LTPAC Roundtables3.amazonaws.com/rdcms-himss/files/production...• Long Term Care Facilities (6)...
44
LTPAC Roundtable Meeting 4 LTPAC Health IT Leadership Challenges and Strategies April 12, 2016
Transcript of LTPAC Roundtables3.amazonaws.com/rdcms-himss/files/production...• Long Term Care Facilities (6)...

LTPAC Roundtable Meeting 4 LTPAC Health IT Leadership Challenges and Strategies
April 12, 2016

Gregory L. Alexander, PhD Professor Sinclair School of Nursing University of Missouri [email protected]
John F. Derr, RPh. CEO JD & Associates Enterprises, Inc. [email protected]
Lorren Pettit, MS, MBA Vice President, Research HIMSS North America [email protected]

• To provide LTPAC IT leaders (providers and vendors) with a forum for informing HIMSS North America (HNA) on ways the HNA association can help;
– advance the adoption and use of health information technologies within LTPAC provider organizations,
and
– advocate LTPAC’s IT needs and concerns to external healthcare IT organizations (e.g. acute-care providers; HIT vendors; policymakers).
LTPAC ROUNDTABLE: Mission

LTPAC Health IT Leadership Challenges and Strategies
April 2016

Denni McColm Chief Information Officer Citizens Memorial
Chuck Czarnik Vice President, HIT Strategy and Support Brookdale Senior Living Solutions

How does LTPAC look? Multidimensional, Widespread, Complex, Chronic -1.5 million residents whose average length of stay is just over 2 years. -Leading primary diagnoses circulatory system (25%), mental disorders (16%), and diseases of the nervous system and sense organs (14%). -98% of NH residents receive assistance with ADLs, such as bathing, dressing, toileting, transferring and eating; and 51% received assistance with all 5 activities. -35% have bowel or bladder incontinence. -Residents with pressure ulcers (10.7%) ranged from stage 1 (2.6%) to stage 2 or higher (8.1%)
National Sample
Ownership N %
For Profit
Corporation 8558 57.7
Individual 535 3.6
Limited Liability 104 0.7
Partnership 1123 7.6
Government
City 86 0.6
City/County 94 0.6
County 456 3.1
Federal 6 0.04
Hospital district 131 0.9
State 149 1
Non-Profit
Church related 663 4.5
Corporation 2645 17.8
Other 288 1.9
*Region
Metro (>50000) 9448 63.8
Micro (10000-49999) 2186 14.8
Small Town (2500-9999) 1801 12.2
Rural (<2500) 1373 9.3
*Bed size
>120 4354 29.4
60-120 7580 51.1
<60 2903 19.6

Healthcare Team Role and Tasks: Where does IT fit in?
• Timely assessments • Determine appropriate level of care Accept responsibility for resident care
• Provide necessary discharge information at discharge Support discharges and transfers
• Provide legible progress notes in a timely fashion • Review and approve a patients treatment and care plan
Perform periodic pertinent resident visits
• Assess and manage change in condition • Guide end of life decisions Provide appropriate resident care
• Timely and legible medical orders • Accuracy of orders Provide appropriate and timely orders
• Pertinent explanations of medical decisions
Appropriate , timely, pertinent documentation
• Provide high quality care • Always keep the well being of patients in mind Perform and act appropriately
Source: Levenson, S.A. (2016) The role of practitioners and the medical director. In: Post Acute and Long Term Care Medicine: A Pocket Guide 2nd Ed. Pamela Fenstemacher & Peter Winn Ed. pp. 73-91. Springer:Switzerland.

Some IT leaders say successful implementation depends on the technology Infrastructure:
• Be interoperable
• Allow transference of health information
• Be secure
• Support collaboration among multiple disciplines

LTPAC: Key Issues and IT impacts
Issues How Technology Helps Reduce Costs Electronic processes improve worker
productivity, fewer administrative staff needed to process paperwork, reduced paper and storage costs.
Influences on Quality of Care
Anytime, anywhere access to patient information improves ability to provide care and responsiveness to residents/family members.
Higher Reimbursements Can more accurately document care given which results in full/higher reimbursement
Staff Recruitment and Retention
Improves work processes resulting in higher job satisfaction. Able to devote more time to resident care instead of paperwork.
Resident Recruitment Better documentation of care can improve CMS five star rating. Wireless access is becoming a “must have” for residents and their families.

