 2000Wong et al. 1997
Chen et al. 2002Cheng et al. 2004Geiger et al. 2001Lee et al. 1996Sackley et al. 1997
Shumway-Cook et al. 1988Walker et al. 2000 (Grant et al. 1997-subset analysis)Winstein et al. (1989)Wong et al. 1997
Individual Studies
Table 9.11 Treatment of Balance Disorders Post Stroke
Author, YearCountry
PEDro Score
Methods Outcomes
Shumway-
Cook et al.1988USA4 (RCT)
Static force plate system was used to
examine postural sway characteristics in 16hemiplegic patients and 34 normal elderlysubjects. Mean number of days since thetime of stroke onset for patients was 37 +15 days. Effectiveness of postural swaybiofeedback was compared to conventionalphysical therapy practices in establishingstance stability.
Postural sway abnormalities in hemiplegic
patients included significant mean lateraldisplacement of sway toward the non-affected leg and increased total swayarea. Postural sway biofeedback wasmore effective than conventional loadingof the affected leg. However, post-treatment changes in total sway areawere not significantly different betweenthe groups.
Winstein et al.1989USA
No Score
42 post acute hemiplegic patients receivedeither 3-4 weeks of standing balancetraining with a specifically designed
feedback device, the standing feedbacktrainer (SFT) or were assigned to a controlgroup with no SFT. Evaluations includedStanding Balance and Locomotorperformance measures.
There were significant between-groupdifferences of improved static standingsymmetry favouring the feedback device
group (p
-
7/27/2019 Module 9 Mobility
20/174
9. Mobility and the Lower Extremity pg. 20 of 174www.ebrsr.com
a sit to stand exercise or to a controlcondition. Both treatments were provided in12 treatment sessions, over 4 weeks.Evaluations included the Rivermead MotorFunction Assessment and the Nottingham10 Point ADL Scale, as well as measures ofstance symmetry and sway, undertaken at
0,4 and 12 weeks.
at 12 weeks.
Wong et al.1997Taiwan5 (RCT)
60 stroke patients were randomized toreceive one of two training methods: (1)Standing training table (STT): height-adjustable worktable, a pelvic belt and asuspension system to help the clientmaintain symmetry in an upright stance,while performing a task of pushing andpulling a load by means of resistivemovements of the upper limb. Thesubject/therapist did not know how muchweight is actually transferred to the
affected leg during the training program;(2) Standing biofeedback training device(SBT): modification of STT with a real-timevisual weight bearing biofeedback displayswith numerical light-emitting diodes andbalance scale and auditory alarm system.Patients were trained for 5 days a week for3 to 4 weeks.
Ability to maintain stance by percentageof postural symmetry in the group trainedwith SBT was significantly better than thattrained with STT at week 4. Immediatelearning effect after the first day oftraining in group SBT was significantlybetter than group STT.
Grant et al.1997Canada5 (RCT)
16 patients were randomized to receiveeither standard physiotherapy includingbalance training or to receive standardphysiotherapy with biofeedback balancetraining, including 30 minutes of additional
balance training/day for 19 sessions.
No significant differences were foundbetween the 2 groups on any of theoutcomes measures.
Walker et al.2000Canada5 (RCT)
54 patients were randomized to 1 of 3groups: (1) visual feedback training; (2)conventional balance training; and (3)control group. The 2 treatment groupsreceived additional balance training given 5days/wk for 3-8 wks, depending on lengthof rehabilitation stay. Patients wereadmitted within 4 months of stroke onset.
At 1-month follow-up there were nosignificant differences between the groupson any of the outcome measures overtime.
Cheng et al.2001Taiwan
6 (RCT)
54 patients with hemiplegic stroke wererandomly assigned to receive conventionalstroke rehabilitation or conventional stroke
rehabilitation plus symmetrical standingtraining and repetitive sit-to-stand trainingwith a standing biofeedback trainer.
Patients receiving extra trainingdemonstrated a significant improvementin sit-to-stand performance. Body weight
was distributed more symmetrically inboth legs with less mediolateral swaywhen rising and sitting down.
