Le emergenze ipertensive: cosa fare e cosa non fare?
128
Le emergenze ipertensive: cosa fare e cosa non fare? Maria Lorenza Muiesan Università di Brescia ASST Spedali Civili di Brescia
Transcript of Le emergenze ipertensive: cosa fare e cosa non fare?

Le emergenze ipertensive: cosa fare e cosa non fare?
Maria Lorenza Muiesan
Università di Brescia
ASST Spedali Civili di Brescia

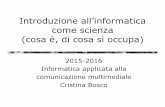
n engl j med 381;19 nejm.org November 7, 2019
A 58-year-old woman with known hypertension comes to the ED and reports headaches and blurred vision for the past 3 days. Her prescribed medications are amlodipine, HCTZ, and lisinopril, spotty adherence (no drugs in previous 3 weeks. She is anxious but comfortable. The average of multiple seated BP is 242/134 mm Hg, HR is 68 b/minFunduscopy shows arteriolar narrowing, bilateral flame hemorrhages, cotton-wool spots, and papilledema; auscultation reveals a fourth heart sound. ECG = left ventricular hypertrophy.Other laboratory tests and chest radiography are normal. Emergency computed CT of the head shows heterogeneous hypoattenuation of subcortical white matter in the posterior parieto-occipital regions bilaterally but no hemorrhage or infarction.
How would you further evaluate and treat this patient?

van den Born BH et al, Eur Heart J Cardiovasc Pharmacother. 2018
Abandon the term «hypertensive crisis»
Simplified stratification system: Hypertensive Emergency

DEFINITION OF HYPERTENSIVE EMERGENCIES
➢ Very high BP values associated with acute hypertension-mediated organ damage
➢ Key target organs: heart, retina, brain, kidneys, and large arteries
➢ Immediate BP reduction required to limit extension or promote regression of target organ damage
➢ The type of target organ damage is the principal determinant of the choice of treatment, target BP, and timeframe by which BP should be lowered
P van den Born et al. Management of hypertensive emergencies. European Heart Journal - Cardiovascular Pharmacotherapy 2018

An Italian survey: progetto GEAR (Gestione dell’Emergenza e urgenza in ARea critica)
European Journal Intern Med 2019
667 questionnaires

Trends in the Incidence of Hypertensive Emergencies in US Emergency Departments From 2006 to 2013
J Am Heart Assoc. 2016;5:e004511
incidence of 1640 per million adult ED visits in 2013, yielding an estimated rate increase of 13.9% per year
35%

Hospital Admissions for Hypertensive Emergencies and Urgencies
<Pinna et al , 2014

Prospective analysis
N = 1551
2.2% of admission to the ED
1551 (90%)
20%
80%
Emergencies
Urgencies
Age 70 ± 14 yrs,
range 18-102
M 44 %; F 56 %
Salvetti M et al J Hypertens 2019
N =1214
1.75 % of admission to the ED

Update 2019

STRATIFICATION OF HYPERTENSIVE EMERGENCIES ACCORDING TO THE CONDITION OR TARGET ORGAN INVOLVED
P van den Born et al. Management of hypertensive emergencies. European Heart Journal - Cardiovascular Pharmacotherapy 2018
advanced retinopathy, acute renal failure, and/or thrombotic microangiopathy (TMA)

Stratification of hypertensive emergencies according
to the condition or target organ involved
van den Born BH et al, Eur Heart J Cardiovasc Pharmacother. 2018
Acute and severe increases in BP can be precipitated by pheochromocytoma or by ingestion of sympathomimetics (meta-amphetamine or cocaine.) This can result in a hypertension emergency when there is evidence of acute HMOD

Adelaide Conti, Anna Paini, Chiara Rossetti, Marzia Bernini, Maria Lorenza Muiesan, Massimo Salvetti
The American Journal of Medicine, Vol 131, No 5, May 2018
A 25-year-old man was found unconscious by his wife in the bathroom of his apartment. She called emergency services and cardiopulmonary resuscitation was promptly initiated within a few minutes. The patient was intubated, transferred to the Emergency Department (ED) of a local hospital, and after 1 hour of advanced cardiac life support he was pronounced dead. His relatives reported a history of cocaine abuse; he had complained of epigastric discomfort during the previous 2 days


Table 30 Diagnostic workup for patients with a suspectedhypertension emergency
ESH ESC 2018 Hypertension Guidelines
diagnostic studies in patients with
suspected hypertensive emergency

In a patient admitted to the emergency department for acute hypertension,
a funduscopic examination may particularly helpful in identifying the
presence of exudates, haemorrages and/or papilledema.
The detection of these retinal changes indicates the presence of acute
organ damage and allows the diagnosis of hypertensive emergency and
of malignant hypertension

Traditional ophtalmoscope Smartphone small optical device (D-Eye, Si14 S.p.A.)
Muiesan Ml et al J Hypertens 2017
2 observers (1 trained not expert, 1 expert ophtalmologist )

BP lowering target/timing in hypertensive emergency
AHA/ACC , 2017• For adults with a compelling condition (i.e., aortic dissection,
severe preeclampsia or eclampsia, or pheochromocytomacrisis), SBP should be reduced to less than 140 mm Hg during the first hour and to less than 120 mm Hg in aortic dissection.
• For adults without a compelling condition, SBP should be reduced by no more than 25% within the first hour; then, if stable, to 160/100 mm Hg within the next 2 to 6 hours; and then cautiously to normal during the following 24 to 48 hours.
• In adults with a hypertensive emergency, admission to an intensive care unit is recommended for continuous monitoring of BP and target organ damage and for parenteral administration of an appropriate agent

Hypertension emergencies are situations in which severe hypertension (grade 3) is associated with acute HMOD, which is often lifethreatening and requires immediate but careful intervention to lower BP, usually with intravenous(i.v.) therapy.