Some Visions for LTPAC and Acute Care HIT Leadership
Accountability
Partnerships
Access
Leverage technology to generate, innovative efficient business and service strategies & models to establish a leadership role in the future of health wellness delivery. LTPAC HIT Collaborative: HIT Policy Priorities

• The regional/smaller LTPAC provider experience
• The multi-state/large LTPAC provider experience
• Summary Themes and Questions
Agenda

Denni McColm Chief Information Officer Citizens Memorial

• Hospital – 86 Beds – Med/Surg – ICU/Telemetry – Birthplace – Wellness (Psychiatry)
• Emergency Services
– Level III trauma center – Ambulance services – Hosted air ambulance
• Home Health, Hospice, HME, Health Transit
• Long Term Care Facilities (6) • Residential Care Facility (1)
• Physician Clinics • Rural Health Clinics
• Outpatient Services
• Ambulatory Surgery Center
• Carrie J. Babb Cancer Center

CMH By the Numbers
• Employees = 1,900 • Service Area = 5 counties • Service Area Population = 100,000
• The Joint Commission Accredited
• Sole Community Provider • Organization
– Public Hospital District and – Non Profit Foundation

Project Infocare Vision
• Enable a patient to enter anywhere into our continuum of care and have a personal identity that is maintained across that continuum
• Physicians and other caregivers will have access to all of that patient’s information within the healthcare system and across the community
• Providers will be able to document efficiently within the software system, which will free them to have more time to spend with patients
• The investment of time, talent and money will enable CMH to be a technologically advanced healthcare organization poised to grow and offer new services to our patients and the community at large

Factors that have shaped the role of IT and IT leadership at CMH
– IT is seen as a foundational tool to support organizational strategies – specifically continuity of care, growth and adaptability
–Serving patients across the continuum of care, including LTPAC

Challenges
• The normal . . . clinician adoption, resources, workflow redesign, security
• Specific to LTPAC – adapting software to those environments while still maintaining continuity of patient record

Medication Management
• Home med list vs. LTPAC med list • Provider order entry • Prescriptions vs. supply from central pharmacy
– Retail pharmacies – Barcoding – Resupply

Citizens Memorial Healthcare Acute Care Services (Hospital, EMS)
Long Term & Post Acute (Home Health, Hospice, LTC, Residential Care, HME) Ambulatory Services (Physician Practices, Rehab, ASC)
Other Acute Care Providers
Other Long Term & Post
Acute Providers

CMH Acute/LTPAC/Ambulatory – Internal

CMH Acute to Other Acute Provider CMH Acute to Other LTPAC Provider • Nurse calls report • Pertinent information for patient on paper
– H&P, Discharge Summary, Progress Notes, Imaging Reports/Images, Medication List
– Sent with patient, also may be Faxed to receiving facility
– Oh, yes. And for 10% we also send the CDA electronically through Direct Messaging to meet the Meaningful Use Measures

Other Acute Provider to CMH LTPAC Services
• Referral Management Systems – Data extracted to PDF or similar documents and made
available on a secure portal – Initiated by other acute care providers
– Oh, yes. And for a small % we also receive a CDA via Direct Messaging so the other provider can meet Meaningful Use

Other LTPAC to CMH LTPAC Services • Nurse calls report • Pertinent information for patient on paper
– H&P, Discharge Summary, Progress Notes, Imaging Reports/Images, Medication List
– Sent with patient, also may be Faxed to receiving facility
– No CDA electronically through Direct Messaging to meet the Meaningful Use Measures as LTPAC providers don’t have incentive to do so

Working with other LTPAC providers
• Distinction between small/community and large/chain – Small/community providers
• Lack knowledge about possibilities • Lack IT resources • Lack incentive
– Large/national • Understand possibilities • Have IT resources • Interested or already implementing

Greatest IT Challenges
• Complexity – Regulatory requirements – Payment models – Systems (software, medical devices, ancillary,
infrastructure • Security
– HIPAA – Cybersecurity

Example of Complexity & Impact on IT Alphabet Soup of Payment Reform • ACO, BCPI, CJR … eCQM ... MACRA, MIPS, MSSP …
PQRS, QRUR … SGR, VBP – Quality reporting (increasingly electronic) – Business & clinical intelligence >> Predictive
analytics – Case/care management
• Medical Home • Episodic
– Scale

HIMSS Role?
• Convener to share examples of success in navigating the new complex challenges
• Standards for interoperability – Helping maintain the focus on the important
few standards and getting those right/constrained without optionality
• Identifying and promulgating innovative and break through solutions

• The regional/smaller LTPAC provider experience
• The multi-state/large LTPAC provider experience
• Summary Themes and Questions
Agenda

Chuck Czarnik Vice President, HIT Strategy and Support Brookdale Senior Living Solutions

• Approximately 1,100 communities, 100,000 residents, 82,000 employees.
• Full-spectrum senior housing and post-acute care, including IL, AL, memory care, SNF, home health, hospice, therapy, in-home custodial care.
• Systems & Support: – Mobile-first EMR platforms for home health, therapy (Android-
based). – Full EMR for SNF (browser based). – Proprietary software for IL / AL / memory care. – Appx. 300 “IT / Support” staff, ~225 within IT dept., ~75 spread
throughout various business units. • About me:
– Former IT, now in analytics / business strategy. – This discussion will focus on information challenges /
interoperability.
About Brookdale
30

