Mental Health Managed Care Outpatient Provider Manual
53
Revised February 2014 Solano County Health & Social Services Mental Health Managed Care Outpatient Provider Manual February 2014
Transcript of Mental Health Managed Care Outpatient Provider Manual

Revised February 2014
Solano County Health & Social Services
Mental Health Managed Care Outpatient Provider Manual
February 2014

Revised January 2014
This page left blank intentionally

Table of Contents
Revised January 2014
Page #
I. Phone and Address Directory ............................................................................................... 1
II. Kaiser Permanente Role in Solano County ..................................................................... 2
III. Definitions and Acronyms..................................................................................................... 3
IV. Access Protocols .................................................................................................................... 5
Screening and Referral (Access) Line ..................................................................................... 5
Assessment Procedures ......................................................................................................... 5
Interpreter Services ............................................................................................................... 5
Access Standards & Monitoring ............................................................................................ 6
Outpatient Authorization ...................................................................................................... 6
Service Authorization Letters ................................................................................................ 6
V. Getting Ready for Referrals .................................................................................................. 6
Outgoing Voicemail Message ................................................................................................ 6
Forms ..................................................................................................................................... 7
Who to Contact ...................................................................................................................... 7
VI. Authorization Criteria and Guidelines ................................................................................. 7
Medi-Cal Medical Necessity Criteria: Outpatient ................................................................. 7
Authorization Guidelines – Psychologist, LCSW, LMFT Providers ......................................... 9
Authorization Guidelines – Psychiatrist Providers .............................................................. 10
VII. Chart Forms/Requirements ................................................................................................ 10
Acknowledgement of Receipt…………………………….…………………………………………………………. 10
Biopsychosocial Assessment…………………………………………………………………………………………. 11
Biopsychosocial Assessment Update………………….…………………………………………………………. 11
Client Services Information Sheet (CSI)…………………………………………………………………………. 11
Closing Summary………………………………………………..…………………………………………………………. 11
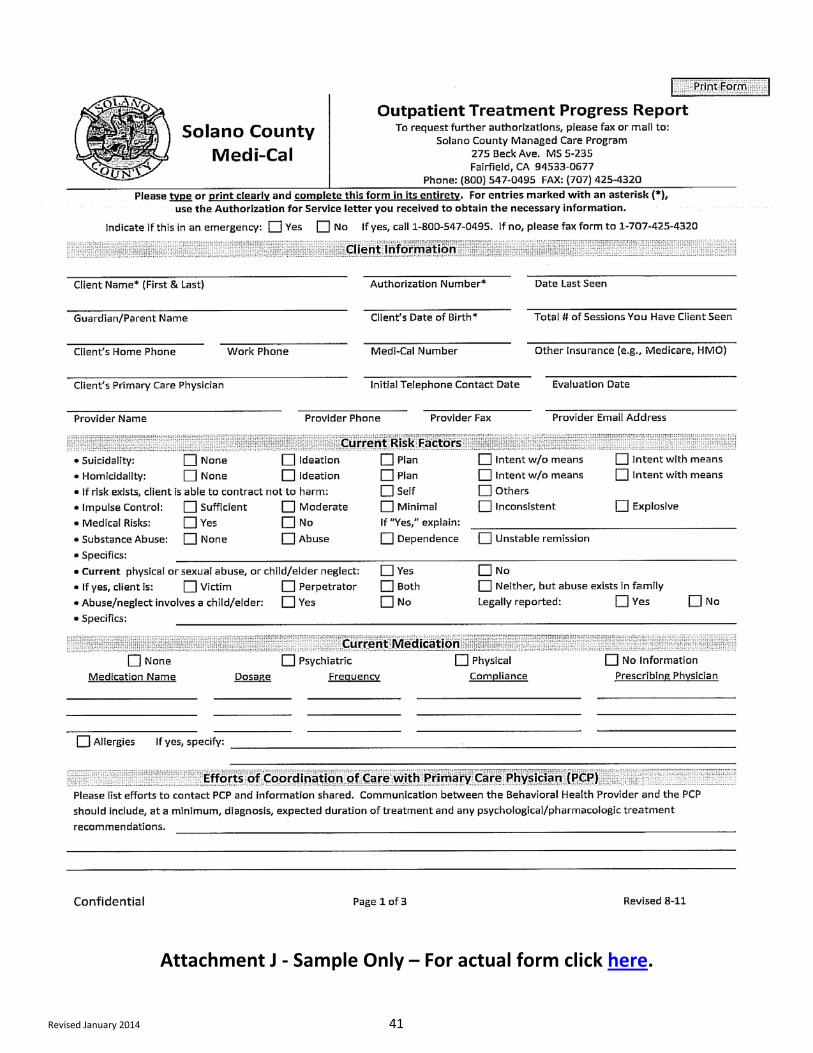
Outpatient Treatment Progress Report……………..…………………………………………………………. 11
Progress Notes……………………………………………………………………………..………………………………. 12
Psychiatric Medication Evaluation/Progress Report..……………………………………………………. 12
VIII. Verifying Eligibility .............................................................................................................. 12
Verifying Member Medi-Cal Eligibility ................................................................................. 12
Share of Cost (SOC) .............................................................................................................. 13
IX. Claims and Billing Instructions ........................................................................................... 13

