JMA—President’s Speech JMA Policies Research and … · JMAJ, May/June 2008 — Vol. 51, No. 3...
80
JMA—President’s Speech Policy Address Yoshihito KARASAWA ...................................................................................................................................... 141 JMA Policies Guidelines on End-of-Life Care Japan Medical Association ................................................................................................................................... 143 Research and Reviews Construction of Modules for International Cooperation Method in School Health —Technical cooperation in school health education in Thailand and Myanmar— Seiji OHSAWA ...................................................................................................................................................... 149 Recent Issues in Administrative Measures for School Health Education Shusho OKADA .................................................................................................................................................... 159 School Crisis and Mental Care—The crisis response team (CRT) Michihide KAWANO ........................................................................................................................................... 164 Present State and Issues of Workplace Mental Health Satoru SHIMA ....................................................................................................................................................... 169 Japanese Encephalitis Vaccine Chiaki MIYAZAKI ............................................................................................................................................... 175 Current Status of Vaccination in Japan and the World: A pediatrician’s point of view Hiroshi WATANABE .......................................................................................................................................... 181 Perspective on Current Vaccination Policy in Japan Taro TSUKAHARA ............................................................................................................................................. 186 Combined Measles and Rubella (MR) Vaccine Introduced in Japan Nobuhiko OKABE ................................................................................................................................................ 191 From the Japanese Association of Medical Sciences Hypertension Research in Japan and the Japanese Society of Hypertension Hiroaki MATSUOKA .......................................................................................................................................... 197 Recent Advances in Electronic Endoscopes: Image-enhanced endoscopy Hisao TAJIRI, Hirohumi NIWA ........................................................................................................................ 199 Vol. 51 No. 3 May-June 2008
Transcript of JMA—President’s Speech JMA Policies Research and … · JMAJ, May/June 2008 — Vol. 51, No. 3...

JMA—President’s Speech
Policy Address
Yoshihito KARASAWA ...................................................................................................................................... 141
JMA Policies
Guidelines on End-of-Life Care
Japan Medical Association ................................................................................................................................... 143
Research and Reviews
Construction of Modules for International Cooperation Method in School Health—Technical cooperation in school health education in Thailand and Myanmar—
Seiji OHSAWA ...................................................................................................................................................... 149
Recent Issues in Administrative Measures for School Health Education
Shusho OKADA .................................................................................................................................................... 159
School Crisis and Mental Care—The crisis response team (CRT)
Michihide KAWANO ........................................................................................................................................... 164
Present State and Issues of Workplace Mental Health
Satoru SHIMA ....................................................................................................................................................... 169
Japanese Encephalitis Vaccine
Chiaki MIYAZAKI ............................................................................................................................................... 175
Current Status of Vaccination in Japan and the World: A pediatrician’s point of view
Hiroshi WATANABE .......................................................................................................................................... 181
Perspective on Current Vaccination Policy in Japan
Taro TSUKAHARA ............................................................................................................................................. 186
Combined Measles and Rubella (MR) Vaccine Introduced in Japan
Nobuhiko OKABE ................................................................................................................................................ 191
From the Japanese Association of Medical Sciences
Hypertension Research in Japan and the Japanese Society of Hypertension
Hiroaki MATSUOKA .......................................................................................................................................... 197
Recent Advances in Electronic Endoscopes: Image-enhanced endoscopy
Hisao TAJIRI, Hirohumi NIWA ........................................................................................................................ 199
Vol. 51 No. 3 May-June 2008
Contents
Local Medical Associations in Japan
The Medical Association Needs the Power from Hospital-based Physicians andHospital-based Physicians Also Need the Power from the Medical Association
Norio TAKEDA .................................................................................................................................................... 204
Activities of the Kanagawa Prefecture Medical Association Focusing onIts Academic Area
Isao YAMAMOTO ............................................................................................................................................... 207
Recent Activities of Hiroshima Prefectural Medical Association
Shizuteru USUI ...................................................................................................................................................... 209
International Medical Community
Promoting Medicine, Supporting Doctors: The BMA in action
Vivienne NATHANSON ..................................................................................................................................... 212
Essay
Eulogy for Dr. André WynenThe man who rescued the WMA from the threat of collapse and establishedthe basis for the Declaration of Helsinki
Tatsuo KUROYANAGI ...................................................................................................................................... 215
From the Editor’s DeskMasami ISHII ......................................................................................................................................................... 218

141JMAJ, May/June 2008 — Vol. 51, No. 3
JMA—President’s Speech
Policy Address*1
JMAJ 51(3): 141–142, 2008
Yoshihito KARASAWA*2
of scientific technology and national healthcareissues in the future, and efforts to address theprovision of specialized medicine and the harshworking environments of hospital-based doctors.
In recent Diet debates, opinion has been dividedon issues such as tax issues that greatly affectlocal governments, such as the incorporation ofspecial road accounts into general revenue andthe so-called expiration of temporary gas tax ratemeasures.
The national government’s healthcare systemreforms are currently in a state where it is impos-sible to escape from the finance-driven model,and depending on the future direction of govern-ment policies, there are grave concerns that thesereforms will result in an increased burden on thepublic and a decrease in healthcare quality, lead-ing down the path of destruction of local health-care systems. The tax system problem, which alsoconcerns the financial backing of an appropriatehealthcare provision system, will continue infuture to require the utmost attention.
The core philosophy of the JMA is to encour-age all members in their continuous study in thefast-evolving medical and healthcare fields, andcontribute to public healthcare in accordancewith medical ethics. The public hold high expec-tations for us to achieve this primary objective.Moreover, the raison d’etre of each and everyone of our members, regardless of how intenselybusy their days may be, lies in the tremendoussense of satisfaction achieved by providingcontinuous quality healthcare and perseveringwith local healthcare activities. Based on thegrassroots of such healthcare activities, thehealthcare required by the public must be safeand of high-quality. For patients, it is vital thatdoctors persevere in providing warmhearted,
*1 This is a revised English version of the reappointment address originally delivered in Japanese by Dr. Yoshihito Karasawa at the 118th RegularGeneral Assembly of the JMA House of Delegates held in Tokyo, April 2, 2008.*2 President, Japan Medical Association, Tokyo, Japan ([email protected]).*3 1 US dollar�120 yen.
I am honored to report that, with the support ofJMA members from regions throughout Japan,I was reelected for a 2nd term as JMA Presidentat the 118th Regular General Assembly of theJMA House of Delegates. I would also like toexpress my warmest thanks for the generous sup-port and guidance I received during my previous2-year tenure.
Looking back over my initial 2 years as JMAPresident, I feel as if we were hit full-on by roughseas from our start, coming as it did in the midstof a truly unparalleled period of change for thehealthcare system. With the Council on Economicand Fiscal Policy announcing a shrinking over 5years of social security costs, which has a fiscalbase of 1.1 trillion yen (9.2 billion US dollars),*3
and the introduction of laws related to healthcaresystem reform without due examination of thesystem, among other incidents, it felt as if wespent the entire 2 years battling for dear life as wetried to pull the brakes on a runaway train thathad already jumped the tracks.
In running the JMA, I intend to continue topush forward undaunted with sincerity and ingood faith, confronting head-on the difficult situ-ation surrounding healthcare and working withour richly experienced officers from around thecountry who gave me their nomination to addressthe mountain of issues we face by bringing togetherideas and opinions and fully exercising our com-prehensive strength.
The environment surrounding healthcare hasbecome much more difficult in recent years.Certainly, changes to the social structure such asthe super-ageing society and industrial economyhave hugely affected the direction of the entiresocial security system, beginning with the correc-tion of disparities between regions, the progress

142 JMAJ, May/June 2008 — Vol. 51, No. 3
Karasawa Y
highly satisfying healthcare. Moreover, fromthe perspective of public healthcare, it is of theutmost importance that we make efforts to estab-lish a universal and equitable healthcare provi-sion system.
In order to establish a large, enduring move-ment to achieve these objectives, we need topresent healthcare policies and principles withfuture potential—the cornerstone for all JMAmembers—and make the pursuit of the kind ofhealthcare required by the public our primaryobjective.
With the arrival of the super-aging society, wemust quickly establish a stable and permanentmedical system that will form the core of thesocial security system, encompassing health ser-vices, the medical care system, the nursing caresystem, and the pension system, in order to main-tain the health and quality of life of peoplethroughout their lifetimes, as well as to createa prosperous longevity society. For each of therelated factors—advances in medicine and health-care and the growing aged population, changesin disease structure, and heath management ofthe current working population, etc.—it is trulyimportant that convincing healthcare policies beformulated based on evidence and implementedwith the understanding and cooperation of vari-ous parties.
Looking at the situation from this standpoint,I believe that, in regard to the central issues forthe JMA—from gathering detailed informationabout local healthcare activities such as socialmedicine analysis, medical economics analysis,and epidemiological analysis of disease emer-gence conditions, as well as immediate treatmentof illness such as emergency care, to the observa-tion, examination, and analysis of the conditionsof all local healthcare systems and cultivation ofthe foresight and backbone required to presentproposals and recommendations regarding thesetopics, future outlooks, and countermeasures—we must make such efforts the headwaters of ouractivities.
In order to secure public health under the cur-rent circumstances, in which so many difficult-to-assess problems exist, the JMA needs to continuepouring its maximum efforts into invigorating
and establishing support for local healthcare inpreparation for the construction of a futurehealthcare system with an indomitable spirit,keeping in perspective the opinions of membersthroughout the country and the future vision ofhealthcare desired by the public.
Before summer, the Council on Economic andFiscal Policy is expected to compile their “BasicPolicy 2008” in preparation for the government’sbudget planning for the next fiscal year. ThisBasic Policy, which is already under discussionby the Cabinet Office’s National Commission onSocial Security, is expected to strongly influencethe shape of social security, including funding.
Last year the JMA prepared and published acompilation of general and specific statementsentitled “Grand Design 2007.” As the subtitleof this document indicates, what we should beaiming for is the reconstruction of “OptimalHealthcare that the Public Can Trust.” I recog-nize that the required role of the JMA is toensure that the contents of the Grand Designare reflected in government policies.
Respecting the “Saitama Declaration” and“Okinawa Declaration” prepared by the Hospital-based Doctor Committee Liaison Council, whichreflects the voices of clinic doctors, hospital-based doctors, residents, young doctors, andwomen doctors nationwide, and based on impor-tant statements such as our “Policy Regarding aSystem of Providing Home Healthcare and Nurs-ing Care” and the “JMA Proclamation on theSupport of Children,” the JMA needs above allto bring together the opinions of all members andstrive to present effective proposals and recom-mendations regarding the direction healthcareshould take in future. We will proactively take upand address these issues in the course of our dailyactivities.
I conclude my remarks with a promise to exer-cise my duties as JMA President wholeheartedly,working together with the new executive memberstowards securing national health and revitalizingcommunity healthcare.
In future I will also take opportunities to reporton the progress of our efforts, and I ask for yourcontinued understanding and support.
143JMAJ, May/June 2008 — Vol. 51, No. 3
JMA Policies
quality of life rather than the pointless attempt tosustain life, end-of-life care should be practicedconsidering the options of withholding and with-drawing life-sustaining treatment depending onindividual cases. In such situations, we are facedwith problems involving procedures such as theadministration of drugs, artificial respiration, andnutrition. The withdrawal of such treatments leadsto the death of the patient, and therefore thedecision to take such actions must be made withprudence. Judgment regarding the withholdingand withdrawal of life-sustaining efforts shouldnot be made by the attending physician alone, butshould be adequately supported by the opinionof the medical care team comprising other physi-cians and various healthcare professionals.
Two important prerequisites for withholdingor withdrawing therapeutic actions are: 1) thefact that the patient is affected by an incurabledisease and is in terminal stage, where there is nohope of recovery and death is expected in thenear future; and 2) the presence of a currentlyvalid indication of the patient’s wishes requestingthe withholding or withdrawal of therapeuticactions.
The decision regarding the impossibility ofrecovery and the inevitability of death, men-tioned in 1) above, is made by the medical careteam. The indication of the patient’s wishes, men-tioned in 2), must be confirmed by such means asthe oral statement of the patient or, in the casethat the patient has lost the ability to make soundjudgment, an advance written indication pro-vided by the patient (a living will or an advance
The problem of how medical care should be pro-vided in the terminal stage of life, including theinitiation, withholding, alteration, and withdrawalof treatment, has long been one of the most impor-tant challenges for healthcare professionals.
The 10th Bioethics Council of the Japan Medi-cal Association hereby proposes guidelines con-cerning the actions of physicians in end-of-lifecare.
In these guidelines, we opted not to defineend-of-life care. The terminal stage is experi-enced differently in different cases, and weconsider that decisions should be made by themedical care team*2 based on the conditions ofeach patient. We recommend that the readersconsult Grand Design 2007—Specific Discus-sions published by Japan Medical Association,which defines the terminal stage both in a widersense and in a narrower sense (Appendix 1).
Introduction
Recent advances in medicine and healthcarehave enabled us to save the lives of many patients.Nevertheless, there are increasing cases where ter-minally ill patients with no possibility of recoveryare receiving life-sustaining treatment contraryto the wishes of the patients, their family and/orother appropriate persons.*3 Increasing opinionis being raised that excessive treatment should bediscontinued, because it is not only meaninglessbut also a potential infringement of the dignityof patients.
Placing greater emphasis on the patient’s
Guidelines on End-of-Life Care*1
JMAJ 51(3): 143–148, 2008
Japan Medical Association
*1 These guidelines were issued in February, 2008 by the 10th Bioethics Council of the JMA.*2 As a rule, the medical care team consists of the attending physician, one or more physicians other than the attending physician, nurses, social
workers, and other healthcare professionals.In the case of home care, a system to support the decision of physicians engaged in home care (e.g., establishment of a committee) should
be constructed by appropriate organizations such as local medical associations. In this endeavor, the committee of the local medicalassociation or other organization providing support should stipulate relevant internal rules and keep the minutes of meetings.
*3 “Patient’s family and/or other appropriate persons” may include not only legal relatives but also the persons who are entrusted by the patient.It is desirable that the patient has a proxy designated in advance to speak for the patient in the terminal stage.

144 JMAJ, May/June 2008 — Vol. 51, No. 3
directive). Some professionals consider that evenif the advance indication of the patient’s wishes isnot obtained directly from the patient, a decisionmay be made based on the wishes expressed bythe patient’s family and/or other appropriatepersons, provided that they are sufficient for theinference of the patient’s wishes. In this case, it isimportant that the physician obtains sufficientinformation from the family and/or other appro-priate persons as the basis for the inference of thepatient’s wishes. The physician should have fulldiscussion with the patient’s family and/or otherappropriate persons and consider what would bethe best for the patient.
Principles of End-of-Life Care
(1) The decision that a patient is in the terminalstage should be made by the medical careteam led by the physician and consisting ofseveral healthcare vocations.
(2) The initiation, withholding, alteration, andwithdrawal of treatment should be decidedprudently by the medical care team accord-ing to the patient’s wishes and based onmedical reasonability and suitability.
(3) Pain and other distressing symptoms shouldbe alleviated to the extent possible and com-prehensive treatment and care should beprovided including the mental and social sup-port to the patient, the family and/or otherappropriate persons.
(4) Actions such as active euthanasia and physi-cian-assisted suicide are not acceptable.
Basic Procedures for DeterminingEnd-of-Life Care Strategies
The initiation, withholding, alteration, andwithdrawal of treatment in the terminal stagemay have serious consequences. In particular, thewithdrawal of treatment is likely to result in thedeath of the patient. Therefore, physicians mustbe extremely prudent in determining the strate-gies for end-of-life care. The following describesthe basic procedures that should be followed inthe initiation, withholding, alteration, and with-drawal of treatment in the terminal stage.(1) If it is possible to confirm the patient’s wishes,
Japan Medical Association
strategies should be determined by the medi-cal care team respecting the patient’s wishesbased on informed consent. In this process,the physician should have sufficient discus-sion with the patient, the patient’s family,and/or other appropriate persons, avoidingcoercion, and should document the contentof discussion.
In this case, explanation should be givenand the patient’s wishes should be reconfirmedwhenever necessary, depending on the passageof time, changes in the patient’s condition,and the revision of medical evaluation. Unlessthe patient refuses, the content of the deci-sion should be made known to the patient’sfamily and other appropriate persons.
In the case of emergency care, the decisionon the initiation of medical treatment shouldbe left to the discretion of the attending phy-sician based on the dignity of life.
(2) If the patient is unable to express his or herwishes and there is advance written indica-tion of the patient’s wishes provided bythe patient*4 (hereinafter referred to as “thewritten advance directive”), the validity ofthe written advance directive should beconfirmed with the patient’s family and/orother appropriate persons, and a decisionshould be made by the medical care team. Ifthere is no written advance directive but thepatient’s wishes can be inferred from theinformation from the patient’s family and/orother appropriate persons, treatment strate-gies respecting the inferred wishes should beemployed. The consent of the patient’s familyand/or other appropriate persons needs tobe obtained also in this case. If it is impossibleto infer the patient’s wishes, treatment strat-egies that are the best for the patient shouldbe employed, considering the decision of thepatient’s family and/or other appropriatepersons.
However, if it is impossible to contact thepatient’s family and/or other appropriatepersons, they do not indicate any decision, orthere is disagreement of opinion amongthem, the medical care team should makedecision and obtain the approval of thepatient’s family and/or other appropriate
*4 The “ written advance directive provided by the patient” refers to the document in which the patient provides advance wishes regarding theend-of-life care to be given to him or her.

145JMAJ, May/June 2008 — Vol. 51, No. 3
GUIDELINES ON END-OF-LIFE CARE
persons regarding this decision as a rule.*5
In all of the above cases, the confirmation,consent, and approval of the patient’s familyand/or other appropriate persons must beobtained in writing.
(3) If it is difficult to determine the content ofmedical care within the medical care team, orthe discussion between the patient and themedical personnel has not reached an agree-ment regarding the content of reasonableand suitable medical care, a separate commit-tee comprising several healthcare vocationsshould be established to examine and adviseon treatment strategies and other issues.
Concluding Remarks
We have thus far described the basic principlesand procedures regarding end-of-life care, focus-ing on the initiation, withholding, alteration, andwithdrawal of treatment in the terminal stageand referring to the Guidelines on the DecisionMaking Processes in End-of-Life Care published
*5 The wording “as a rule” is used here because there may be situations in which the approval of the patient’s family and/or other appropriatepersons is unobtainable because such persons are unreachable or absent.
by the Ministry of Health, Labour and Welfare.It is necessary to establish an institutional
framework to protect healthcare professionalsfrom civil and criminal legal liabilities for with-drawing life-sustaining treatment according tothe procedures shown in these guidelines inthe case that a terminally ill patient rejects life-sustaining treatment or the patient’s family and/orother appropriate persons reject life-sustainingtreatment when it is impossible to confirm thepatient’s wishes.
The problems related to end-of-life care aregoing to be all the more important with theincrease in the aged population in Japan. It isimportant that medical students, as well as allhealthcare professionals, seriously consider theproblems related to end-of-life care, and theseshould be incorporated in the curriculums ofmedical education.
Appendix 2, which shows a flow chart of theprocedures to be followed in determining treat-ment strategies in end-of-life care, may help fur-ther understanding.

146 JMAJ, May/June 2008 — Vol. 51, No. 3
Appendix 1
Japan Medical Association
The “Terminal Stage” in the Wider Sense(Unless otherwise specified, the term “terminal stage” is used in this sense.)
(1) The stage in which the best available medical care would
not stop progressive aggravation of the condition and death
is considered inevitable in the near future.
(2) The “terminal stage” begins when the presence of the
condition described in (1) above is declared by more than
one physician including the attending physician, nurses,
and more than one other pertinent healthcare professional,
and is understood and agreed on by the patient or, when
the patient is unable to make decisions, the patient’s family
and/or other persons (including not only legal relatives but
also the persons entrusted by the patient) who can infer
the patient’s wishes.
The “Terminal Stage” in the Narrower Sense(Near-death condition)
The near-death condition in which death is imminent.
Source: Grand Design 2007—Specific Discussions

147JMAJ, May/June 2008 — Vol. 51, No. 3
Appendix 2
GUIDELINES ON END-OF-LIFE CARE
Procedures Leading to the Determination of Treatment Strategies in End-of-Life Care
Medical care team declares the terminal stage
Documentation of agreement
Consent of family or others(approval by patient)
Reconfirmation of wishes
Consent of family and/or others
Documentation ofagreement
Decision by familyand/or others
Documentation of agreement
Approval by family and/or others, as a rule
Documentation of agreement
Family and/or othersare unreachable orunable to makea decision
Decision by medicalcare team
Medical care team determines end-of-life care strategies
Examination and advice by the committee comprisingseveral healthcare vocations
Determination by medical care team is difficult
Patient’s wishescannot be inferred
Patient’s wishescan be inferred
Patient’s wishes can be confirmed Patient’s wishes cannot be confirmed
The validity of writtenindication is confirmedwith family and others
There is a writtenadvance directive
There is no written advance directive
Sufficient discussion with patient

148 JMAJ, May/June 2008 — Vol. 51, No. 3
The 10th Bioethics Council of the Japan Medical Association (2006–2007)
Chair
Fumimaro TAKAKU President, Japanese Association of Medical Sciences,President, Jichi Medical University
Members (Alphabetical order)
Kiyoshi AOKI Professor Emeritus, Sophia University
Tsutomu FUKUTA President, Toyama Medical Association
Akihiro IGATA President, Nagoya University of Arts and Sciences
Tetsuya ISEKI President, Nagasaki Medical Association
Hisatake KATO Professor Emeritus, Kyoto University
Takashi KOMORI President, Ishikawa Medical Association
Mariko KUSUMOTO Executive Officer, Japanese Nursing Association
Atsuko MATSUNE Vice-chairman, Japan Society for Dying with Dignity
Taketo MUKAIYAMA Palliative Care Department Director,The Cancer Institute Hospital of Japanese Foundation for Cancer Research
Naoki NABESHIMA Professor, Faculty of Law, Ryukoku University
Takeshi NARAHARA Special Writer, Kyodo News Service
Giro SASAKI President, Aomori Medical Association
Satoko TAMURA Director of Department of Social Work, Higashi Sapporo Hospital
Takao YAMADA Professor, Nihon University Law School
Observers
Rintaro SAWA Research Director, Japan Medical Association Research Institute
Wataru MIZUTANI Senior Researcher, Japan Medical Association Research Institute
Japan Medical Association
149JMAJ, May/June 2008 — Vol. 51, No. 3
Research and Reviews
developing countries.The first sphere is mainly for utilizing foreign
school health information in Japan, while thesecond sphere is mainly for utilizing Japan’s pastexperience in order to improve school healthtargeting pupils and students in developing coun-tries. Accordingly, the international health activi-ties have two different aspects. It can be said thatinternational school health has ambiguity.
Compared to the volume of accumulatedexperience in the first sphere, the second spherecan rely on an extremely small amount of experi-ence. The second sphere is still trying to find itsway, mostly depending on the results of future
Introduction—Two spheres of actionregarding international cooperation ineducation
Activities regarding international cooperation ineducation in Japan are grouped into two spheresof action: i) a theoretical sphere dedicated to theintroduction of school health trends in foreigncountries and programs of foreign academicsocieties and associations as the Japanese Asso-ciation of School Health and the JapaneseSociety of School Health have been doing, andii) a practical sphere to provide assistance to
*1 Professor, Otsuma Women’s University, Tokyo, Japan ([email protected]).
Construction of Modules for InternationalCooperation Method in School Health—Technical cooperation in school health education
in Thailand and Myanmar—
JMAJ 51(3): 149–158, 2008
Seiji OHSAWA*1
AbstractThis “Activity project aimed at the sustainable development of cooperation in school health” was started in 2002as a project for International Cooperation in Education by the Ministry of Education, Culture, Sports, Science, andTechnology (MEXT). The improvement module carried out in Thailand and Myanmar in the last 5 years demon-strated a high degree of effectiveness in terms of sustainability, high cost-benefit performance, verification ofpositive results, sequence of short-term results to long-term results, and multiplied effects from school to com-munity. The project consists of four phases: (1) Targeting 30 experts who have experience in internationalassistance, a Delphi survey was conducted to determine urgency, cost effectiveness, the likelihood of positiveeffects, and how easy it would be to transfer Japan’s successful experience. Based on the results, the followingsix fields were selected for phase 2; (2) A) Establishment and management of a school health improvement team;B) Establishment of healthcare rooms, preparation of minimum equipment, and provisions for training in themeasuring method; C) Life-style improvement through health quality control (HQC); D) Improvement of schoolenvironment and hygiene through HQC; E) Promotion of school safety through HQC; F) Fostering of animals andplants and instruction on nutrition. The activity manuals for the above fields were prepared in Japanese and Thai,and their effectiveness was verified in Thailand; (3) The effectiveness of the improved modules was verified inThailand and Myanmar; and (4) The modules will be introduced throughout Myanmar, and will be extended intoother countries.
Key words School health, International cooperation, Thailand, Myanmar, Assistance module

150 JMAJ, May/June 2008 — Vol. 51, No. 3
implementation and research by internationalcooperation projects. Under such circumstances,we have implemented school health improvementmodules in Thailand and Myanmar in the past5 years. Here we introduce the modules, whichshowed effectiveness in terms of sustainability,high cost effectiveness, verification of results bydata, sequence of short-term results to long-termresults, and multiplied effects from school tocommunity.
Objective of Research
The project, titled “Activity project aimed at thesustainable development of cooperation in schoolhealth,” was started in 2002 as a project in inter-national cooperation in education by MEXT. It isaimed at constructing an effective and sustain-able methodology for school health cooperationtargeting mainly Southeast Asia. To this end, thefollowing procedure has been established. First,assistance is given by providing practical knowl-edge and technology concerning specific themesthrough workshops and on-site training in theschool. Later, the school independently carriesout the school health improvement project forseveral months according to their own program.The results are evaluated objectively. If a success-ful result is confirmed by assessing the data, themethod is regarded as one of the cooperationmodules. The module is further considered if it istransferred to other areas.
The researchers’ group represented byOhsawa was organized by placing its researchbase in the Institute of human living science,Otsuma Women’s University. Researchers fromTottori University, Kanazawa University, ChukyoUniversity, Nagoya Gakuin University, NiigataUniversity, International Budo University, Uni-versity of Tsukuba, Tokyo Metropolitan Univer-sity and Tokyo Institute of Technology joinedthe project.
Construction of Methodology
Phase 1: In order to search for target countries,areas, themes, and methods, we conducted aDelphi survey targeting 30 researchers who havepractical experience in international coopera-tion. The survey asked what kind of fields shouldhave priority among the various fields of schoolhealth; if projects should adopt the top-down
Ohsawa S
method or bottom-up method; what are theissues hindering the development of cooperationprojects; what kind of projects have the highesturgency, high cost-benefit performance, or makeit easier to transfer Japan’s successful experience.
For this survey, at first 250 Japanese expertswere recruited. Among them, 30 experts wereselected, and they were asked the same surveyquestions three times in a 6-month period untilthey reached conclusion. Their responses weresummed up.
As a result, the following six priority areaswere selected:A) Establishment and management of school
health improvement teams;Under the leadership of the school principal,all teachers, representatives of students, par-ents, health center, administrative institutions,and other organizations make up the teamsin order to carry out continuous activitiesaccording to the plan.
B) Establishment and management of schoolhealth offices;School health offices are to be established inorder to store basic minimum equipment andprovide training on measuring methods.Three to four implementation leaders as wellas the principal play central roles in develop-ing the HQC movement (a method formu-lated by applying QC methods developed inJapan to health promotion).
C) Life-style improvement through HQC (healthquality control)1–3;Based on the concept that the solution toall health problems starts with life-styleimprovement, life-styles are checked in orderto prepare for various health problems.
D) Improvement of school environment andhygiene through HQC;Movement for systemic and organized im-provement is to be developed using HQC.Using equipment and measuring methodmentioned in B, teachers take leadership inthe implementation of the health improve-ment movement based on scientific data. Theimprovement team mentioned in A will playan important role.
E) Promotion of school safety through HQC;Based on the HQC method, all students,teachers and community residents are to fixdangerous items, and the health movement isto be carried out according to the improve-
151JMAJ, May/June 2008 — Vol. 51, No. 3
CONSTRUCTION OF MODULES FOR INTERNATIONAL COOPERATION METHOD IN SCHOOL HEALTH
ment plan.F) Fostering of animals and plants and nutrition
guidance;The school itself tries to earn cash and securefood by growing rice, vegetables, medicalherbs, fish, cattle, and fruit, in addition to pro-viding nutrition guidance and managing themeal supply.
The improvement team mentioned in A playsa leading role in the implementation of all theseprograms. Data are collected without fail beforeand after the improvement project to holds areport meeting about once every 6 months.* When the school suggests its own improvement
program in addition to these programs, we sup-port it as much as possible.
Phase 2: Japanese manuals for each of theabove six fields (From A to F) have been pre-pared. These manuals were translated into Thai,Myanmar, and Nepali, to hold workshops inUbon and Chiang Mai provinces in Thailand. Atotal of 33 schools joined the workshop. After theworkshop, each school was asked to submit theirown school health improvement program. Thesubmitted programs were screened in coopera-tion with local relevant individuals. As a result,five schools were selected as model schools. Theyinclude three schools in the poorest area alongthe national border in Ubon province and twoschools in minority hill tribe communities, theMon and Karen tribe communities in ChiangMai province. Targeting these schools, a technicalworkshop was held a total of seven times. Eachschool made and implemented its original programconsidering the characteristics of its region, andestablished a school health committee. After 3years of implementation of various improvementprojects, their results were reported. Accord-ing to these results, a development cooperationmodule for each field was proposed. The modelschools continuously introduce and extend theproposed module to the neighboring schools.Local NGOs also join and support the program.
Phase 3: The effectiveness of the improvementmodule established in Thailand has been verifiedin Myanmar. In October 2006, The Foreign AffairsPolicy Committee (FAPC), the highest foreignpolicy-making institution in the nation, autho-rized the implementation of the program. Cur-rently, foreigners are never able to enter schools
without this permission. In the total of 40 schoolsin Yangon, Mawlamyine, Mandalay, and Pathein,workshops were held. In the workshops, the mea-surement equipment was provided, and instruc-tions were given on the measurement method,the improvement method, the recording methodand others. Furthermore, 12 schools were desig-nated as model schools. We visited those schoolsand provided on-site training. Each model schoolmade detailed improvement programs in the sixfields, and carried out them in cooperation withlocal human resources. After a 6-month programimplementation, outcomes were evaluated and asignificant effect was confirmed in the open pre-sentation meeting. These improvement programscontinued to be carried out in this second year,having remarkable effects.
Phase 4: As feasibility of the method was con-firmed as shown in the above, the module is to beintroduced and developed throughout Myanmar.The project will continue in cooperation withsupporting business entities and NGOs also inthe future.
Supporting institutions and organizations:Ministry of Education of Kingdom of Thailand,Education office of Ubon province, Educationoffice of Chiang Mai province, NGO inside Thai-land, 20 hill tribe-related NGOs inside Thailand,Ministry of Education of the Union of Myanmar,Japanese Myanmar-related NGOs, MEXT Japan,The Toyota Foundation, Japan Society of HumanGrowth and Development
Outcome
Part of the outcomes of the six programs aredescribed below.
A) Establishment and management ofschool health improvement team
School health activities can obtain outcomeswhen they are conducted organizationally. Threeto four important teachers as well as the princi-pal are to join the workshop. In the workshop,participants learn how to carry out improvementactivities through practical training using amanual in the local language. Participants goback to their school and organize a team askingall teachers. As the activities draw more attention,the team can involve children, parents, schoolsupporters, health center, village office, and NGOs