De Seze et al.2001France6 (RCT)
20 hemiplegic stroke patients with axialpostural disturbances were randomized toeither a device group (DG), in whichpatients followed experimental program for1 hour a day using the Bon Saint Comedevice for axial postural rehab, or to a
On day 30 postural (Trunk Control Testand the Upright Equilibrium Index) andneglect tests improved significantly in DGvs. CG. A significant benefit remained atday 90. Gait improved earlier in DG thanCG. FIM scores improved equally
-
7/27/2019 Module 9 Mobility
21/174
9. Mobility and the Lower Extremity pg. 21 of 174www.ebrsr.com
control group, in which patients receivedconventional neurorehab for 2 hours a dayfor 1 month (CG). After an experimentalperiod, all patients received 2 months ofconventional neurorehab for 2 hours a day.Patients were assessed on days 0, 30 and90 by a battery of postural test, gait
evaluation, the Bells neglect test and FIMinstrument.
between DG and CG.
Geiger et al.2001USA3 (RCT)
13 patients were randomized to receiveeither biofeedback training or regularbalance training therapy. Both groupsreceived interventions to improve balanceand mobility 2-3 x/wk for 50 min for 4 wkswhile the experimental group received anadditional 15 minutes of biofeedbacktraining. Patients were able to standwithout manual assistance for 2 minutes.
At 4 weeks, there were no significantdifferences observed between the 2groups on either outcome measures.
Chen et al.
2002Taiwan4 (RCT)
41 hemiplegic, ambulatory stroke patients
were randomly allocated to either a trainedgroup or to a control group. The trainedgroup received visual feedback balancetraining with the Smart Balance Masterdevice plus the same therapy received bythe control group. The control groupreceived conventional physical andoccupational therapy. Patients receivedtreatments for 20 minutes a day, 5 days aweek for a 2-week period.
The trained group were able to use more
ankle strategies than the control groupbut there was no significant difference inmaximum stability and centre of gravityalignment between the groups in regardsto static balance. With regards todynamic balance, significant improvementin axis velocity, directional control, andend point excursion in the trained groupwas noted compared to the control group.Ability of self-care and sphincter controlsignificantly improved for the trainedgroups compared to the control group.
Pollock et al.
2002UK5 (RCT)
28 stroke patients who had achieved 1
minute of independent sitting balance wererandomized to receive either standardphysiotherapy or were assigned toindependent practice. The independentgroup received 4 weeks of independentpractice aimed at improving aspects ofbalance involving a series of motor tasks.The standard physiotherapy group receivedphysiotherapy based on the Bobathapproach. Patients were assessed by aspecially designed measurement systeminvolving a chair which recorded body
symmetry. Outcomes were recorded as theproportion of patients achieving normalsymmetry of weight distribution duringsitting, standing, and rising to stand, sittingdown and reaching. Patients were free ofprevious disability, pathology orneurological deficits affecting mobility priorto stroke.
No significant differences in proportion of
patients that achieved normal symmetrywere noted between groups.
Morioka et al. 28 stroke patients were randomly assigned Parameters indicating postural sway were
-
7/27/2019 Module 9 Mobility
22/174
9. Mobility and the Lower Extremity pg. 22 of 174www.ebrsr.com
2003Japan6 (RCT)
to either perceptual learning exercises or toa control group, which did not receiveperceptual-learning exercises. Both groupsparticipated in rehabilitation programconsisting of physio- and occupationaltherapy. Perceptual learning exercise wasdesigned to discriminate the hardness of a
sponge rubber placed under the sole of thefoot. Outcomes measured were length,enveloped area and rectangular area of theparameter of postural sway measured by astabilometer on entry into the study andafter 10 days.
significantly decreased in theexperimental group compared to thecontrol group.
Bonan et al.2004France6 (RCT)
20 patients with hemiplegia after strokewere randomly assigned to one of two-balance rehabilitation groups: Visiondeprived in which eyes were blinded with amask (without visual cues) or to free vision(with visual cues).
After completing the program balance,gait velocity, and self-assessment of gaitimproved significantly in both groups.However, balance improved more in thevision-deprived group than in the freevision group.
Cheng et al.2004TaiwanNo Score
52 hemiplegic stroke patients receivedeither conventional therapy + visualfeedback rhythmic weight training (n=28)or conventional therapy only (control).Evaluations included: the number of falls,dynamic balance performance, staticbalance in various sensory components, onaxis velocity & directional control duringrhythmic weight-shift.
At 6-months follow-up, there were nostatistically significant between-groupdifferences for any outcome measures.However, for the post-training testpatients in the experimental groupimproved more in dynamic performancemore then control (p6 months poststroke participated in an 8-week (1 hr2x/week) task-oriented exercise programfocusing on balance and mobility exercisesand were randomized to one of two groups.Exercises were performed under normal
conditions by the control group and underconditions of vision (eyes closed/open) andsurface manipulation (firm/hard surface) bythe experimental group. Pre- and post-testassessments involved the measurement ofthe center of pressure (COP) displacementduring double-legged stance and sit-to-stand under four sensory conditions: (1)eyes open, normal surface; (2) eyes open,
Results showed significant improvements(P
-
7/27/2019 Module 9 Mobility
23/174
9. Mobility and the Lower Extremity pg. 23 of 174www.ebrsr.com
soft surface; (3) eyes closed, normalsurface; and (4) eyes closed, soft surface,as well as the 10-m walking test.
