
Location Coronary Arterial Occlusions and Their Relation...
8
Location of Coronary Arterial Occlusions and Their Relation to the Arterial Pattern By BERTRAM PITT, M.D., PAUL M. ZOLL, M.D., HERRMAN L. BLUMGART, M.D., AND DAVID G. FREIMAN, M.D. THE INCIDENCE and localization of coronary artery occlusion have assumed increasing importance because of the current exploration of cardiac lesions in patients by angiography and surgery. We wish to report the results of a large series that extends the previous studies by Schlesinger and Zoll oia anatomic variations in coronary arterial pat- terns and on the incidence and localization of coronary arterial occlusions.1-3 Methods The injection plus dissection method of Schles- inger was employed.4 Briefly, this method con- sists of (1) injecting radiopaque lead-agar mass of different colors into the coronary arteries; (2) unrolling the heart so that the entire coronary tree lies in one plane; (3) taking a roentgenogram of the unrolled heart; and (4) carefully dissecting the coronary arteries with use of the film as a guide. This technic discloses all narrowings and occlusions, larger anastomoses, and the anatomic pattern of the coronary arterial tree. In this study angina pectoris was defined in accordance with the usual criteria, and myocardial infaretion was defined as a grossly visible sear or lesion confirmed by histologic examination. This definition, it should be stressed, does not include microscopic necrosis or grossly visible scat- tered areas of fibrosis that may be isehemic in origin. The term coronary occlusion refers to complete occlusion and does not include arterial narrowing, no matter how marked. The presence or absence of atherosclerosis was determined after dissection of the coronary arteries, and the degree of involvement was based on an estimation of the over-all extent of arterial narrowing and obstruc- tion. The extent of the atherosclerotic process was graded as absent (0), slight (+), moderate (+±), or marked (+++). The results of 1,576 necropsies in which the From the Departments of Medicine and Pathology, Harvard Medical School and the Medical Research Department, Yamins Research Laboratories, Beth Israel Hospital, Boston, Massachusetts. Aided by grants (H-4151 and HE-06316) from the United States Public Health Service. Circulation, Volume XXVIII, July 1968 hearts were injected at the Beth Israel Hospital, in an unselected and almost consecutive series from 1936 to 1949, were analyzed. This series includes the smaller group of cases previously reported by Schlesinger.1' 2 Incidence and Localization of Coronary Artery Occlusions Of the 1,576 hearts in the present study 378 were found to have coronary arterial oc- clusions; the total number of occlusions, both old and recent, was 969. This incidence is similar to the previous finding of an average of 2.5 occlusions per heart in cases with oc- clusion.5 In our present study, of all 378 hearts with complete occlusions, 62 per cent had more than one occlusion per heart (table 1), and 48 per cent of the hearts had occlusion of at least two of the three main coronary arteries. Multiple occlusions were present in one of the coronary arteries in one third of the cases (table 1). In many previous investigations the left anterior descending coronary artery was found to be the most frequent site of occlu- sion.6 Schlesinger and Zoll3 found 38 per cent of occlusions in the left anterior descending, 26 per cent in the left circumflex, and 35 per cent in the right coronary artery. Our pres- ent series of 969 occlusions, both old and recent, confirms their observations and the findings of Horne et al.7 in emphasizing the frequency of occlusion in the right coronary artery. All of the cases with complete coronary occlusions (in whieh an adequate history was available) were subdivided into those with angina pectoris, those with congestive heart failure, and those without clinical symptoms of coronary artery disease (table 2). This analysis re-emphasizes the severity of the oc- clusive process in patients with angina pee- 35 by guest on July 16, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Location Coronary Arterial Occlusions and Their Relation...
Location of Coronary Arterial Occlusions and TheirRelation to the Arterial Pattern
By BERTRAM PITT, M.D., PAUL M. ZOLL, M.D., HERRMAN L. BLUMGART, M.D.,AND DAVID G. FREIMAN, M.D.
