Mandibular Growth Anomalies || Parts of the Facial Skeleton
7
CHAPTER 3 Parts of the Facial Skeleton In order to make things easily understandable I will use the following terms in the discussion of the subject. I will talk about the mandible meaning the whole lower jaw and about the maxilla, the upper jaw. From my point of view the chin has to be evaluated separately, as do the zygomatic bones (zygoma) or the nasal framework (nose) or the frontal bone. Primarily it seems very important that in the termi- nology one distinguishes between the base of the jaw, and the alveolus and the occlusion. Therapeutically, there are several different anatomical sections of each jaw which have to be considered. In spite of a normal mandibular base, and on top of it a normally formed and situated alveolus, an occlusal anomaly may exist for solely dental reasons. In this description I will not in- clude any malpositioning of the teeth within an alveolus which is normal in shape, size and position on the base of that jaw. I will only include anomalies of the bony parts of the jaws and will talk about the angulation of the teeth in relation to their pertinent jaw base. The term "norma-" will be used to describe the max- illa, the mandible, the chin, the zygomas, the nose and the frontal bone which are normal in size, shape and po- sition and in relation to the other facial skeletal parts and normal for that specific patient. With other expres- sions a specific name will refer to what, in my opinion, is abnormal. So all the terminology to be suggested has, as a pre- requisite, the necessity to first establish the ideal profile for the patient in question. 3.1 The Mandible The mandible normally consists of two equal halves, ex- tending from the symphysis up to the condylar and co- ronoid processes. The symphysis is the fusion line of the two mandibular halves. Each half is called a hemiman- dible. Its length extends from the symphysis to the artic- ular surface of the condylar process. The term "parasymphysis" is often used in the USA to describe the area lateral to the symphysis. However, such a term does not exist in anatomical textbooks. Al- though that term is used to describe a part of the chin of one side it is still not equal to half of the chin promi- nence. In general we talk about a parasymphyseal area where a specific pathology may be located. But we do not use the term "parasymphysis" in the description of man- dibular anomalies nor in orthognathic surgery at all. The surgeon who has to deal with the many different shapes and positional anomalies of the mandible, while respecting the position of the teeth and the occlusion, will soon recognize that in diagnosis and treatment, one cannot just use the term "mandible" since it consists of several different parts: the horizontal ramus, consisting of the body or base of the mandible and the alveolar process (with the teeth), the chin and the ascending ra- mus with the condylar and coronoid processes. Their shape and position in relation to each other has to be clearly evaluated in order to make the diagnosis and to plan the proper treatment of the case. Surgery may ei- ther move the whole mandible, almost never including the condylar processes, or only parts of it. 3.1.1 Anomalies of the Mandible I use the term normomandibulism to describe a man- dible normal in length, width, height and position rela- tive to the other facial skeletal parts. Therefore by the term retromandibulism I mean such a mandible in which the horizontal rami are short as if they were shift- ed into the ascending rami, while in antemandibulism they seem to be "pulled out" of the ascending ramus as is done in the sagittal splitting procedure for advance- ment. The term micromandibulism means that the man- dible is small in all dimensions, as in the bird face ap- pearance, while in macromandibulism the mandible is large in all three dimensions. We talk about mandibular asymmetry when the two halves of the mandible are un- equal as in hemimandibular hyperplasia or hemiman- dibular elongation. In lateromandibulism the mandible is shifted to one side, both halves being of equal length. Combinations do, of course, occur. 3.1.2 The Horizontal Ramus The most important part of the mandible is its horizon- tal ramus. Its shape and position mainly determine the H. L. Obwegeser, Mandibular Growth Anomalies © Springer-Verlag Berlin Heidelberg 2001
Transcript of Mandibular Growth Anomalies || Parts of the Facial Skeleton

CHAPTER 3
Parts of the Facial Skeleton
In order to make things easily understandable I will use the following terms in the discussion of the subject. I will talk about the mandible meaning the whole lower jaw and about the maxilla, the upper jaw. From my point of view the chin has to be evaluated separately, as do the zygomatic bones (zygoma) or the nasal framework (nose) or the frontal bone.