Katz-Leurer etal. 2006Israel5 (RCT)
24 patients with recent stroke wererandomly assigned to receive routineinpatient rehabilitation or rehabilitation + adaily cycle training program for 3 weeks.
Outcomes included the Postural AssessmentScale for Stroke Patients (PASS) and theFugl-Meyer (FM) and FIM, assessed at 3and 6 weeks.
PASS (dynamic, standing and total), FMand FIM (motor) scores were higher forpatients receiving additional cyclingtraining.
Van Nes et al.2006Netherlands9 RCT
53 patients were randomized to receiveeither whole-body vibration (n=27) orexercise therapy on music (n=26) inaddition to a regular inpatient rehabilitationprogram. Whole-body vibration, was usedas a novel method of somatosensorystimulation to improve postural control andactivities of daily living The whole-body
vibration group received 4x45-secondstimulation on platform vibration device, 5days per week during 6 weeks. Outcomevariables included the Berg Balance Scale,Trunk Control Test, Rivermead MobilityIndex, Barthel Index, Functional AmbulationCategories, Motricity Index, andsomatosensory threshold at 0, 6, and 12weeks follow up.
Both at 6 and 12 weeks follow up, noclinically relevant or statistical differencesin outcome were observed between thegroups.
Yavuzer et al.2006Netherlands5 (RCT)
50 rehabilitation inpatients, post strokeonset of 6 months were randomized toreceive conventional rehab with (n=25) andwithout (n=25) additional balance training.
Patients in the balance training groupreceived 15 min of balance training once aday, 5 days a week for 3 weeks, using theNor-Am Target Balance Training System.Time-distance and kinematic gaitparameters were assessed followingtreatment.
Pelvic excursion in frontal plane improvedsignificantly more in the experimentalgroup compared with control (p=0.021).The difference between before-after
change scores of the groups wassignificant for pelvic excursion in frontalplane (p=0.039) and vertical groundreaction force (p=0.030) in favour ofexperimental group. The control group didnot show any statistically significantdifference regarding gait characteristics.
Allison et al.2007UK5 (RCT)
17 stroke rehabilitation patients wererandomized to receive conventionalphysiotherapy for the duration of theirinpatient stay (n=10), provided for 45minutes, 5 days a week, or to an
intervention group (n=7) who received anadditional 45 minutes of standing balancetraining in addition to conventionalphysiotherapy. Treatment involved use ofstanding frames, tilt tables or standingtables, used to provide support. Outcomesassessed at baseline, week 1,2 and 12included Berg Balance score, Gross FunctionTool of Rivermead Motor Assessment Scale
At the end of 12 weeks the onlysignificant difference between groups wasin the change in Berg Balance scores frombaseline, favouring the interventiongroup. BBS scores changed from 8 to 37
in the intervention group and 16.5 to 20.5in the control group.
-
7/27/2019 Module 9 Mobility
24/174
9. Mobility and the Lower Extremity pg. 24 of 174www.ebrsr.com
and the Trunk Control Test.
Eser et al.2008Turkey6 (RCT)
41 rehabilitation inpatients with a mediantime since stroke of 6 months wererandomly assigned to receive conventionalstroke inpatient rehabilitation (n=19) or toreceive 15 sessions of balance training(using force platform biofeedback) in
addition to the conventionalprogram(n=22). The main outcomemeasures assessed before and one-weekafter treatment included Brunnstromstaging, Rivermead Mobility Index, (RMI)and FIM.
Motor recovery, mobility and activity levelimproved significantly in both groups overthe treatment period. Between-groupdifference of mean change score was notsignificant for the Brunnstrom stages,(0.23 vs. 0.26) RMI (2.9 vs. 2.2) or FIM
score (10.7 vs. 11.5).
