Inflammatory Bowel Diseases - Mucosal Immunology...2 Definition of Inflammatory Bowel Diseases (IBD)...
49
1 Wednesday Feb. 25 th 2015 8:15 – 9:00 Master's Course in Gastroenterology Universitätsklinik für Viszerale Chirurgie und Medizin Inselspital, Bern Source: MGH Crohn’s and colitis center Inflammatory Bowel Diseases Dr. med. P. Juillerat, MSc Oberarzt I Head of IBD clinical studies Source: medicaldaily.com
Transcript of Inflammatory Bowel Diseases - Mucosal Immunology...2 Definition of Inflammatory Bowel Diseases (IBD)...

1
Wednesday Feb. 25th 2015 8:15 – 9:00 Master's Course in Gastroenterology Universitätsklinik für Viszerale Chirurgie und Medizin Inselspital, Bern
Source: MGH Crohn’s and colitis center
Inflammatory Bowel Diseases
Dr. med. P. Juillerat, MSc Oberarzt I Head of IBD clinical studies
Source: medicaldaily.com

2
Definition of Inflammatory Bowel Diseases (IBD) Chronic relapsing inflammatory diseases involving : - The whole GI tract
Crohn‘s disease
11% : unclassified = undeterminate / unspecified colitis
- Colon and Rectum Ulcerative colitis
3
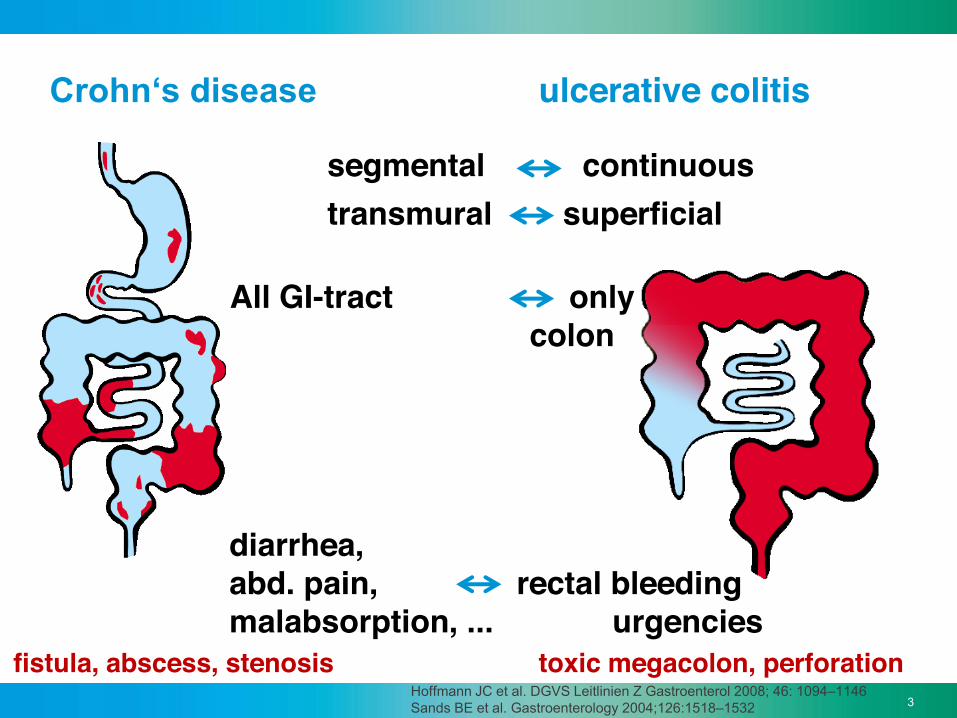
Crohn‘s disease ulcerative colitis
segmental continuous
diarrhea, abd. pain, rectal bleeding malabsorption, ... urgencies
All GI-tract only colon
transmural superficial
fistula, abscess, stenosis toxic megacolon, perforation Hoffmann JC et al. DGVS Leitlinien Z Gastroenterol 2008; 46: 1094–1146 Sands BE et al. Gastroenterology 2004;126:1518–1532

4
Prof. M. Neurath, Nature reviews 2014 ; vol. 14 : 329- 42
genes and environnment
The intestinal barrier is impaired
immune deficiency
Inappropriate «overreaction» of the immune system
Pathogenesis of IBD I

5
N= 14,763 CD, 10,920 UC and 15,977 controls Æ 193 suceptibility loci, among 71 new
Lees CW, Satsangi J. et al, Gut. 2011;60(12):1739-53. Jostins, et al nature 2012
Genetic of IBD (based on GWAS) Nature 2001

6
Pathogenesis of Inflammatory Bowel Diseases
Æ10 years ago
The Th1/Th2 paradigm. from Romagnani S. TH1/TH2 Cells. Inflamm Bowel Dis 1999;5:285–294.

