Keratoconus Problem? … NO PROBLEM! booklet.pdf · Keratoconus Problem? … NO PROBLEM! All you...
26
Keratoconus Problem? … NO PROBLEM! All you wanted to know about keratoconus … and more.
Transcript of Keratoconus Problem? … NO PROBLEM! booklet.pdf · Keratoconus Problem? … NO PROBLEM! All you...

Keratoconus
Problem?
… NO
PROBLEM!
All you wanted to know about keratoconus … and more.

2
• Introduction• Corneal Collagen Cross-linking• Prevalence of Keratoconus in the Population• Etiology of Keratoconus• Genetics in Keratoconus• The Environment and Keratoconus• Associated Conditions• Hallmarks of Keratoconus• Types of Keratoconus• Puberty-Onset Keratoconus• Late-Onset Keratoconus• Keratoconus Fruste• Use of Corneal Topography for Assessment of Keratoconus• Clinical Management of Keratoconus• Spectacle Correction in Keratoconus• Wave Contact Lenses• Contact Lens Designs for Early Keratoconus• Surgical Treatments for Corneal Ectasia• Penetrating Keratoplasty• Lamellar Graft• Intrastromal Rings/Intacs-Ferrara Rings• Laser Surgery for Keratoconus
INDEX

3
IntroductionKeratoconus, also called conical cornea,results in the cornea changing from dome-shaped to cone-shaped through theprogressive thinning of the cornea.Because the cornea is the part of the eyethat refracts most of the light entering, thechange of its shape prevents incominglight from being focused properly,ultimately distorting vision. In addition,vision may be impaired as a result ofswelling and scarring of tissue.Keratoconus is a slow-developingdisorder that almost always affects botheyes, though each eye may be affecteddifferently. It is also almost fortuitous thatusually one eye is much more affectedthan the other. This allows many patientsto carry on with their normal activities.However, it is also responsible for delayeddiagnosis in many cases.
UNDERSTANDING KERATOCONUS
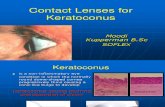
Keratoconus is a condition of obscureetiology that is characterized by thethinning and steepening of the centraland/or para-central cornea. The conditionusually occurs in the second or thirddecade of life resulting in a moderate tomarked decrease in visual acuitysecondary to irregular astigmatism andcorneal scarring. (Figure 1.)Keratoconus most often occurs bilaterally,however there is often asymmetry withone eye affected more than the other andgenerally the first eye to develop thecondition has a more marked progression.(Figure 2.)
Figure1: Corneal ectasia in keratoconus
Figure 2. Bilateral keratoconus with one eye(right eye) affected more than the other.This differential rate of progression maybe an important consideration whencounseling patients on the progression ofthe condition. Cases of unilateralkeratoconus are rare but can occasionallybe seen in clinical practice.The clinical management of keratoconusvaries depending on the severity of the

4
condition and can range from non-surgicaloptions such as glasses and contactlenses to surgical interventions includingIntacs, partial grafts, and penetratingkeratoplasty once Keratoconus progress’sto an advanced state. This is why an earlycross-linking treatment is advised as earlyas possible.
Keratoconus HistoryEarly reference to keratoconus was madeby Mauchart in 1748 and by Taylor in1766, but the condition was firstadequately described and distinguishedfrom other corneal ectasia by Nottinghamin 1854.As mentioned by Nottingham in hisclassical treatise on keratoconus writtenin 1854 (yes, that is how long we haveknown about keratoconus) “... a candle,when looked at, appears like a number oflights, confusedly running into oneanother”At that time, the treatment of keratoconusconsisted of cauterizing the conical areawith silver nitrate and the instillation ofmiotics accompanied by a pressuredressing.In the early months of 1888, a Frenchophthalmologist, Eugene Kalt, began workon a crude glass shell designed to“compress the steep conical apex therebycorrecting the condition.” This was the firstknown application of a contact lens for thecorrection of keratoconus. (Figure 3.)
Figure 3. Eugene Kalt, MD, first to proposethe use of a contact lens for keratoconus.
Prevalence of Keratoconus in thePopulationKeratoconus occurs with approximatelyequal gender distribution in every regionand every ethnicity throughout the world.Many studies have been conducted toestimate the incidence and prevalence ofthe condition, and, although the incidencevaries somewhat from to country tocountry, a 1986 population-based studyin the US indicated that approximately 5in 10,000 people have keratoconus.Studies from various other areas of theworld have reported prevalence from ahigh of 1 in 250 to 1 in 2000 population.This Prevalence figure will increasebecause of the use of modern diagnosticequipment which is becoming morereadily available and cheaper these days.It is anecdotally felt by some, that theprevalence in India would vary from 1 in2000 to 1 in 4000 population.An early onset and increased severity ofkeratoconus was found in recent studiesin ethnic (Asian) groups. This may berelated to a combination of genetic and/