152 JMAJ, May/June 2008 — Vol. 51, No. 3
as activity supporters. Some improvement teamsconsist of only children. Beforehand, the districtsuperintendent of education and others shouldbe asked to participate in the workshop. (InMyanmar, key post officials including chiefs ofbureaus in the Ministry of Education also par-ticipated.) (Figs. 1, 2)
B) Establishment and management ofschool health offices
While human resource factors were mentionedin the above, in this field the focus is on spatialfactors. Space is to be secured as a base place formember meetings, team holding, team manage-
Fig. 1 Extension image of project system in Thailand
Ohsawa S
Project development in Thailand (Branched cluster type)
Cooperationby village
Cooperation byprovince and
district
Holding ofworkshop
three timesa year
First/Second/Third schooldistrict, Ubon Province
P school G school N school
P schoolG school
N school
M school N school
(Project implementation) (Project implementation)
Second school district,Chiang Mai Province
Third school district
Japaneseteam
NGOLocal collaborator
Fig. 2 Extension image of project system in Myanmar
Project development in Myanmar (Base point development type)
WS in the central (Yangon)
Townshiprepresentative
Model schoolrepresentative
Townshiprepresentative
Model schoolrepresentative
Townshiprepresentative
Model schoolrepresentative
Townshiprepresentative
Model schoolrepresentative
WS in Mawlamyine
WS in Mandalay WS in Magwey
(On-site training)
(On-site training)
(On-site training)
(On-site training)
Japanese team andlocal collaborators
153JMAJ, May/June 2008 — Vol. 51, No. 3
ment, improvement activities, and health educa-tion. It is also to be used for storing measuringequipment, medical supplies, and various records,as well as to provide student with a place for rest-ing and temporary medical care. In many devel-oping countries, schools do not have a schoolhealth office. For school management, however,setting up a school health office means a lot morethan merely giving first-aid. If there is no spacefor a school health office in the school, a corner ofthe principal’s office will do. In the workshop, thebasic items for implementation of the module areprovided. Among them are: height measuringrod, sitting height measuring rod, tape measure,skin fold caliper, weight scale, eye chart (long-sight/short-sight), tuning fork, as well as an illu-minance meter, a water quality test kit, mesh typesoap bar holder, and a school health improve-ment manual.
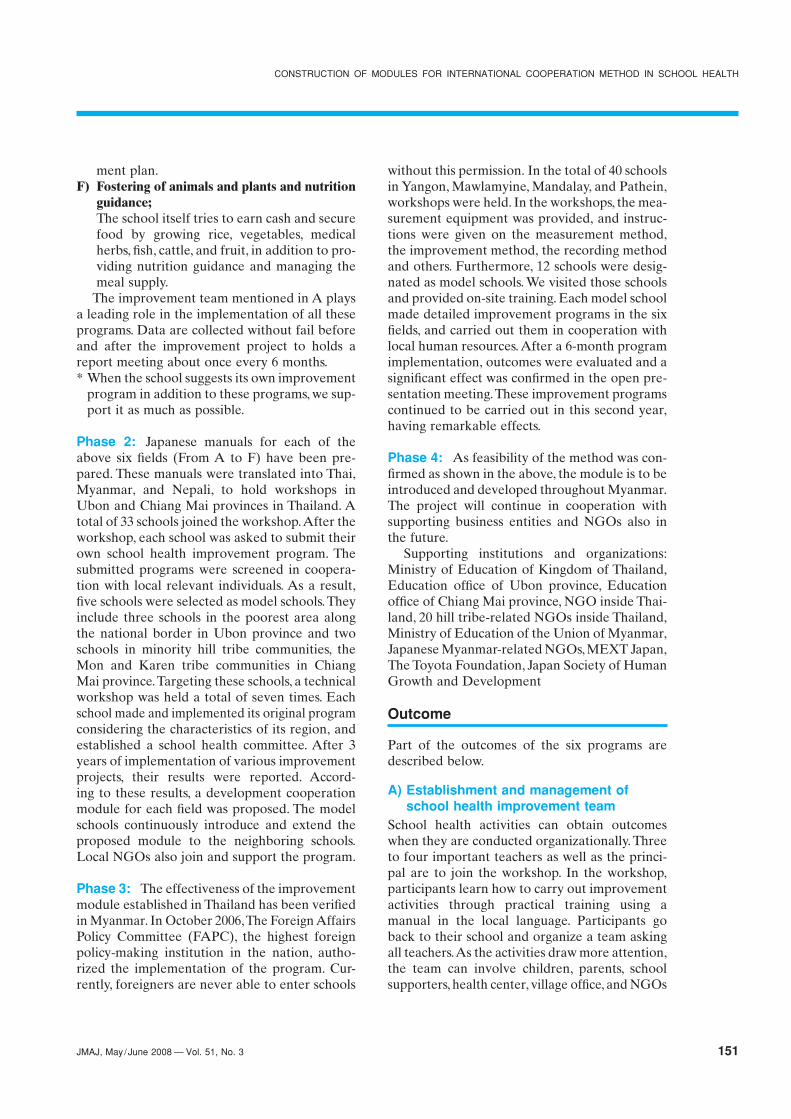
C) Life-style improvement through HQCThis is a school health method to which the QCmethod was applied. Using this method, even alife-style which seems difficult to improve can beimproved in several months. As parasitic diseasesand infectious diseases are largely related to life-style, instructions are given to enable the stu-dents to manage their own basic life-style basedon their age. Recommended life-style activitiesinclude: washing hands, feet, and face; garglingthe throat; taking a bath (bathing); refrainingfrom eating raw meat/fish; food management;early to bed and early to rise; getting enoughsleep; cleaning up clothing and housing; wear
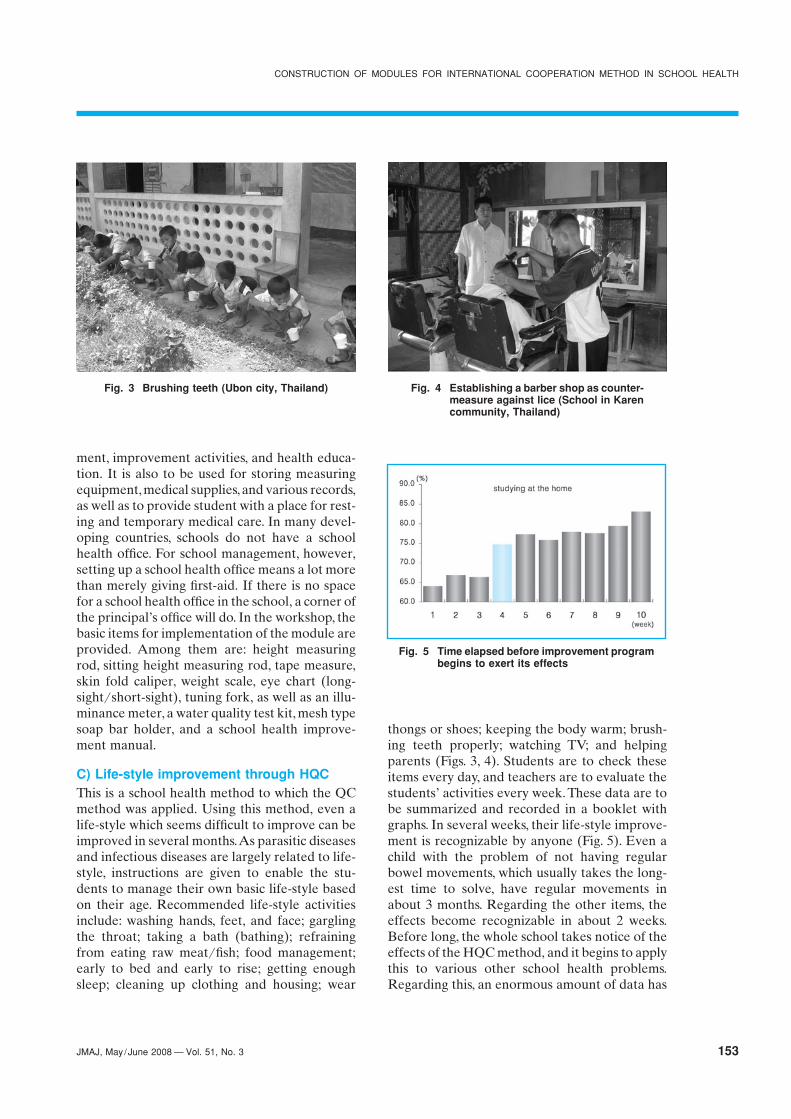
thongs or shoes; keeping the body warm; brush-ing teeth properly; watching TV; and helpingparents (Figs. 3, 4). Students are to check theseitems every day, and teachers are to evaluate thestudents’ activities every week. These data are tobe summarized and recorded in a booklet withgraphs. In several weeks, their life-style improve-ment is recognizable by anyone (Fig. 5). Even achild with the problem of not having regularbowel movements, which usually takes the long-est time to solve, have regular movements inabout 3 months. Regarding the other items, theeffects become recognizable in about 2 weeks.Before long, the whole school takes notice of theeffects of the HQC method, and it begins to applythis to various other school health problems.Regarding this, an enormous amount of data has
Fig. 3 Brushing teeth (Ubon city, Thailand) Fig. 4 Establishing a barber shop as counter-measure against lice (School in Karencommunity, Thailand)
Fig. 5 Time elapsed before improvement programbegins to exert its effects
CONSTRUCTION OF MODULES FOR INTERNATIONAL COOPERATION METHOD IN SCHOOL HEALTH
154 JMAJ, May/June 2008 — Vol. 51, No. 3
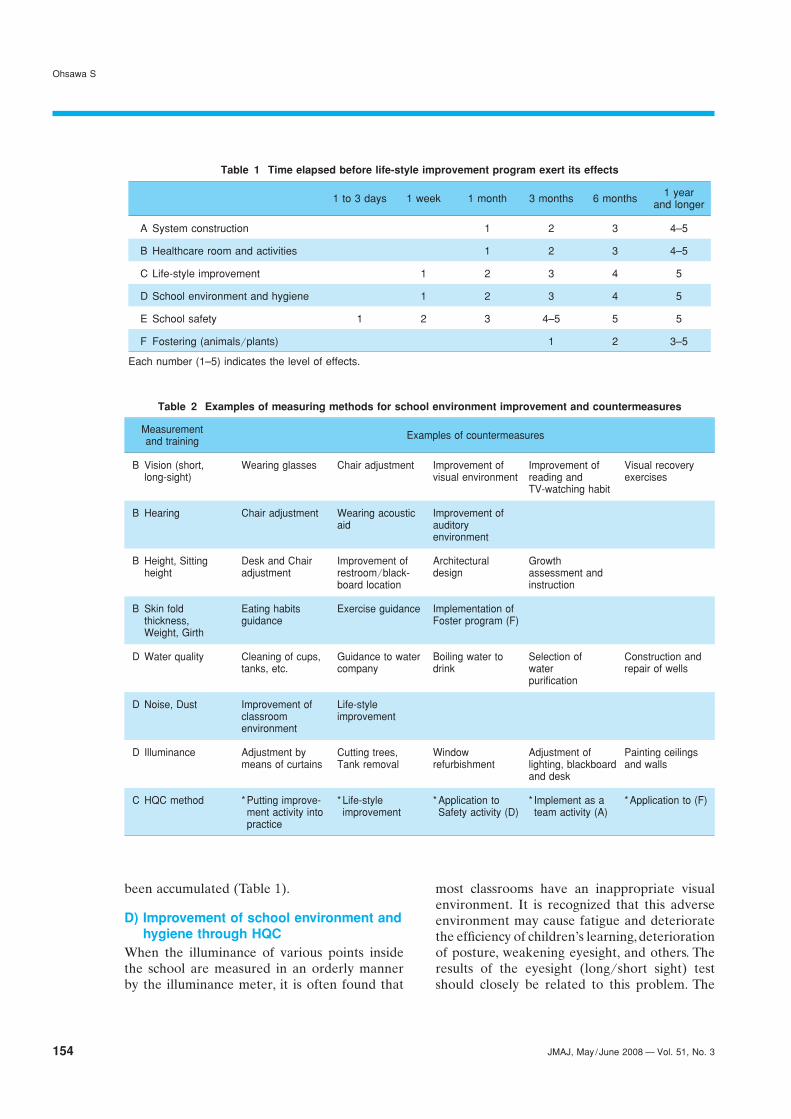
been accumulated (Table 1).
D) Improvement of school environment andhygiene through HQC
When the illuminance of various points insidethe school are measured in an orderly mannerby the illuminance meter, it is often found that
most classrooms have an inappropriate visualenvironment. It is recognized that this adverseenvironment may cause fatigue and deterioratethe efficiency of children’s learning, deteriorationof posture, weakening eyesight, and others. Theresults of the eyesight (long/short sight) testshould closely be related to this problem. The
Table 1 Time elapsed before life-style improvement program exert its effects
1 to 3 days 1 week 1 month 3 months 6 months 1 yearand longer
A System construction 1 2 3 4–5
B Healthcare room and activities 1 2 3 4–5
C Life-style improvement 1 2 3 4 5
D School environment and hygiene 1 2 3 4 5
E School safety 1 2 3 4–5 5 5
F Fostering (animals/plants) 1 2 3–5
Each number (1–5) indicates the level of effects.
Table 2 Examples of measuring methods for school environment improvement and countermeasures
Measurementand training Examples of countermeasures
B Vision (short, Wearing glasses Chair adjustment Improvement of Improvement of Visual recoverylong-sight) visual environment reading and exercises
TV-watching habit
B Hearing Chair adjustment Wearing acoustic Improvement ofaid auditory
environment
B Height, Sitting Desk and Chair Improvement of Architectural Growthheight adjustment restroom/black- design assessment and
board location instruction
B Skin fold Eating habits Exercise guidance Implementation ofthickness, guidance Foster program (F)Weight, Girth
D Water quality Cleaning of cups, Guidance to water Boiling water to Selection of Construction andtanks, etc. company drink water repair of wells
purification
D Noise, Dust Improvement of Life-styleclassroom improvementenvironment
D Illuminance Adjustment by Cutting trees, Window Adjustment of Painting ceilingsmeans of curtains Tank removal refurbishment lighting, blackboard and walls
and desk
C HQC method * Putting improve- * Life-style * Application to * Implement as a * Application to (F)ment activity into improvement Safety activity (D) team activity (A)practice
Ohsawa S

155JMAJ, May/June 2008 — Vol. 51, No. 3
issue is what to do. The improvement teammembers discuss methods to achieve a classroomwith well-balanced brightness or countermea-sures for children with visual disorders. Counter-measures taken for the solved problems are tobe indicated on the table. Improvement is to beachieved by deciding details such as measure-ment, evaluation, improvement plan, budget,responsible persons, and improvement schedule,in that order. Improvement takes several weeksor so (Table 2).1) Improvement of water qualityWater quality testing is to be conducted in orderto secure an appropriate level of drinking waterquality. Drinking water of many schools is con-taminated with coliform bacteria. In some cases,the water shows positive results for other testitems, such as ammonia and COD. For example,response measures are easily taken when dirtyglasses or water taps cause pollution of thebottled water that should be safe. However,sometimes water itself runs short in mountainousarea, wells are not usable in the rainy season,or water is polluted by human and animal waste.In these cases, it is often necessary to formulateanother improvement plan for securing safedrinking water. In most of these cases, however,the problems have been solved by the wholeorganization’s recognizing the fact and consider-ing the measures. The important point is that thewhole school considers the solution involving thelocal community. Some schools demanded thatthe drinking water company improve the pollu-tion. Water quality testing provides the scientificfoundation for finding such problems.2) AnthropometryMeasurement of height, sitting height, skin foldthickness, and chest girth enables to evaluategrowth and nutritious conditions objectively. Inpractice, however, these measurements affectmanagement and use of school supplies, such asdesks, chairs, blackboards, and restrooms to agreat extent. In developing countries, childrenvery often use learning equipment and suppliesthat do not fit their sizes. This should be improveddepending on their standard physical size. Inmany cases, the school building itself is just atemporary shanty. Often, even school buildingsconstructed with donations from volunteer sup-porters turn out to have been built in a haphaz-ard way. There are countless examples of this:such school buildings have corridors that are too
narrow, steps that are too steep, grab rails thatare way too low, blackboards placed too high, andother problems. Measurement of the students’physical size will lead to the construction ofschool buildings based on ergonomic criteria anda rational classroom environment. Of course,many developing countries do not have standardvalues for growth and nutrition. Accordingly,assistance institutions in those countries tend tocontinue unsystematic efforts with little scientificbasis. It is necessary to conduct other tests gradu-ally, including tests for dust, noise, ventilation,and others.3) Waste ManagementIn any country, the issue of waste management isone of the familiar themes that have long beenunresolved. In Thailand or Myanmar, the mosteye-catching sight is discarded waste. In orderto solve this, the project team is instructed todecompose the problem using the fishbone dia-gram of the HQC or CUDBAS method (Curricu-lum Development Based on Ability Structure).4
Problem decomposition is carried out consid-ering why waste generates, why people do notclear up waste, and how they can solve the prob-lem. In this way, the team members come to seethe waste disposal issue as a familiar task anyonecan carry out. Then, they come to focus on thewhole school’s engagement in the core of thisproblem, by sorting out, incineration, landfilling,selling out, and cleaning. The school in the Karen-tribe community started exchanging waste formoney, naming the system “waste bank.” Thismotivated and involved the residents of thewhole community. As a result, not only the school
Fig. 6 Sorting out waste (Ubon city, Thailand)
CONSTRUCTION OF MODULES FOR INTERNATIONAL COOPERATION METHOD IN SCHOOL HEALTH

156 JMAJ, May/June 2008 — Vol. 51, No. 3
but also the Karen village became drasticallyclean. This took only 3 months. This program canbe carried out in any school at hand. Someschools can earn as much as 5,000 baht a yearadopting this program (Fig. 6).4) Management and Cleaning of RestroomsThis program is aimed at involving school teachersin restroom improvement as their own problem.There are restrooms without water, schools thatdo not teach how to use restrooms, uncleanrestrooms, clogged restrooms, those close to thewells (water pollution source), and those gener-ating worms and maggots. Many schools boughtcleaning equipment, set up turns for restroomcleaning duty, and let children compete in termsof cleaning and hygiene management. Manyschools newly construct restrooms with theirearnings from the waste bank and sales of veg-etables and fish in the next F program.
E) School Safety ManagementIn any country, accidents are one of main causesof death. The numbers become enormous if weinclude cases of accidental physical impairmentand injury as well as cases of death by accident.In Japan, the number of cases where insurancebenefits are paid by the government due to stu-dents’ death, impairment, and injury under thesupervision of school amounts to 2 million in ayear. Potential risks for accidents are inherent inthe school environment. In a developing country,there is a great number of dangerous points inthe school environment, and among teachers,parents, and children there is a very low level ofsafety awareness and concern. Accordingly, acci-dents causing physical impairment and injuryoccur on a daily basis. To make it worse, in gen-eral there are no statistics on accidents. Althoughacute infectious diseases and parasite infectionare important issues in these countries, children’saccidents occur with a much greater frequency.Considering that the emergency rescue system ishardly improved, the prevention of accidents isa priority issue in school health. Accordingly,safety management in the school environment isfirst explained, and then, HQC activities for acci-dent prevention are introduced in the workshop.In the practical training in the school, teachersare asked to check every place in the school incooperation with students, in order to identifydangerous points. The dangerous points they findare plotted on a large school map to make a haz-
ard map. Dangerous points on the hazard mapare to be improved by formulating an improve-ment plan based on HQC method. Many schoolspost the hazard map in the school to draw theattention of all students, and develop improve-ment activities. As the Mon tribe village had notraffic signs, all students of the school cooperatedin making and placing hazard signs and trafficsigns. As the effects of this program can beconfirmed instantly as shown in Table 1, the pro-gram is important as a pioneering improvementactivity. In the implementation of this program, itis recommended to keep photographic records ofbefore and after the improvement as well as thestatistics on accidents (Fig. 7).
F) Fostering of Animals and Plants (fosterprogram)
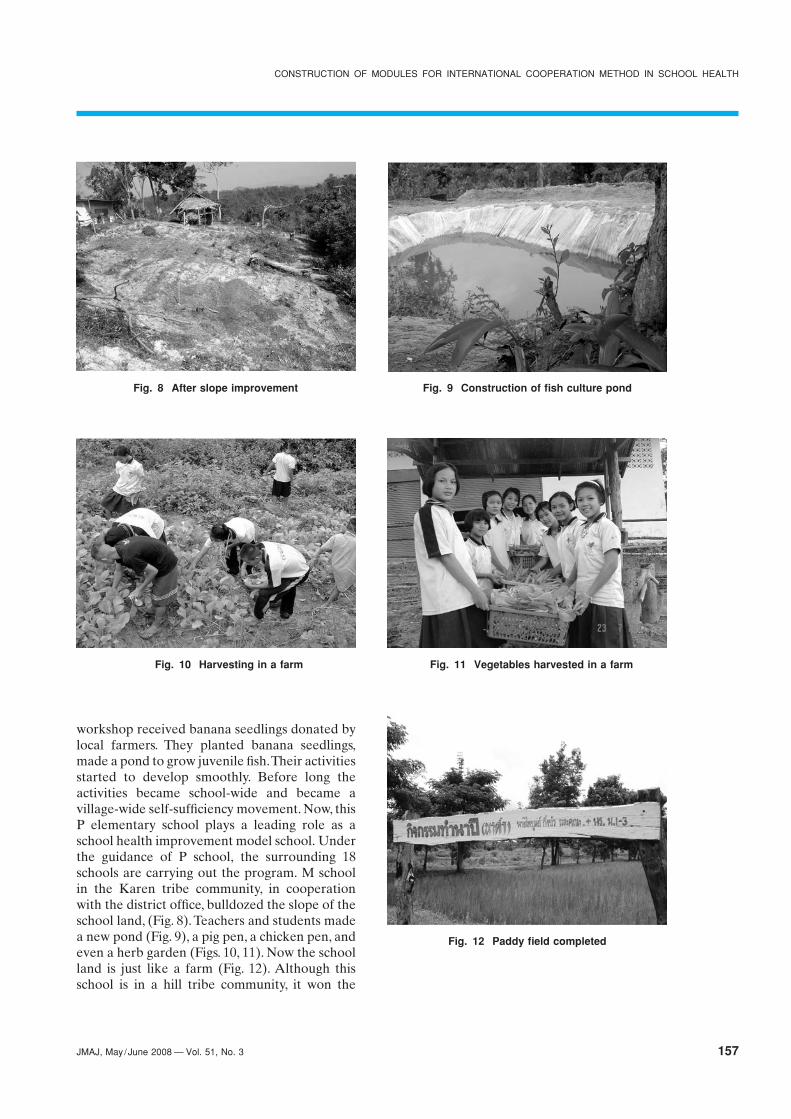
In this program, teachers and students growanimals and plants by themselves, and use themfor school meals or sell them. In the workshop it isrecommended to get a large yield by growing vari-ous vegetables, medical herbs, fish, pigs, chickens,frogs, rice, bananas from seeds, chicks, or juvenilefish, and sell them in order to get funding forimprovement activities or to use them to makeup nutritious school meals. This program can becarried out more actively in the rural schools witha vast expanse of school land. P elementaryschool, which is located in the poorest area inThailand along the border with Laos, had toomany problems to carry out improvement activi-ties after the workshop. The principal was alsounwilling to carry out the activities. However,three young teachers who participated in the
Fig. 7 Village residents’ activity for school route safety
Ohsawa S
157JMAJ, May/June 2008 — Vol. 51, No. 3
workshop received banana seedlings donated bylocal farmers. They planted banana seedlings,made a pond to grow juvenile fish. Their activitiesstarted to develop smoothly. Before long theactivities became school-wide and became avillage-wide self-sufficiency movement. Now, thisP elementary school plays a leading role as aschool health improvement model school. Underthe guidance of P school, the surrounding 18schools are carrying out the program. M schoolin the Karen tribe community, in cooperationwith the district office, bulldozed the slope of theschool land, (Fig. 8). Teachers and students madea new pond (Fig. 9), a pig pen, a chicken pen, andeven a herb garden (Figs. 10, 11). Now the schoolland is just like a farm (Fig. 12). Although thisschool is in a hill tribe community, it won the
CONSTRUCTION OF MODULES FOR INTERNATIONAL COOPERATION METHOD IN SCHOOL HEALTH
Fig. 8 After slope improvement Fig. 9 Construction of fish culture pond
Fig. 10 Harvesting in a farm Fig. 11 Vegetables harvested in a farm
Fig. 12 Paddy field completed

158 JMAJ, May/June 2008 — Vol. 51, No. 3
second prize in school health competition inChiang Mai Province last year. The school thatwon the first prize also developed HQC activities.This school is engaging in the improvementactivities so enthusiastically that it dispatches ateacher to the next district to give guidance onimprovement activities.
Conclusion
This school health improvement program requireseasy tests and skills any non-expert can carry out
in a school setting. It consists of various activities,so that effects can be expected in various phases;from the day the program starts to several weeksor several months later. The method, to which thisQC is applied, can not only improve school healthin a sustainable way in any area at a moderateprice, but can also improve the whole school.Furthermore, it can develop into environmentaleducation and other life-style improvements inthe local community. In the future, methods forsolving issues more closely related to the localcommunity should be formulated.
References
1. Ohsawa S. Health quality control and life styles. Kenkou Kyositu.1980;479:4–18. (in Japanese)
2. Nakano T, Nishijima T, Ohsawa S. Proposal for the improvementof life style with regard to school health in Thailand using theHQC method. School Health. 2005;1:15–21.
3. Nakano T, Ohsawa S, Sagawa T. An examination of the period
when an effect of the lifestyle improvement appears. Japan Jour-nal of Human Growth and Development Research. 2008;37:17–24. (in Japanese)
4. Overseas Vocational Training Association. Progressive systemfor instructors Prots manual. Kaigai Shokugyou Kunren Kyoukai;1989:1–40.
Ohsawa S

159JMAJ, May/June 2008 — Vol. 51, No. 3
Research and Reviews
dren have been identified according to the ratiobetween the measured body weight and the stan-dard body weight calculated from sex, age, andheight (degree of obesity), as specified in theManual for Health Examination of Children andStudents (Revised Edition) published by theJapanese Society of School Health in March2006. Children with a ratio of 120% or more areconsidered overweight, while those with a ratioof 80% or less are considered underweight.
According to this definition, the prevalence ofoverweight among boys was 2.6% at age 5, 11.8%at age 11, 11.2% at age 14, and 12.9% at age 17;that among girls was 3.0% at age 5, 10.0% at age11, 9.2% at age 14, and 9.7% at age 17. On theother hand, the prevalence of underweightamong boys was 0.4% at age 5, 2.5% at age 11,
Development and Health Status ofChildren and Students
The Ministry of Education, Culture, Sports,Science and Technology (MEXT) is regularlyconducting a “school health statistics survey” tocharacterize the development and health statusof children, students, and infants on a yearly basis.In the following sections, we review the develop-ment and health status of children based on theresults of the report on the 2006 school healthstatistics survey published in March 2007.
Prevalence of overweight and underweightchildrenFrom 2006, overweight and underweight chil-
*1 School Health Education Division, Sports and Youth Bureau, Ministry of Education, Culture, Sports, Science and Technology, Tokyo, Japan(Present affiliation: Blood and Blood Products Division, Pharmaceutical and Food Safety Bureau, Ministry of Health, Labor and Welfare; email:[email protected]).
Recent Issues in Administrative Measures forSchool Health Education
JMAJ 51(3): 159–163, 2008
Shusho OKADA*1
AbstractSchool health in Japan is now undergoing a period of transition. While the traditional focus of school health hasbeen the management of infectious diseases including tuberculosis and parasitism, dental caries, and heart andkidney diseases, we are now seeing the emergence of mental health, allergic diseases, and obesity as centralissues reflecting recent changes in the health problems of schoolchildren and students.
These new health issues may not be addressed effectively with the conventional methodology of healthmanagement centered on regular health examination conducted by school doctors and yogo teachers (schoolnurse-teachers). Finely tuned cooperation among teachers and other school employees, guardians, and medicalpractitioners and medical institutions (various clinical departments) in the community is essentially needed forsolution of these problems.
Since 2004, the national government and the Ministry of Education, Culture, Sports, Science and Technologyhave been promoting the School-Community Health Collaboration Program to induce a shift from school healthactivities in a school to those open to the community, and this effort has been making steady progress.
For the future, we are endeavoring to promote school health measures responding to modern health problemsof schoolchildren and students, including the amendment of the School Health Law providing the basis forschool health.
Key words School health, Allergic disease, Mental health, Metabolic syndrome, School doctor

160 JMAJ, May/June 2008 — Vol. 51, No. 3
1.5% at age 14, and 1.4% at age 17; that amonggirls was 0.4% at age 5, 2.5% at age 11, 2.8% atage 14, and 1.2% at age 17.
Prevalence of leading diseases andabnormalities (Table 1)The statistics for the prevalence of various dis-eases and abnormalities show that the mostprevalent condition is “tooth decay (dentalcaries)” at all school levels, followed by “unaidedvision below 1.0.”
Okada S
Recent Issues in AdministrativeMeasures for School Health Education
Infectious disease control at schoolsRecent global epidemics of highly pathogenicavian influenza (H5N1) and the repeated spo-radic reports of infection to humans have causedconcern about the possible emergence of newtypes of influenza. According to the announce-ment of the World Health Organization (WHO),human cases of highly pathogenic avian influenza(H5N1) reported since November 2003 include
Table 1 Summary of trends in leading diseases and abnormalities(%)
Unaided Nose Oral and Toothvision Ear and throat decay ECG Protein ParasiteDivision below disease sinus disease (dental abnormality excretion eggs Asthma
1.0 disease and caries)abnormality
Preschool 1996 21.4 1.7 2.7 3.6 73.7 — 0.5 1.3 1.0
2002 26.5 2.0 3.5 2.4 61.5 — 0.4 0.4 1.3
2003 25.3 2.2 3.0 3.2 58.8 — 0.3 0.4 1.5
2004 20.8 1.8 2.7 2.3 56.9 — 0.6 0.3 1.3
2005 20.4 2.1 3.2 2.0 54.4 — 0.6 0.2 1.6
2006 24.1 2.9 3.4 2.0 55.2 — 0.5 0.2 2.4
Elementary 1996 25.8 3.6 10.0 2.3 85.7 2.0 0.6 2.6 1.6school 2002 25.7 4.3 11.2 2.2 73.9 2.2 0.6 0.9 2.7
2003 25.6 4.5 11.1 2.2 71.3 2.3 0.6 0.8 2.9
2004 25.6 4.3 10.4 1.9 70.4 2.5 0.6 0.7 3.1
2005 26.5 4.5 11.2 1.9 68.2 2.4 0.6 0.5 3.3
2006 28.4 4.9 11.9 1.9 67.8 2.3 0.7 0.5 3.7
Junior high 1996 49.8 1.9 7.8 1.2 84.8 2.6 1.9 — 1.5school 2002 49.0 2.6 9.4 1.3 71.2 3.1 2.1 — 2.2
2003 47.8 2.7 10.1 1.2 67.7 3.5 1.9 — 2.3
2004 47.7 2.7 9.3 1.1 64.6 3.3 2.0 — 2.4
2005 47.8 2.8 10.6 12 62.7 3.2 2.1 — 2.7
2006 50.1 3.1 10.7 1.1 59.7 3.3 2.3 — 3.0
High school 1996 62.7 0.9 5.9 0.8 90.1 2.6 1.8 — 0.8
2002 63.8 1.7 7.7 0.8 82.3 3.1 1.8 — 1.4
2003 60.0 1.2 7.4 0.8 77.9 3.3 1.7 — 1.3
2004 59.3 1.3 6.8 0.7 76.0 3.3 1.9 — 1.5
2005 58.4 1.3 8.1 0.8 72.8 3.2 1.8 — 1.7
2006 58.7 1.7 8.2 0.7 70.1 3.5 2.4 — 1.7
Notes: 1. Figures have been rounded to the first decimal place.2. ECG abnormality is examined only at ages 6, 12, and 15.3. The tests for Parasite eggs are conducted only at ages from 5 to 8.
(Quoted from the Report of 2006 School Statistics Survey, MEXT.)