7
Source: Baumgart et al. Lancet 2012
Anti-TNF alpha
Other Cytokines
Anti- integrin
ÆNOW !

8
Pathogenesis IBD II Microbiom «Dysbiosis»
Sokol H, Curr . Op .Gastro . 2010 . Round JL, Nat. Rev. Immunol. 2009
• ↓ Diversity of Bacteroidetes
• ↓ Firmicutes (e.g. Clostridium)
• ↑ Proteobacteria
• ↓ „good“ bacteries („Symbionts“ e.g. F. prausnitzii)
R. Navus F.Nucleatus Ecoli AIEC
F. prausznitzii R. intestinalis A. muciniphyla

9
HOW FREQUENT ?? Do you know people with IBD???
?

10
One Study on prevalence in Canton de Vaud � 1/500 individual has inflammatory bowel disease (IBD) In Switzerland : (Vaud is very similar to Switzerland for age and gender)
12’000 IBD patients (6100 CD; 5900 UC)
Juillerat et al. Journal of Crohn's and Colitis (2008) 2, 131–141

11
Switzerland compared to Europe
USA + Canada
Sud de l’Europe et Europe de l’Est
Nord de l’Europe
et Grande-Bretagne
Juillerat et al. Journal of Crohn's and Colitis (2008) 2, 131–141

12
First peak of prevalence between 20 and 40 years old
2nd peak of prevalence Around 60-70 years old But 20 – 30% of the patients are < 20 years old
Juillerat et al. Journal of Crohn's and Colitis (2008) 2, 131–141

13
Paradoxal effect of SMOKING
Deleterious for Crohn’s disease (OR >2), but protective for ulcerative colitis !! (OR 0.5)
however … no reason to smoke !
Cosnes J et al. Best Pract Res Clin Gastroenterol. 2004;18:481-496.

14
Crohn
Smoking and IBD Diagnosis
05
1015202530354045 UC Smoking cessation
Jahren
Cosnes J et al. Clin Gastroenterol Hepatol 2004; 2: 41-48
N= 1784 IBD, 1096 UC , 688 Crohn
279 (61%)
52 (12%)

15
Crohn’s Disease

16
Crohn‘s disease ILEITIS and COLITIS
17
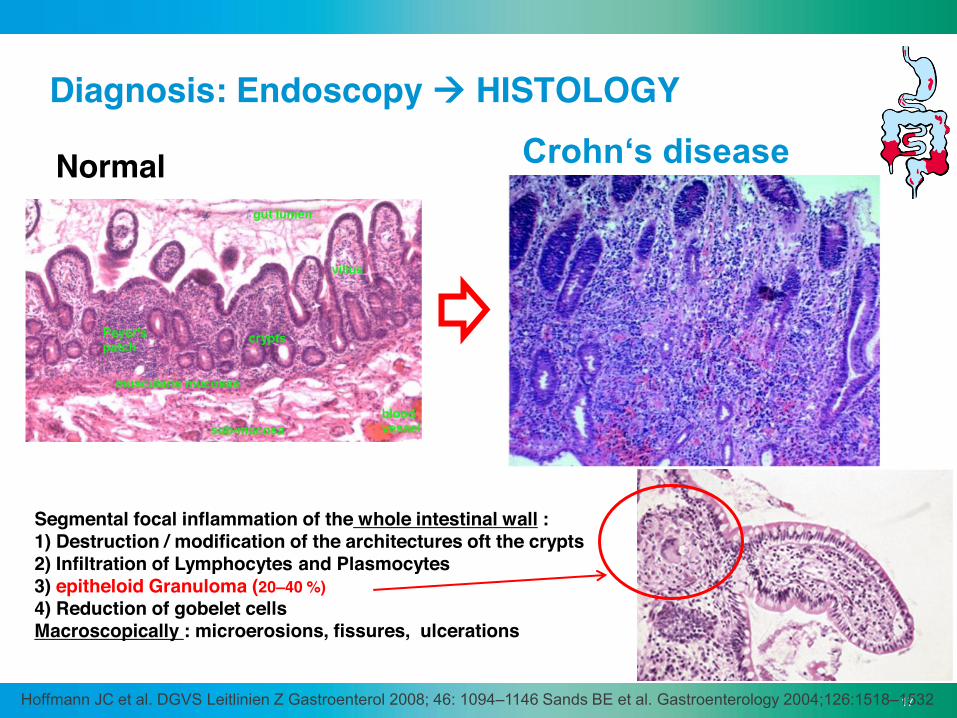
Diagnosis: Endoscopy Æ HISTOLOGY
Hoffmann JC et al. DGVS Leitlinien Z Gastroenterol 2008; 46: 1094–1146 Sands BE et al. Gastroenterology 2004;126:1518–1532
Segmental focal inflammation of the whole intestinal wall : 1) Destruction / modification of the architectures oft the crypts 2) Infiltration of Lymphocytes and Plasmocytes 3) epitheloid Granuloma (20–40 %) 4) Reduction of gobelet cells Macroscopically : microerosions, fissures, ulcerations
Crohn‘s disease Normal