Yelnik et al.2008France7 (RCT)
68 stroke patients able to walk withouthuman assistance were entered from 3 to15 months (mean, 7 months) after a firsthemispheric stroke were randomized to a 4-week program of either multisensorialrehabilitation, an approach based on higher
intensity of balance tasks and exerciseduring visual deprivation, or to aconventional neurodevelopmental theory-based treatment (NDT) that used a generalapproach. The primary outcome was the 30day Berg Balance Scale (BBS) score.Secondary outcomes included velocity,double stance phase, climbing 10 steps,amount of walking per day, FIM and theNottingham Health Profile (NHP)assessment at 30 and 90 days.
All subjects improved significantly inbalance and walking parameters. Therewas no significant between groupdifferences on the primary outcome.There were significant differences in FIMscores and NHP scores at both 30 and 90
days, favouring the experimental group.
Noh et al.2008
South Korea7 (RCT)
25 ambulatory chronic stroke patients wererandomized to an 8-week (3days/wk x 1hr)
exercise program- either aquatic therapyconsisting of Ai Chi and Halliwick methods,which focused on balance and weight-bearing exercises or conventional therapywho performed gym exercises. The primaryoutcome measures were Berg Balance Scalescore and weight-bearing ability, asmeasured by vertical ground reaction forceduring four standing tasks (rising from achair and weight-shifting forward, backwardand laterally) assessed before and aftertreatment. Secondary measures were
muscle strength and gait.
The aquatic therapy group attainedsignificantly greater improvements in
Berg Balance Scale scores (7.6 vs. 2.02points, p
-
7/27/2019 Module 9 Mobility
25/174
9. Mobility and the Lower Extremity pg. 25 of 174www.ebrsr.com
kinaesthetic ability training static anddynamic balance indices, balance and lowerextremity subscores of the Fugl-MeyerStroke Assessment Instrument (FMA) andtotal motor and locomotor sub item scoresof the FIM.
improvements in balance subscores ofFMA, static and dynamic balance indexesin the experimental group and in sub-itemscores of FIM and lower extremity scoresof FMA within both groups.
Au-Yeung et
al. 2009China7 (RCT)
136 subjects >6 months after stroke were
randomly assigned to a control group (n =62) practicing general exercises or a Tai Chigroup (n = 74) for 12 weeks of training.Each week, 1 hour of group practice wassupplemented by 3 hours of self-practice.The short-form of Tai Chi consisting of 12forms that require whole-body movementsto be performed in a continuous sequencewas used. Assessments were conducted atbaseline, 6 weeks (mid-program), 12 weeks(end-program), and 18 weeks (follow-up).The 3 outcome measures were (1) dynamic
standing balance evaluated by the center ofgravity (COG) excursion during self-initiatedbody leaning in 4 directions, (2) standingequilibrium evaluated in sensory challengedconditions, and (3) functional mobilityassessed by Timed-up-and-go score.
Compared with the controls, the Tai Chi
group showed greater COG excursionamplitude in leaning forward, backward,and toward the affected and nonaffectedsides (P < .05), as well as faster reactiontime in moving the COG toward thenonaffected side (P = .014) in the end-program and follow-up assessments.There were no significant differencesbetween groups at follow-up on any of theother outcomes.
Verheyden etal. 2009Belgium6 (RCT)
33 patients admitted for inpatientrehabilitation were randomly assigned to anexperimental group (n = 17) or a controlgroup (n = 16). In addition to conventionaltherapy, the experimental group received10 hours of individual and supervised trunkexercises; 30 minutes, 4 times a week, for
5 weeks. Trunk performance was evaluatedby the Trunk Impairment Scale (TIS) andits subscales of static and dynamic sittingbalance and coordination, before and aftertreatment.
No significant pretreatment differenceswere found between the 2 groups.Following treatment, there weresignificant improvements in the mean TISscores of patients in both groups. Asignificantly greater improvement wasnoted in the experimental group
compared to the control group for thedynamic sitting balance subscale only.There were no differences in the total TISscore, static sitting balance orcoordination.
Goljar et al.2010Slovenia6 (RCT)
44 patients admitted for inpatientrehabilitation who were able to walk for 10m (independently or with assistance) wererandomized to either a control or balancetrainer device group. Patients trained for 20min per day, 5 days per week for 4 weeksand received an additional 25 min of
physiotherapy. Balance was assessed bythe Berg Balance Scale (BBS), one-legstanding, Timed Up and Go (TUG) Test and10 m walk before and after treatment.