Table of Contents
Revised January 2014
Page #
Billing Procedures ................................................................................................................ 13
Where to Mail Claims .......................................................................................................... 14
Payment Policies .................................................................................................................. 14
Explanation of Benefit (EOB) Claims Voucher Mailed to Providers Details ........................ 15
Coordination of Benefits ...................................................................................................... 15
Billing Inquiries ..................................................................................................................... 15
Important Points Regarding Claims ..................................................................................... 16
Claims Processing Overview ................................................................................................ 16
X. Provider Responsibilities .................................................................................................... 16
XI. Problem Resolution and Appeals Process .......................................................................... 17
Grievances ............................................................................................................................ 17
Appeals Process ................................................................................................................... 18 Attachments A- Sample Letter to Beneficiary - Initial Authorization for Services 19
B- Sample Letter to Provider - Initial Authorization for Services 20
C- Acknowledgement of Receipt Form 21
D- Biopsychosocial Assessment 23
E- Biopsychosocial Assessment Sample of pages 4-6 29
F- Biopsychosocial Assessment Update 32
G- Client Services Information Sheet (CSI) 36
H- Closing Summary Report 38
I- HCFA CMS-1500 Claim Form 40
J- Outpatient Treatment Progress Report 41
K- Progress Note 44
L- Psychiatric Medication Evaluation/Progress Report 45
M- 2013 CPT Codes, Rates and Service Descriptions 47
All attachments listed above can be found at: http://solano.networkofcare.org/mh/content.aspx?id=293&parentId=290

Revised February 2014 1
I. Phone and Address Directory Claims Submission………………………………………………………………………………..…800-547-0495, Option 4 Mail to: Solano County Mental Health Plan Managed Care Claims Division 275 Beck Avenue MS 5-210 Fairfield, CA 94533 Credentialing Updates………………………………………………………………………………800-547-0495, Option 5 Mail to: Solano County Mental Health Plan Managed Care Credentialing 275 Beck Avenue MS 5-235 Fairfield, CA 94533 Screening, Referral and Customer Services Line……………………………………….800-547-0495, Option 2
Solano County Mental Health Services Crisis Stabilization Unit ..................................................................................................707-428-1131 Managed Care Fax Number ...........................................................................................707-425-4320 Mental Health Plan ........................................................................................................800-547-0495 Provider Forms…………………………………………………………………………………………………………………………..…. http://solano.networkofcare.org/mh/content.aspx?id=293&parentId=290 Resource, Rights and Support Guide for Beneficiaries…….…………………………………………...................... https://admin.solanocounty.com:4433/civicax/filebank/blobdload.aspx?blobid=16876
Partnership HealthPlan of California Information Line ............................................................................................................707-863-4100 Automated Eligibility Verification………………………………………………………..……707-863-4120, Option 3 Or .................................................................................................................. 800-863-4155, Option 3 Member Services (Medi-Cal & Healthy Kids) ................................................................707-863-4120 Or ...................................................................................................................................800-863-4155 Member Services (PartnershipAdvantage) ...................................................................866-264-3626 Care Coordination ..........................................................................................................707-863-4276 Or ...................................................................................................................................800-809-1350 Fax Numbers Main ...............................................................................................................................707-863-4117 Member Services ...........................................................................................................707-863-4415

Revised January 2014 2
II. What role does Kaiser Foundation Health Plan play in providing Mental Health Services?
Kaiser Foundation Health Plan will provide covered Mental Health Services, including assessment, screening, crisis services, outpatient treatment, and medication support for Partnership Health Plan (PHC) Medi-Cal members assigned to Kaiser Foundation Health Plan. Solano Mental Health Plan is responsible for provision of long-term care services; e.g., case management, residential treatment, crisis intervention and Institution for Mental Disease (IMD)/State Hospital care; for PHC Medi-Cal members assigned to Kaiser Foundation Health Plan who meet medical necessity criteria for coordinated services, including:
• Seriously emotionally disturbed children or adolescents; • Adults and older adults who have a serious and/or persistent mental disability which interferes
substantially with primary activities of daily living and which may result in an inability to maintain stable adjustment and independent functioning without treatment, support and rehabilitation for a long or indefinite period of time;
• Adults or older adults who require, or are at risk of requiring, acute psychiatric treatment because of a mental disorder with symptoms of psychosis, suicidality, or danger to self or others.

Revised January 2014 3
III. Definitions and Acronyms The following is a list of terms and their abbreviations as commonly used in this manual
Access Line/Unit: Access to the system of care is through a centralized 1-800 number for all Medi-Cal Beneficiaries seeking mental health treatment. In addition, by calling this number, Providers and Beneficiaries are able to ask questions from the clinical staff about authorization for mental health services, referrals, or express a concern or complaint. A Provider may also call this number to obtain information on claims, and/or contact Provider Relations and member services. Beneficiary: Medi-Cal eligible individual (Solano County resident status) requesting mental health treatment. Parents or a legal guardian may also call to request services on behalf of the Beneficiary. Care Manger: A mental health clinician or nurse who links Beneficiaries to mental health services. Other functions include screening/assessment, authorization, coordination, referral, providing information and education, reviewing ongoing care and making a decision about medical necessity. Primarily talks to Providers, and Beneficiaries regarding mental health services. Medical Necessity: The justification for mental health specialty services. Medical necessity for access to the mental health system is provisionally determined by an initial phone screening by a Care Manager. Medical necessity for ongoing care is based upon the results of an evaluation or progress update, and the agreement of the Care Manager. Medi-Cal: California’s version of the Federal Medicaid program. This is a State and Federal funded health insurance for low-income individuals and families. Mental Health Plan (MHP): An entity that enters into a contract with the California Department of Health Care Services to provide directly or arrange and pay for specialty mental health services to Beneficiaries in a county. A MHP may be a county, counties acting jointly or another governmental or non-governmental entity. Pre-Authorization: Providers must call a Care Manager to obtain authorization for mental health services prior to those services beginning. Outpatient pre-authorization is obtained by calling 800-547-0495. Emergency services do not require pre-authorization. Partnership HealthPlan of California (PHC): A Medi-Cal countywide system, under contract to the State, designed to provide a more economical organization of health care resources on a case management basis and to improve continuity of care. Providers: Licensed mental health professionals that have contracted with Solano County Mental Health Managed Care to provide evaluation and treatment to Medi-Cal Beneficiaries. Provider Relations Coordinator: Managed Care staff member tasked to oversee Provider recruitment, retention and contractual activities and assisting with processing of complaints, concerns and grievances. Screening: The process of triaging callers, checking eligibility, gathering demographic data, determining problem, assessing for emergency, and providing appropriate referral on intervention.

