Inflammatory bowel disease (ibd) drug information page
60
Inflammatory Bowel Disease By : Dr. Ibrahim Gomaa’ Drug Information page
-
Upload
ebrahim-gomaa -
Category
Spiritual
-
view
326 -
download
4
Transcript of Inflammatory bowel disease (ibd) drug information page
Inflammatory Bowel DiseaseBy : Dr. Ibrahim Gomaa’Drug Information page
Inflammatory Bowel Disease
Chron’s disease
Ulcerative Colitis

Chron’s disease
Chronic episodic inflammatory
condition of gut affecting entire wall of bowel
region involved
Affect any part of GIT from lips to
anal margin
Current treatment is
palliative not curatice

Epidemiology
Most commonly in patients between 15-40
years
More common in females

Etiology
Immunology
Genetic factors
Diet
Infective agents
There
is no
specifi
c cau
se of
IBD

EtiologyImmunology
Characterized as autoimmune
disease
Occue when immune system attacked &
leading to GIT discomfort by increasing GIT wall
inflammation
Improvement in nutitional status
may improve immune system
There
is no
specifi
c cau
se of
IBD

EtiologyGenetic factors
genetic incidence hasnot been
established although 10 % of patients have 1st degree relative to disease
There
is no
specifi
c cau
se of
IBD

EtiologyDiet
Patients with chron’s disease :
Increase intake of sweet , fatty or
refines food
Decrease intake of fructose , fruits , water , K , Mg &
vitamin C
There
is no
specifi
c cau
se of
IBD

Etiology
Infective agents
Patholoical similarities between chron’s & TB focus attention on mycobacterium
species
Have higher fecal counts of aerobic gram –ve rods & gram +ve coccoid rods from
cporococcus & peptosterptococcus
There
is no
specifi
c cau
se of
IBD

Clinical Manifestation
Anorexia&
Wieght loss
Nausea DiarrheaAbdominal
painAbdominal tenderness
Depending on the severity & site of activity so the patient can present with systemic &
intestinal symptoms
Most Significant
Non Specific

Investigation
Endoscopy
Radiology
Histology
Blood test

Endoscopy
Colonoscopy
Most reliable diagnosis as it allow direct visualization of colon & terminal ileum
Finding of patchy distribution of disease
with involvement of colon or ileum but not
rectum
indicate Chron’s disease
Standard
test

Radiology
Double contrast barium enema

Histology
Differentiate between small bowel & colonic lesions wrongly labeled chron’s disease

Blood tests
Test for anemia & vitamin B12 deficiency
Test for up regulation of immune system

Ulcerative Colitis
Disease of colon characterized by
ulcers & inflammation in
colon
Chronic relapsing inflammatory
disease affecting colonic & rectal
mucosa
AffectingOnly rectal mucosa =
proctitisRectum & sigmoid
colon = asproctosigmoiditis
Other organs = colitis

Epidemiology
More common in non smokers
No variation between men & women or in
socioeconomic groups

Etiology
Genetic factors
Environmental factors
There
is no
specifi
c cau
se of
IBD

Etiology
Genetic factors
Familial or genetic incidence of ulcerative colitis has wide variation from
1-16 %
There
is no
specifi
c cau
se of
IBD

EtiologyEnvironmental
factors
Infective agents
There
is no
specifi
c cau
se of
IBD
Diet Psychological stress

Clinical Manifestation
Abdominal pain
Diarrhea mixed with
blood & mucous
Elderly suffering from
proctosigmoiditis may complain of
constipation
Patients complain from systemic & intestinal symptomsProctitis = Only intestinal symptoms
Proctosigmoiditis = More severe symptoms

Clinical Manifestation
Determination of severity of ulcerative colitis quantitavily by monitoring:
The number of bowel motions
Macroscopic appearance of blood in
stools
Anemia Erythrocyte sedimentation
rate

Investigation
Endoscopy
Radiology
Laboratory tests

Endoscopy
Sigmoiscopy
Used to confirm diagnosis of ulcerative colitis

Radiology
Double contrast barium enema

Laboratory tests
Microbiological examination of stool
Haematological & biochemical values
High WBC countsIron deficiency anemia
Low ESR Low serum albumin
May provide evidence of infection as a cause of colonic
inflammation