Primarily it seems very important that in the terminology one distinguishes between the base of the jaw, and the alveolus and the occlusion. Therapeutically, there are several different anatomical sections of each jaw which have to be considered. In spite of a normal mandibular base, and on top of it a normally formed and situated alveolus, an occlusal anomaly may exist for solely dental reasons. In this description I will not include any malpositioning of the teeth within an alveolus which is normal in shape, size and position on the base of that jaw. I will only include anomalies of the bony parts of the jaws and will talk about the angulation of the teeth in relation to their pertinent jaw base.
The term "norma-" will be used to describe the maxilla, the mandible, the chin, the zygomas, the nose and the frontal bone which are normal in size, shape and position and in relation to the other facial skeletal parts and normal for that specific patient. With other expressions a specific name will refer to what, in my opinion, is abnormal.
So all the terminology to be suggested has, as a prerequisite, the necessity to first establish the ideal profile for the patient in question.
3.1 The Mandible
The mandible normally consists of two equal halves, extending from the symphysis up to the condylar and coronoid processes. The symphysis is the fusion line of the two mandibular halves. Each half is called a hemimandible. Its length extends from the symphysis to the articular surface of the condylar process.
The term "parasymphysis" is often used in the USA to describe the area lateral to the symphysis. However, such a term does not exist in anatomical textbooks. Although that term is used to describe a part of the chin of one side it is still not equal to half of the chin promi-
nence. In general we talk about a parasymphyseal area where a specific pathology may be located. But we do not use the term "parasymphysis" in the description of mandibular anomalies nor in orthognathic surgery at all.
The surgeon who has to deal with the many different shapes and positional anomalies of the mandible, while respecting the position of the teeth and the occlusion, will soon recognize that in diagnosis and treatment, one cannot just use the term "mandible" since it consists of several different parts: the horizontal ramus, consisting of the body or base of the mandible and the alveolar process (with the teeth), the chin and the ascending ramus with the condylar and coronoid processes. Their shape and position in relation to each other has to be clearly evaluated in order to make the diagnosis and to plan the proper treatment of the case. Surgery may either move the whole mandible, almost never including the condylar processes, or only parts of it.
3.1.1 Anomalies of the Mandible
I use the term normomandibulism to describe a mandible normal in length, width, height and position relative to the other facial skeletal parts. Therefore by the term retromandibulism I mean such a mandible in which the horizontal rami are short as if they were shifted into the ascending rami, while in antemandibulism they seem to be "pulled out" of the ascending ramus as is done in the sagittal splitting procedure for advancement. The term micromandibulism means that the mandible is small in all dimensions, as in the bird face appearance, while in macromandibulism the mandible is large in all three dimensions. We talk about mandibular asymmetry when the two halves of the mandible are unequal as in hemimandibular hyperplasia or hemimandibular elongation. In lateromandibulism the mandible is shifted to one side, both halves being of equal length. Combinations do, of course, occur.
3.1.2 The Horizontal Ramus
The most important part of the mandible is its horizontal ramus. Its shape and position mainly determine the
H. L. Obwegeser, Mandibular Growth Anomalies© Springer-Verlag Berlin Heidelberg 2001

18 CHAPTER 3 Parts of the Facial Skeleton
appearance of the face. It includes the body and the alveolar process. Its vertical dimension, called its height, consists of the body or base of the mandible and the alveolar process, with or without teeth.
Its inferior horizontal dimension, its actual length, extends in the lateral cephalogram from the G-point of the angle to the symphysis (Sy) which is synonymous with the mental protuberance (Pg-point). In order to be able to compare measurements between right and left hemimandibles the cephalograms (lateral and p.a. projection) are useless.
On the panoramic radiograph we will use that Pgpoint in the chin area, generally recognizable as a whitish spot, in measurement of the length of the horizontal ramus. The length of the horizontal ramus (HRL) is measured from that Pg-point to the G-point, the most dorsal point (lateral on the OPT) of the angle. Thus we can compare the length of the left and right body of the mandible.