Revised January 2014 4
Share of Cost (SOC): The amount determined by Medi-Cal an individual or family can afford to pay towards medical expenses before Medi-Cal will pay for medical expenses. The individual must meet (pay) the share of cost amount to become Medi-Cal eligible. A person with an unmet SOC is not Medi-Cal eligible.

Revised January 2014 5
IV. Access Protocols
Screening and Referral (Access) Line Assistance is available 24-hours a day, seven days a week by calling 1-800-547-0495.
Note: All Routine Services Must Be Pre-Authorized Access Assessment Procedures Pre-authorization is not required for emergency services. Most Beneficiaries will go to their local emergency room to be evaluated by the Solano County Crisis Stabilization Unit for urgent care; however, if any eligible Medi-Cal Beneficiary/consumer contacts a Provider for emergency services, pre-authorization for treatment is not required. The Provider must contact Solano MHP as soon as possible afterwards to receive retro-authorization for treatment provided. Care Manager will verify eligibility. Calls regarding non-Medi-Cal eligible individuals will be assessed and triaged to an appropriate resource. Kaiser eligibles will be referred to closest Kaiser Behavioral Health Department. Care Manager will obtain information necessary to establish need for assessment and appropriate referral:
• Determine eligibility • Presenting problem • Brief recent treatment history • Current risk factors • Geographic location • Appropriate clinician and specialty areas • Other clinician characteristics requested or deemed appropriate by the Care Manager i.e. gender,
ethnicity, language, other cultural preferences, etc.
Emergency procedures will be utilized as needed, including telephone safety checks, emergency response services triage, child and elder abuse reporting, Tarasoff Warning, etc. Referral to the Solano County Crisis Stabilization Unit may also be facilitated for immediate risk assessment.
A referral will be made based upon level of care required to either an internal Provider or external Provider, or possibly to a community resource. When a referral is made to an external Provider, the caller will be provided with the clinician's name, address, phone number, an authorization number and be instructed to call the clinician for an appointment.
Interpreter Services
• The county will arrange interpreter services for Providers who need to utilize this service. Providers are encouraged to utilize professional interpreters rather than family members. To make arrangements for an interpreter, please call 800-547-0495, Option 5.

Revised January 2014 6
Access Standards and Monitoring Access standards as defined below will be monitored for:
• Urgent assessments: the Provider will schedule appointments within three (3) days. • Routine (non-urgent) outpatient evaluations: the Provider will respond to call from Beneficiary
within five (5) business days and; • The Provider will schedule an appointment within fourteen (14) business days of the Beneficiary’s
call.
Outpatient Authorization Beneficiaries must call the Provider within 30 days from the Authorization Start Date. The Provider has a total of forty-five (45) days from the Authorization Start Date in which to see the Beneficiary or the initial authorization will be invalid. In addition, all other authorizations that have not been used within 12-months from approval date will be invalid.
This policy does not apply to medication management. Authorizations for medication management may be used over a period of 12-months from initial approval date. However, the initial authorization must be used within forty-five (45) days from the authorization start date to remain valid.
Service Authorization Letters A letter will automatically be sent to the Beneficiary, unless Beneficiary requests letter not be sent, which will confirm that an authorization has been made. (See Attachment A for sample)
An authorization letter will also be sent to the Provider confirming the authorization. (See Attachment B for sample)
V. Getting Ready for Referrals Outgoing Voicemail Message As a Provider in Solano MHP Network, you must ensure you have an after-hour message when you are unavailable. All Providers are required to include the following for their outgoing message:
• Name of Provider (including licensure status i.e. MFT, LCSW, etc.) or Agency
• Identify whether the voice mail is confidential/private (or not)
• Emergency contact information including instructions to call 911, or to the nearest ER, or call the Solano County Crisis Services Unit at 707-428-1131.
An example may be: “You have reached the confidential voice mail for John Smith, Licensed Clinical Social Worker. I am unable to take your call at this moment. Please leave your name and phone number with a good time to return your call. If you are experiencing a life threatening emergency, please call 9-1-1 or go to the nearest Emergency Room. If you are a Solano County Medi-Cal Beneficiary and feel you are in crisis, please call their Crisis Stabilization Unit at 707-428-1131.” If you speak more than one language in your practice, you must duplicate the message in all of those languages.

Revised January 2014 7
Forms Forms you will need when meeting a client for the first time:
• Acknowledgement of Receipt (Attachment C, refer to VII. Chart Forms/Requirements on page 11) • Client Services Information Sheet (Attachment G, refer to VII. Chart Forms/Requirements on page
11) • Biopsychosocial Assessment (Attachment D, refer to VII. Chart Forms/Requirements on page 11) • Progress Note (Attachment K, refer to VII. Chart Forms/Requirements on page 12)
All of these can be found under Chart Forms at: http://solano.networkofcare.org/mh/content.aspx?id=293&parentId=290. You will soon receive an informational packet in the mail similar to the one our Beneficiaries receive upon their authorization for services. These forms can also be found at http://solano.networkofcare.org/mh/content.aspx?id=293&parentId=290 under Informing Materials. Please keep this packet on hand for your reference, or in the event that the Beneficiary may ask for a form such as the Grievance Form. Please refer to Section X. Provider Responsibilities on page 16. Who to Contact Call the Access Line at 800-547-0495 and select the appropriate option for any of your needs.
• Option 3: To request additional sessions for a client • Option 4: For claims or payment inquiries • Option 5: To update your contact information, change status of accepting referrals, or for
general inquires.
You can also send an e-mail to: [email protected] for updating your contact information, changing status of accepting referrals, or for general inquiries.
VI. Authorization Criteria and Guidelines
Authorization Criteria
Medi-Cal Medical Necessity Criteria: Outpatient Consumers must meet the following criteria for medical necessity and be Medi-Cal eligible in order for services to be reimbursable. All three criteria – 1, 2, and 3 – must be met.
1) Diagnosis: Included Diagnosis: • Pervasive Developmental Disorders, Excluding Autistic Disorder • Attention Deficit and Disruptive Behavior Disorders • Feeding and Eating Disorders of Infancy or Early Childhood • Elimination Disorders • Other Disorders of Infancy, Childhood, or Adolescence • Schizophrenia and Other Psychotic Disorders • Mood Disorders • Anxiety Disorders • Somatoform Disorders