18
Crohn‘s disease lesions
• Most frequent : terminal ileum & caecum
• Upper GI : rare
• rectum : rare and mostly associated with fistula
Harrisons Gastroenterologie und Hepatologie, 1. Auflage; Martin Zeitz, Hartmut H.-J. Schmidt, Christian Bojarski (Hrsg.); ABW Wissenschaftsverlag, 2011.
Upper GI : 4% Ileum & colon 40-55% Ileum only 30-40% Colon only 15-25%

19
Silverberg MS, et al. Can J Gastroenterol 2005; 19:5–36. Quelle: Baumgart et al. Lancet 2012
Montréal classification of Crohn‘s disease
20
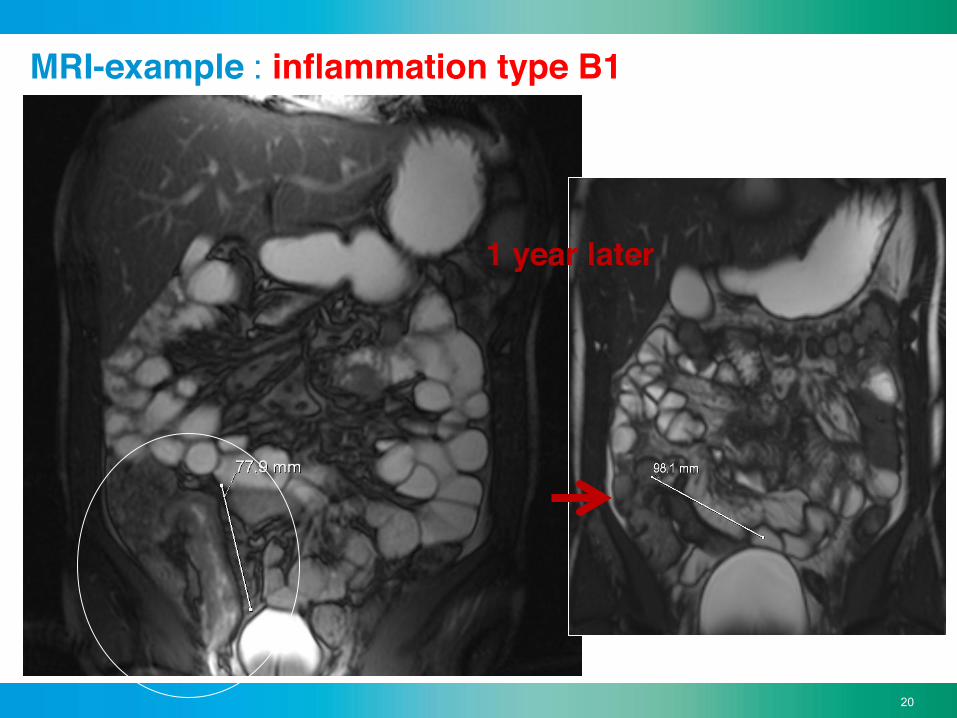
MRI-example : inflammation type B1
1 year later

