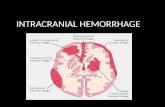
INTRACRANIAL HEMORRHAGE By Dr Ambreen Assistant Professor Medicine.
Upload
stevenp302Category
view
814download
0
Management of Intracranial Hemorrhage
Steven Podnos MD

Epidemiology
• Cerebral Catastrophe• Overall Mortality 40%• Only 25% of survivors are independent at 6
months

Pathophysiology
• 85% occurs as spontaneous event related to rupture of small penetrating arteries damaged by hypertension and/or amyloid angiopathy

Presentation
• ICH is an evolving process, with hematoma enlargement in almost 75% of patients in first 24 hours
• Management strategies :• Prevention of further bleeding/hematoma
expansion• Minimize cerebral ischemia

ICH
• Evidence suggests that control of BP improves outcomes
• Intubation for GCS equal to or less than 8• ICU care• Reversal of Anticoagulation-Vit K, FFP• Platelet dysfunction due to Plavix/ASA causes
increased risk for ICH, but platelet transfusion has not been shown to be of benefit

HBP
• In contrast to Ischemic CVA, BP control is felt to be important in preventing hematoma expansion
• Guidelines: Keep CPP > 60, reduce SPB to 160, MAP 110 with monitoring

Other Modalities
• No consensus on ICP monitoring or Rx• Seizures occur in 4-9%. Prophylactic meds not
indicated. Rx seizures actively however. Consider subclinical seizures in patients with poor consciousness
• Glycemic Control-suggest only control glucose over 180. Avoid hypoglycemia

Other Modalities Rx in ICH
• SCD on admit• Use chemical agent for DVT prophylaxis 1-4
days after bleeding felt to have stopped• Temperature control reasonable but
unproven. No data on hypothermia yet.• Neurosurgery-Ventriculostomy for
hydrocephalus. Other surgery (hematoma evacuation) in study.

Neuroprotection in ICH
• No good data





![Non-aneurysmal subarachnoid hemorrhage in a case of ... · associated with aneurysmal subarchnoid and intracranial hemorrhage [5]. In our case this was a primary subarchnoid hemorrhage](https://static.fdocuments.in/doc/165x107/5ed55eea6933f508e973f10c/non-aneurysmal-subarachnoid-hemorrhage-in-a-case-of-associated-with-aneurysmal.jpg)