Measurement of Coronary Blood Flow by External …circ.ahajournals.org/content/33/5/708.full.pdf ·...
12
Measurement of Coronary Blood Flow by External Counting with Radioactive Rubidium Critical Appraisal and Validation of the Method By L. DONATO, M.D., G. BARTOLOMEI, M.D., G. FEDERIGHI, M.D., AND G. TORREGGIANI, M.D. T HE MYOCARDIAL clearance of potas- sium (MCK) can be measured by means of precordial counting after single intravenous injection of 42KC1 or 86RbCl.1 It may be considered to measure coronary blood flow per unit mass of myocardium under the as- sumption that the average extraction of the indicator by the myocardium during the first minutes after injection does not differ signifi- cantly from the average total body extraction. Theoretical considerations and experimental evidence suggest that these conditions actual- ly occur in rats, dogs, and humans." 2 When a precordial counter is used to mea- sure myocardial radioactivity, the obtained value for MCK represents the mean flow per unit mass, and it is conventionally expressed per 100 g of myocardium.1 Absolute flow cannot be determined with a precordial count- er since individual variability in depth and size of the heart prevents an absolute estimate of myocardial uptake of the radioisotope. If the geometric dependence of the measurement could be overcome, coronary blood flow could be estimated as a fraction of cardiac output or in absolute terms. In fact, under conditions of uniform counting efficiency for the entire heart, the fraction of injectate taken up by the myocardium shortly after injection of 86Rb or 42K would equal the fraction of the cardiac output perfusing the myocardium.1 2 The present series of experiments has been designed with the following purposes: (1) From the Medical Clinic and the Center of Nuclear Medicine of the University of Pisa. This work was carried out under the Association Contract Euratom-University of Pisa-U.L.B.-026- 63-4-BIAC. 708 to verify the validity of the assumptions un- derlying the method using 86Rb; (2) to compare t-he results obtained with the pre- cordial counting method with the values of coronary blood flow simultaneously measured with the nitrous oxide method; and (3) to evaluate a counting apparatus designed to reduce the dependence on geometry of the values obtained by counting. Methods Measurement of CBF by 86RbC1 Injection Instruments and Operating Conditions The instrument used for monitoring intracardiac and myocardial radioactivity is shown in figure 1. It is a twin counter system (TCS*),,3 comprising two Nal scintillation counters (3 by 3 inches), the combined output of which is fed to an amplifier and single-channel pulse-height analyzer. The high voltage supply to the two phototubes is adjusted in order to obtain superposable y- spectra from the two detectors. Pulses from the analyzer are fed to a scaler and a linear ratemeter, operating in parallel, and the output of the rate- meter is fed to a DC amplifier of an oscilloscopic recorder. The scintillation detectors are housed in lead collimators, with cylindrical collimating channels. The crystals are recessed 40 cm in the collimators, and the diameter of the collimating channels can be adjusted from 7.5 to 9 cm. The two collimators are mounted on a movable stand arranged so that the two crystals face each other on the same vertical axis. The lower detector can be positioned under the catheterization table and the distance of the upper detector can be adjusted. This arrangement yields a rather uniform distribution *This instrument was developed as part of the work performed under the sponsorship of the U. S. Atomic Energy Commission, Contract AT( 30-1)- 2648. Circulation, Volume XXXIII, May 1966 by guest on June 2, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Measurement of Coronary Blood Flow by External …circ.ahajournals.org/content/33/5/708.full.pdf ·...

Measurement of Coronary Blood Flow byExternal Counting with Radioactive
RubidiumCritical Appraisal and Validation of the Method
By L. DONATO, M.D., G. BARTOLOMEI, M.D., G. FEDERIGHI, M.D.,AND G. TORREGGIANI, M.D.
T HE MYOCARDIAL clearance of potas-sium (MCK) can be measured by means
of precordial counting after single intravenousinjection of 42KC1 or 86RbCl.1 It may beconsidered to measure coronary blood flowper unit mass of myocardium under the as-sumption that the average extraction of theindicator by the myocardium during the firstminutes after injection does not differ signifi-cantly from the average total body extraction.Theoretical considerations and experimentalevidence suggest that these conditions actual-ly occur in rats, dogs, and humans." 2When a precordial counter is used to mea-
sure myocardial radioactivity, the obtainedvalue for MCK represents the mean flow perunit mass, and it is conventionally expressedper 100 g of myocardium.1 Absolute flowcannot be determined with a precordial count-er since individual variability in depth andsize of the heart prevents an absolute estimateof myocardial uptake of the radioisotope. Ifthe geometric dependence of the measurementcould be overcome, coronary blood flowcould be estimated as a fraction of cardiacoutput or in absolute terms. In fact, underconditions of uniform counting efficiency forthe entire heart, the fraction of injectate takenup by the myocardium shortly after injectionof 86Rb or 42K would equal the fraction of thecardiac output perfusing the myocardium.1 2The present series of experiments has been
designed with the following purposes: (1)
From the Medical Clinic and the Center of NuclearMedicine of the University of Pisa.
This work was carried out under the AssociationContract Euratom-University of Pisa-U.L.B.-026-63-4-BIAC.
708
to verify the validity of the assumptions un-derlying the method using 86Rb; (2) tocompare t-he results obtained with the pre-cordial counting method with the values ofcoronary blood flow simultaneously measuredwith the nitrous oxide method; and (3) toevaluate a counting apparatus designed toreduce the dependence on geometry of thevalues obtained by counting.
MethodsMeasurement of CBF by 86RbC1 InjectionInstruments and Operating ConditionsThe instrument used for monitoring intracardiac
and myocardial radioactivity is shown in figure1. It is a twin counter system (TCS*),,3 comprisingtwo Nal scintillation counters (3 by 3 inches),the combined output of which is fed to anamplifier and single-channel pulse-height analyzer.The high voltage supply to the two phototubesis adjusted in order to obtain superposable y-spectra from the two detectors. Pulses from theanalyzer are fed to a scaler and a linear ratemeter,operating in parallel, and the output of the rate-meter is fed to a DC amplifier of an oscilloscopicrecorder.The scintillation detectors are housed in lead
collimators, with cylindrical collimating channels.The crystals are recessed 40 cm in the collimators,and the diameter of the collimating channels canbe adjusted from 7.5 to 9 cm. The two collimatorsare mounted on a movable stand arranged sothat the two crystals face each other on the samevertical axis. The lower detector can be positionedunder the catheterization table and the distanceof the upper detector can be adjusted. Thisarrangement yields a rather uniform distribution
*This instrument was developed as part of thework performed under the sponsorship of the U. S.Atomic Energy Commission, Contract AT( 30-1)-2648.
