Management of Inflammatory Bowel Diseases (IBD): 2019 & …Management of Inflammatory Bowel Diseases...
54
Management of Inflammatory Bowel Diseases (IBD): 2019 & Beyond Adam C. Ehrlich, MD, MPH Assistant Professor of Medicine, Section of Gastroenterology Co-Medical Director, Temple IBD Program Associate Program Director, Gastroenterology Fellowship Lewis Katz School of Medicine at Temple University Advances in Digestive Diseases 2019 June 1, 2019
Transcript of Management of Inflammatory Bowel Diseases (IBD): 2019 & …Management of Inflammatory Bowel Diseases...
Management ofInflammatory Bowel Diseases
(IBD): 2019 & Beyond
Adam C. Ehrlich, MD, MPH
Assistant Professor of Medicine, Section of Gastroenterology
Co-Medical Director, Temple IBD Program
Associate Program Director, Gastroenterology Fellowship
Lewis Katz School of Medicine at Temple University
Advances in Digestive Diseases 2019
June 1, 2019
Disclosures
• Consultant: Level Ex, Vindico Medical Education
• Scientific Advisory Board: Praeventix LLC, Janssen
Topics to Cover
• Management with traditional therapies– 5-ASA withdrawal in CD
– Anti-TNFs in pre-operative period in IBD
– FMT for C difficile in IBD
• Management with recent therapies– Ustekinumab in UC
– Vedolizumab vs adalimumab in UC
– Tofacitinib in UC in real life
• Touch on future therapies
Stopping 5-ASAs in Crohn’s Disease
Patients Starting Biologic Therapy Does
Not Increase the Risk of Adverse Clinical
Outcomes: Analysis of Two National
Population-Based Cohorts
Ryan C. Ungaro, Berkeley N. Limketkai, Camilla Bjørn Jensen, Clara Yzet,Kristine H Allin, Manasi Agrawal, Thomas Ullman, Johan Burisch, Tine Jess,and Jean-Frederic Colombel
Presentation 110, Digestive Disease Week 2019
Background
• 5-ASA has limited efficacy in CD and its use is generally not
recommend by clinical guidelines
• 5-ASA are one of the most commonly used medications in CD
• 5-ASA use poses significant cost and pill burden on patients
• There has been significant research on de-escalation of
immunomodulators and biologics in CD but little to no data on
stopping 5-ASA
• It is unknown if it is safe to stop 5-ASA in CD patients who
require escalation of therapy to anti-TNF agents
Lichtenstein G et al Am J Gastro 2018
Siegel C et al DDW 2017
Torres J et al Gastro 2015
Methods• U.S. Cohort: Truven Health MarketScan Commercial Database
• Over 450 million entries per year from 2007-2016 followed up to 3 years
• CD patients identified using ICD-9 and 10 codes
• Danish cohort: Drawn from 3 nationwide Danish health registers Inpatient and
outpatient data on all Danish patients
•All Danish patients from 1995 -2014 followed up to 9 years
•CD patients identified using ICD-8 and 10 codes
• Inclusion criteria
• Prescribed Anti-TNF with continuation for at least 90 days
• Prescribed 5-ASA for at least 90 days prior to initiating anti-TNF therapy
• Primary Outcome was composite of adverse clinical events defined as:
• Need for new oral steroid therapy (at least 90 days after biologic prescription)
• IBD-related hospitalization (CD diagnosis as primary code)
• IBD-related surgery (small/large bowel surgeries)
•Secondary Outcomes: individual components of the primary composite
• Variable of interest: Discontinuation of 5-ASA
• Defined as discontinuation of 5-ASA within 90 days of starting anti-TNF
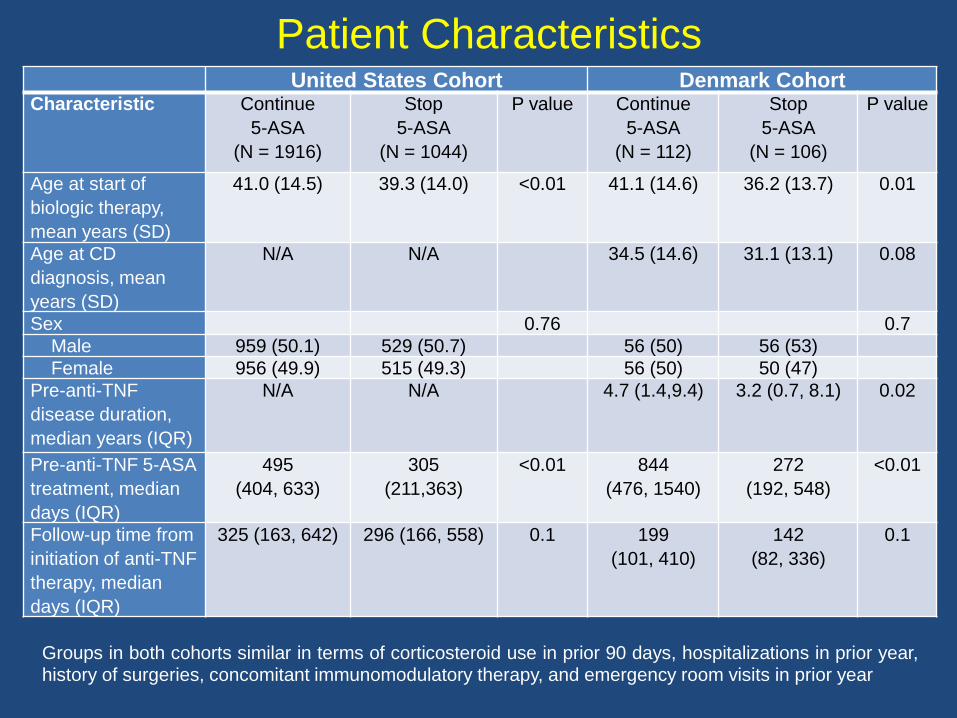
Patient CharacteristicsUnited States Cohort Denmark Cohort
Characteristic Continue
5-ASA
(N = 1916)
Stop
5-ASA
(N = 1044)
P value Continue
5-ASA
(N = 112)
Stop
5-ASA
(N = 106)
P value
Age at start of
biologic therapy,
mean years (SD)
41.0 (14.5) 39.3 (14.0) <0.01 41.1 (14.6) 36.2 (13.7) 0.01
Age at CD
diagnosis, mean
years (SD)
N/A N/A 34.5 (14.6) 31.1 (13.1) 0.08
Sex 0.76 0.7
Male 959 (50.1) 529 (50.7) 56 (50) 56 (53)
Female 956 (49.9) 515 (49.3) 56 (50) 50 (47)
Pre-anti-TNF
disease duration,
median years (IQR)
N/A N/A 4.7 (1.4,9.4) 3.2 (0.7, 8.1) 0.02
Pre-anti-TNF 5-ASA
treatment, median
days (IQR)
495
(404, 633)
305
(211,363)
<0.01 844
(476, 1540)
272
(192, 548)
<0.01
Follow-up time from
initiation of anti-TNF
therapy, median
days (IQR)
325 (163, 642) 296 (166, 558) 0.1 199
(101, 410)
142
(82, 336)
0.1
Groups in both cohorts similar in terms of corticosteroid use in prior 90 days, hospitalizations in prior year,history of surgeries, concomitant immunomodulatory therapy, and emergency room visits in prior year
0.00
0.25
0.50
0.75
1.00
Ris
k o
f m
ajo
r ad
ve
rse
ou
tco
me
1044 288 90 32Stop 5-ASA
1916 583 203 85Cont 5-ASA
Number at risk
0 1 2 3Years after initiation of biologic therapy
Cont 5-ASA Stop 5-ASA
0.00
0.25
0.50
0.75
1.00
Ris
k o
f m
ajo
r a
dve
rse
ou
tcom
e
1044 417 173 75Stop 5-ASA
1916 849 388 172Cont 5-ASA
Number at risk
0 1 2 3Years after initiation of biologic therapy
Cont 5-ASA Stop 5-ASA
0.00
0.25
0.50
0.75
1.00
Ris
k o
f m
ajo
r a
dve
rse
ou
tcom
e
1044 375 139 58Stop 5-ASA
1916 755 327 141Cont 5-ASA
Number at risk
0 1 2 3Years after initiation of biologic therapy
Cont 5-ASA Stop 5-ASA
0.00
0.25
0.50
0.75
1.00
Ris
k o
f m
ajo
r a
dve
rse
ou
tcom
e
1044 318 112 40Stop 5-ASA
1916 641 243 102Cont 5-ASA
Number at risk
0 1 2 3Years after initiation of biologic therapy
Cont 5-ASA Stop 5-ASA
C D
B
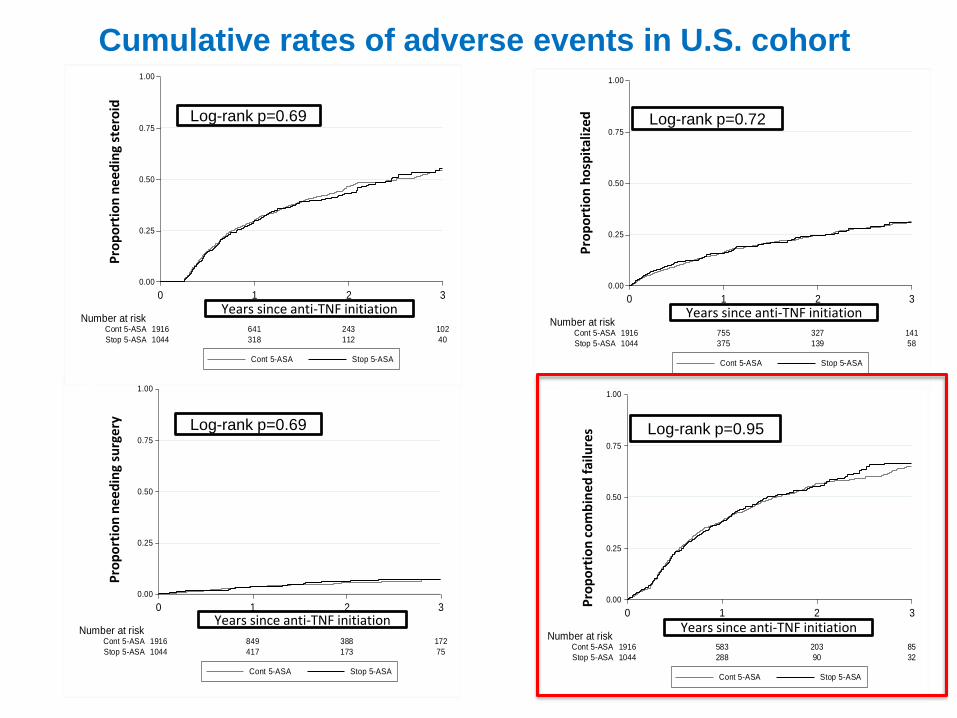
Log-rank p=0.69 Log-rank p=0.72
Log-rank p=0.69 Log-rank p=0.95
Pro
po