5
or environmental factors. However it alsoindicates that in non-western countries theprevalence of Keratoconus could be much(4.4 times) higher than what it’s thoughtto be.If all the prevalence of corneal thinningdisorders closely related to Keratoconuswas all added together then this figurewould be high from the outset.Keratoconus is routinely mis-diagnosed(it’s confused as “normal” Astigmatismregularly) and under diagnosed. Here aresome of the categories where figures arelost.Corneal Ectasia (keratoglobus, pellucidmarginal corneal degeneration, Terrien’smarginal degeneration, Posterior Ectasia,forme fruste keratoconus)Corneal Dystrophies (epithelialbasement membrane dystrophy andstromal dystrophies such as granular,lattice, or macular dystrophy)Corneal Warpage secondary to rigidcontact lens wear or irregular astigmatism.Many people in the general populationwear glasses without knowing it is due tothem having keratoconus or even theoptician who prescribed them the glassesknowing this. Mild forms of Keratoconusare common, and it is only in the advancedstages of the disorder a referral to an eyehospital is made for diagnoses.Therefore, only advanced stages ofKeratoconus are noted for statisticalpurposes generally. This is when it is toolate and the Keratoconus has becomeproblematic. We at Clear Vision EyeCenter, Mumbai, India strongly feel that
the improved early detection ofKeratoconus is vital, because with theadvent of the cross-linking treatmentmilder forms of Keratoconus can betreated before they get advanced andproblematic. Milder keratoconus patientsare the ones who can be helped the most,to stay out of the medical loop, andtherefore an earlier intervention with theCrosslinking treatment is warranted as it’sbeen proved to be a preventativemeasure.
Primary Corneal EctasiaThis is a new term being used to describeKeratoconus and all the other forms ofcorneal thinning disorders of the cornea.Keratoconus is the most common out ofall of them.The thinning characteristic of all thecorneal thinning disorders is the commonfeature between them, and it’s the thinningaspect which needs to be addressed byusing this term to describe it.
Secondary Corneal Ectasia(Also called Keratectasia or IatrogenicKeratectasia)This is when excessive thinning of the eyewall can cause the shape and focusingpower of the eye to become unstable afterLaser eye treatment as an uncommoncomplication arising out it.Careful screening to detect pre-existingcorneal abnormalities (Keratoconus),conservative limits on treatment (notremoving too much corneal tissue), andpre-operative measurement of cornealthickness all combine to limit this risk.

6
However, to date there is no foolproofmethod to detect potential cases prior tothe Laser Surgery.Every thing which has been discussedabove about the prevalence ofKeratoconus shows that the prevalenceof Keratoconus is much more commonthan previously thought, and with theincreasing use of modern diagnosticequipment it is even higher. The first thingan eye care specialist looks at is the frontsurface of the eye of a patient, whichneeds to be checked with the latestmodern diagnostic testing equipmentthese days. Many of the Primary CornealEctasia can be picked up sooner andtreated earlier, which would not have beenpicked-up other-wise.In most circumstances most practicesdon’t even have access to a cornealtopography machine, which should be astandard feature of any modernpractice. The front surface of the eye isvery important, because the cornea isresponsible for most of the eye’s totalfocusing power; and also it’s where mostmedical intervention are done to the eyeto treat and correct the visual errors thata patients has. Therefore it is imperative,that a practice modernizes to have thelatest corneal diagnostic test equipmentto-hand.
Etiology of KeratoconusThere has always been speculation as tothe cause of keratoconus, but during thepast 10 years our scientific knowledge ofthe condition has steadily increased.
Although we now have a much betterunderstanding of the cellular andmolecular changes that occur in thiscondition, keratoconus remains acondition of unknown etiology.Recent research conducted by StevenWilson, MD, at the University ofWashington suggests that keratoconussomehow accelerates the process ofkeratocyte apoptosis, which is theprogrammed death of corneal cells thatoccurs following injury. Minor externaltraumas, such as eye rubbing, poorly fittedcontact lenses, and ocular allergies canrelease cytokines from the epithelium thatstimulate keratocyte apoptosis (theearliest observable stromal response toan epithelial injury).Although keratocyte apoptosis is virtuallynever detectable in the absence ofepithelial injury in normal patients, a highpercentage of keratoconus patients showevidence of such cell death. This typicallytakes place first in the anterior stroma andis manifested by breaks in Bowman’s layer(Figure 4) and later as stromal thinning(Figure 5). Wilson has also suggested thatgenetics may play a role in the etiology ofkeratoconus, in that some patients mayhave a genetic predisposition to chronickeratocyte apoptosis.

7
Genetics in KeratoconusOne of the strongest arguments for agenetic component in keratoconusetiology is that the condition can run infamilies. Although most patientsdiagnosed with keratoconus report nopositive family history, the likelihood thatkeratoconus will be found in one or moremember of the immediate family is 3.4%,which is 15 to 70 times higher than thegeneral population rate. In addition,keratoconus has been reported inidentical twins and in two or moregenerations of many families.The advent of computerized cornealmapping techniques has made earlierdetection of sub-clinical, and/or slowlyprogressive forms of the condition moreprecise. Therefore, it is suspected thatfamilial prevalence rates will most likelyincrease. Using corneal topographicalfindings, in 1990 Rabinowitz and hiscolleagues from UCLA, California,showed that 50% of randomly selectedfamily members of keratoconus patientsdisplayed subtle topographicalabnormalities somewhat suspect ofkeratoconus.Studies to identify the association ofkeratoconus with various chromosomeshave been performed. Reports on a smallnumber of families with keratoconus showa connection between keratoconus anddefects on chromosomes 21, 17, and 13.However, at this time it is unknown exactlywhat specific parts of these chromosomesare defective or how the defects mightcause keratoconus.
It has been suggested that keratoconuscorneas may have increased enzymeactivities and decreased levels of enzymeinhibitors. This combination results in theproduction of toxic by-products that bringabout a cascade of events throughout thecornea, resulting in corneal thinning andscarring.Two chief mechanisms for thedevelopment of keratoconus have beenput forward. One proposes that ectasia isclosely associated with tissue degradationor reduced maintenance, whereas theother suggests that it is due to slippagebetween collagen fibrils, with no overalltissue loss.
Figure 4. Breaks in Bowman’s layer.
Figure 5. Central versus mid-peripheralthickness changes in advanced keratoconus.

