Keratoconus - Dr Shylesh B Dabke
41
Dr Shylesh B Dabke Resident, Dept Of Ophthalmology KMC, Mangalore Keratoconus ly download and watch in Slideshow mode ne viewing will be disgusting Kindly download and watch in Slideshow Online viewing will be disgusting
-
Upload
shylesh-dabke -
Category
Health & Medicine
-
view
49 -
download
7
Transcript of Keratoconus - Dr Shylesh B Dabke

Dr Shylesh B Dabke Resident, Dept Of OphthalmologyKMC, Mangalore
Keratoconus
Kindly download and watch in Slideshow modeOnline viewing will be disgusting
Kindly download and watch in Slideshow modeOnline viewing will be disgusting

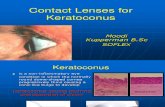
•Keratoconus a noninflammatory corneal ectasia, is characterized by progressive corneal thinning and apical protrusion
•Described first by Burchard Mauchart(Staphyloma Diaphanum). John Nottingham(1854) clearly described keratoconus and distinguished it from other ectasia’s of cornea
•Preoperative topographic screening prior to keratorefractive surgery has largely focused on keratoconus
Introduction

•Earlier reported to be higher in women than in men•However recent studies suggested it to be higher in men or that there is
no significant difference
• It is bilateral in over 90% of patients•Prevalence - 54.5 per one lakh population•Asians have a fourfold higher incidence and are younger at presentation
compared to westerns
Sex Predilection
Prevalence & Statics

• Isolated sporadic •Heredity•Eye rubbing•Associated systemic conditions*
•Hormonal changes*
•Rigid contact lens wear
Etiology*

•Biomechanical hypothesis proposes keratoconus to result from interlamellar and interfibrillar slippage of collagen within stroma*
• In addition to biomechanical changes, the concept of tissue degradation based on the demonstration of collagen loss and proteoglycan changes in affected cornea and on the up-regulation of degradative enzymes have also been postulated
Pathophysiology

1• Same collagen content like normal cornea
2• Decreased corneal stability
3• 2 times higher rate of degradation of cornea
Keratoconus
Reduced amount of cross linking

•Although can present in any age group, it more commonly affects patients in their late teens or early twenties
•The condition almost always progressive but the rate of progression and severity is variable
•Tends to progress more rapidly in young patients
•About 10-20% eventually require corneal transplant
Clinical Features

•Symptoms are highly variable and depend on the stage of the progression of the disorder
•Early in the disease there may be no symptoms & may be noted simply because the patient cannot refracted to a clear 6/6 corrected vision
Symptoms

Deteriorating visual acuity, distortions, glare
Frequent change in refraction
Visual acuity not correctable to 6/6
Monocular polyopia or Ghosting
Symptoms

Corneal thinning
Munson’s sign
Rizutti’s sign
Signs

Vogt’s striae(40%)
Fleischer ring(50%)
Corneal apical scarring(20%)
Prominent corneal nerves
Slit lamp signs

Hydrops

Scissoring reflex on retinoscopy
Oil droplet sign(“charleaux sign”)
Retro-illumination
signs

Compression of mires inferotemporally or centrally
Egg shaped mires
Photo-keratoscopic
signs

Localized increase of surface power*
Inferior-superior diopteric asymmetry
Video-keratography signs

•Keratoconus- Clinical slit-lamp signs of keratoconus
- Scissoring on retinoscopy - Keratoconus topography pattern
•Early/subclinical keratoconus- No slit lamp findings- Scissoring of reflex of the retinoscopy - Keratoconus topography pattern
•Keratoconus-suspect- No clinical signs, no scissoring- Keratoconus topography pattern
Terminology

• Increased area of corneal power surrounded by concentric areas of decreasing power
• Inferior-superior power asymmetry•Skewing of the steepest radial axes above and below the horizontal
meridian(asymmetric bow tie with skewed radial axes (AB/SRAX) pattern)
Characteristic Keratoconus Topographic Pattern*