Circulation, Volume XXXIII, May 1966
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
MEASUREMENT OF CORONARY BLOOD FLOW
Figure 1
The twin counter system (TCS) is shown with thePerspex block in position for calibration of the invivo measurement (see text).
of counting efficiency within a cylinder definedby the collimating channels. A detailed discussionof this point is given in the appendix, and itincludes the procedure for calibration.
Experimental ProcedureThe procedure on the patients is essentially
the same as that previously described for pre-cordial counting.' The anteroposterior diameterof the chest at precordial level is measured atthe beginning of each study, and the heartsilhouette is outlined at fluoroscopy. The TCS isthen moved over the heart area, and the distanceof the upper counter is adjusted to provide a30-cm interspace between the ends of the twocollimators. As a result, for a chest with ananteroposterior diameter of 20 cm, the two crystalsare at the same distance from an ideal planeseparating the anterior one third from the posteriortwo thirds of the chest, assumed to be thecentral plane for the heart. 1311 as RIHSA (radio-iodinated human serum albumin) and 86RbClare successively injected to measure the intra-vascular and the intravascular +myocardial pre-cordial radioactivity. The injections are made intothe superior vena cava through a polyethylenetube having a total capacity of 0.25 ml, threadedinto the median vein through a needle. From areservoir syringe, 0.2 ml of solution of 86RbCl
Myocardial concentrationArea of primary arterial concentration curve
or 131IHSA are transferred into the polyethylenetube, and its proximal end is clamped. Injectionsare made by flushing the tube with 0.5 ml ofsaline. This procedure has been found satisfactoryfor recording radiocardiographic curves.
In some cases, activity equal to that of theinjectate was introduced into a 250-ml sphericcontainer enclosed in a Perspex block that was
equal in thickness to the anteroposterior diameterof the patient's chest. The counting on the phan-tom was then carried out with the TCS set up
as for counting over the patient (fig. 1).
CalculationsCoronary blood flow per 100 g of myocardium
was calculated from MCK, as previously de-scribed.' The successive steps of the calculationsare as follows.
1. The amount of 86Rb extracted by the myo-
cardium in the first 30 seconds after single injec-tion is estimated by subtracting from the precor-
dial counting rate between 30 and 90 seconds thecontribution due to intravascular radioactivity. Thelatter is determined from the precordial countingrate between 30 and 90 seconds after injectionof 131IHSA, and the corresponding concentrationsof 86Rb and 131IHSA in arterial blood. Thegeometrical efficiency factors, required to make131IHSA measurements comparable with 86Rbmeasurements, are calculated for each case takinginto account the anteroposterior diameter of thechest, as shown in the appendix.The values thus obtained for myocardial 86Rb
content equal the product of average myocardialconcentration times the effective volume of themyocardium (volume of myocardium times aver-
age counting efficiency for it).2. The area under the 86Rb radiocardiographic
curve (RCG) is measured after extrapolationbeyond apparent recirculation. This area equalsthe integral of the primaly arterial concentrationcurve times the effective volume4 of the heartchambers including any other vessel contributingto the curve (volume of chambers times averagecounting efficiency for them).
3. Since the effective volumes of myocardiumand the heart chambers differ very little fromeach other' (see also appendix), the ratio ofmyocardial 86Rb content to area of 86Rb-RCGequals the ratio of myocardial 86Rb concentrationto the area of primary arterial concentration curve.
4. Equating volume to mass units for the myo-cardium, the above ratio gives flow in millilitersper gram of myocardium. In fact, dimensionally,
Counts/g of myocardium-Counts/ml of blood x Duration of curve
= ml of blood/ g of myocardium/min
Circulation, Volume XXXIII, May 1966
709
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
DONATO ET AL.
which multiplied by 100 gives flow in ml/ 100 g/min.
Coronary blood flow as a fraction of cardiacoutput (CBFr) was obtained by dividing theexternal counting rate due to myocardial activityinto the injectate activity measured on the phan-tom.
Body versus Coronary ExtractionA Goodale Lubin catheter was inserted into
the coronary sinus, and a no. 7 Cournand catheterinto the right ventricle. The proximal ends of thetwo catheters and the indwelling brachial arteryneedle were connected to three syringes mountedon a slightly modified Harvard pump. Injectionof the 86RbCl was made into the right branchof the pulmonary artery through a no. 5 Cournandcatheter to avoid contamination of the right ven-tricular blood with primary circulating radio-activity. The connecting tube between the arterialneedle and the pump was led through a shieldedNal scintillation counter with a hole drilled init, and the output of the counter was fed to aratemeter and recorder. Sampling was started 5seconds before injection and continued for 90seconds afterward.Calcutlations. The average radioactivity concen-tration in each syringe was equal to
F x(t) dtx
Ft Ft (1)where X and x are respectively the total activityand the mean radioactive concentration in thesyringe, F is the rate of withdrawal and t theduration of sampling.The integral represents the area of the concen-
tration curve from beginning to end of sampling.Multiplication of x by t yields this area.
In the record, the primary arterial concentrationcurve was completed by extrapolation beyondapparent recirculation; its area was then calculatedand subtracted from the total area from beginningto end of sampling.
Comparison of the Nitrous Oxide Methodwith MCK
Coronary blood flow was measured by thenitrous oxide saturation method as modified forthe coronary circulation.5 The coronary sinus wascannulated with a Goodale-Lubin catheter. MCKwas measured with the usual technique immedi-ately before and after the measurement of coro-nary blood flow with nitrous oxide.
Studies PerformedSixty-three patienits were studied: 43 were
young subjects with noimal cardiovascular systems;13 had hypertensive heart disease (HHD) andseven had ischemic heart disease (IHD) withoutarterial hypertension. The diagnosis had beenestablished on the basis of clinical and electro-cardiographic data.
In all cases MCK was measured under basalconditions. In 12 cases (nine normal subjects andthree with IHD), a second measurement wasperformed under the same conditions, from 10to 20 min after the first one.
In 18 cases (11 normal subjects and seven withHHD), the injectate activity was measured asindicated above for the evalution of fractionalCBF, which was then calculated.
In 11 cases (eight normal subjects and threewith IHD) N20 measurement of coronary bloodflow was performed: in 10 cases between twoMCK measurements; in one case, after a singleMCK measurement. Finally, in two additionalcases the average body extraction was comparedwith the myocardial extraction.