161JMAJ, May/June 2008 — Vol. 51, No. 3
RECENT ISSUES IN ADMINISTRATIVE MEASURES FOR SCHOOL HEALTH EDUCATION
281 patients (169 deaths) in 12 countries as ofMarch 20, 2007.
In Japan, the government has been makingconcerted efforts to address this problem basedon the Pandemic Influenza Preparedness ActionPlan issued in December 2005.
MEXT formulated the MEXT Action Plan forPhase 4 and Later Influenza Control1 in Septem-ber 2006. This plan specifies what MEXT requestslocal education boards and other relevant orga-nizations to do in phase 4 (outbreak of new typeinfluenza) and later phases, as well as instructionsregarding the survey and research that must beconducted urgently at relevant research institu-tions and the instructions to children and studentsattending Japanese schools.
The Enforcement Order relating to the Infec-tious Disease Prevention Law was amended inJune 2006, and in response the EnforcementRegulations relating to the School Health Lawwere amended. The regulations after amendmentclassify influenza (H5N1) as a class 1 infectiousdisease in the list of infectious diseases requiringpreventive actions at schools. In addition, throughissuance of notice to schools via local educationboards, MEXT is calling for actions such asencouraging children and students to performmouth and hand washing, developing a systemfor communication among schools, and improv-ing the distribution of information to parents.
Allergic diseasesMEXT established the Research Committee onAllergic Diseases consisting of relevant expertsin October 2004, in response to the increase inthe number of children and students with asthma
reported in the School Health Statistics Surveyand the increase in allergic diseases among chil-dren revealed in other epidemiological studies.The Committee conducted a nationwide survey,conducted analysis and evaluation of results, anddeveloped future plans. A report was publishedin April 2007.
The survey conducted in this research projectwas a complete count survey covering 36,830public elementary schools, junior high schools,high schools, and secondary schools (12.77 millionchildren and students). Survey forms were dis-tributed to schools via local education boards inDecember 2004, and the data as of the end ofJune 2004 were collected. The survey investi-gated (1) the present state of allergic diseasesamong children and students, and (2) the currentactions taken at each school against each disease.
The results of the survey regarding (1) thepresent status of allergic diseases among childrenand students are summarized in Fig. 1 showing theprevalence of allergic diseases among all childrenand students. Please visit the MEXT website(http://www.mext.go.jp/b_menu/houdou/19/04/07041301.htm) for more detailed information.
Regarding (2) the current actions taken ateach school against each allergic disease, the sur-vey investigated various actions taken at schoolsagainst allergic diseases. The following summa-rizes the survey results and the evaluation andanalysis of results.• Asthma. Only 58% of all schools are prepared
for emergency response. Schools need to ensurethat teachers and school personnel know emer-gency care and the procedure for requestingambulance transport in the event of a serious
(Quoted from the Research Report on Allergy Diseases, MEXT, March 2007.)
Fig. 1 Prevalence of allergic diseases among all children and students
(%)
10.0
8.0
6.0
4.0
2.0
0.0Asthma
5.7
Atopicdermatitis
5.5
Allergicrhinitis
9.2
Allergicconjunctivitis
3.5
Flood allegy
2.6
Anaphylaxis
0.14

162 JMAJ, May/June 2008 — Vol. 51, No. 3
asthma attack.• Atopic dermatitis. Only 46% of all schools are
using precautions in physical education andother classes. It is important that teachers andschool personnel understand the basic knowl-edge that sweat, ultraviolet light, swimmingpool disinfectants, etc. may aggravate the condi-tions of children and students with atopic der-matitis and appropriate precautions are taken.
• Food allergy. Over 80% of elementary andjunior high schools with a complete schoollunch service are taking precautions in pro-viding school lunches. The most importantpoint is to prevent allergic symptoms resultingfrom school lunches. For this purpose, schoolsshould promote measures such as the provisionof alternative menus according to the physician’sjudgment of the need for food avoidance anddepending on the actual situation of each school.
• Anaphylaxis. Only 13% of all schools are pro-viding places for safekeeping of medications.Self-injectable drugs are sometimes prescribedto children and students with a history of ana-phylaxis, so that they can inject the drugs whenthey experience premonitory symptoms. Theprovision of places for safekeeping of medi-cations, as well as safekeeping of medications byschool personnel, benefits such children andstudents. An effective step for promoting suchmeasures is to establish standard methodsthrough investigation and analysis of leadingcases, focusing on concrete methods used in suchcases and what the school and parents need todiscuss before implementing such measures.
After the presentation of survey results andevaluation, this report provided the followingconclusions.• Allergic diseases are not rare among children
and students. School healthcare should be con-sidered on the assumption that there are chil-dren and students with various allergic diseasesin schools and classes.
• Based on this recognition, actions to addressallergic diseases should aim at the followinggoals.(1) To establish a mechanism ensuring that the
actions for individual children and studentsare based on the instructions of physicians.
(2) To ensure that various actions at schools arebased on medical evidence and implementedin a safe, reliable, and efficient manner.
The Committee further provided the follow-
ing recommendations to improve the presentsituation.
(1) Establishment of a mechanism centered onthe “School Life Management GuidanceForm” incorporating response to allergicdiseases.
(2) Study on the implementation methods ofvarious measures based on investigation andanalysis of leading cases.
Mental health problemsTo address the aggravating mental health prob-lems in children, MEXT established the MentalHealth Building Committee under the JapaneseSociety of School Health. The Committee con-ducted the Survey on Mental Health Buildingcovering elementary, junior high, and highschools across Japan to grasp the present situa-tion and identify problems, and investigated waysof improving the organizational mechanismswithin schools and collaboration with relevantorganizations in the community.
According to the Survey on Mental HealthBuilding, “the percentage of schools in whichthere were children who received direct supportconsidered necessary by school nurses” was78.0% of elementary schools, 95.3% of juniorhigh schools, and 95.4% of high schools. The mostcommonly observed problems included “prob-lems of personal relationships with friends,family, etc.”; “problems of school refusal, stayingin the infirmary, unwillingness to attend school,withdrawal, etc.”; “problems of maladjustment togroup life such as mild developmental disability”;and “problems related to sex.” The survey on “thenumber of children who actually sought medicalcare after recommendation from school nurses”showed that elementary school children visitedpediatricians, institutions operated by localeducation boards, and psychosomatic medicineclinics in decreasing order; junior high schoolstudents visited psychosomatic medicine clinics,psychiatrists, and pediatricians in decreasingorder; and high school students visited psychoso-matic medicine clinics, psychiatrists, and internalmedicine clinics in decreasing order. “The percen-tage of schools in which there were children whoreceived support for problems related to mentalhealth” was 13.3% of elementary schools, 11.8%of junior high schools, and 15.5% of high schools.
Based on these results, the Committeeconcluded that enrichment of organizational
Okada S

163JMAJ, May/June 2008 — Vol. 51, No. 3
References
1. MEXT. The MEXT action plan for phase 4 and later influenzacontrol. 2006 Sep 19. http://www.mext.go.jp/b_menu/houdou/18/09/06091515.htm. (in Japanese)
mechanisms within schools and strengtheningof collaboration with relevant organizationsin the community are essential to the actionsfor addressing the mental health problems ofchildren.
School and Community HealthCollaboration Program
From Fiscal 2004, MEXT has been promotingthe School and Community Health Collabora-tion Program in cooperation with local medicalassociations and other relevant organizations. Inthis Program, specialist physicians (psychiatry,obstetrics and gynecology, orthopedics, derma-tology, etc.) are sent to schools responding to therequest from schools, guidance and advice aregiven to teachers and school personnel, andhealth counseling and health education relatedto the mental and physical health of children areprovided.
Initiated as a model program intended to helppromote school and community health collabo-ration for the future, this program was imple-mented in all prefectures in 2005, and is stillcontinued as of 2007.
The specialist physicians sent to schools inFiscal 2005 were psychiatrists, obstetricians/gynecologists, orthopedists, dermatologists, andpediatricians in decreasing order. They servedas lecturers at seminars for teachers and schoolpersonnel, and also provided health counselingfor parents, children, and students.
Future School Health Activities
Changes in health issuesSchool healthcare has long been dealing withinfections, dental caries, heart disease, kidney
disease, and other disorders as the main prob-lems affecting child and student health. Thesedisorders will remain an important focus ofschool healthcare. However, in addition to thesephysical disorders, mental health problems havebeen emerging in recent years.
Changes are occurring even in physical dis-orders. We are now faced with the threat of pre-viously unknown infections with the potential ofserious social impact, such as new type influenza.Responses to modern problems such as allergicdiseases and obesity are also needed urgently.
Strengthening school and communitycollaborationWith the dramatic changes in the problems ofchild and student health, school healthcare isrequired to promote actions based on evidence inthe same sense as that in medical care. To be ableto cope with various health issues at schools, weneed new methodologies crossing conventionalborders, including the strengthening of schooland community collaboration.
In particular, the response to modern issuessuch as mental health problems and allergic dis-eases requires increased involvement of specialists.While we are now promoting the School andCommunity Health Collaboration Program as amodel program, we need to analyze the resultsachieved so far and identify better ways forschool and community health collaboration.
At the same time, school healthcare within theconventional framework should also be enrichedfurther to keep up with the expectations of thechildren, students, and parents. A particular arearequiring special attention in this endeavor isthe protection of personal information and theprivacy of children and students.
RECENT ISSUES IN ADMINISTRATIVE MEASURES FOR SCHOOL HEALTH EDUCATION

164 JMAJ, May/June 2008 — Vol. 51, No. 3
Research and Reviews
The blame on the school hurts teachers andundermines their effectiveness in protectingchildren, while the hunt for the culprit impelschildren to reproach one another. This is a sadsituation. Although evasion of responsibility isby no means acceptable, what we need to protectchildren in the first instance is cooperation of theschool, families, and communities.
The school and the education board aredemanded to account for the incident or accidentthat has already happened. In such a case, anexternal crisis response team (CRT) independentof schools and education boards can provideeffective support. The name “CRT” was takenfrom that of similar organizations in the UnitedStates,1–3 and we adopted the basic concept of“sending a specialist team for a limited periodmainly to support caretakers.” However, CRTsin Japan are organized on a prefectural basis,and their activities are limited to schools for thetime being.
Introduction
Suicides of young students involving problems ofbullying frequently made the headlines in 2006,and schools and education boards often becamethe target of criticism. There is no differenceamong a school, an enterprise, and a hospital inthe importance of crisis management in the eventof a serious criminal incident or an accident.Due to the very nature of a crisis, poor responseto an event tends to cause a chain of secondaryproblems and lead to expansion of damage. Arush of mass media reporters, sorrow and angerof the bereaved, growing distrust of parents, andfatigue of teachers and school personnel form avicious spiral, and the most important cause of“protecting children” may be left behind.
The general public blames the school forallowing the incident to happen, and hastily looksfor the cause, asking, “who bullied the victim?”
*1 This is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Separate Vol.136, No.4, 2007,pages 39–42). The article is based on a presentation made at the School Doctor Seminar hosted by the Japan Medical Association at the JMAHall on February 24, 2007.*2 Director, Yamaguchi Prefectural Mental Health Center, Hofu, Japan ([email protected]).
School Crisis and Mental Care—The crisis response team (CRT)*1
JMAJ 51(3): 164–168, 2008
Michihide KAWANO*2
AbstractIn 2001, a man with a knife walked into an elementary school in Japan and killed 8 students. Triggered by thistragic incident, mental health specialists in Yamaguchi Prefecture organized a rescue team for mental care, calleda crisis response team (CRT), in 2003. CRTs were subsequently organized also in Nagasaki, Shizuoka, andWakayama Prefectures. A CRT is a team of consisting of specialists such as psychiatrists, clinical psychologists,psychiatric social workers, public health nurses, and nurses. During the period of up to 3 days following theoccurrence of an emergency incident, they support the crisis management by schools and education boards, andprovide emergency mental care. A CRT is an external team working independently of schools and educationboards. The Prefectural Mental Health Center serves as the headquarters of CRT. Providing support from anexternal team within a limited time span is considered an effective means to deal with serious accidents or criminalincidents in schools.
Key words Crisis response team, Crises in schools, Trauma, Mental health center
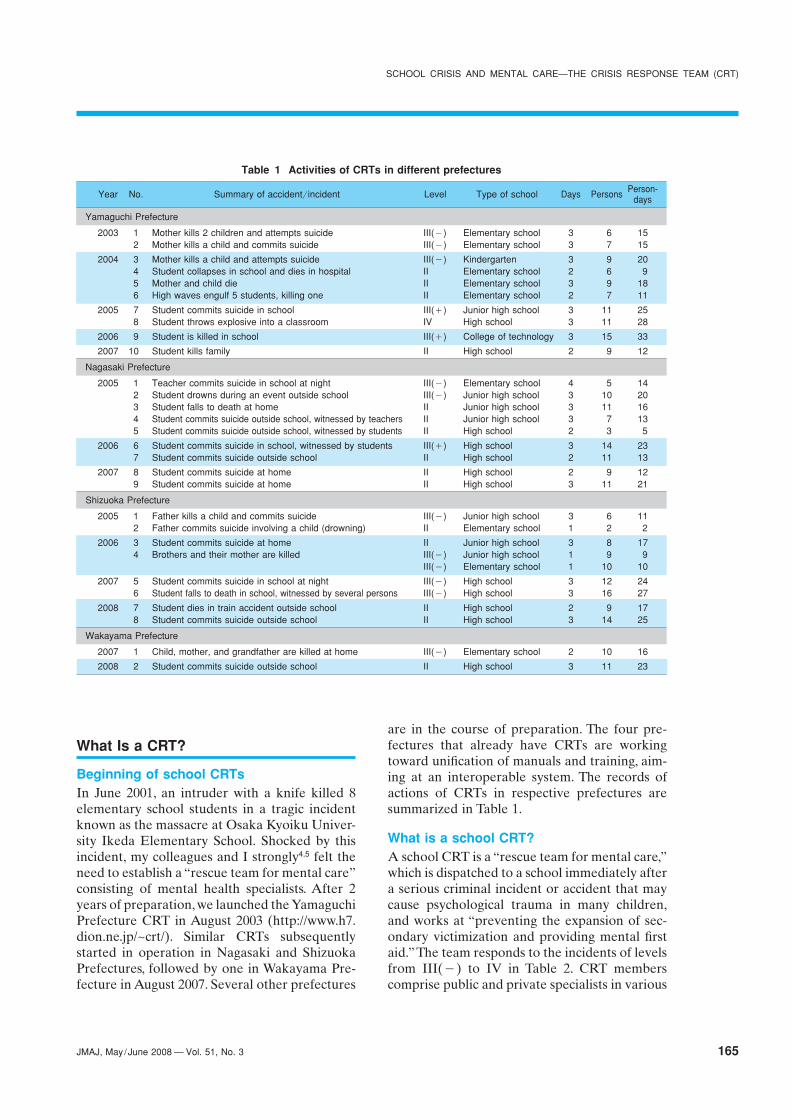
165JMAJ, May/June 2008 — Vol. 51, No. 3
What Is a CRT?
Beginning of school CRTsIn June 2001, an intruder with a knife killed 8elementary school students in a tragic incidentknown as the massacre at Osaka Kyoiku Univer-sity Ikeda Elementary School. Shocked by thisincident, my colleagues and I strongly4,5 felt theneed to establish a “rescue team for mental care”consisting of mental health specialists. After 2years of preparation, we launched the YamaguchiPrefecture CRT in August 2003 (http://www.h7.dion.ne.jp/~crt/). Similar CRTs subsequentlystarted in operation in Nagasaki and ShizuokaPrefectures, followed by one in Wakayama Pre-fecture in August 2007. Several other prefectures
are in the course of preparation. The four pre-fectures that already have CRTs are workingtoward unification of manuals and training, aim-ing at an interoperable system. The records ofactions of CRTs in respective prefectures aresummarized in Table 1.
What is a school CRT?A school CRT is a “rescue team for mental care,”which is dispatched to a school immediately aftera serious criminal incident or accident that maycause psychological trauma in many children,and works at “preventing the expansion of sec-ondary victimization and providing mental firstaid.” The team responds to the incidents of levelsfrom III(�) to IV in Table 2. CRT memberscomprise public and private specialists in various
Table 1 Activities of CRTs in different prefectures
Year No. Summary of accident/incident Level Type of school Days Persons Person-days
Yamaguchi Prefecture
2003 1 Mother kills 2 children and attempts suicide III(�) Elementary school 3 6 152 Mother kills a child and commits suicide III(�) Elementary school 3 7 15
2004 3 Mother kills a child and attempts suicide III(�) Kindergarten 3 9 204 Student collapses in school and dies in hospital II Elementary school 2 6 95 Mother and child die II Elementary school 3 9 186 High waves engulf 5 students, killing one II Elementary school 2 7 11
2005 7 Student commits suicide in school III(�) Junior high school 3 11 258 Student throws explosive into a classroom IV High school 3 11 28
2006 9 Student is killed in school III(�) College of technology 3 15 33
2007 10 Student kills family II High school 2 9 12
Nagasaki Prefecture
2005 1 Teacher commits suicide in school at night III(�) Elementary school 4 5 142 Student drowns during an event outside school III(�) Junior high school 3 10 203 Student falls to death at home II Junior high school 3 11 164 Student commits suicide outside school, witnessed by teachers II Junior high school 3 7 135 Student commits suicide outside school, witnessed by students II High school 2 3 5
2006 6 Student commits suicide in school, witnessed by students III(�) High school 3 14 237 Student commits suicide outside school II High school 2 11 13
2007 8 Student commits suicide at home II High school 2 9 129 Student commits suicide at home II High school 3 11 21
Shizuoka Prefecture
2005 1 Father kills a child and commits suicide III(�) Junior high school 3 6 112 Father commits suicide involving a child (drowning) II Elementary school 1 2 2
2006 3 Student commits suicide at home II Junior high school 3 8 174 Brothers and their mother are killed III(�) Junior high school 1 9 9
III(�) Elementary school 1 10 10
2007 5 Student commits suicide in school at night III(�) High school 3 12 246 Student falls to death in school, witnessed by several persons III(�) High school 3 16 27
2008 7 Student dies in train accident outside school II High school 2 9 178 Student commits suicide outside school II High school 3 14 25
Wakayama Prefecture
2007 1 Child, mother, and grandfather are killed at home III(�) Elementary school 2 10 16
2008 2 Student commits suicide outside school II High school 3 11 23
SCHOOL CRISIS AND MENTAL CARE—THE CRISIS RESPONSE TEAM (CRT)

166 JMAJ, May/June 2008 — Vol. 51, No. 3
vocations including psychiatrists, clinical psy-chologists, mental health workers, public healthnurses, and nurses, etc. The Mental Health Centerserves as the headquarters of CRT. The team is anexternal organization independent of educationboards.
Developing the system for the response tolocal disasters and other incidents outsideschools is an issue that must be addressed in thefuture. For the time being, we need to developa workforce with sufficient crisis response capa-bility through accumulation of experiences inschool crisis response. The ability to deal withunpredictable contingency, which is required incrisis response, is not developed merely frommanuals and exercises. We can have veteransamong CRT members only after the team hasbeen active for a few years and experiencedseveral turnouts.
The following describes the support providedby the CRT.
Support Provided by the CRT
Advice to the headmasterLeadership is important in a crisis. Therefore, theCRT first of all supports the headmaster. Thecaptain of the CRT stays with the headmasterand gives advice whenever needed.
Advice and support to teachers and schoolpersonnelTeachers must remain calm and be able to react
appropriately. Therefore, the CRT approachesteachers before it approaches children. The teamhelps teachers solve problems, gives advice regard-ing the response to children’s needs, and evenprovides counseling to teachers. The memberssometimes enter classrooms and infirmaries insupport of teachers. They evaluate the damage tochildren and develop a care plan. In addition,they hold a meeting of teachers and give lectureson what to do for children (psychological educa-tion). It is not recommendable to hold a largemeeting on the first day children attend schoolafter the incident, as panic may spread from childto child and an uncontrollable situation may result.
Support to parents attending childrenMany of the children who were not directlyharmed and did not witness the incident areexpected to stabilize, if the parents remain com-posed and provide appropriate care. Specialistsshould tell parents what to do for their children(psychological education) on occasions such asthe meeting of parents held by the school.Parents should be instructed: “When the childis trying to speak, listen attentively and do notchange the subject”; “If the child is not willing tospeak, do not be inquisitive and say, ‘I will be herefor you whenever you want to talk’”; and “Chil-dren feeling strong anxiety can be paradoxicallyhigh-spirited. So, do not scold them.”
In the cases involving fatalities, the team advisesthe school on the relations with the bereaved andthe participation in funerals.
Table 2 Levels of school crises
Level Example
VI Terrorist attack at the school in North Ossetia
V An intruder kills 8 elementary school students at Osaka Kyoiku University Ikeda Elementary School
IV An elementary school student kills a classmate using a snap cutter at an elementary school in Nagasaki Prefecture
A high school student throws explosive into classroom at a high school in Yamaguchi Prefecture, injuring 58 persons (17 hospitalized)
III(�) A junior high student commits suicide by jumping in school, witnessed by many
An elementary school student drowns to death in the school’s swimming pool, witnessed by many students
III(�) A parent kills his or her child and many media reporters gather in the school
II A student collapses and dies after being sent to hospital
I A student dies in traffic accident during a family trip
CRTs are dispatched in response to incidents from level III(�) to level IV.
Kawano M

167JMAJ, May/June 2008 — Vol. 51, No. 3
Emergency responses for children andparentsEnsuring the stability of the school communityas a whole through the above actions, the teamapproaches the cases requiring individualizedcare. Face-to-face counseling and telephonecounseling are provided on request. Cases requir-ing continued care are handed over to schoolcounselors for follow-up. If medical care is needed,students are advised to visit medical institutions,and school doctors may also play important rolesas the most accessible care providers. In additionto treating patients, school doctors are expectedto help relieve the anxiety of parents, cooperatewith the school, and make referral to psychiatriccare, as required.
Support in media relationsSchool managers are busy with the nerve-wrackingtask of dealing with the onslaught of mass media.The CRT supports the school and the educationboard in media relations to facilitate faithful andproactive disclosure of information. Announce-ments regarding the specific description of mentalcare are given directly from the CRT.
Problems and Proposals
Strengthening the crisis response capabilitiesof schools and education boardsThe education board needs to dispatch an overlysufficient number of personnel immediately. Thenumber of persons needed during the first 3 days(excluding specialists), according to past experi-ence, is as follows.
Level IV crisis:4 or more persons at any time
Level III(�) crisis:3 or more persons at any time
Level II and III(�) crisis:2 or more persons at any time
Most public elementary and junior highschools in Japan are under the control of munici-pal education boards. Level III or more severeincidents occur only at a rate of 1 or 2 times peryear in a rural prefecture with a population of1 million, whereas individual personnel stay ina position only for a few years. The educationboards of smaller municipalities, therefore, havedifficulty in gaining expertise through experi-ence. As first-hand experience makes a differ-
ence in crisis response, it is important that theprefectural education boards dispatch personneland let them gain first-hand experience. In thisway, the prefectural education board should main-tain a workforce with sufficient crisis responsecapabilities.
Enrichment of mental care provided byschools and education boardsIn Japan, school counselors (usually part-timeworkers serving 1–2 times a week) are posted atmany public junior high schools and some otherschools. These school counselors generally havesufficient capability for the mental care after alevel I incident. In the case of level II and moresevere incidents, the education board would haveto dispatch specialists including school counse-lors. In practice, rural prefectures are short ofspecialists and would have difficulty in musteringspecialists. If the number of specialists dispatchedwere insufficient, the burden on them would beexcessively large. In addition, there is a funda-mental problem that specialists under the direc-tion of the education board cannot effectivelyplay the leading role that they should performas specialists. In Fukuoka Prefecture,6 an emer-gency support system has been established withthe cooperation of Fukuoka Society of CertifiedClinical Psychologists. However, this methodimposes a heavy burden on specialists, and itsapplicability is limited to highly populated areassuch as Fukuoka, Chiba, and Kyoto Prefectures.
External support from the CRTThe dispatch of the CRT as an external team isdesirable in the case of level III and severerincidents. The CRT is a team specializing in theinitial response to “level III and more severeincidents for 3 days at the maximum.” It is notdispatched in level II or lesser incidents. TheCRT of Yamaguchi Prefecture begins on-sitesupport within 4 hours of a request. The durationof service is limited to 3 days because of thephysical and mental limits of team members, asmembers need to return to their usual work andfamily life and prepare for the next turnout. Thisrestriction also prevents the overdependence ofschools. When members are dispatched, they areremoved from their usual work, and this maycause a great deal of trouble to the organizationsthey belong to. We deeply appreciate their under-standing and cooperation.
SCHOOL CRISIS AND MENTAL CARE—THE CRISIS RESPONSE TEAM (CRT)

168 JMAJ, May/June 2008 — Vol. 51, No. 3
As a CRT is a mixed team consisting of vari-ous professionals belonging to different publicand private organizations, fostering a strongsense of teamwork through routine practice isessential. It is the ties among team members thatprotect them from intense stress. It should beemphasized that every member more or lesssuffers from a degree of secondary traumatiza-tion as a result of exposure to the psychologicaltrauma of others.
The number of members to be dispatched isdetermined by the CRT. For example, a level IVincident requires 15 or more specialists (includ-ing CRT members and school counselors) perday. The CRT comprises members performingthree types of activities: command, mental care,and logistics support. The members in charge ofcommand make decisions on important issues,discuss with the principal, and interact with themass media. The members in charge of mentalcare give advice to teachers and provide indi-vidualized care to children and parents. Those incharge of logistics support perform service andsupport activities focusing on logistics includingrecording, documentation, assistance in counsel-ing, and preparation of meals.
The mental care for a traumatized child oftenextends over a year or more. The school and theeducation board should take responsibility for
providing specialists such as school counselorsfor mid- and long-term care after the withdrawalof the CRT. However, a school is primarily theplace for education rather than therapy, andspecialists are too busy to work for long periodson an outreach basis. For these reasons, childrenrequiring therapeutic care should basically betreated at medical institutions.
Conclusion
A CRT is an external team, which is not estab-lished by the education board. In the administra-tive system, it is organized under the lead of thehealth and welfare department. However, simplyallocating a budget does not put the team intooperation. The enthusiasm and techniques of usspecialists are crucially required. Of course, CRTsdo not take over the responsibilities of schoolsand education boards. Parents and inhabitants inthe community should also stand up and takeaction to protect children, without leaving thematter to schools and specialists. A CRT canprove its worth only through a widespread move-ment in which specialists, local governments,schools and education boards, and parents andinhabitants “carry out their responsibility” and“do what they can.”
References
1. Johnson K. Crisis response to schools. Int J Emerg Ment Health.2000;2(3):173–180.
2. Kline M, Schonfeld DJ, Lichtenstein R. Benefits and challengesof school-based crisis response teams. J Sch Health. 1995;65(7):245–249.
3. Eaves C. The development and implementation of a crisisresponse team in a school setting. Int J Emerg Ment Health.2001;3(1):35–46.
4. Kawano M. Activities of the crisis response team (CRT)—Anattempt in Yamaguchi Prefecture. In: Fujimori K ed. Psychologi-
cal Traumas in Schools and Mental Care for Children. Practice.For Teachers, School Nurses, and School Counselors. Tokyo:Seishin Shobo; 2005:136–157. (in Japanese)
5. Fujimori K. Crisis intervention in schools. Study group on post-traumatic stress-related disorders. In: Kin Y ed. Understandingand Care of Psychological Trauma, 2nd ed. Tokyo: Jihou; 2006:183–209. (in Japanese)
6. Kubota Y, Mukasa A, Hayashi M, et al. Guidebook on Emer-gency Support to School Community. Tokyo: Kongo Shuppan;2005. (in Japanese)
Kawano M