•ESH/ESC guidelines 2018 and ESC/ESH position paper Eur Heart J Cardiovasc Pharmacother. 2018

DRUG CHOICE ACCORDING THE CAUSE AND MECHANISM OF THE HTN EMERGENCY


Stroke. 2019;50:e•••–e•••.

2019 Guidelines for Management of Acute Ischemic Stroke

Anderson C et al Lancet 2019; 393: 877–88
✓Fewer patients in the intensive group(160 [14·8%] of 1081) than in theguideline group (209 [18·7%] of 1115)had any intracranial haemorrhage (OR0·75, 0·60–0·94, p=0·0137).

Drug choice according the cause and mechanism of the HTN Emergency

- nitroglycerin, oxygen, aspirin,benzodiazepines, or calciumantagonists, alpha blockers
- Beta-blockers should beadministered with caution, sincetheir use may worsen vasospasm byallowing unopposed stimulation ofalpha receptors.
New England Journal of Medicine, 348;6
Treatment

“…A review of the literature revealed reports of serious adverse effects
such as cerebrovascular ischemia, stroke, numerous instances of
severe hypotension, acute myocardial infarction, conduction
disturbances, fetal distress, and death. Sublingual absorption of nifedipine
has been found to be poor; most of the drug is absorbed by the intestinal
mucosa. Given the seriousness of the reported adverse events and the lack
of any clinical documentation attesting to a benefit, the use of nifedipine
capsules for hypertensive emergencies and pseudoemergencies
should be abandoned”
JAMA 1996

An Italian survey: progetto GEAR (Gestione dell’Emergenza e urgenza in ARea critica)
European Journal Intern Med 2019

Need for a follow-up
• patients with hypertensive emergencies may have this condition because they are not adherent to their medications
• follow-up will allow for educating the patient about home BP monitoring that may improve hypertension control
• medications may not be enough to improve BP
• some patients with acute hypertensive emergencies may have a secondary cause for hypertension and an investigation for secondary hypertension is needed

Event-rate in emergencies and urgencies
(events/100pts/yrs)
14,5
11,8
7,5
42,7
4,33,5
0
5
10
15
Emergencies
4,53,6
1,9 1,7 0,9 1,7 2,3 2,380,9
0
5
10
15
Urgencies
Clinica Medica Università di Brescia & DEA Spedali Civili di Brescia, Muiesan et al ESH 2011
Cardiovascular event-rate during FU

Kumar N et al Hypertension. 2019;73:60-67.
Among patients with initial hospitalization for acute hypertensive emergency 17,8 % were hospitalized again within 30 days of the index admission.
Two prevalent conditions: acute HF, CKD

An Italian survey: progetto GEAR (Gestione dell’Emergenza e urgenza in ARea critica)
Are you aware of a protocol
for the management of
hypertensive
emergencies/urgencies ?
Are you using a fast-track for short
term re-evaluation of patients with
hypertensive emergencies/urgencies by
an hypertension specialist in your
hospital?
Yes No I don’t know Yes No
Eur Journal Intern Med 2019 Submitted

n engl j med 381;19 nejm.org November 7, 2019
The patient had acute severe hypertension complicated by PRES ie an hypertensiveemergency precipitated by nonadherence to antihypertensive therapy. She should be admitted to the intensive care unit and immediately begin IV nicardipine (given the relatively low HR) therapy guided by invasive intraarterial blood-pressure monitoring. BP was lowered by approximately 20 to 25% in the first hour, aiming for a blood pressure of approximately 160/100 mm Hg by 6 hours. Then, amlodipine and lisinopril were restsrted and her diuretic was restarted the following day, if needed. Nicerdipine was weaned over a period of 18 to 36 hours, although the timingshould be guided by close blood-pressure monitoring.Dischanrge when BP is controlled for at least 24 hours without the use of intravenous therapy, and arrangements for a follow-up office appointment within 1 week.
Do you agree ?

Asymptomatic uncontrolled hypertensionSBP or DBP >180 or >110 mmHg, respectively, in which OD is excluded
van den Born BH et al, Eur Heart J Cardiovasc Pharmacother. 2018

Acute BP increase (>180/110)
Absence of organ damage Presence of organ damage
Author NCV risk/ year
(approximated)
Vlcek M, 2008 384 6 %
Merlo C, 2012 50 6 %
Patel KK, 2016 58.535 1,8 %
Guiga H, 2017 285 8,9%
Author NCV risk/ year
(approximated)
Keith NM, 1939 200 78%
Guiga H, 2017 385 39%

Cardiovascular events*
Follow up (days)
Log Rank (Mantel-Cox) p<0.001
Emergencies
Urgencies
Emergencies
Urgencies
Log Rank (Mantel-Cox) p<0.0001
* Acute coronary syndromes, cerebrovascular events or hospitalizations for heart failure
0
4
8
12
16
20
Urgencies Emergencies
Events/100 patients/years
Muiesan et al, J Hypertens 2011 (abst)

• Male, 37 years, indian. • No previous diseases, no treatment• Left sided body weakness and numbness• BP 165/100 HR 70 bpm SpO2 98% AA. • Admitted to the Stroke Unit

• 4 hours after admission in the Stroke Unit chest pain
• BP 210/110 mmHg
• At echocardiography “ hypokinetic IV septum EF 55%”;
troponin I normal.
• Administration of IV nitroprussiate.