Its superior horizontal dimension is measured from a point in the symphysis region at the level of the apices of the first incisors (B-point) to the curvature in the retromolar region (Rm-point). It is equal to the length of the alveolar process. The inferior length of the horizontal ramus is important for the profile evaluation while its upper length is important for the space available for the teeth. The difference between the upper and inferior lengths varies naturally from one patient to another, depending on the breadth of the ascending ramus. But it can also vary between left and right in the same patient.
The horizontal ramus can be normal in length, or longer or shorter than normal. Its height can be normal or can be smaller or greater (lower or higher than normal). By the term "thickness" of the horizontal ramus we mean the medio-lateral width of the body. It might be normal, or thin (slim) or thick (bulky). By "anterior mandibular height" is meant the full height of the chin including the alveolus in the vertical dimension.
3.1.3 The Mandibular Body or Base
The mandibular body, or base, is defined (Reed and Sheppard 1976) as that part of the horizontal ramus which extends from the lower border of the mandible to the mental foramen. As it is measured as length we need an upper line not just the foramen. In my definition the mandibular body is that part of the horizontal ramus which extends from its inferior border to the upper border of the mandibular canal and its anterior branch. That distance, in the vertical dimension, is called the body height (BH). I define the extent or length of the body from the G-point to the Pg-point. It is equal to the horizontal ramus length (HRL). The alveolus with its teeth sits on top of the mandibular body or base.
3.1.4 The Ascending Ramus
The ascending ramus, often just called the ramus, follows the horizontal ramus dorso-cranially. It begins at the angle of the mandible at its most inferior point (Agantegonial point) where in most cases the convexity of the angle usually turns into a slight concavity of the horizontal ramus, and ends at the highest point of the articular surface of the condylar process (HC-highest point of the condyle). That distance is called the height (or length) of the ramus. The ramus can also vary in form and volume and so can the angle which is formed together with the mandibular body.
When discussing with American and British friends the shape and size of the different parts of the mandible, I found great difficulties in expressing myself to their satisfaction in these usages. While the British often talk about the length of the ascending ramus, the Americans call it its height, as we do in the German language. So, ramus height and ramus length are the same. Because of these differences it seems necessary to define strictly the meaning of the different adjectives used.
For measurement reasons the ascending ramus must be divided into several clearly distinguishable parts as in unilateral growth anomalies we want to know in which section of the ramus the abnormal growth takes place. The main part I will call the trunk of the ramus. Its height or length (TL) I define as the distance from the Ag-point to the most inferior point of the semilunar notch (I name it IS-point, derived from its Latin name incisura semilunaris). It can be normal or longer (higher) or shorter in relation to its processes or to the body or the other facial skeletal parts.
Its lateral aspect is its breadth or width while its meclio-lateral measurement is called the thickness. The width can be normal or wider or narrower than normal. Its thickness can be normal or thicker or thinner or slim.
On top of the trunk are the articular and the coronoid processes. They are not just a part of the ramus. They must be clearly distinguished from the ramus. The horizontal and ascending rami together form the mandibular angle.
3.1.5 The Articular (Condylar) Process
The articular process consists of the condylar head, I will just use the term "condyle", and the condylar neck. For the latter I will just use the word "neck". They are diagnostically and from the therapeutic point of view of special interest and importance. The length of the neck (NL) of the condylar process extends from its base up to the base of the condyle, which I define as the insertion

of the condylar capsule. On the radiograph this is not recognizable. As the base of the condylar neck I define a perpendicular line from the IS-point to a tangential line along the neck's posterior surface. Occasionally there is a type of a bend formation between the neck and the trunk. In such a case a line from the IS-point to the middle of that bend may be used to define the base of the neck. The length of the neck may be within average or normal, or it may be short or long or clearly elongated. The neck's antero-posterior dimension is called breadth or width (WN). It may vary from average to thick or slim (thin).