Revised January 2014 8
• Factitious Disorders • Dissociative Disorders • Paraphilia • Gender Identity Disorders • Eating Disorders • Impulse-Control Disorders Not Elsewhere Classified • Adjustment Disorders • Personality Disorders, Excluding Antisocial Personality Disorder • Medication-Induced Movement Disorder • An Included Diagnosis when an Excluded Diagnosis is also Present
Excluded Diagnosis: • Autistic Disorder • Learning Disorders • Motor Skills Disorder • Communication Disorders • Tic Disorders • Delirium, Dementia, Amnesic, and Other Cognitive Disorders • Mental Disorders Due to a General Medical Condition • Substance-Related Disorder • Sexual Dysfunction • Sleep Disorders • Antisocial Personality Disorder • Other Conditions That May be a Focus of Clinical Attention, Except Medication Induced
Movement Disorders Which are Included • Mental Retardation
2) Impairment Criteria:
Must have one of the following as a result of the mental disorder(s) identified in the diagnostic criteria. • A significant impairment in an important area of life functioning. • A probability of significant deterioration in an important area of life functioning. • Children also qualify if there is a probability the child will not progress developmentally as
individually appropriate.
3) Intervention-Related Criteria: Must have all of the following: • The focus of proposed intervention is to address the condition identified in impairment
criteria • It is expected the Beneficiary will benefit from the proposed intervention by significantly
diminishing the impairment, or preventing significant deterioration in an important area of

Revised January 2014 9
life functioning, and/or for children it is probable the child will progress developmentally as individually appropriate.
• The condition would not be solely responsive to physical healthcare-based treatment Authorization Guidelines – Psychologist, LCSW, LMFT Providers
• Emergency or urgent assessments require immediate phone report by Provider. Complete Biopsychosocial Assessment (Attachment D).
• Sessions may be authorized for a frequency of once per week or other frequency as appropriate and medically necessary. If frequency of more than once per week is required, Provider must obtain prior authorization. The request may be done in writing or by calling 1-800-547-0495 for verbal authorization.
• Beneficiaries must call the Provider within thirty (30) days of the Authorization Start Date. • Provider has a total of forty-five (45) days from the Authorization Start Date in which to see the
Beneficiary or the authorization will be invalid. • For Adult Beneficiaries (18 years or older), authorization is limited to a maximum of eighteen (18)
sessions for the first year and sixteen (16) sessions for subsequent years. • For Child and Adolescent Beneficiaries (17 years or younger), authorization is limited to a maximum
of twenty-four (24) sessions for the first year and twenty-two (22) sessions for subsequent years. Initial Authorization
• Four sessions will be authorized by Access based on the Beneficiary’s provisional diagnosis and impairments.
• Provider submits Biopsychosocial Assessment within four weeks of the Initial Authorization Start Date.
Re-Authorization #1 – First Year of Service • Provider is responsible for requesting additional treatment for the Beneficiary. • Adult Beneficiary: Up to seven (7) additional sessions may be authorized upon submission of the
Biopsychosocial Assessment provided sufficient medical necessity criteria are documented. • Child or Adolescent Beneficiary: Up to ten (10) additional sessions may be authorized upon
submission of the Biopsychosocial Assessment provided sufficient medical necessity criteria are documented.
Re-Authorization #2 – First Year of Service
• To request additional treatment for the Beneficiary, Provider submits Outpatient Treatment Progress Report (Attachment J)
• Adult Beneficiaries: Up to seven (7) additional sessions may be authorized upon submission of the Outpatient Treatment Progress Report provided sufficient medical necessity criteria are documented.
• Child and Adolescent Beneficiaries: Up to ten (10) additional sessions may be authorized upon submission of the Outpatient Treatment Progress Report provided sufficient medical necessity criteria are documented.

Revised January 2014 10
• Providers are encouraged to send the Outpatient Treatment Progress prior to the end of the currently authorized group of sessions to avoid the risk of non-authorization and non-payment of services.
• The standard time for processing an Outpatient Treatment Progress Report is fourteen (14) calendar days after receipt.
Yearly Update
• If the Beneficiary requires further treatment, Provider contacts Care Manager and justifies ongoing medical necessity.
• Two (2) sessions will be authorized by Care Manager. • Provider submits Biopsychosocial Assessment Update (Attachment F) within two (2) weeks of the
Yearly Update Authorization Start Date.
Re-Authorization #1 – Subsequent Year of Service • Provider is responsible for requesting additional treatment for the Beneficiary. • Adult Beneficiary: Up to seven (7) additional sessions may be authorized upon submission of the
Biopsychosocial Assessment Update provided sufficient medical necessity criteria are documented. • Child or Adolescent Beneficiary: Up to ten (10) additional sessions may be authorized upon
submission of the Biopsychosocial Assessment Update provided sufficient medical necessity criteria are documented.
Re-Authorization #2 – Subsequent Year of Service
• To request additional treatment for the Beneficiary, Provider submits Outpatient Treatment Progress Report.
• Adult Beneficiaries: Up to seven (7) additional sessions may be authorized upon submission of the Outpatient Treatment Progress Report provided sufficient medical necessity criteria are documented.
• Child and Adolescent Beneficiaries: Up to ten (10) additional sessions may be authorized upon submission of the Outpatient Treatment Progress Report provided sufficient medical necessity criteria are documented.
Authorization Guidelines – Psychiatrist Provider
• One Medication Evaluation session plus up to eleven Medication Management sessions may be authorized by Access or Care Manager.
• To request additional treatment for the Beneficiary, Provider submits Psychiatric Medication Evaluation/Progress Report (Attachment L).
• Provider has a total of forty-five (45) days from the Authorization Start Date in which to see the Beneficiary or the authorization will be invalid.
VII. Chart Forms/Requirements
Acknowledgement of Receipt A packet is sent to client upon their authorization for services. In addition to the Initial Authorization for Services Letter (Attachment A), clients are sent an informative packet including an Advance Directives Fact