169JMAJ, May/June 2008 — Vol. 51, No. 3
Research and Reviews
sooner or later.The high-growth period following the post-
war WWII restoration in Japan continued until itwas checked by two oil shocks and the PlazaAgreement. Overcoming these adversities, theeconomy entered the bubble era. The collapse ofthe bubble in 1991 marked the beginning of thelong period of sluggish economy. In and around1993, companies started to undergo drastic restruc-turing, and M&As (mergers and acquisitions)became common. The systems of lifetime employ-ment and seniority, considered the secret ofsuccess for the post-war Japanese economy,faded out following the collapse of the bubbleeconomy. A dramatic transformation of compa-nies took place not only in Japan but also in othercountries as their economies globalized. However,the changes in Japan were particularly suddenand extensive. The globalization of the economy
Introduction
As mental health problems spread among sociallyweak people in a “society with widening dispari-ties,” mental health in the workplace is becominga critical issue. The problem is how to supportsuch people. They need individualized support,because they have become socially weak as a resultof various background factors and there are nostandardized measures that apply to all people.Drug treatments are effective for depression,anxiety, and other conditions occurring as reac-tions to underlying causes, and such treatmentscan achieve temporary recovery from mentalhealth problems. However, unless measures aretaken to modify the causative factors in the work-place and the individuals’ ability to cope withstress, symptoms are likely to return and patientswill suffer a relapse of mental health problems
*1 Professor, Department of Clinical Psychology, Kyoto Bunkyo University. Industrial Mental Health Institute, Kanda-Higashi Clinic, Tokyo, Japan([email protected]).This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.136, No.1, 2007,pages 19–24).
Present State and Issues of Workplace MentalHealth
JMAJ 51(3): 169–174, 2008
Satoru SHIMA*1
AbstractAfter the collapse of the bubble economy, dramatic changes have occurred in the environment around workers,including those in the labor market and personnel management systems. According to the Worker Health Survey,the percentage of workers feeling stress continued to increase until 1997, but the increase stopped in 2002. Theleading cause of stress is interpersonal relations in the workplace, followed by the nature of the job and thevolume of work. The number of suicides in Japan has exceeded 30,000 for 8 consecutive years. Middle- and high-aged workers suffering from economic difficulties, struggling workers in their 30s, and delicate young workers arepresenting serious social problems. Mental health activities in industrial health have evolved from the Total HealthPromotion Plan to Creation of Comfortable Workplaces and then to the Guidelines for Promoting Mental Care inEnterprises. The guidelines indicate four types of care: self-care, line care, professional care, and outside care.The revised Mental Health Guidelines, based on the amended Occupational Safety and Health Law, comprehen-sively encompass from primary to tertiary prevention.
Key words Mental health, Suicide from overwork, Mental Health Guidelines, Industry, Stress

170 JMAJ, May/June 2008 — Vol. 51, No. 3
and the IT revolution, affecting all aspects ofpeople’s lives, has caused radical alterations inthe work environment, which seem to becomeeven more profound in the 21st century.
The metabolic syndrome, recently attractingkeen attention, is not unrelated to mental health.In the stressful life of today, some people resortto unhealthy eating habits such as overeating asa means of coping with stress, while many indi-viduals are working long hours without timefor leisure activities or physical exercise. Suchlifestyle is considered responsible for the devel-opment of metabolic syndrome. In other words,lifestyle factors that are emphasized in relation tometabolic syndrome are similarly important inmental health.
This article summarizes the present state andproblems of workplaces and workplace mentalhealth, and outlines the framework of measuresto promote mental health.
Work Environment of Today
After the collapse of the bubble economy in1991, dramatic changes occurred in the environ-ment around workers in Japan, including those inthe labor market and the personnel managementsystems of companies. The following changesoccurred in the work environment.
Changes in the employment environmentAfter the collapse of the bubble economy,demand in employment shrank as a result of thebusiness reorganization of companies. Manyfirms promoted payroll reduction through suchmeans as reducing the employment of contingentworkers, withholding the recruitment of newregular employees, loaning and transferring ofemployees, giving incentives for early retirement,and encouraging voluntary retirement. In 1997,many leading companies went bankrupt, nota-bly Yamaichi Securities Co., Ltd. and HokkaidoTakushoku Bank. As a result, the unemploymentrate soared from 2.1% in 1990 to 5.4% in 2002. Inthis situation, the suicide rate started to increasemarkedly in 1998.
The long period of restrained recruitment ofnew graduates or the ‘ice age of employment’ is afactor contributing to the increase in mentalhealth problems among workers who are in their30s now.
Shima S
Personnel management policiesAbout 10 years have passed since so-called results-oriented management was introduced as a pro-gressive approach. Although to differing extents,many companies are using results-oriented man-agement, which places much more importance onachieving final results than the processes (skills,knowledge, efforts, etc.) towards achievement,and rewards workers differently according toachievement. Naturally, this approach requiresgreater transparency and accountability regard-ing the evaluation of workers’ performance.
Results-oriented management gives a lot ofstress not only to the persons being evaluated butalso to the persons performing the evaluation.As a consequence of this change, managers,who used to rate workers almost uniformly inperformance assessment and evaluation, are nowforced to conduct more strict evaluation, makingit difficult for managers to perform their functionof “observing and supporting.” This is having aserious impact on the mental health of workers.
Employment systemsWhen an end was put to Japanese-style manage-ment, such as lifetime employment and theseniority system, workers experienced the loss ofthe quasi-family organization that had supportedthem and the stability of employment was under-mined. Workplaces nowadays consist of a mixtureof regular and contingent employees, who arereceiving very different treatment. This situationhas created a new type of stress involving inter-personal relations.
High skill levels, specs, and human abilitiesrequired for regular employeesSimple jobs that do not require a high skill levelare usually outsourced, particularly in large com-panies. On the other hand, regular employees arerequired to have high skill levels and specializa-tions. Aside from the need for computer literacy,employees are pressed continuously to learn newknowledge and skills reflecting the shorteninglife cycle of goods, and have no time to relax.Personnel changes including conversion to differ-ent job functions are also frequent. Even regularemployees with very short experience afterrecruitment are assigned the task of directing andmanaging temporary agency workers and part-time workers. In addition, the shift of industrial

171JMAJ, May/June 2008 — Vol. 51, No. 3
PRESENT STATE AND ISSUES OF WORKPLACE MENTAL HEALTH
structure to tertiary industries is increasing thenumber of occasions when workers need to com-municate with other people.
Present State of Stress and MentalHealth among Workers
Results of survey on stress in the workplaceAccording to the Worker Health Survey1 con-ducted by the Ministry of Health, Labour andWelfare at intervals of 5 years, the percentage ofworkers feeling stress increased steadily until1997, but the increase stopped and the percent-age in 2002 was similar to that in the previoussurvey. The leading cause of stress was interper-sonal relations in the workplace, followed by thenature and volume of the job. Workers are notgiven leeway in the workplace and interpersonalrelations are aggravating the situation with man-power reduction, increasing workload, and fluidi-zation of organization.
Present state of mental health of workersThe number of suicides in Japan has remained atabnormally high levels exceeding 30,000 for 8consecutive years from 1999. Nearly half of allcases committed suicide due to economic andlivelihood related problems including debts andthe hardships of life. This illustrates the continu-ing struggles of middle-aged and older citizens inthe face of economic hardships such as restruc-turing and unemployment. The high occurrenceof suicide among middle-aged and older workers“in the prime of life” is astounding. The closeassociation between suicide and mental dis-orders is widely acknowledged, and about 70% ofworkers committing suicide are reported to havedepression. Suicide from overwork with underly-ing depression is prevalent among middle-agedand older workers. Occupational stress arisingfrom chronically long overtime, underachieve-ment of the work quota, etc. is inferred to occurin the background. Please refer to my book2 fordiscussion regarding the suicide of workers.
The background factors to the mental healthproblems may differ from case-to-case, but thesecan be divided broadly into increasing stress,weakening support in the workplace and at home,and decreasing the stress resistance of individualworkers. Each of these involves serious problemsand solutions are not easy to find. In particular,the following issues need to be highlighted.
Middle-aged and older workers who find itdifficult to adjust to the timesThere are many cases of mental health problemsamong middle-aged and older workers who findit difficult to adjust to the dramatic changes inindustrial structure and workplace environment.Typical changes in the workplace environmentresult form business reorganization, forcingworkers to deal with different products and workin different job functions, and workers sufferfrom maladjustment in their efforts to performnew assignments. Middle-aged and older workerswith declining flexibility and adaptability are fail-ing to cope with the changing times.Struggling workers in their 30sWorkers who were recruited in the bubbleeconomy era, now in the 35–39 age range, are com-peting fiercely over the diminished number ofmanagerial posts. After years of friendly non-competitive relationships, they are now competingagainst colleagues of a similar age. On the otherhand, workers in the 30–34 age range, recruitedafter the collapse of the bubble economy, areunsure what to do before approaching the agelimit for a job change. As they were employed ata time when recruitment was extremely restrained,they have little chance of promotion. In the begin-ning, many of them started their careers againsttheir will in the ‘ice age of employment’ andare asking themselves whether their choiceswere right.Delicate young workersThe number of young workers with mentalhealth problems has been increasing over the lastseveral years. Generally described as being deli-cate, they develop mental health problems inresponse to slight problems in interpersonal rela-tions in the workplace or scolding from theirsuperiors as a result of their low resistance tostress. Many young workers have no experienceof being scolded, and are scolded in the work-place for the first time in their life. Managersoften complain that young workers cannot dothings that are not written in manuals, or cannoteven do the things that are written in manuals.While young workers were once described as“waiting for directions” (unable to act on theirown without directions from superiors), the situ-ation is further changing for the worse. In manycases, young workers are slow to recover aftertaking a rest, they are vulnerable, and their powerof self-healing from traumas is weak.

172 JMAJ, May/June 2008 — Vol. 51, No. 3
Mental Health Activities in IndustrialHealth
Originally, the basic aim of industrial health wasto maintain and promote mental and physicalhealth without directly addressing diseases andimpairments, and the focus was on primary pre-vention. However, mental health problems ofworkers and suicide apparently related to themcame to be regarded as a serious social problemin the later half of the 1990s, and this made itnecessary to include diseases in the coverage ofindustrial health. Mental health activities pro-moted by the national government in the area ofindustrial health have evolved from the TotalHealth Promotion Plan (THP) to the Creationof Comfortable Workplaces and then to theGuidelines for Promoting Mental Health Carein Enterprises (Mental Health Guidelines).
THP (1988)THP is the first government program that pavedthe way to the present mental health activities inworkplaces, and its concept of “mental and physi-cal health building” has proved an outstandingsuccess. The concept is to measure the health sta-tus of each person and use the results of measure-ment for exercise guidance, nutritional guidance,health guidance, and psychological counseling.The aim is the primary prevention of diseasesand the maintenance and promotion of health,similarly to the concept of special health exami-nation and special health guidance introducedin 2008 as a measure against the metabolic syn-drome. In this respect, industrial health has beena step ahead of community health.
Japan Industrial Safety & Health Associationis providing training courses for THP instructors,issuing certificates to persons completing pro-grams. In the field of mental health, the Associa-tion is training psychological counselors.
Creation of comfortable workplaces (1992)The program for the creation of comfortableworkplaces aims at improving organizations. Thenotion of comfort here has two meanings: one isthe comfort of the physical environment and theother is the psychological comfort chiefly con-cerning interpersonal relations in the workplace.This program for the creation of comfortableworkplaces and the THP for individual workers
are supposed to work in complementary roles inindustrial health. However, these have becomesomewhat insufficient in dealing with the mentalhealth problems of the present day.
Guidelines for promoting mental healthcare in enterprises (2000)3
These guidelines were formulated in response tothe rapid deterioration of workplace mentalhealth in and after 1990. Following the publica-tion of these guidelines, many companies havecome to exhibit much interest in mental healthmeasures, and the number of companies takingaction for mental health has certainly increased.Although national public servants are not coveredby these guidelines, the essence of the guidelineshas been reflected in the mental health measuresof National Personnel Authority governingnational public servants (see the information onthe NPA website, http://www.jinji.go.jp/kenkou_anzen/health_mentalpage.htm). Local govern-ment employees are also covered by the guide-lines, but they are not under its supervisingauthority. The guidelines indicate the followingfour types of care:(1) Self-care: While the need for self-care is con-
sidered a matter of course, it is often the casethat mental health problems may not beaddressed relying totally on the self-awarenessand self-help efforts of the workers them-selves. The awareness of disease is ofteninsufficient, some patients deny the presenceof disease, and there are persistent prejudicesamong some patients and their familiesagainst mental problems. Such prejudicesmust be eliminated through educationalactivities.
(2) Line care: This is the care provided by themanagers supervising workers in the businessorganization. It is very important that super-vising managers perceive the problems oftheir subordinates and provide care and sup-port to them. However, managers are in facttoo busy to take care of subordinate workers.As the term “game-playing manager” illus-trates, managers often have their own work,and are fatigued in all companies. Managerswho are supposed to provide care are actuallyin need of care from higher-up managers.Recent emphasis is therefore placed onthe care provided by leader workers undermanagers.
Shima S

173JMAJ, May/June 2008 — Vol. 51, No. 3
(3) Professional care by in-house industrial healthstaff, etc.: This is care provided by profes-sional staff including industrial physicians,public health nurses, nurses, counselors, healthsupervisors, and personnel/labor manage-ment staff in companies. The teamwork andcooperation between personnel/labor man-agement staff and industrial health staff areextremely important. At present, there aremore than 70,000 industrial physicians autho-rized by the Japan Medical Association.While an increasing number of physicians arechoosing a career as industrial physicians,there are few industrial physicians who areconversant with mental health.
(4) Care by outside resources: The collaborationwith outside resources (medical institutions,counseling organizations, etc.) is very impor-tant in practical case management, but suchcollaboration is not sufficient in the presentsituation. Clinicians in non-industrial settingsdo not have sufficient knowledge and under-standing of industrial health. Training in indus-trial health for psychiatrists started in 2004.Psychiatrists to take charge of patients havelittle time to spare and collaboration is oftenunpaid.
Partial amendment of the occupationalsafety and health lawIn October 2005, a bill amending part of theOccupational Safety and Health Law passed theDiet. This amendment was a measure against thepersistently high rates of death and suicide fromoverwork. It aimed to correct overworking, facili-tate early detection of health impairment fromoverwork, and prompt the patients to seek medi-cal care. Focusing mainly on cardiovascular dis-eases and mental disorders such as depression,a health screening is offered to persons whoare working more than 100 hours overtime permonth, feel accumulated fatigue, and want tohave an examination. They are advised to seektreatment, if considered necessary.
Guidelines for maintaining and promotingworker’s mental health (New Mental HealthGuidelines) (2006)4
Concurrently with the partial amendment of theOccupational Safety and Health Law, the MentalHealth Guidelines were also revised. While theseguidelines inherited the basic skeleton of the old
Mental Health Guidelines without majorchanges, several alterations were made to meetrecent needs. The key points are described below.(1) The guidelines are now prescribed by law:
This is the most important point of the newMental Health Guidelines. As they are basedon law, enterprises are required to follow theguidelines more strictly than before.
(2) Comprehensive guidelines including fromprimary to tertiary prevention: It is importantthat the new guidelines indicate more com-prehensive measures than the old guidelines.This amendment marked the completion ofthe framework of mental health measures inthe national policy for industrial health.
(3) Inclusion in the study agendas of health com-mittees: The amended Occupational Safetyand Health Law and the new Mental HealthGuidelines emphasize the use of health com-mittees and other relevant organizations. Theinclusion of mental health measures in thestudy agendas of such organizations meansthat enterprises are required to take effectivemeasures.
(4) Addition of face-to-face guidance to the tasksof industrial physicians: The amended Occu-pational Safety and Health Law and the newMental Health Guidelines added face-to-faceguidance to the tasks of industrial physicians.While the methods of interviews in mentalhealth do not differ much from those forpsychological and brain diseases, objectivefindings are scarcer in the case of mentalhealth. Therefore, information obtained dur-ing the interview should provide the basisfor judgment regarding immediate action forthe relevant worker.
(5) Reference to cooperation with families: Thesupport from family members to workers isextremely important. It is often the case thatthere are stress factors at home and the sup-port in the workplace alone may not be effec-tive. It is important to consider how to obtainsupport from families and how to cooperatewith families, and the new guidelines refer tothe support from families.
(6) New designation of in-house mental healthpromoters: The new guidelines newly pro-vided for the designation of in-house mentalhealth promoters. Public health nurses, nurses,health supervisors, health promoters, etc. aresupposed to take charge of this role. When
PRESENT STATE AND ISSUES OF WORKPLACE MENTAL HEALTH

174 JMAJ, May/June 2008 — Vol. 51, No. 3
outside resources are used, each enterpriseneeds to have a division and persons takingcharge of appropriate management of outsideresources. Please refer to my book5 for detaileddiscussion.
Problems of Mental Health Measures inWorkplaces
There are many problems, a few of which are dis-cussed below.
There are few mental health specialistsamong industrial health staff in enterprises.A lack of specialists with a certain level of knowl-edge and skills in mental health causes difficultyin promoting mental health measures and per-forming case management of workers with mentalhealth problems. The solution is either to employmental health specialists or to conduct appropri-ate education and training of existing industrialhealth staff.
Physicians used as outside resources lacksufficient knowledge and understanding ofindustrial health.The physicians should have a certain level ofknowledge and understanding of industrial health.In addition, it is ideal if they have a grasp of thepresent situation of the workplace of referredworkers, including industrial health systems andworkplace culture. In the background of thisproblem is the undesirable habit of enterprisesnot paying for physicians collaborating withenterprises. Expansion and enrichment of under-
graduates and continuing education in industrialhealth is needed.
Non-specialists are entering the market,seeking business opportunities in workplacemental health measures.Workplace mental health measures are aimed atprotecting the safety and health of workers, andeven their lives in the case of problems that maylead to suicide. Despite this fact, many unquali-fied firms are operating in this field, considering ita business. To improve this situation, physicianswith specialist knowledge and skills shouldwork with the managers and personnel officialsof companies to ensure that they have correctunderstanding of mental health, and shouldappropriately lead mental health activities inworkplaces.
Conclusion
A major cause of mental health problems amongworkers is the dramatic change in the environ-ment around them. This is a global problem, anda radical solution to this problem is extremelydifficult to find. Mental health problems tendto occur more frequently in workplaces whereinterpersonal relations are unsound or thin.Sufficient support in the workplace and at homehelps workers to cope with such problems. Themainstays of mental health measures are the con-trolling of overwork and the establishment of asupport system. It is also important to securehuman resources that play key roles in the pro-motion of mental health measures.
Shima S
References
1. Statistics and Information Department, Ministry of Health,Labour and Welfare. Worker Health Survey; 2002. (in Japanese)
2. Takano T, Shima S. Hatarakizakari no jisatsu yobou [Preventionof suicide in the prime of life]. Japanese Journal of Psycho-therapy. 2006;32:568–576. (in Japanese)
3. Industrial Health Division, Industrial Safety and Health Depart-ment, Labour Standards Bureau, Ministry of Health, Labour andWelfare. Guidelines for Promoting Mental Health Care in Enter-
prises; 2000. (in Japanese)4. Industrial Health Division, Industrial Safety and Health Depart-
ment, Labour Standards Bureau, Ministry of Health, Labour andWelfare. Guidelines for the Maintaining and Promoting Worker’sMental Health; 2006. (in Japanese)
5. Shima S. Guidelines for maintaining and promoting worker’smental health. Occupational Mental Health. 2006;14:172–175.(in Japanese)
175JMAJ, May/June 2008 — Vol. 51, No. 3
Research and Reviews
Japanese Encephalitis and Its Virus
Although the incidence of symptomatic Japaneseencephalitis is low, and there is no human-to-humantransmission, it is a severe disease that causesdeath in 17% of those affected and sequelae in48.5% of patients, according to the Japanesestatistics.3 The virus, which is amplified in pigs, istransmitted to humans by the mosquito Culextritaeniorhynchus. The positive conversion ratiofor the antibody is high every year, particularlyamong pigs in western Japan, reflecting a substan-tial presence of the virus in this country.2 Recentisolates include a new type I as well as the con-ventional type III.4,5 The recent marked decreasein the number of patients with this infectionseems to be largely attributable to the decreased
Introduction
In Japan, several thousand patients were affectedby Japanese encephalitis every year duringthe 1960s. However, since 1992, the number ofpatients per year has remained at fewer than 10(Fig. 1).1 The Japanese government discontinuedits aggressive recommendation of the currentJapanese encephalitis vaccine in May 2005, andabandoned the third stage of the routine vaccina-tion program in July of the same year.2 A newtissue-cultured inactivated vaccine, which wasexpected to appear soon, is not yet available.The current status and future prospects of vac-cination against Japanese encephalitis will bedescribed below.
*1 Director, Fukuoka-West Rehabilitation Center for Children, Fukuoka, Japan ([email protected]).This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.135, No.10, 2007pages 2179–2183).
Japanese Encephalitis Vaccine
JMAJ 51(3): 175–180, 2008
Chiaki MIYAZAKI*1
AbstractThroughout each year of the 1960s Japan had several thousand patients with Japanese encephalitis. In 1954,the national government began to take extensive measures aimed at susceptible individuals by administering aninactivated Japanese encephalitis vaccine. The number of patients decreased to less than 10 per year in and after1992. After 1990, the genotype of the prevalent strain changed from the previous type 3 to type 1. The decreasein the number of patients may be attributable not only to the efficacy of routine vaccination in children under theImmunization Law but also to the influences of changing lifestyle and environment. The rate of seroconversionfrom negative to positive results in pigs, the animal in which the virus is amplified, remains high every year. Thegovernment suspended its aggressive recommendation for Japanese encephalitis vaccination in May 2005, soonafter a 14-year-old patient with severe acute disseminated encephalomyelitis that was linked to a boosterinoculation of Japanese encephalitis vaccine was recognized as resulting from the vaccine. Over the subsequent3 years, the numbers of susceptible children have been accumulating. A new type of inactivated Japaneseencephalitis vaccine produced using a culture cell line (Vero cells) has been developed to replace the currentvaccine that is produced using the mouse brain, and a clinical trial of this vaccine is now underway. When thisvaccine is approved, the national government intends to resume its recommendation of the vaccination. The newvaccine is expected to be approved in 2009.
Key words Japanese encephalitis, Japanese encephalitis vaccine, Acute disseminated encephalomyelitis,Tissue-cultured vaccine

176 JMAJ, May/June 2008 — Vol. 51, No. 3
exposure to the virus resulting from social factors,including a decrease in the Culex tritaeniorhyn-chus population, a marked decrease in piggeries,and the spread of air conditioners, as well as theeffect of preventive vaccination.1
Withholding of AggressiveRecommendations for the CurrentJapanese Encephalitis Vaccine andthe Abolition of Third-stage Inoculation
The Japanese government issued a notice on May30, 2005, that its aggressive recommendation ofthe current Japanese encephalitis vaccine bewithheld, following the fact that the Ministryof Health, Labor and Welfare affirmed a causalrelationship between the Japanese encephalitisvaccine and severe cases of acute disseminatedencephalomyelitis (ADEM) occurring afterthird-stage (age of 14–15 years) inoculation ofthe vaccine. The government explained that itsdecision was made in consideration of the follow-ing factors. Japanese encephalitis currently occursin only a few persons of advanced age annually,shows hardly any incidence in children, and has
Miyazaki C
the attributes of personal immunity rather thanmass immunity. In all, 13 cases (including 4 severecases) of ADEM have been recognized as a resultof the vaccination since 1991, and the severity ofthese cases should be noted.
In addition, the government discontinuedthird-stage inoculation of Japanese encephalitisvaccination on July 29 of the same year. This actwas based on the fact that there were almost nopatients in the late teens despite the fact that thevaccination rate for the third stage was only 50%.Japanese encephalitis vaccines may be given tochildren as if requested at both the first stage(6 months to less than 90 months after birth) andthe second stage (9 years to less than 13 years)in the form of routine vaccinations if their guard-ians provide consent based on thorough informa-tion. However, currently, these vaccinations areseldom undertaken.
Efficacy and Adverse Effects ofthe Vaccine
The Japanese encephalitis vaccine currentlyavailable is produced by inactivation and purifi-
2,1002,0001,9001,8001,7001,6001,5001,4001,3001,2001,1001,000
900800700600500400300200100
0
(persons)19
6519
6619
6719
6819
6919
7019
7119
7219
7319
7419
7519
7619
7719
7819
7919
8019
8119
8219
8319
8419
8519
8619
8719
8819
8919
9019
9119
9219
9319
9419
9519
9619
9719
9819
9920
0020
0120
0220
0320
0420
05
100908070605040302010
0
(persons)
(year)
(year)
(year)
1972
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
14121086420
(persons)
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
Fig. 1 Reported number of patients with Japanese encephalitisFrom Infectious Diseases Weekly Report. The figure for 2005 is provisional.
(Cited from Taya K, et al. Pediatrics of Japan 2006;47:289–295)

177JMAJ, May/June 2008 — Vol. 51, No. 3
JAPANESE ENCEPHALITIS VACCINE
cation of the virus, using mouse brains infectedwith the virus (Beijing strain).5 This vaccineachieved an efficacy rate of 81–91% in large-scalefield trials carried out in Taiwan and Thailand. Ahistorical review of changes in the preventive
vaccination policy, the amount of vaccine sup-plied, and the incidence of patients by age alsodemonstrated the efficacy of the vaccine.6 Atleast three inoculations of the currently availablevaccine seem to allow the persistence of the neu-
0
1
2
3
4
5
6
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Days after inoculation
Rat
e of
occ
urre
nce
First dose in the first stage
(%)
(days)
Second dose in the first stage
Booster in the first stage
Second stage
Third stage
Fig. 2 Local reaction after inoculation of the Japanese encephalitis vaccine (fiscal 2003)
(Report of the results of a survey on health status after preventive vaccination,by the Ministry of Health, Labor and Welfare)
Table 1 Reported adverse reactions after Japanese encephalitis vaccination
Total Within 24h 1–3 days 4–7 days 8–14 days 15–28 days 29 daysor more
Total 825 611 153 26 17 14 4
1 Immediate systemic 252 224 26 1 1reaction
1A Anaphylaxis 122 119 3
1B Generalized urticaria 130 105 23 1 1
2 Encephalitis, 32 1 7 9 6 7 2encephalopathy
3 Convulsion 45 27 11 2 4 1
4 Motor dysfunction 3 1 2
5 Other neurological 25 14 3 5 2 1disorders
6 Abnormal local 12 10 2swelling
7 Generalized eruption 44 30 13 1
8 Fever of 39°C or 161 107 48 3 3more
9 Other abnormal 65 56 6 1 1 1reactions
10 Unrelated cases 186 141 37 5 1 2
[Ministry of Health, Labor and Welfare report of adverse reactions after vaccination (fiscal 1996–2004)]

178 JMAJ, May/June 2008 — Vol. 51, No. 3
tralizing antibody at a level 10-fold the protectiveantibody level.7
A common adverse effect is local reactions,whose incidence increases with increased num-bers of inoculations. The incidence of immediategeneral reactions decreases, and the incidence oflocal reactions decreases by half, by removing,reducing, or replacing the additives gelatin andthimerosal (Fig. 2).8
ADEM occurs relatively frequently in children.This condition is an acute, transient encephalitischaracterized by demyelination of the centralnervous system following viral or bacterial infec-tion or vaccination. Several surveys conducted bya Research Group of the Ministry of Health, Laborand Welfare9–12 revealed that ADEM in childrenoccurs at a mean age of 6–7 years, is slightly morefrequent in boys, shows no clear seasonality, andhas a relatively good vital prognosis. Patients withpost-infectious ADEM account for about 70% ofall patients. The annual incidence is 0.33–0.64 per100,000 children 15 years of age or younger, andthe total number of patients per year is estimatedat about 60–100.
Table 1 shows the reported cases of adversereactions to Japanese encephalitis vaccination(there might be erroneous inclusions because nodefinite causal relation was required) during the9-year period between fiscal 1996 and 2004.13
The 32 cases of encephalitis or encephalopathyare shown in the table. Based on the total numberof vaccinees, the incidence of reported ADEM isapproximately one per 2,600,000 inoculations, andthe incidence of a recognized health hazard is lessthan one per 4,000,000 inoculations (Table 2).Since there is a wide variation in the period from
inoculation to onset among individual cases, itis difficult to identify any causal relationship.According to an analysis of the relationshipbetween the number of vaccinees at each stageof vaccination and reported cases of encephalitisor encephalopathy, the risk of ADEM (includingerroneous cases) is likely to be high in children inthe third stage (Table 2).
Current Status of Tissue-culturedVaccine Development
When the national government halted aggressiverecommendation of the current Japanese encepha-litis vaccine, it stated that recommendation ofJapanese encephalitis vaccination was slated tobe resumed when the development of a presum-ably safer tissue-cultured vaccine became avail-able and its supply secure. The current vaccine ishighly purified, and is considered to have only atrace amount of myelin basic protein. Therefore,there is no definite evidence that the brain tissuecomponent is the cause of ADEM followingvaccination. However, the current vaccine is nec-essarily subject to theoretical concerns and dis-cussions of its responsibility for causing ADEMas long as infected mouse brains are used as thesource.
Much is expected from the development ofa tissue-cultured Japanese encephalitis vaccine,which would preclude contamination by unknownpathogens, protect the rights of animals, andsecure a steady supply.14 At present, two domes-tic companies are applying for approval of tissue-cultured inactivated vaccines produced usingVero cells. These vaccines achieve a favorable
Table 2 Incidence of ADEM after Japanese encephalitis vaccine
Stage of routine First stage Second stage Third stage Totalvaccination (age) (3–7) (9–12) (14–15)
No. of reported cases 1994–2006 14 1 6 21of ADEM (13 years) 1/3 million 1/10 million 1/1.2 million (1/2.6 million doses)
No. of recognized health 1989-2006 10 0 6 16hazard cases of ADEM (18 years) 1/5 million 1/1.8 million (1/4.8 million doses)
Annual No. of 2.8 million 0.8 million 0.6 million 4.2 million dosesinoculations
* No. of inoculation and incidence of ADEM are round numbers.(National Institute of Infectious Diseases. Infectious Disease Surveillance Center)
Miyazaki C

179JMAJ, May/June 2008 — Vol. 51, No. 3
increase in antibody titer, but can cause ratherfrequent local reactions, requiring additionalclinical trials. It seems that one or a few moreyears will be required before a tissue-culturedvaccine becomes commercially available.
Long-terms Effects of Discontinuationof Japanese Encephalitis Vaccination
To examine the long-term effects of discontinua-tion of the third stage of vaccination and sus-pended aggressive recommendation of the firstand second stages of vaccination, it is necessaryto observe the trend of the virus among pigsand transmitting mosquitos, the pathogenicityof wild strains of the virus, antibody prevalenceby locality and age group, occurrence of acuteencephalitis or meningitis of unknown etiology,and the overall trend of patient infection through-out Asia.
Since the infection rate is low (an annual infec-tion rate of 0.07% among young children, esti-mated from the results of preinoculation serumantibody test in participants in clinical trialsof tissue-cultured vaccines), a lack of Japaneseencephalitis vaccination may not cause an instant,sharp increase in pediatric patients. However, it iswell known that about one million susceptiblechildren accumulate each year. The risk of infec-tion should increase gradually among individualsof age groups characterized by increased outdooractivities during the evening hours in summerand autumn. As a result of these circumstances,the Japan Pediatric Society submitted a writteninquiry and demand to the Japanese governmentin July 2006, inquiring as to how the governmentplans to address these issues in the future (see thehome page of the Society: http://www.jpeds.or.jp/saisin-j.html). On August 31 of the same year,the Japanese government gave notice to localgovernments that they cannot refuse to provideroutine vaccination against Japanese encephalitisto children if their guardians request such vaccina-tion, even though the aggressive recommendationfor Japanese encephalitis vaccination remainssuspended. Readers are referred to a relateddocument, an explanatory leaflet about the Japa-nese encephalitis vaccine, because the Japanesegovernment’s view on Japanese encephalitis andADEM is expressed in the leaflet.
Since the advent of a new vaccine is beingdelayed, some doctors, particularly those in clini-cal practice in areas showing a high prevalence ofthe virus, have begun to recommend inoculationof the current vaccine again, going beyond theposition of the national government. There is nodoubt that attaining basic immunity lowers therisk of developing Japanese encephalitis. It ishoped that the Japanese government will takemeasures to relieve individuals who exceed thetarget age of routine vaccination during this periodof discontinuation of the aggressive recommen-dation. Vaccination against Japanese encephalitis(primary or booster inoculation) is desirablebefore traveling or residing overseas becausetens of thousands of individuals are affectedevery year in Southeast Asia, China, India, andother countries.1
Relation with West Nile Fever
The virus responsible for West Nile fever/encepha-litis, whose epidemics have been seen in the USsince 1999, belongs to the Flavivirus family,together with the Japanese encephalitis virus.These viruses are closely related to each otherfrom the antigenic aspect, and both are classifiedas belonging to the Japanese encephalitis sero-type group. The infection cycle of the West Nilevirus is maintained by birds and mosquitos. Culextritaeniorhynchus may be the major transmittingmosquito in Asian areas. It is possible that anepidemic of this infection could spread to Japanthrough birds flying here from Southeast Asia.Although the results of some animal experimentssuggest that the Japanese encephalitis vaccinehas a preventive effect against this infection, aWest Nile virus vaccine seems to be necessaryfrom a practical viewpoint.
Conclusion
There is an urgent need to collect scientific infor-mation about epidemics in Asian areas, includingJapan, to examine seroepidemiology, virus preva-lence among pigs and transmitting mosquitos,viral variation (genotype and pathogenicity), andthe efficacy and safety of a new vaccine. It will bedesirable to reconstruct vaccination strategiesbased on such information.
JAPANESE ENCEPHALITIS VACCINE