• 100% medium IVA occlusion with collaterals (Cdx).
• Occlusion 80 % LP Cdx
• Tubular stenosis 60% Cfx
• No PTCA because of recent ischemic stroke
• Patients moved from the Stroke Unit to the UTIC
100%
80%
60%

• Unstable angina
during hypertensive
crisis
• Coronary artery
disease
• Ischemic stroke
• Resistant
hypertension
• Diabetes mellitus
• Dyslipidemia
drug dosage
Ticagrelor 90 mg
+ASA 100mg
Amlodipine 10 mg 1cp x 2
Carvedilol 25mg Carvedilolo 25mg x 2
Ramipril 10mg 1cp
Doxazosin 4mg 1cp x 3
Candesartan 32 mg 1cp
Canrenone 100mg 1cp
NTG TTS 15 8→20
Aliskiren 150 mg 1cp x 2
Insulin lispro +
glargine
According to glycemia
Atorvastatin 40mg 1cp
Nitroprussiato ev During hypertensive
crisis with chest pain

In UTIC , despite treatment, BP values are still elevated;- PTCA is not performed because of fever and diarrhea (acute gastroenteritis).- Aorta and renal arteries angio-CT performed with the indication to evaluate elegibility for renal arteries denervation)
Moved from UTIC to Internal Medicine “Urgency Unit”

• Aorta + renal arteries Angio CT + adrenal CT : normal
• 24 hrs urinary metanephrine , PRA and palsma aldosterone , cortisol and TSH (all normal)
• Toxicology = negative
• No nocturnal SO2 desaturation (OSAS absent )

• Fundus oculi (II KW grade hypertensive retinopathy, no
diabetic retinopathy)
• Creatinine : 0.8 mg/dL
• Albumine/creatinine ratio 43,6 mg/g.
• Carotid Doppler US: IM Thickening and small plaques


• Unusual changes in BP when ev therapy (NTG +
labetalol) is stopped and changed to oral drugs
(ACE-I + CCB)
-20
20
60
100
140
180
220
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
PAS
PAD
EV EV EV


Event-rate in emergencies and urgencies
(events/100pts/yrs)
14,5
11,8
7,5
42,7
4,33,5
0
5
10
15
Emergencies
4.53.6
1.9 1.70.9
1.7 2.3
0
5
10
15
Urgencies
Clinica Medica Università di Brescia & DEA Spedali Civili di Brescia, Muiesan et al ESH 2011
Cardiovascular event-rate during FU

The term ‘hypertension urgency’ has also been used to describe severe hypertension in patients presenting to the emergency department in whom there is no clinical evidence of acute HMOD. Whilst these patients require BP reduction, they do not usually require admission to hospital,and BP reduction is best achieved with oral medication according to the drug treatment algorithm. However, these patients will require urgent outpatient review to ensure that their BP is coming under control

Park SK et al, J Hypertens 2017;35:1474-1480
CLINICAL EFFICACY OF RESTING VS ANTI-HYPERTENSIVE
TREATMENT IN HYPERTENSIVE URGENCIES
N.138 patients with hypertensive urgency randomized to resting vs resting + telmisartan 80 mg

EPISTASSI
✓60% della popolazione
✓PRIMARIE / SECONDARIE
✓Anteriori / posteriori

American Journal of the Medical Sciences: July 1930 - Volume 180 - Issue 1 - ppg 47-58
Epistaxis and hypertension

Kikidis D et al Eur Arch Otorhinolaryngol 2014;271(2):237-43.
Studies evaluation the relationship between epistaxis and hypertension

BP and epistaxis
Systolic BP Diastolic BP
*
126 subjects (84 M, age range 15-93 yrs march 2014-february 2015
Personal data, 2015


Conclusions The presence of high arterial blood pressure during the actual episode of nasal bleeding cannot establish a causative relationship with epistaxis, because of confounding stress and possible white coat phenomenon, but may lead to initial diagnosis of an already installed arterial hypertension.

Cerebral edema consequenceof an acute hyperperfusion
Symptoms : severe hypertensionseizures, lethargy, cortical blindness and coma, in the absence of an alternative explanation
Histopathological changes :cerebral oedema, microscopichaemorrhages and infarctionsPosterior reversible encephalopathysyndrome (PRES)
Hypertensive encephalopathy
10 % patients with malignant hypertension

Uncontrolled hypertension (>180/110)
Absence of organ damage Presence of organ damage
Author NCV risk/ year
(approximated)
Vlcek M, 2008 384 6 %
Merlo C, 2012 50 6 %
Patel KK, 2016 58.535 1,8 %
Guiga H, 2017 285 8,9%
Author NCV risk/ year
(approximated)
Keith NM, 1939 200 78%
Guiga H, 2017 385 39%

Shah M et al. Am J Hypertens. 2016
Trends in hospitalization for hypertensive emergency
2002–2012 nationwide inpatient sample database to identify patients with HTNE129,914 admissions, 630 (0.48%) patients died during their hospital stay
Presence of acute cardiorespiratory failure, stroke/TIA, chest pain, and aortic dissection were most predictive of higher hospital mortality.