Revised January 2014 11
Sheet, Notice of Privacy Practices, Provider Directory and Guide to Medical Mental Health Services, Grievance Form, Appeal Form, Beneficiary Rights & Problem Resolution Guide, Compliment/Suggestion Form, and Request to Change Service Provider Form. (Some of these forms can be found at: http://solano.networkofcare.org/mh/content.aspx?id=293&parentId=290.) Those forms not posted on the Network of Care Managed Care web page can be requested by calling 800-547-0495, Option 5 or by e-mailing: [email protected].
We require that you have a signed copy of the Acknowledgement of Receipt Form (Attachment C) in each client’s file. By signing this form, our client is acknowledging that they received the information sent in the packet. Please, ask your client to sign it at their first session, and retain it in their file in the event of a future audit. Biopsychosocial Assessment The Biopsychosocial Assessment (Attachment D) is to be completed (legibly) for any new Beneficiary. Please submit to the Care Manager prior to the end of the initial four (4) sessions.
Helpful Hint: Refer to Attachment E, which is an excellent example of how you would complete pages 4-6 of the Biopsychosocial Assessment. Biopsychosocial Assessment Update The Biopsychosocial Assessment Update (Attachment F) is to be completed (legibly) and submitted to the Care Manager within two (2) weeks of the yearly update authorization start date. Client Services Information Sheet (CSI) The Client Services Information Sheet (CSI) (Attachment G) is to be completed (legibly) for any new Beneficiary, or if the Beneficiary’s information needs to be updated. Please submit to the Care Manager prior to the end of the initial four (4) sessions or when information needs to be updated. Closing Summary Providers must complete (legibly) and send a Closing Summary Report (Attachment H) to the Care Managers when treatment is completed, or if member drops out of treatment. Note: The standard time for submitting a Closing Summary Report is fourteen (14) calendar days after
last session. Outpatient Treatment Progress Report The Outpatient Treatment Progress Report (Attachment J) is completed (legibly) and submitted to the Care Manager when requesting additional treatment for the Beneficiary for a second time within a year. Providers are encouraged to send the Outpatient Treatment Progress Report form prior to the end of the currently authorized group of sessions to avoid risk of non-authorization and non-payment of services. It is important to provide sufficient medical necessity criteria to be approved additional treatment. The standard time for processing this form is fourteen (14) calendar day after receipt, and the authorization is valid for up to one (1) year from the authorization start date.

Revised January 2014 12
Helpful Hint: Refer to VI. Authorization Criteria and Guidelines on page 7 for medical necessity criteria. Also, refer to Attachment E, which is an excellent example for how you would complete pages 2-3 of the Outpatient Treatment Progress Report. Progress Notes Progress Notes (Attachment K) are required for each contact with a client and should be retained in the Beneficiary’s chart. Only submit Progress Notes to the Care Manager when you are billing for Case Management Services. They all must be distinct, non-repetitive, and individualized to each session. Solano MHP has a standard Progress Note available or Providers may use their own form. Each note must be legible and include:
• Beneficiary’s (Client) Name • Date, duration, and location of service • An account of the Beneficiary’s culture and language in understanding the Beneficiary’s problems • The client’s diagnosis and related presenting problems, impairments and symptoms, and treatment
objectives. Be sure to document ongoing medical necessity in your reference to these factors • Type of service provided • Intervention(s) used for the service • A distinct, non-repetitive, and individualized report of each session. • Beneficiary’s response to the intervention described • Beneficiary progress toward achieving their identified goal(s) and plans for future treatment • Documentation that justifies the time billed • Referrals to community resources, when appropriate. A list of community resources can be found
in the Resource, Rights and Support Guide for Beneficiaries found on Solano County Mental Health web page at: https://admin.solanocounty.com:4433/civicax/filebank/blobdload.aspx?blobid=16876
• Provider’s printed or stamped name, signature and license type Psychiatric Medication Evaluation/Progress Report The Psychiatric Medication Evaluation/Progress Report (Attachment L) form is used by Psychiatrist Providers to request additional treatment for the Beneficiary.
VIII. Verifying Eligibility Verifying Member Medi-Cal Eligibility Membership Eligibility: Provider is responsible to verify eligibility of Beneficiary for the month of service. Verification is necessary every month for each recipient to assure accurate payments to Providers of mental health care services. This must be accomplished before services are provided.
The Automated Eligibility System can be accessed 24 hours a day – 7 days a week by calling (707) 863-4120, Option 3 or 800-863-4155, Option 3 or by visiting the Partnership HealthPlan of California (PHC) website at http://www.partnershiphp.org/. Please contact Solano County Managed Care Provider Relations at 800-547-0495, Option 5 to request a user name and password.