rtio
n h
osp
ital
ize
dP
rop
ort
ion
co
mb
ined
fai
lure
s
Years since anti-TNF initiation Years since anti-TNF initiation
Years since anti-TNF initiationYears since anti-TNF initiation
Pro
po
rtio
n n
ee
din
g st
ero
idP
rop
ort
ion
nee
din
g su
rger
y
A
Cumulative rates of adverse events in U.S. cohort

Cumulative rates of adverse events in Danish cohort
CD
Log-rank p=0.85
Log-rank p=0.48 Log-rank p=0.55
Pro
po
rtio
n c
om
bin
ed f
ailu
res
Years since anti-TNF initiation
Years since anti-TNF initiationYears since anti-TNF initiation
Pro
po
rtio
n n
ee
din
g st
ero
idP
rop
ort
ion
nee
din
g su
rger
y
A
Pro
po
rtio
n h
osp
ital
ize
d
Years since anti-TNF initiation
Log-rank p=0.01
B
D
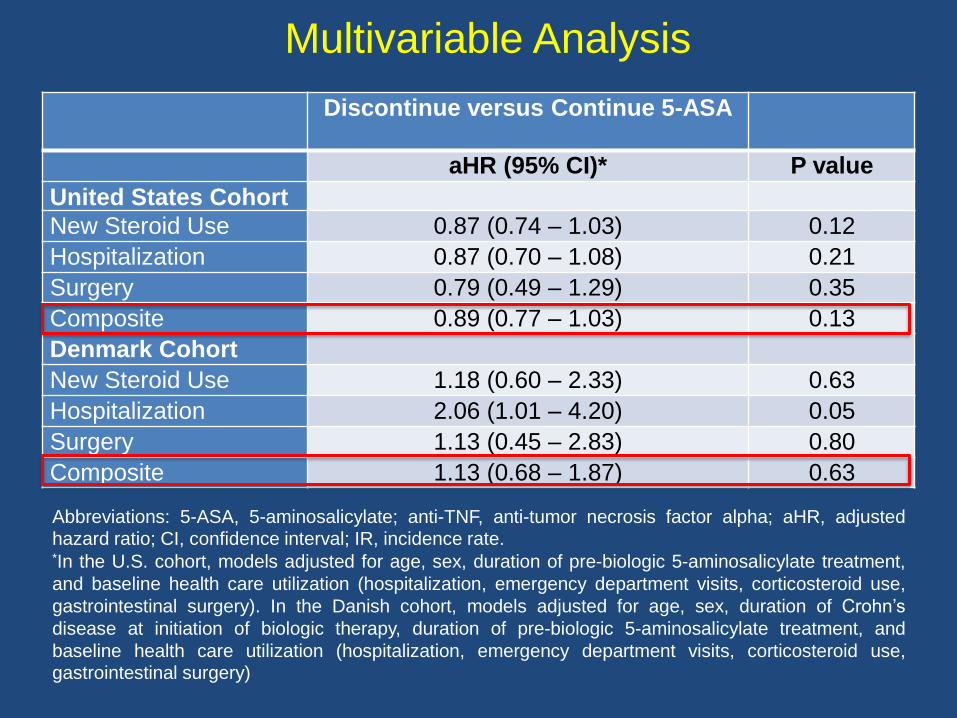
Multivariable Analysis
Discontinue versus Continue 5-ASA
aHR (95% CI)* P value
United States Cohort
New Steroid Use 0.87 (0.74 – 1.03) 0.12
Hospitalization 0.87 (0.70 – 1.08) 0.21
Surgery 0.79 (0.49 – 1.29) 0.35
Composite 0.89 (0.77 – 1.03) 0.13
Denmark Cohort
New Steroid Use 1.18 (0.60 – 2.33) 0.63
Hospitalization 2.06 (1.01 – 4.20) 0.05
Surgery 1.13 (0.45 – 2.83) 0.80
Composite 1.13 (0.68 – 1.87) 0.63
Abbreviations: 5-ASA, 5-aminosalicylate; anti-TNF, anti-tumor necrosis factor alpha; aHR, adjustedhazard ratio; CI, confidence interval; IR, incidence rate.*In the U.S. cohort, models adjusted for age, sex, duration of pre-biologic 5-aminosalicylate treatment,
and baseline health care utilization (hospitalization, emergency department visits, corticosteroid use,
gastrointestinal surgery). In the Danish cohort, models adjusted for age, sex, duration of Crohn’s
disease at initiation of biologic therapy, duration of pre-biologic 5-aminosalicylate treatment, and
baseline health care utilization (hospitalization, emergency department visits, corticosteroid use,gastrointestinal surgery)
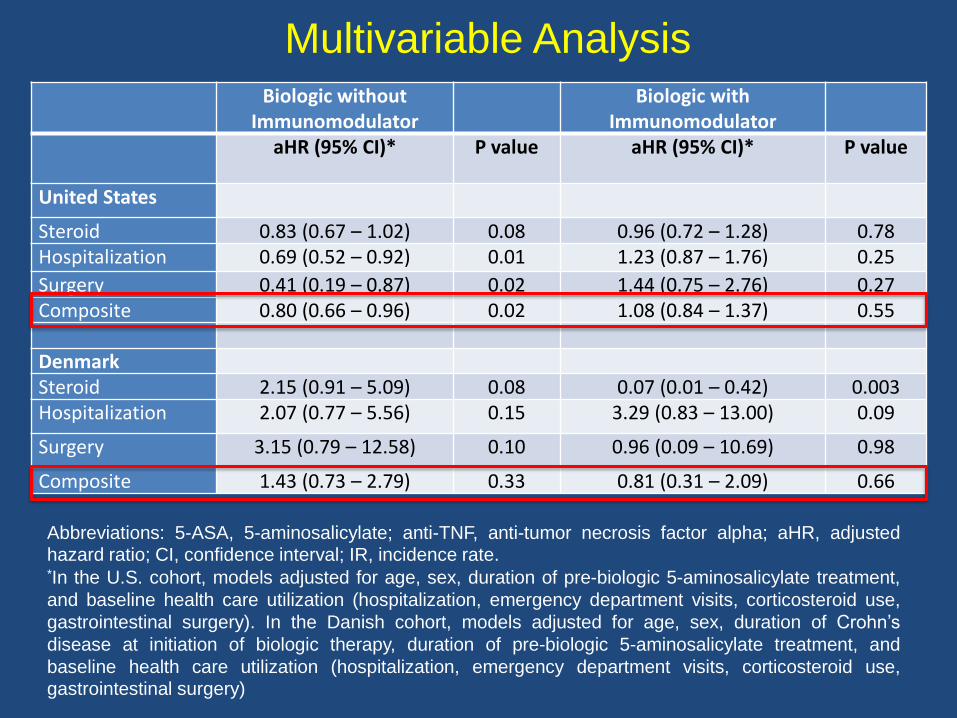
Multivariable Analysis
Abbreviations: 5-ASA, 5-aminosalicylate; anti-TNF, anti-tumor necrosis factor alpha; aHR, adjustedhazard ratio; CI, confidence interval; IR, incidence rate.*In the U.S. cohort, models adjusted for age, sex, duration of pre-biologic 5-aminosalicylate treatment,
and baseline health care utilization (hospitalization, emergency department visits, corticosteroid use,
gastrointestinal surgery). In the Danish cohort, models adjusted for age, sex, duration of Crohn’s
disease at initiation of biologic therapy, duration of pre-biologic 5-aminosalicylate treatment, and
baseline health care utilization (hospitalization, emergency department visits, corticosteroid use,
gastrointestinal surgery)
Biologic without Immunomodulator
Biologic with Immunomodulator
aHR (95% CI)* P value aHR (95% CI)* P value
United States
Steroid 0.83 (0.67 – 1.02) 0.08 0.96 (0.72 – 1.28) 0.78Hospitalization 0.69 (0.52 – 0.92) 0.01 1.23 (0.87 – 1.76) 0.25
Surgery 0.41 (0.19 – 0.87) 0.02 1.44 (0.75 – 2.76) 0.27Composite 0.80 (0.66 – 0.96) 0.02 1.08 (0.84 – 1.37) 0.55
DenmarkSteroid 2.15 (0.91 – 5.09) 0.08 0.07 (0.01 – 0.42) 0.003Hospitalization 2.07 (0.77 – 5.56) 0.15 3.29 (0.83 – 13.00) 0.09
Surgery 3.15 (0.79 – 12.58) 0.10 0.96 (0.09 – 10.69) 0.98
Composite 1.43 (0.73 – 2.79) 0.33 0.81 (0.31 – 2.09) 0.66
Conclusions
• In two national databases, CD patients on 5-ASA for at least 90 days and startedon anti-TNF who then discontinued 5-ASA medications did not have anincreased rate of adverse clinical events (new corticosteroid use, IBD-relatedhospitalization or surgery)
• After adjusting for potential confounders, there was no significant difference inthe risk of adverse clinical events when comparing CD patients whodiscontinued or continued 5-ASA after initiation of anti-TNF
• These results suggest that CD patients may safely discontinue 5-ASA afterstarting biologic therapy but should be validated in a prospective study
Prospective Cohort of Ulcerative Colitis
and Crohn’s Disease Patients
Undergoing Surgery to Identify Risk
Factors for
Post-Operative INfection I (PUCCINI)
Benjamin Lee Cohen, Phillip Fleshner, Sunanda V. Kane, Hans H. Herfarth, Nicole Palekar, Francis A. Farraye, Jonathan A. Leighton, Jeffry Katz, Russell D. Cohen, Mark Edward Gerich, Raymond K. Cross, Peter D.R. Higgins, Andrew Tinsley, Sarah Camille
Glover, Corey A. Siegel, Jaime L. Bohl, Heba Iskandar, Samantha Raymond, Ruiqi Huang, Mayte Suarez-Farinas, Bruce E. Sands
Presentation 415a, Digestive Disease Week 2019
Redacted at request of authors
Jessica R. Allegretti, Jonathan Hurtado, Madeline Carrelas, Jenna Marcus, Emily Phelps, Wing Fei Wong, Julian R. Marchesi, Benjamin H. Mullish, Julie A.K. McDonald, Alexandros Pechlivanis,
Grace F. Barker, Jesus Miguens Blanco, Sashidar Sagi, Matthew Bohm, Collen Kelly, Zain Kassam, Ari Grinspan, and Monika Fischer
The ICON Study: Inflammatory Bowel
Disease and Recurrent Clostridium
difficile Infection: Outcomes after Fecal
Microbiota Transplantation
Presentation 7, Digestive Disease Week 2019
• Prevalence is 2.5-8 fold higher then non-IBD patients
• 10% lifetime risk
• 4.5-fold higher risk of recurrence
• Patients with UC are at the highest risk
CDI in IBD
Sequela of CDI in IBD
• Exacerbations of IBD
• Increased hospitalizations
• Increased LOS
• Escalation in IBD therapy
• Colectomy
• Higher mortality rates
• Failure of CDI medical therapy
• More CDI recurrences
• Increased health care costs.