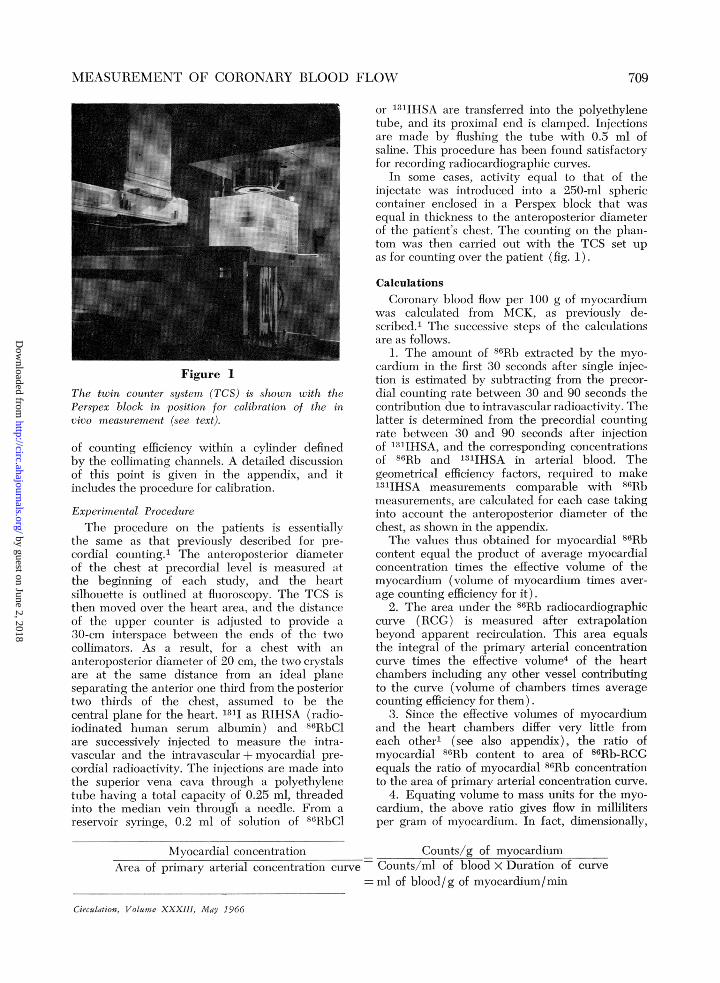
ResultsCoronary Blood Flow Values by the MCK MethodBasal values for MCK averaged 80.3 + 18.5
(SD) ml/min/100 g of myocardium in thenormal group, 56.8 ± 7.0 (SD) ml/min/100g of myocardium in the HHD group, 46.8 + 4.9(SD) ml/min/100 g of myocardium in theIHD group. The average values for bothHHD and IHD groups differ significantlyfrom the mean normal value (P < 0.001). Thedistribution of the results obtained is shownin the histograms of figure 2.
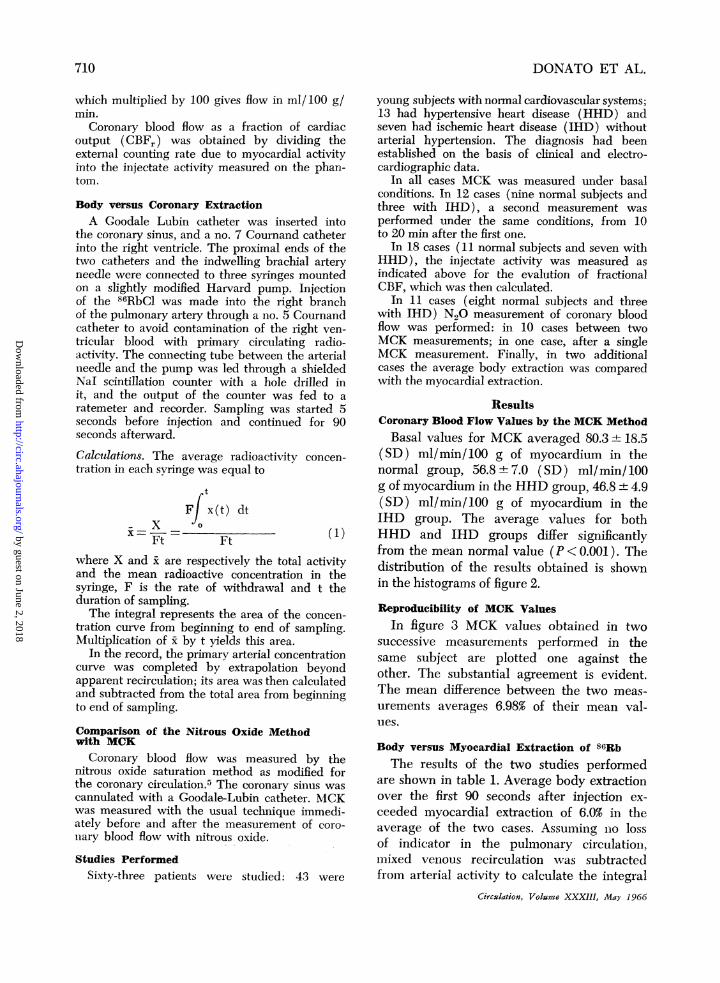
Reproducibility of MCK ValuesIn figure 3 MCK values obtained in two
successive measurements performed in thesame subject are plotted one against theother. The substantial agreement is evident.The mean difference between the two meas-urements averages 6.98% of their mean val-ues.
Body versus Myocardial Extraction of 86RbThe results of the two studies performed
are shown in table 1. Average body extractionover the first 90 seconds after injection ex-ceeded myocardial extraction of 6.0% in theaverage of the two cases. Assuming no lossof indicator in the pulmonary circulationi,mixed venious recirculation was subtractedfrom arterial activity to calculate the integral
Circulation, Volume XXXIII, May 1966
710
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
MEASUREMENT OF CORONARY BLOOD FLOW
CARDIOVASCULAR NORMALS
Om20 40 60 80 100 120 140
'HYPERTENSIVE HEART DISEASE
-1- -I -1
I I i 1§Q20 40 60 80 100 120 140
ISCHAEMIC HEART DISEASE
Qm20 40 60 80 100 io 140
ml /min/100 g
Figure 2Distribution of values of coronary flow per 100 g ofmyocardium (Qm) as measured from MCK. Continu-ous line represents the Gaussian distribution for nor-mal subjects calculated from observed mean valueand standard deviation.
of the primary arterial circulation. When cal-culated in this way, recirculating activityduring the first 90 seconds after injection was34.5% of total arterial activity during the en-tire period in both cases.
This figure compares well with the valueof 31% obtained in one case by direct mea-surement of the primary arterial circulationfrom the recorded curve, thus confirming thenegligible loss of indicator in the pulmonarycirculation within the time of observation.