Revised January 2014 13
If Provider is unable to verify eligibility using the PHC website they may call the PHC Members Services Department (707) 863-4120 or (800) 863-4155. Authorizations for services that cover more than one calendar month do not establish nor guarantee Beneficiary’s Medi-Cal eligibility; it is the Provider’s responsibility to assure that services are provided to eligible Beneficiaries. Individual Medi-Cal eligibility is established monthly by the Department of Social Services. Individual members who are eligible are classified into different "Aid Codes" which represent different Medi-Cal eligibility programs. All Medi-Cal recipients with identification number beginning with County Code "48" (Solano County) who are eligible to receive medical benefits under Medi-Cal or as Medicare/Medi-Cal crossovers are served through the Partnership HealthPlan of California. When a Beneficiary has Medicare and/or other insurance, the other insurance or Medicare must be pre-authorized and billed first. Medi-Cal will only reimburse what the Beneficiary’s other insurance does not cover, up to the allowed Medi-Cal reimbursement amount for the service rendered.
Share of Cost (SOC) Depending upon a person's monthly income, Medi-Cal may determine that they must meet a SOC before Medi-Cal will pay for medical expenses. Therefore, the person may not be eligible for Medi-Cal benefits until their Share of Cost is met.
IX. Claims & Billing Instructions
Billing Procedures Claims must be submitted on the HCFA CMS-1500 Form (Attachment I). Please refer to direction below for each. These forms must be filled out completely and legibly to be processed for payment. HCFA CMS-1500 (Outpatient) Form: The Provider must complete items 1 through 33 on the claim form. Box 1-a Beneficiary’s Social Security Number or CIN
Box 2 Beneficiary’s Last Name, First Name, Middle Initial (if any)
Box 3 Beneficiary’s Date of Birth and Sex
Box 11-c “Solano County Medi-Cal”
Box 12 Either Obtain Signature OR Enter “Signature on File” as appropriate AND Enter Date
Box 17-b Your NPI Number
Box 19 Enter Your Reporting Unit #, Enter a dash “-,” and Enter Your Provider #
Box 21 Minimum of one Covered ICD-9 (same as DSM-IV-TR) Code Enter Code to the greatest diagnostic specificity (include 4th or 5th digit)
Box 23 Enter authorization number from the Authorization for Services Letter

Revised January 2014 14
Box 24-A Date of Service
Box 24-D Procedure Code (CPT Code). Refer to the Service Authorization letter for “Services Authorized” and “Service Codes Allowable”. Refer to Attachment B for sample letter.
Box 24-E If CPT Group Code 90853 is entered in Box 24-D, list number of members in group.
Box 24-F Charges. Refer to Attachment M for the appropriate charges on the list of codes by licensure type.
Box 24-G Units = Number of Minutes (include documentation time)
Box 25 Federal Tax I.D. Number
Box 28 Total Charges for All Services Listed
Box 31 Your Signature and the Date Signed. Signature of Provider must be original (no copies, stamps or “signature on file”).
Box 33 Your Address (where you want check sent) & Phone number
Where to Mail Claims
For Outpatient Claims:
Solano County Mental Health Plan Managed Care Claims Division 275 Beck Avenue MS 5-210 Fairfield, CA 94533
Claims must be received in our Claim's Office within sixty (60) days following the month in which services were rendered. This requirement is referred to as the 60-day billing limit. Claims received after sixty (60) days may be denied.
Claims for family therapy must be billed under the name of the primary Beneficiary.
Payment Policies You have agreed to the Solano County Mental Health Managed Care Medi-Cal fee schedule. Reimbursement levels are determined by the practitioner's licensure (not degree) and the type of service provided.
Medi-Cal guidelines do not allow payment of sessions for which a Beneficiary fails to show.
Medicare/Medi-Cal "Crossover" claims. Services for Solano County Medi-Cal Recipients with Medicare as the primary insurer do need pre-authorization from Solano MHP. Provider must bill Medicare prior to billing Medi-Cal. Ensure a copy of Medicare EOB is attached to claim. Claims must be received within sixty (60) days of EOB date at Solano MHP. Claims are generally paid within thirty (30) days of submission.
Billing Tip: Attach a dated copy of Medicare/HMO EOB for the date of service, to the claim. Payment

Revised January 2014 15
cannot be made without proof of payment/denial from HMO.
Explanation of Benefit (EOB) Claims Voucher Mailed to Providers Details: • Providers name & address • Members’ name • Authorization numbers • Date of service • Amount you billed (your standard rate) • Amount allowed (Medi-Cal Reimbursement Rate) • Other insurance payment • Co-payment • Amount paid • Explanation of Benefit (EOB) code which explains the action taken on the claim or reasons for denial
of submitted charges.
Coordination of Benefits Many Beneficiaries are covered under more than one insurance plan. When this is the case, the “other insurance” is considered to be the Primary Insurer. In order to control health care costs and to prevent overpayment of plan benefits, Solano MHP Medi-Cal Managed Care Program applies standard coordination of benefit rules where applicable.
When Medi-Cal is the secondary insurer, Solano MHP will only reimburse, as the secondary payer, the difference between the Medi-Cal rates for the services billed, minus the payment amount by the primary insurer. The total reimbursement will not exceed Solano MHP Managed Care rates.
Note: (M.D., Ph.D. and LCSW) - If you are not currently a Medicare Provider, you can download a Provider
application at the Centers for Medicare and Medicaid Services website at www.cms.gov or call 855-609-9960 for assistance. If you are treating Medicare/Medi-Cal Beneficiaries, it will be necessary for you to be Medicare authorized so that you will be able to bill Medicare.
Medicare Part B (non-institutional) Medical services for Medicare/Medi-Cal recipients will be reimbursed as explained above, with pre-authorization.
Claims missing the Medicare EOB will be denied.
Billing Inquiries Billing inquiries may be made by calling 800-547-0495, Option 4.
An inquiry is used to reconcile claims that have over or underpayments or to request a tracer or status on a claim line that has not appeared on an EOB.
Inquiry time lines: Providers have six (6) months to inquire about a claim from the original date of the denial on the Solano MHP EOB. Inquiries made after six months are subject to denial.