• Distinguishing active infection from flare
• Choice and duration of antibiotic therapy
• Escalation or de-escalation of immunosuppression
• Where to position FMT
• Lack of prospective data
– Need to extrapolate from non-IBD data
Treatment of CDI in IBD: Challenges
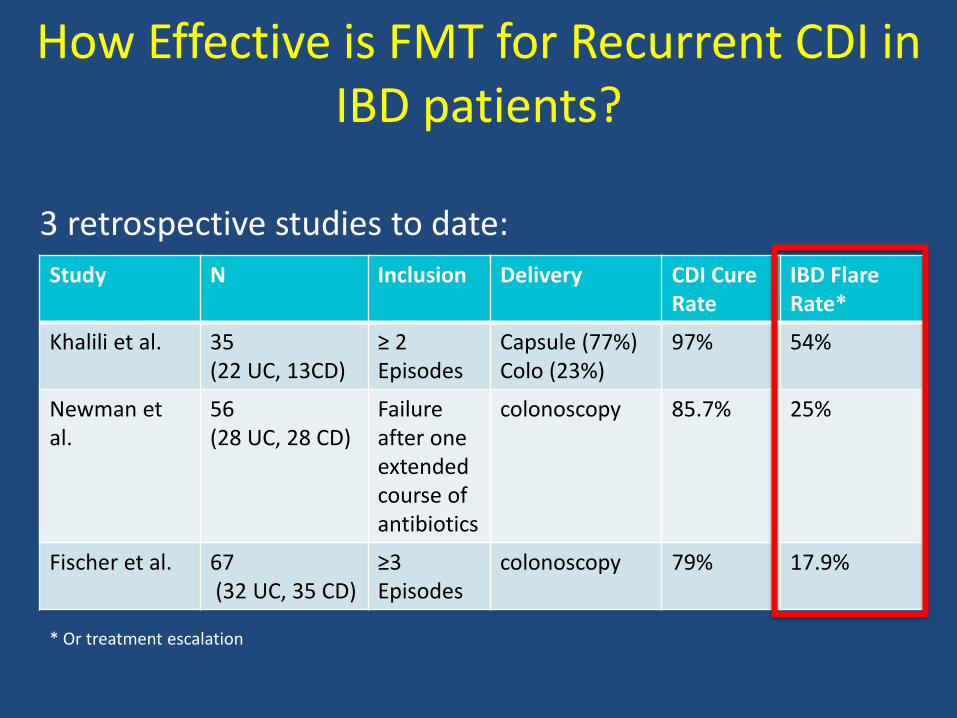
How Effective is FMT for Recurrent CDI in IBD patients?
3 retrospective studies to date:
Study N Inclusion Delivery CDI Cure Rate
IBD FlareRate*
Khalili et al. 35 (22 UC, 13CD)
≥ 2 Episodes
Capsule (77%)Colo (23%)
97% 54%
Newman et al.
56 (28 UC, 28 CD)
Failureafter one extended course of antibiotics
colonoscopy 85.7% 25%
Fischer et al. 67(32 UC, 35 CD)
≥3 Episodes
colonoscopy 79% 17.9%
* Or treatment escalation
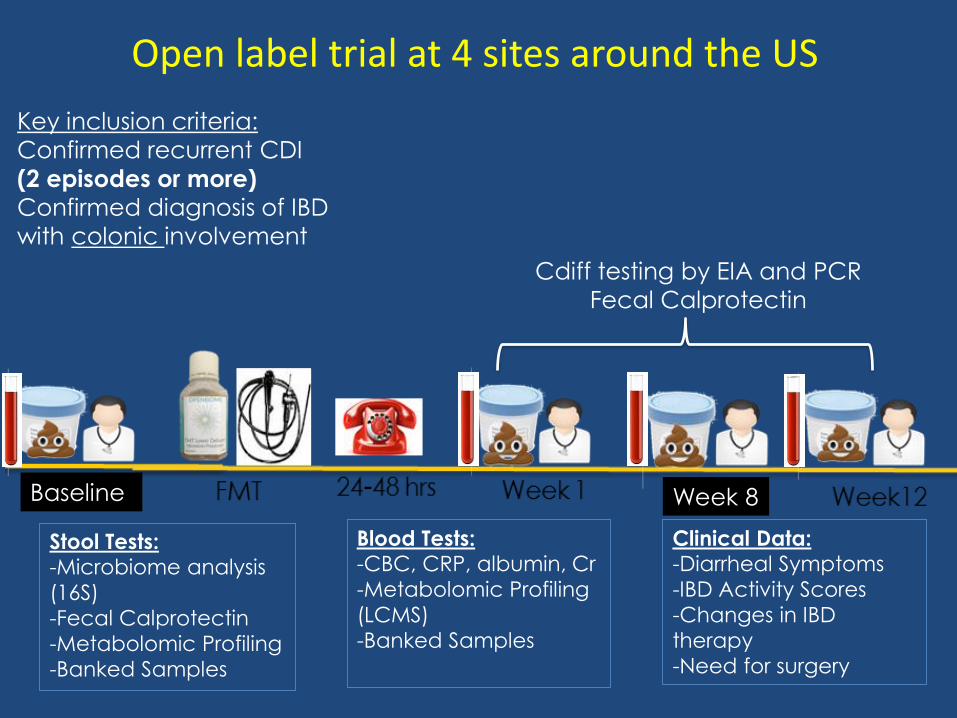
Baseline
Stool Tests: -Microbiome analysis
(16S)
-Fecal Calprotectin
-Metabolomic Profiling
-Banked Samples
Blood Tests: -CBC, CRP, albumin, Cr
-Metabolomic Profiling
(LCMS)
-Banked Samples
Clinical Data: -Diarrheal Symptoms
-IBD Activity Scores
-Changes in IBD
therapy
-Need for surgery
Week 8
Cdiff testing by EIA and PCR
Fecal Calprotectin
Key inclusion criteria:
Confirmed recurrent CDI
(2 episodes or more)
Confirmed diagnosis of IBD
with colonic involvement
Open label trial at 4 sites around the US
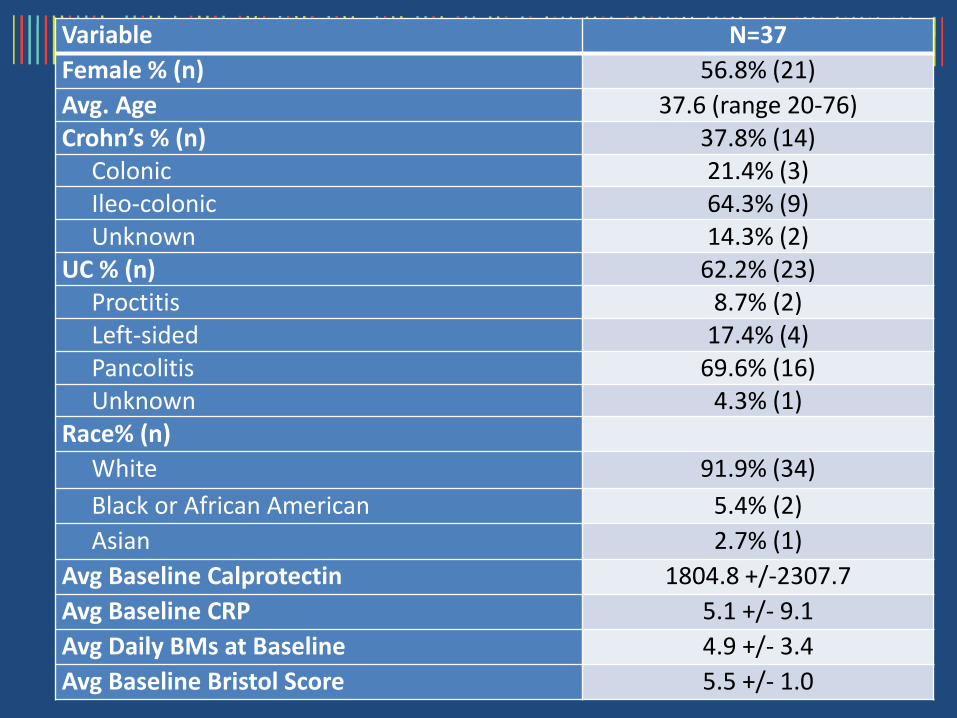
Variable N=37
Female % (n) 56.8% (21)
Avg. Age 37.6 (range 20-76)Crohn’s % (n) 37.8% (14)
Colonic 21.4% (3)Ileo-colonic 64.3% (9)Unknown 14.3% (2)
UC % (n) 62.2% (23)Proctitis 8.7% (2)Left-sided 17.4% (4)Pancolitis 69.6% (16)Unknown 4.3% (1)
Race% (n)
White 91.9% (34)
Black or African American 5.4% (2)
Asian 2.7% (1)
Avg Baseline Calprotectin 1804.8 +/-2307.7