Comparison with the N20 Saturation Method
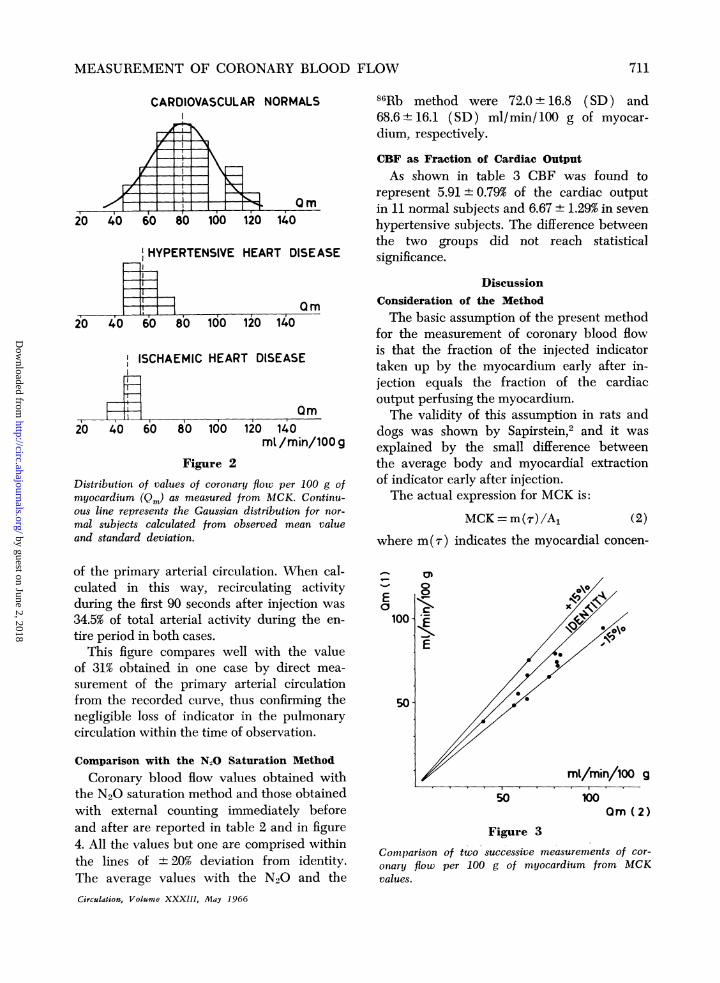
Coronary blood flow values obtained withthe N20 saturation method and those obtainedwith external counting immediately beforeand after are reported in table 2 and in figure4. All the values but one are comprised withinthe lines of ± 20% deviation from identity.The average values with the N20 and theCirculation, Volume XXXIII, May 1 9G6
86Rb method were 72.0 + 16.8 (SD) and68.6 ± 16.1 (SD) ml/min/ 100 g of myocar-dium, respectively.
CBF as Fraction of Cardiac Output
As shown in table 3 CBF was found torepresent 5.91+±0.79% of the cardiac outputin 11 normal subjects and 6.67 + 1.29% in sevenhypertensive subjects. The difference betweenthe two groups did not reach statisticalsignificance.
DiscussionConsideration of the Method
The basic assumption of the present methodfor the measurement of coronary blood flowis that the fraction of the injected indicatortaken up by the myocardium early after in-jection equals the fraction of the cardiacoutput perfusing the myocardium.The validity of this assumption in rats and
dogs was shown by Sapirstein,2 and it wasexplained by the small difference betweenthe average body and myocardial extractionof indicator early after injection.The actual expression for MCK is:
MCK = m(r)/A1 (2)
where m(zr) indicates the myocardial concen-
'-
Ea
100 -
50-
0
EE"Io~c
E
mI/min/100 g
50 100Om (2)
Figure 3
Comparison of two successive measurements of cor-onary flow per 100 g of myocardium from MCKvalues.
XII~~~~~~~~~~~~~ -L
. .
711
III
IIIIII.I
I I
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
DONATO ET AL.
Table 1
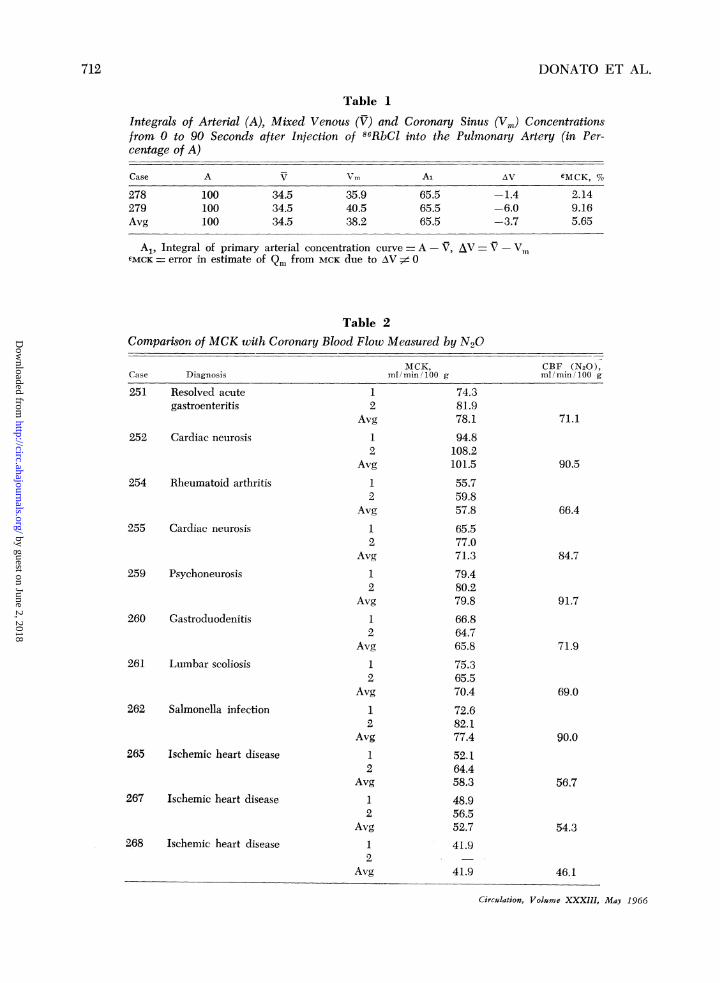
Integrals of Arterial (A), Mixed Venous (V) and Coronary Sinus (Vm) Concentrationsfrom 0 to 90 Seconds after Injection of 86RbCl into the Pulmonary Artery (in Per-centage of A)
Case A V Al AV 5MCK, %
278 100 34.5 35.9 65.5 -1.4 2.14279 100 34.5 40.5 65.5 -6.0 9.16Avg 100 34.5 38.2 65.5 -3.7 5.65
A1, Integral of primary arterial concentration curve = A - V, AV V-,,EMCK error in estimate of Qm from MCK due to AV ;z$ 0
Table 2Comparison of MCK with Coronary Blood Flow Measured by N20
MCK, CBF (N20),Case Diagnosis mlI min/100 g ml/ min 100 g
251 Resolved acute 1 74.3gastroenteritis 2 81.9
Avg 78.1 71.1252 Cardiac neurosis 1 94.8
2 108.2Avg 101.5 90.5
254 Rheumatoid arthritis 1 55.72 59.8
Avg 57.8 66.4255 Cardiac neurosis 1 65.5
2 77.0Avg 71.3 84.7
259 Psychoneurosis 1 79.42 80.2
Avg 79.8 91.7260 Gastroduodenitis 1 66.8
2 64.7Avg 65.8 71.9
261 Lumbar scoliosis 1 75.32 65.5
Avg 70.4 69.0262 Salmonella infection 1 72.6
2 82.1Avg 77.4 90.0
265 Ischemic heart disease 1 52.164.4
Avg 58.3 56.7267 Ischemic heart disease 1 48.9
2 56.5Avg 52.7 54.3
268 Ischemic heart disease 1 41.92
Avg 41.9 46.1
Circulation, Volume XXXIII,
712
May 1966
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

MEASUREMENT OF CORONARY BLOOD FLOW
tration of the indicator at the time of measure- the expression for coronary blood flow per
ment, and A, the integral of the primary ar- unit mass of myocardium is:
terial concentration curve. On the other hand,m (T) (3)
ol ~~~~~~~~Al+(V -Vm)0
150 ° where V and Vm are the concentration inte-grals for the mixed venous and coronary sinus
E recirculation, respectively.' From equations2 and 3 it is evident that MCK equals Qm pro-
E A vided (V-Vm) = 0. It is easy to show that100- -, differences between V and Vrn will be re-
% , /., / flected in erroneous estimates of Qm from^ /*/* / MCK in the following way:
Go /, vMCK = AV/Al (4)
50 // where AV -Vm.The average error in estimate of Qm from
this difference in the two cases examined
II CBF (N2 0]m/mi /1009 amounts to -5.65%. To cause a 10% error, thecoronary integral would need to exceed t-he
50 100 150 mixed venous integral of about 20%. It seems
Figure 4 unlikely, therefore, that this source of error
Comparison of coronary blood flow (CBF) as mea- may be of relevant importance.