There was significant improvement inmean BBS scores (P
-
7/27/2019 Module 9 Mobility
26/174
9. Mobility and the Lower Extremity pg. 26 of 174www.ebrsr.com
rehabilitation machine for 30 minutes/day,5 days a week for plus 40 minutes ofconventional training using the Bobathapproach for two weeks, followed byconventional training only for another twoweeks. Group B (n = 15) underwent thesame training in reverse order. The main
outcome measures were FunctionalAmbulation Category (FAC), Berg BalanceScale (BBS), Six-Minute Walk Test (6MWT),Timed Up and Go Test TUG), KoreanModified Barthel Index (K-MBI), ModifiedAshworth Scale and Manual Muscle Test,assessed before and after treatment.
control period. There were alsostatistically significant differences(p
-
7/27/2019 Module 9 Mobility
27/174
9. Mobility and the Lower Extremity pg. 27 of 174www.ebrsr.com
weeks. The main outcome measures werethe Trunk Impairment Scale and BrunelBalance Assessment, assessed before andafter treatment.
Saeys et al.2011Belgium
7 (RCT)
33 patients, an average of 35 daysfollowing stroke were randomly assigned toan experimental group (n = 18) or a control
group (n = 15). In addition to conventionaltherapy, patients in the experimental groupreceived 16 hours of truncal exercises. Thecontrol group received 16 hours of shamtreatment. Outcomes were assessed atbaseline and at the end of treatment andincluded the Trunk Impairment Scale (TIS)and the Tinetti Test. The Romberg witheyes open and eyes closed, Four TestBalance Scale (FTBS), Berg Balance Scale(BBS).
Patients in the experimental groupperformed significantly better on all onthe outcomes:TIS (P < .001), Tinetti Test
(P < .001), FTBS (P = .014) and BBS (P= .007.
Lisinski et al.
2011Poland4 (RCT)
26 patients, an average of 17 months post
stroke were randomly assigned to Group A:Balance training on a platform for 20 days,or Group B: no balance training,observation only. Both groups werecompared to Group C: 15 healthy controls.Static balance was assessed using theMetitur Good Balance platform pre and postintervention. Movement selectivity wasassessed using the Brunnstrom gradingscale.
Post intervention weight bearing
symmetry and Brunnstrom scores weresignificantly improved in Group A only.
Ahn et al.2011
South Korea4 (RCT)
36 patients, within 2 years post stroke wererandomized to receive either selective-task
or set-task balance training. The trainingsessions were conducted for 30 mins, 3days/week for 8 weeks. Assessments werecompleted at baseline, 8 weeks and 3months. Outcome measures included theBerg Balance Scale (BBS), Plantar footpressure distribution, and Lower extremitysubscale of the Fugl-Meyer Assessment(FMLE).
There were significant differencesbetween groups, favoring the selective-
task specific group, in terms of BBSscores, plantar foot pressure and FMLEscores (p0.05) at 8 weeks and at the 3month follow up.Both groups showed significantimprovement over time as measured -bythe BBS, plantar foot pressure and FMLEscores.
Shin et al.2011Korea
4 (RCT)
21 patients between 6 month and 5 yearspost stroke were randomly assigned to acombined aerobic and functional training
group or a conventional training group.Both groups received 60 minutes oftraining, 5 days/week for 4 weeks. Staticbalance was assessed using a forceplatform and dynamic balance wasassessed using the Berg Balance Scale(BBS), pre and post intervention
Both groups demonstrated improvedstatic and dynamic balance at the postintervention assessment (p
-
7/27/2019 Module 9 Mobility
28/174
9. Mobility and the Lower Extremity pg. 28 of 174www.ebrsr.com
South Korea5 (RCT)
dual task training (MDT) (b) cognitive dualtask training (CDT) (c) motor and cognitivetask training (MCDT). In these groups,balance training was augmented by anadditional motor task, cognitive task orboth. Sessions were carried out for 30minutes, 3/week for 6 weeks. Outcome
measures used included the Korean BergBalance Scale (K-BBS), FIM and center ofpressure (COP) measurements usingGaitview.
BBS scores, FIM scores and COPmeasures (p0.05). There was significantdifference among groups in terms of K-BBS and FIM scores, favoring the MCDTgroup (p
-
7/27/2019 Module 9 Mobility
29/174
9. Mobility and the Lower Extremity pg. 29 of 174www.ebrsr.com
methods, platform training, additional strength training and cycle training.