THE INCIDENCE and localization ofcoronary artery occlusion have assumed
increasing importance because of the currentexploration of cardiac lesions in patients byangiography and surgery. We wish to reportthe results of a large series that extends theprevious studies by Schlesinger and Zoll oiaanatomic variations in coronary arterial pat-terns and on the incidence and localization ofcoronary arterial occlusions.1-3
MethodsThe injection plus dissection method of Schles-
inger was employed.4 Briefly, this method con-sists of (1) injecting radiopaque lead-agar massof different colors into the coronary arteries;(2) unrolling the heart so that the entire coronarytree lies in one plane; (3) taking a roentgenogramof the unrolled heart; and (4) carefully dissectingthe coronary arteries with use of the film as aguide. This technic discloses all narrowings andocclusions, larger anastomoses, and the anatomicpattern of the coronary arterial tree.
In this study angina pectoris was defined inaccordance with the usual criteria, and myocardialinfaretion was defined as a grossly visible searor lesion confirmed by histologic examination.This definition, it should be stressed, does notinclude microscopic necrosis or grossly visible scat-tered areas of fibrosis that may be isehemic inorigin. The term coronary occlusion refers tocomplete occlusion and does not include arterialnarrowing, no matter how marked. The presenceor absence of atherosclerosis was determined afterdissection of the coronary arteries, and the degreeof involvement was based on an estimation of theover-all extent of arterial narrowing and obstruc-tion. The extent of the atherosclerotic process wasgraded as absent (0), slight (+), moderate (+±),or marked (+++).The results of 1,576 necropsies in which the
From the Departments of Medicine and Pathology,Harvard Medical School and the Medical ResearchDepartment, Yamins Research Laboratories, BethIsrael Hospital, Boston, Massachusetts.Aided by grants (H-4151 and HE-06316) from
the United States Public Health Service.
Circulation, Volume XXVIII, July 1968
hearts were injected at the Beth Israel Hospital,in an unselected and almost consecutive seriesfrom 1936 to 1949, were analyzed. This seriesincludes the smaller group of cases previouslyreported by Schlesinger.1' 2
Incidence and Localization ofCoronary Artery Occlusions
Of the 1,576 hearts in the present study378 were found to have coronary arterial oc-clusions; the total number of occlusions, bothold and recent, was 969. This incidence issimilar to the previous finding of an averageof 2.5 occlusions per heart in cases with oc-clusion.5
In our present study, of all 378 hearts withcomplete occlusions, 62 per cent had morethan one occlusion per heart (table 1), and48 per cent of the hearts had occlusion of atleast two of the three main coronary arteries.Multiple occlusions were present in one of thecoronary arteries in one third of the cases(table 1).In many previous investigations the left
anterior descending coronary artery wasfound to be the most frequent site of occlu-sion.6 Schlesinger and Zoll3 found 38 per centof occlusions in the left anterior descending,26 per cent in the left circumflex, and 35 percent in the right coronary artery. Our pres-ent series of 969 occlusions, both old andrecent, confirms their observations and thefindings of Horne et al.7 in emphasizing thefrequency of occlusion in the right coronaryartery.
All of the cases with complete coronaryocclusions (in whieh an adequate history wasavailable) were subdivided into those withangina pectoris, those with congestive heartfailure, and those without clinical symptomsof coronary artery disease (table 2). Thisanalysis re-emphasizes the severity of the oc-clusive process in patients with angina pee-
35
by guest on July 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

PITT ET AL.
C C]C] r-,i r
Ci] C] CC
'C
Cq C], L-
toris, 60 per cent having two or more occlu-sions; conversely, there was a relatively largepercentage of patients, 30 per cent, withcoronary occlusions not having clinical mani-festations.