Within the range of normal, the condyle appears in great variations in its size and shape. In spite of its great variations within normal, it is often possible to call a condyle enlarged or reduced in size, in particular in relation to the condyle of the other side.
3.1.6 The Muscle (Coronoid) Process
The muscle process also exists, within the range of normal, in variations of size and forms. Nevertheless, occasionally it is clearly shorter or longer than normal and smaller or larger in its width (antero-posterior dimension) at its base. It extends from its base up to its tip. As
the base of the coronoid process (CPB) I define a perpendicular line from the IS-point to a tangential line along its anterior contour. Its end may be normal somewhat or very pointed, or rounded. Its thickness does not need to be described specially.
Clinically, the coronoid process does not play an important role in facial skeletal anomalies, whatever its shape may be. Only cases with remarkable elongation of the coronoid process may cause problems because of the resulting restricted mouth opening. This problem, often wrongly called "coronoid hypertrophy", instead of "coronoid elongation", seems to develop before or during pubertal growth, independent of any other facial skeletal anomaly. If a patient does not have an incisal opening of more than 25 mm, without any obvious joint, muscular or other soft tissue origin, elongation of the coronoid processes must be considered. It is mostly bilateral, but occurs also unilaterally. The diagnosis is simple. When forced mouth opening is absolutely blocked, with restricted opening as mentioned, one has to think of coronoid elongation. The panoramic radiograph will clarify this situation.
The problem is usually solved by cutting through the coronoid processes, without removing them. Postoperative opening exercises are very necessary until normal mandibular opening is secured. These exercises will create scar tissue in a position that will not interfere with the mouth opening.
3.1 The Mandible 19
3.1.7 The Angle of the Mandible
The angle of the mandible is formed by the confluence of the body and the ascending ramus. Both play an important part in its formation. No distinct line, natural or constructed, demarcates the two from each other, nor is such a demarcation necessary. When measuring the length of the ramus or the body we just include the angle area of the other. Anteriorly, the angle starts at the curvature in the retromolar area (Rm-point). Posteriorly, we include visually the G-point.
The angle can vary quite a bit in its shape and angulation. In the average adult, that angle should be about 124° (±6°) in the male and 122° (±4°) in the female. Therefore, we will talk about a normal angulation or a stretched or pronounced or distinct angle. Its protuberance can be within the normal range, or flat (as in some hemimandibular elongation cases) or protruding (as often found in cases with masseter hypertrophy). The medio-lateral dimension of the angle area may be thick or thin or normal.
3.1.8 The Chin and Its Anomalies
Although the chin does not seem to have its own embryogenetic development, independent of the base of the mandible, it can be variable in its form and consequently deserves independent special corrective surgery. It is located in front of the mandibular base. I determine it by a vertical line drawn from the Frankfort plane to point B (as defined on the lateral cephalogram) extending to the inferior border of the horizontal ramus. From point B downwards we call it the height of the chin and from that vertical line forwards or backwards it is called the prominence of the chin. The chin extends laterally from one mental foramen area to the other.
As mentioned previously, chin anomalies have to be evaluated independently. Normogenia refers to a chin prominence that is adequate in height, projection and width in relation to the mandible. In antegenia such a chin prominence is too far forward, while in retrogenia the prominence is too far back. In macrogenia the chin prominence is too large in all three dimensions and in microgenia too small. In laterogenia the prominence is shifted to one side. Hypergenia and hypogenia describe a chin prominence which is too high (deep) or not high enough (shallow) in the vertical dimension but otherwise normal in shape, width and position. Unfortunately, the chin prominence does not depend on its skeletal elements alone. In addition, variations may exist in soft tissue thickness in the chin region, which require either

20 CHAPTER 3 Parts of the Facial Skeleton
a reduction or increase in its thickness or even a displacement. Combinations of the various skeletal elements and soft tissue configurations from normal to abnormal also exist.
3.1.9 Measuring the Mandible
In asymmetrical mandibular growth anomalies we must be able to compare every section of the two hemimandibles in order to diagnose where the unilateral anomaly becomes abnormal compared with the other side. The various sections of the mandible have to be clearly defined for determining which part is mainly influenced by the abnormal growth, and to what extent.