The optimum therapy, treatment is dictated by consensus on the basis of:- particular presentation of the clinical situation- end-organ complications
-not on the absolute value of blood pressure

van den Born BH et al, Eur Heart J Cardiovasc Pharmacother. 2018

ULTIMA DIAPOSITIVA
Treatment aspects of hypertensive emergencies and urgencies vary widely according to a patient’s clinical conditions and are largely based on consensus from clinical experience , observations and comparisons of intermediate outcomes
Further research is needed to assess the impact of acute hypertension-mediated organ damage on future cardiovascular risk and its therapeutic consequences in these patients

Flow chart for acute BP elevation
[
]
Muiesan ML et al ESH Manual of Hypertension 2018

Treatment aspects of hypertensive emergencies and urgencies vary widely according to a patient’s clinical conditions and are largely based on consensus from clinical experience , observations and comparisons of intermediate outcomes
Further research is needed to assess the impact of acute hypertension-mediated organ damage on future cardiovascular risk and its therapeutic consequences in these patients
Conclusions

•
• Which of the following is used to define a hypertensive emergency?
– The velocity of acute rise in blood pressure
– The presence of clinical organ damage
– The presence of comorbidities
– The sympathetic nervous system activation
•
• Among the following diagnostic examinations, which one is useful for the diagnosis of a hypertensive emergency ?
• Blood pressure monitoring
• Fundus oculi examination
• Kidney ultrasound
• Abdominal ultrasound
•
• Among the following , which drug is more likely used for the treatment of a patient with an hypertensive emergency ?
• Oral Captopril
• Intravenous nitrate
• Transdermal nitrate
• Sublingual nifedipine
•
• Which drug is less indicated for the treatment of cocaine induced acute coronary syndrome?
• ASA
• Beta-blockers
• Heparin
• benzodiazepines
•
• In a patient with hypertensive encephalopathy the time line and BP target are
• Minutes, < 90 mmHg
• Minutes , - 20-25 % MAP
• Hours , < 140 mmHg
• Several hours, < 120 mmHg

A 58-year-old woman with known hypertension comes to the emergency department
and reports headaches and blurred vision for the past 3 days. Her prescribed medications
include amlodipine, hydrochlorothiazide, and lisinopril, but she acknowledges
spotty adherence and has not taken any of the drugs in approximately 3 weeks. On
examination, she is anxious but comfortable. The average of multiple seated bloodpressure
measurements is 242/134 mm Hg, and the heart rate is 68 beats per minute.
Funduscopy shows arteriolar narrowing, bilateral flame hemorrhages, cotton-wool
spots, and papilledema; auscultation reveals a fourth heart sound. The remainder of
the examination is normal. The electrocardiogram shows left ventricular hypertrophy.
Other laboratory tests and chest radiography are normal. Emergency computed
tomography of the head shows heterogeneous hypoattenuation of subcortical white
matter in the posterior parieto-occipital regions bilaterally but no hemorrhage or
infarction. How would you further evaluate and treat this patient?

Massimo Salvetti Medicina Interna & 2a Medicina
Università di Brescia-ASST Spedali Civili di Brescia
Le emergenze ipertensive:
il trattamento delle forme più comuni

Donna 42 aa
- Ipertensione arteriosa nota da almeno 7 anniTerapia solo per alcuni mesi, autosospesa dalla paziente per benessere soggettivo
- Familiarità per ipertensione arteriosa
- Da un mese circa riferisce dispnea da sforzo, ortopnea

Accesso in PS per:
- improvviso peggioramento della dispnea a riposo
- comparsa di ortopnea
- cefalea pulsante
- Non dolore toracico
✓ Dispnoica; PA 260/145 mmHg (dx=sn); FC 120 r ; SatO2 88% in aa, T 36C°
✓ Rantoli crepitanti bilaterali campi medi e basi polmonari
Emocromo: nella normaCreatininemia 0,7 mg/dlLieve incremento AST e ALTTroponina I 0,02 ng/mL; CK-MB normaliCoagulazione: normaleD-dimero: negativoEAB arterioso : lieve ipossiemia

Tachicardia sinusale; IVS; sovraccarico VS

• RX Torace

In DEA: Labetalolo ev 75 mg
PA 170/120 mmHg
Ricoverata UTIC: PA 180/130 mmHg; Fc 80 bpm (r)

Ecocardiogramma:
- Marcata ipertrofia VS concentrica
- Sezioni destre nella norma
- Conservata funzione sistolica globale e regionale (EF 57%)
- IM ++; IT ++ PAPs 64 mmHg
- VCI congesta
- Disfunzione diastolica VS (E/e’ 15)