Avg Baseline CRP 5.1 +/- 9.1
Avg Daily BMs at Baseline 4.9 +/- 3.4
Avg Baseline Bristol Score 5.5 +/- 1.0
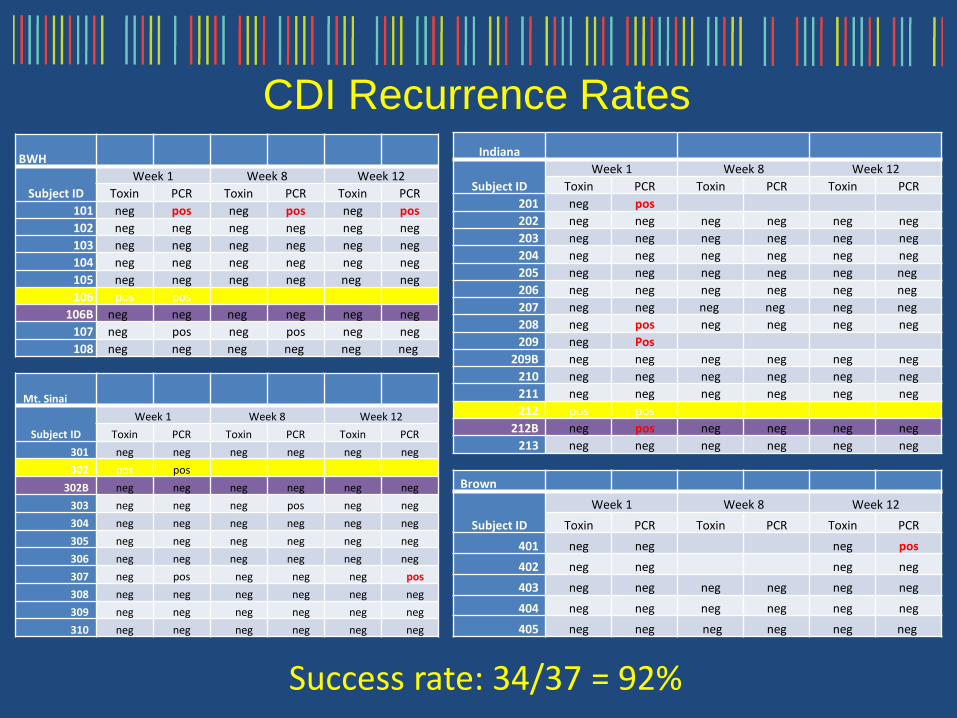
CDI Recurrence Rates
BWH
Subject ID
Week 1 Week 8 Week 12
Toxin PCR Toxin PCR Toxin PCR
101 neg pos neg pos neg pos
102 neg neg neg neg neg neg
103 neg neg neg neg neg neg
104 neg neg neg neg neg neg
105 neg neg neg neg neg neg
106 pos pos
106B neg neg neg neg neg neg
107 neg pos neg pos neg neg
108 neg neg neg neg neg neg
Indiana
Subject ID
Week 1 Week 8 Week 12
Toxin PCR Toxin PCR Toxin PCR
201 neg pos
202 neg neg neg neg neg neg
203 neg neg neg neg neg neg
204 neg neg neg neg neg neg
205 neg neg neg neg neg neg
206 neg neg neg neg neg neg
207 neg neg neg neg neg neg
208 neg pos neg neg neg neg
209 neg Pos
209B neg neg neg neg neg neg
210 neg neg neg neg neg neg
211 neg neg neg neg neg neg
212 pos pos
212B neg pos neg neg neg neg
213 neg neg neg neg neg neg
Mt. Sinai
Subject ID
Week 1 Week 8 Week 12
Toxin PCR Toxin PCR Toxin PCR
301 neg neg neg neg neg neg
302 pos pos
302B neg neg neg neg neg neg
303 neg neg neg pos neg neg
304 neg neg neg neg neg neg
305 neg neg neg neg neg neg
306 neg neg neg neg neg neg
307 neg pos neg neg neg pos
308 neg neg neg neg neg neg
309 neg neg neg neg neg neg
310 neg neg neg neg neg neg
Brown
Subject ID
Week 1 Week 8 Week 12
Toxin PCR Toxin PCR Toxin PCR
401 neg neg neg pos
402 neg neg neg neg
403 neg neg neg neg neg neg
404 neg neg neg neg neg neg
405 neg neg neg neg neg neg
Success rate: 34/37 = 92%
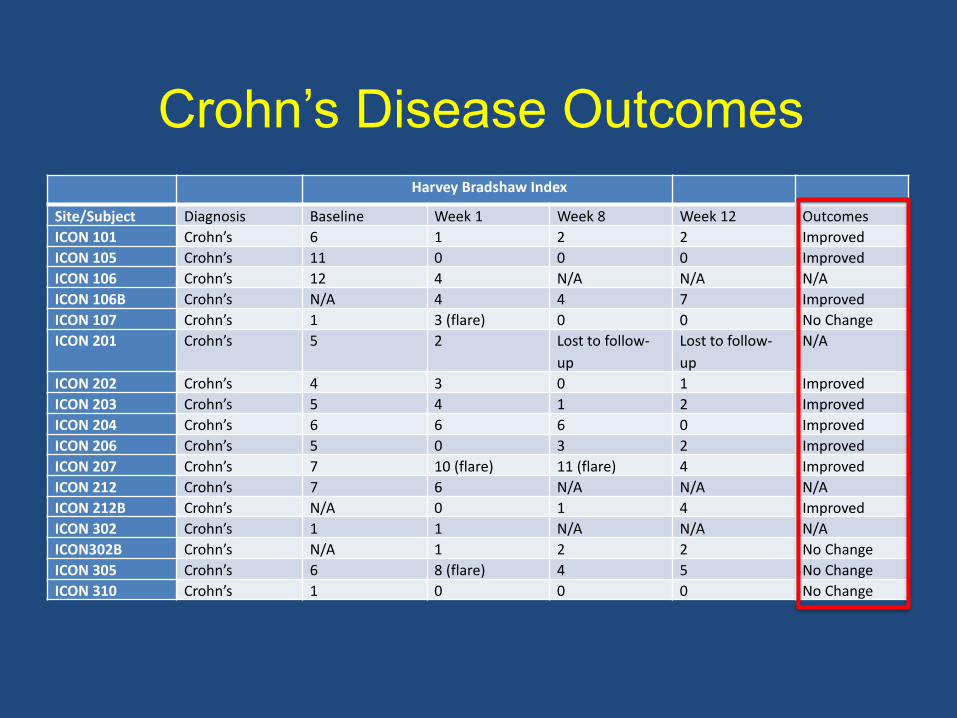
Crohn’s Disease Outcomes
Harvey Bradshaw Index
Site/Subject Diagnosis Baseline Week 1 Week 8 Week 12 Outcomes