Revised January 2014 16
If the issue is not resolved, the Provider may submit an appeal within ninety (90) days inquiry. See Section XI: Problem Resolution and Appeals Process.
Important Points Regarding Claims Treatment of any Medi-Cal Beneficiary must be performed by the practitioner to whom the referral was made. You may not bill in your name for treatment provided by another practitioner or an assistant.
You may not in any case bill the Beneficiary for amounts above the Medi-Cal rate.
Solano MHP will not reimburse for covered services that were improperly submitted to other insurance carriers.
Claims Processing Overview All incoming paper claims and other documents are date stamped.
All claims are subject to a comprehensive series of edits and audits by Claim Representative. Claims missing pertinent information e.g., Beneficiary name, procedure codes, diagnosis codes, or billing amount will be returned to Provider with a cover letter identifying missing information or other problems. Claims that are denied are included on the Explanation of Benefits, (EOB) along with the reason why the claim was denied.
Billing Tip: Ensure each claim submitted is fully completed.
X. Provider Responsibilities Medi-Cal Beneficiaries receiving or seeking mental health services shall be informed of how to access the Problem Resolution process. They shall be provided or have easy access to brochures for Beneficiary Rights, Appeal Form, Grievance Form, and Request to Change Provider Form. These forms are mailed to the Beneficiary upon first request for service. Beneficiaries shall be informed of their right to access advocate assistance if they wish to submit a grievance, appeal or expedited appeal at any time during the problem resolution process. Beneficiaries must also be informed of their option to request a State Fair Hearing.
At the request of the Provider, Solano MHP will assist in the education and/or training of Providers and their staff in Medi-Cal billing procedures.
Treatment shall be provided in a culturally competent manner by providing services in a language appropriate and culturally sensitive manner, in a setting accessible to diverse communities. Contact Solano MHP if you desire a copy of the Solano County Mental Health Services Cultural Competence Plan.
Notify Beneficiaries they are entitled to the following rights: • Respectful treatment by all mental health staff • Service provided in a safe environment • Informed consent to treatment and informed consent to prescribed medications and options

Revised January 2014 17
available • Protection of personal health information • Participate in treatment planning • Request a change in the level of care, change of therapist, and a second opinion • Consideration of a problem or concern about services by the staff person or agency providing care • File a Grievance regarding services • File for a State Fair Hearing following an Action • File an Appeal regarding an Action • Delegate a person to act on their behalf during the Grievance, Appeal or State Fair Hearing process • Culturally sensitive services • Use of an interpreter at no cost • Request and receive a copy of his/her medical records, and request they be amended or corrected • Be free from any form of restraint or seclusion used as a means of coercion, discipline, convenience,
or retaliation • The right to an Advanced Health Directive
XI. Problem Resolution and Appeals Process
Problem Resolution and Appeals Process These procedures are designed to enable Providers to resolve complaints or concerns about authorizations, claims, or other issues. Solano County Mental Health Plan will make every effort to utilize informal problem resolution whenever possible. Informal Problem Resolution A Provider can call the Access line at (800) 547-0495 to register a complaint or concern and discuss informal problem resolution. A Provider may also submit a complaint or concern in writing to: Solano County Mental Health Plan Managed Care Provider Relations Coordinator 275 Beck Ave., MS 5-235 Fairfield, CA 94533 Within five working days, the Provider will be contacted by either the Managed Care Provider Relations Coordinator or the Managed Care Clinical Supervisor to discuss actions, plans, etc. to resolve the problem. Grievance Process A Provider may register a grievance if the complaint or concern is not resolved informally to the Provider’s satisfaction. Grievances are to be filed in writing to: Solano County Mental Health Plan Managed Care Provider Relations Coordinator 275 Beck Ave., MS 5-235 Fairfield, CA 94533

Revised January 2014 18
There shall be a twenty-five (25) working day resolution period during which time Solano County Mental Health Plan staff shall prepare a resolution to the Provider in writing. If the proposed resolution is not satisfactory, the Provider may request a meeting of the Grievance Review Committee. The Grievance Review Committee is composed of the Managed Care Program Manager or designee, Medical Director or medical staff designee, and two Mental Health Providers Members (licensure based on circumstance of complaint and/or licensure level of grievant). The committee will meet monthly based on need. A hearing will be scheduled to review the grievance at the earliest possible date. Decisions of the Grievance Review Committee are binding unless reversed through the appeal process. Appeals Process A Provider may file a written appeal when the complaint or concern involves (a) an authorization or (b) the processing or payment of a claim. The appeal must include all supporting documentation regarding the Provider’s complaint or concern. Providers have the right to access the appeals process--before, during, or after an informal or grievance process. The written appeal should be submitted to: Solano County Mental Health Plan Provider Appeals Coordinator 275 Beck Ave., MS 5-250 Fairfield, CA 94533 The written appeal must reach Solano County Mental Health Plan within ninety (90) calendar days of the authorization decision or the dispute regarding the claim. Solano County Mental Health Plan will have sixty (60) calendar days from receipt of the appeal to inform the Provider in writing of the decision. This will include a statement of the reasons for the decision that addresses each issue raised by the Provider and any action required by the Provider to implement the decision. Solano County Mental Health Plan will also provide the name of a person who may be contacted regarding the status of the appeal. Solano County Mental Health Plan will utilize personnel not involved in the initial decision to determine the appeal decision. If the appeal is upheld, the Provider Appeals Coordinator will notify the Provider of the decision. The Provider shall submit a revised authorization request or claim to the Managed Care Unit within thirty (30) calendar days from receipt of the Provider Appeals Coordinator’s decision. If the appeal is denied or not granted in full, the Provider will be notified of his/her further right (second level appeal) for review. If a second level appeal is requested, the Provider must submit the request within thirty (30) days of receipt of the appeal denial to the Solano County Behavioral Health Director. The Provider will be notified in writing within sixty (60) days of the Provider’s appeal to the Behavioral Health Director of his/her decision. The decision of the Behavioral Health Director shall be final. If the Behavioral Health Director upholds the Provider’s appeal, Solano County Mental Health Plan will have fourteen (14) calendar days to take any other corrective action described within the decision. The Provider may be requested to submit a revised claim under the circumstances of specific decisions by the Behavioral Health Director.