8
Future investigations will most likelyconclude that more than one gene isassociated with the diverse clinicalpresentations seen in keratoconus. Thisis based on the fact that there isconsiderable variation among individualswith keratoconus and so multiple genesare most likely involved. For example,keratoconus manifests in many forms anddegrees of severity:• It can be unilateral or bilateral,• It can affect the central or mid-
peripheral cornea,• It can be mild or severe,• It can start in childhood or later in
life, and• It can occur in more than one family
member or in one individual only.
The Environment and KeratoconusAlthough it is generally believed thatkeratoconus has a genetic component,there are increasing data that suggest theenvironment might also play a role in thedevelopment of the condition.Research has discovered that corneaswith keratoconus have been exposed toa number of factors that can producereactive oxygen species (i.e., freeradicals). These include ultraviolet light,atopy, mechanical eye rubbing, and poorlyfitted contact lenses. They propose thatsusceptible corneas exhibit an inability toprocess reactive oxygen species becausethey lack the necessary protectiveenzymes (e.g., ALDH3 and superoxidedismutase). The reactive oxygen speciesresult in an accumulation of toxic by-
products such as MDA and peroxynitritesthat can damage corneal proteins andtrigger a cascade of events that disrupt thecornea’s cellular structure and function.This can result in corneal thinning, scarring,and apoptosis. (Figure 6.)
Figure 6. Reactive oxygen species within thekeratoconus cornea result in an accumulationof toxic by-products that can trigger corneathinning, scarring, and apoptosis.
If this theory is valid, it might be prudentfor keratoconus patients to minimize thefactors that can cause reactive oxygenspecies to be formed. It might be helpfulfor patients to do the following:• Reduce exposure to ultraviolet (UV)
light by wearing UV protectingsunglasses outdoors.
• Avoid excessive mechanical traumasuch as vigorous eye rubbing andpoorly fitting contact lenses.
• Manage atopy/allergies throughenvironmental and/or pharmacologicintervention.
• Use preservative-free artificial tearsand lens care products that areefficacious compatible with thepatient’s ocular surface.
Although the environmental damagetheory is interesting, at this time there is

9
no conclusive evidence to support the factthat changes in diet, environment, oremotional state can influence the eventualcourse of the disease. This is supportedby the fact that keratoconus occursthroughout the world in a wide range ofgeographic, social, and dietary conditions.
Associated ConditionsKeratoconus has been associated with anumber of systemic conditions includingDown’s syndrome (trisomy ofchromosome 21). A number of authorshave reported that the incidence ofkeratoconus in Down’s syndrome isbetween 5.5% and 15%, which isconsiderably higher that the incidence ofapproximately 5 per 10,000 (0.05%) citedfor the general population. Occasionally,keratoconus is also seen in individualswith connective tissue disorders such asOsteogenesis Imperfecta, Ehlers-DanlosSyndrome, and joint hypermobility.
Hallmarks of KeratoconusAlthough the etiology of keratoconusremains somewhat obscure, its clinicalmanifestations have been welldocumented. Some on the majorhallmarks of keratoconus include:• A decline in visual acuity (usually
greater in one eye than the other).• A distorted retinoscopy reflex in which
there is rapid movement of the light inthe periphery and slow movement inthe center of the pupil. The reflexappears to spin or swirl around a pointcorresponding to the apex of the cone.
• Distortion of or an inability tosuperimpose the bottom rightkeratometry mire.
• Frequent changes in spectaclecylinder power and axis.
• Increased myopia.• Squeezing of the eyelids to create a
pinhole effect.• The appearance of halos or starbursts
around light during nighttime viewing.• Associated atopic disease.
Types of KeratoconusIn clinical practice, three distinct forms ofkeratoconus have been identified, eachwith a unique clinical presentation.Differentiating between the three formscan be helpful in counseling patientsabout what to expect regarding eventualprogression of the disease. However, theclinical classification of keratoconusshould be viewed as only a general guide.It is important to communicate to thepatient that the condition can be extremelyunpredictable and that its ultimate coursecan only be determined with time.
Puberty-Onset KeratoconusPuberty-onset keratoconus is by far themost common form of the condition, and,as its name indicates, it begins in earlyadolescence at about age 12 to16 years.This is shifting to younger age groups. Inour experience on the Indian sub-continent, younger age at onset is muchmore common compared to the westerncountries. In fact various researchers fromIndia and Middle East Asia havedocumented that the age of onset is earlier