C]
'4 Lc0 C] ,4 C CI: CCm
in o : C CA cCy'. Cc05C(Z (, ' r-
10H O H 00 ) C1
r-- (m0 c ICAC CA r- l C]
1010 0 -it
m-C CA - Cy"
COt. Cy
. C10 CC 0)C] 0)r
- Or-H
C C;C; C
C) C
C; °~C)O Cm Q
CCCC]0O ]
000
Ca Ca Ca.' 4'. 4'C) C) eC]']'CCCH
VC
C;
o oo )0Hv*
o CO
C.-v*
Ca CC h fC
CA
C]
COC]
XCA
C]:-"
CC COC0) C]
C -4~ -
CC;
c] C) C)1
C Cd
4a . - '0t X
e 4 OC
C) CCCw
o a o~>
a 0 Ca-s ,] s- C X- C
The Coronary Arterial Pattern
Schlesinger differentiated three main varia-tions in pattern of the right and left eircum-flex coronary arteries. 2 The first and mostcommon group (48 per cent) showed rightcoronarv artery predominance" with the
right coronary artery extending beyond theposterior deseending branch and supplyingthe right ventricle, the posterior half of theinterventricular septum, and part of the leftventricle. The second group (34 per cent)was found to have a "balanced circulation"with each of the two ventricles receiving itsblood supply from the corresponding coro-nary artery: the right coronary artery extendsas far as the crux of the heart to give off the
X posterior descending braneh so that it sup--e plies the right ventricle plus the posterior
,' half of the interventricular septum, and the~ left coronary artery supplies the whole left
ventricle plus the anterior half of the inter-ventricular septum. The third pattern (18
.t2 per cent) was "left coronlary artery prepon-&v^ derant," the left coronary artery giving off
the posterior descending branch so as to sup-= ply the whole left ventricle, the entire inter-
'p<^ ventricular septum, and in some cases part ofthe right ventricle. The coronary artery pat-
I: tern is fixed throughout life and is unchangedeven with hypertrophy.8 9 The amount of
i9 blood normally supplied to anv one part of&v^ the myocardiunm is independenit of the coro-
nary artery pattern.Although there are some minor differences,
t the results in the present, larger series (table<1> 3 ) confirm the relative frequencies of theW three patterns found by Schlesinger.1 2 The° incidence of these three patterns is similar to