ICON 101 Crohn’s 6 1 2 2 Improved
ICON 105 Crohn’s 11 0 0 0 Improved
ICON 106 Crohn’s 12 4 N/A N/A N/A
ICON 106B Crohn’s N/A 4 4 7 Improved
ICON 107 Crohn’s 1 3 (flare) 0 0 No Change
ICON 201 Crohn’s 5 2 Lost to follow-
up
Lost to follow-
up
N/A
ICON 202 Crohn’s 4 3 0 1 Improved
ICON 203 Crohn’s 5 4 1 2 Improved
ICON 204 Crohn’s 6 6 6 0 Improved
ICON 206 Crohn’s 5 0 3 2 Improved
ICON 207 Crohn’s 7 10 (flare) 11 (flare) 4 Improved
ICON 212 Crohn’s 7 6 N/A N/A N/A
ICON 212B Crohn’s N/A 0 1 4 Improved
ICON 302 Crohn’s 1 1 N/A N/A N/A
ICON302B Crohn’s N/A 1 2 2 No Change
ICON 305 Crohn’s 6 8 (flare) 4 5 No Change
ICON 310 Crohn’s 1 0 0 0 No Change
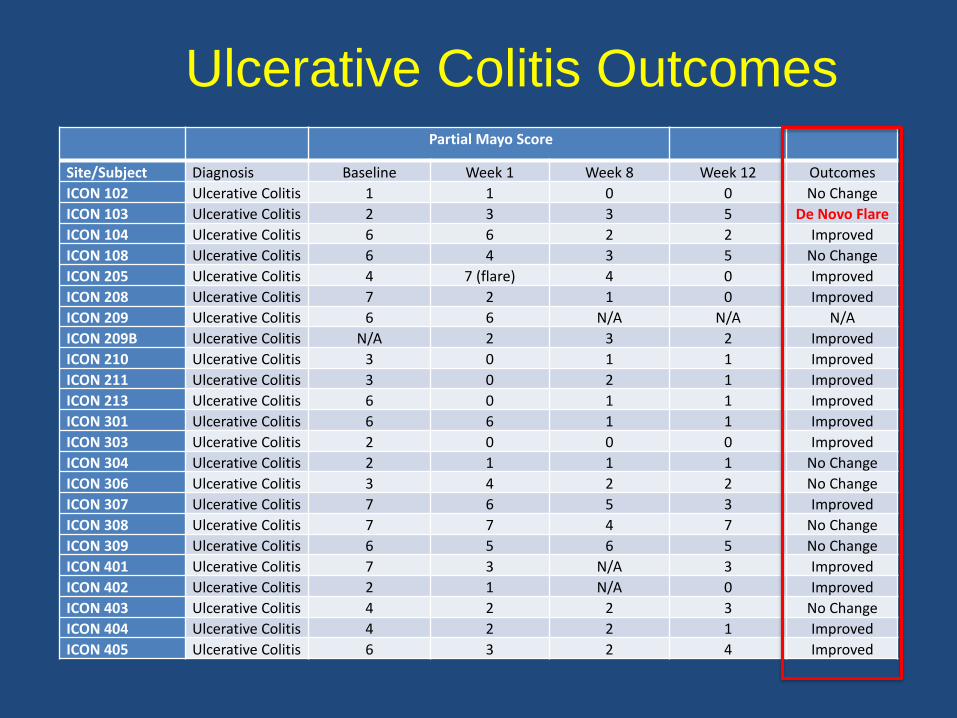
Partial Mayo Score
Site/Subject Diagnosis Baseline Week 1 Week 8 Week 12 Outcomes
ICON 102 Ulcerative Colitis 1 1 0 0 No Change
ICON 103 Ulcerative Colitis 2 3 3 5 De Novo Flare
ICON 104 Ulcerative Colitis 6 6 2 2 Improved
ICON 108 Ulcerative Colitis 6 4 3 5 No Change
ICON 205 Ulcerative Colitis 4 7 (flare) 4 0 Improved
ICON 208 Ulcerative Colitis 7 2 1 0 Improved
ICON 209 Ulcerative Colitis 6 6 N/A N/A N/A
ICON 209B Ulcerative Colitis N/A 2 3 2 Improved
ICON 210 Ulcerative Colitis 3 0 1 1 Improved
ICON 211 Ulcerative Colitis 3 0 2 1 Improved
ICON 213 Ulcerative Colitis 6 0 1 1 Improved
ICON 301 Ulcerative Colitis 6 6 1 1 Improved
ICON 303 Ulcerative Colitis 2 0 0 0 Improved
ICON 304 Ulcerative Colitis 2 1 1 1 No Change
ICON 306 Ulcerative Colitis 3 4 2 2 No Change
ICON 307 Ulcerative Colitis 7 6 5 3 Improved
ICON 308 Ulcerative Colitis 7 7 4 7 No Change
ICON 309 Ulcerative Colitis 6 5 6 5 No Change
ICON 401 Ulcerative Colitis 7 3 N/A 3 Improved
ICON 402 Ulcerative Colitis 2 1 N/A 0 Improved