180 JMAJ, May/June 2008 — Vol. 51, No. 3
References
1. Taya K, Arai S, Sato H et al. Epidemiologic status of Japaneseencephalitis in Japan. Pediatrics of Japan. 2006;47:289–295. (inJapanese)
2. Miyazaki C. Present status of Japanese encephalitis vaccine inJapan. Pediatrics of Japan. 2006;47:311–318. (in Japanese)
3. Kimura M, Hirayama M, Sakai H. A Guide to Vaccination(10th ed.). Tokyo: Kindai Shuppan Co., Ltd.; 2005:244–264.(in Japanese)
4. Morita K. Epidemiologic status of Japanese encephalitis in Asia.Pediatrics of Japan. 2006;47:296–302. (in Japanese)
5. Infectious Disease Surveillance Center, National Institute ofInfectious Diseases: Japanese encephalitis 1999–2002. InfectiousAgents Surveillance Report. 2003;24:149–150. (in Japanese)
6. Miyazaki C. Efficacy of Japanese encephalitis vaccine. In: SakaiH ed. New “All about Vaccination.” Tokyo: Shindan To ChiryoshaCo., Ltd.; 1997:243–258. (in Japanese)
7. Okada K. Frequency of vaccination: diphtheria-pertussis-tetanusvaccine and Japanese encephalitis vaccine. Japanese Journalof Pediatrics. 2001;54:1599–1606. (in Japanese)
8. Tuberculosis and Infectious Diseases Control Division of theHealth Service Bureau, Ministry of Health, Labor and Welfare.Report of the Results of Survey on Health Status after PreventiveVaccination (fiscal 2003 and other years). (in Japanese)
9. Miyazaki C. Adverse reactions to preventive vaccination: acuteneurological diseases. Journal of Pediatric Practice. 2005;67:2056–2062. (in Japanese)
10. Torisu H, et al. Epidemiologic study of acute disseminatedencephalomyelitis and its related diseases in children. TheFiscal 2003 General and Segmented Reports of the Study onImmune-related Neurological Diseases [supported by the Healthand Labor Sciences Research Grant (study project for intrac-table diseases control)]. 2004;86–89. (in Japanese)
11. Miyazaki C, et al. Characteristic features of acute disseminatedencephalomyelitis (ADEM) found in the AND 7 study. The Fiscal2005 Report of the Study on Measures for Securing the Qualityof Vaccines to Achieve Enhanced Safety [supported by theHealth and Labor Sciences Research Grant (comprehensiveproject of drugs and medical devices regulatory science)]. 2006:215–219. (in Japanese)
12. Miyazaki C, et al. Epidemiologic study of acute disseminatedencephalomyelitis in children. The Fiscal 2005 General Report ofthe Study on Preventive Vaccination Required for Future Controlof Infectious Diseases Including Varicella, Mumps, and Pneumo-coccal Pneumonia [supported by the Health and Labor SciencesResearch Grant (emerging and reemerging infectious diseasesstudy project)]. 2006;129–132. (in Japanese)
13. Tuberculosis and Infectious Diseases Control Division of theHealth Service Bureau, Ministry of Health, Labor and Welfare.Report of Adverse Reactions after Preventive Vaccination (fiscal2004). 2005. (in Japanese)
14. Kurane I. Japanese encephalitis vaccine under development.Pediatrics of Japan. 2006;47:321–325. (in Japanese)
Miyazaki C

181JMAJ, May/June 2008 — Vol. 51, No. 3
Research and Reviews
In fact, many children in developing countriesare dying from infectious diseases that areseldom observed in industrialized countries.With the primary objective of saving as manyof these children’s lives as possible, WHO andthe United Nations Children’s Fund (UNICEF)are primarily supporting countries that find itfinancially difficult to promote vaccination. Aspart of this activity, the Expanded Programme onImmunization (EPI) was inaugurated by WHOin 1974.
EPI Vaccines
EPI initially designated six kinds of vaccines(diphtheria, pertussis, tetanus, polio, measles, andBCG) as those that should be given to childrenthroughout the world, and activities that dissemi-nated and assisted inoculations were facilitated.Aware of the importance of disease prevention,WHO urged in 1992 that the routine use of hepa-titis B vaccine be introduced to every nation inthe world by 1997. WHO also recommended in1998 that the Haemophilus influenza type b (Hib)
Vaccination and the World HealthOrganization (WHO)
Vaccination is the most powerful means of pre-venting infectious diseases. Although the era ofinfectious diseases was once thought to be over,no one currently believes that this is true. Inrecent memory, potential threats of bioterrorismwith smallpox virus have been made, and the pro-duction of smallpox vaccine has been resumedto create an adequate stockpile.
Most vaccinations have the attributes of bothpersonal and herd immunity. Vaccination is notonly a welfare project for children but also anissue of national security. Because of this back-ground, the system of vaccination is peculiar toeach country.
Vaccination is often implemented as a nationalproject. In developing countries, where the nationalbudget is relatively limited, there may be restric-tions on vaccination. However, an inadequatevaccination system may become a substantialobstacle to the maintenance of children’s health.
*1 Associate Professor, Department of Pediatrics, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan([email protected]).This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.135, No.10, 2007,pages 2163–2166).
Current Status of Vaccination in Japan andthe World: A pediatrician’s point of view
JMAJ 51(3): 181–185, 2008
Hiroshi WATANABE*1
AbstractThis paper discusses the variety of currently available routine vaccinations in Japan in comparison with those ofother countries. According to materials from the World Health Organization, routine vaccines commonly availablein developing countries include BCG, live polio, DPT, and measles vaccines. Vaccination in Japan is similar,except that a combined measles and rubella vaccine is used instead of the measles vaccine. In some developingcountries, hepatitis B vaccine and Haemophilus influenza type b vaccine are already in routine use. To reach thelevel of other industrialized countries, routine vaccination in Japan should include these two vaccines as well asinactivated poliovirus, MMR, pneumococcus, influenza, and varicella vaccines.
Key words Vaccination, Children, Newly introduced vaccine, EPI

182 JMAJ, May/June 2008 — Vol. 51, No. 3
vaccine, which has a potent preventive effect, beintroduced as a routine vaccination whenevereconomically feasible.
Vaccination in Developing Countries
The State of the World’s Vaccines and Immuniza-
Watanabe H
tion1 issued by WHO in 2003 has an annex thatpresents a typical routine vaccination schedulefor infants in developing countries (Table 1). Anote to the table states that developing countriesin Africa, where yellow fever epidemics occur,are assumed in the table.
Table 1 shows that all initially designated EPI
Table 2 A national immunization schedule for infants in industrial countries
VaccineAge
Birth 1 month 2 months 3 months 4 months 5 months 6 months �1 year*5
BCG*6 � �
Hepatitis B �*1 � � �
DTP � � �
Hib � � �
Polio OPV/IPV OPV/IPV OPV/IPV OPV IPV
Measles, MMR �
Pneumococcal � � �
Other vaccines*2
- Influenza*3 �
- Varicella �
- Hepatitis A*4 variable
*1 Given with HBIG if mother is HBsAg-positive.*2 Only used by some countries, and frequently only for selected populations.*3 Generally only given from 6 months of age to high risk selected infants annually.*4 Generally only given to high risk selected infants in the first year of life.*5 Variable additional doses of these vaccines are scheduled as boosters during the next two decades.*6 BCG is administered in certain industrialized countries, but to widely differing ages and in varying numbers of doses.
[Cited from WHO: State of World’s Vaccines and Immunization. 2003;88–89 (Annex 3)]
Table 1 A national immunization schedule for infants in developing countries
VaccineAge
Birth 6 weeks 10 weeks 14 weeks 9 months
BCG �
Oral polio �* � � �
DPT � � �
Hepatitis B† � � �
Haemophilus influenzae type B† � � �
Yellow fever �**
Measles �***
* In epidemic countries.** In countries where yellow fever poses a risk.
*** In addition, a second opportunity to receive a dose of measles vaccine should be provided for all children.This may be done either as part of the routine schedule or in a campaign.
† Only a few African countries have been able to introduce the vaccines to date.[Reproduced from WHO: State of the World’s Vaccines and Immunization. 2003;88–89 (Annex 3)]

183JMAJ, May/June 2008 — Vol. 51, No. 3
CURRENT STATUS OF VACCINATION IN JAPAN AND THE WORLD
vaccines (BCG, polio, DPT, and measles) arecovered. The recommended age of infants atimmunization is generally low, probably to reflectthe existing situation in which the risk of mor-bidity is substantial. This also should be truefor measles vaccine, for which the recommendedage is 9 months. Hepatitis B vaccine and Hib vac-cine are also included for the aforementionedreason. Yellow fever vaccine is included becausecountries that have epidemic Yellow fever areassumed for this table.
In actuality, many African nations provide vac-cination according to an immunization schedulesimilar to that of this table.2 Since many Africannations provide vaccination under the support ofWHO and other organizations, it seems that theyhave reasonably similar vaccination programsthat are in accordance with the recommendationsof WHO rather than having individual vaccina-tion programs.
Vaccination in Industrialized Countries
Table 2 shows a typical routine vaccinationschedule for infants in industrialized countries,which is also given in the annex to the State of theWorld’s Vaccines and Immunization.1 All EPIvaccines, i.e., BCG, polio, DPT, measles, hepatitisB, and Hib vaccines, are included.
When compared with Table 1, one can noticethat the recommended ages of infants at immu-nization with DPT, polio, and Hib vaccines areslightly higher than those in developing countries.This is probably because the schedule reflects adifferent situation of epidemics of these infections.
The use of inactivated polio vaccine, ratherthan live vaccine, also represents a major differ-ence from Table 1. This is a policy parallelingthe currently continuing eradication program of
polio. According to 2005 WHO data, 38 nations inthe world were using inactivated polio vaccine.
Measles vaccine is recommended for 1-year-old or older infants, because major emphasis isplaced on improvement of the efficacy rate ofthe vaccine rather than prevention of infectionbefore 1 year old. Another major difference fromdeveloping countries is that the use of MMR(measles, mumps, rubella) vaccine instead ofmeasles vaccine is predominant among industri-alized countries.
In addition to these WHO-recommended vac-cines, pneumococcus vaccine, influenza vaccine,varicella vaccine, and hepatitis A vaccine (vari-able) are listed in Table 2. Although the use ofhepatitis A vaccine is not universal because of thevarying situation of epidemics among differentcountries, other vaccines are commonly regardedas routine vaccines for children in industrializedcountries. Incidentally, the pneumococcus vaccinereferred to here is a protein-conjugated polysac-charide vaccine of the next generation, unlike theone currently used in Japan. The other three vac-cines have already been approved for voluntaryvaccination in Japan.
Vaccination in Japan
The current routine vaccination schedule (as of2006) for infants in Japan is shown in Table 3,in the same format as Tables 1 and 2. There aredistinct differences between the Japanese vacci-nation schedule and the typical routine vaccina-tion schedule for an industrialized country shownin Table 2. Comparison with the typical routinevaccination schedule for a developing countryshown in Table 1 shows little difference apartfrom Japanese encephalitis vaccine and yellowfever vaccine.
Table 3 National immunization schedule for infants in Japan
VaccineAge
Birth 3 months 6 months 9 months �1 year
BCG �
Oral polio (twice)
DPT (3 times) �
Japanese encephalitis (4 times)
MR �
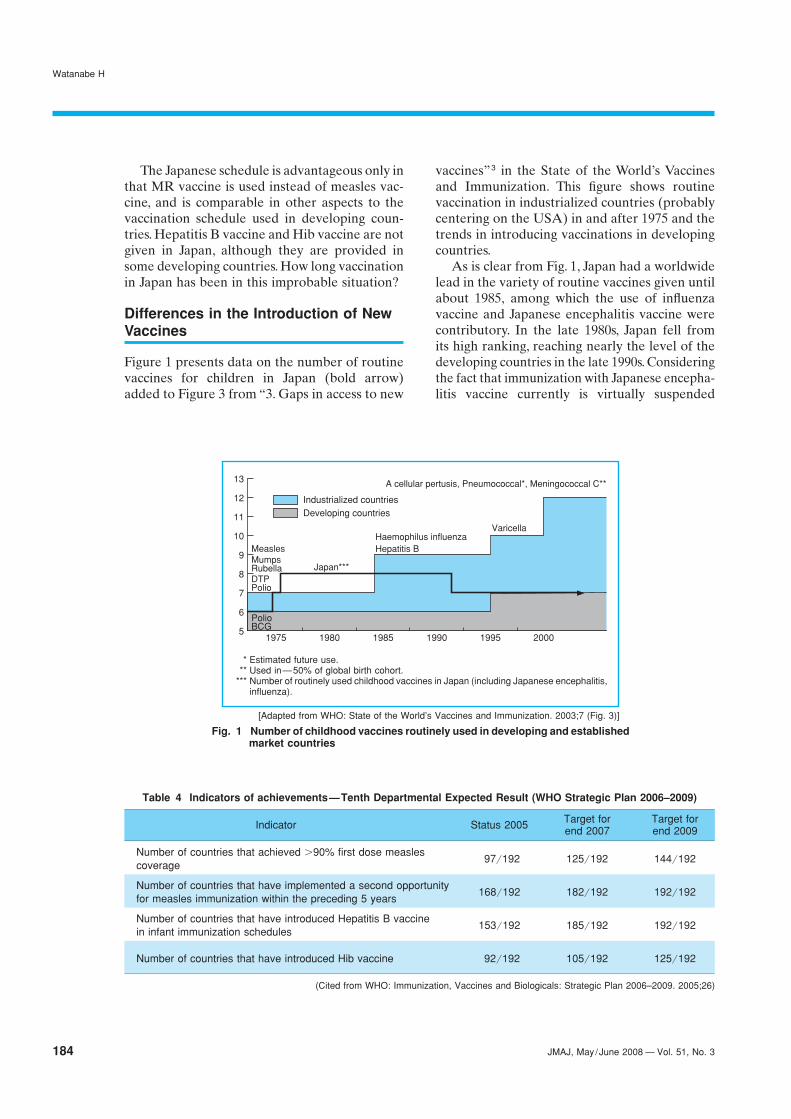
184 JMAJ, May/June 2008 — Vol. 51, No. 3
Watanabe H
The Japanese schedule is advantageous only inthat MR vaccine is used instead of measles vac-cine, and is comparable in other aspects to thevaccination schedule used in developing coun-tries. Hepatitis B vaccine and Hib vaccine are notgiven in Japan, although they are provided insome developing countries. How long vaccinationin Japan has been in this improbable situation?
Differences in the Introduction of NewVaccines
Figure 1 presents data on the number of routinevaccines for children in Japan (bold arrow)added to Figure 3 from “3. Gaps in access to new
vaccines”3 in the State of the World’s Vaccinesand Immunization. This figure shows routinevaccination in industrialized countries (probablycentering on the USA) in and after 1975 and thetrends in introducing vaccinations in developingcountries.
As is clear from Fig. 1, Japan had a worldwidelead in the variety of routine vaccines given untilabout 1985, among which the use of influenzavaccine and Japanese encephalitis vaccine werecontributory. In the late 1980s, Japan fell fromits high ranking, reaching nearly the level of thedeveloping countries in the late 1990s. Consideringthe fact that immunization with Japanese encepha-litis vaccine currently is virtually suspended
Table 4 Indicators of achievements—Tenth Departmental Expected Result (WHO Strategic Plan 2006–2009)
Indicator Status 2005 Target for Target forend 2007 end 2009
Number of countries that achieved �90% first dose measles97/192 125/192 144/192
coverage
Number of countries that have implemented a second opportunity168/192 182/192 192/192
for measles immunization within the preceding 5 years
Number of countries that have introduced Hepatitis B vaccine153/192 185/192 192/192
in infant immunization schedules
Number of countries that have introduced Hib vaccine 92/192 105/192 125/192
(Cited from WHO: Immunization, Vaccines and Biologicals: Strategic Plan 2006–2009. 2005;26)
Fig. 1 Number of childhood vaccines routinely used in developing and establishedmarket countries
Industrialized countriesDeveloping countries
Varicella
MeaslesHaemophilus influenzaHepatitis B
MumpsRubellaDTPPolio
Japan***
13
8
9
10
11
7
5
12
1995
6
20001980 19901975 1985
PolioBCG
A cellular pertusis, Pneumococcal*, Meningococcal C**
[Adapted from WHO: State of the World’s Vaccines and Immunization. 2003;7 (Fig. 3)]
* Estimated future use.** Used in—50% of global birth cohort.
*** Number of routinely used childhood vaccines in Japan (including Japanese encephalitis,influenza).

185JMAJ, May/June 2008 — Vol. 51, No. 3
CURRENT STATUS OF VACCINATION IN JAPAN AND THE WORLD
because of associated adverse effects, the linein the figure representing the use of vaccines inJapan in and after 2005 may well be even lower.
Future Vaccination in Japan
Finally, Table 4 introduces goals for improvingthe implementation rate of routine vaccinationextracted from Table 104 in “Immunization, Vac-cines and Biologicals: Strategic Plan 2006–2009”issued by WHO in 2005. Presumably, Japan hasachieved the first goal of a measles vaccinationrate �90%. Another goal, implementation of thetwo-vaccinations strategy for measles vaccinewas achieved as late as June 2006, behind mostother countries in the world. The existing situa-tion is that the goals for hepatitis B vaccine andHib vaccine are unlikely to be achieved by 2009.
Thus, the vaccination system for children inJapan has lagged far behind the rest of the worldduring the past two decades. There are, of course,other countries that lag behind in vaccination,but the reason is usually economic. At present,financial difficulties, if any, can be solved to someextent with support from UNICEF or other aidorganizations. In actuality, a number of develop-ing countries have a more advanced system ofvaccination than Japan. The vaccination systemin Japan is less advanced probably for reasonsother than economic ones, and therefore the issueappears complicated and difficult to solve.
It would be desirable for the sake of Japan’schildren that the routine vaccination system ofthe country reach the level of other industrializedcountries in the world as soon as possible.
References
1. World Health Organization. State of the World’s Vaccines andImmunization; 2003:88–89.
2. The United Nations Children’s Fund. Immunization Summary2006. United Nations Publications; 2006.
3. World Health Organization. State of the World’s Vaccines and
Immunization; 2003:7.4. World Health Organization. Immunization, Vaccines and Biologi-
cals: Strategic Plan 2006–2009; 2005:26 (http://www.who.int/immunization/aboutus/842.pdf).

186 JMAJ, May/June 2008 — Vol. 51, No. 3
Research and Reviews
History of the Preventive VaccinationProgram
The Preventive Vaccination Law was promul-gated in Japan in 1948. The initial vaccinationinitiative was compulsory, and failure to complycarried penalties because halting the spread ofinfectious diseases was strongly needed at thattime, when a large number of infectious caseswere occurring.
Later, as the number of patients with infec-tious diseases decreased, health hazards causedby preventive vaccination became a social prob-lem following various accidents in smallpox vac-cination in the latter half of the 1960s. Therefore,a system was legislated to relieve injury to healthcaused by vaccination, and the penalty for failure
Introduction
It has been approximately half a century sincethe introduction of the current program of pre-ventive vaccination, which has become a principalpillar of infection control. During this period, vac-cination has contributed greatly to the decreasedoccurrence of infectious diseases in Japan. On theother hand, the preventive vaccination programhas resulted in increased awareness of humanrights and issues regarding adverse reactions.This paper introduces changes in the preventivevaccination program to date, addresses recenttopics in the field, and discusses government-sponsored actions regarding preventive vaccina-tion in Japan.
*1 Professor, Center for Community Medicine, Jichi Medical University, Tochigi, Japan ([email protected]).This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.135, No.10, 2007,pages 2159–2162).
Perspective on Current Vaccination Policyin Japan
JMAJ 51(3): 186–190, 2008
Taro TSUKAHARA*1
AbstractIt has been approximately half a century since the current preventive vaccination program was set up in Japan.Initially, this program covered smallpox, typhoid, paratyphoid, diphtheria, pertussis, and some others. Since then,the diseases targeted by the vaccination program have been altered according to changes in patient infection andtechnological development, and have contributed substantially to a progressive decline in the incidence ofinfectious diseases. On the other hand, a relief system for adverse effects of vaccination was legislated as a resultof increased awareness of human rights and issues pertaining to adverse reactions, with the result that receivingvaccinations was changed from a compulsory obligation to an individual decision, representing a great changein the preventive vaccination program in Japan.
Under these circumstances, a two-dose schedule of vaccination with a measles-rubella combination vaccinewas introduced in April 2006. It is expected that this vaccination schedule will help enhance mass immunityagainst the two diseases, creating a giant step toward the goal of eliminating measles by 2012. It would bedesirable to further promote governmental action in the area of preventive vaccination in response to the actualstatus of infectious diseases, including the introduction of inactivated polio vaccine and the promotion of its usein the form of a combination vaccine, defining policies for the use of combination vaccines in patients infected withat least one of the target diseases of the combination vaccine, and developing a pandemic influenza vaccine.
Key words Infectious disease, Laws, Preventive vaccination, Measles-rubella combination vaccine

187JMAJ, May/June 2008 — Vol. 51, No. 3
to be vaccinated was abandoned except in casesof emergency.
In addition, while the number of patients withinfectious diseases was decreasing markedly, ajudicial ruling was handed down in regard tocollective lawsuits concerning adverse reactionsto vaccination, and the Preventive VaccinationLaw was amended in 1994 to make vaccination amatter of individual choice, thereby respectingthe decision of the person or guardian as towhether or not to be vaccinated (each person isobliged to make an effort to be vaccinated).
The target diseases initially covered by thePreventive Vaccination Law included smallpox,typhoid, paratyphoid, diphtheria, and pertussis.Subsequently, the target diseases were alteredaccording to the current status of infections thatwere prevalent and the development of vaccinetechnologies. The transition of the target diseasesfrom the initiation of the vaccination programto the present day is shown in Fig. 1. The targetdiseases as of April 1, 2006, were diphtheria, per-tussis, acute anterior poliomyelitis (polio), measles,rubella, Japanese encephalitis, and tetanus—allClass 1 diseases—and influenza, a Class 2 disease,specified by amendment of the Law in 2001. Vac-cination of Class 2 diseases is left up to individual
decision, with no obligation imposed.
Revision of the Measles and RubellaVaccination Program
Introduction of the two-dose measles-rubellacombination vaccineTwo-dose vaccination with a dried, attenuatedlive measles-rubella combination vaccine (MRvaccine) was introduced on April 1, 2006, to pre-vent measles and rubella. The major revisionswere as follows: 1) the period of vaccination, 12months or more and less than 90 months afterbirth, was divided into a period of 12 months ormore and less than 24 months after birth (firststage) and a period of one year before entranceinto elementary school (second stage); and 2) thevaccines in use were changed from mono-antigenvaccines to MR vaccines.
The two-dose schedule was introduced toachieve enhanced immunity by the second dosein vaccine recipients who failed to acquire immu-nity after the first dose (primary vaccine failure)or those in whom the immunity acquired withthe first dose decreased afterward (secondaryvaccine failure). This revision was meant to pro-duce strong mass immunity in individuals who
Fig. 1 Target diseases of the Preventive Vaccination Law
1940 1950 1960 1970 1980 1990 2000 (year)
Routine vaccination General vaccination as needed
Smallpox (1948–) *Vaccination is limited to cases of emergency in 1976–2002.
Diphtheria/pertussis (1948–)
Typhoid/paratyphoid
Routine vaccination (1948–1970)
Vaccination as needed (1976–1994)
(1970–1976)
Tuberculosis (1948–) *Shifted to the Tuberculosis Prevention Law
Acute anterior poliomyelitis (polio) (1961–)
Measles/rubella (1976–)
(2001–)Influenza (1948–1994)
Weil’s disease (1948–1994)
Typhus/cholera/plague
(1994–)
(1948–1976)
Scarlet fever (1948–1958)
Japanese encephalitis
Tetanus (1994–)
PERSPECTIVE ON CURRENT VACCINATION POLICY IN JAPAN
188 JMAJ, May/June 2008 — Vol. 51, No. 3
experienced the first stage of vaccination underthe new vaccination program.
In determining the vaccines to be used, MRvaccines alone were adopted for the convenienceof vaccinees, resulting in an improved rate ofvaccination, and lowering the risk of adversereactions. This enabled us to expect that theparticularly low rubella vaccination rate wouldincrease to the level of the measles vaccinationrate.
Interval until implementation of the MRvaccinationRevision of the MR vaccination program resultedin individuals who previously were covered bythe former vaccination program but not by thenew program. Specifically, those who were ineli-gible included the following: 1) children 24 monthsold or older who were more than a year awayfrom entrance into elementary school, 2) chil-dren who were attending an elementary school atthe beginning of the new program, 3) those whowere given only one of the two vaccines underthe former vaccination program, and 4) thosewith a history of one of the two diseases.
These individuals were strongly encouraged toreceive the relevant vaccination by April 2006,when the new program was to start. As a transi-tional measure, local governments were asked toapply the same vaccination fee as that of the legalMR vaccination to ineligible 1-year-old childrenwhen they failed to receive relevant vaccinationby March 31, 2006, and requested MR vaccina-tion after April 1.
Initiation of the second dose of MR vaccineand addition of the mono-antigen vaccineThe decision to introduce the two-dose scheduleof MR vaccination from April 2006 was made inJuly 2005. At that time, vaccination of the seconddose was to be initiated after corroborative dataon the efficacy and safety of the vaccine amongJapanese people had been obtained. Therefore,when the new program began in April 2006, indi-viduals eligible for routine MR vaccination werelimited to 1) infants between 12 and 24 monthsafter birth and 2) children who would enterelementary school within 1 year and had notreceived inoculation of either rubella or measlesmono-antigen vaccine.
Collection of corroborative data on the effi-cacy and safety of the two-dose schedule of MR
vaccination was begun by a Research Group ofthe Ministry of Health, Labor and Welfare in theAutumn of 2005, and it was determined thatthe efficacy in terms of the serum antibody titerafter the second dose and safety in terms of theincidence of adverse reactions such as fever anderuptions following vaccination were compa-rable to those of the conventional mono-antigenvaccines.
Therefore, the government ordinance in regardto vaccination was revised again on May 30, 2006,1) to allow children in the second stage who hada history of vaccination under the former vacci-nation program to be covered by the second doseof MR vaccine, and 2) to add mono-antigen vac-cines as legally assigned vaccines.
These two actions are expected to promote theacquisition of stronger mass immunity againstthe two diseases and are expected to eliminatemeasles by 2012, the goal set forth by Japan andother countries in the WHO Western PacificRegion.
Revision of the Japanese EncephalitisVaccination Program and Discontinuationof This Vaccination
Abolition of the third stage of Japaneseencephalitis vaccinationIn July 2005, the third stage (given at age 14–15)of Japanese encephalitis vaccination was discon-tinued. The number of patients with Japaneseencephalitis has decreased greatly in Japan. Thereported number of patients in the late teens wasonly one in the past 22 years, although the vacci-nation rate for the third stage is only about 50%.On the other hand, more than 100 cases of adversereactions were recognized as having been causedby Japanese encephalitis vaccination betweenfiscal 1989 and 2004. For these reasons, the thirdstage of the Japanese encephalitis vaccinationwas discontinued.
Eliminating aggressive recommendationsfor Japanese encephalitis vaccinationIn May 2005, the Minister of Health, Labor andWelfare recognized that acute disseminatedencephalomyelitis (ADEM) following Japaneseencephalitis vaccination was caused by the vac-cine, based on the fact that opinions regardingthe causal relationship between Japanese encepha-litis vaccine and severe ADEM were expressed at
Tsukahara T