Inizia infusione con nitroprussiato ev e boli di furosemide evMetoprololo ev
In circa 3 ore
PA 260/145 mmHg → 170/120 mmHg→ PA 140/90 mmHg
Trasferita presso la nostra Divisione (sezione Medicina d’Urgenza)
Netta regressione della dispneaComparsa di “discomfort” retrosternaleComparsa di alterazioni della ripolarizzazione all’ECG (T negative)Troponina I sempre negativa
→ PA 120-130/80-85 mmHg in 20 ore


Sospeso nitroprussiato ev
Prosegue con Furosemide boli ev
Shift a terapia per os:- Bisoprololo- Amlodipina- Doxazosina
Medicina d’Urgenza C/O Clinica Medica/2 Medicina Spedali Civili BS

Angio-TAC
“… coronarie pervie…”

Alterazioni ECG durante la prima fase di trattamento (rapida-brusca riduzione dei valori di PA)
Pz con spiccata ipertrofia VS e valori di PA elevati:
M.Pepi, M.Alimento, D.Guazzi, Eur Heart J 1988
la rapida riduzione dei valori di PA (terapia e.v.)
In ipertrofia VS da ipertensione arteriosa Alterata riserva coronarica Alterato rapporto media:lume nei vasi di resistenza (ipertrofia della media)→Elevati valori di PA necessari per adeguata perfusione coronarica→ rapida riduzione PA (→ “furto coronarico”)→ sofferenza subendocardio
→ alterazioni ECG suggestive per sofferenza miocardio (T neg.) in parallelo alle modificazioni dei valori di PA

2015 ESC Heart Failure Guidelines, European Heart Journal 2016

J Cardiac Fail 2016;22:618–627
“…Hypertensive acute heart failure (H-AHF) isdefined as the rapid onset of pulmonarycongestion in the setting of a systolic bloodpressure >140 mm Hg, and often >160 mm Hg…”

Presentations of Hypertensive Acute Heart
Failure Darling et al J Cardiovasc Dis Diagn. 2017
four historical, cross-sectional cohorts with AHF who were admitted to tertiary care medical centres in the North-eastern USA in 1995, 2000, 2006, and 2011–13.
Hypertensive Acute HF

Aortic dissection
Stroke
37%
79 % ischemic
21% hemorrhagic37.5%
Acute Heart Failure
Acute Coronary Syndrome
25%
0,5 %
Journal of Hypertension 2019

✓ Acute heart failure precipitated by rapid andexcessive increase in arterial blood pressuretypically manifests as acute pulmonary oedema.
✓ A prompt reduction in blood pressure should beconsidered as a primary therapeutic target andinitiated as soon as possible.
✓ Aggressive blood pressure reduction (in the rangeof 25% during the first few hours and cautiouslythereafter) with i.v. vasodilators in combinationwith loop diuretics is recommended.
ESC Heart Failure Guidelines, European Heart Journal 2016


Indication Drugs Goal of treatment BP goal Adverse effects
Acute heart
failure
Systolic dysf
Nitroglycerin,
sodium nitroprusside,
furosemide, nesiritide (for
improvement of dyspnea)
Reduce peripheral
resistance and
cardiac workload,
without affecting
cardiac contractility
Reduce 15 % of
baseline BP, until
resolution of acute
pulmonary edema
Non invasive
ventilation may induce
a rapid BP ↓
Avoid SBP ↓ < 110
mmHg
Acute heart
failure
Diastolic dysf
Nitroglycerin, sodium
nitroprusside,
furosemide, betablockers
or nonDHPD CCB
Reduce peripheral
resistance and
cardiac workload
(heart rate)
Reduce 15 % of
baseline BP, until
resolution of acute
pulmonary edema
Non invasive
ventilation may induce
a rapid decrease of BP
Muiesan ML et al J Cardiovasc Med 2015

Peackock FW et al Am Heart J 2014;167:529-36
Clevidipine in acute heart failureBlood Pressure Control in Acute Heart Failure
A Pilot Study (PRONTO)
Serious adverse events (24% vs 19%) and 30-day mortality (3 vs 2) were similar between clevidipine and SOC, respectively, and there were no deaths during study drug administration

Aortic dissection
Stroke
37%
79 % ischemic
21% hemorrhagic37.5%
Acute Heart Failure
Acute Coronary Syndrome
25%
0,5 %
Journal of Hypertension 2019

Higher BP
Myocardial stress and oxygen needs

Muiesan ML et al J Cardiovasc Med 2015
European Heart Journal 2016
Indication Drugs Goal of treatment BP goal
Acute coronary
syndrome + HT
Emergency
Nitroglycerin, (sodium nitroprusside),
labetalol, metoprolol, esmolol,
nicardipine
Reduce cardiac
workload and improve
coronary perfusion
Reduce 25 % of
baseline BP in 3-4
hours
5.1 Pharmacological treatment of ischaemia5.1.1 General supportive measuresThe goal of pharmacological anti-ischaemic therapyis to decrease myocardial oxygen demand(secondary to a decrease in heart rate,blood pressure, preload or myocardial contractility)or to increase myocardial oxygen supply (byadministration of oxygen or throughcoronary vasodilation)

“…A review of the literature revealed reports of serious adverse effects
such as cerebrovascular ischemia, stroke, numerous instances of
severe hypotension, acute myocardial infarction, conduction
disturbances, fetal distress, and death. Sublingual absorption of nifedipine
has been found to be poor; most of the drug is absorbed by the intestinal
mucosa. Given the seriousness of the reported adverse events and the lack
of any clinical documentation attesting to a benefit, the use of nifedipine
capsules for hypertensive emergencies and pseudoemergencies
should be abandoned”
JAMA 1996