10
and the progression to severe disease isseen more often in the Asian-Indianpopulation.The condition is usually bilateral with oneeye affected more than the other.Following its onset, there is often adramatic progression of the condition forthe next 8 to 10 years. This is typicallyfollowed by a period in which the conditionseems to stabilize. Clinical experience hasshown that the earlier in life thekeratoconus occurs, the more severe thecondition will be. Therefore, a 12 year old,exhibiting the optical and topographicalmanifestations of early keratoconus ismore likely to have a more severe form ofthe condition than an individual that showssimilar findings in their late 20’s.
Late-Onset KeratoconusIn late-onset keratoconus, the earliestsigns and symptoms begin in the late 20’sor early 30’s. Both eyes are frequentlyaffected to a similar degree, with little orno asymmetry. This is often a more benignform of the condition, and, unlike pubertyonset keratoconus, its progression issignificantly less severe, rarely requiringsurgical intervention in the form of acorneal transplant.
Keratoconus FrusteThe third form of keratoconus is called“form fruste” and was first described byAmsler in 1937. It is essentially anextremely mild form of keratoconus thatcan occur at anytime throughout life. Thecondition manifests as a central or para-central zone of irregular astigmatism of
unknown etiology. The most strikinghallmark of form fruste keratoconus is itslack of progression with the conditionstaying stable throughout the patient’s life.
Clinical Management ofKeratoconus
Corneal Collagen Cross-linkingTreatmentCorneal collagen cross-linking induced bytreatment of impregnating Riboflavin (B2)in to the cornea and exposure toultraviolet-A light is a safe and effective,minimally invasive procedure both toreduce disease progression, increase thestrength of the cornea and to improveupon the cornea’s optical properties ineyes with early keratoconus.
Figure 7. CXL
As long as keratoconus is diagnosed earlyenough - a stabilization of clinical findingsand visual acuity can be achieved withouta need for a corneal transplant or furtherprogression.It is the first treatment for Keratoconus. Ittreats the cause not the symptoms,

11
therefore the number of penetratingkeratoplasty surgeries can be significantlyreduced in the future. The treatment isrelatively easy and low in costs and isavailable through out the world. Avoidingadvanced Keratoconus because of theproblems it causes is what the aim is withthis treatment.The early use of the cross-linking treatmentmust be advised to the patient as an optionfor them to halt any further progressiononce Keratoconus has been diagnosed. Sothat they have a chance to avoid advancedKeratoconus and all the problems that itcan cause with vision correction.
Spectacle Correction in KeratoconusIn the early stages of keratoconus, thepatient’s refractive error can often besuccessfully managed with spectaclelenses. It is important to communicate tothe patient that there is no evidence tosupport the theory that early contact lensintervention is of therapeutic benefit inpreventing or lessoning the progressionof the disease. However, wearing contactlenses typically provides the patient withbetter visual acuity than can be obtainedwith glasses by neutralizing the regularand irregular refractive errors induced bythe condition. As keratoconus progresses,spectacle lenses often fail to provideadequate visual acuity, especially at night.This can be further complicated by the factthat the patient’s glasses prescription maychange frequently and can be limited bythe degree of myopia and astigmatismthat must be corrected. Also, keratoconus
is often asymmetric therefore fullspectacle correction may be intolerablebecause of anisometropia andanisokonia. However, despite theselimitations, spectacles can often providesurprisingly good visual results in the earlystages of the condition.
Wave Contact LensesWave Contact Lenses are Contact Lenseswhich are custom designed from yourcorneal “fingerprint”, its a new technologywhich is being used to aid for a better fitand visual accuracy. Corneal Topographyequipment digitally maps your cornea withthousands of numbers. The doctor usesthe map data and Wave-front specialdesign software to create a custom lensthat follows almost every tiny shape onyour cornea. Custom designed lensesdiffer greatly from plain “mass produced”lenses. The doctor using Wavefronttechnology for contact lenses will specifythe lens diameter and thickness forcomfort and adjust the position of theoptics for best visual performance. In allthere are 26 different adjustments, offeringinfinite design possibilities.Keratoconus Post Refractive Patient’s arethe most challenging to fit with off-theshelve contact lenses and most in needof Wave-front contact lenses custom“match the cornea” design philosophy.
Contact Lens Designs for EarlyKeratoconusThe successful fitting of contact lenses forkeratoconus requires that three objectivesbe met:

12
• The lens-to-cornea fitting relationshipshould create the least possiblephysical trauma to the cornea.
• The lens should provide stable visualacuity throughout the patient’s entirewearing schedule.
• The lens should provide all daywearing comfort.
Although it may be impossible to meet allof these objectives for every patient, weshould remain focused on utilizing all ofthe modern lens designs and fittingtechniques at our disposal to achieve thebest possible outcomes.Surgical Treatments for Corneal EctasiaSince the 1950’s, penetrating keratoplastyhas been the primary surgical procedurefor treatment of keratoconus. (Figure 8.)
• The contact lenses fail to provideadequate visual acuity due to cornealscarring.
• Sharp bilateral visual acuity is requiredfor recreational or professionalrequirements.
It is important to recognize that certainpatients are perfectly content with 20/50to 20/60 (6/15 to 6/18) visual acuity. Overthe years, these individuals havedeveloped blur interpretation skills thatallow them to function surprisingly well intheir daily endeavors. The major limitingfactor for these individuals is difficultydriving at night. For most surgeons,keratoplasty is not considered untilcontact lens options have beenexhausted.
Surgery involves risks that include:• Graft rejection,• Infection,• Glaucoma,• High post operative regular and/or
irregular astigmatism, and• Steep or flat grafts.Patients should be informed thatkeratoplasty for keratoconus has a successrate of approximately 92% for a cleartransplant on the first surgery and thatoccasionally a second or third transplantmight be needed secondary to post-operative great rejection, infection, or woundhealing complications. Patients should alsobe advised that following keratoplasty,approximately 85% of them will find itnecessary to wear a contact lens to correct
Figure 8. Penetrating keratoplasty fortreatment of keratoconus.
The decision to pursue keratoplasty is onethat must be made by the individualsurgeon and the patient. The factors thatcan influence the decision include:• The patient can no longer tolerate or
be fitted adequately with contactlenses.