189JMAJ, May/June 2008 — Vol. 51, No. 3
the Diseases and Disorders Recognition ReviewBoard of the Ministry of Health, Labor and Wel-fare. As a result, aggressive promotion of routineJapanese encephalitis vaccination was withheld.
However, Japanese encephalitis vaccines maybe given to individuals who strongly wish to receivethem after such individuals provide consent basedon thorough information regarding its efficacyand adverse effects. If a health hazard occursafter inoculation of the Japanese encephalitisvaccine, and a causal relationship is recognizedby the Minister of Health, Labor and Welfare, thecase is covered by the health hazard relief systemunder the Preventive Vaccination Law, in thesame manner as previously.
A new type of Japanese encephalitis vaccineproduced by the tissue culture method, which hasa lower risk of ADEM occurrence, is now underdevelopment. When this vaccine is approved andits supply is secured, a conclusion may be drawnas to the policy of vaccination against Japaneseencephalitis. Until then, inoculation of the vac-cine to individuals who request vaccination willbe continued while withholding aggressive rec-ommendations. A notice of such intention hasrecently been sent to local governments.
Future Perspectives
Introduction of inactivated polio vaccineand promotion of the combination vaccineSince there is some indication of a worldwideresurgence of poliomyelitis, the continuation ofpolio vaccination is considered necessary inJapan at this time. Currently, oral live polio vac-cine is used. Although the problem is rare, thisvaccine has been associated with the occurrenceof vaccine-related polio paralysis in vaccinees ortheir families. Therefore, it is necessary to replacethis live vaccine with an inactivated vaccine.
In order to adopt the inactivated polio vaccine,the use of a 4-component combination vaccineagainst diphtheria, pertussis, tetanus (DPT) andpolio is under consideration for the convenienceof vaccinees, resulting in an improved rate ofvaccination, and lowering the risk of adversereactions.
Use of the combination vaccine in affectedpersonsUnder the current program of vaccination pre-scribed by the Preventive Vaccination Law,
persons already affected by a target disease areexcluded from subjects eligible for vaccinationagainst the disease in question, in accordancewith the provisions of Article 1-2 of the govern-ment ordinance. This is based on the followinglegal and medical reasons: it is not appropriateto recommend vaccination that carries a risk ofadverse reactions as an obligation of persons whoalready have some immunity against the disease.
However, with the promotion of combinationvaccines, such as DPT and MR vaccines, it some-times happens under this provision that individu-als affected by at least one of the combineddiseases are excluded from coverage of vaccina-tion with the combination vaccine. At the timethe MR vaccine was introduced, this issue wassolved by temporarily adding mono-antigen vac-cines. A similar issue exists for the DPT vaccine.Therefore, to promote the use of combinationvaccines in the future, it is hoped that this govern-ment ordinance be revised to allow the use ofcombination vaccines in persons who have beenaffected by at least one of the combined diseases.Currently, the Research Group of the Ministry ofHealth, Labor and Welfare is proceeding withthe collection of corroborative data.
Revision of the target diseases ofthe Preventive Vaccination LawIn 2006, the national government lost severallawsuits related to vaccination, such as themeasles-mumps-rubella vaccine (3-componentcombination vaccine) government liability case(April, Tokyo High Court) and the mass vacci-nation-related hepatitis B government liabilitycase (June, Supreme Court). These adjudicationsestablished that obligatory preventive vaccina-tion implemented by the government in healthyindividuals (whether compulsory or by choice)requires greater safety than general medicaltreatments given to patients, and that burdenof proof concerning safety is imposed on thenational government, but not on the claimant,thereby changing the burden of proof.
Therefore, considering that the rationale ofthe government’s recommendation of preventivevaccination for healthy individuals despite therisk of adverse reactions is a social defense toprevent the spread of infections, the target dis-eases of the Preventive Vaccination Law shouldbe determined after due consideration of thecontagiousness and seriousness of the infectious
PERSPECTIVE ON CURRENT VACCINATION POLICY IN JAPAN

190 JMAJ, May/June 2008 — Vol. 51, No. 3
disease as well as the efficacy and safety of thevaccine. Among the target diseases of the currentVaccination Law, the designation of tetanus as aClass 1 disease that obligates individuals to makean effort to be vaccinated needs to be reviewedbecause tetanus is not transmitted between humanbeings. In addition, in regard to Hib vaccine andpneumococcal vaccine, whose coverage by theVaccination Law is highly desirable, thoroughand careful consideration of the contagiousnessand seriousness of the diseases as well as confir-mation of the efficacy and safety of the vaccinesis required.
Pandemic influenza vaccineEpidemics of prepandemic influenza (type A,subtype H5N1) were initially restricted to South-east Asia, but in 2006 patients with this infectionwere found in both Europe and Africa. Thus, thedevelopment of a vaccine to halt the occurrenceof pandemic influenza is urgently needed. A clini-cal study of a vaccine developed using a viralstrain (H5N1) isolated in Viet Nam was begun inJanuary 2006. This vaccine is intended to be givento those critical to maintaining social functioningsuch as healthcare workers, according to the Pan-demic Influenza Preparedness Action Plan of theJapanese Government. At present, the selectionof eligible vaccinees and the method of vaccina-
tion are under consideration. If this vaccine isapproved, it is expected to shorten the develop-ment and approval period for a pandemic influ-enza vaccine that can be made available for theentire nation in the event of an influenza epidemic.
Conclusion
There is no question as to the efficacy of preventivevaccination for the control of infectious diseases.In particular, it is necessary for people to achievestrong mass immunity when serious infectiousdiseases with strong human-to-human infectivityoccur. Thus, expectations for governmental actionin the area of preventive vaccination will con-tinue to be high.
However, the implementation of all vaccina-tions under the Preventive Vaccination Law haslimitations, given the increasing emphasis on self-reliance and the fact that judicial judgments onvaccination-related health hazards are availableto the public.
It would be desirable for governmental actionsin the arena of preventive vaccination to be madeon the basis of an understanding of the featuresof infectious diseases, including the promotion ofresearch on and development of vaccines and thepromotion of information on infectious diseasesand vaccines among the population.
Tsukahara T

191JMAJ, May/June 2008 — Vol. 51, No. 3
Research and Reviews
Their hopes were not completely in vain, how-ever. The notification released by Ministry ofHealth, Labour, and Welfare (MHLW) in Junethe same year removed many such limitations,and the 2-dose measles and rubella immuniza-tion virtually started in Japan.
Why Measles and Rubella ImmunizationRequires a 2-dose Schedule
Measles and the measles vaccineMeasles is an extremely infectious disease andhas the potential to cause very severe symptoms.When complicated with pneumonia or encepha-litis, it often leads to death. The fatality rate isabout 0.1% in developed countries and rangesfrom several to 30% in developing countries. The
Introduction of MR Vaccine and 2-doseSchedule for Measles and RubellaVaccination
From April 2006, the partial amendment of thePreventive Vaccination Law introduced a 2-doseschedule for measles and rubella vaccinationsand the use of a combined measles and rubellavaccine (MR vaccine) for this purpose, which hadbeen long awaited by many pediatricians andpublic health professionals in Japan. However, tothe disappointment of those who had been work-ing energetically towards measles and rubellacontrol, this amendment was not effective in fullydelivering its intended purposes due to variouslegal limitations and interpretation problems.
*1 Director, Infectious Disease Surveillance Center, National Institute of Infectious Diseases, Tokyo, Japan ([email protected]).This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.135, No.10, 2007,pages 2173–2177).
Combined Measles and Rubella (MR) VaccineIntroduced in Japan
JMAJ 51(3): 191–196, 2008
Nobuhiko OKABE*1
AbstractThe number of patients with measles in Japan decreased dramatically after the introduction of the measlesvaccine, but the epidemic in 2001 mainly affecting infants increased the estimated total number of patients to170,000–330,000. In response, measles vaccination in 1-year-old infants was encouraged, and the total numberof patients was believed to have fallen generally below 10,000 in 2005 and 2006. Later, the combined measles-rubella vaccine (MR vaccine) was introduced to Japan on April, 2006 and the 2-dose regimen using this vaccineat age 1 (first dose) and within 1 year before entry to elementary school (second dose) started in June 2006,providing an effective means to control measles and rubella in the routine vaccination program. This articlediscusses the background to the introduction of the 2-dose MR vaccination and its significance in Japan.
After the writing of this article, an epidemic of measles occurred mainly affecting young people in 2007.Triggered by this experience, the schedule for measles and rubella routine vaccination in Japan was revised toinclude supplementary vaccination at ages corresponding to the first year of junior high school and the third yearof high school, to be implemented for 5 years from April 1, 2008. With the reinforcement of the first and secondvaccination and the introduction of the supplementary vaccination, Japan has taken a step forward to therealization of measles elimination, which the WHO Regional Office for the Western Pacific (WPRO) aims to attainby 2012, and congenital rubella syndrome elimination as well.
Key words Measles, Rubella, Vaccine, MR vaccine
192 JMAJ, May/June 2008 — Vol. 51, No. 3
World Health Organization (WHO) estimatesthat 530,000 persons worldwide died of measlesin just the year of 2003 alone. Even non-fatalcases frequently see complications such as pneu-monia, otitis media, and encephalitis develop andabout 1/3 of patients with measles develop someform of complications. The measles vaccine is avital tool to prevent measles, which is a seriousdisease.
Prior to the introduction of the measles vac-cine in 1960s, virtually all children contractedmeasles and many lives were lost. With the wide-spread use of vaccines with improved efficacyand safety, a 95% decrease in the number ofdeaths was achieved by 2003. The goal of globalmeasles control was originally a decrease in thenumber of patients and reduction in mortality.Later, efforts towards regional measles elimina-tion started, targeting the complete eliminationof infection transmission.
Rubella and the rubella vaccineIn contrast, rubella is a disease with basicallygood prognosis. Although complications such asthrombocytopenic purpura and acute encepha-litis develop quite often in cases, the prognosis ofsuch cases is generally good. The most importantproblem associated with rubella is that of con-genital rubella syndrome (CRS), which occurs ata high rate when the primary infection takes placein pregnant women during the early stages ofgestation. This may cause a fetal infection, result-ing in various symptoms, including birth defects.
The birth defects caused by CRS include con-genital heart disease, hearing loss, cataracts, andretinopathy, which may occur in combination oras a single symptom such as hearing loss or visualimpairment, which may be difficult to diagnose.Aside from congenital defects, symptoms that mayoccur in the neonatal period include low birthweight, thrombocytopenic purpura, hemolyticanemia, interstitial pneumonia, and meningo-encephalitis. CRS may also cause conditionssuch as progressive rubella panencephalitis anddiabetes mellitus, both during and after infancy.
There is no virus-specific treatment for CRS.As a means of individual protection, it is importantthat women receive vaccines to acquire immunityagainst rubella before getting pregnant. At thelevel of social protection, the vaccination rateshould be kept in high level to prevent a rubellaepidemic and minimize the exposure of preg-
Okabe N
nant women to the rubella virus. It has beenreported that artificial abortion increases duringan epidemic of rubella, reflecting the fear of thepossibility of CRS in babies, previously in Japan.
Current coverage of measles and rubellavaccination and the effectiveness inpreventionMeasles vaccine is recognized as a vaccine thatis necessary for all children in the world (oneof the Expanded Programme on Immunization[EPI] vaccines) and has been introduced in mostcountries. On the other hand, the introductionof the rubella vaccine depends considerably onthe economic circumstances of each country.While it is used in 92% of advanced industrial-ized countries (developed countries), as classifiedby the United Nations, it is used in only 36% ofcountries with medium economic developmentand 28% of developing countries.
Both the measles and rubella vaccines arelive, and are reported to have at least more than95% preventive effects. However, the vaccina-tion proves ineffective in about less than 5% ofpeople (named as primary vaccine failure), whoremain susceptible to infection and accumulatein the population. It was once believed thatpeople who received live vaccines and achievedan immune reaction would retain the serum anti-bodies and cellular immunity for life, becausethey would acquire immunity very close to thatresulting from natural infection. However, ithas become clear that a person having acquiredimmunity may experience gradual waning ofimmunity after a long absence of antigen stimuli(the stimulation from natural infection ceaseswhen the disease is controlled to a certain extent),particularly in the case of measles (named assecondary vaccine failure).
When immunity has waned, the disease maymake an onset unexpectedly, depending on theextent of the waning. Although symptoms areusually mild, the problem is that the patient cantransmit a secondary infection to susceptiblepeople, which may be a source of regional out-break. The same situation is considered to occurwith rubella.
Purpose of 2-dose immunizationWe would need no special measures, if we suf-ficed with a certain degree of measles and rubellacontrol and a reasonable decrease in the number

193JMAJ, May/June 2008 — Vol. 51, No. 3
COMBINED MEASLES AND RUBELLA (MR) VACCINE
of patients. However, there will always be morepeople who contract measles and develop severeconditions (both children and adults) and morecases of CRS. If we want to minimize the numberof people contracting measles and rubella as faras possible and prevent severe cases and CRS asmuch as possible, we need to further reinforcemeasures against these diseases.
One method introduced to achieve that is the2-dose measles and rubella vaccination. The sec-ond dose is given for the following three purposes:(1) A person who missed the first opportunity for
vaccination and who remains susceptible isgiven a second opportunity for vaccinationand acquires immunity;
(2) A person having failed to acquire immunityafter the first vaccination receives the secondvaccination and acquires immunity; and
(3) A person having acquired immunity butwho later becomes susceptible amid waningimmunity receives re-stimulation (a booster)to re-establish immunity.
All these are measures targeted at susceptiblepersons, with the dual meanings of individualprevention to protect individuals from infectionon the one hand and the elimination of measlesand rubella from society through an increasein the percentage of immunized individuals onthe other.
Does the Availability of the SecondVaccination Opportunity Mean thatthe First Dose May Be Delayed orMissed? (Meaning of 2-Dose Schedule)
For both diseases, vaccination should be given asearly as possible (as soon as possible after a childhas reached the age of 1 year, for improvedsafety). If children were left without immunityfor an extended period, possible exposure tovirus would increase the risk of infection and theonset of disease, notwithstanding the fact thatthe number of patients has decreased. In the caseof rubella, disease onset in children may havesignificant impacts on adults. Therefore, the basicprinciple is to ensure the first vaccination andmaintain a high vaccination rate, which does notrepresent any change from the traditional stance.The availability of the second vaccination oppor-tunity does not mean that one may postpone thefirst vaccination.
Incidentally, the law amendment in April 2006
required that routine preventive vaccinationagainst measles and rubella should be conducted“using an MR vaccine.” This resulted in a serioussituation whereby there were no vaccines forroutine vaccination that could be given to indi-viduals needing only the measles or rubella vac-cine respectively (there is a legal restriction thata person already having had the target disease isnot covered by routine vaccination—this in itselfis a controversial issue). The notification releasedby MHLW in June remedied this situation. Thesingle measles vaccine and single rubella vaccinewere restored to the list of vaccines able to beused as routine vaccinations, and the problemwas generally resolved.
Is the Best Timing for the SecondVaccination the Time before Entranceinto Elementary Schools?
If we emphasize (1) and (2) among the above-mentioned three purposes of the second vaccina-tion, the interval between the first and seconddoses should be as short as possible. However,the goal of (1) can also be substantially achievedthrough efforts to maintain the vaccination rateof the first dose as high as possible.
On the other hand, the goal of (3) is betterachieved if the second dose is given when immu-nity is likely to wane and approach the minimumeffective level. In the case of measles, waning ofimmunity is reported to begin 5 to 6 years aftervaccination at the age of 1 in an environmentwithout natural measles. Some report that a dropbelow the minimum effective level occurs laterin the higher grades of elementary schools. Theimmunity against rubella persists longer thanthat against measles. To ensure immunity duringchild-bearing age, it may be desirable that thesecond dose ideally be given in the late teens.
However, under present circumstances, themost practical timing to ensure effective provi-sion of the vaccination opportunity is around thetime of entrance into elementary schools. Profes-sionals in Japan and overseas generally agreethat vaccination later than this would result in adrop in the vaccination rate. In most countriesusing the 2-dose schedule for measles and rubellavaccination, the second dose is given around thetime of entrance into elementary schools.

194 JMAJ, May/June 2008 — Vol. 51, No. 3
Why the MR Vaccine Is Used
Minimizing the number of vaccination dosesgiven to a child was an important point con-sidered during the introduction of the 2-dosemeasles and rubella vaccination. If 4 doses, 2doses each for each disease, were to be given,the burden on children would be large, as wellas the manpower requirement and the cost ofvaccination, resulting in a drop in the vaccinationrate. A larger number of vaccination doses wouldalso increase the possibility of coincidental dis-eases that might be confused with a side reactionfrom the vaccination (so-called coincidental acci-dents), which might lead to misunderstandingregarding the safety of the vaccination. The MRvaccine was introduced for these reasons.
A question arises here regarding the reasonwhy MMR (measles, rubella, and mumps) vac-cine was not introduced. In Japan, the use of theMMR vaccine was discontinued in 1993 becauseof the frequent occurrence of acute viral menin-gitis caused by the mumps virus contained inthe MMR vaccine. Regrettably, the developmentof a Japanese-made mumps vaccine, targeting therelease of a new MMR vaccine, has since madelittle progress. It would be too time-consumingwere we to wait for the introduction of a Japanese-made MMR vaccine.
A brand of foreign-made MMR vaccine hasalready undergone clinical trials in Japan, but thisvaccine has not yet been introduced into thecountry due to the high occurrence of fever aftervaccination. Another possible option would be acombined vaccine, consisting of a foreign-mademumps virus strain and a Japanese-made measlesand rubella virus strains. However, at present,no foreign vaccine manufacturer exists that iswilling to export a mumps virus strain singly, andthe practical use of such a vaccine is unlikely.Under such circumstances, Japan decided to usethe domestically-produced MR vaccine.
Efficacy and Adverse Events ofthe MR Vaccine
Two companies in Japan produce and marketthe MR vaccine, which is produced by mixingthe conventional measles and rubella vaccinestogether in the production process. At the drugapproval stage, the MR vaccine has been shown
to be effective enough to achieve an antibodypositive rate of about 100% for measles and98–100% for rubella. The adverse events profileis similar to that of conventional single vaccines,including fever in 22–27% and skin rash in 10–22%. No serious adverse events have not beenreported so far, and they are considered to besimilar to those reported for single vaccines.Post-marketing studies are ongoing.
Global Measles and Rubella ControlMeasures
Globally speaking, EPI activities are promotedusing a vaccination strategy that targets the glo-bal control of polio; diphtheria, pertussis, andtetanus (DPT); tuberculosis (BCG); measles; andhepatitis B.
Recent experiences, including the outbreakof measles in the Netherlands and Ireland, theepidemic of rubella in Greece, and the frequentoccurrence of CRS have demonstrated that asuboptimal level of herd immunity may allow theresurgence of measles infection and death, aswell as CRS. It is considered important to main-tain the percentage of immunized individuals ata level of 90–95%. The basic strategy, in the caseof measles, is a 2-dose vaccination using a singleor combined vaccine (MR or MMR vaccine). The2-dose measles vaccination had been introducedin 114 countries (as of 2004) and most developedcountries use the MMR vaccine. Over 250 milliondoses of MMR vaccine are used in over 35 coun-tries, recording a high level of safety.
In contrast to measles, countries incorporat-ing rubella into national strategies are mostlydeveloped countries. As mentioned before, theintroduction of the rubella vaccine is delayedin countries with poor economic standing.
History of International Measles Control
The 1989 general assembly of the WHO declaredthe goal of achieving a 90% reduction in measlesprevalence and a 95% decrease in measles mor-tality by 1995 relative to the pre-vaccine era. TheWorld Summit for Children the following yearapproved the goal of raising the vaccination rateamong children to 90%.
The world is divided into six regions under theglobal WHO policy. With the progress of measlescontrol activities, each of these regions is shifting
Okabe N

195JMAJ, May/June 2008 — Vol. 51, No. 3
from a decrease in measles prevalence to theelimination of the disease itself. In 1994, the PanAmerican Health Organization (PAHO) set theyear 2000 as the target year for the regionalelimination of measles, and succeeded in elimi-nating endemic measles transmission in 2002. Inother regions, the European Regional Office(EURO) set 2007 and the Eastern MediterraneanRegional Office (EMRO) set 2010 respectivelyas the target years for measles elimination.
In contrast to the zero-virus goal of “eradi-cation” pursued for smallpox and polio, “elimi-nation” is defined by the WHO as “a dynamicsituation in a large and well-populated geographi-cal area where no endemic measles transmissionoccurs and where the importation of measles virusdoes not result in sustained transmission.” Thismeans that any occasional importation of measlesdoes not cause the expansion of secondary andtertiary infections.
The West Pacific Regional Office (WPRO) ofthe WHO, where Japan belongs, did not have aregional elimination target until 2005, but severalcountries promoted control measures settingnational elimination targets, and achieved theelimination of transmission in each country. InSeptember 2005, the Regional Committee Meet-ing in the WPRO decided that 2012 would be thetarget year for measles elimination in this region,following the agreement among Japan, China,and other countries.
Future Measles and Rubella Control inJapan
The introduction of the 2-dose measles andrubella vaccination and that of the MR vaccinein April and June 2006, respectively, made itpossible to integrate the measures for measlescontrol and those for rubella control, represent-ing significant progress in measles and rubellacontrol in Japan. However, this amendment hasleft some problems. The period for which a childcan receive routine preventive vaccination againstmeasles and rubella has been shortened, whilesusceptible individuals older than elementaryschool age are not covered by routine vaccinationand accumulate in society. We need to be awareof the limitations concerning what can be donethrough routine vaccination conducted based onthe law.
In order that the introduction of 2-dose vac-
cination using MR vaccine may be an effectivestep to achieve the WPRO goal of eliminatingmeasles by 2012, it is necessary to ensure highvaccination coverage for both doses in all agegroups. We need the prompt development of anational vaccination strategy, targeting not onlymorbidity reduction but also measles eliminationand CRS eradication. We need to continue ourefforts to tackle these diseases, always keepingin mind the essential problems of measles andrubella, despite the fact that they are graduallyvanishing.
Addendum:After the writing of this article, there have beensome major developments in the measles andrubella control measures in Japan, as outlinedbelow.
In 2007, Japan experienced an outbreak ofmeasles, which mainly affected young people andcaused temporary closure of many high schoolsand universities. This was pronounced an inter-national problem, as there were cases such as thestudent who developed measles during an over-seas school trip, as well as the elementary schoolstudent who developed symptoms during aninternational sport event and caused secondaryand tertiary transmission of infection amonglocal inhabitants.
This outbreak took place when the measlesvirus that existed in the streets was brought intoschools. Students living in group settings in theseschools are classified as follows:1) those who had not received measles vacci-
nation and fortunately had not contractedmeasles (approximately 10%),
2) those who had received measles vaccinationin infancy but had not acquired immunity (pri-mary vaccine failure; 2–3%), and
3) those who had undergone gradual declineof immunity as a result of the lowering ofmeasles prevalence and a lack of opportuni-ties to receive stimulation (secondary vaccinefailure; approximately 10%).The fact that students engage in various activi-
ties in various places helped the expansion of theepidemic.
This outbreak of measles posed three problems:1) Infection in individuals without immunity
causes severe conditions irrespective of theage of patient, and presents high risks to indi-viduals including the risk of complications.
COMBINED MEASLES AND RUBELLA (MR) VACCINE

196 JMAJ, May/June 2008 — Vol. 51, No. 3
2) Although individuals who have undergonegradual decline of immunity do not developtypical and serious measles symptoms, theycan become sources of infection and affectfamilies, friends, neighbors and society as awhole.
3) “Elimination” is the common goal pursued inthe world. As seen from other countries, thesituation in Japan invokes the notion of why arespected country such as Japan should stillhave measles. Exportation of measles fromJapan is actually a great nuisance to othercountries, and control measures in Japan aregenerally considered unsatisfactory.To solve these problems and to realize measles
elimination, which the WHO Regional Office forthe Western Pacific (WPRO) aims to attain by2012, Japan belatedly has started major improve-ment in measles control measures. The first cleardeclaration of the need for measles control as anational policy was made in the Minister’s Noti-fication “Guidelines for Prevention of SpecifiedInfections Regarding Measles” dated December28, 2007. These guidelines stipulate the goalof “achieving measles elimination by the fiscalyear 2012 and maintaining the condition after
elimination.”In specific terms, the reporting requirements
for measles under the Law Concerning Infec-tious Diseases were amended, and the previoussystem of reporting from approximately 3,000pediatric sentinels was changed to the reportingfrom all physicians covering all cases in Category5 classes in Infectious Disease Control Law.Similarly, the reporting of rubella cases was alsochanged to notifiable diseases for the purposeof supporting simultaneous implementation ofmeasures for the congenital rubella syndrome(CRS).
It was also decided that routine vaccinationwould be conducted at ages corresponding tothe first year of junior high school and the thirdyear of high school, to be implemented for 5years from April 1, 2008, as supplementary vac-cination. MR vaccine will be principally used inthis program.
With the reinforcement of the first and secondvaccination and the introduction of this supple-mentary vaccination plan, Japan has taken a stepforward to the realization of measles elimination,which the WHO WPRO aims to attain by 2012,and CRS elimination as well.
Okabe N
References
1. Infectious Disease Surveillance Center, National Institute ofInfectious Diseases. Present State of Measles and FutureMeasles Control Measures; 2002 October (http:// idsc.nih.go.jp/disease/measles/report2002/measles/top.html). (in Japanese)
2. Task Team for Study Projects on Emerging and Resurging Infec-tions Conducted under Scientific Study Subsidy of the Ministry ofHealth, Labour and Welfare, “Study on the Development of Pre-ventive Measures against Mother-to-Child Infection Associated
with Rubella Epidemic.” Emergency Proposal Regarding RubellaEpidemic and Prevention of the Congenital Rubella Syndrome;2004 August. (in Japanese)
3. Website of Infectious Disease Surveillance Center, NationalInstitute of Infectious Diseases (http:// idsc.nih.go.jp/ index-j.html).(in Japanese)
4. Okabe N, Taya K (Eds.). Q & A’s about Vaccination, 2006 version.Tokyo: Saikin Seizai Kyokai; 2006. (in Japanese)

197JMAJ, May/June 2008 — Vol. 51, No. 3
From the Japanese Association of Medical Sciences
*1 President, the Japanese Society of Hypertension, Tokyo, Japan ([email protected]).
Hypertension Research in Japan andthe Japanese Society of Hypertension
JMAJ 51(3): 197–198, 2008
Hiroaki MATSUOKA*1
seminars on these guidelines to disseminate themamong clinicians all over Japan. At present,JSH is working toward issuing new guidelines(JSH2009) in 2009. At the time when JSH2000was developed, there was very little evidenceoriginating in Japan. The only notable interna-tionally recognized achievement was the epide-miological study in Hisayama Town. Data havelater accumulated as a result of several epidemio-logical studies including the Ohasama Study andthe Tanno Sobetsu Study.
Japan has historically been reluctant to con-duct randomized intervention studies to evaluatethe efficacy of hypotensive agents, partly becauseof the mass media’s perception that such studieswould be experiments using patients. However,we are now seeing reports of large-scale ran-domized intervention studies conducted usingpatients with hypertension in Japan. This reflectsthe enthusiasm and efforts of researchers, aswell as the people’s understanding of large-scaleintervention studies. We are now endeavoring tomake the best use of the results from these epide-miological studies and large-scale interventionstudies in Japan as a source of evidence to sup-port JSH2009.
Japan has long made an excellent internationalcontribution in the basic study of hypertension.For example, many substances involved in bloodpressure control were reported by researchersin Japan. More than a century ago, Takamineet al. discovered adrenalin in 1901. Arakawa et al.determined the structure of angiotensin 1 in1967, and Murakami et al. cloned the cDNA forhuman renin in 1983. In 1984, Kangawa, Matsuo,et al. determined the structure of the hypotensivepeptide ANP, followed by the subsequent deter-mination of the structure of ANP family peptides
This article describes the hypertension research(both basic and clinical) conducted in Japan andthe issues the Japanese Society of Hypertension(JSH) is trying to solve.
More than 30 million Japanese are classified ashaving hypertension, defined by a systolic bloodpressure of 140 mmHg or more, or a diastolicblood pressure of 90 mmHg or more, or the use ofa hypotensive agent. The blood pressure level ofthe Japanese people has been decreasing steadilyafter a peak in about 1965. The widespread avail-ability of hypertension therapy is considered tohave contributed to this decrease. Stroke, a con-dition closely associated with hypertension, hasalso been showing decreases in prevalence andmortality rates after peaking in 1965–1970. Inthis way, the widespread availability of hyperten-sion therapy may be regarded as a factor in theJapanese being the world’s longest living people.
Japan has an excellent health care systembased on health insurance programs coveringall citizens, which ensures that all patients withhypertension have access to appropriate care.However, the decline in the mortality rate fromstroke has slowed in recent years, and the mor-tality rate from ischemic heart disease is showinga tendency to gradual increase. These changesmay be attributed to the increases in the numberof people with diabetes and dyslipidemia result-ing from the Westernization of eating habits anda lack of exercise in an automobile dependentlifestyle. Comprehensive management of hyper-tension, diabetes, and dyslipidemia incorporatinglifestyle changes is essential to the prevention ofcardiovascular diseases.
JSH published guidelines for hypertensiontreatment in 2000 and 2004 (JSH2000 andJSH2004), and has been organizing educational
Japanese Society of Hypertension

198 JMAJ, May/June 2008 — Vol. 51, No. 3
Matsuoka H
such as BNP and CNP. These achievements haveled to the use of ANP in heart failure treatmentand BNP in the staging of heart failure. In 1988,Yanagisawa et al. discovered the hypertensivepeptide endothelin, and endothelin antagonistsare now used in the treatment for pulmonaryhypertension. In addition, Kitamura, Kangawa,et al. discovered the hypotensive peptide adreno-medullin in 1993. The discovery of these peptidesis revolutionizing the etiology, pathology, andtreatment of not only hypertension but also othercardiovascular diseases.
Furthermore, the spontaneously hypertensiverat (SHR), an animal model for essential hyper-tension produced by Okamoto and Aoki, made abreakthrough in the study of the pathogenesisand pathology of essential hypertension, as wellas the development of hypotensive agents. Thesestudies undoubtedly have been making a greatcontribution to the advancement of hypertensionresearch in the world. With this as the back-ground, the 12th and the 21st Scientific Meetingsof the International Society of Hypertensionwere held in Kyoto in 1988 and Fukuoka in 2006,respectively.
JSH is going to celebrate its 30th anniver-sary this year. The Society originally started asa gathering of researchers specializing in hyper-tension, where presentations and discussion ofselected themes were given. However, consider-
ing that wider participation is needed for furtherevolution of JSH, we are now widely invitingpresentations from clinicians and co-medicalprofessionals, and welcoming the participation ofmany interested persons.
The activities of JSH include: 1) holding anannual scientific meeting; 2) issuing the guide-lines for hypertension treatment at intervals ofseveral years; 3) co-sponsoring and supportinglarge-scale intervention studies; 4) issuing Hyper-tension Research, the monthly official journal ofthe Society in English (the impact factor in 2006was 3.177); 5) organizing educational seminarsacross Japan; 6) organizing working groups onsuch themes as salt reduction, diuretics, homeblood pressure monitoring, and the diagnosticcriteria for secondary hypertension to discussappropriating blood pressure evaluation, diag-nosis of hypertension, and treatment; 7) pro-moting educational and outreach programs forthe general public through the establishmentof the Japanese Association of Hypertension;and 8) promoting international research coop-eration through participation in the InternationalSociety of Hypertension and China-Japan JointHypertension Symposium. Finally, as the intro-duction of a specialist program was approved bythe JSH general meeting last year, we are work-ing hard preparing for the launch of the specialistprogram in 2008.
199JMAJ, May/June 2008 — Vol. 51, No. 3
From the Japanese Association of Medical Sciences
*1 Professor and Chairman, Division of Gastroenterology and Hepatology, Department of Internal Medicine, Jikei University School of Medicine,Tokyo, Japan ([email protected]).*2 President of the Japan Gastroenterological Endoscopy Society, Tokyo, Japan. Professor, Department of Internal Medicine, St. MariannaUniversity School of Medicine, Kawasaki, Japan.
Recent Advances in Electronic Endoscopes:Image-enhanced endoscopy
JMAJ 51(3): 199–203, 2008
Hisao TAJIRI,*1 Hirohumi NIWA*2
endoscopy is sub-divided into optical, digital,optical-digital and chromoendoscopy methods(Fig. 1). Of all the various image-enhanced endos-copy methods currently available, “special lightobservation,” a term which has recently begun tobe used at meetings of academic societies andresearch organizations, refers specifically to theoptical-digital method.
The optical-digital method of “image-enhancedendoscopy” involves conversion of the opticalcharacteristics of the light used for illuminationor imaging with a light source differing in opticalcharacteristics from ordinary white light. Thismethod also involves signal processing withina video processor in a specially designed wayto yield enhanced images. This method usuallyencompasses NBI, auto-fluorescence imaging(AFI) and infra-red imaging (IRI).
Light penetration can be restricted to surfacelayers using a blue filter from amongst the spec-tral transmittance of the three Red, Green andBlue (RGB) optical filters used in sequentialframing to create a narrow band that cuts longwavelengths. With NBI, the central wavelengthis optimized at 415 and 540 nm, correspondingto the wavelengths most intensely absorbed byblood and those showing intense reflection andscattering at the mucosal surface. Using a narrowspectrum range, the objective of this method is toemphasize fine mucosal structures and mucosalmicrovasculature on the gastrointestinal (GI)tract surface.
A study using magnifying endoscopy com-bined with the NBI system has shown thatmicrovascular patterns of superficial depressed
Gastrointestinal endoscopy began with the intro-duction of the gastroscope, which prompted activeclinical use of endoscopes in subsequent years.After the gastroscope was introduced, variousfiberscopes began to be used clinically. In 1983,electronic videoendoscopes were also developed.Unlike fiberscopes, which directly check lightsignals, electronic videoendoscopes convert elec-tronic signals into images via semiconductorelements and allow various forms of electronicimage processing and analysis.
Recently, it has been demonstrated that narrowband imaging (NBI) (Olympus Medical SystemsCo., Tokyo, Japan) is useful in early diagnosis ofcancers of the oropharynx, hypopharynx, esopha-gus, stomach and large intestine.1 This findinginvited many responses not only from Japaneseinvestigators but also colleagues in many othercountries, and NBI has been attracting consider-able attention amongst academic societies andresearch organizations. In Japan, the term “spe-cial light (observation)” is now used frequently.A succession of similar techniques were latermade public and the meaning of the term “speciallight (observation)” came to have differ amongstacademic societies and research organizations. Inview of this problem and the necessity of estab-lishing internationally applicable terminology forendoscopy, we propose object-oriented classifica-tion as new classification for endoscopic imaging.
Endoscopic imaging is divided into categories:(1) conventional endoscopy (white light endos-copy (WLE)); (2) image-enhanced endoscopy; (3)magnified endoscopy; (4) microscopic endoscopy;and (5) tomographic endoscopy. Image-enhanced
Japan Gastroenterological Endoscopy Society