Revised January 2014 19
Attachment A - Sample Only

Revised January 2014 20
Attachment B - Sample Only

Revised January 2014 21
COUNTY OF SOLANO DEPARTMENT OF HEALTH & SOCIAL SERVICES MENTAL HEALTH DIVISION
Acknowledgement of Receipt
I have received the following items at the start of service with this Provider. In addition, I understand that I may receive any of the following information upon request. I have also been informed that alternative formats are available and have been given information on how to access these formats:
Initial all that apply
Document Provided
Mental Health Service Provider Notice of Privacy Practices The Notice of Privacy Practices tells you how your Mental Health Service Provider may use or disclose information about you. Not all situations will be described. As your Mental Health Service Provider, we are required to give you a notice of our privacy practices for the information we collect and keep about you.
Solano County MHP “Guide to Medi-Cal Mental Health Services” The MHP “Guide to Medi-Cal Mental Health Services” contains information on how a member is eligible for mental health services, how to access mental health services, who our service providers are, what services are available, what your rights are, our Grievance and State Fair Hearing process and includes important phone numbers regarding our Mental Health Plan.
Advance Directive Fact Sheet The Advance Directive Fact Sheet explains your rights to make decisions about your medical treatment. It includes how to appoint a health care agent who can make decisions on your behalf and how to change your directives at anytime.
Do you have an Advance Directive?
Please circle one:
Yes
No
N/A
If Yes, can you provide a copy for our
Medical Records?
Please circle one:
Yes
No
N/A
Solano County MHP Provider List The MHP Provider List is a list of MHP Providers in our community. You may contact the MHP Access Unit at 1-800-547-0495 for further information regarding this list of Providers.
I, , (Print Client Name) have been given a copy of the above-initialed documents and have had a chance to ask questions regarding these documents.
Client Signature: Client Number: Date:
Signature of Legal Representative of Client (If applicable): Relationship to Client: Date:
Revised February 2012
Attachment C - Sample Only – For actual form click here.

Revised January 2014 22
DEPARTAMENTO DE SERVICIOS SOCIALES Y DE SALUD DEL CONDADO DE SOLANO DIVISIÓN DE SALUD MENTAL
Acuse de recibo
Cuando este proveedor comenzó a prestar sus servicios, recibí los siguientes artículos. Además, entiendo que puedo recibir cualquier información de la siguiente si así lo deseo. Yo también he sido informado que formatos alternativos están disponibles y han sido dado información en cómo conseguir acceso a estos formatos:
Firme con
sus iniciales todo lo que
corresponda
Documento entregado
Notificación de Prácticas de Privacidad del Proveedor de Salud Mental La Notificación de Prácticas de Privacidad le informa de qué manera el Proveedor de Salud Mental puede usar o divulgar información acerca de usted. No se describirán todas las situaciones. Proveedor de Salud Mental debe brindarle una notificación de nuestras prácticas de privacidad para la información que reunimos y guardamos sobre usted.
“Guía para los servicios de salud mental de Medi-Cal” del Plan de Salud Mental (Mental Health Plan, MHP) del Condado de Solano La “Guía para los servicios de salud mental de Medi-Cal” del MHP contiene información sobre cómo un miembro es elegible para los servicios de salud mental, cómo acceder a los servicios de salud mental, quiénes son nuestros proveedores de servicios, qué servicios están disponibles, cuáles son sus derechos, nuestro proceso de Quejas y Audiencia Estatal Imparcial, e incluye números de teléfono importantes relacionados con nuestro Plan de Salud Mental
Hoja informativa sobre las directivas anticipadas La hoja informativa sobre las directivas anticipadas le explica sus derechos para tomar decisiones sobre su tratamiento médico. Incluye información sobre cómo nombrar un agente para el cuidado de la salud que pueda tomar decisiones en su nombre y cómo cambiar las directivas en cualquier momento.
¿Tiene una directiva anticipada?
Encierre con un círculo una
ió
Si
No
N/A
Si la respuesta es Sí, ¿puede brindarnos una
copia para nuestros expedientes médicos?
Encierre con un círculo una
ió
Si
No
N/A
Lista de proveedores del MHP del Condado de Solano La lista de proveedores del MHP es una lista de los proveedores del MHP en nuestra comunidad. Puede comunicarse con la Unidad de Acceso del MHP al 1-800-547-0495 para obtener más información acerca de esta lista de proveedores.
Yo, , (nombre del cliente en letra de imprenta) he recibido una copia de los documentos que firmé con mis iniciales anteriormente y he tenido la oportunidad de hacer preguntas relacionadas con dichos documentos.
Firma del cliente: Número de cliente: Fecha:
Firma del representante legal del cliente (si corresponde): Relación con el cliente: Fecha:
Revised February 2012 Attachment C - Sample Only – For actual form click here.

Revised January 2014 23
.
Attachment D - Sample Only – For actual form click here.

Revised January 2014 24
Attachment D - Sample Only – For actual form click here.

Revised January 2014 25
Attachment D - Sample Only – For actual form click here.

Revised January 2014 26
Attachment D - Sample Only – For actual form click here.

Revised January 2014 27
Attachment D - Sample Only – For actual form click here.

Revised January 2014 28
Attachment D - Sample Only – For actual form click here.

Revised January 2014 29
Attachment E - Sample Only

Revised January 2014 30
Attachment E - Sample Only

Revised January 2014 31
Attachment E - Sample Only

Revised January 2014 32
Attachment F - Sample Only – For actual form click here.

Revised January 2014 33
Attachment F - Sample Only – For actual form click here.

Revised January 2014 34
Attachment F - Sample Only – For actual form click here.

Revised January 2014 35
Attachment F - Sample Only – For actual form click here.

Revised January 2014 36
Attachment G - Sample Only – For actual form click here.

Revised January 2014 37
Attachment G - Sample Only – For actual form click here.

Revised January 2014 38
Attachment H - Sample Only – For actual form click here.

Revised January 2014 39
Attachment H - Sample Only – For actual form click here.

Revised January 2014 40
Attachment I - Sample Only – For actual form click here.
Revised January 2014 41
Attachment J - Sample Only – For actual form click here.

Revised January 2014 42
Attachment J - Sample Only – For actual form click here.

Revised January 2014 43
Attachment J - Sample Only – For actual form click here.

Revised January 2014 44
Attachment K - Sample Only – For actual form click here.

Revised January 2014 45
Attachment L - Sample Only – For actual form click here.

Revised January 2014 46
Attachment L - Sample Only – For actual form click here.

Revised January 2014 47
Attachment M

Revised January 2014 48
Attachment M

Revised January 2014 49
Attachment M