Adelaide Conti, Anna Paini, Chiara Rossetti, Marzia Bernini, Maria Lorenza Muiesan, Massimo Salvetti
The American Journal of Medicine, Vol 131, No 5, May 2018
A 25-year-old man was found unconscious by his wife in the bathroom of his apartment. She called emergency services and cardiopulmonary resuscitation was promptly initiated within a few minutes. The patient was intubated, transferred to the Emergency Department (ED) of a local hospital, and after 1 hour of advanced cardiac life support he was pronounced dead. His relatives reported a history of cocaine abuse; he had complained of epigastric discomfort during the previous 2 days

“…The risk of myocardial infarction onset was elevated 23.7 times over baseline (95% CI 8.5 to 66.3) in the 60 minutes after cocaine use. The elevated risk rapidly decreased thereafter…” Circulation. 1999


- nitroglycerin, oxygen, aspirin,benzodiazepines, or calciumantagonists, alpha blockers
- Beta-blockers should beadministered with caution, sincetheir use may worsen vasospasm byallowing unopposed stimulation ofalpha receptors.
New England Journal of Medicine, 348;6
Treatment

“…Beta-blockers should not be administered inpatients with symptoms possibly related tocoronary vasospasm or cocaine use, as theymight favour spasm by leaving alpha-mediatedvasoconstriction unopposed by beta-mediatedvasodilation…”
2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation

Aortic dissection
Stroke
37%
21% hemorrhagic
79 % ischemic37.5%
Acute Heart Failure
Acute Coronary Syndrome
25%
0,5 %
Journal of Hypertension 2019

✓ incidence of 24.6 per100.000 person-years
✓ 10 to 20% of all strokes inCaucasians
✓ Mortality:40% at 1 month55% at 1 year
✓ only 18 to 39% of patientsliving independently at 1year
Intracerebral hemorrhage

✓ High BP is associated with increased risk of death, disability or neurological deterioration in patients with hemorrhagic stroke
✓ Hematoma volumes > 30 ml are related to increased mortality rates (60%-90%) at 1 month after ICH
✓ Increased BP is related to hematoma growth and formation of cerebral edema
✓ Hematoma expansion is a frequent complication of ICH, occurring in 30% of patients (mainly in the first 24 hours)
✓ for each 1 ml increase in hematoma expansion, the risk of death and dependency will increase by 5%

Prevalence of Elevated Blood Pressure in 563,704 Adult Patients Presenting to the Emergency Department with Stroke in USA
Qureshi AI et al Am J Emerg Med. 2007; 25(1): 32–38.
SBP > 140 mmHg- ICH 75%- SAH 100%

Mortality rate according to admission BP (all strokes)
Journal of Internal Medicine 2004
0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100
Mortality at one month in hemorrhagic stroke (%)
SBP DBP

The already compromised cerebral blood flow (CBF) in
the perihematomal area due to the compression of
small arteries by the hematoma and the associated
edema might be further reduced by aggressive BP
lessening and might led to perihematomal ischemia
Theroretical risks associated with BP lowering in acute stroke

Linear regression indicated no relationship between the absolute change in systolic bloodpressure (BP) and perihematoma relative cerebral blood flow (rCBF) in the <150 mm Hg (R=0.00005; 95% CI, −0.001 to 0.001) or <180 mm Hg target groups (R=0.000; 95% CI, −0.001 to 0.001).
Conclusions—Rapid BP lowering after a moderate volume of ICH does not reduce perihematoma CBF. These physiological data indicate that acute BP reduction does not precipitate cerebral ischemia in ICH patients.
ICH ADAPT Investigators, Stroke 2013
n=75

INTERACT2 Investigators, N Engl J Med 2013
- We randomly assigned 2839 patients who had had a spontaneous intracerebralhemorrhage within the previous 6 hours and who had elevated systolic bloodpressure to receive intensive treatment to lower their BP (with a target SBP of <140mm Hg within 1 hour) or guideline-recommended treatment (with a target SBP of<180 mm Hg) with the use of agents of the physician’s choosing.
Intensive BP treatment was safe and associated with significantly better health-related quality of life than standard BP treatment. The two groups did not differ significantly in terms of all-cause mortality and hematoma expansion.
(Baseline hematoma vol 11, IQ range 6-20)

2015 AHA/ASA Guidelines for the Management of Spontaneous Intracerebral Hemorrhage
RecommendationIn acute ICH within 6 h of onset, intensive blood pressure reduction (systolic target <140 mmHg in <1 h) is safe and may be superior to a systolic target <180 mmHg. No specific agent can be recommended. Quality of evidence: ModerateStrength of recommendation: Weak
2014 European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage
Recommendations1. For ICH patients presenting with SBP between 150 and 220 mm Hg and without
contraindication to acute BP treatment, acute lowering of SBP to 140 mm Hg is safe (Class I; Level of Evidence A) and can be effective for improving functional outcome (Class IIa; Level of Evidence B). (Revised from the previous guideline)
2. For ICH patients presenting with SBP >220 mm Hg, it may be reasonable to consideraggressive reduction of BP with a continuous intravenous infusion and frequent BP monitoring (Class IIb; Level of Evidence C). (New recommendation)