Table 9.12 Summary of RCTS with PEDro Scores 6 Examining Balance Treatments
Author PedroScore
N Experimental Treatment Outcome
Van Nes et al. 2006 9 53 Whole body vibration -
Mudie et al. 2002 8 40 Task Specific; Bobath methods; BalancePerformance Monitor (BPM) feedbacktraining
+BPM
Karthikbabu et al.2011
8 30 Task-specific trunk exercises on a physio ball +
Jiejiao et al. 2012 8 92 Cognitive dual-task training +
Howe et al. 2005 7 35 Additional Therapy -
Yelnik et al. 2008 7 68 Visual Cue Deprivation -
Noh et al. 2008 7 25 Aquatic therapy +
Alptekin et al. 2008 7 30 Kinaesthetic ability training (KAT) +
Au-Yeung etal.2009
7 136 12 weeks of Tai Chi +
Chen et al. 2011 7 35 Thermal stimulation -
Saeys et al. 2011 7 33 Truncal exercises +
Lee et al. 2012 7 40 Balance control trainer +
Goljar et al. 2010 6 44 Balance trainer -
Cheng et al. 2001 6 54 Symmetrical standing training and repetitivesit-to-stand training
+
Morioka et al. 2003 6 28 Perceptual Learning +
Bonan et al. 2004 6 20 Visual Cue Deprivation +
De Seze et al. 2001 6 20 Bon Saint Come device +
Sackley & Lincoln1997
6 26 Visual biofeedback vs. sham treatment +
Eser et al. 2008 6 41 Visual feedback using Nor-Am TargetBalance Training System
-
Verheyden et al.2009
6 33 Additional trunk exercises +/-
Grant et al. 1997 5 16 Biofeedback Balance Training -
Allison et al. 2007 5 17 Standing practice -
Yavuzer et al. 2006 5 50 Nor-Am Target Balance Training System +
Wong et al. 1997 5 60 Standing training device vs. visual feedbacktraining device
+(feedback)
Walker et al. 2000 5 54 Visual Feedback Training -
Pollock et al. 2002 5 28 Independent Practice -
Katz-Leurer et al.2006 5 24 Cycling training +
Chen et al. 2002 4 41 Visual biofeedback with devise SmartBalance Master
+
Shumway-Cook etal. 1988
4 50 Visual biofeedback -
Bayouk et al. 2006 4 16 Physical therapy + manipulationproprioception of feet/ankles and/or vision
+
Geiger et al. 2001 3 13 Biofeedback training -
-
7/27/2019 Module 9 Mobility
30/174
9. Mobility and the Lower Extremity pg. 30 of 174www.ebrsr.com
Many different approaches includingadditional therapy and a variety ofdevices were examined amongpatients in both the acute andrehabilitation phases of stroke.
Although a majority of studiesdemonstrated a benefit of balancetraining, the heterogeneity ofinterventions and outcome measuresdoes not allow for definitiveconclusions regarding the effect ofbalance training post-stroke.
Conclusions Regarding BalanceDisorders
There is strong (Level 1a) evidence that
balance training post s troke improvesoutcomes, although some treatmentapproaches are more effective thanothers.
Balance training, using specificdevices or exercises, post stroke isbeneficial.
9.3.2 Falls Prevention
Falls are relatively common among theelderly. Each year 30% of those overthe age of 65 will experience a fall.(Weber et al. 1996). Those havingexperienced a stroke are at greaterrisk. During inpatient rehabilitation thereported incidence of falls ranged from25%-39% (Dromerick & Reding, 1994and Nyberg & Gustafson 1995). Uponreturn to the community, the risk isincreased further. Forster & Young(1995) reported that up to 73% of
persons had fallen within 6 months ofdischarge from hospital followingstroke. Falls can result in injuries,which range from mild, involving softtissues, to severe, including hipfracture. Fortunately, most falls areminor; less than 10% of falls result infracture (Campbell 1990; Tinetti1988). Loss of bone mineral density
following stroke increases the risk ofhip fracture, especially among women,above that seen in community-dwelling older people.
In addition to advancing age, factorsassociated with falls include femalesex, depression, cognitive impairment,functional disability, medications,urinary incontinence and poor balance(Eng et al. 2008). Additional specificrisk factors among stroke survivorsinclude greater standing sway,impulsivity and slower response times(Hyndman et al. 2002). Due tovisuospatial neglect, proprioceptiveimpairments and attention deficits,
persons with right-sided stroke are atincreased risk of falling compared topersons with left-sided lesions (Eng etal. 2008).
There is limited evidence regardingfalls prevention programs followingstroke. A study protocol designedspecifically to address this interventionhas been published. (Batchelor et al.2009). The FLASSH (FaLls prevention
After Stroke Survivors return Home)project has been designed as a RCT toevaluate the effectiveness of a multi-factorial falls prevention program forstroke survivors who are at high riskof falling when they return home afterrehabilitation. The interventionconsists of a home exercise programas well as individualised fallsprevention and injury minimisationstrategies based on identified riskfactors for falls. Participants will be
advised to undertake the exerciseprogram at least 5 times per week.The study aims to recruit a target of214 subjects. The primary outcome isthe number of falls at 12 months,using a falls diary.