21 21
Complication of the behavior of Crohn‘s disease: ulcerations Æ Stenosis – stricturing Type -
Courtesy of Prof. Dr. med. R. Ehehalt
ulcerations stenosis
22
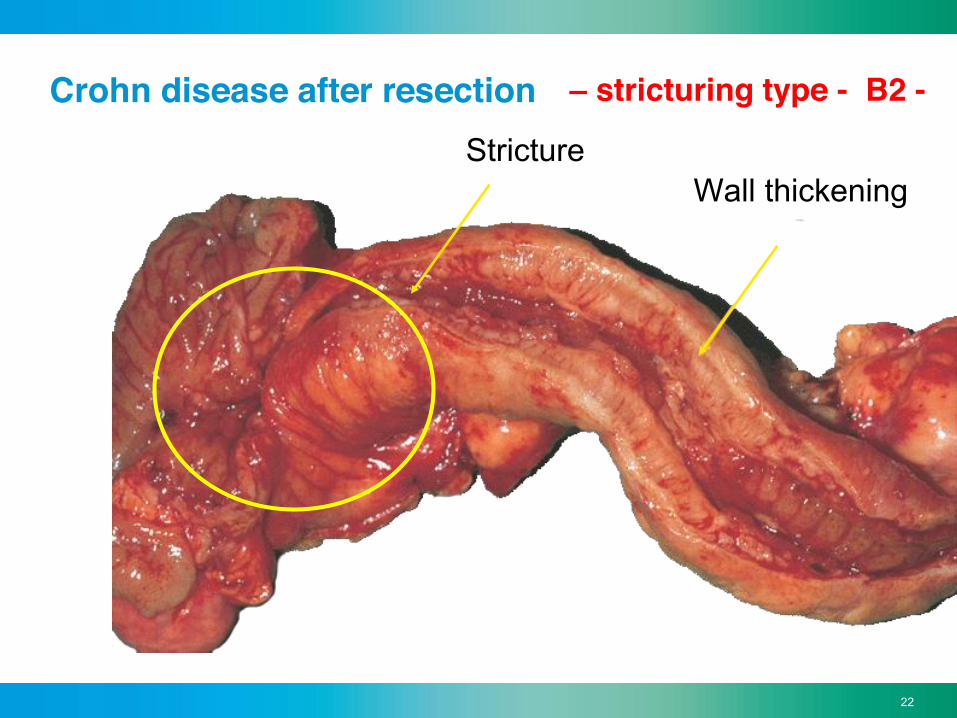
Crohn disease after resection
Wall thickening Stricture
– stricturing type - B2 -

23
Complication of the behavior of Crohn‘s disease: Perforations Æ Fistula – penetrating type - B3 - fistulizing perianal - +P -

24
Crohn disease : evolution
Cosnes J, et al. Gastroenterology 2011 ;140 (6):1785–1794

25
Progression of digestive damage and inflammatory activity in a theoretical patient with CD Pre-clinical Clinical
Inflamm
atory Activity
(CD
AI, CD
EIS, PCR)
Surgery
Stricture
Stricture
Fistula/abscess
Disease onset
Diagnosis Early disease
Dig
estiv
e D
amag
e
Progression of digestive disease damage (Lémann score) and inflammation
Pariente B et al. Inflamm Bowel Dis 2011;17(6):1415-22
Typ B1
Typ B2 Typ B3
TREATMENT