ICON 403 Ulcerative Colitis 4 2 2 3 No Change
ICON 404 Ulcerative Colitis 4 2 2 1 Improved
ICON 405 Ulcerative Colitis 6 3 2 4 Improved
Ulcerative Colitis Outcomes
• FMT is safe and effective for patients with IBD-CDI
• FMT failures are lower then previously reported (92% success)
– done earlier (1st recurrence)
• Only one patient (2.7%) experienced a de novo flare
Conclusions
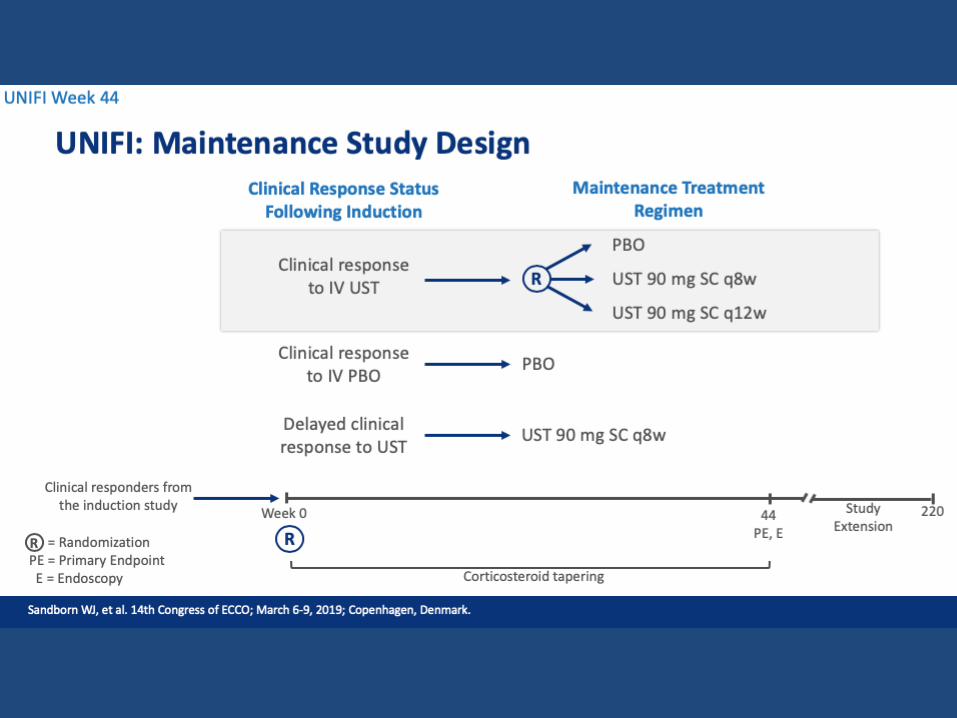
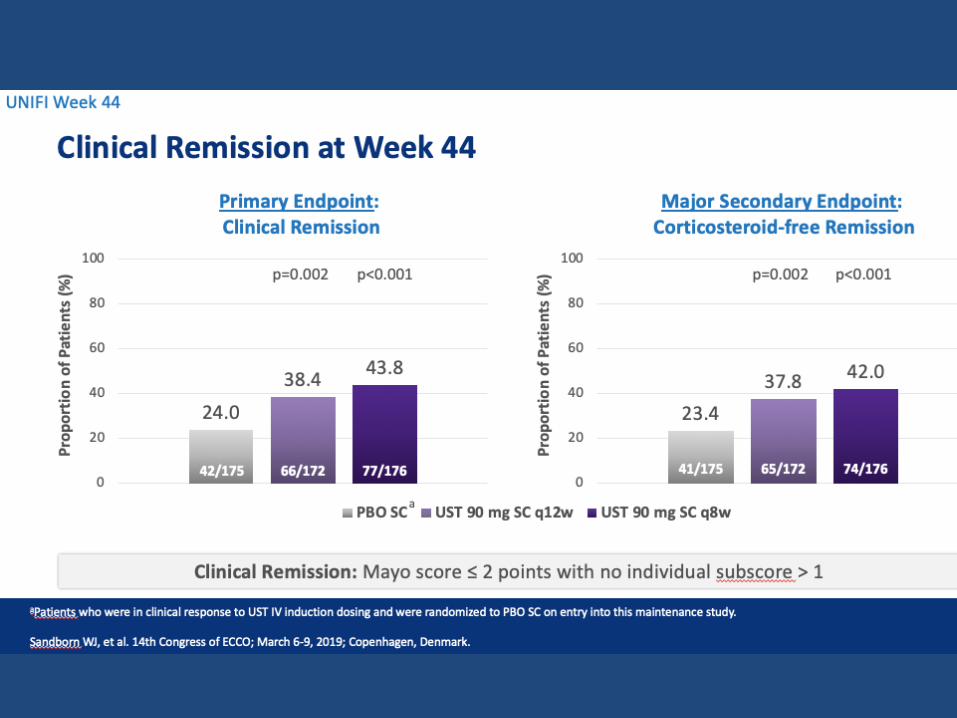
Efficacy and Safety of Ustekinumabas Maintenance Therapy in Ulcerative Colitis:
Week 44 Results From UNIFI
W.J. Sandborn, B.E. Sands, R. Panaccione, C.D. O’Brien, H. Zhang, J. Johanns, L. Peyrin-Biroulet, G. van Assche, S. Danese, S. Targan,
M.T. Abreu, T. Hisamatsu, P. Szapary, C. Marano
Presentation 833, Digestive Disease Week 2019
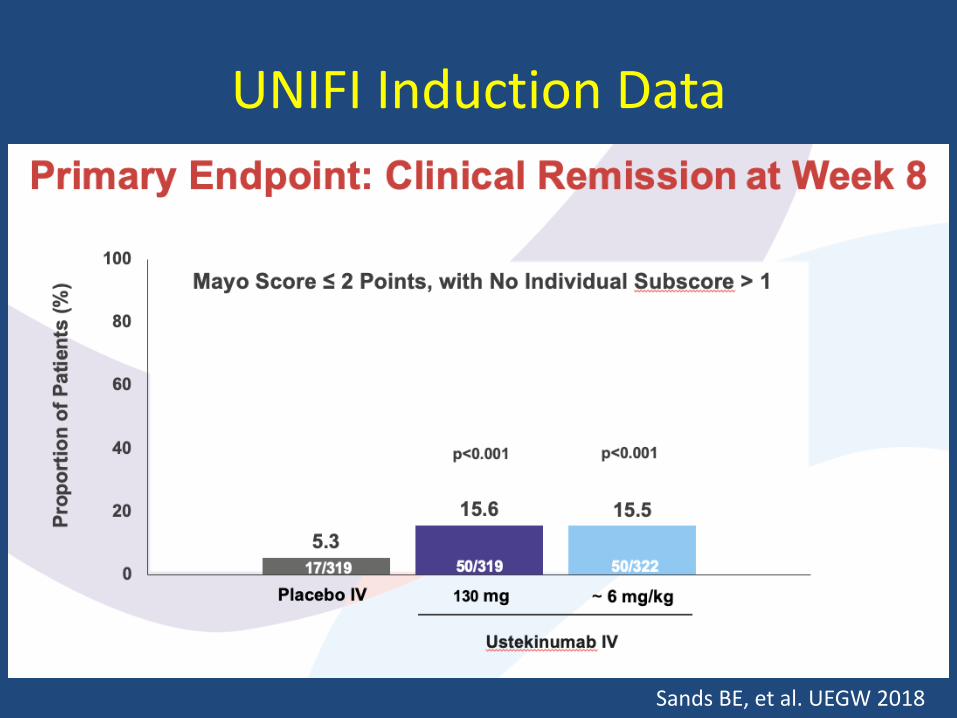
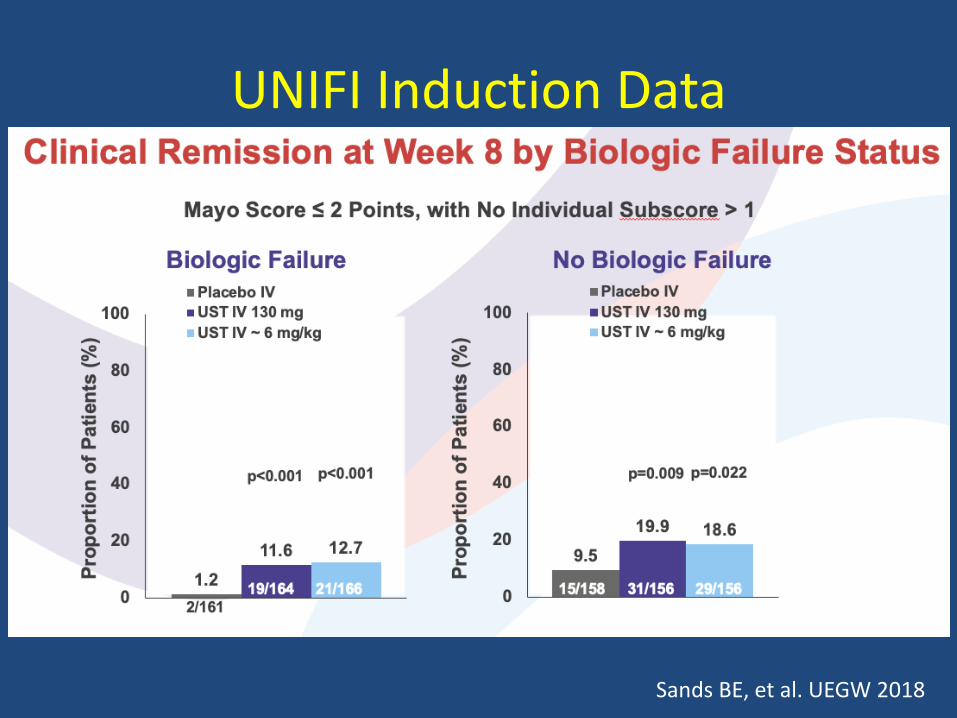
UNIFI Induction Data
Sands BE, et al. UEGW 2018
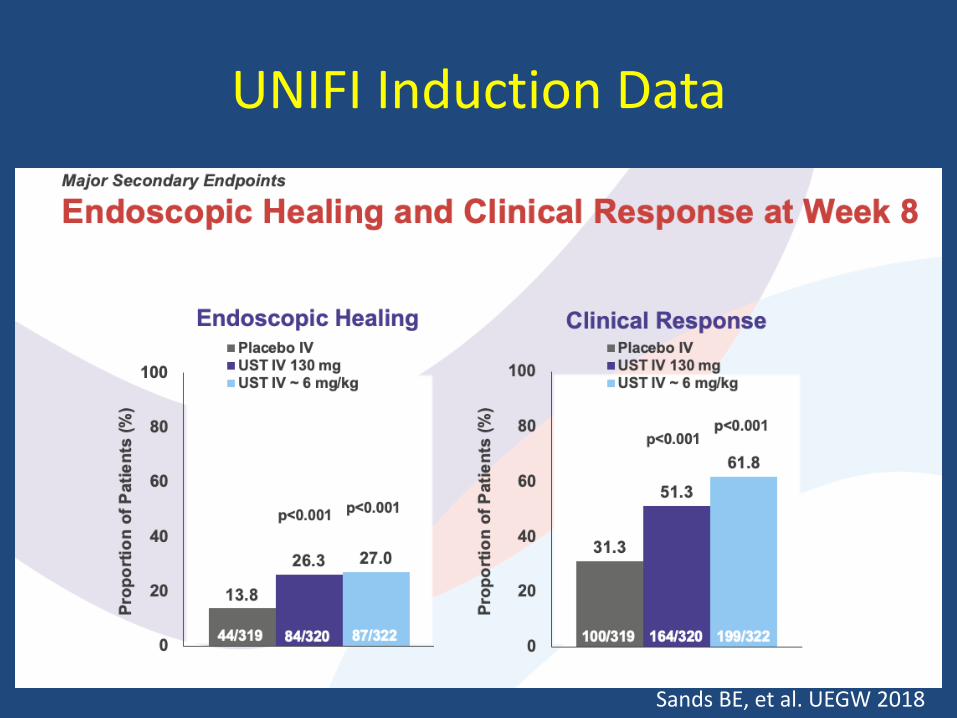
UNIFI Induction Data
Sands BE, et al. UEGW 2018
UNIFI Induction Data
Sands BE, et al. UEGW 2018
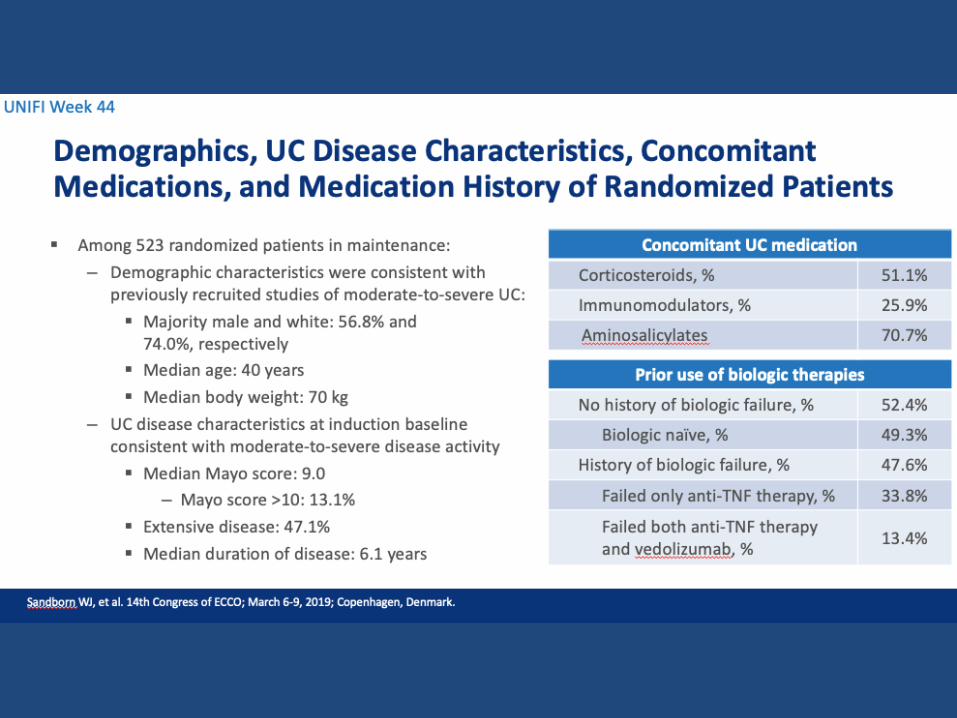
Conclusions
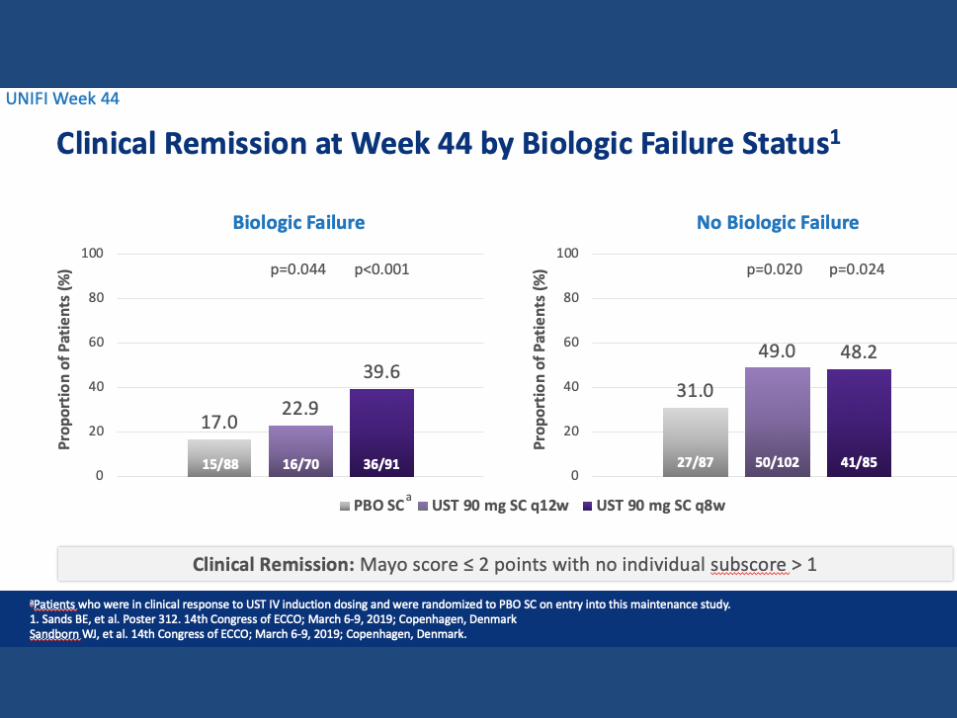
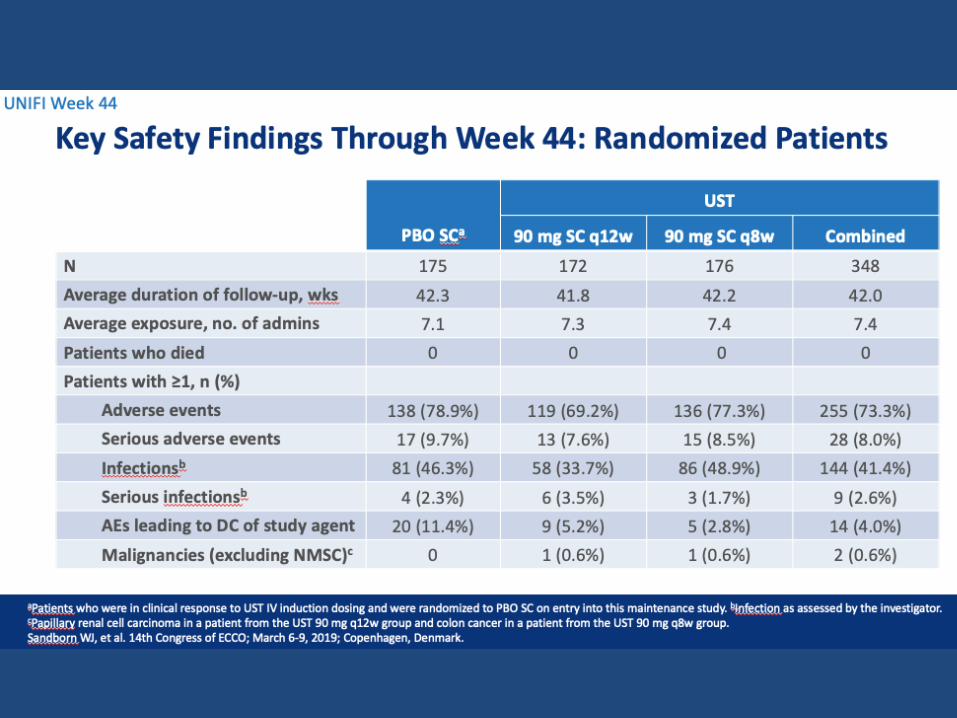
• UST effective for maintenance in UC patients who respond to induction
• Overall remission at week 44: 44% (~all in CSF remission as well)
• Non-biologic failure patients do better
• Potential for q12w dosing (instead of q8w for biologic naïve)
• No new safety signals
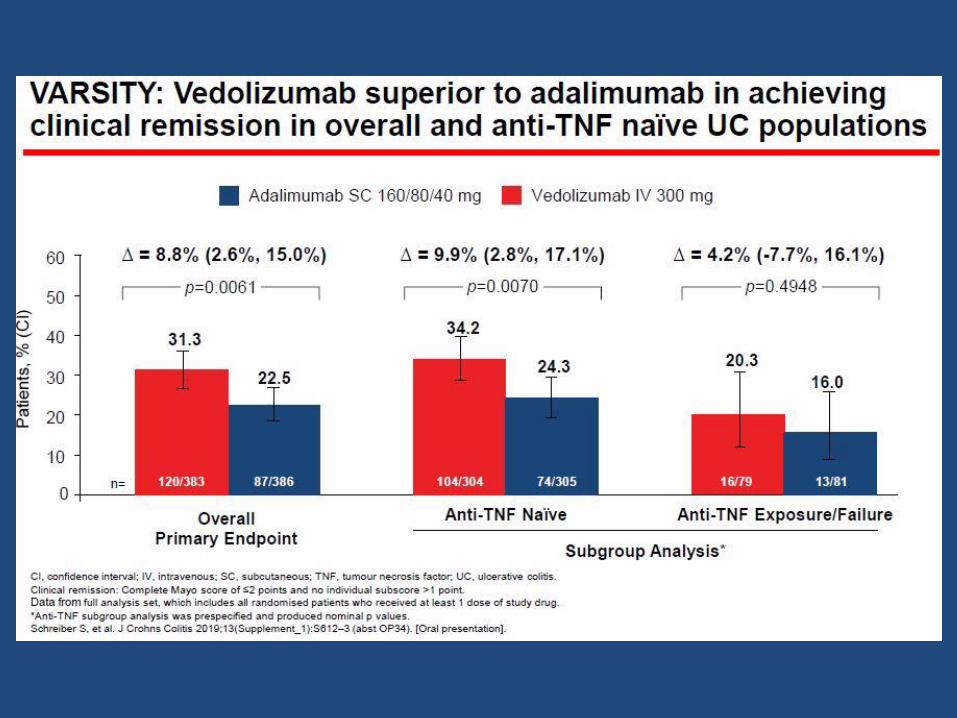
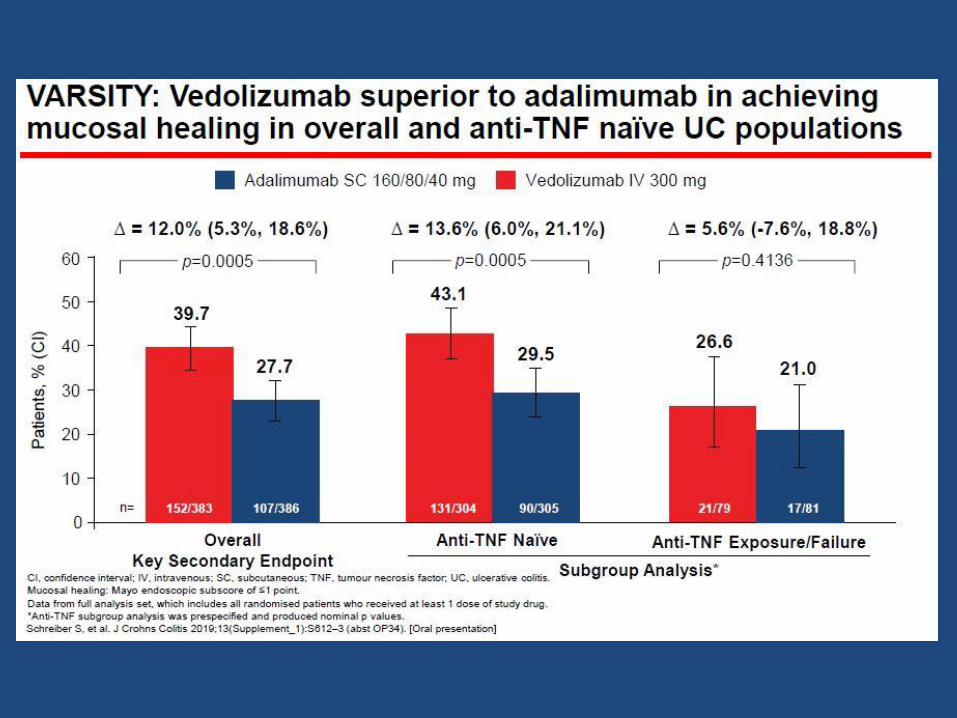
Vedolizumab Shows Superior Efficacy Versus Adalimumab: Results of VARSITY – the First Head-to-Head Study of Biologic Therapy for