that noted recently by James in 106 hearts,104,W but his suggestion of a significant variation
in pattern with sex is not confirmed in our
>,< larger series.In his original small series Schlesingerl'
Circulation, Volumne XXVIII, Jutly 1963'
36
CC- m Rti- ?4Dt-r- Obq0MLO
CC CCD C] -~r~
in1D O 1 H i I !:~
-4
Q>1-cis'a4
0
CZ
CD
.0
C)CO
o
._
0
C)
EO
0a
C
M
08
C)
00
08
O00
0
el00
kCa
a)
A
Am
._m
0
Co)b
Ez
Co
I,
ca
Co
C
0b
*CCQ
0I'
cJ0z
0
0
C
0
c0
CC CA
C] C]00i L-
m
4.)0a
CC)
+
4 m
C1) C)4wCCce W
0 0
rn m
by guest on July 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
CORONARY ARTERIALI OCCL(SIONS
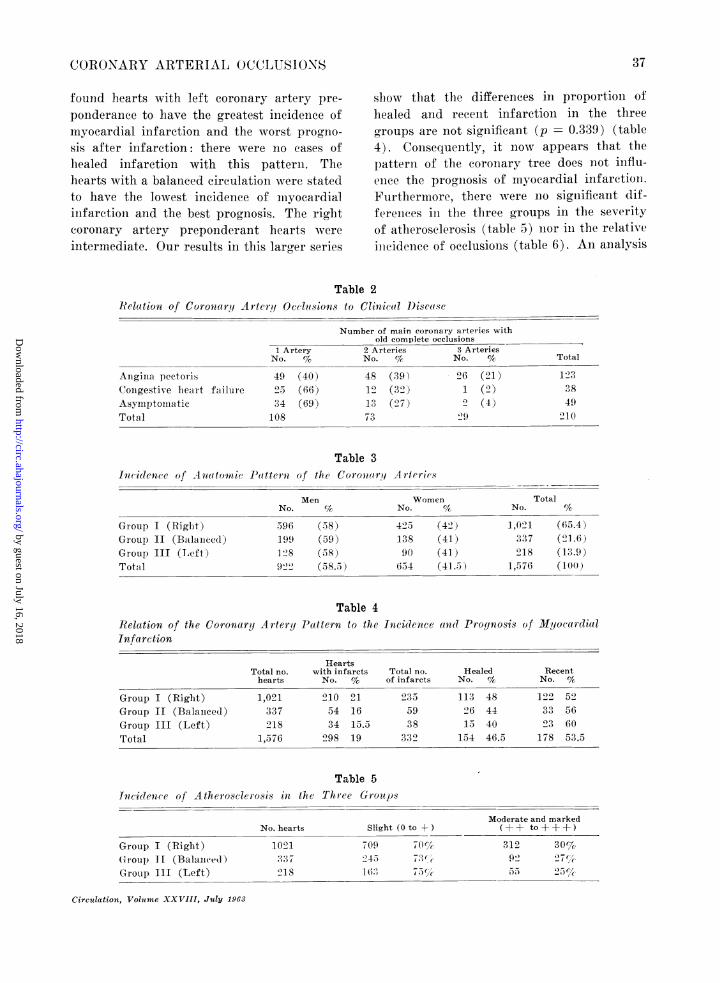
found hearts with left coronary artery pre-ponderance to have the greatest incidenee ofmyocardial infaretion and the wNvorst progno-sis after infaretion: there were no cases ofhealed infaretion with this pattern. Thehearts with a balanced circulation were statedto have the lowest incidence of niyocardialinifaretion and the best prognosis. The rightcoronary artery preponderant hearts wereintermnediate. Our results in this larger series
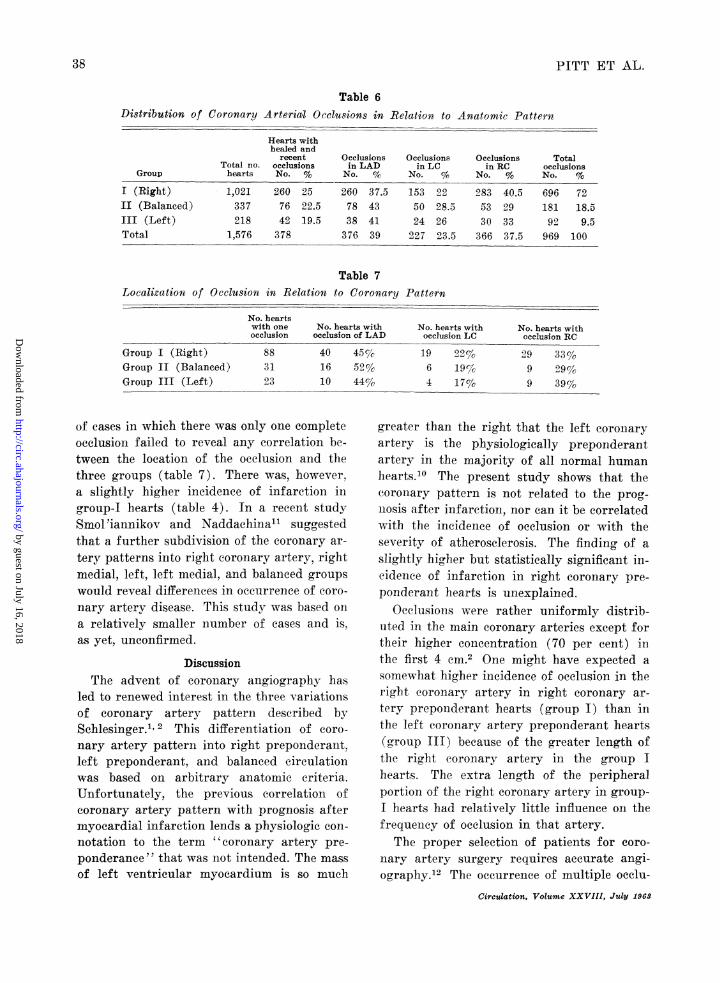
slhow that the differences in proportioni ofhealed and recenlt infaretioin in the threegfroups are not significant (p = 0.339) (table4). Consequently, it now appears that the)atterln of the coronary tree does not influ-eniee the prognosis of myocardial infaretioni.Furthermore, there were no signiificanlt dif-fereniees in the tlhree groups in the severityof atheroselerosis (table 5) nior in. the relativeillcideniee of occlusionis (table 6). Anl analysis
Table 2Relation of Corona riy A}rterq Occlusions to Clinical D)isease
Anginia pectorisCoingestive heart failur e
AsymptoinatieTotal
1 ArteryNo. %
49 (40)2>5 (66)34 (69)108
Number of main coronary arteries withold complete occlusions
2 Arteries 3 ArteriesNo. % No. %/ Total
48 (39) 96 (21) 12312 (32) 1 (2) 38
13 ('27) 2 (4) 4973 29 210
Table 3Incidence of A4-natoinic Pattern of the Corona rq A ritrics
Men WomeNo. %G No.
Group I (Right) 396 (38) 423 (Group II (Balanced) 199 (59) 138 (Group III (Left) 128 (38) 90Total 9'22 (38.5) 6.34
?n
(42')(41)(41 )(41.5)!