13
the surgically-induced regular and irregularastigmatism and anisometropia.
Lamellar GraftA lamellar graft (also known as DALK ora partial graft) replaces part, rather thanall, of the thickness of the cornea. It canbe used instead of a penetrating graft ifthe deeper layers of the cornea arehealthy.
Intrastromal Rings/Intacs, Ferrara, andCornealRing RingsIntacs inserts are 150 degree PMMA ringsegments that are placed in the peripheralstroma of the cornea, typically to correct
horizontally in the cornea at 12 and 6o’clock. Intacs are indicated for contactlens intolerant patients with earlykeratoconus who have minimal centralstromal scarring. (Figure 9.)
Figure 9. Intra-stromal rings for treatment ofkeratoconus.
myopia. However, the technique has alsobeen recently US FDA approved for thetreatment of keratoconus. (Figure 9.)The inserts are designed to be placed ata depth of approximately two-thirds thecorneal thickness and are surgicallyinserted through a small radial incisioninto a trough created within the cornealstroma. The inserts shorten the cornealarc length and have a net effect offlattening the central cornea. The amountof flattening is determined by the insert’sthickness. Rings are available inthicknesses of 0.250, 0.275, 0.300, 0.325and 0.350 mm and are oriented
In theory, the inserts are designed toflatten the central cornea and providereinforcement for the peripheral cornea.The procedure may also decrease thecornea surface irregularity and improvesthe patient’s best-corrected visual acuity.It’s been reported that sometimes usingone segment is sufficient and favorable.Ferrara Rings works in a similar way toIntacs, but there are some differences inwhen they are used, depending on thesize of the flattening that needed and alsothe pupil size of the patient.Ferrara Ring, which like Intacs have ringsegments 150º of arc but have a smallerinner and outer diameter (4.4mm and5.6mm) and are triangular in cross-section. They range in thickness from0.2mm to 0.35mm in 0.05mm increments.Ferrara Rings are approved in Europe forKeratoconus.CornealRing is another modifiedintracorneal ring system. It differs from the
Figure 9. Intacs rings flatten the central corneain keratoconus by an amount proportional tothe thickness of the two 150 degree arcsegments.

14
Intacs and Ferrara Rings in that it has a5mm inner diameter and a fusiform shapethat reduces the stress on the cornealstromal fibers. This is supposed to helpreduce the problems associated with theother two systems.
Laser Surgery for KeratoconusClinicians typically rule out LASIK surgeryfor patients with keratoconus because ofa greater risk for scarring and excessivethinning leading to possible post-LASIKectasia. However, some surgeons havereported success in performing a
smoothing procedure for patients over theage of 40 years with stable keratoconus.Candidates for the procedure are mostoften individuals with mild keratoconuswho are contact lens intolerant andreluctant to pursue corneal transplantsurgery.Studies are now available where thepatients have had a cross linkingprocedure simultaneous to the surfaceLaser surgery to reduce numbers orsubsequently after the cross linkingprocedure.

15
What part of the eye is affected inkeratoconus?
The cornea is the clear, transparent frontcovering which admits light and begins the
refractive process. It is this clear convexcornea which bends (refracts) a ray of lightand slows it down. It also shrinks the lightto a manageable size (a little smaller thana one rupee coin). It is this front coveringof the eye that is affected in keratoconus.
What is keratoconus?
Keratoconus is a degenerative non-inflammatory disorder of the eye in whichstructural changes within the corneacause it to thin and change to a moreconical shape than its normal gradualcurve. It derives the name from (kerato –cornea and konus – cone)
How frequent is this disease?
Keratoconus is the most commondegenerative disease of the cornea. Theincidence is believed to vary from 1 in
2000 to 1 in 1, 00,000 in different regionsof the world. Though there are no exactfigures for our country, most expertsbelieve it to range between 1 in 2000 to 1in 5000 population. You are not the onlyone affected by this problem. Clear VisionEye Center itself handles hundreds ofsuch eyes every year.
When does it usually present?
Keratoconus is usually seen from earlyteens to the late twenties. It can presentas early as eleven to twelve years of age.It may progress and achieve its most severestate in the age group of twenties or thirties.
Does keratoconus affect both eyes?
Keratoconus is normally seen affectingboth eyes, although the distortion isusually asymmetric and is rarelycompletely identical in both corneas.Unilateral cases tend to be uncommon,and may in fact be very rare if a very mildcondition in the better eye is simply belowthe limit of clinical detection. It is commonfor keratoconus to be diagnosed first inone eye and not until later in the other.
What causes keratoconus?
The causes of keratoconus are stillunknown despite our long experience withit. There has been no shortage ofspeculation or study and numeroustheories have been proposed.
UNDERSTANDING KERATOCONUS

16
One scientific view is that keratoconus isdevelopmental (i.e., genetic) in origin. Thissuggests that it is the consequence of anabnormality of growth, essentially acongenital defect. Another view is that KCrepresents a degenerative condition. Stilla third view is that KC is secondary tosome disease process. A less widely heldhypothesis suggests that the endocrinesystem may be involved. This idea gainedcredence from the usual appearance ofthe disease because it is generally firstdetected at puberty.
Heredity influences in KC are suggestedby studies that show that approximately13% of patients have other familymembers with the disease.
What are the problems in my visionthat suggest keratoconus?
People with early keratoconus typicallynotice a minor blurring of their vision andcome to their clinician seeking correctivelenses for reading or driving.
At early stages, the symptoms ofkeratoconus may be no different fromthose of any other refractive defect of theeye. As the disease progresses, visiondeteriorates, sometimes rapidly.
Vision becomes impaired at all distances,and night vision is often quite poor. Someindividuals have vision in one eye that ismarkedly worse than that in the other eye.
Some develop photophobia (sensitivity tobright light), eye strain from squinting inorder to read, or itching in the eye, but
there is normally little or no sensation ofpain.
As mentioned by Nottingham in hisclassical treatise on keratoconus writtenin 1854 (yes, that is how long we haveknown about keratoconus) “... a candle,when looked at, appears like a number oflights, confusedly running into oneanother” — Nottingham
What are the most common “sights”seen in keratoconus?
In its earliest stages, keratoconus causesslight blurring and distortion of vision andincreased sensitivity to glare and light.These symptoms usually first appear inthe late teens and early twenties.
The classic symptom of slightly more
advanced keratoconus is the perception
of multiple ‘ghost’ images, known as
monocular polyopia. The above image is
an artist’s rendition of the same effect
(picture used in line with GNU free
documentation license). In keratoconus,
surface thinning can create multiple
optical zones that individually focus thesame image to different areas of the