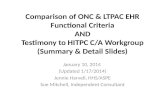
IT Components Across the Enterprise (Simplified)
31
C-Suite / E-Committee
CIO / IT (225)
Infrastructure / Support
Apps / Dev
R&D / BI
Operations
Clinical Informatics / S&P (40)
Clinical Analytics (6)
Ops FP&A (6)
Shared Services
Revenue Cycle / FP&A (6)
Sales Systems / Resident
Engagement (10)
ERP / Human Capital (6)
Integration Office (PMO)

• Acquisition-oriented culture – Systems architecture- blending and standardizing. E.g.
Emeritus integration – Execution in scale- e.g. 50 sites / quarter = 6 years – Often first-to-market in R&D, but scale can be a barrier
• Healthcare industry transition: – Volume to Value framed as a transition from a model of
“Service” to a model of “Insight.” Monetize what you “know” along with what you “do”
– Leverage the “continuum” – New delivery models:
• In-home care • Hospital -> SNF diversion • SNF -> AL diversion
Current Factors Affecting IT Leadership
32

• New delivery models / insight-based delivery driving appetite for answers: customer / patient / operations
– However, every delivered answer creates exponentially more questions
– Challenge: How to satisfy the appetite in a sustainable way?
• Strategy: – Information governance reform – End user self-service – Simplify knowledge and tools for the business – Avoid in-house development – Mobile-first approach
Current Factors Affecting IT Leadership
33

• Physician portals – HH and SNF
• CMMI grant – INTERACT transitions of care interoperability components
• DIRECT messaging
• HIE challenges
Brookdale Acute Care Interaction – Successes and Challenges
34

• Web- and mobile-app based tools that allow physicians to access HH and SNF charts
– 100’s of users in HH, expansion underway; recently launched for SNF
– Order entry, e-signature, care plan oversight, chart review functions
• Challenges: – Physicians manage multiple portals for providers – Legal consents / access agreements – Industry needs better authentication methods (2-factor,
etc.) – Not true “interoperability” – data not exchanged between
EMR’
Brookdale Acute Interaction – Physician Portals
35

• 3 yr., $7.9MM grant to expand and deploy INTERACT in SNF, AL, HH, IL.
– “Interventions to Reduce Acute Care Transfers” developed by FAU. Partnership between FAU, Brookdale, UNTHSC (2012-2015)
– Funding to interconnect Brookdale systems with hospitals for transition of care workflow and grant reporting. ~70 ADT connections established
• Lessons Learned: – Very tedious process to interconnect, even using CCD
standards. – Meaningful Use “disincentive” – Post-grant use case
Brookdale Acute Interaction – CMMI Grant
36

• Launched 2015, primarily supporting SNF • Inbound message to Brookdale upon referral to SNF • Allows Hospitals to attest MU e-transfer to LTPAC • Challenges:
– Messaging functions not integrated into clinical workflow (EMR limitation, timing issues). Data is often redundant. No attachment functions
– Single mailbox per site (no person to person), no provider directory
– Attachment functions – Complex / costly process to establish HISP relationship
Brookdale Acute Interaction - DIRECT
37

• Highly varied cost structure – Florida HIE Patient Lookup Service $49k+
annually – Colorado (CORHIO) Service $2k + $10/user/mo. – Economic feasibility for non-affiliated LTPACs?
• CMMI Grant – Possibly the largest LTPAC, multi-state HIE
assembled to date – Sustainability questions
Brookdale Acute Interaction – HIE Challenges
38

• Analytics – Lack of data for key metrics. E.g. LTPAC hospitalization and
utilization rates – Utilization data should be available without the need for HIE
connections. • “Meaningful,” affordable HIE focused upon LTPAC’s
needs: – Order entry, e-signatures, care planning – Pharma – Labs
• Secure messaging as DIRECT alternative – As simple as texting (or faxing) – Avoid walled gardens
Unmet LTPAC Needs
39

• The regional/smaller LTPAC provider experience
• The multi-state/large LTPAC provider experience
• Summary Themes and Questions
Agenda

• There is a pressing need to connect clinicians, for example, technology has advanced to the point where dozens of secure messaging solutions are now available. So, why does it seem that true collaboration between clinicians is more elusive than ever?
• When one clinician needs to coordinate with another
clinician outside of his own organization, the EHR was very rarely used. What are some solutions to address this problem?
• What are some suggestions to bring together multiple stakeholders to build community relationships and collaboration across LTPAC and Acute care?
DISCUSSION: Questions (1 of 2)

• What role could / should HIMSS play in facilitating the care transition conversations?
• How are HIT leadership in Acute Care and LTPAC organizations incorporating accessibility of existing data into strategic plans and operations?
• Some of models forecast greater shared accountability – How can IT systems fit into that model ? – How is sharing accomplished? – How is accountability accomplished?
DISCUSSION: Questions (2 of 2)

Next LTPAC Roundtable Meeting
2:00 pm CT
May 10, 2016

Gregory L. Alexander, PhD Professor Sinclair School of Nursing University of Missouri [email protected]
John F. Derr, RPh. CEO JD & Associates Enterprises, Inc. [email protected]
Lorren Pettit, MS, MBA Vice President, Research HIMSS North America [email protected]