Models of District Support - AMCHAM
18
PEPFAR Update American Chamber of Commerce Health and Wellness Forum Meeting July 9, 2014 1
Transcript of Models of District Support - AMCHAM

PEPFAR Update
American Chamber of Commerce Health and Wellness Forum Meeting
July 9, 2014
1

GLOBAL VISION FOR PEPFAR MOVING
FORWARD



Adhere to Congressional Care & Treatment Directive while maintaining focus on:
Combination Prevention (PMTCT, ART, Condoms, VMMC)
Prevention (effective/targeted)
Neglected & Hard to Reach Populations • Pediatrics
• Adolescent girls
• Key populations – MSM & TG, FSW, PWID
Health Systems, especially human resources for health, supply chain, lab, and strategic information
Return to Core: Focusing on Highest
Impact Interventions

First PEPFAR priority is controlling the epidemic to achieve a sustainable response
• Epidemic control requires sustained high coverage of core combination prevention interventions
• Continued aggressive work towards vaccine development is critical
As epidemic control is being achieved, shifting towards greater host country financing and management
True sustainability includes both service delivery and finance
• Sustaining high levels of coverage of core interventions for impact
• Services must include strengthening systems and the full continuum of care – from community to facility
• Sustainable financing including domestic resource mobilization, joint engagement of Departments of Health & Finance, and innovative partnering
Shared Responsibility & Sustainability Epidemic Control is Key to Sustainable Response

Key PEPFAR partners include government, civil society, NGOs, faith based organizations, the private sector, bilateral and multilateral partners including GFATM, UNAIDS, WHO, and the UN family
Strengthen PEPFAR & GFATM Collaboration to achieve decreased costs, greater impact and efficiencies to maximize return on all available resources to fight HIV/AIDS
Private sector mobilization is critical to scaling service delivery and achieving a sustainable response
Shared Responsibility & Sustainability Partnering for Sustainable Impact

PEPFAR IN SOUTH AFRICA

PEPFAR in South Africa: Implemented by
Multiple USG Agencies
PEPFAR
(OGAC)
HHS
HRSA/
NIH
USAID
Dept. of Defense
Dept. of State
Peace Corps
HHS
CDC

More than 120 prime implementing partners including SA government & parastatals, NGOs, FBOs and academic & research institutions
Approx. 80% of the PEPFAR programmatic budget is allocated to local South African entities
PEPFAR works with the following departments at National and Provincial levels:
• Health
• Correctional Services
• National Defense Force (including Military Health Services)
• Social Development
• Basic Education
• Higher Education and Training
• Treasury
• Public Service and Administration
• Women, Children, and People with Disabilities
• International Relations and Cooperation
PEPFAR Partnerships

Partnership Framework
Implementation Plan (PFIP)
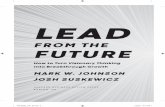
SAG –USG Partnership Framework Implementation Plan (PFIP) signed in August 2012.
Mutually agreed, phased transition of PEPFAR investments from direct clinical care and treatment service delivery to support for system strengthening, prevention, and health services innovation.
PEPFAR investments aligned with priorities outlined in South Africa’s National Strategic Plan for HIV, STIs and TB (2012 – 2016) and other important SAG strategy documents.
Over five years (2012-2017), PEPFAR funding decreases to half historical levels. PEPFAR financial support for NSP decreases from 29% in 2012 to 12% in 2017.

0
2
4
6
8
10
12
14
16
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
SAG (in billions ZAR)
PEPFAR (in billions ZAR)
PEPFAR (in 100 millions USD)
South Africa SAG-USG Funding

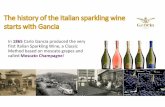
Technical Area 2012 2013 2014 % Change
Biomedical Prevention $ 76,019,692 $ 36,019,690 $ 36,119,690 0%
Sexual Prevention $ 49,346,519 $ 45,358,005 $ 42,990,104 -5%
PMTCT $ 32,044,617 $ 35,924,264 $ 35,488,354 -1%
Adult Care and Treatment $ 165,744,544 $ 147,355,389 $ 125,756,582 -15%
Pediatric Care and Treatment $ 26,157,379 $ 35,929,397 $ 37,004,536 3%
ARV Drugs $ 7,262,801 $ 2,799,022 $ - -100%
Counseling and Testing $ 14,861,764 $ 18,550,280 $ 18,750,280 1%
OVC $ 41,590,878 $ 41,465,878 $ 39,185,255 -5%
Laboratory Infrastructure $ 5,406,676 $ 4,906,676 $ 5,406,676 10%
TB/HIV $ 32,601,260 $ 40,902,529 $ 41,748,480 2%
Subtotal: Prevention, Treatment and Care $ 451,036,130 $ 409,211,130 $ 382,449,957 -7%
Health Systems Strengthening $ 27,446,033 $ 27,464,547 $ 30,000,000 9%
Strategic Information $ 14,830,568 $ 15,418,322 $ 15,317,589 -1%
Management and Operations $ 30,428,120 $ 31,906,001 $ 31,232,454 -2%
Total: All Program Areas $ 523,740,851 $ 484,000,000 $ 459,000,000 -5%
South Africa PEPFAR Funding 2012 to 2014
13