Moderate-to-Severe Ulcerative Colitis
Bruce Sands, Laurent Peyrin-Biroulet, Edward Loftus, Silvio Danese, Jean-Frederic Colombel, Brihad Abhyankar, Jingjing Chen, Raquel
Rogers, Richard Lirio, Jeffrey Bornstein, Stefan Schreiber
Presentation 416a, Digestive Disease Week 2019
Conclusions
• Vedolizumab superior to adalimumab in key endpoints of clinical remission and mucosal healing at end of 1 year
• Most of benefit occurs in TNF naïve patients
• Major limitations are lack of dose intensification and presence of TNF exposed patients
• Important first step in comparative effectiveness

Real-World Effectiveness of Tofacitinib in Ulcerative Colitis:
A Multi-Centre Study
Anish Patel1, Marc Fenster2, Geoffrey Bader1, Christina Dimopoulos2, Parakkal Deepak3, Ryan Ungaro2, Matthew Ciorba3, Andrew Yarur5,Robert Hirten2, George Christophi3, Aava Khatiwada3, Bixuan Lin5,
Jean-Frederic Colombel2, Christina Ha4, Benjamin Cohen2, Joel Pekow6, Poonam Beniwal-Patel5, Gaurav Syal4
Presentation 797, Digestive Disease Week 2019
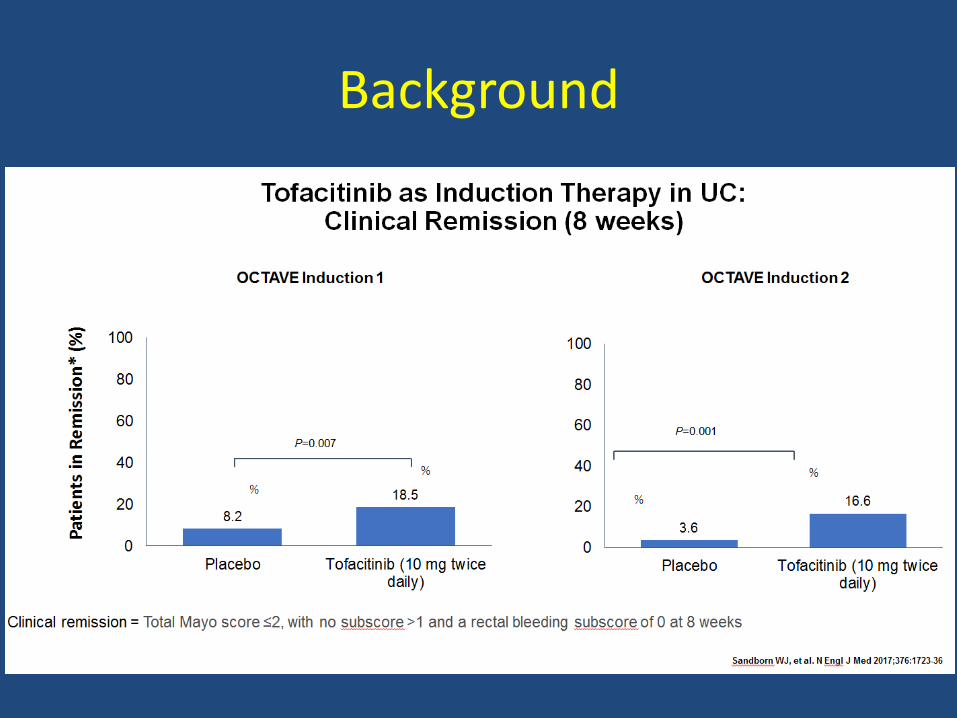
Background
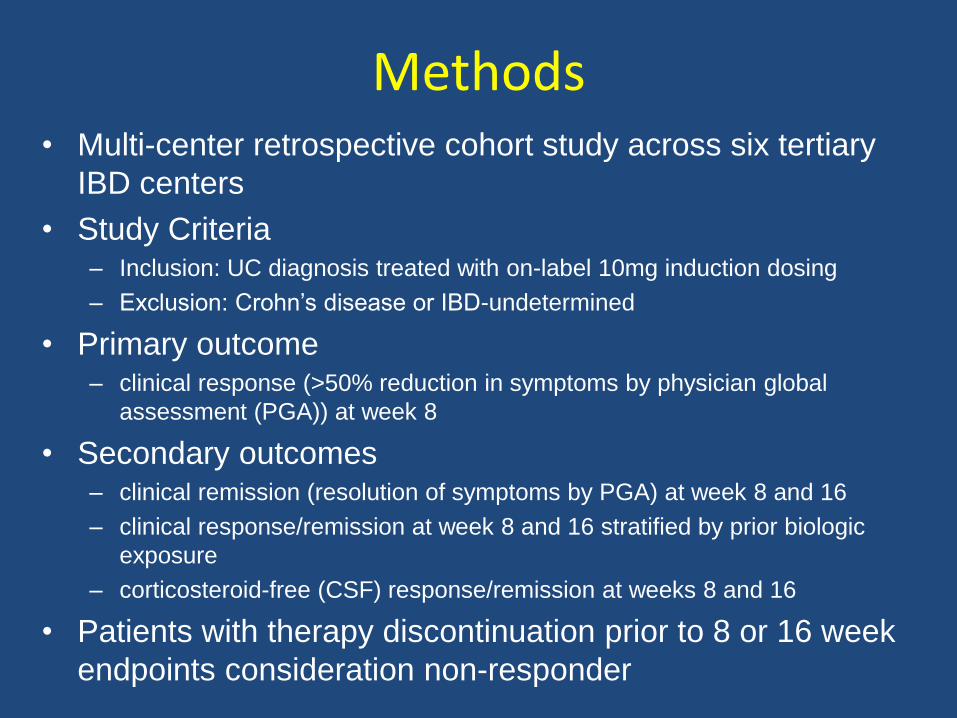
• Multi-center retrospective cohort study across six tertiary
IBD centers
• Study Criteria– Inclusion: UC diagnosis treated with on-label 10mg induction dosing
– Exclusion: Crohn’s disease or IBD-undetermined
• Primary outcome– clinical response (>50% reduction in symptoms by physician global
assessment (PGA)) at week 8
• Secondary outcomes– clinical remission (resolution of symptoms by PGA) at week 8 and 16
– clinical response/remission at week 8 and 16 stratified by prior biologic
exposure
– corticosteroid-free (CSF) response/remission at weeks 8 and 16