200 JMAJ, May/June 2008 — Vol. 51, No. 3
Tajiri H, Niwa H
carcinomas of the stomach can be classified intotwo types: fine network patterns and corkscrewpatterns, which correspond to well and poorlydifferentiated adenocarcinoma, respectively.2
Therefore, the NBI system can be a powerful toolin the optical pathology of gastric tumors and canbe utilized in gastric cancer treatments such asendoscopic submucosal dissection (ESD).
The usefulness of magnifying endoscopycombined with the NBI system has been studiedwith regard to the detection of specialized intes-tinal metaplasia (SIM) in columnar-lined esopha-gus and Barrett’s adenocarcinoma.3 Fifty-eightpatients, including 4 with superficial Barrett’sadenocarcinoma, were enrolled in this study. Themost characteristic endoscopic patterns of SIMwere revealed to be the cerebriform fine mucosalpattern (sensitivity 56%; specificity 79%) andivy-or DNA-like capillary pattern (sensitivity77%; specificity 94%). Magnifying endoscopycombined with the NBI system enabled precisevisualization of the structure of capillaries in thesuperficial mucosal layer. The addition of capil-
lary patterns for fine mucosal patterns appearedto improve the diagnostic value for detectingSIM and superficial Barrett’s adenocarcinomaupon observation using NBI.
A multicenter prospective randomized con-trolled study has been conducted in Japan on thedetection rate and diagnostic accuracy for super-ficial squamous cell carcinoma in the esophagus(ESCC) and the head and neck region (HNSCC),NBI vs. WLE.4 Three hundred and twenty patientswith ESCC were randomly assigned into 162 NBIfollowed by WLE, and 158 WLE followed byNBI. In the first examination, the detection ratesfor the superficial lesion using NBI were sig-nificantly higher than those using WLE (H&Nregion 22 vs. 2, P�0.0001; Esophagus 130 vs. 65,P�0.0001). Diagnostic accuracy for histologi-cally confirmed ESCC and HNSCC using NBIwas high compared to WLE (90.1% and 56.8%,respectively). These results indicate that NBIcould be a standard examination for achievingaccurate diagnosis of superficial ESCC andHNSCC (Fig. 2).
Fig. 1 Object-oriented classification of endoscopic imagingFICE: Fujinon (flexible) imaging color enhancement; RIM: real time image mapping;AFI: auto-fluorescence imaging; SAFE: simultaneous auto-fluorescence endoscopy;NBI: narrow band imaging; IRI: infra-red imaging.
Endoscopic Imaging
Contrast method
Lineation enhanced method
Auto-fluorescent method
Narrow band light method
Infra-red ray method
Stain method
Contrast method
ie: Ultraviolet/Infra-red observation
ie: FICE/RIM
ie: Structure enhancement
ie: AFI/SAFE
ie: NBI
ie: IRI
ie: Lugol
ie: Indigocarmine
ie: Optical zoom endoscopy
ie: Digital zoom
ie: EndoCytoscopy
ie: Endomicroscopy
Conventional Endoscopy (White Light)
Image-Enhanced Endoscopy
Optical Method
Digital Method
Optical-Digital Method
Chromoendoscopy Method
Magnified Endoscopy
Optical Method
Digital Method
Microscopic Endoscopy
Optical Method
Digital Method
Tomographic Endoscopy
Optical Coherence Tomography
Endoscopic Ultrasonography

201JMAJ, May/June 2008 — Vol. 51, No. 3
RECENT ADVANCES IN ELECTRONIC ENDOSCOPES: IMAGE-ENHANCED ENDOSCOPY
Fig. 2 Endoscopic images of superficial esophageal squamous cell carcinoma (0-IIc)Conventional endoscopic findings show reddish area formation (a). The demarcated brownish area can be seen with NBIobservation (b). Magnified endoscopic findings combined with NBI show changes in dilatation, tortuosity, and calibre ofthe intra-papillary capillary loop (IPCL) pattern (c). The size of the area unstained by iodine (d) and the NBI observationscorresponded closely. A lesion was diagnosed as well differentiated squamous cell carcinoma (m3).
Fig. 3 Endoscopic images of a laterally-spreading tumor (LST) with granular changes to the rectum(25mm in size, white light endoscopy used) (a) and auto-fluorescence endoscopy (b)
The one-push button changes the light from white light endoscopy to auto-fluorescent endoscopy simply and easily.With auto-fluorescent endoscopy, the tumor margin can be seen clearly as magenta color. The lesion was diagnosedhistologically as well differentiated adenocarcinoma after endoscopic mucosal resection (EMR).
a
c d
b
a b

202 JMAJ, May/June 2008 — Vol. 51, No. 3
With regard to colorectal lesions, it has beenreported that accuracy in the differentiation ofneoplastic and non-neoplastic lesions was thesame for chromoendoscopic imaging and NBI.5
Sano et al.6 reported that capillary vessels wereenhanced more than usual in colorectal neo-plasm, and classified capillary patterns (CP) intomajor three classes: CP Type I is invisible orfaintly visible microvessels; CP Type II is clearlyvisible and slightly thicker capillaries with loosecapillary density; and CP Type III is clearlyvisible and uneven-sized thicker capillaries withbranching, curtailment, and irregularity withthick capillary density. In this third type, vascularcasts of colonic carcinoma are characterized bya disorganized structure and density of micro-vessels, and the increased number and densityof microvessels results in formation of nodularclusters of capillaries. In addition, many endosco-pists in Japan are researching capillary patternsfrom various standpoints in order to further thequality of endoscopic diagnosis., NBI is also indi-cated to be an effective examination method inevaluating the mucous membrane and discover-ing displasia and colitic cancer in inflammatorybowel disease. NBI is an examination methodwith great potential.
Fluorescence endoscopy used to detect earlycarcinomas and discriminate between normaland neoplastic lesions has recently attractedconsiderable attention. Collagen, the fluores-cence of which is in the green wavelength range,is one of the major sources of tissue auto-fluorescence (AF). However, there are importanttissue changes other than, or in addition to,changes in gross tissue morphology. These mayinclude alterations in the local blood volume, tis-sue metabolic activity, and relative fluorophoreconcentrations.
For AF endoscopy, a new AF imaging video-scope system (AFI, Olympus Medical SystemsCo.) has been developed. The new AFI systemfeatures a switch for selecting either Red, Green,or Blue (RGB) illumination light for WLE or anexcitation/reflected light-illumination light com-bination for AFI. The light source incorporates arotary filter, which is designed in a double-wheelconfiguration with two concentric wheels: anRGB filter wheel for normal imaging and an AFIfilter wheel. When the AFI mode is selected, thelight emitted from the xenon lamp is input intothe rotary filter and divided between the 390 to
470 nm excitation light and 540 to 560 nm greenlight. The AFI scope incorporates a monochromeCCD that has a barrier filter for cutting the exci-tation light to capture weak AF. A pseudo-colorimage is reconstructed based on the AF inputsignals so that high AF intensity is a greenishcolor and low intensity is magenta.
If the blue light for excitation reaches thesubepithelial layer, AF is generated. Fluorescentobservation attempts to convert AF into animage which highlights a tumorous lesion as anarea differing in fluorescence intensity or colorfrom the adjacent intact tissue with the goal offacilitating the detection and diagnosis of tumor-ous lesions. The new AFI system is very easy touse because the one-push button changes thelight from WLE to AF simply and easily.
A comparative study was conducted with theWLE and AFI systems to differentiate neoplasticfrom non-neoplastic lesions in 190 cases.7 Resultsfound the sensitivity, specificity and accuracy tobe 98%, 92% and 99%, respectively. These resultssuggested that AFI might enable easy differen-tiation of neoplastic from non-neoplastic lesionsin the colon (Fig. 3). In addition, we conducted aprospective blinded study that systematicallycompared AFI with WLE use in the detection ofsuperficial gastric neoplasia.8 One quarter of theelevated gastric neoplasia cases were detectedonly with AFI. It is thought that AFI is a systemwith great promise for diagnosing early carcino-mas and premalignant lesions in the GI tract asan adjunct to WLE. In particular, it has potentialas a method of identifying small or flat tumors,tumor margins, grading, and premalignant lesions,and for assessing tumor response to therapy.
Dramatic advances in the diagnosis of diseasein the GI tract have been made with “image-enhanced endoscopy” in electronic endoscope,including NBI and AFI as mentioned above. Thefrequency of less-invasive targeting treatmentmethods, with which affected sites may betreated more precisely and non-affected sitesmay be preserved as much as possible by utilizingdiagnostic images, is expected to increase. Diag-nostic endoscopy will be divided into two oppo-site directions in the future.9 In one direction, thediameter of endoscopes is decreasing and exami-nation will progress to screening tests using wire-less capsule endoscopy. In the other direction,highly precise imaging techniques are progress-ing. In the former, who will perform the screening
Tajiri H, Niwa H

203JMAJ, May/June 2008 — Vol. 51, No. 3
References
1. Tajiri H. Future perspectives of gastrointestinal endoscopyand joint academic-industrial research following technologicalinnovation in medical and biological engineering. Dig Endosc.2005;17:S97–S104.
2. Nakayoshi T, Tajiri H, Matsuda K, et al. Magnifying endoscopycombined with narrow band imaging system for early gastriccancer: correlation of vascular pattern with histopathology.Endoscopy. 2004;36:1080–1084.
3. Goda K, Tajiri H, Ikegami M, et al. Usefulness of magnifyingendoscopy with narrow band imaging for the detection of spe-cialized intestinal metaplasia in columnar-lined esophagus andBarrett’s adenocarcinoma. Gastrointest Endosc. 2007;65:36–46.
4. Muto M, Saito D, Tajiri H, et al. Multicenter prospective random-ized controlled study on the detection and diagnosis of super-ficial squamous cell carcinoma by back-to-back endoscopicexamination of narrow band imaging and white light observation.
Gastrointest Endosc. 2007;65:AB110 (abstract).5. Machida H, Sano Y, Hamamoto Y, et al. Narrow-band imaging
in the diagnosis of colorectal mucosal lesions: a pilot study.Endoscopy. 2004;36:1094–1098.
6. Sano Y, Horimatsu T, Fu KI, et al. Magnifying observation ofmicrovascular architecture of colorectal lesions using narrowband imaging system. Dig Endosc. 2006;18:S44–S51.
7. Tajiri H. Autofluorescence endoscopy for the gastrointestinaltract. Proc Jpn Acad Ser B. 2007;83:248–255.
8. Kato M, Kaise M, Yonezawa J, et al. Autofluorescence endos-copy versus conventional white light endoscopy for the detectionof superficial gastric neoplasia: a prospective comparative study.Endoscopy. 2007;39:937–941.
9. Tajiri H. What do we see in the endoscopy world in 10 year’stime? Dig Endosc. 2007;19:S174–S179.
RECENT ADVANCES IN ELECTRONIC ENDOSCOPES: IMAGE-ENHANCED ENDOSCOPY
test and how the medical expenses should bestructured will become issues. Endoscopy per-formed by a properly trained endoscopist is saferand better, produces a higher yield, and is more
cost effective, as the endoscopist translates endo-scopic information into the patients’ manage-ment files.

204 JMAJ, May/June 2008 — Vol. 51, No. 3
Local Medical Associations in Japan
physicians and not just for physicians in privatepractice, and for hospital-based physicians andthose in private practice to collaborate to addressand resolve various issues towards the achieve-ment of better medical care for the health ofpeople.
In the “Speaking Up” column in the 20 August2004 edition of JMA Newsletter, PresidentAriumi wrote, “Since private practitioners haveexperience as hospital-based physicians andhospital-based physicians may, in future, go onto open their own practices, it should not bedifficult for them to share approaches to correct-ing the distortions in current medical practice,”and “Interest should be taken in the fact that theroot cause underlying the uneven distribution inhospital-based physicians and their work over-load is Japanese governmental policies.” It isagainst this background that the YMA is engagedin the following efforts:
I would like to discuss the issue of hospital-basedphysicians, one that we have lately been engagedwith in the Yamagata Medical Association (YMA).
Hospitals in Japan are currently beset by wide-ranging waves of transformation and diversedemands, not least healthcare system reform,management reform and efficiency measures. Ibelieve that we, as healthcare personnel, shouldaccept this wave of reforms and demands as acontemporary trend of our era. Although it willrequire manpower, time and money to tacklethese issues properly, the fact is that hospital-based physicians, whose hands are already fullwith their medical practices, will have to find thetime from their own schedules to act on theseissues; moreover with hardly any personnel orfinancial support. However, it is no exaggerationto say that even if hospital-based physicians areindividually aware of the issues, they lack anymeans to collate, analyze and study the facts orseek potential solutions to the problems.
Understanding these circumstances faced byhospital-based physicians, the YMA, under the ini-tiative of President Miyuki Ariumi, has embarkedon a number of measures to ascertain the circum-stances of hospital-based physicians, analyze theproblems and study the nature of proposals andsupport that the medical association could offertowards resolving the same. We are also hopingthat this would bring a call for awareness amonghospital-based physicians that the medical asso-ciation supports the healthcare activities of all
*1 Executive Board Member, Yamagata Medical Association, Deputy Hospital Director, Yamagata Prefectural Central Hospital, Yamagata, Japan([email protected]).This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.134, No.9, 2005,pages 1760–1761).
Tochigi
Yamagata
Pop. 1.2mil.Area 6,700km2
Tokyo
The Medical Association Needs the Power fromHospital-based Physicians and Hospital-basedPhysicians Also Need the Power fromthe Medical Association
JMAJ 51(3): 204–206, 2008
Norio TAKEDA*1
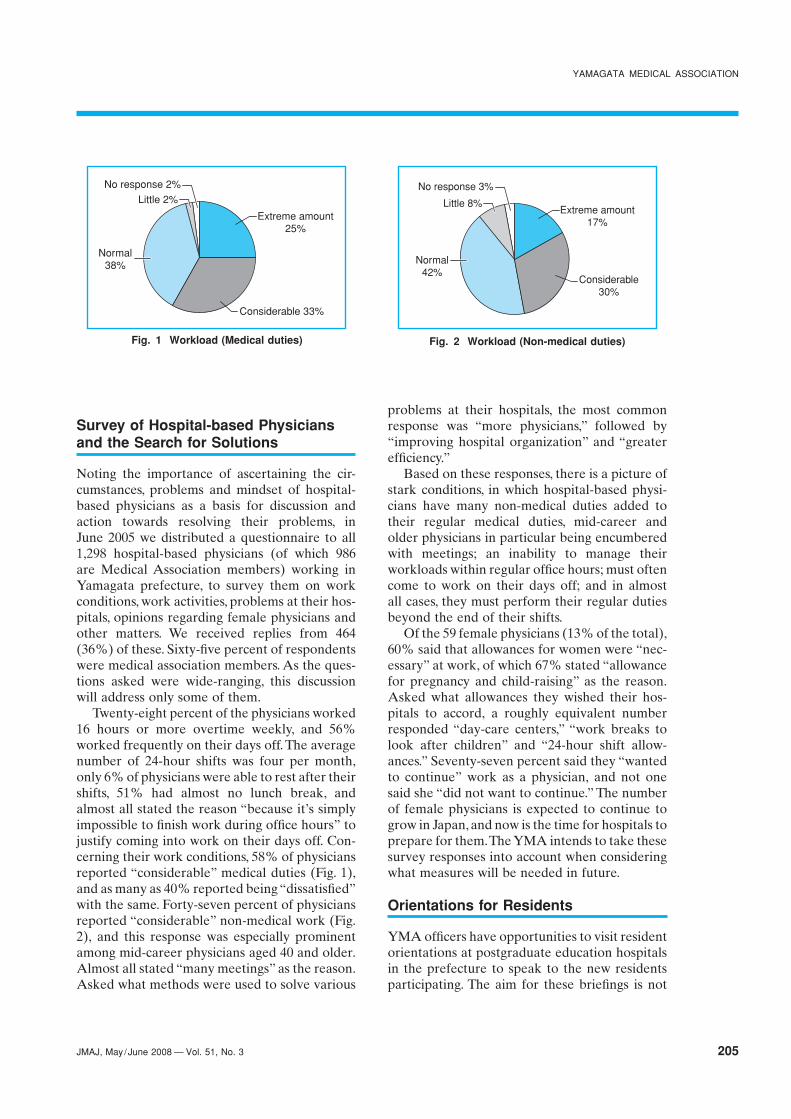
205JMAJ, May/June 2008 — Vol. 51, No. 3
Survey of Hospital-based Physiciansand the Search for Solutions
Noting the importance of ascertaining the cir-cumstances, problems and mindset of hospital-based physicians as a basis for discussion andaction towards resolving their problems, inJune 2005 we distributed a questionnaire to all1,298 hospital-based physicians (of which 986are Medical Association members) working inYamagata prefecture, to survey them on workconditions, work activities, problems at their hos-pitals, opinions regarding female physicians andother matters. We received replies from 464(36%) of these. Sixty-five percent of respondentswere medical association members. As the ques-tions asked were wide-ranging, this discussionwill address only some of them.
Twenty-eight percent of the physicians worked16 hours or more overtime weekly, and 56%worked frequently on their days off. The averagenumber of 24-hour shifts was four per month,only 6% of physicians were able to rest after theirshifts, 51% had almost no lunch break, andalmost all stated the reason “because it’s simplyimpossible to finish work during office hours” tojustify coming into work on their days off. Con-cerning their work conditions, 58% of physiciansreported “considerable” medical duties (Fig. 1),and as many as 40% reported being “dissatisfied”with the same. Forty-seven percent of physiciansreported “considerable” non-medical work (Fig.2), and this response was especially prominentamong mid-career physicians aged 40 and older.Almost all stated “many meetings” as the reason.Asked what methods were used to solve various
problems at their hospitals, the most commonresponse was “more physicians,” followed by“improving hospital organization” and “greaterefficiency.”
Based on these responses, there is a picture ofstark conditions, in which hospital-based physi-cians have many non-medical duties added totheir regular medical duties, mid-career andolder physicians in particular being encumberedwith meetings; an inability to manage theirworkloads within regular office hours; must oftencome to work on their days off; and in almostall cases, they must perform their regular dutiesbeyond the end of their shifts.
Of the 59 female physicians (13% of the total),60% said that allowances for women were “nec-essary” at work, of which 67% stated “allowancefor pregnancy and child-raising” as the reason.Asked what allowances they wished their hos-pitals to accord, a roughly equivalent numberresponded “day-care centers,” “work breaks tolook after children” and “24-hour shift allow-ances.” Seventy-seven percent said they “wantedto continue” work as a physician, and not onesaid she “did not want to continue.” The numberof female physicians is expected to continue togrow in Japan, and now is the time for hospitals toprepare for them. The YMA intends to take thesesurvey responses into account when consideringwhat measures will be needed in future.
Orientations for Residents
YMA officers have opportunities to visit residentorientations at postgraduate education hospitalsin the prefecture to speak to the new residentsparticipating. The aim for these briefings is not
Fig. 2 Workload (Non-medical duties)
Considerable30%
Normal42%
Little 8%
No response 3%
Extreme amount17%
Fig. 1 Workload (Medical duties)
Considerable 33%
Normal38%
Little 2%
No response 2%
Extreme amount25%
YAMAGATA MEDICAL ASSOCIATION

206 JMAJ, May/June 2008 — Vol. 51, No. 3
only to brief fresh physicians on the medical asso-ciation and urge them to pay attention to health-care policy, but also to show our faces and to givethe residents a sense of familiarity with the Medi-cal Association and YMA officers themselves.
Gathering for Board Members ofthe YMA and Hospital-based Physicians
Working from the results of the questionnairesurvey of hospital-based physicians, in 2006 theboard members of the medical association visited11 leading hospitals in Yamagata prefecture tomeet informally with hospital-based physicians.In these meetings almost all hospital-based phy-sicians responding to the another questionnaireperformed before these meetings listed “emer-gency care,” “overtime” and “24-hour shifts” asthe top three issues they wish to see addressed,
the most common response of them was “emer-gency care.” A major issue raised at these meet-ings was that too many emergency patients whodo not need surgical or medical admission weredelivered to the nighttime emergency stations ofcore hospitals designated to provide third-degreeemergency care regionally. Medical collaborationand governmental administrative support will beimportant to the resolution of this problem, andwe are currently holding discussions with localmedical associations and the prefectural authori-ties in search of a better strategy.
We hope continued and varied discussionswill contribute to consolidating the relationshipbetween the medical association and hospital-based physicians and that we both will be able tocombine our wisdom and cooperate in workingtowards the resolution of these problems.
Takeda N

207JMAJ, May/June 2008 — Vol. 51, No. 3
Local Medical Associations in Japan
in different regions in the Kanagawa prefecturearea, which are valued as a source of valuableinformation for devising tailor-made therapiesthat will be of great importance in future.
A social meeting on advanced medicine is alsoheld once a year to study the state of variousaspects of advanced medicine and issues theypresent with the objective of finding a way to theestablishment of a more advanced system for thesupply of healthcare. In 2005 Prof. Tomio Inoueof the Department of Radiology at YokohamaCity University presented a lecture on “RecentTrends in Diagnostic Imaging of Cancers UsingPET/CT.”
Kanagawa Prefecture is home to four univer-sity medical faculties—Tokai University, KitasatoUniversity, St. Marianna University School ofMedicine and Yokohama City University—andthree hospitals affiliated with university medicalfaculties—Teikyo University School of MedicineUniversity Hospital Mizonokuchi, Nippon Medi-cal School Musashi Kosugi Hospital and ShowaUniversity Fujigaoka Hospital. The professorsfrom these universities, the members of the KMAand the directors of the KAMS have regular
As of December 2005 the Kanagawa PrefectureMedical Association (KMA) had a membershipof 8,090. In discussing the association’s activities,I would like to focus on the academic aspects ofthe Kanagawa Association of Medical Sciences(KAMS).
With the addition of the Clinical OrthopedicAssociation in 2003, the KAMS now comprises 21sectional groups (Table 1). The association worksto foster these sectional groups, holding an infor-mal meeting once a year with the presidents ofthese sectional groups as an occasion for exchangeof opinion on such matters as the requestsheld by the sectional groups and each year onNovember 23 holding an academic conferenceand general meeting of the association featuringawards presented to distinguished academics,general lectures, special lectures and symposia.In view of the opening in August 2006 as theKanagawa Special Biomedical Industrial Zone,which in July became the first authorized inJapan, of a hospital performing such advancedcosmetic treatments as breast regeneration withstem cells derived from fat, the acclaimed sympo-sium addressed the state and future outlook forregenerative medicine, including dermal, cardiacand neural regeneration as well as soft tissuessuch as breasts.
The association’s academic Kanagawa IgakkaiZasshi (Journal of the Kanagawa Medical Asso-ciation) publishes two issues annually compilingpapers submitted by its members and abstractsfrom sectional group meetings. Most of originalpapers describe field surveys of various illnesses
*1 Board Member, Kanagawa Prefecture Medical Association, Yokohama, Japan ( [email protected]).This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.135, No.4, 2006,pages 866–867).
Tochigi
Kanagawa
Pop. 8.8mil.Area 2,400km2
Tokyo
Activities of the Kanagawa PrefectureMedical Association Focusingon Its Academic Area
JMAJ 51(3): 207–208, 2008
Isao YAMAMOTO*1
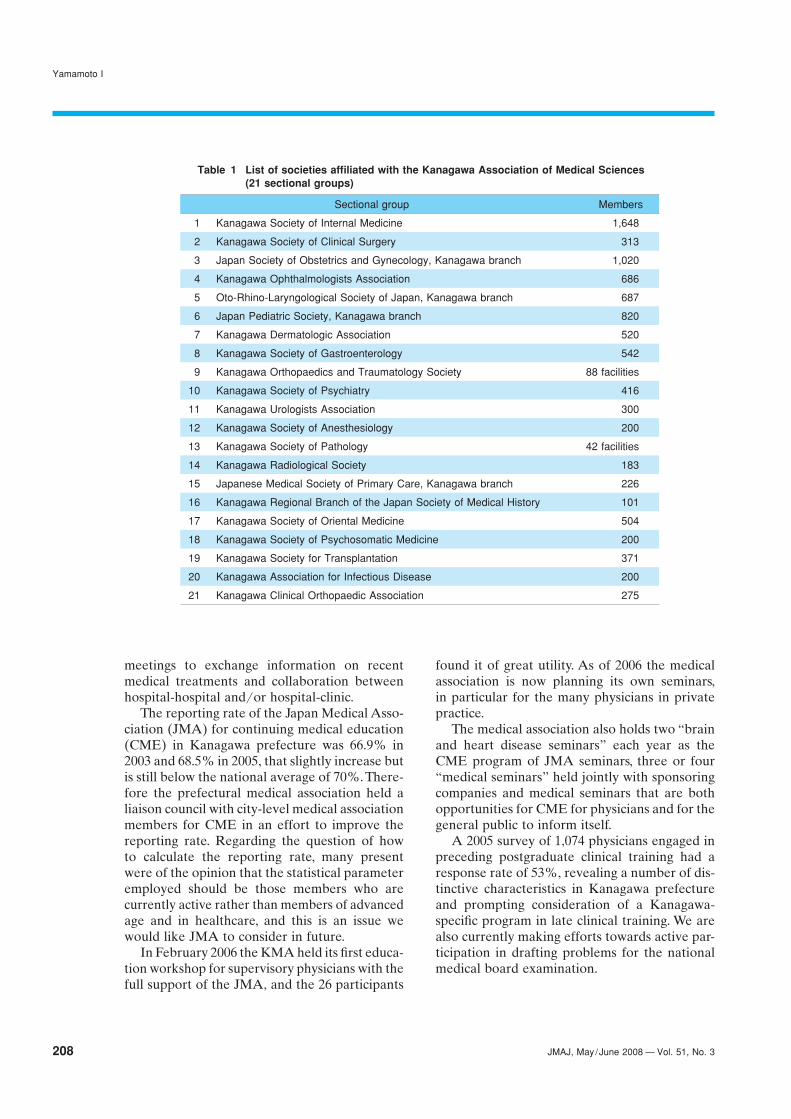
208 JMAJ, May/June 2008 — Vol. 51, No. 3
meetings to exchange information on recentmedical treatments and collaboration betweenhospital-hospital and/or hospital-clinic.
The reporting rate of the Japan Medical Asso-ciation (JMA) for continuing medical education(CME) in Kanagawa prefecture was 66.9% in2003 and 68.5% in 2005, that slightly increase butis still below the national average of 70%. There-fore the prefectural medical association held aliaison council with city-level medical associationmembers for CME in an effort to improve thereporting rate. Regarding the question of howto calculate the reporting rate, many presentwere of the opinion that the statistical parameteremployed should be those members who arecurrently active rather than members of advancedage and in healthcare, and this is an issue wewould like JMA to consider in future.
In February 2006 the KMA held its first educa-tion workshop for supervisory physicians with thefull support of the JMA, and the 26 participants
Yamamoto I
found it of great utility. As of 2006 the medicalassociation is now planning its own seminars,in particular for the many physicians in privatepractice.
The medical association also holds two “brainand heart disease seminars” each year as theCME program of JMA seminars, three or four“medical seminars” held jointly with sponsoringcompanies and medical seminars that are bothopportunities for CME for physicians and for thegeneral public to inform itself.
A 2005 survey of 1,074 physicians engaged inpreceding postgraduate clinical training had aresponse rate of 53%, revealing a number of dis-tinctive characteristics in Kanagawa prefectureand prompting consideration of a Kanagawa-specific program in late clinical training. We arealso currently making efforts towards active par-ticipation in drafting problems for the nationalmedical board examination.
Table 1 List of societies affiliated with the Kanagawa Association of Medical Sciences(21 sectional groups)
Sectional group Members
1 Kanagawa Society of Internal Medicine 1,648
2 Kanagawa Society of Clinical Surgery 313
3 Japan Society of Obstetrics and Gynecology, Kanagawa branch 1,020
4 Kanagawa Ophthalmologists Association 686
5 Oto-Rhino-Laryngological Society of Japan, Kanagawa branch 687
6 Japan Pediatric Society, Kanagawa branch 820
7 Kanagawa Dermatologic Association 520
8 Kanagawa Society of Gastroenterology 542
9 Kanagawa Orthopaedics and Traumatology Society 88 facilities
10 Kanagawa Society of Psychiatry 416
11 Kanagawa Urologists Association 300
12 Kanagawa Society of Anesthesiology 200
13 Kanagawa Society of Pathology 42 facilities
14 Kanagawa Radiological Society 183
15 Japanese Medical Society of Primary Care, Kanagawa branch 226
16 Kanagawa Regional Branch of the Japan Society of Medical History 101
17 Kanagawa Society of Oriental Medicine 504
18 Kanagawa Society of Psychosomatic Medicine 200
19 Kanagawa Society for Transplantation 371
20 Kanagawa Association for Infectious Disease 200
21 Kanagawa Clinical Orthopaedic Association 275