sured from MCK (86Rb) and the N20 method. The second set of assumptions deals withTable 3
Fractional Coronary Blood Flow Versus Flow per 100 g of Myocardium as Measuredfrom MCK
CBFr,
MCK, of cardiacCase Diagnosis ml/min/ 100 g output
219 Cardiac neurosis 90.8 6.1220 Psychoneurosis 69.0 5.6221 Chickenpox 109.6 4.2222 Resolving thrombophlebitis 87.5 6.3223 Cervico-arthrosis 68.1 5.3228 Irritable colon 105.1 6.0229 Resolving bronchitis 109.4 5.4230 Pleurisy 80.9 6.7231 Psychoneurosis 65.9 6.4232 Hysteria 56.5 6.1235 Psychoneurosis 80.6 6.9
imn 83.9 5.91SD -+18.7 _±0.79
224 Renal hypertension 48.2 5.3225 Renal hypertension 70.0 7.8226 Renal hypertension 50.3 4.8227 Essential hypertension 58.1 6.0233 Renal hypertension 54.1 7.3236 Essential hypertension 61.8 7.9237 Essential hypertension 57.6 7.6
On ~~~~~~~57.1 6.67SD - 7.6 -+- 1.29
Circulation, Volume XXXIII, May 1966
713
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

DONATO ET AL.
the feasibility of using external counting toestimate the myocardial content of indicator.In the case of the measurement of MCK therelevant assumption is that the "effeCtivevolume" contributing counts from the heartcavities and vessels is the same as the "effec-tive volume" contributing counts from themyocardium.1 It has been shown that thedifference is contained within narrow limitseven for relatively large volumes in case ofprecordial counting: the conditions are im-proved further with the TCS which has amuch greater uniformity of counting efficiency.
In the case of fractional CBF the relevantassumption is that of the adequacy of simulat-ing self-absorption and scattering of radiationwithin the chest of the patients by countingon Perspex phantoms. Model experiments re-ported in the appendix suggest that the ex-ternal counting rate is essentially unaffectedby variations in heart size and depth, at leastwithin the range of interest.These elements, derived from physical con-
siderations and phantom studies, are presentlythe only ones in support of the latterassumption. However, the significance of theresults obtained is an indirect supportingargument that will be examined in the nextparagraph.
Considerations of the ResultsCBF values per gram of myocardium in
normal subjects agree well with previousestimates with the indirect Fick method6 v 8
and with our previous series with precordialdetectors.1 The results obtained in the isehe-mic group agree with the expectancy on thebasis of clinical and ECG findings. Data inthe hypertensive group also show a significantreduction of CBF per unit heart mass. Thislatter finding is in agreement with postmortemperfusion studies in hypertrophied hearts,9and with current knowledge concerning x'as-cularization of hypertrophied myocardium.On the other hand, previous studies withN20"'01I have failed to demonstrate reductioniof flow per gram of myocardium in hyper-tenisive cases. As Gregg and Fisher poinitedout, however, limitations inherent in the in-
direct Fick method as applied to CBF mayaccount for the results in cardiac hypertro-phy. 12, 13The reproducibility of the measurements
appears quite satisfactory in the series ex-amined: it will be noted that the secondestimates tend systematically to exceed slight-ly the first one. No satisfactory explanation ispresently available for such tendency.
Comparisons with N20 values, measuredduring the same study, also seem to be highlysatisfactory. The agreement was excellent overthe entire range of values explored, from 40to 110 ml/min/ 100 g myocardium.
Fractional CBF values may be comparedonly with similar estimates in rats and dogsby Sapirstein.2 CBF in man has been admittedto vary between 5 and 10% of the cardiacoutput,13 and this is in agreement with theresults of some attempts to use the dilutionprinciple to measure CBF.14The average values obtained in the groups
examined are within this range, but this state-ment is obviously of limited value. At themoment, no elements are available to validatethe significance of our estimates of fractionalCBF, but it is nevertheless of some import-ance that the values be distributed withinthe range of expectancy.
It should be pointed out that CBF inabsolute value and the mass of the heartcould be derived from fractional CBF andMCK provided cardiac output is measuredat the same time.
Advantages and Disadvantages of the MethodDuring the last few years a large number
of new methods or variants have been pro-posed for the measurement of coronary bloodflow. This probably reflects the inadequacyof currently available methods to meet therequirements for CBF measurement in man.
Precordial measures of myocardial uptakeduring intravenous infusion of 86Rb havebeen used by Love and Burchb5 in the attemptto estimate coroniary flow. Difficulties in de-termining the uptake of the heart alone,separated from surroundinig organis, and thereduction of myocardial extractioni with time'
Circulation, Volu-me XXXIII, May 1966
714
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
MEASUREMENT OF CORONARY BLOOD FLOW
have prevented development of this approachinto a practical technique. Some of the techni-cal difficulties may be overcome by infusingthe positron-emitting 84Rb, in place of 86Rbas proposed by Bing and associates.16 Thislatter method, however, yields a "coronaryflow equivalent" which may be of clinicalvalue, but, as pointed out by its authors, itdoes not represent a procedure for quantita-tive measurement of coronary flow.