Treatment
Non- Pharmacological
Pharmacological
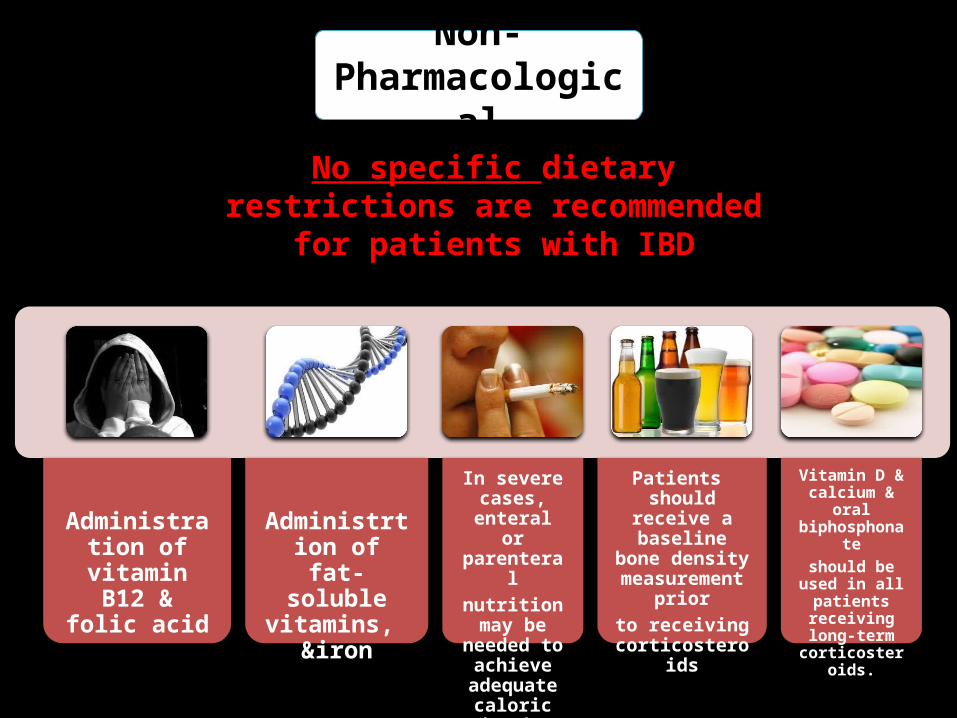
Non- Pharmacological
No specific dietary restrictions are recommended for patients with IBD
Nutritional strategies :in patients with long-standing
Administration of vitamin B12
& folic acid
Administrtion of fat-soluble
vitamins, &iron
In severe cases, enteral or parenteral
nutrition may be needed to
achieve adequate
caloric intake
Patients should receive a baseline
bone density measurement
priorto receiving
corticosteroids
Vitamin D & calcium & oral biphosphonate
should be used in all patients
receiving long-term
corticosteroids.

Drug treatment
Corticosteroids
Aminosalicylates
Immuno suppressants
Cyclosporin
Other agents

Corticosteroids
Eg
Predinoslone
Steroid of choice as it can be used
orally , rectally & parentrally in
emergency Adverse
effects
CataractsSkin
AtrophyHyper -tension
Hyper glycemia
Adrenal suppression
Osteo-porosis
increased risk of
infection
Increased when dose < 40mg/day
Avoided by
Alternate day regimen
Steroid sparing properties of Azathioprone

Corticosteroids
Eg
Predinoslone
Steroid of choice as it can be used
orally , rectally & parentrally in
emergency
Dose :20–60 mg orally or IVUsed up to 2 weeks

Corticosteroids
Eg
Hydrocortisone
300 mg IV in three divided doses100 mg rectally at
bedtime90 mg rectally once or
twice daily
25–50 mg rectally twice daily

Corticosteroids
Eg
Budesonide
Induction: 9 mg orallyMaintenance: 6 mg orally
May prevent some long-term adverse effects in patients who
have steroid-dependent IBD.

Amino salicylates
Eg
SulfasalazineThe most effective in
maintaining remission in ulcerative colitis
( Anti-inflammatory )
Adverse effects
Nausea &
Vomiting
Haemo-lytic
anemiaHeadache Skin rash
Hepatic & pulmonary dysfunction
Aplastic anemia
Azo- spermia
Dose related Idiosyncratic

Amino salicylates
Eg
Sulfasalazine
DoseMaintain remission : 2-4 g / day
Acute attacks : 4-8 g / day
The most effective in maintaining remission in
ulcerative colitis
( Anti-inflammatory )