• Patients with therapy discontinuation prior to 8 or 16 week
endpoints consideration non-responder
Methods
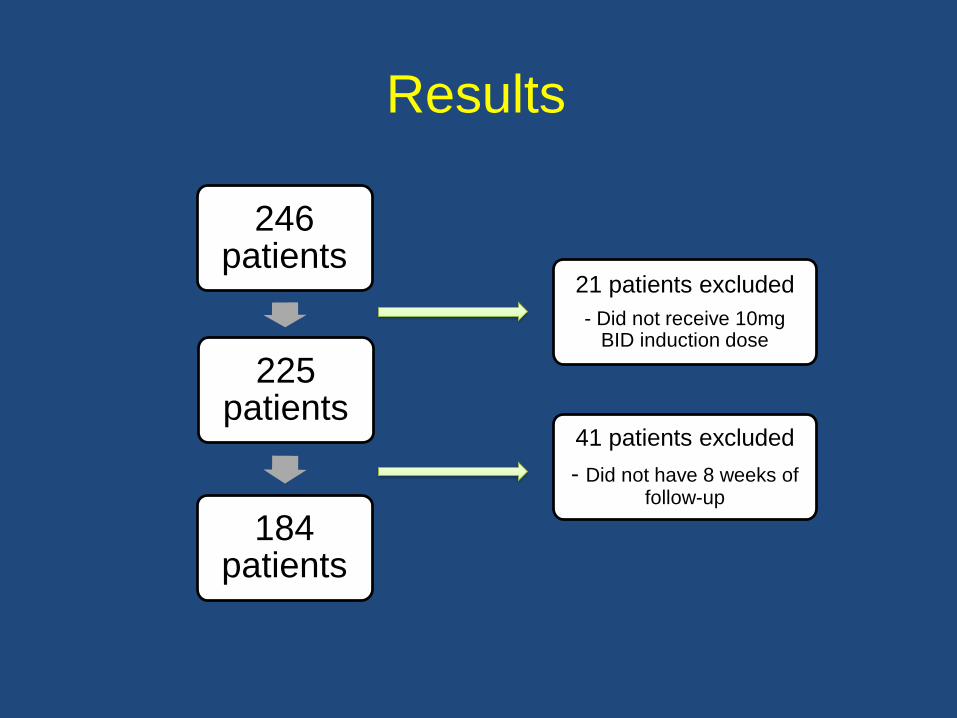
Results
246 patients
225 patients
184 patients
21 patients excluded
- Did not receive 10mg BID induction dose
41 patients excluded
- Did not have 8 weeks of follow-up
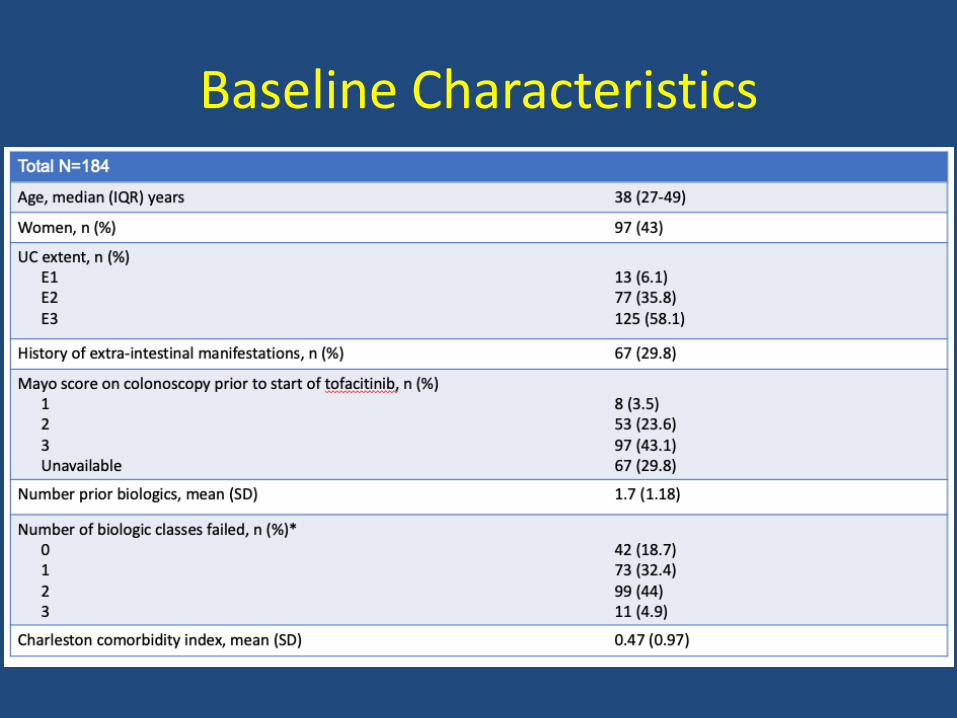
Baseline Characteristics
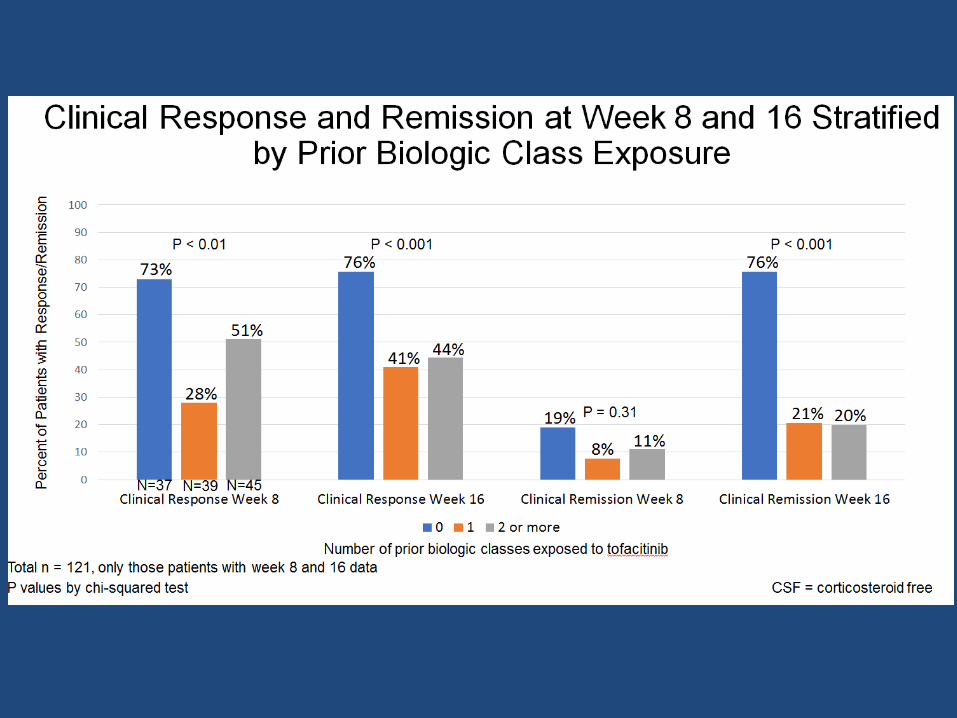
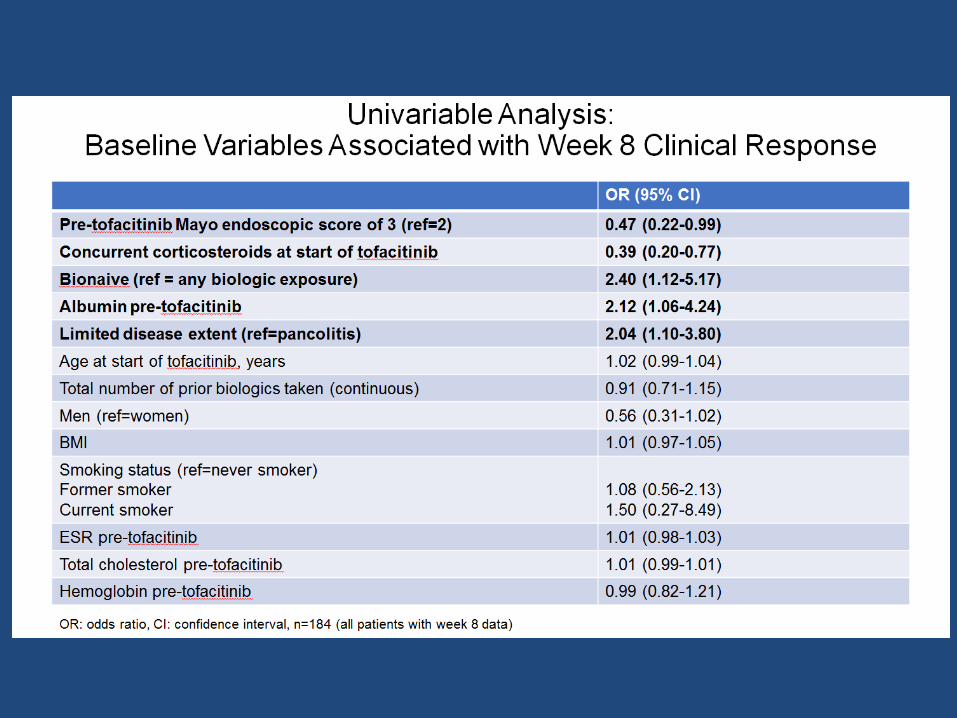
Conclusions
• Tofacitinib is effective at inducing short-term
clinical response/remission in a real-world
clinical setting by week 8
• Increase remission rates at 16 weeks compared
to 8 weeks though most who respond do so by 8
weeks
• Prior biologic exposure is associated with
decreased rates of clinical response/remission
One Line Highlights for Future Therapies
• Mirikizumab (anti-IL23) effective in Phase 2 trial in CD and UC
• ABX464 (increase miRNA124) effective in Phase 2a trial in UC
• Etrasimod (S1P modulator) effective in Phase 2 trial in UC
• Upadacitinib (JAK-1 inhibitor) effective in Phase 2 trial in CD and UC
Overall Summary
• Stopping 5-ASA when starting anti-TNF in CD does not result in worse outcomes compared to continuing 5-ASA
• No evidence for increased peri-operative infections in IBD patients on anti-TNF undergoing surgery
• FMT safe and effective for CDI in IBD patients
Overall Summary
• Ustekinumab effective for maintenance in UC in patients who respond during induction
• Vedolizumab superior to adalimumab in UC in first head-to-head trial comparing biologics with some notable limitations
• Tofacitinib effective in real-world analysis in UC