26
Therapeutical Arsenal
« Optimizing» therapy means currently: Æ An « accelerated» step –up ! OR …

27
Evolution of the need for surgery in CD since the 1930's and impact of medications
1930 1940 1950 1960 1970 1980 1990 2000 2010 2020 2030 0
10% 20% 30% 40% 50% 60% 70% 80% 90%
100% Probability of receiving biologics at 5 years Probability of receiving immunosuppressants at 5 years
Rate of surgery at 5 years
Disease duration before introduction of biologics (yr)
3-5 7-8 1-2
0 10% 20% 30% 40% 50% 60% 70%
Population-based studies (within 5 yr)
Randomised controlled trials (at 1 yr)
Referral centre trials (within 5 yr)
Before the era of biologics In the era of biologics
44.4
29
9.1 3.7
23.6 21.4
Courtesy LPB Bouguen and Peyrin-Biroulet, Gut 2011
28
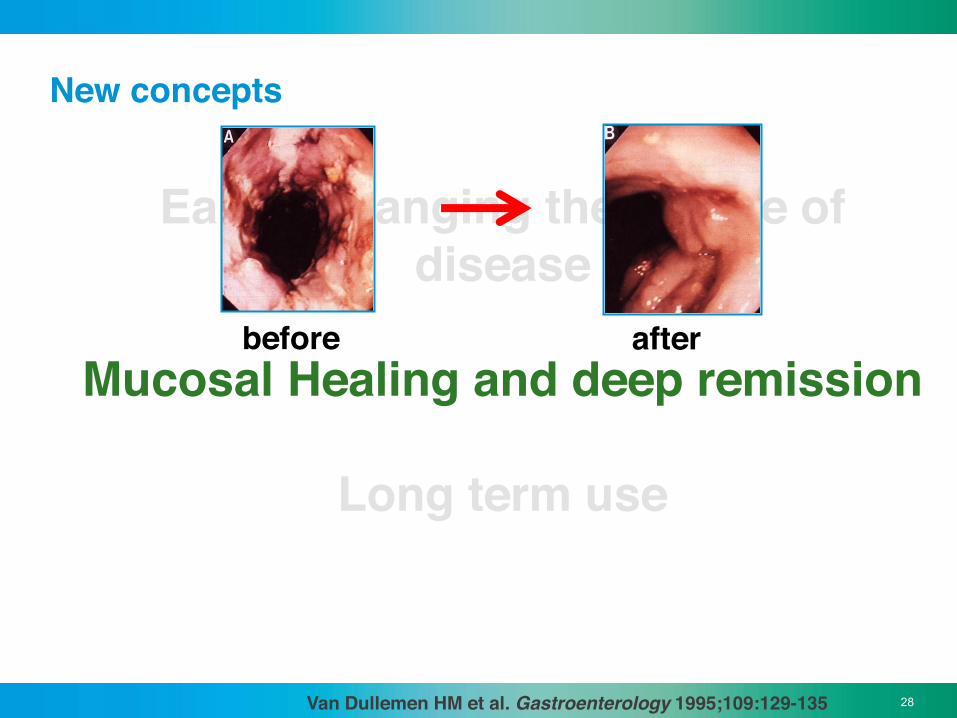
New concepts
Early : changing the course of disease
Mucosal Healing and deep remission
Long term use
before after
Van Dullemen HM et al. Gastroenterology 1995;109:129-135