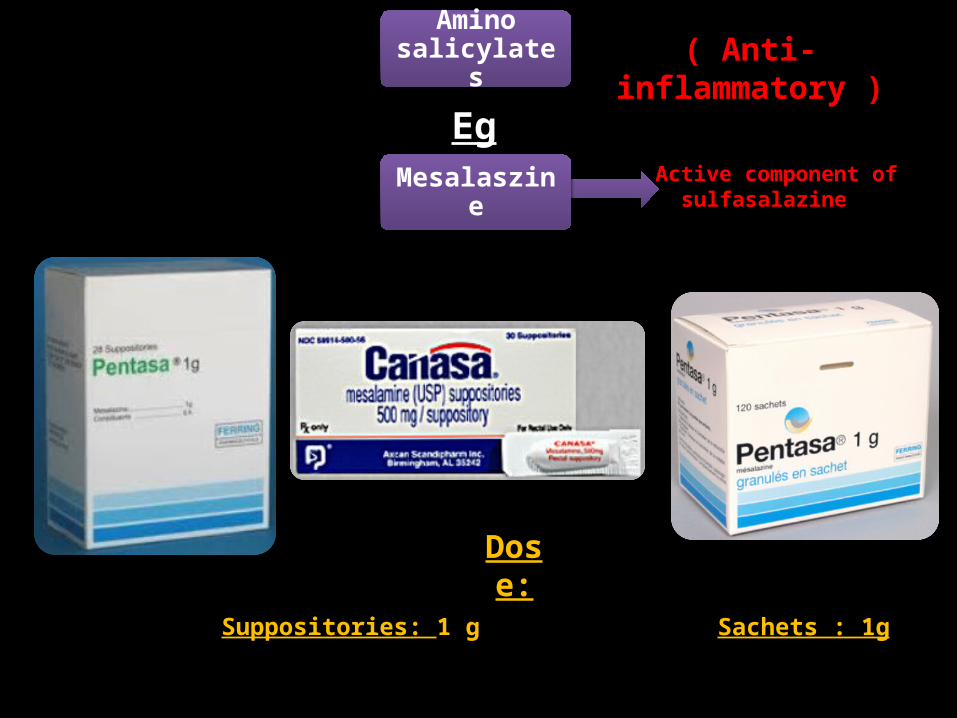
Amino salicylates
Eg
Mesalaszine
DoseDelayed release tablets : 1.6–4.8 g
Active component of sulfasalazine
( Anti-inflammatory )
Amino salicylates
Eg
Mesalaszine
Suppositories: 1 g
Active component of sulfasalazine
( Anti-inflammatory )
Sachets : 1g
Dose:

Amino salicylates
Eg
MesalamineActive component of
sulfasalazine
( Anti-inflammatory )
Dose:Enemas : 4 g
Amino salicylates
Eg
OlsalazineUses two Mesalamine
molecules linked together
( Anti-inflammatory )
Dose:Capsules: 1–3 g

Amino salicylates
Eg
Balsalazide
( Anti-inflammatory )
Dose:Capsules : 2–6.75 g

Used in patients unresponsive to steroid & amino salicylates
Immuno suppressants
Eg
Azathioprine
Dose:1.5–2.5 mg/kg per day orally
Inhibit purine biosynthesis & reduce IBD-associated GI
inflammation
Most useful fo
r maintaining
remission of IB
D or reducin
g
the need for lo
ng-term
use
of cortico
steroids

Used in patients unresponsive to steroid & amino salicylates
Immuno suppressants
Eg6-
Mercaptopurine
Most useful fo
r maintaining
remission of IB
D or reducin
g
the need for lo
ng-term
use
of cortico
steroids
Dose:1.5–2.5 mg/kg per day orally
Active form of Azathioprine

Used in patients unresponsive to steroid & amino salicylates
Immuno suppressants
Eg
MethotrexateMost
useful for m
aintaining
remission of IB
D or reducin
g
the need for lo
ng-term
use
of cortico
steroids
Dose:15–25 mg weekly
(IM/SC/orally)

Used in patients unresponsive to steroid & amino salicylates
Immuno suppressants
Eg
CyclosporineMost
useful for m
aintaining
remission of IB
D or reducin
g
the need for lo
ng-term
use
of cortico
steroids
Dose:4 mg/kg per day
Effective in patients refractory to cenventional drug therapy

Immuno suppressants
Eg
Infliximab
Adverse effects
Intravenous administration
Fever Chest Pain
Hypo-tension
Dyspnea
Associated with
reactivation of serious infections
Exa- cerbation of heart failure
infusion-related reactions
Effective in patients whose conventional therapy failed
Dis advantages
Significant drug cost Potential for adverse effects

Immuno suppressants
Eg
Infliximab Effective in patients whose conventional therapy failed

Other agents
Eg
Metronidazole
Dose:Adults : 500mg 3times for 7-10 days.
Children : 125-250mg./8Hrs.for 7-10 days.
Used in chrons disease & maybe effective in U.colitis
Other agents
Eg
Antibiotics
Dose:Adults < 12 yrs : 250 - 500mg / 12 hrs for 7-14 days.
Eg. Ciprofloxacin
For active chrons disease accompained by fever

Other agents
Eg
Antibiotics
Dose:Adults & children: 250 - 1000mg / 6 hrs for 7-14 days.
Eg. Cephazolin
For active chrons disease accompained by fever

Other agents
Eg
Antibiotics
Dose:Adults : 500 - 1000mg / 6-8 hrs for 5-10 days.Children: 50-100 mg/ 6-8 hrs for 5-10 days.
Eg. Ampicillin
For active chrons disease accompained by fever