-
7/27/2019 Module 9 Mobility
31/174
9. Mobility and the Lower Extremity pg. 31 of 174www.ebrsr.com
Two RCTs have assessed theeffectiveness of exercise interventionprograms to reduce the risk of fallspost stroke, one during inpatient
rehabilitation and the other amongcommunity dwelling stroke survivors.(Table 9.13).
Table 9.13 Exercise-based Falls Prevention Programsuthor, Year
CountryPEDro Score
Methods Outcomes
Cheng et al.2001Taiwan6 (RCT)
54 patients with hemiplegic stroke wererandomly assigned to receive conventionalstroke rehabilitation or conventional strokerehabilitation plus symmetrical standingtraining and repetitive sit-to-stand trainingwith a standing biofeedback trainer(intervention group).
At 6 months, fewer subjects in theexperimental group had experienced afall (16.7% vs. 41.7%).
Marigold et al.
2005Canada8 (RCT)
61 community-dwelling chronic stroke
patients were randomized to an exerciseprogram that emphasized both stretching andweight-shifting or agility. Sessions were onehour in length, 3 x per week and continuedfor 10 weeks. Falls were tracked for 1 yearfrom the start of the interventions.
There was no significant difference
between the groups in the number offalls. There were 75 falls in thestretching group (16 people) and 25falls in the agility group (11people)(p=0.20).
Tilson et al.2012USA5 (RCT)
Further reporting on the LEAPS trial. 408patients with stroke onset of 2 months wererandomized to undergo one of 3 trainingregimens: early treadmill training with partialbody-weight support (within 2 months ofstroke) (n=139), late treadmill training withpartial body-weight support (6 months afterstroke) (n=143) and a home-based exerciseprogram (n=126). All programs consisted of90 min sessions, 3x/week for 12 to 16 weeks.Incidence of falls was recorded by participantsand this data was collected via a a standardquestionnaire administered over the phone at12 months.
There was no significant difference inthe number of reported falls across all 3intervention groups (p=0.80).
Dean et al.2012 Australia7 (RCT)
151 community based stroke patientswere randomized to an intervention orcontrol group. The intervention groupreceived exercise and task relatedtraining. The control group performed on
upper extremity strength training andcognitive tasks. The primary outcomemeasures were the number of falls andcharacteristics of mobility including the6-MWT and 10-m Walk test. Secondaryoutcome measures were falls risk score,habitual physical activity, QOL,community participation, and healthsystem contact.
At 12 month follow up, theexperimental group showedsignificant improvement in 6-MWT(CI=19-50: P
-
7/27/2019 Module 9 Mobility
32/174
9. Mobility and the Lower Extremity pg. 32 of 174www.ebrsr.com
Conclusions Regarding Falls PreventionPrograms
There is stong (Level 1a) evidence thatexercise based falls preventionprograms do not reduce the rate of fallsfollowing stroke.
9.4 Gait Retraining
Restoration of gait is considered to beone of the primary goals of strokerehabilitation. Mobility is oftennegatively impacted by stroke due toresidual impairments and disabilitiesincluding impaired balance, spasticityand decreased motor control (Pohl etal. 2004). Hesse et al. (2003) notesthat three months following a stroke,approximately 20% of stroke survivorsremain primary wheelchair users, and
walking is limited in another 60%(Jorgensen et al. 1995, Wade et al.1987). Adults with acute of subacutestroke ambulate only 40-50% of thedistance that community dwellingadults without stroke are reported towalk. (Pohl et al. 2004). Manytechniques are currently in use to aidin the recovery of gait. In this section,
we include an examination ofconventional gait training techniquesthat include task-specific training andtreadmill training. An examination oftwo lesser known techniques,rhythmic auditory stimulation andvirtual reality is also included.
9.4.1 Repetitive Task Training
Proponents of task-specific trainingcite that intense training is not alwaysnecessary for positive outcomes instroke patients, but instead suggestthat therapy designed to be moretask-specific within normal contacttime (30 to 45 minutes per session)could be more efficacious (Page2003). Hesse et al. (2003) notesthat,Task-specific therapy can enable
hemiplegic patients to practice walkingrepetitively, in contrast to
conventional treatment in which tone-inhibiting manoeuvres and gait-
preparatory tasks during sitting andstanding dominate.