1.000 participants with intracerebral hemorrhage (volume, <60 cm3) and a Glasgow ComaScale score of 5 or more to a SBP target of 110 to 139 mm Hg (intensive treatment) or atarget of 140 to 179 mm Hg (standard treatment); intravenous nicardipine to lower bloodpressure was administered within 4.5 hours after symptom onset (+ labetalol if needed)Enrollment was stopped because of futility after a prespecified interim analysis
The mean minimum systolic blood pressure during the first 2 hours was 128.9±16 mm Hg in the intensive treatment
- 141.1±14.8 mm Hg in the standard-treatment
ATACH-2 Trial Investigators

Carandini et al, Intern Emerg Med 2017
- six studies for a total of 4385 patients (mean age 62 years, 62.3% men)

ESC Council on hypertension position document on the management of hypertensive emergencies
European Heart Journal - Cardiovascular Pharmacotherapy 2018

Lowering blood pressure after acute intracerebral haemorrhage:protocol for a systematic review and meta-analysis using individualpatient data from randomised controlled trials participating in theBlood Pressure in Acute Stroke Collaboration (BASC)
BMJ Open 2019
✓ Introduction Conflicting results from multiple randomized trials indicate that themethods and effects of blood pressure (BP) reduction after acute intracerebralhaemorrhage (ICH) are complex.
✓ The Blood pressure in Acute Stroke Collaboration is an international collaboration, whichaims to determine the optimal management of BP after acute stroke including ICH.
✓ The primary outcome will be functional outcome according to the modified RankinScale.
✓ Safety outcomes will be early neurological deterioration, symptomatic hypotension and✓ serious adverse events.✓ Secondary outcomes will include death and neuroradiological and haemodynamic
variables.

Aortic dissection
Stroke
37%
21% hemorrhagic
79 % ischemic37.5%
Acute Heart Failure
Acute Coronary Syndrome
25%
0,5 %
Journal of Hypertension 2019

Prevalence of Elevated Blood Pressure in 563,704 Adult Patients Presenting to the Emergency Department with Stroke in USA
Qureshi AI et al Am J Emerg Med. 2007; 25(1): 32–38.
SBP > 140 mmHg: In > 75 % of pts

Bangalore et al, European Heart Journal (2017) 38, 2827–2835
✓ Patients in the Get With The Guidelines-Stroke registry with acute ischaemic stroke were included (n= 309 611 )

collateral flow by
loss of autoregulation due to
ischemia, increasing
infarction size
cerebral edema,
hemorrhagic transformation
favour long term BP control
Early BP lowering in ischemic stroke

Lee M et al. Stroke. 2015;46:1883-1889.
Effect of Blood Pressure Lowering in Early Ischemic Stroke
Relative risk with 95% confidence interval (CI) estimates
for death or dependency (early blood pressure lowering vs control)
at 3 months or at trial end point among patients with ischemic stroke.

2018 AHA/ASA Guidelines for the Early Management of Patients With Acute Ischemic Stroke

✓ Nine studies were included, for a total of 1037 patients.
✓ The heterogeneity in findings with respect to BP monitoring and studied parameters precluded a
meta-analysis
Stroke. 2019;50:00-00

✓ We recommend that systolic blood pressure should be maintained >140
mm Hg (fluids and vasopressors) and <180 mm Hg (with or without IV tPA),
and diastolic blood pressure <105 mm Hg (class IIa, level of evidenceB).
✓ We also recommend that blood pressure targets may be adjusted (lowered) in
communication with the neurointerventionalists and neurologists following
successful recanalization of occluded vessel(s) (class IIb, level of evidence
C), as reperfused brain often lacks autoregulation leading to high risk of
hyperperfusion leading potentially to hemorrhagic conversion.
Society for Neuroscience in Anesthesiology and Critical Care Expert Consensus Statement:
Anesthetic Management of Endovascular Treatment for Acute Ischemic Stroke
Stroke. 2014;45:e138-e150
Recommendations for Periprocedural Hemodynamic Management

Indication Drugs Goal of
treatmentBP goal
Adverse
effects
Acute ischemic
stroke
Labetalol, esmolol,
nicardipine, clevidipine*,
nitroglycerin, urapidil,
sodium nitroprusside (only if
DBP > 140 mmHg)
Avoid hemorrhagic
conversion and
enlargement of ischemic
penumbra
Reduce 15 % of
baseline BP (if
>220/115) in 2-3 hours
Acute but gentle BP
reduction indicated only if
fibrinolysis is planned
(BP < 185/110 mmHg)
Hypertensive
encephalopathy
Labetalol, nicardipine,
esmolol
Reduce intracranial
pressure
Reduce 25 % of
baseline BP in 2-3
hours
Muiesan ML et al J Cardiovasc Med 2015

Lancet 2019
Prehospital treatment withtransdermal GTN does not seem toimprove functional outcome inpatients with presumed stroke
✓ 1149 adults with presumed stroke within 4 h of onset, systolic blood pressure 120 mmHg or higher.
✓ Randomly assigned (1:1) to receive transdermal GTN (5 mg once daily for 4 days; theGTN group) or a similar sham dressing (the sham group) in Ukbased ambulances byparamedics
✓ 597 (52%) patients had ischaemic stroke, 145 (13%) had intracerebral haemorrhage, 109(9%) had transient ischaemic attack, and 297 (26%) had a non-stroke mimic at the finaldiagnosis of the index event.
✓ In the GTN group, SBP was lowered by 5·8 mm Hg compared with the sham group(p<0·0001), and DBP was lowered by 2·6 mm Hg (p=0·0026) at hospital admission.
Distribution of mRS score at day 90