29
« Mucosal Healing » = best prognosis
• longer period of steroid free remission
• ↓ hospitalizations
• ↓ intestinale resections (Crohn’s disease) or less colectomies (ulcerative colitis)
• ↓ neoplasia (↓ inflammation; UC)
80 vs 27% (Baert et al, 2010)
19 vs 28% ( Rutgeerts 2006) (Schnitzler IBD 2009) (Froslie, Gastroenterology + Am J Gastro 2007; Sjoberg
Gut 2008 [Abstract])
(Rutter 2004, Rubin 2006, Gupta 2007)
Congrès de l’ASPE, 12 sept. 2013 - Dr P. Juillerat MSc. Hôpital de l’île. Berne
30
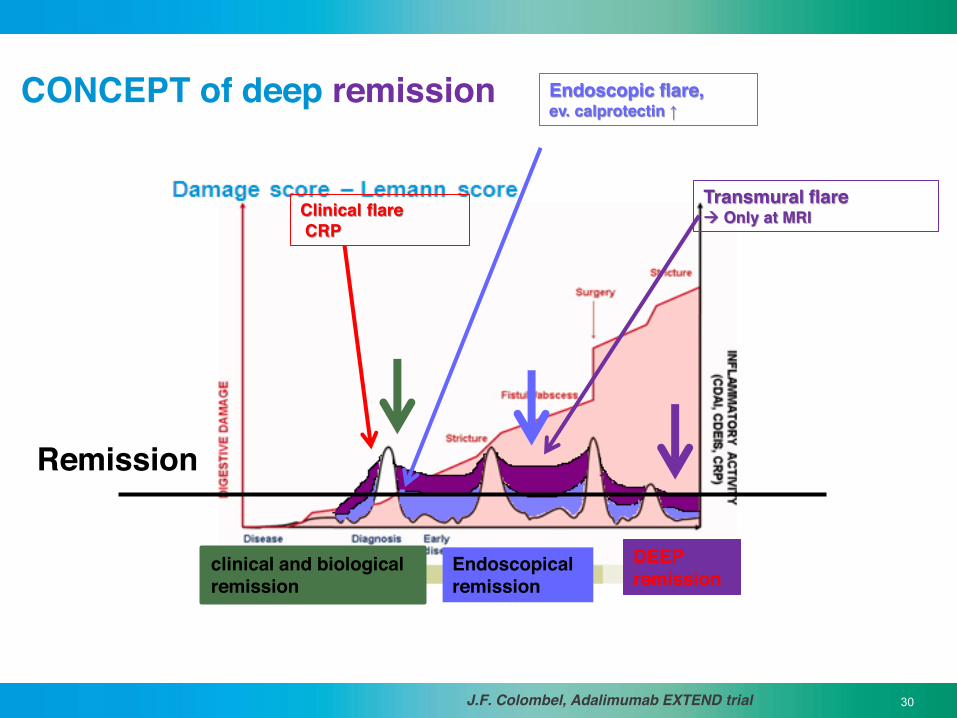
CONCEPT of deep remission
J.F. Colombel, Adalimumab EXTEND trial
clinical and biological remission
Endoscopical remission
Clinical flare CRP
Endoscopic flare, ev. calprotectin ↑
Transmural flare Æ Only at MRI
DEEP remission
Remission
31
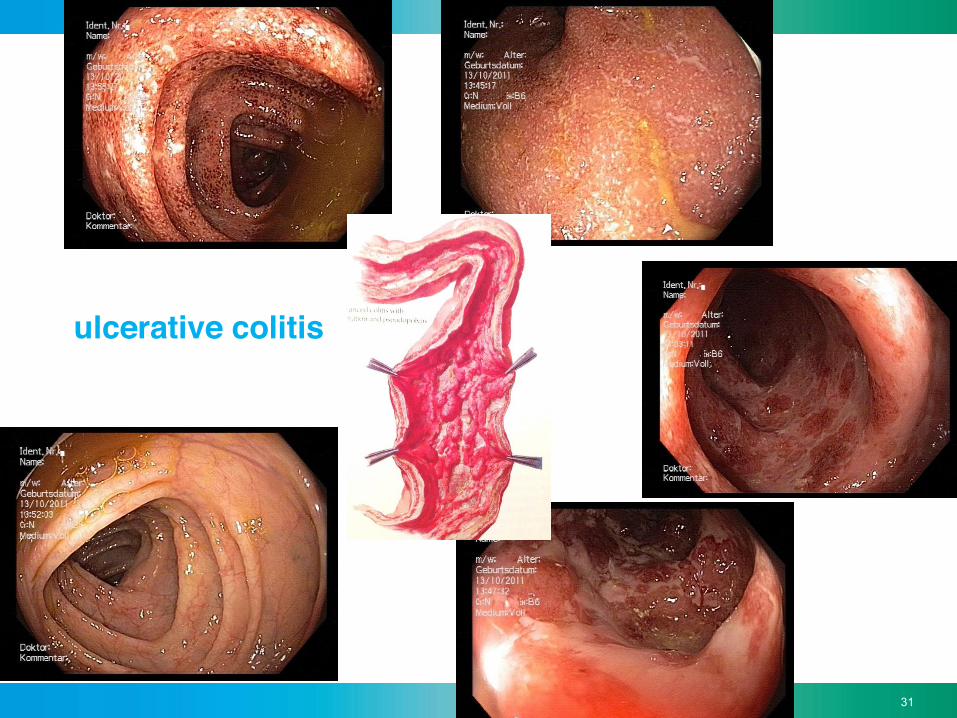
ulcerative colitis

32
Colitis ulcerosa – Befallsmuster
32
Harrisons Gastroenterologie und Hepatologie, 1. Auflage; Martin Zeitz, Hartmut H.-J. Schmidt, Christian Bojarski (Hrsg.); ABW Wissenschaftsverlag, 2011.
•Proctitis (40–50 %)
• rectal pain, urgency • stool incontinence • blood - mucus
Left sided colitis (30–40 %)
• bloody diarrhea • obstipation
Pancolitis (20 %)
• weight loss • fever • severe bleeding • abdominal pain
Backwash-Ileitis (10–20 % of patients with Pancolitis)
Montréal classification for ulcerative colitis E1 E2 E3