Other agents
Eg
Anti DiarrhealRelief diarrhea symptoms
associated eith IBD
Diphenoxylate LoperamideCodiene
Delay corre
ct diagnosis
because masking
inflammation , infecti
on ,
obstructi
on or colonic
dilatation

Other agents
EgNa
CromoglycateReduce degranulation of mast cells & inhibits passage of Ca
ions across cell membrane
Treatment of IBD in Special Populations
Elderly Patients
Children & Adolescents
Pregnant Women
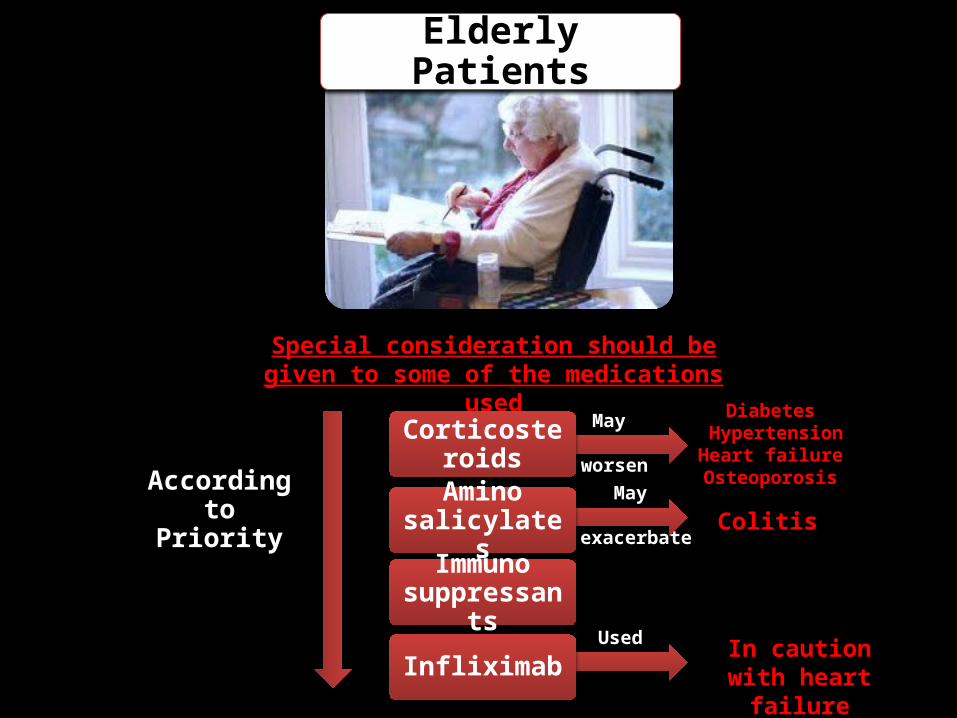
Elderly Patients
Special consideration should begiven to some of the medications used
CorticosteroidsDiabetes
HypertensionHeart failureOsteoporosis
May
worsen
Amino salicylates Colitis
May
exacerbate
Immuno suppressants
InfliximabUsed In caution with
heart failure
According to Priority

Children & Adolescents
major issue in children with IBD is the risk of growth failure secondary to inadequate nutritional intake
Amino salicylates
Azatioprine & 6-mercaptopurine
viable options for treatment and
maintenance of IBDin pediatric patients
infliximab
Corticosteroidshigher risk for IBD-
associated bone demineralization
According to Priority

Pregnant Women
Amino salicylates
Corticosteroids
Safe to use inpregnancy, but
sulfasalazine is associated with folate malabsorption
Azatioprine & 6-mercaptopurine
infliximab
For active disease not maintenance of remissionAccording to
PriorityCyclosporine
Methotrexate
Minimal risk in pregnant
Abortifacient & contraindicated during
pregnancy

Patient Education

Patient Education
Patients taking
steroids must be issied with steroid card
If symptoms recur patient should hhave
written instructions to
increase the dose of current
therapy
Effective home treatment of
proctitis is important
Patient Education
Infertility assoiciated with sulphasalazine
so use alternative
aminosalicylates
When considering
treatment with azathioprine or
6-MP, obtain baseline CBC & liver function
tests
Pregnant patients treated with sulfasalazine
should besupplemented
with folic acid 1 mg orally twice
daily

DRUG INFORMATION
PAGE HTTPS://WWW.FACEBOOK.COM/PAGES/DRUG-
INFORMATION/468006543282058
![Inflammatory Bowel Disease - BSWHealth.med · Inflammatory Bowel Disease: ... • Infectious colitis: Salmonella, E. coli, ... IBD Path Pitfalls Handout.ppt [Compatibility Mode]](https://static.fdocuments.in/doc/165x107/5cc8e3e088c9937c048b644f/inflammatory-bowel-disease-inflammatory-bowel-disease-infectious.jpg)