Excluding the methods that demand directinjections in the coronary arteries or in themyocardium, which can be only of limitedpractical value, the indirect Fick method,with N20, inert radioactive gases or 1311-anti-pyrine, seems the best available approach.More recently, thermodilution seems to bea promising approach to the problem ofdirectly measuring coronary sinus outflow.'7An evaluation of the potential merits and
disadvantages of the present method in com-parison with indirect Fick and thermodilutionmay be attempted.The main and immediately evident advan-
tage of the present technic over the other twois the avoidance of coronary sinus catheteriza-tion. While this feature may enhance thepractical value of the method, its limitationis inherent in the fact that any investigationof myocardial metabolism demands coronarysinus catheterization anyhow. However, inso-far as changes in oxygen requirements of theheart are essentially met by changes inflow,18-20 a CBF measurement may be of valueper se.The second unique feature of the present
technique is that of measuring the average flowto the entire myocardial mass, independentlyof the venous drainage. Unperfused areas,which do not contribute to the Fick valuessince they do not extract the indicator, con-tribute to the MCK or CBF values by thepresent method, in which the indicator con-tent of the entire heart is averaged, so thatareas with no indicator actually contributewith their zero value to the obtained average.The third, and probably most significant
point, is that the- flow value measured byMCK undoubtedly represents actual flow to
Circulation, Volume XXXIII, May 1966
true capillaries. The relevance of this featureis best appreciated if considered in the lightof the demonstration of arteriovenous anasto-motic circuits in the myocardium2' recentlyconfirmed to occur from the arterioles andmeta-arterioles to the venules.22 To our knowl-edge no estimates are presently available ofthe relative importance of flow shunting cir-cuits in the coronary vascular bed, nor abouttheir modifications in changing states. How-ever, the occurrence of such circuits and thedemonstration of nerve endings at the sphinc-teric structures of the anastomotic vessels22are suggestive of the potential importance ofdiversion of flow from true capillaries in theresponse of the coronary circulation to differ-ent stimuli.
Should this flow pattern be of some im-portance, most of the presently acceptedconclusions concerning the physiology, patho-physiology, and pharmacology of the coro-nary circulation would require reinvestigation,on the basis of a method capable of assessingtrue capillary flow.A further advantage of this method in
comparison with Kety's technique is its inde-pendence from prolonged steady state con-ditions: the fact that the entire measurementmay be completed in 90 seconds is an obviousadvantage in comparison with the indirectFick method, which demands long equilibra-tion periods. Repeatability at time intervalsas short as 5 minutes is an important featurethat stems from the previous considerations,although from this point of view the methodcan obviously not compete with thermodilu-tion.The main present drawback to the method,
which also limits its repeatability in the samepatient, stems from dosimetric considerations.The small percentage of y-radiations emit-ted by 86Rb demands the use of relativelylarge radioactive doses, which limit the num-ber of measurements that may be performedin the individual patient to a maximum oftwo. The use of 42K cuts down the patientdose by an important factor, but the shortnessof its physical half-life makes 42K a somewhatimpractical isotope to use.
7151
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
DONATO ET AL.
AppendixGeometrical efficiency factors required to
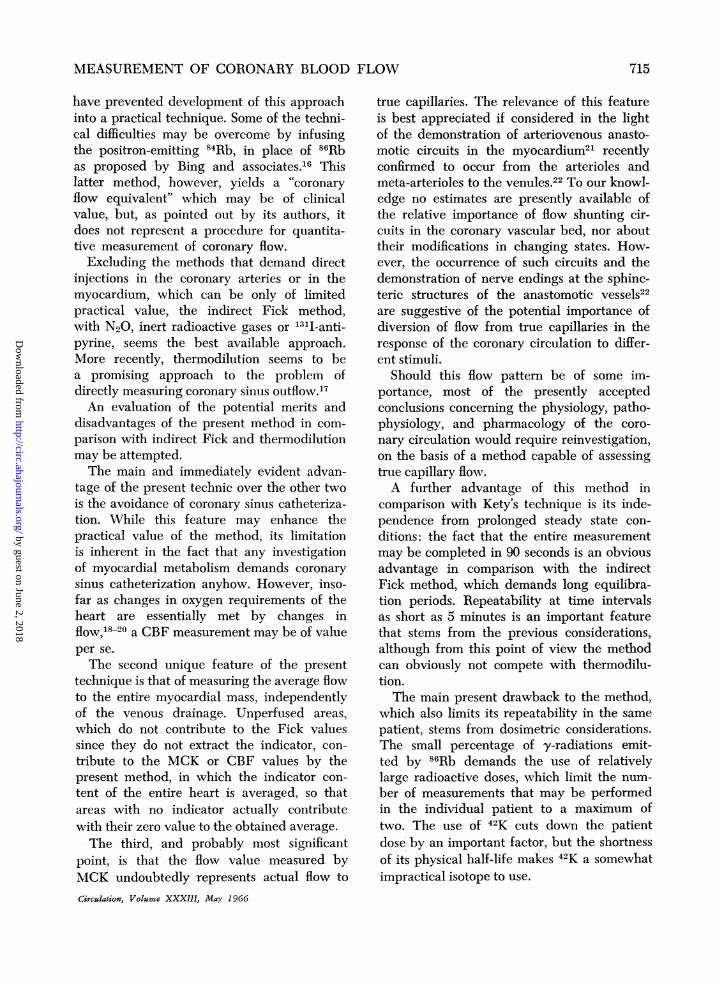
make precordial measurements of 1311 radio-activity from RIHSA comparable with 86Rbmeasurements were calculated by using aPerspex phantom.The phantom was made up of Perspex
slices of variable thickness (0.5 to 1 cm)that could be superimposed to simulate differ-ent chest diameters. Spheric containers of vari-able volumes (100 to 1000 ml) filled withradioactive solution can be included in thePerspex phantom in different positions.The following experiments were performed
counting with the TCS on the phantom:
Effect of Source VolumeThe same amount of radioactivity was
diluted in water-filled spheric containers ofsizes ranging from 100 to 1000 ml, placedat the center of the phantom, the thickness ofwhich along the TCS axis was 20 cm. Whenthe results are expressed as percentage dif-ferences from the counting rate for a 100-mlvolume, it is seen from figure 5 thbat deviationsare always smaller than 5% for both 131I and86Rb, and smaller than 2.5% up to 700 ml.