The panoramic view is the best routinely taken radiograph which permits comparison of the two halves of the mandible. Radiographs should not be used to evaluate cases when distortions, due to technical origins, are noted.
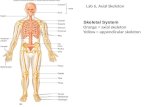
I am fully aware that some radiographs will not allow all necessary measurement points to be determined precisely, particularly for the articular process. As we know that mandibular asymmetry due to misregulation of condylar growth activity has its origin located close to the surface of the condyle, we are very interested to learn how the individual condyle reacts in its size and shape due to the hyperactivity of one or the other or both condylar growth regulators. As it is not possible to determine the base of the condyle on the radiograph, only the length of the whole condylar process and the width (anterio-posterior extent) of the condyle and its neck can be measured. Accurate measurements of the length and width of the various parts can be obtained on tracings of high-quality panoramic radiographs. For this, measuring points generally known in the evaluation of the lateral cephalogram can be used along with the addition of new measuring points (Fig. 4).
Measurement Points
G: gonion point, the most dorsal point of the angle Pg: pogonion point, equivalent to the mental protu
berance, in most radiographs visible as a whitish spot
B: point in the symphysis region at the level of the apices of the first inferior incisors
Sy: symphysial point, most inferior point of the symphysis just below the Pg
Ag: antegonion point, most inferior point of the angle
HC: height of condyle point, most cranial point of the condylar surface
IS: incisura semilunaris point, the most inferior point of the semilunar notch
CP: coronoid process point, tip of the coronoid process
AL: alveolar point, the highest point of the alveolar crest
Rm: retromolar point, anterior begin of the angle of the mandible
Measurable Lengths
HRL: horizontal ramus length, from pogonion to gonion point
HRH: horizontal ramus height, from inferior border to the crest top of the alveolus. One has to define in which area the measurement was taken
BH: body height, from inferior border to cranial line of the mandibular canal
AH: alveolus height, from cranial line of mandibular canal to crest top of the alveolus. One has to define in which area the measurement was taken
ARL: ascending ramus length, from Ag-point to HCpoint (highest point of condyle)
TL: length of trunk of the ascending ramus, from Ag- to IS-point
Fig. 4. On the tracing of a panoramic radiograph all wanted measurement points and measurable lengths are shown

APL: articular process length, from base of neck to HC-point
APB: articular process base, from IS-point to the most anterior point of the posterior ramus border
NB: neck base, equal to APB NL: neck length, from NB to base of condyle WN: width of condylar neck, the smallest distance
between the anterior and posterior surface of the neck
WC: width of condyle, the largest antero-posterior distance of the condyle
CPB: coronoid process base, a perpendicular line from IS-point to a line tangenital to the anterior ramus rim
CPL: coronoid process length, from CPB- to CP-point AHL: articular fossa height line, line between the
height of the two articular fossae MSE: maxillary sinus extension, most inferior exten
sion of the maxillary sinus from AHL
The angle on the affected side can change greatly, owing to condylar hyperactivity. Therefore the non-affected side should be compared with the affected one. The gonial angle can be accurately measured only on the lateral cephalogram or on good sagittal tomograms. The lateral cephalogram is of no use for comparing the left with the right side, except when the left and right horizontal and ascending rami can be very clearly distinguished. Knowing that the size of the angle on the panoramic view does not permit any conclusion regarding its actual measurement, comparison of the left and right sides can be done on that radiograph.
In some cases, in addition to the panoramic radiograph, good TMJ-ramus tomograrns and lateral cephalograms allow the two sides to be clearly distinguished. Unexpectedly large differences have been found in measuring the angles on the three radiographic projections. The measurements on the lateral cephalogram and on the TMJ-ramus tomogram were most likely to be similar, but the measurements of the angles on the panoramic view could differ by as much as 10° in comparison with the two other possibilities. The most accurate measurement is achieved when good TMJ-ramus tomograms are used, as long as enough length of the horizontal ramus can be seen on the roentgenogram.