A recent Cochrane review authored byFrench et al. (2007) evaluated the
Batchelor et al.2012 Australia7 (RCT)
156 stroke patients, at high risk of falls.were randomized into a tailoredmultifactorial falls prevention group orthe control group which consisted ofusual care. The falls prevention programconsisted of usual care, an individualizedhome based exercise program, falls risk
strategies, education, and injury riskminimization strategies. The primaryoutcomes were the rate of falls andproportion of fallers. Secondary outcomemeasures included the number ofinjurious falls, falls risk, participation,activity, let strength, gait speed, balance,and falls efficacy.
The results showed that theintervention group was no moreeffective than usual care inreducing falls in stroke patientswho are at high risk of falls. Theprimary outcome measures: Fallrates between groups (intervention
group had 1.89 falls/person-year,and the control group had 1.76falls/person-year, incidence rateratio=1.10, P=0.74), proportion offallers between groups (riskratio=.83, (%% CI=0.6-1.14),injurious fall rate (intervention 0.74injurious falls/person-year, control0.49 injurious falls/person-year,incidence rate ratio=1.57, P=0.25).No significant differences betweengroups were identified in thesecondary outcome measures.
-
7/27/2019 Module 9 Mobility
33/174
9. Mobility and the Lower Extremity pg. 33 of 174www.ebrsr.com
effect of repetitive task training, onboth upper and lower-extremityfunction. With respect to interventionsaimed at improving mobility task-specific training was associated withimprovements in walking distance,
speed and performance in sit-to-stand. The authors concluded thattask-specific training was associatedwith modest improvement in lowerlimb function.
Van de Port et al. (2007) identified 14RCTs examining the benefit of gait-oriented training programs. There wasa significant treatment effect of suchprograms on the outcome measures ofgait speed and walking distance.
There was no significant treatmenteffect with respect to improvedbalance, ADL or IADL performance.
Task-oriented circuit class training is aspecific form of task-specific therapy,usually defined as therapy thatinvolves a tailored interventionprogram targeted at improvingstrength, balance and range ofmovement and includes walking
practice. The therapy also involvesgroups rather than individualsphysically moving between workstations set up at different workstations. Circuit class training is mostoften provided in addition to individualphysical therapy sessions (English etal. 2007). The benefits of this type oftraining include peer support andsocial interaction as well as moreefficient use of therapy staff.
Wevers et al. (2009) also reported asignificant treatment effect of task-oriented circuit class training onseveral measures of gait in a meta-analysis including the results from 6studies (307 participants). The effectsizes in favour of task-oriented circuitclass training for walking distance
were 0.43 (95% CI, 0.17 to 0.68;P
-
7/27/2019 Module 9 Mobility
34/174
9. Mobility and the Lower Extremity pg. 34 of 174www.ebrsr.com
an example of this form of therapy,we have included this treatment underits own section. Similarly, studiesspecifically evaluatingcardiorespiratory fitness training andstrengthening programs have also
been included in other sections. Weidentified 11 RCTs that evaluated avariety of interventions that weconsidered under the rubric ofrepetitive task training.
Table 9.14 Repetitive Task Training
Author , YearCountry
PEDro Score
Methods Outcomes
Dean & Shepherd1997Australia5 (RCT)
20 chronic patients were randomized to eitherthe treatment or control group. Treatmentgroup participated in a standardized trainingprogram involving practice of reaching beyondarms length while control received a shamtraining involving completion of cognitive-manipulative tasks within arms length.Performance of reaching in sitting wasmeasured before and after training. Variablestested were movement time, distancereached, vertical ground reaction forcesthrough the feet, and muscle activity.Subjects were also tested on sit-to-stand,walking, and cognitive tasks.
After training, experimental subjectswere able to reach faster and further,increase load through the affected foot,and increase activation of affected legmuscles compared with the controlgroup (P < .01). The experimentalgroup also improved in sit-to-stand.The control group did not improve inreaching or sit-to-stand. Neither groupimproved in walking.
Dean et al. 2000Canada5 (RCT)
A randomized controlled trial of 12 chronicstroke patients were randomized to either acontrol group or an experimental group. Allpatients participated in exercises classes 3times a week for 4 weeks. For theexperimental group, exercise was designed as
a circuit program with workstations designedto strengthen the muscles in the affected legin a functionally relevant way and providepractice of locomotor tasks. The controlgroups exercise class was designed similarlyexpect that group training was designed toimprove the