+10
+5
A%/o 0
-5
-10
0 500 1000SPHERE VOLUMEFigure 5
Changes of TCS counting rate on Perspex phantomfor the same amount of activity in spheric containersof increasing size, placed at the center of the phan-tom, on the counter axis. Changes are expressed as
percentage of the counting rate for a 100 ml con-
tainer. Closed circles, 131I; open circles, 86Rb.
+10r
4. 51-
A% Of
-10L0 500 1000
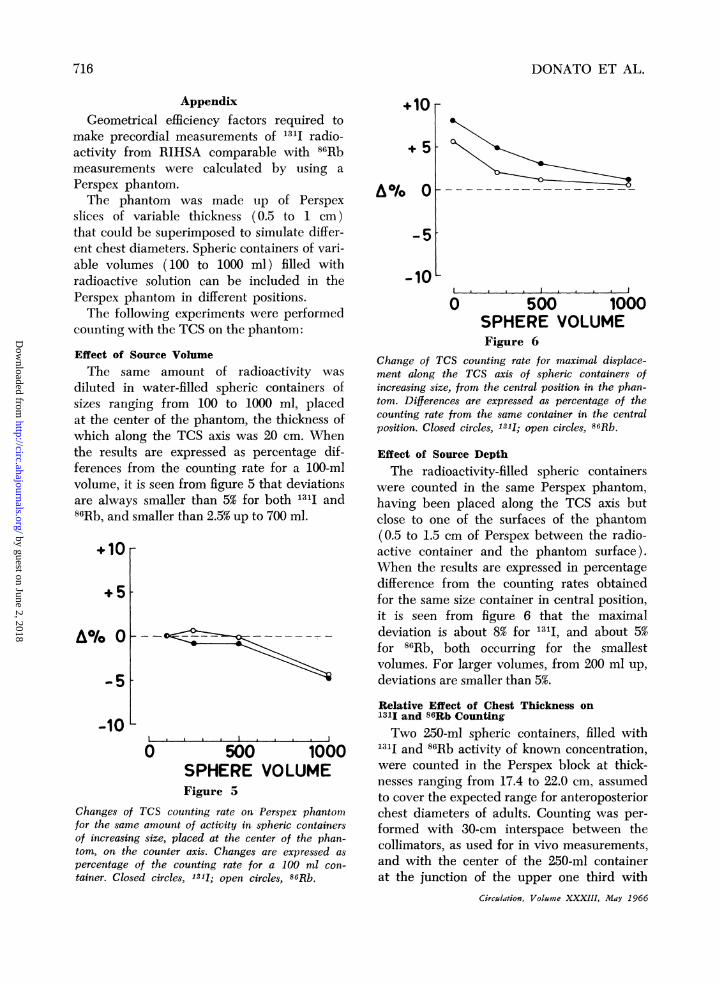
SPHERE VOLUMEFigure 6
Change of TCS counting rate for maximal displace-ment along the TCS axis of spheric containers ofincreasing size, from the central position in the phan-tom. Differences are expressed as percentage of thecounting rate from the same container in the centralposition. Closed circles, 1311; open circles, 86Rb.
Effect of Source Depth
The radioactivity-filled spheric containerswere counted in the same Perspex phantom,having been placed along the TCS axis butclose to one of the surfaces of the phantom(0.5 to 1.5 cm of Perspex between the radio-active container and the phantom surface).When the results are expressed in percentagedifference from the counting rates obtainedfor the same size container in central position,it is seen from figure 6 that the maximaldeviation is about 8% for 1311, and about 5%for 86Rb, both occurring for the smallestvolumes. For larger volumes, from 200 ml up,deviations are smaller than 5%.
Relative Effect of Chest Thickness on1311 and 86Rb CountingTwo 250-ml spheric containers, filled with
1311 and 86Rb activity of known concentration,were counted in the Perspex block at thick-nesses ranging from 17.4 to 22.0 cm, assumedto cover the expected range for anteroposteriorchest diameters of adults. Counting was per-formed with 30-cm interspace between thecollimators, as used for in vivo measurements,and with the center of the 250-ml containerat the junction of the upper one third with
Circulation, Volume XXXIII, May 1966
716
-5t
&I
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
MEASUREMENT OF CORONARY BLOOD FLOW
a:0
I.-;<2.2
<20LL~2Q
0 1.8I I
17 19 21 23CHEST A- P DIAMETER
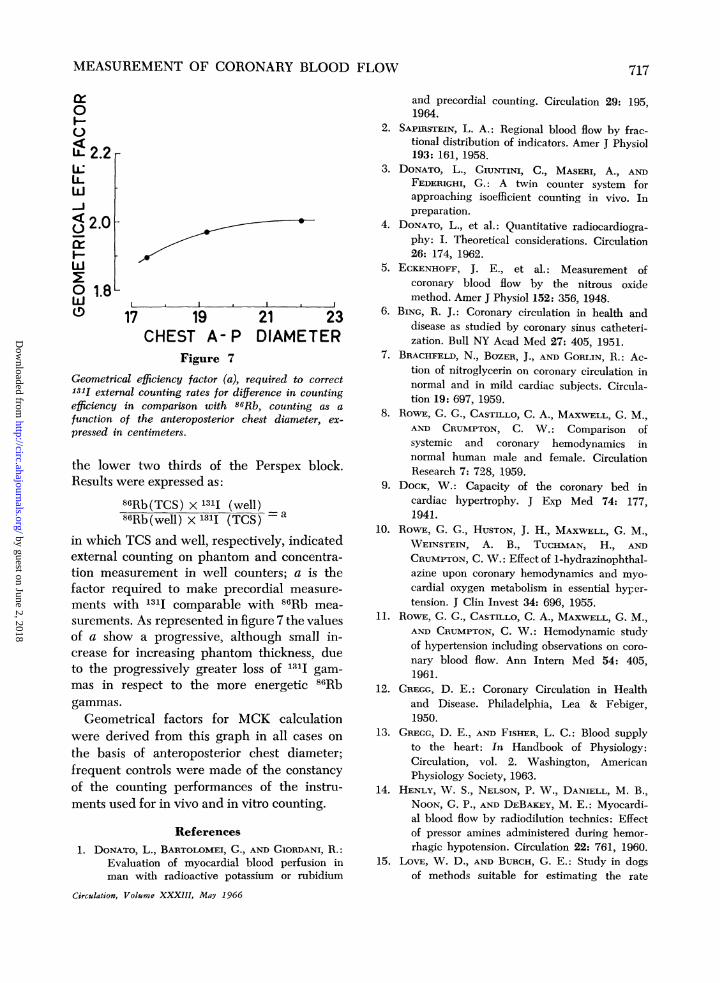
Figure 7
Geometrical efficiency factor (a), required to correct131I external counting rates for difference in countingefficiency in comparison with 86Rb, counting as a
function of the anteroposterior chest diameter, ex-
pressed in centimeters.
the lower two thirds of the Perspex block.Results were expressed as:
86Rb(TCS) x 131I (well)86Rb(well) x 1311 (TCS)
in which TCS and well, respectively, indicatedexternal counting on phantom and concentra-tion measurement in well counters; a is thefactor required to make precordial measure-
ments with 1311 comparable with 86Rb mea-
surements. As represented in figure 7 the valuesof a show a progressive, although small in-crease for increasing phantom thickness, dueto the progressively greater loss of 131I gam-
mas in respect to the more energetic 86Rbgammas.