209JMAJ, May/June 2008 — Vol. 51, No. 3
Recent Activities of Hiroshima PrefecturalMedical Association
JMAJ 51(3): 209–211, 2008
Shizuteru USUI*1
Local Medical Associations in Japan
surveys as of adult diseases, pollution, healthadministration in agricultural communities, emer-gency healthcare and maternal and pediatrichealthcare, and it has also pursued research alongother lines in keeping with secular currents. In2004 the council engaged in research in suchwide-ranging fields as action on the shortage ofphysicians, the promotion of medical information,emergency healthcare, wide-area disaster medi-cine, palliative care, child-care support, abuse pre-vention, cancer screening quality control, mentalhealthcare, fitness and communicable diseasepolicies. Specifically, the four component groupsset up objective-specific committees, which pub-lished the results of their research in individualreports, with the ultimate objective of having theresults of their research reflected in governmentpolicy.
In addition to this prefecture-level council, wehave convened local study groups, 12 such during2006, as opportunities for healthcare, medical andwelfare service providers in Hiroshima prefectureto meet and exchange information in furtheranceof closer collaboration with local study groupsestablished on a local basis within the prefecture.
Hiroshima prefecture is a distinctly temperateregion bounded by the Chugoku mountain rangeto the north and the Seto Inland Sea to the south.Comprising coastal cities and depopulated inlandregions, the prefecture constitutes a microcosmof Japan.
The Hiroshima Prefectural Medical Associa-tion (HMA) has a membership of some 6,500(as of 1 Aug. 2007), of which 3,700 are staff phy-sicians at university hospitals, national publichospitals and private hospitals.
For reasons of space, this article addressesonly the following three of its primary activities.
Regional Healthcare Council ofHiroshima Prefecture
Since calls emerged in 1960 for the establishmentof regional healthcare study groups as the core ofregional healthcare promotion, the Japan MedicalAssociation and prefecture-level medical associa-tions throughout the country have advocated theorganization of these study groups.
The efforts of the HMA, in recognition oftheir philosophy and importance, on behalf ofpreparations for the establishment of a regionalgroup resulted in January 1969 in the establish-ment of the Regional Healthcare Council ofHiroshima Prefecture comprising the HiroshimaUniversity Medical Faculty, the Hiroshima Pre-fecture Medical Department and the HMA. In1995 the ordinance-designated city of Hiroshimajoined these three as the fourth component.
At the time of its inauguration, the councilengaged in analysis of cause-specific death sta-tistics and illness statistics and performed such
*1 President, Hiroshima Prefectural Medical Association, Hiroshima, Japan ([email protected]).This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.134, No.4, 2005,pages 644–645).
Tochigi
Hiroshima
Pop. 2.9mil.Area 8,500km2
Tokyo

210 JMAJ, May/June 2008 — Vol. 51, No. 3
Myocardial infarction forecastingWith the assistance of partners including theJapan Weather Association and the regionalhealthcare council, the HMA initiated myocar-dial infarction forecast services on 1 November2004.
In order to expand to all areas of the prefec-ture the myocardial infarction forecast servicesthat the Hiroshima City Medical Association hadbeen performing in the city and nearby areas, theSpecial Committee for Promotion of MyocardialInfarction Forecasting, established within thecouncil, conducted a survey of the relationshipbetween meteorological conditions and the inci-dence of myocardial infarction in three sectorswithin the prefecture (the Hiroshima area, theFukuyama area and the Bihoku area) and fore-cast their incidence there.
Based on their survey and analysis of the rela-tionship between meteorological conditions andemergency conveyances for myocardial infarctionover the past 3 years in these three sectors, theHMA website (http://www.hiroshima.med.or.jp/)is updated daily with predictions of myocardialinfarction forecasts for the two areas of northernHiroshima prefecture and southern Hiroshimaprefecture of Critical where the average atmo-spheric temperature is under 6°C, the averageatmospheric pressure under 1,013 hPa and a coldfront passed, of Caution where the average atmo-spheric temperature is under 6°C, the averageatmospheric pressure 1,013 hPa or over and ahigh-pressure front obtains, and of No Forecastotherwise.
The myocardial infarction forecast also ap-pears daily in the regional newspaper ChugokuShimbun, and we expect it to prove of use for thegeneral public in their daily lives and for medicalassociation members in diagnosing and counsel-ing emergency patients and outpatients.
Special HMA Committee on MedicalAccidents
The increase in recent years in medical accidentsand medical disputes is an issue that the medicalcommunity as a whole should be truly concernedabout, and Hiroshima prefecture is no exceptionin treating it as one of its most pressing tasks.
In February 1963 the HMA established itsSpecial Committee on Medical Accident Pro-cessing and in the more than 40 years since thenhas worked to achieve resolution in the medicalaccidents and disputes of its members. In 1997the committee was renamed the Special Com-mittee on Medical Accidents and now appliesitself not only to dispute resolution, but also toaccident prevention and medical safety. Thecommittee has a membership of 21, includingits chair, vice chairs, members and legal coun-sels. Five subcommittees organized along linesof medical specialization examine the specificsof incidents brought to their attention with theobjective of achieving fair and satisfactory dis-pute resolution based on medical judgment.
As a precaution against accidents involvingmedical association members, the committeemanages a million-yen (US$8,333)*2 insurancepolicy automatically subscribed by all membersand facility-contract and corporate insurancepolicies. It is most distinctive in the enduringspirit of mutual aid among the members since itsfoundation and its mutual benefit program ofcontributing up to 50 million yen (US$41,667)towards expenses paid out by members for pur-poses of dispute resolution. This assistance pro-gram is utilized effectively in a variety of casesand serves to mitigate the financial burden of themedical association’s members.
Currently some 1,200 cases of dispute havebeen reported since the establishment of thecommittee, and the medical association’s journalHiroshima Igaku published in its issue 5, volume57 (May 2004) an article titled “Summary of1,000 Medical Dispute Cases Handled” that sum-marizes 1,000 individual recent disputes. We hopethat closer analysis in future and feedback to thecommittee will help to prevent medical accidentsand medical disputes.
Japanese Physicians for the Preventionof Nuclear War
There is an organization called InternationalPhysicians for the Prevention of Nuclear War(IPPNW). A neutral, nonpartisan, global federa-tion of physicians organizations founded in 1980during the Cold War by a handful of heart diseasespecialists from the former Soviet Union and the
Usui S
*2 Based on a yen-dollar exchange rate of 1 dollar�120 yen.

211JMAJ, May/June 2008 — Vol. 51, No. 3
United States, IPPNW currently embraces amembership of some 100,000 physicians in 60countries. It was awarded the Nobel Peace Prizein 1985 in recognition of its efforts to spreadthroughout the world the message that nuclearweapons must not ever be used.
Since its establishment within the HMA in1982, Japanese Physicians for the Prevention ofNuclear War (JPPNW), the Japanese affiliate ofIPPNW, has worked closely as an organization ofmedical specialists with the other national affili-ates of IPPNW through the organization’s cen-tral office outside the American city of Bostontowards the total abolition of nuclear weapons.
IPPNW holds world congresses and regional
HIROSHIMA PREFECTURAL MEDICAL ASSOCIATION
conferences in alternating years, and in 1989Hiroshima hosted the 9th IPPNW World Con-gress. In August 2005, the 60th anniversary of theatomic bombing, the 5th IPPNW North AsiaRegional Conference was held in Hiroshima, andIPPNW members from throughout the worldattended along with those from Northeast Asia.
Contrary to people’s hopes, the risk of nuclearwar has grown since the end of the Cold War, andthe activities of IPPNW have never been morecrucial. Japan being the sole country to sufferatomic bombing, Hiroshima continues to speakwith a strong voice of the need for the total abo-lition of nuclear weapons.

212 JMAJ, May/June 2008 — Vol. 51, No. 3
International Medical Community
mony—not major health products.At the same time the BMA called for the
development of a comprehensive health caresystem that would be available to all and free atthe point of use. This was—as far as I know—thefirst major call for a national health service.
From those early beginnings a major part ofour work has been to promote high quality medi-cal care, and to raise the standards of medicalpractice. We are also very heavily involved in theHealth of the Public, and were major players inwork to get the UK to pass smoke free publicplaces legislation. Other current lobbying is ondiet and exercise, further tobacco control law andguidance, dealing with the alcohol abuse seen inour streets and weapons control—an area we firstworked on in 1897. Our Board of Science carriesout the research and publishes scientific reportsthat help us in our work as health lobbyists. Areport on what doctors can do to combat climatechange will be published on 3 April; amongstother things it advises on how the National HealthService could become carbon neutral or at leastless of a part of the problem.
The Professional Activities Directorate includesthe Board of Science and Education, Ethics,Conferencing, Medical Education, the Library,International Affairs and a Doctors Health Depart-ment. Although not part of our trades uniondirectorate there is close co-operation. After all,if doctors are forced to work excessive hoursthere are risks not only to their health and wel-fare but to patient safety. Ensuring that ourpolicy arenas understand the work each other aredoing is a challenge when we are active in somany areas. Our members see the benefits of thecomplex activity.
The BMA is currently celebrating our 175th anni-versary. We are a complex organisation—a tradeunion without a political fund (and thereforewithout party political alleigance), a professionalassociation, a company limited by guarantee anda medical publisher.
Although the BMA does not have a modernmission statement we do have a set of guidingprinciples. Our first article of Association reads:“To promote medicine and the allied sciences, tomaintain the honour and interests of the medicalprofession and to promote the achievement ofhigh quality health care.” That means in today’scomplex health environment that we work toimprove the health of the public, and the healthcare experience of those who become patients aswell as the working conditions of doctors and thequality of care they are able to offer.
We were established at a time when largenumbers of medical practitioners had no qualifi-cations, not even having completed the appren-ticeship route to becoming a doctor. It makessense then that one of the BMA’s first actions wasto compile a report on the dangers these quacksposed to patients, which led in a few years to theestablishment of the General Medical Councilwhich maintains the register of qualified doctorsin the UK.
At the end of the 19th century we exposed thepatent medicine trade—the poor had little accessto health professionals and were spending moneyon potions and lotions advertised in the news-papers. The BMA report Secret Remedies set outchemical analyses of these products as well as thetrue cost of manufacture. The profit margins wereenormous; most contained active ingredients butthey were substances such as arsenic and anti-
*1 Director of Professional Activities, British Medical Association, London, UK ([email protected]).
Promoting Medicine, Supporting Doctors:The BMA in action
JMAJ 51(3): 212–214, 2008
Vivienne NATHANSON*1

213JMAJ, May/June 2008 — Vol. 51, No. 3
Trades unionism is currently unpopular withmany key stakeholders, including many electedpoliticians. The fact that the BMA is so muchmore than a trade union makes it difficult forgovernment and the media to ignore us. At timeswhen our trade union actions, defending therights of our members, or successfully negotiatingnew contracts for doctors, make us unpopular withgovernment, this complexity makes it impossiblefor them to refuse to include us in discussionson matters which affect our members and ourmembers’ patients.
The media profile of the BMA shows the com-plexity of the organisation. The public see us asadvocates for health and for better health care.While advocacy against tobacco or alcohol leavesus open to accusations of being the “health Nazis”(an especially unpleasant phrase used in someelements of the right wing press), most recognisethat this is about protecting the vulnerable.The expertise of our public affairs departmentin ensuring that these complex and sometimesunpopular messages get to the public via themedia, is immense. The challenge for the futurewill be satisfying all the new media outlets as wellas the traditional ones.
A mainstay of our activity is the work we do inour ethics department. The department is notmeant to be academic, but to prepare adviceand guidance for our members. The fact, as oneProfessor of Philosophy and past chair of theInternational Association of Bioethics said, thatthe advice and guidance is academically excellentis a bonus for our members rather than a purposeor end in itself.
The BMA has had an ethics committee formany decades; the format of the committee haschanged many times. Currently there are 10medical practitioner members who are electedby our annual meeting and by our Council. Tothese we add 8 more members who bring otherexpertise including academic philosophy, medi-cal law and secular and religious ethicists. Theethics staff has a wide variety of backgrounds andsome have Masters degrees in medical law andethics. They are not only the major contributorsof written material but also take part in the vigor-ous debates in committee.
So what exactly does our ethics departmentdo?
First and foremost we provide advice to mem-bers. We have guidance notes on common issues
on the BMA website—these pages currentlyenjoy over 14,000 hits a month. They are designedto help members find answers to their questions.As with all the publications we produce they area complex mix of law and ethics. As we developevery new piece of advice we look at our domes-tic law and see what relevance both statute andcase law have to the matter at hand. As the UKgradually devolves many decisions to the devolvedgovernments of Scotland, Wales and NorthernIreland the complexity of analysing those lawsincreases.
Several years ago we were asked to produce abrief textbook of medical ethics. It grew, becausethe amount of legal analysis needed had grownso much to around 800 pages. Since we printed it(Medical Ethics Today, published by BMJ Pub-lishing Group) we have committed to provideregular on-line updates setting out the relevanceof key legislative and case law changes.
We also deal with several thousand directqueries every month—some are readily helpedby guidelines or extracts from the text book.Many of the callers need to discuss the clinicalmatter with an adviser, and to talk through thefactors they should take into account in resolvingthe problem. We rarely tell a doctor what theanswer to his/her query is. We prefer to leadthem through the questions they should ask, theanalysis they should make and the route to theirsolution. Each discussion therefore helps to edu-cate the doctor and to help him/her in the future.
Why should doctors contact us? Why shouldthey buy our book when there are many dozensof alternatives available? The simple answer isthat as well as academic excellence we are prac-tical. We know doctors. We write advice thatunderstands the clinical situations in which doc-tors face these dilemmas so that the solutionsmake clinical sense are not academic absurdities.
One example of the practicality is the produc-tion of toolkits to help newly qualified doctorsdeal with getting consent in real clinical situa-tions. This is sent to all new graduates in medicinein the UK and will be joined this year by a toolkiton confidentiality and soon after by a toolkit onthe working of the Mental Capacity Act. Thesethree include sets of pocket sized cards thatdescribe common clinical situations and how toassess the best course of action. We know they areneeded as they cover areas of common enquiries.We know they work as we have field tested them
PROMOTING MEDICINE, SUPPORTING DOCTORS: THE BMA IN ACTION

214 JMAJ, May/June 2008 — Vol. 51, No. 3
with medical students and young doctors. And weknow they are a very real and tangible benefit ofbeing a BMA member.
From time to time the ethics department iden-tifies a specific area on which more extendedguidance is needed. This has included a bookexplaining law, ethics and practice on Withdraw-ing and withholding medical treatment, now inits third edition and a forthcoming report onethical issues relating to care of elderly patients.These books are written by departmental staffand commented on, and amended by the ethicscommittee.
Another area of work is advocacy about legis-lation or public policy. As an example the govern-ment initiated a new piece of primary legislationseveral years ago in response to the Shipman andAlder Hey scandals. The Human Tissue Bill wasdesigned to ensure that never again would tissuebe taken from deceased patients and stored fordecades without reference. The key componentwas to give patients the right to decide on thestorage and use of tissue, including ensuringparents made these decisions for their youngchildren. The problem was that some of thehurdles built into the legislation made the practi-calities of practising medicine impossible. TheBMA ethics team got together people affectedby the potential legislation, including the RoyalCollege of Pathologists and the medical researchcommunity and worked out what we all wantedin the form of change and which elements weretolerable if undesirable. We then co-ordinatedmedical input to those officials writing andrewriting the Bill as it progressed through Par-liament. While the final outcome—the HumanTissue Act is not perfect, it is acceptable. And—importantly—it meets the large majority of thepublic concerns that led to its development.
Another current area of work is on organtransplantation. The BMA has worked for overa decade with charities, medical organisations,patients groups and others to increase publicunderstanding of organ transplantation, and toincrease the number of people who put theirnames on the voluntary donor register. For someyears we have also called for a system of pre-sumed consent—that is every person having the
opportunity to put their names on a register ofthose not willing to donate organs after theirdeath. This would then mean that the state coulduse your organs if you had not indicated yourrefusal. There are, of course, a lot of caveats to theprocess and we would require many protectionsto be built into the system. But this is our policy.And our Patient Liaison Committee agrees withthe policy. Despite a lack of real public educationwe have had increasing public acceptance of theconcept—now at a level of 64%. And willingnessto be a donor is seen in up to 90% of the UKpopulation.
A recent government taskforce has just advo-cated major system changes in the organisationof transplant services; we have welcomed theirreport. And we are delighted that the same task-force is now considering the opt-out or presumedconsent matter. Giving evidence in Parliamenton the length and depth of our involvement wasenormously positive. The doctors’ organisationis seen as key to; informing the public, helpingdesign a system which allows the wishes of theindividual to be respected, increasing the avail-ability of organs for transplant so that people donot die on the donor waiting list and to dealingwith the mismatch in certain minority populationgroups between donation and recipient levels.
While organ donation remains a controversialissue in some arenas this is not the case in the UK.Controversy only exists around the relative impor-tance of different legal and practical changes.
These are just a very few examples of the chal-lenges we face. We spend a significant amount oftime trying to predict the challenges for next yearand thereafter to provide advice. One of myproudest moments was predicting that fetal tis-sue transplantation to patients with advancedParkinson’s Disease was likely to become an issueand to have completed the process of writing andadopting guidelines on this experimental tech-nique before the first case studies were reported.That helped our members understand the limits.And more importantly it helped patients to seethat medical science does not proceed uncon-strained, but that rules are in place to protectthem and the society in which they live.
Nathanson V

215JMAJ, May/June 2008 — Vol. 51, No. 3
Essay
main theme for the scientific session held in con-junction with the Tokyo General Assembly, andpreparations for the meeting proceeded steadily,with approaches made to leading healthcareeconomists both in Japan and overseas at anextremely early stage. At the same time, theWMA Committee and Council submitted threeimportant resolutions that all remain today foradoption at the Tokyo General Assembly: aresolution concerning broad revisions to the1964 Declaration of Helsinki (DoH); a reso-lution concerning the prohibition of torture;and a statement on the use and misuse of psycho-tropic drugs.
Before this, however, in 1972 the AmericanMedical Association (AMA) withdrew fromthe WMA. The reason for this was that that anincreasing number of national medical associa-tions belonging to the WMA had been allowinggovernment officials to represent them withinthe WMA, resulting in a bias towards WHOactivities. At the WMA General Assembly inMunich in 1973, Dr. Wynen was elected as Chairof Council. In the same year, Dr. A.Z. Romualdezof the Philippines, who had had a close relation-ship with the AMA, resigned from his long-heldpost as WMA Secretary-General and was suc-ceeded by Sir William Refshauge, who was Direc-tor-General of Health of the commonwealth ofAustralia and a former chairperson of the WHO.
The 1974 General Assembly held in Stockholm,was presided over by Sir W. Refshauge, butbecause a resolution tailored to the wishes of theWHO were submitted, the Japanese delegationheaded by Dr. Takemi (who opposed the resolu-
Dr. Andre Wynen, Secretary General Emeritusof the World Medical Association (WMA),passed away on June 10, 2007. Belated as theyare, here I would like to respectfully express myheartfelt condolences.
According to Volume 53 of the World MedicalJournal (WMJ), Dr. Wynen was born on Decem-ber 8, 1923, in Brussels, Belgium, and joinedthe Belgian Army at age 16 during the SecondWorld War. Following the German occupation,he attempted to escape to Africa but failed, even-tually joining the Resistance Movement. In 1942,he passed his first examination at the then-illegalmedical faculty in Namur, but was soon afterarrested and imprisoned at the Breendonk con-centration camp, then later transferred to theBuchenwald concentration camp on the outskirtsof Weimar. Here he was exposed to typhus inbiological experiments but survived and nursedmany of the other victims. In 1945 he returned toBelgium after liberation by Allied forces, but wasfound to have contracted tuberculosis and wastreated in Switzerland. Following his recovery, in1947 he was finally able to resume his medicalstudies, qualifying in 1950.1
At the WMA Council Meeting held in Tokyoin May 1971, it was decided to hold the 1975General Assembly in Tokyo, and the 1976 Gen-eral Assembly in the United States, which wouldbe celebrating its bicentennial in that year. At theGeneral Assembly held in autumn 1974, Dr. TaroTakemi, President of the Japan Medical Associa-tion (JMA), was elected as the President-elect ofthe WMA. Dr. Takemi chose “Development andAllocation of Medical Care Resources” as the
*1 JMAJ Advisory Member, Legal Advisor, Japan Medical Association, Tokyo, Japan ([email protected]).
Eulogy for Dr. André WynenThe man who rescued the WMA fromthe threat of collapse and establishedthe basis for the Declaration of Helsinki
JMAJ 51(3): 215–217, 2008
Tatsuo KUROYANAGI*1
Dr. André Wynen in Tokyo, 2000
216 JMAJ, May/June 2008 — Vol. 51, No. 3
tion) caused an incident when they walked out ofthe assembly in protest.2 Incidentally, at the endof 1970 the JMA under the presidency of Dr.Takemi requested that the Japanese Governmentsignificantly raise medical fee, while at the sametime requesting revision of the Medical Insur-ance Law (a request that was rejected). Con-sequently, following meticulous preparations, itwas decided that from July 1, 1971 all JMA mem-bers would resign as health insurance doctors,and procedures to implement the strike (limitedto health insurance treatment) began. After 1month without health insurance doctors, all thedoctors involved returned to providing healthservices. Following the mass resignation of thehealth insurance doctors, Japan’s largest laborunion, the General Council of Trade Unions ofJapan (Executive), filed a lawsuit with the TokyoDistrict Court against the JMA officers, claimingthat the mass resignation was illegal. The authoracted as representative of the defendant in thiscase, in which the court ruled in favor of the JMAwon in May 1973.
At the Council Meeting held in Paris in May1975, the host of the Tokyo General Assemblyand WMA President-elect, Dr. Takemi, pre-sented the following report, asking the followingquestions: The autumn WMA General Assemblyis to be held in Tokyo, but despite our efforts, theJapanese Government is not expected to issuevisas to the South African delegation in keepingwith the UN Resolution to this effect. Shouldwe cancel the General Assembly altogether?Or should we hold it at another venue? Wehave already spent quite a large amount onpreparations for the Tokyo General Assembly.2
The JMA’s interpretation may be incorrect, butunder the WMA Constitution, when a memberfrom a certain country cannot attend a GeneralAssembly due to international conflict or otherunavoidable reasons, the General Assembly mustbe cancelled and restaged at a venue where allmembers can attend. These regulations wouldseem to apply to the holding of the Tokyo Gen-eral Assembly.
In response, on the condition that the WMASecretary-General discussed with United Nationsofficials, it was decided unanimously by Councilto hold the Tokyo General Assembly as planned.However, the WMA Secretary-General took noaction and aimless days passed with the issueof the South African delegation gaining entrance
Kuroyanagi T
to Japan remaining unsolved. There was a realdanger that the Tokyo General Assembly couldnot be held if the situation were to continueunchanged.
Meanwhile, those involved in preparing adraft revision of one of the WMA’s most impor-tant declarations, the DoH, were encounteringincredible difficult due to the extensiveness ofthe changes to be made to the original 1964Declaration. The drafters of the Declaration of1975, chosen from three northern Europeancountries, were Clarence Blomquist (Sweden),Erik Enger (Norway), and Povl Riis (Denmark).There was extremely strong opposition to thedraft revision, particularly from the Europeanpharmaceutical industry. In fact, the chairpersonof the Bundesverbandes der PharmazeutischenIndustrie, Hans-Otto Scholl, sent a bizarre letterto the JMA dated August 28, 1975, requestingthat the JMA oppose the revisions to the DoH,alleging they were the isolated work of Scandina-vian medical groups, and stating that ProfessorSewering of the German Medical Association andcolleagues intended to vote against the revisions.
However, WMA President-elect Taro Takemiactively supported the expansion of the DoH’sscope to include biomedical as well as medicalissues; he made meticulous preparations for therevisions, appointing as a key member of theJapanese Preparation Committee Dr. TatsujiNomura, the founder and Director of the CentralInstitute for Experimental Animals, and senthim as Japan’s representative to internationalmeetings. Moreover, on June 27, 1975, the JMAhad already responded to the WMA Secretary-General, stating that Japan basically supportedthe draft revision, while expressing the opinionthat standards concerning the term “biomedical”and animal testing were in need of clarification.
One month prior to the Tokyo General Assem-bly, the WMA received a telegram from Japan,and Chair of Council Wynen and Dr. Takemi hada discussion. Dr. Takemi said, “I did my best. Ispared no effort, but there was no getting thevisas. It was impossible to secure them. What isyour decision?” The Secretary-General opposedholding the Tokyo Assembly, but as Chair ofCouncil, Dr. Wynen advocated the holding of theAssembly and began to think of a compromiseplan. He said, “As Chair of Council, and as apracticing surgeon and doctor in Belgium, Ipulled out a whole week of pages from my diary

217JMAJ, May/June 2008 — Vol. 51, No. 3
EULOGY FOR DR. A. WYNEN
and bought a round-the-world ticket (Brussels-Tokyo-Sao Paulo-Geneva) as a salesman for aproposal, the intention of which was to save theTokyo Assembly.”
Incidentally, Dr. Wynen’s proposal was to“hold the Tokyo General Assembly as planned,on the condition that any of the items discussedand voted on in Tokyo could be taken up again,and if necessary re-voted on that the followingAssembly, which the South African delegationwould be able to attend.” Prior to departing forJapan, Dr. Wynen held discussions with SouthAfrica and Brazil to obtain their agreement tothe proposal in advance.2 He paints a vividpicture of the scene at the discussions in Tokyo inhis “Recollections on WMA’s 50th Anniversary,”published in Vol. 43 of the WMJ. Of course, Dr.Takemi accepted this proposal.
It is said that in history there are no “ifs,” butwithout the dedicated efforts of Dr. Wynen, it ishighly likely that the JMA would have followedthe path of the AMA and withdrawn from theWMA. As described above, Dr. Takemi hadseveral years previously led the JMA to victory ina confrontation with the Japanese Governmentwith the mass resignation of health insurancedoctors. Under the circumstances, what do yousuppose happened not only to the WMA, butalso the DoH revisions? Even now, I shudderat the thought of it. However, the Tokyo GeneralAssembly was successfully held 1 month later.Not only this, Dr. Takemi invited several econo-mists from the United States and other countriesas well as AMA representatives to the scientificsession held in conjunction with the GeneralAssembly, steadily paving the way for the AMAto rejoin the WMA. Speaking of the DoH,according to the official minutes of the TokyoAssembly, there was apparently quite some debateover the terms “medical” and “biomedical,” andat the suggestion of the Canadian Medical Asso-ciation, a compromise draft adding “involvinghuman subjects” to “biomedical research” wasdrawn up. The minutes show that Professor
Sewering, President of the German MedicalAssociation, and his colleagues actively praisedthe revision proposal.3,4 Furthermore, Japanhired a charter airplane to send its delegationof more than 100 to the 1976 General Assemblyin Brazil.
Dr. Wynen saved not only the Tokyo Assem-bly, but also the very existence of the WMA, as aresult of which the DoH and various other WMAdeclarations and statements were also saved.
I had the honor of meeting Dr. Wynen some-time after 1993. There are two instances in par-ticular that I will never forget. One is the scene atthe time of the associate members meeting forthe Somerset West, South Africa General Assem-bly, when Dr. Wynen made a logical statement insupport of the JMA. The other is the scene at the2004 Tokyo General Assembly when Dr. Wynen,accompanied by his wife and wearing the necktiehe had been presented by the JMA many yearspreviously, spoke of his memories of his relation-ship with Dr. Takemi and the JMA. In Japanthere is an expression “Fusho Fuzui (A wifeshould do her husband’s bidding),” and I wasreminded of this whenever I saw Dr. Wynen andhis wife together.
Dr. Wynen! Your successors in the WMA ineach of their countries are all striving to helptheir patients as best they can. Please watch overour efforts so we don’t make mistakes.
Reference
1. Dr. André Wynen 1924–2007. WMJ. 2007;53:30–31.2. Wynen A. Recollections on WMA’s 50th Anniversary. WMJ.
1997;43:49–53.
3. Official Summary Minutes of XXIXth World Medical Assembly;1975 Oct; Tokyo, Japan.
4. JMA Newsletter. 1975 Oct 20. (in Japanese)

218 JMAJ, May/June 2008 — Vol. 51, No. 3
of increasing violence at healthcare facilities fromso-called “monster” patients.
Paradoxically, in some cases these patients areventing their strong dissatisfaction towards unfa-vorable results on their healthcare staff, eitherdirectly with violence or indirectly by legal means,despite the quality of health services rising toachieve marked improvements in mortality andmorbidity rates. Thus, there seem to exist seriousand fundamental discrepancies between health-care quality and patient satisfaction levels.
The discussions and communications held inthe peaceful Chateau De Divonne surroundedby lilac and horse chestnuts in full bloom werevery useful for identifying and understandingsuch relevant issues. Following the meeting, wetraveled on to Geneva to join the World HealthProfessions Conference on Regulation (WHPCR)meeting on our way back to Japan.
The next general assembly of the WMA willbe held in Seoul, Republic of Korea, this October.We have observed significant development in theROK’s universal health insurance system sup-ported by information technology. I look forwardto attending the next assembly in Seoul, one ofthe major Asian cities, and communicating withparticipants from all over the world.
Masami ISHII, Executive Board Member, Japan Medical Association( [email protected]), Secretary General, Confederation ofMedical Associations in Asia and Oceania (CMAAO), CouncilMember, World Medical Association.
WMA Council Meeting in Divonne-les-BainA WMA council meeting was held in Divonne-les-Bains, a small French town near Geneva. Itwas an active meeting with an increased numberof council members and other participants. Atthe beginning of the session, I had the opportu-nity to express my deep concern and sympathy tothe victims of the Myanmar cyclone and Chinaearthquake disasters as the Secretary Generalof CMAAO (Confederation of Medical Associa-tions in Asia and Oceania), sentiments that wereshared by all the participants of the meeting.
There were several important topics discussed,including the Declaration of Helsinki (DoH) andother various issues in specific areas. It seems arecent trend to discuss issues about global healthin relation to global climate change and otherenvironmental and energy issues.
Migration issues are becoming increasinglyimportant from the global perspective because itharms the sustainability of health services andcauses inequality in the level of health resourceswithin community health in terms of both qualityand quantity. In this way, the breakdown of socialsecurity systems, including health support, willcause further migrations of people, triggeringfurther social imbalances. Such social insecuritymay be largely solved by adopting a policy ofuniversal health insurance.
On the one hand, new issues concerninghealth personnel safety are now arising because
From the Editor’s Desk
Participants in the 179thWMA Council Meetingin Divonne-Les-Bains,2008Picture by kind permissionof Dr. Peteris Apinis,Editor-in-Chief of the WorldMedical Journal.