Relation of the Coronary A rteryInfarction
Table 4Patterin to the Incidence aind Prognosis of Myocardial
Group I (Right)Group II (Balaiieed)Group III (Left)Total
Total no.hearts
1,021337918
1,576
Heartswith infarcts
No. %
210 2154 1634 15.5
298 19
Total no.of infarcts
2355938
332
Table 5Incidence of Atherosclerosis in the Three Groups
Group I (Right)G roup) 1f (Balanced)Group III (Left)
No. hearts
1021337_218
Slight (0 to + )
7092.45'1 68;.,
_i0 /ch73 ((~7_,..
Moderate and marked(-+ + to+++)
31292)
30%77 ,
25) , c
TotalNo. %
1,021337218
1,576
(65.4)(21 .6)(13.9)(lo())
HealedNo. %
113 4826 4415 40
154 46.5
RecentNo. '4
122 5933 5603 60
178 53.5
Circulation, Voluime XXVIII, July 1963
37
by guest on July 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
PITT ET AL.
Table 6Distribution of Coronary Arterial Occlusions in Relation to Anatomic Pattern
Hearts withhealed and
recentTotal no. occlusions
Group hearts No. %
I (Right) 1,021 260 25II (Balanced) 337 76 22.5III (Left) 218 42 19.5Total 1,576 378
Occlusionsin LAD
No. %
260 37.578 4338 41376 39
Occlusionsin LC
No. %
153 2250 28.524 26227 23.5
Occlusionsin RC
No. %
283 40.553 2930 33366 37.5
TotalocclusionsNo. %o
696 72181 18.592 9.5969 100
Table 7Localization of Occlusion in Relation to Coronary Pattern
No. heartswith one No. hearts withocclusion occlusion of LAD
No. hearts with No. hearts withocclusion LC occlusion RC
Group I (Right)Group II (Balanced)Group III (Left)
of cases in which there was only one completeocclusion failed to reveal any correlation be-tween the location of the occlusion and thethree groups (table 7). There was, however,a slightly higher incidence of infarction in
group-I hearts (table 4). In a recent studySmol 'iannikov and Naddachina"l suggestedthat a further subdivision of the coronary ar-
tery patterns into right coronary artery, rightmedial, left, left medial, and balanced groupswould reveal differences in occurrence of coro-
nary artery disease. This study was based on
a relatively smaller number of cases and is.as yet, unconfirmed.
DiscussionThe advent of coronary angiography has
led to renewed interest in the three variationsof coronary artery pattern described bySchlesinger.1 2 This differentiationi of coro-
nary artery pattern into right preponderant,left preponderant, and balanced circulationwas based on arbitrary anatomic criteria.Unfortunately, the previous correlation ofcoronary artery pattern with prognosis aftermyocardial infarction lends a physiologic con-
notation to the term "coronary artery pre-
ponderance " that was not intended. The mass
of left ventricular myocardium is so mueh
greater than the right that the left coronary
artery is the physiologically preponderantartery in the majority of all normal humanhearts.10 The present study shows that thecoronary pattern is not related to the prog-
nlosis after infaretion, nor can it be correlatedwith the incidence of occlusion or with theseverity of atherosclerosis. The finding of a
slightly higher but statistically significant in-cidence of infaretion in right coronary pre-
ponderant hearts is unexplained.Occlusions were rather uniformly distrib-
uted in the main coronary arteries except fortheir higher concentration (70 per cent) inthe first 4 em.2 One might have expected a
somewhat higher incidence of occlusion in theright coronary artery in right coronary ar-
tery preponderant hearts (group I) than inthe left coronary artery preponderant hearts(group III) because of the greater length ofthe right coronary artery in the group I
hearts. The extra length of the peripheralportion of the right coronary artery in group-I hearts had relatively little influence on thefrequency of occlusion in that artery.