Geometrical factors for MCK calculationwere derived from this graph in all cases on
the basis of anteroposterior chest diameter;frequent controls were made of the constancyof the counting performances of the instru-ments used for in vivo and in vitro counting.
References
1. DoNATo, L., BARTOLOMEI, G., AND GIORDANI, R.:Evaluation of myocardial blood perfusion inman with radioactive potassium or rubidium
Circulation, Volume XXXIII, May 1966
and precordial counting. Circulation 29: 195,1964.
2. SAPIRSTEIN, L. A.: Regional blood flow by frac-tional distribution of indicators. Amer J Physiol193: 161, 1958.
3. DONATO, L., GIUNTINI, C., MASERI, A., ANDFEDERIGHI, G.: A twin counter system forapproaching isoefficient counting in vivo. Inpreparation.
4. DONATO, L., et al.: Quantitative radiocardiogra-phy: I. Theoretical considerations. Circulation26: 174, 1962.
5. ECKENHOFF, J. E., et al.: Measurement ofcoronary blood flow by the nitrous oxidemethod. Amer J Physiol 152: 356, 1948.
6. BING, R. J.: Coronary circulation in health anddisease as studied by coronary sinus catheteri-zation. Bull NY Acad Med 27: 405, 1951.
7. BRACHFELD, N., BOZER, J., AND GORLIN, R.: Ac-tion of nitroglycerin on coronary circulation innormal and in mild cardiac subjects. Circula-tion 19: 697, 1959.
8. ROWE, G. G., CASTILLO, C. A., MAXWELL, G. M.,AND CRUMPTON, C. W.: Comparison ofsystemic and coronary hemodynamics innormal human male and female. CirculationResearch 7: 728, 1959.
9. DOCK, W.: Capacity of the coronary bed incardiac hypertrophy. J Exp Med 74: 177,1941.
10. RowE, G. G., HUSTON, J. H., MAXWELL, G. M.,WEINSTEIN, A. B., TUCHMAN, H., ANDCRUMPTON, C. W.: Effect of 1-hydrazinophthal-azine upon coronary hemodynamics and myo-cardial oxygen metabolism in essential hyper-tension. J Clin Invest 34: 696, 1955.
11. ROWE, G. G., CASTILLO, C. A., MAXWELL, G. M.,AND CRUMPTON, C. W.: Hemodynamic studyof hypertension including observations on coro-nary blood flow. Ann Intem Med 54: 405,1961.
12. GREGG, D. E.: Coronary Circulation in Healthand Disease. Philadelphia, Lea & Febiger,1950.
13. GREGG, D. E., AND FISHER, L. C.: Blood supplyto the heart: In Handbook of Physiology:Circulation, vol. 2. Washington, AmericanPhysiology Society, 1963.
14. HENLY, W. S., NELSON, P. W., DANIELL, M. B.,NOON, G. P., AND DEBAKEY, M. E.: Myocardi-al blood flow by radiodilution technics: Effectof pressor amines administered during hemor-rhagic hypotension. Circulation 22: 761, 1960.
15. LOVE, W. D., AND BURCH, G. E.: Study in dogsof methods suitable for estimating the rate
717
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
7DONATO ET AL.
of myocardial uptake of Rb86 in man and theeffect of l-norepinephrine and pitressin onRb86 uptake. J Clin Invest 36: 468, 1957.
16. BING, R. J., BENNISH, A., BLUIEMCHEN, G.,COHEN, A., GALLAGHER, J. P., AND ZALESKI,E. J.: Determination of coronary flow equiva-lent with coincidence counting technic. Circu-lation 29: 833, 1964.
17. FRONEK, A., AND GANZ, V.: Measurement offlow in single blood vessels including cardiacoutput by local thermodilution. CirculationResearch 8: 175, 1960.
18. ECKENHOFF, J. E., HAFKENSCHIEL, J. H., LAND-MESSER, C. M., AND HARMEL, M.: Cardiacoxygen metabolism and control of the coronarycirculation. Amer J Physiol 149: 634, 1947.
19. FOLTZ, E. L., PAGE, R. G., SHELDON, W. F.,WONG, S. K., TUTDDENHAM, W. J., AND WEISS,
A. J.: Factors in variation and regulation ofcoronary blood flow in intact anesthetizeddogs. Amer J Physiol 162: 521, 1950.
20. ALELLA, A., WILLIAMS, F. L., BOLENE-WIL-LIAMS, C., AND KATZ, L. N.: Interrelation be-tween cardiac oxygen consumption and coro-nary blood flow. Amer J Physiol 183: 570,1955.
21. PRINZMETAL, M., SIMPKIN, B., BERGMAN, N. C.,AND KRUGER, H. E.: Studies on the coronarycirculation: II. The collateral circulation in thenormal heart by coronary perfusion with radio-active erythrocytes and glass spheres. AmerHeart J 33: 420, 1947.
22. PROVENZA, D. V., AND SCHERLIS, S.: Demonstra-tion of muscle sphincters as a capillary com-ponent in the human heart. Circulation 20:35, 1959.
Introduction of Students to the Meath HospitalYou come here to convert theoretical into practical knowledge; to observe the symp-
toms of diseases previously known to you only through the medium of books or lectures;to learn the art of recognising these symptoms, and of appreciating their relative im-portance and value; to study their connexion with morbid alterations of internal organs;and, finally, to become acquainted with the best method of relieving your patients, bythe application of appropriate remedies.
Such, gentlemen, are the objects you seek in coming here; and in proportion to thenumber and importance of these objects, are the degree of responsibility attached toyour clinical instructors, and of blame to yourselves, should the opportunities whichthis institution offers for your benefit be neglected.-ROBERT J. GRAVES: Clinical Lec-tures on the Practice of Medicine, ed. 2. vol. 1. Dublin, Fannin and Co., 1848, p. 1.
Circulation. Volume XXXIII, May 1966
718
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from
L. DONATO, G. BARTOLOMEI, G. FEDERIGHI and G. TORREGGIANIRubidium: Critical Appraisal and Validation of the Method
Measurement of Coronary Blood Flow by External Counting with Radioactive
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1966 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.33.5.708
1966;33:708-718Circulation.
http://circ.ahajournals.org/content/33/5/708.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 2, 2018http://circ.ahajournals.org/
Dow
nloaded from