3.2 The Maxilla
In the maxilla, only its base can be differentiated from the alveolus (with or without teeth). The assessment of the base of the maxilla can only be made in its relationship to the mandible and the other parts of the facial skeleton. The assessment of the alveolar process must be made solely in relationship to its relevant base of the maxilla.
3.3 The Alveolar Processes 21
In treatment, it is very important to differentiate between the base of the maxilla and its alveolar process, as the base can hardly be influenced in its size and shape by orthodontic therapy. The opposite is true for the alveolar process. The orthodontist decides where he wants it to be. In patients with extreme overexpansion, the alveolar process may even be beyond the actual base of the jaw.
3.2.1 The Maxillary Base and Its Anomalies
The two palatal bones together make the base of the maxilla. Its thickness is normally around 2 mm only, but I have also found it up to 5 mm and more in pathological conditions (cases of craniostenosis, facial hemihypertrophy, facial osteopetrosis, fibrous displasia, Cooley's anaemia and others).
Normomaxillism is a maxillary base which is normal in length, width and position. Retromaxillism is a maxillary base which is normal in length and width but which is too far retroposed. Antemaxillism is defined by a maxillary base of normal length and width which is positioned too far forward. In micromaxillism the maxillary base is too small in length and width. In most cases it also lies too far back and then it may additionally be described by the term retromaxillism. However, when we advance such a maxilla forwards it still remains a micromaxillism but in a normal position. In macromaxillism the maxillary base is too large in all dimensions. Hypermaxillism means that the maxilla is too large in height (=vertical maxillary excess). Hypomaxillism means the oposite ( = vertical maxillary deficiency). However, in both cases it is rather an anomaly of the maxillary alveolus than of the base of the maxilla. Maxillary asymmetry means that the maxillary base is asymmetrical in length and width and maybe also in position. The classical example is the maxilla in a severe, hemifacial microsomia deformity. Lateromaxillism means that a maxillary base of normal size and width is shifted laterally, while in maxillary rotation it is rotated with or without any other anomalies of the maxillary base. For each the most common cause is trauma or in some situations the anomaly occurs after a forceps delivery. Combinations of all these anomalies of the maxillary base may occur.
3.3 The Alveolar Processes
The alveolar processes of the mandible and the maxilla evolve with the development and eruption of the contained tooth germs. Although it sits on the base of the jaws the alveolar process has the capacity to exist independent of a mandibular base underneath it. This is occasionally seen in congenital mandibular defects as in

22 CHAPTER 3 Parts of the Facial Skeleton
cases of hemifacial microsomia (see Fig. 18g). It is also seen in those cases in which the base of the mandible has been lost due to surgery or trauma, while the alveolar process containing the teeth remained unchanged for years.
Even in situations without an obvious cause, the alveolar process does not always develop in the same positional relationship to the base of the jaws. This finding is proof of the alveolar process being a separate type of bone structure. It alone allows us to understand why the alveolar process occasionally develops too far forward, distally, laterally or medially and in different shapes.
The positional anomalies of the alveolar processes may develop spontaneously or arise through orthodontic, surgical or other influences. Within the alveolus, the teeth can be in correct angulation or be tilted relative to the pertinent base of the jaw. There can be too little or too much space between them or they may be just perfectly in alignment.
3.3.1 Anomalies of the Alveolar Processes
For treatment, alveolar anomalies have to be diagnosed separately and named accordingly, independently of the anomalies of the bases of the mandible and the maxilla. Normoalveolism is an alveolar process normal in height, width and position relative to the respective base of the jaw. In antealveolism, an alveolus normal in size and width is positioned forward on the base of that jaw, and in retroalveolism the alveolus is situated too far posteriorly. These anomalies are not infrequently found in the mandible. In macroalveolism and microalveolism, the alveolar process is either too large or too small in all dimensions and in hyper- and hypoalveolism an alveolar process in normal position is either too high or too low in the vertical dimension. We also speak of latera- and mesioalveolism, when the alveolus is shifted laterally on the base of the jaw, or mesially. Tilting of the alveolus has to be described separately. Since these anomalies can occur in both the mandible and in the maxilla, in the whole alveolar arch or only locally, we will have to add to the description of the existing anomaly of the alveolar process the words maxillary or mandibular, complete or local. Combinations also exist.