33
Mayo clinic (Rochester, USA) classification
Mayo 1 = mild - erythema + -↓ partial loss of vascular pattern
Mayo 2 = moderate - Erythema ++ - complete loss of vascularity - contact bleeding - Erosionen
Mayo 3 = hochgradig - Spontaneous bleeding - ulcerations Rutgeerts P, et al.. N Engl J Med. 2005 Dec 8;353(23):2462-76.
0 = Remission
34
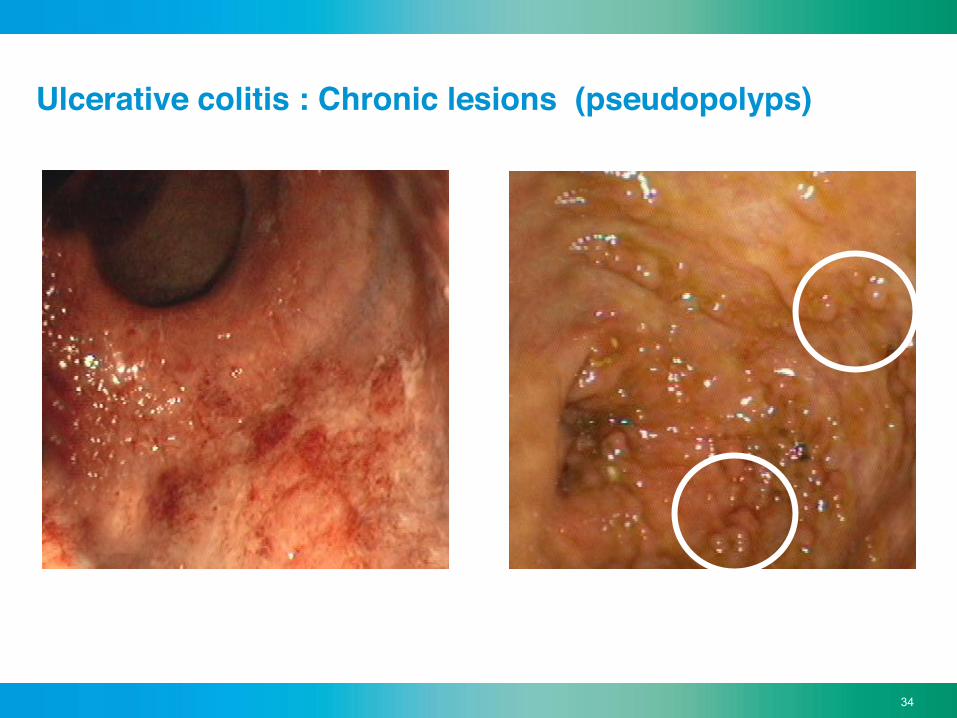
Ulcerative colitis : Chronic lesions (pseudopolyps)
Initial inflammation Æ Pseudopolyps

35
activity mild - moderate severe
Number stool/ d < or = 5 > 5
Blood in the stool few a lot
Temperatur < 37,5°C > = 37,5°C
Puls < 90/min > = 90
BSR < 30 mm/h > = 30mm/h
Hemoglobin > 10g/dl < = 10g/dl
Truelove SC, Witts LJ. Cortisone in ulcerative colitis; final report on a therapeutic trial. BMJ 1955;4947:1041–8
Fulminante or toxic colitis:
• > 10 Stool/d, continously with blood loss, Abdominal tenderness • Radiological wall thickening and potential dilatation of the proximal colon (megacolon)
Ulcerative colitis : evaluation of severity / TW criteria

36
Ulcerative colitis : fulminant colitis Æ colectomy
Source : Wikipedia
37
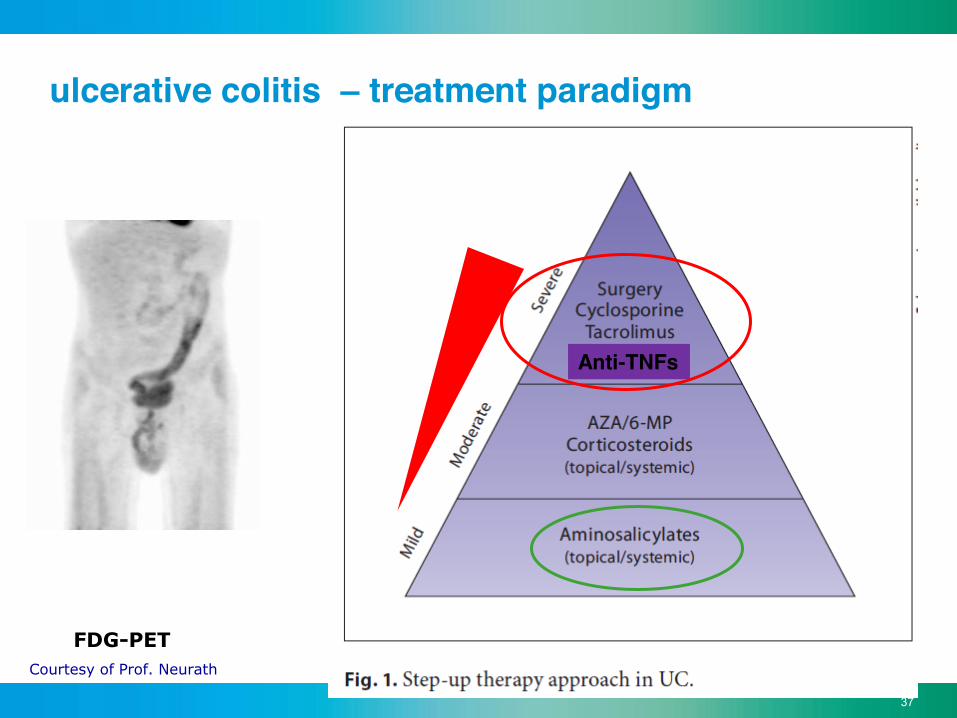
FDG-PET Courtesy of Prof. Neurath
ulcerative colitis – treatment paradigm
Anti-TNFs