Strategically Focus Prevention Interventions
Expand comprehensive prevention services through geographic targeting to achieve population level coverage including support for:
• HIV Testing & Counseling • Voluntary Medical Male Circumcision • Positive Health Dignity & Prevention (Prevention with HIV+ Persons) • Condom Promotion • Behavioral & Structural Interventions • PMTCT & ART (Through Care & Treatment Partners)
Support select national programs such as medical male circumcision, communications, and surveillance, and strengthen systems/structures that implement and coordinate prevention services including AIDS Councils and Departments of Social Development and Education
Implement Targeted Projects that may fall outside of geographic areas for:
• Key Populations with high prevalence and stigma (e.g. Sex workers, MSM, etc.) • New technologies/innovation (e.g. point of care CD4, Prepex) • Operations Research (e.g. PrEP, microbicides) • Costing and cost effectiveness studies

Comprehensive HIV Care and Treatment
Tailored support to all districts; > 4,000 clinics (majority government)
Comprehensive services including HCT, pediatric & adult HIV care and treatment, TB/HIV and PMTCT
Gradual shift from direct services (equipment, staffing, drugs, etc.) to technical assistance (systems, capacity building & training)
Model: one or two PEPFAR partners per district, with objectives:
• Strengthen testing to treatment cascade including TB
• Improve patient retention and quality outcomes through continuum of care
• Support quality improvement of care and treatment
• Focus on pediatrics and adolescent program support
• Follow mothers and babies through first 1000 days
• Assist with roll-out of Integrated Chronic Disease Model
• Build program management capacity at district level (District Health Management Team)
• Strengthen data and data management at facilities and district level
• Support for supervision, M&E, planning and supply chain

Mitigate the Impact of HIV on OVC and Vulnerable Populations
Transitioned to a focused service delivery program with capacity building technical assistance for DSD
Increase support to manage & strengthen social welfare workforce serving children
Build knowledge base & conduct operations research for evidence based programming
Maintain system strengthening focus and support integration and coordination across Health, Social Development, and Education Departments
Focus funding on reaching the 0-3 age group in vulnerable households & strengthen linkages to treatment programs.

Health System Strengthening
Support supply chain management
• Planning; Provincial pharmaceutical management; Roll out of Rx Solutions; Direct delivery systems for pharmaceuticals
Support for Leadership and Management Academy and standardization of L&M qualifications
Capacity building of clinical pre-service training institutions
Capacity building support to the Regional Training Centers (RTCs)
Cost-effectiveness and operations research to identify best practices in service delivery
Expansion and utilization of SKILLSMART
Capacity building for community health workers to support the ward based outreach teams
Surveillance including supporting improvement of DHIS and core national surveillance systems
Strengthen laboratory services and information systems

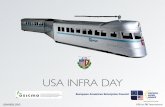
PEPFAR SA Annual Program
Results (2013) & Draft Targets (2014)
Objective Description 2013
Result
% of 2013
Target
2014 Target
2015 Target
Treatment Number of adults and children with advanced HIV infection receiving antiretroviral treatment
2,400,000 96% 3,000,000 3,600,000
PMTCT HTC Number of pregnant women with known HIV status
910,972 92% 1,200,000 1,200,000
PMTCT ARV Number of HIV-infected pregnant women who received antiretrovirals to reduce the risk of mother-to-child transmission
202,555 82% 285,000 285,000
VMMC Number of males circumcised as part of the minimum package of MC for HIV prevention services
295,000 66% 440,000 513,816
Testing and Counseling
Number of individuals who received Testing and Counseling (T&C) services for HIV and received their test results
6,617,300 120% 6,650,000 TBD
OVC Number served by PEPFAR OVC programs for children and families affected by HIV/AIDS 177,000 NA* 105,655 113,568
* Individual OVC Target not set prior to FY2014.