Classification

Nipple cone
Oval cone
Globus cone
Cone type & position

Mild <48D
Moderate 48-54D
Severe >54D
Corneal curvature

Differential Diagnosis

Pellucid marginal degeneration
Terrien marginal corneal degeneration
Keratoglobus
Posterior keratoconus

•Keratometry- mires commonly are steep, highly astigmatic, irregular and often appear egg shaped.- Also shows increased keratometry values between 45-52D or more
•Videokeratography- Commonly shows inferior corneal steeping
Diagnosis

•Consists of three corneal topographic derived indices which when abnormal should alert the clinician to consider keratoconus as diagnosis
•The indices are:- Keratometry value quantifies the central steepening of cornea. (A value of 47.2D or more)- I-S value quantifies inferior versus superior corneal dioptric asymmetry (Value 1.4D or more)
KISA percent incorporates the K and I-S values with a measure quantifying the regular and irregular astigmatism into one index
•KISA percentage of >100 - Frank Keratoconus 60-100 - Kerataconus suspect
The Rabinowitz Diagnostic Criteria

• The Orbscan Corneal Topography II system uses the combination of placido and scanning optical slit design to calculate the corneal thickness and posterior surface of the entire cornea.

Kerataconus

Treatment Modalities

•The patient’s refractive error can often be successfully managed with spectacle in the early stages
•However Contact lens provides better visual acuity than that obtained by spectacles
Spectacle Correction

•Traditionally lenses for keratoconus have been hard or rigid gas permeable contact lens variety
•For most of patients three point touch contact lens is ideal
•The most accurate way to fit keratoconic patients is to place a diagnostic lens on the eye, check the fit and then modify the fit*
Contact Lenses

• In mild to moderate keratoconus the lens diameter selected is usually 7.5-8.5mm- small size facilitates tear exchange and allows a steeper fit to accommodate the cone
•Central nipple cones do best with small diameter lenses
•When the cone is displaced peripherally as with oval or globus cones fitting a larger flatter lens may be required

•Soper lenses : One of best known lens with bicurve design with a deep central curve to accommodate the steep central cone and a flat peripheral curve to align with the peripheral cornea
•Hybrid lenses : Lenses with rigid gas permeable optic zone surrounded by a soft skirt to ensure comfortable fit
• “Piggyback” lenses : Gas permeable rigid lenses are worn over soft lenses
Especially designed contact lense

• The Rose K lenses : Unique keratoconus lens design with nor complex computer generated peripheral curves based on precollected data
• Scleral lenses : Sometimes prescribed for cases of advanced or very irregular keratoconus
• Refractive surgeries : LASIK or Photorefractive keratectomy is contraindicated-Phototherapeutic keratectomy can be done in selected cases to reduce steepness of cone in patients who have become Contact lens intolerant- The resultant flattening of the cone makes contact lens fitting easier

•A recent surgical alternative to corneal transplant is the insertion of intrastromal ring segments (ICRS)
•These implants are designed to be placed at a depth approximately 2/3rd the corneal thickness*
•They act by shortening the corneal arc length and have a net effect of flattening the central cornea*
• ICRS have be indicated for contact lens intolerant patients with early keratoconus who have minimal central stromal scarring
Intrastromal Corneal Ring Segments

INTACS
Ferrara rings
ICRS

Mechanism of Action
Ste
epest
M
eri
dia
n

•This treatment have been shown to slow down or arrest the progression of keratoconus and in some cases reverse it
•The need to keratoplasty thus might be significantly reduced
•Clinical trials are continuing and the technique is definitely showing promise in treating early cases
Corneal Collagen Cross linking with Riboflavin

•Corneal stroma soaked in riboflavin 0.1% eyedrops in 20% dextran and activated by approximately 30mins illumination with UV-A light
Treatment procedure


•Approximately 10% of patients will progress to a point- where visual correction is not possible- thinning becomes excessive - scarring as a result of contact lens wear
Corneal Transplant

Penetrating keratoplasty

Lamellar Keratoplasy/Deep Anterior Lamellar Keratoplasty(DALK)