17
retina, thus creating the additionalperceived images. This effect is mostclearly seen with a high contrast field,such as a point of light on a darkbackground. Instead of seeing just onepoint, a person with keratoconus seesmany images of the point, spread out in achaotic pattern. This pattern does nottypically change from day to day, but overtime it often takes on new forms. Patientsalso commonly notice streaking andflaring distortion around light sources.
What is difference betweenkeratoconus and “common”astigmatism and what do the numbersmean?
Astigmatism is a common condition wherethe curvature of one or more of the opticalsurfaces of the eye (the cornea and lenssurfaces) are more “round” in onedirection than the other. In “regular”astigmatism the maximum and minimumpowers are aligned at 90 degrees to eachother while in “irregular” astigmatism theydo not align. An egg is a good example of
a surface with “regular astigmatism”.
Keratoconus is a degenerative condition
where the cornea thins in affected areas.
This can lead to astigmatism - often
regular at first but becoming increasingly
irregular as the disease progresses.
How will my Keratoconus specialistdiagnose my problem?
There are a variety of tests that will be
used by your eye care practitioner. They
range from simple vision test, slit lamp
examination, retinoscopy, placido disk
evaluation, and the most recent and now
the very widely used corneal topography.
The key to early diagnosis still remains
high degree of suspicion by the eye care
practitioner.
An advanced case is usually readily
apparent to the examiner, and can provide
for an unambiguous diagnosis prior to
more specialized testing. It is the
diagnosis of the early that remains a
challenge to the specialist.

18
What is the future of patients with thisproblem?
Keratoconus does not lead toblindness.
It is amazing that most patients with
keratoconus managed by us believe that
they will go blind sometime in their life.
This occurs simply because they have
seen their vision get worse and worse so
they believe that the eye condition will
continue to degrade to the point that
nothing can be done to recover the vision.
Some people have seen a number of eye
care practitioners over time and no one
has been able to fit them with contact
lenses or glasses and they are too scared
to pursue corneal transplant surgery. They
then try to function with poor vision and
believe it is only a matter of time before
they will see nothing at all.
The reality is that no one goes blind from
keratoconus.
There are currently multiple options before
corneal Transplantation may be required.
Even for cornea transplantation the
success rates are in excess of 95% in
good hands.
How rapidly will the problemprogress?
When diagnosed in the early stages, KCmay be corrected with glasses which mayrequire frequent changes in theastigmatism prescription. The continuedthinning of the cornea usually progressesslowly for 5 to 10 years and then tends tostop. Occasionally, it is rapidly progressive.
Both you and your eye care specialistwould like to know how your case is goingto behave. However, the rate ofprogression for a particular patient isimpossible to predict. Some patientsadvance rapidly for six months to a yearand then stop progressing, with no furtherchange. Often there are periods of severalmonths with significant changes followedby months or years of no change; this maythen be followed by another period ofrapid change. In the CLEK Study (one ofthe largest studies on keratoconus in theworld with more than a thousand patientsstudied for more than 7 years), the slopeof the change of flat K was approximately0.20 D diopters per year; over sevenyears; this translated into an expectedsteepening of 1.44 D. Steepening of 3 Dor more in either eye had an incidence
COPING WITH KERATOCONUS

19
of 23%.
In the advanced stage, the patient mayexperience a sudden clouding of vision inone eye that clears over a period of weeksor months. This is called “acute hydrops”and is due to the sudden infusion of fluidinto the stretched cornea. In advancedcases, superficial scars form at the apexof the corneal bulge resulting in morevision impairment.
We can thus say that the course of thedisorder can be quite variable, with somepatients remaining stable for years orindefinitely, while others progress rapidlyor experience occasional exacerbationsover a long and otherwise steady course.Most commonly, keratoconus progressesfor a period of ten to twenty years, beforethe course of the disease generallyceases.
How do other people with this problemmanage?
In my practice over the years, I have foundthat people react differently to the newsthat they have KC. Lack of knowledgeoften creates fear, so I encourage allindividuals to learn all that they can aboutthis condition. It is a good idea to askquestions and discuss your concerns withyour doctor and others who havekeratoconus. This will be both enlighteningand reassuring.
From a medical standpoint, the mostimportant thing you can do is to keep intouch with your eye care practitioner andfollow his/her instructions.
From an emotional and psychologicalstandpoint, it is important to understandthe nature of keratoconus. Do not try tohide the problem. Talking freely about itwith family and friends helps them to besure that they understand it. We at ClearVision Eye Center, usually suggest that afamily member accompany the subjectduring initial discussions.
If at all possible, talk with otherkeratoconus patients. The mutual sharingof common experiences is both rewardingand reassuring. If you need any help withthis please contact your practitioner.Usually practices who deal withkeratoconus regularly will be able to helpyou find another person with this problem.
Help groups are internationally known tobe a good support. However, we atKeratoconus Center of the Clear VisionEye Center are in the process ofencouraging the first such support groupsoon in Mumbai. For further details visitwww.clearvision.org.in
Over the years, we have had manysubjects who have gone on to besuccessful in their chosen fields despitethis disorder. This proves that KC shouldnot stop you from accomplishing yourgoals. People from all walks of life haveexperienced this disorder, including manyindividuals in the entertainment industry,medicine, sports and business.
It has been our observation that patientswho handle their KC problemssuccessfully develop their own coping