The proper selection of patients for coro-
nary artery surgery requires accurate angi-ography.12 The occurreniee of multiple occlu-
Circulation, Volume XXVIII, July 1963
883123
401610
45 ec52%44%o
1964
22%cc19%17%o
2999
33 %,/290,z39%
38
by guest on July 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

CORONARY ARTERIAL OCCLUSIONS
sions in a large number of cases points tocertain difficulties in the interpretation of theangiograms. Although the angiogram mayshow only one occlusion in a main vessel, fur-ther occlusions will not be detected unlessthere is recanalization or retrograde flowthrough collateral vessels. It has been sug-gested that considerable pathologic changecan be present in the coronary system withoutany abnormality appearing in the clinicalarteriogram.13' 14 Furthermore, the recogni-tion of occlusions in the smaller branches ofthe coronary tree is extremely difficult becauseof the variable distribution and number ofthese vessels.15
Studies in our laboratories have providedmuch of the pathologic and anatomic back-ground necessary for the understanding ofthe clinical manifestations of coronary dis-ease, in particular angina pectoris, and havebeen used as a basis for the consideration ofa surgical approach to coronary artery dis-ease.16 The characteristics of coronary arterialocclusions have been presented in detail3' 17and need only be summarized here. The vas-cular lesions in the coronary system are al-most entirely atherosclerotic in nature: initi-ally they are localized and segmental, but theymay extend to involve most of the vascularwalls. The atherosclerotic process may pro-duce little or no narrowing of the lumen ortotal occlusion may result; the degree of ob-struction may not be closely related to theextent of the atherosclerosis. The lesions oc-cur almost entirely in the epicardial distribu-tion of the main coronary arteries and theirprimary branches. The highest ineidence ofocclusion is not directly at the mouth of thevessel but a short distance distal to the mouth.One half are within 3 cm. and 70 per cent arewithin 4 cm. of the coronary ostia. In the 193occlusions previously studied, 64 per centwere less than 5 mm. in length and 40 percent were less than 3 mm. in length.3 Occlu-sions of the right coronary and left circum-flex coronary arteries were almost as frequentas of the left anterior descending branch ofthe left coronary artery.3 Interarterial coro-Circulation, Volume XXVIII, July 1968
nary anastomoses were markedly increasedwith coronary artery disease.18-20Our present data on coronary artery occlu-
sions indicate the extremely limited role en-darterectomy may be expected to play in thetherapy of angina pectoris. These data do notinclude coronary artery narrowing, whichoften causes significant reduction in coronaryflow and may affect the myocardium evenmore than do occlusions. Involvement of thecoronary arteries with the atheroscleroticprocess may prevent surgical manipulation ofthe walls even in the absence of obstruction.The data on length of occlusion and distanceof occlusion from the ostia, which had beenused as a pathologic basis for endarterectomy,were obtained from an unselected group ofpostmortem cases with complete coronary oc-clusion.16 The present study reveals thatabout one half of the cases did not have an-gina pectoris or myocardial infaretion, thatin 30 per cent of the cases the occlusions wereasymptomatic during life, and that 20 percent of the cases had congestive heart failureonly (table 2). Because the severity of theocclusive process in these patients is signifi-cantly less than in patients with angina pee-toris, the earlier estimates of the applicabilityof endarterectomy for the therapy of anginapectoris should be revised downward. Oncecoronary artery disease becomes manifest asangina, the occlusive process is in most casestoo widespread for surgical intervention. Thepatients with complete occlusions who wereasyniptomatic or who have onily congestiveheart failure, appear to be the ones in whichwe would expect the greatest technical successwith endarterectomy. As the natural historyof these patients is not, as yet, adequatelyknown and the surgical mortality is high,21it seems unwarranted to operate on such pa-tients even if they could be detected. Untilsuch a time as the operative mortality andsecondary failure rate, due to restenosis,22 canbe reduced through new surgical technics,coronary endarterectomy should be consid-ered an experimental procedure to be inves-tigated vigorously in the laboratory, but not
39
by guest on July 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
PITT ET AL.
to be applied for therapeutic purposes in miiani.These conielusions are in agreemnenit wvith therecent findings of Swedlund et al.23The objection might be raised that our
studies were based on postmortenr data rep-resenting the end stage of the disease process,and that the extent of the obstructive coro-nary disease would be much less during life.Since the old occlusions found at autopsy ex-isted prior to the patient's terminal illness,and since many of our patients died of extra-cardiac disease, the postmortem data do seenito provide a fair representation of the patlhol-ogy present for somne time during life. InThal's clinical study of 50 patients with cor-onary angiography there were onily two in-stances in which the obstructions were local-ized or segmental.24 Both of these patienitswere asymptomatic. Direct observation of thecoronary arteries during endarterectoimv'vhas also demonstrated extensive involvementof the coronary inain sterns by occ-lusive dis-ease duringo, life and suggests that this 01)3cc-tion may be discounlted.