3.4 Abnormal Angulations
It is obvious that the angulation between the various components of the facial skeleton, in particular the jaws, affects the external appearance as well as the occlusion. It does not seem useful to recommend a separate terminology for these variations also. They are made sufficiently clear by standard cephalometric evaluation.
3.5 Long and Short Face
The full picture of an anomaly may not be adequately described by the description of the anomalies of the various parts of the facial skeleton alone. In addition to describing anomalies in the sagittal and horizontal planes, it is also necessary to describe and diagnose anomalies in their vertical dimension. Whereas vertical anomalies of the alveolar processes and of the chin are adequately described by terms (hyper- and hypoalveolism or -genia), precise terminology is required for the vertical discrepancy that exists among the bases of the facial thirds. These are the long and the short face anomalies and the open bite cases.
In the American literature, the terms long-face syndrome and short-face syndrome are often used. There is no justification for naming these facial anomalies syndromes. In medical terminology a syndrome is either a disease or an anomaly that involves a number of signs and symptoms and of which at least several signs or symptoms have to be present in order to call the disease or the anomaly a syndrome. This definition is not true for either the long-face or the short-face syndrome. The only consistently present sign is either the vertical shortness of the face or its excessive height. But one sign alone does not constitute a syndrome. Therefore, these anomalies should be just named either long-face or short-face. In addition, the origin of the long- or shortface has to be added. It may be due to the maxilla or the mandible or both. Therefore, the condition should be termed maxillary or a mandibular or a bimaxillary short or long face. It may be that the anomaly is due to a vertical anomaly of the alveolar processes only or of the position or angulation of the bases of the jaws or of the height of the prominence of the chin. Another cause may be the vertical bite relationship as in the deep overbite and the anterior open bite.
A maxillary long face is either a maxillary basal long face (with the base of it positioned too low) or a maxillary hyperalveolism long face (when the alveolus is too high) or both. The maxillary short face will be the reverse. The mandibular long face is either a mandibular basal long face (with the base of the mandible positioned too low) or a mandibular hyperalveolism long face (when the alveolus is too high) or both. The mandibular short face will be the reverse.
3.6 Open Bite Anomalies
The open bite may be due to an anomaly of either the maxilla or mandible or both, basal or alveolar. Almost every open bite situation produces a long face, at least the so-called anterior and so-called total open bite. Anterior open bite refers to an open bite that is limited to as

far back as the premolar regions only. The maxillary anterior open bite may be due to a position of the anterior maxillary segment that is too high or be due to a position of the posterior maxillary segments that is too low. An anterior maxillary hypoalveolism can also be the cause. In all three situations, an overexaggerated curve of Spee is present.
The mandibular anterior open bite can be alveolar or basal, or both.
Total or circular open bite refers to occlusion of the last molars only (uni- or bilaterally). This situation again may be due to an aberrant position of the maxillary or mandibular base only, or of both. And even the height of the alveolar processes may be the cause.
3.7 Conclusion 23
In addition, lateral open bite only or posterior open bite only must be distinguished. The open bite may be uni- or bilateral and may arise in the maxilla or the mandible, or both. Most of these open bite problems are due to hypoalveolism or contralateral hyperalveolism.
3.7 Conclusion
Using the terminology suggested in this chapter should allow more efficient communication among treatment providers and would direct ourselves primarily towards more accurate diagnosis and more effective treatment.


![Cronicon · fractures [2]. Being the most prominent mobile bone of the facial skeleton, Mandibular fractures are among the most common injuries to the facial skeleton, with a 6:2](https://static.fdocuments.in/doc/165x107/5f2b985f1c26767db7383601/cronicon-fractures-2-being-the-most-prominent-mobile-bone-of-the-facial-skeleton.jpg)