20
mechanisms. These include wearingsunglasses for driving, carrying extracontact lenses, and planning ahead forlocal trips.
While it is important that you acceptkeratoconus as a fact in your life andrealize that you have to adapt to it, it isessential for you to understand thatadapting is not surrendering. You controlyour life, keratoconus does not.
How have others before me coped withthis problem?
Tips to cope with this problem aremany, some that I use in my practicein Mumbai are:
Reducing eye rubbing is vital
People that have keratoconus often alsohave allergies. Hay fever, skin allergies,and asthma are common. With theseconditions come itchy eyes. Another groupof people that has keratoconus does notseem to have allergies but have a habitof eye rubbing.
Aggressively rubbing eyes can cause orprogress keratoconus. Therefore it is veryimportant to have strategies to decreasethe urge to rub.
It is felt that rubbing eyes that arepredisposed to keratoconus traumatizesthe cornea causing it to thin and becomedistorted in shape. As discussed before,this distortion in shape then causesdistortion in vision that often cannot becorrected with glasses.
One thing is to know that eye rubbing is aproblem and another is putting a halt to it.
People that get itchy eyes will tell you thatit drives them mad and once they startthey cannot stop until their eyes are redraw. It is this vicious cycle that canprogress keratoconus.
Over the years three strategies haveworked well for our patients:
1. Because allergies contributesignificantly to the urge to rub, it is agood idea to use anti-allergy drops,especially in allergy season.
2. Cold compresses should be usedwhen you feel like you need to rub.The most convenient form of coldcompresses is to purchase a coldpack from the chemist (which is ablue gel in a plastic bag), freeze itand have it ready. When you needto use it wrap it once in a tea toweland then mould it into your eyesockets. You will find relief veryquickly this way. Simply using atowel dipped in ice water is equallyuseful!
3. If you are wearing contact lenses,the solutions that they are stored inare loaded with preservatives whichcan cause itchiness. Rinsing thelenses with preservative freelubricating drops before insertingthem into your eyes will contributeto rubbing your eyes less.
Decreasing eye rubbing cannot beoverstated. Stop rubbing your eyes now!
Maintain a meticulous documentation

21
of your case.
The most important part of keratoconusmanagement is to assess if the problemis stable or progressive in nature. Asmentioned earlier keratoconus does notprogress indefinitely. However, this callsfor proper and periodical maintenance ofyour records to see how things areprogressing. Always ask your practitionerfor your set of records. It is your right. Thisis crucial to decide the kind ofmanagement that a given eye is likely toneed. For example a relatively stable eyecan continue with contact lenses almostindefinitely, a progressive keratoconuseye may need different management. Theidea is preventing your eye from becoming“advanced keratoconus”.
Tips for Selecting Sunglasses :
Many KC patients find that wrap-aroundstyles tend to work best from thestandpoint of comfort, as they not onlyfilter sunlight from directly ahead but alsofrom the sides. Another benefit to wrap-
around glasses is that they also tend tohelp block the wind, making contact lenswear more comfortable outdoors.
• Polarized sunglasses tend to workbest in reducing glare, which oftenhelps significantly improve vision.
• Consider buying more than one pairso that a backup is available in theevent that you misplace yourfavorite pair. Many KC patientspurchase several lower pricedsunglasses to keep at home, work,and other places they might beneeded.
Managing reading and Close-UpVision?
Keratoconus generally results in a highdegree of astigmatism that must becorrected in order to have adequatedistance vision. The problem is that whendistance vision is corrected, close-upvision often suffers, making it difficult toread with a high astigmatism contact lensprescription. An eye doctor or contact lens
fitter will assess close-up vision todetermine the proper magnificationneeded for reading glasses.
Tips for Selecting Reading Glasses
Reading glasses containing an anti-reflective coating are often helpful,especially in situations where a rear lightsource is present, which may reflect offof regular reading glasses.
• If you tend to use a computer duringpart of the day, you should considerreading glasses that have been
Seeing thru a Polaroid glass. look to the leftof the image for sight thru non polarizedsection.