SummaryThe present study shows that the coronary-
artery pattern is not related to the prognosisafter infaretion nor can it be correlated withthe incidence of occlusion or with the severityof atherosclerosis. This analysis re-emphasizesthe severity of the occlusive process in patienitswith angina pectoris and, coniversely, the rela-tively large percenitage of patients havingeoronlary occlusion who had either congestiveheart failure or who were asymptoimatie.The proper selection of patients for coro-
nary artery surgery requires accurate angiog-raphy. The oceurrence of multiple occlusionsin a large number of cases points to certaindifficulties in the interpretation of the coro-nary angiogram anid also indicates the ex-tremely limited role endarterectomy may beexpected to play in the therapy of anginapectoris. Until such a tinme as the operativemortality and secondary failure rate, due torestenosis, can be reduced through new surgi-cal technies, coronary endarterectomy shouldbe considered an experimental procedure to
be investigated v-ig(orously ii the laboratorvbut nlot to be applied for thfierapeutic purposesin man.
References1. SCHLESINGER, MS. J.: Relatioin of the anatomic
pattern to pathologic coiiditioiis of the coronary arteries. Arch. Path. 30: 403, 1940.
2. SCHLESINGER, M. J.: Significant variations inthe anatomic patterni of the coroniary vessels.Am. A. Advaneement Sc. 13: 61, 1940.
3. SCHLESINGER, M. J., AND ZOLL, P. M.: Incidenceand localization of coronary artery occlusions.Arch. Path. 32: 178, 1941.
4. SCHLESINGER, Mi. J.: An injection plus dissectionsttldy of coronlary occlusioiis and anastonToses.Am. Heart J. 15: 528, 1938.
5. BLUlMfGART, H. L., SCHLESINGER, M. J., AND ZOLL,P. M.: Anigina pectoris, coronary failure a.ndmyocardial infaretions. J.A.M.A. 116: 91, 1941.
6. FRoMAENT, R.: ProblWnmes soulevees par la chlirur-gie coronarienne directe. Schweiz. me(l. Wcbn-schllr. 90: 743, 1960.
7. HORN, IIT., AND FINKELSTEIN, L. E.: Arterio-selerosis of the coroinary arteries aand themechanisnms of their occlusion. Am. Heart J.19: 653, 1940.
8. MULLER-MOHNSSEN, H.: Die Koroinarskeleroseim post mortalen Arteriogram. Fortsch. Geb.RWntgenstrahlen und nuklear Med. 86: 539,1957.
9. SCHOENMACHERS, J., AND VIETEN, H.: Post-mortale Angiogramme der Koronararterien beiangeborene und erworbenen Herzfehlern. Deut-sehe med. Wchnschr. 79: 671, 1954.
10. JA'MES, T. N.: Anatomy of the Coronary Arteries.New York, Paul B. Hoeber IncG., 1961.
11. SMOL 'IANNIKOV, V., AND NADDACHINA, T. A.:Blood supply system of the heart. Arkivanatom-1. gistol. i embriol. 38: 117, 1960.
12. LORD, J. W.: Surgery for coroImary artery dis-ease. Surg., Gynec. & Obst. 110: 746, 1960.
1]3. LEHMAN, J. S.: Coronary arteriography: Prac-tical considerations. Progr. Cardiovas. Dis. 2:36, 1959.
14. EuSTERMAIN, J. H., ACHOR, R. W. P., KINCAID,0. W., AND BROWN, A. L., JR.: Atheroscleroticdisease of the coronary arteries. A pathologic-radiologic correlative study. Circulation 26:1288, 1962.
13. TAPIA, F. A., BOLTON, H. E., AND MAZEL, M. S.:Selective coronary einearteriography. Angiology12: 46, 1961.
16. BLUMGWART, H. L., ZOLL, P. M., AND KURLAND,G. S.: Discussion of direct relief of coronaryocclusion. Arch. Int. Med. 104: 862, 1959.
1 7. ZOLL, P. M., WESSLER, S., AND SCHLESINGER,Al. .1.: Interarterial coronary anastoinoses in
(Orcn7ation, Volu.m XXVII, J7ty 1G9.'