Methods - In 2005, AIS cases were ascertained at all 16 hospitals in Greater Cincinnati. BP wasrecorded at emergency department presentation and before and after antihypertensivetreatment. Hypertension was defined as BP 220/120 mm Hg.
Results - A total of 1739 patients with AIS met inclusion criteria. Median age was 72 yearswith 43% male and 25% black.
Conclusions - Only one third of patients with acute ischemic stroke treated withantihypertensives met American Heart Association recommended treatment criteria, andthe rate of change of BP was frequently greater than recommended. Further studies arewarranted to determine the impact of practice patterns on AIS outcomes.
(Stroke. 2012;43:557-559.)

•ESH/ESC guidelines 2018 and ESC/ESH position paper Eur Heart J Cardiovasc Pharmacother. 2018

San Sebastiano, Antonello da Messina (1478)

Grazie


Patients with a hypertensive emergency should be
admitted for close monitoring and, in most cases, treated
with intravenous blood pressure lowering agents to
reach the recommended BP target in the designated
time-frame
ESC Council on hypertension position document on the management of hypertensive emergencies Eur Heart Journal 2018

Management
Place two large bore IVs; monitor heart rate and blood pressure continuously,
preferably using an arterial line.
Control heart rate and blood pressureΔ. Maintain heart rate <60 BPM and systolic
blood pressure between 100 and 120 mmHg.
Administer esmolol (250 to 500 mcg/kg IV loading dose, then infuse at 25 to 50
mcg/kg/minute; titrate to maximum dose of 300 mcg/kg/minute) or labetalol (20 mg
IV initially, followed by either 20 to 80 mg IV boluses every 10 minutes to a
maximal dose of 300 mg, or an infusion of 0.5 to 2 mg/minute IV). If beta blockers
are not tolerated, alternatives are verapamil or diltiazem.
Once heart rate is consistently <60 BPM, give vasodilator therapy. IF the systolic
blood pressure remains above 120 mmHg, initiate nitroprusside infusion (0.25 to
0.5 mcg/kg/minute titrated to a maximum of 10 mcg/kg/minute) or nicardipine
infusion (2.5 to 5 mg/hour titrated to a maximum of 15 mg/hour). Vasodilator
therapy (eg, nitroprusside, nicardipine) should not be used without first
controlling heart rate with beta blockade.
Give IV opioids for analgesia (eg, fentanyl).
Place Foley catheter for assessment of urine output and kidney perfusion.
Blood pressure control in aortic dissection

Clinical features and evaluation
Acute onset of severe, sharp, or knife-like pain in the anterior chest, with radiation to the
neck, back, or abdomen. Pain may be migratory.
Assess risk factors for TAAD*.
Palpate carotid, subclavian, and femoral pulses; note any significant differences between
sides. Obtain blood pressure in both arms.
Auscultate for diastolic cardiac murmur of aortic regurgitation; assess for tamponade
(muffled heart sounds, jugular venous distention, pulsus paradoxus).
Evaluate for signs of ischemic stroke, spinal cord ischemia, ischemic neuropathy, hypoxic
encephalopathy.
Findings suggesting involvement of the ascending aorta include back pain, anterior chest
pain, hemodynamic instability, diastolic cardiac murmur, tamponade, syncope or stroke
(persistent or transient¶; right hemispheric stroke is most common, but bilateral can occur),
Horner syndrome (typically partial with ptosis/miosis), weak or absent carotid or subclavian
pulse, upper extremity pain/paresthesia/motor deficit.
Findings suggesting involvement of the descending aorta include back pain, chest pain,
abdominal pain, weak or absent femoral pulses, lower extremity pain/paresthesia/motor
deficit, acute paraplegia.
Aortic dissection

Findings on initial studies
Obtain ECG. Look for signs of ACS; extension of type A dissection to coronary ostia can cause coronary
ischemia (right coronary artery most commonly affected).
Obtain D-dimer, CBC, basic electrolytes, LDH, cardiac markers, coagulation parameters, and type and
crossmatch. D-dimer <500 ng/dL is less likely to be aortic dissection.
Chest radiograph: Widened mediastinum and/or unexplained pleural effusion are consistent with
dissection, particularly if unilateral.
Vascular imaging
For hemodynamically stable patient without suspicion for ascending aortic involvement: Obtain thoracic
CT angiography or MR angiography, depending upon resources and speed of acquisition. Dissection is
confirmed by presence of intimal flap separating true and false lumen. If these are not readily available or
there is a contraindication, obtain transesophageal echocardiogram.
For hemodynamically unstable patient or for strong suspicion of ascending aortic involvement: Obtain
transesophageal echocardiogram. If not immediately available, obtain CT angiography.
Transthoracic echocardiography may be useful for identifying complications of ascending aortic
dissection (eg, aortic valve regurgitation, hemopericardium, inferior ischemia) but is not sensitive for
identification of dissection.
Aortic dissection