22
designed for computer use. Readingglasses designed for computer useare generally adjusted to be mosteffective at the distance that mostpeople maintain from a computerscreen.
• Don’t settle for the least expensivereading glasses solely based onprice. Higher quality glasses aregenerally more expensive but canprovide much greater comfort andmake reading for extended periodsmuch easier. Higher quality readingglasses will have features such asanti-reflective coatings, better opticalclarity, thinner lenses, and springhinge frames.
• Consider purchasing multiple pairsof reading glasses and keeping themin multiple locations like your car,home, office, etc.
How to use contact lenses in the Indianscenario?
We agree that there are specificchallenges for wearer of RGP contactlenses in our country. One of the keyproblems is that of making sure thatlenses do not fall out easily — or morecorrectly, to keep lenses from getting lostif they do fall out. This can often beaccomplished with sports goggles.Another problem very common to ourcountry is the dusty or windy conditions.Dust can easily get caught under a contactlens, producing a rather painfulexperience until the lens can be removed
and cleaned. For this problem, sunglassescontaining side panels (the kind used bytwo wheeler riders) can be used indaylight condition, while goggles can beused in low-light conditions. This is alsovery useful for people in urban areas whotravel by buses and local trains.
Finally, eye drop products that lubricatethe eyes (a large number are available inthe Indian market – for occasional use anyreputed brand is adequate) can be usedto quickly clear the lens while it is still inthe eye so that it does not need to beremoved in the event that dust becomestrapped underneath.
Treatment options for keratoconus
There are currently multiple options beforecorneal transplantation might be required.They range from:
a. Glasses
b. Soft contact lenses
c. Rigid gas permeable contact lenses(when fitted properly this is the mostsuccessful option).
d. Rigid gas permeable lensespiggybacked on soft disposablecontact lenses
e. Mini-scleral contact lenses
f. Corneal Cross Linking with Riboflavin(C3R)
g. Intracorneal Ring implantation(Corneal Ring)
h. Re-prescribing glasses, soft contactlenses or rigid gas permeable contactlenses after Corneal ring implantation/corneal cross linking with riboflavin.

23
Rigid Gas Permeable (RGP) contactlenses are often the treatment of choicefor moderate to severe KC. The hardsurface of the lenses provides the propercurvature for light to enter the eye andfocus on the retina, while the gaspermeable nature provides sufficientoxygen for the cornea. Additionally, anumber of specialized contact lensesdeveloped specifically for keratoconus arecurrently on the market including: FlexiK,Rose-K, and others. These specializedlenses use computer-modeling to producea lens in which the inside curvature isspecially vaulted to fit over the cornealcone, while still providing an opticallyefficient curvature on the outside of thelens. The contact lens fitter can thenfurther customize the design of the lensfor a particular patient by adjusting size,rim design, prescription, and the degreeof curvature.
Scleral Lenses
Scleral lenses provide the next level ofcontact lens options for keratoconus asthey are much larger and actually fit overthe sclera (white portion) of the eye. Thelenses tend to be more comfortable for
Contact Lenses
patients with severe KC or with sensitivityto smaller RGP lenses. This revolutionarytechnology has helped some patients at
Keratoconus Center of Clear Vision EyeCenter, delay corneal surgery for up to10 years.
Corneal Collagen Cross Linking withRiboflavin (C3R)
C3-R has been proven to strengthen theweak corneal structure.This methodworks by increasing collagen crosslinking, which arethe natural anchorswithin the cornea. These anchors areresponsible for preventing the cornea frombulging out and becoming steep andirregular, consequence of advancedkeratoconus.
Dr Agrawal has successfully performedcorneal cross linking on a number ofpatients from across the country and

24
abroad. He says, “Corneal Cross Linkingis the first real treatment for mykeratoconus patients. The achievement ofstabilization is a dramatic event in the lifeof these patients with a disease that isotherwise progressive and affects botheyes.”
The 30-minute non-invasive C3-Rtreatment is performed in the doctor’soffice. During the treatment, custom-maderiboflavin eye drops are applied to thecornea, which is then activated byultraviolet light. This amazingly simpleprocess has been shown in laboratory andclinical studies to increase the amount ofcollagen cross-linking in the cornea andstrengthen the cornea. In publishedEuropean studies, such treatments wereproven safe and effective in patients(more details on www.clearvision.org.in )
Intracorneal Rings (ICR)
These consist of two small half-ringswhich are implanted on either side of the
cornea. The idea is that the spring actionof the implant helps to reshape the corneato compensate for the bulge in the middle.Since Intracorneal rings are a more
invasive approach than contact lenses,they are generally suggested for patientswho are no longer able to see well withcontact lenses or who are no longer ableto tolerate contacts due to discomfort. Thistechnique has been in use since a decadeand has helped several patients return tocontact lenses.
Cornea TransplantationCorneal TransplantFor patients whose KC has becomesevere to the point of no longer being able
to see well with contacts or implants,corneal transplantation is generally theultimate treatment. In a transplant theweakened central portion of the patient’scornea is removed and the donor corneais stitched into place. Corneal transplantsare often the most successful type oftransplant surgery. Corneal trans-plantation is among the most successfulof organ transplant surgeries. Accordingto the literature, over 90% of the cornealgrafts are successful with some studiesreporting 97% to 99% success rates at 5and 10 years. Transplantation does not

25
provide a complete solution, however, asa significant number of transplant patientswill require RGP contacts after surgery.In a small number of cases, keratoconushas been found to occur in the newlytransplanted cornea.Even in cornealtransplantation there are a number of
modern adaptations, offered at ClearVision Eye Center, like deep lamellarcorneal (keratoplasty) transplantation(DALK) that make the surgical resultsmore predictable and better than everbefore. ( more details available onwww.clearvision.org.in )
- Dr.Vinay Agrawal
MS; DNB Cornea Fellow (LVPEI, India) Cornea Fellow (Univ. of Rochester, USA)Clear Vision Eye Center, 1A, Ashoka, 15, S.V.Road, Opp. Vodafone Gallery
Santacruz (W), Mumbai 400054, India
For Private Circulation OnlyThis material is intended to be purely informational in nature.
It represents the information available currently from a number of sources.It does not intend or purport to replace advice given by a qualified medical practitioner.
Clear Vision and the author disclaims all or any liability to any persons whatsoever.Expert Eye Care advice is recommended prior to any inference on the basis of this book.

26
Glossary