40
by guest on July 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

CORONARY ARTERIAL OCCLUSIONS
the human heart, with particular reference toanemia and relative cardiac anoxia. Circulation4: 797, 1951.
18. BLUMGART, H. L.: Editorial: Anatomy and func-tional importance of intereoronary arterialanastomoses. Circulation 20: 812, 1959.
19. PITT, 13.: Interarterial coronary anastomoses. Oc-currence in normal hearts and in certainpathologic conditions. Circulation 20: 816, 1959.
20. SPAIN, D. M., BRADESS, V. A., IRAL, P., ANDCauz, A.: Intercoronary anastomotic channelsanid suddeni uniexpected dleath froimi advaneedcoronary atherosclerosis. Circulation 27: 12,1963.
21. LoNG-AIalE, W. P., CANNON, J. A., AND KATTUS,A. A.: The surgical therapy of aniginia pee-toris. Arch. Int. Med. 104: 886, 1959.
22. CRAWFORD, C.: Some aspects of surgery forcoronlary artery disease. Surgery 49: 215, 1961.
23. SWEDLUND, H. A., ACHOR, IR. W. P., AND
EDWARDS, J. E.: A clinicopathologic study on
the feasibility of direct surgical treatment ofocclusive coronary arterial disease. Circulation25: 292, 1962.
24. THAL, A. P., RICHARDS, L. S., AND GREENSPAN,R.: Alrteriographic studies of the coironiaryarteries in ischemic heart disease. J.A.M.A.168: 2104, 1958.
Inertia vs New IdeasApart from the happy few whose work has already great prestige or lies in fields that
are being actively expanded at the nmonment, discoverers of new truths always find theirideas resisted. The consideration of this process is often obscured by two assumptions:first it is supposed that the most harmful resistance comnes from obvious and noisy preju-
dice and that the more dangerous resistance of inertia and quasi-rational negation isunimportant; and secondly, it is supposed that workers in science are of course free fronmany resistive tendency but a rational conservatism. Each of these assumptions is an almiostcomplete delusion.The vociferous opposition met with by the ideas of Charles Darwin and of Lister
probably did nothing to hinder the spread of these, and probably brought them withinireach of a larger number of people capable of acceptingi them than would have been theease if the opposition had been well behaved. Again it was not noisy prejudice thatcaused the work of Mendel to lie dead for thirty years, but the sheer inability of con-
temiiporary opinion to distinguish between a new idea and nonsense. That his same inabil-ity may be shown even by the most eminent workers in science scarcely needs demonstra-tion for anyone at all aware of the history of knowledge, but it may be illustrated by an
anecdote which we owe to the third Lord Rayleigh and which is to be found in thedelightful Life of that very great and wise man. J. J. Waterston was an engineer whointerested himself in mathematical physics, and in 1845 wrote a paper on the nloleculartheory of gases which was ten or fifteen years in advance of his time and anticipatedmuch of the work of physicists no less eminent than Joule, Clausius, and even ClerkMaxwell. The only contemporary judgement on this paper that survives is that of thereferee of the Royal Society to whom it was submitted. He said, 'The paper is nothingbut nonsense.' What Waterston might have accomplished if he had had the recognitionand encouragement upon which this genius seems to have been unusually dependent, isbeyond conjecture. He did not get theim. His work lay in utter oblivion for forty-fiveyears until it was exhumed by the pious efforts of Rayleigh. He himself lived on disap-pointed and obscure for nmany years, and then was overtaken by a Yet deeper obscurity,for as the result of sonie strange accident or a long gathering impulse of despair, he
disappeared and left no sign.-The Collected Papers of Wilfred Trotter, F.R.S. London,Oxford University Press, 1946, p. 26.
Circulation, Volume XXVIII, July 1963
41
by guest on July 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
FREIMANBERTRAM PITT, PAUL M. ZOLL, HERRMAN L. BLUMGART and DAVID G.
PatternLocation of Coronary Arterial Occlusions and Their Relation to the Arterial
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1963 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.28.1.35
1963;28:35-41Circulation.
http://circ.ahajournals.org/content/28/1/35located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 16, 2018http://circ.ahajournals.org/
Dow
nloaded from


