38
Treatment algorithm for mild to moderate UC.
from Rogler, Dig Dis 2009;27:542–549
Anti- TNFs

39
Mucosal Healing and : colectomies LOR to infliximab

40
Groupe I: frequent extraintestinal manifestations Rheumatological
Ophtalmological
Dermatological
Hepatological
Peripheral arthritis
Typ I / II
Spondylarthritis
Uveitis (Epi)Scleritis
Stomatitis
Pyoderma gangrenosum Erythema nodosum
PSC
Vavricka SR, et al. Am J Gastroenterol 2011; Su & Lichtenstein Gastroenterol Clin N Am 2002
IBD Patients >35%

41
Dermatologische Stomatitis
Pyoderma gangrenosum
Erythema nodosum
15% IBD patients
Vavricka SR, et al. Am J Gastroenterol 2011; Su & Lichtenstein Gastroenterol Clin N Am 2002

42
Groupe II: Extraintestinale complications ! Æ Associated with bowel dysfunction / malabsorption
• Osteopenia/ porosis • Osteonecrosis
(could be steroid-associated)
• Gallstones •Choledocholithiasis • Leberabscesses • Portal vein thrombosis
Urological: • Renal stones
Hematological : • Anemia • coagulopathy
Pancreas: • Crohn of the papilla
Vavricka SR, et al. Am J Gastroenterol 2011; Su & Lichtenstein Gastroenterol Clin N Am 2002

43
Hypertrophic Osteoarthropathies Polychondritis
• Pyostomatitis vegetans • Psoriasis • Erythema multiformis • Epidermolysis bullosa • Vasculitis • Sweet Syndrome • Cutaneous Crohn
Harnwege: • Amyloidose • Obstructive Uropathie • Fisteln
Hematological, HNT, CNS,
pulmonary and cardiac manifestations
Groupe III: rare EI manifestations and associated diseases
• Pericholangitis • cirrhosis • Steatosis • Granulomatous Hepatitis • Autoimmune Hepatitis
Pancreas: • Granulomatous Pancreatitis
Vavricka SR, et al. Am J Gastroenterol 2011; Su & Lichtenstein Gastroenterol Clin N Am 2002

44
Terzic, Gastroenterology 2010
Ulcerative colitis associated colorectal carcinoma

45
Recommendations for colitis (Crohn or UC) colorectal cancer screening
• Based on disease duration and extension: 8–10 Jahre (pancolitis) 15-20 Jahre (left –sided colitis) • then, controls (in particular with pancolitis)
every 2–3 years after 20 y. dis. duration every 1-2 years after 30 y., 40 y., ...
• CAVE: every year with the diag. of primary sclerosing cholangitis
Farraye AGA Technical review GE 2010, Josh Korzenik MGH , Boston

46
! !
Wang, Loftus et al. Am J Gastro 2013; 108:444-9

47 Farray. AGA Medical Position Statement and Technical Review, Gastroenterology 2010
High grade Dysplasia
DALM: Dysplasia-Associated Lesion or Mass Adenoma-like DALM Non-Adenoma-like DALM
Low grade Dysplasia
3-6 Mo

48
Chromoendoscopy • Dye: Indigocarmin (or methylen blue) vial of 5 ml, with 20 ml NaCl [Spritze] (or 10 ml/50 ml) Æ Spray – catheter => use oft at least 40 ml

49
Lausanne
Genève
Zürich
Basel
St-Gallen
Bern
Æ From November 2006 till now
SWISSIBDcohort study
www.ibdcohort.ch