ISHA CONVENTION 2016 LEARNING OUTCOMES … Group revised.pdf · Must Balance Risks with Chances ......
20
4/20/2016 1 ISHA CONVENTION 2016 MANAGEMENT OF SWALLOWING AND VOICE IN HEAD AND NECK CANCER PATIENTS: CLINICAL GRAND ROUNDS Dawn Wetzel, MAT, CCC-SLP, Associate Clinical Professor, Purdue University Jaime Bauer Malandraki, MS, CCC-SLP, Clinical Instructor, Purdue University Rebecca Risser, MAT, MM, CCC-SLP, Voice Clinic of Indiana Noah Parker, MD, Laryngologist, Voice Clinic of Indiana Stacey Halum, MD, Laryngologist, Voice Clinic of Indiana Barbara Solomon, MA, CCC-SLP, Clinical Professor, Purdue University, Moderator 1 LEARNING OUTCOMES At the conclusion of this presentation, participants will be able to: 1) Identify the swallowing, voice, and oral-motor problems head and neck cancer patients experience while undergoing chemoradiation. 2) Be familiar with preventative exercises for the head and neck cancer patient. 3) Problem-solve solutions for the successful assessment and treatment of the head and neck cancer patient. 2 Swallowing Therapy for Head and Neck Cancer Patients, Therapy improves function during, after cancer treatment. OncoLog, February 2016, Volume 61, Issue 2 – Dr. Kate Hutcheson - The University of Texas MD Anderson Cancer Center. In patients with head and neck cancer, loss of swallowing function may result from radiation therapy, surgery, or the cancer itself and lead to poor health and reduced quality of life. “A large body of evidence suggests that preventive swallowing therapy is the best practice for patients who are going to receive radiation therapy to the head and neck,” Dr. Hutcheson said. “We know that patients who keep their swallowing system engaged during the course of their radiation therapy have a better chance of recovering meaningful swallowing ability after their therapy. USE IT OR LOSE IT! “Swallowing is a huge quality of life issue. The key to improving swallowing function is early and individualized therapy, A dysphagia-specialized speech pathologist—whether seen at MD Anderson or elsewhere—can help maximize a patient’s outcome.” 3 MANAGEMENT OF SWALLOWING AND VOICE IN HEAD AND NECK CANCER PATIENTS Clinical Grand Rounds Noah Parker, MD, Laryngologist, Voice Clinic of Indiana Dawn Wetzel, MAT, CCC-SLP, Clinical Associate Professor, Purdue University Parker & Wetzel, ISHA 2016 4
Transcript of ISHA CONVENTION 2016 LEARNING OUTCOMES … Group revised.pdf · Must Balance Risks with Chances ......

4/20/2016
1
ISHA CONVENTION 2016
MANAGEMENT OF SWALLOWING AND VOICE IN
HEAD AND NECK CANCER PATIENTS:
CLINICAL GRAND ROUNDS
Dawn Wetzel, MAT, CCC-SLP, Associate Clinical Professor, Purdue University
Jaime Bauer Malandraki, MS, CCC-SLP, Clinical Instructor, Purdue University
Rebecca Risser, MAT, MM, CCC-SLP, Voice Clinic of IndianaNoah Parker, MD, Laryngologist, Voice Clinic of Indiana
Stacey Halum, MD, Laryngologist, Voice Clinic of IndianaBarbara Solomon, MA, CCC-SLP, Clinical Professor, Purdue University, Moderator
1
LEARNING OUTCOMES
At the conclusion of this presentation,
participants will be able to:
1) Identify the swallowing, voice, and oral-motor
problems head and neck cancer patients
experience while undergoing
chemoradiation.
2) Be familiar with preventative exercises for the
head and neck cancer patient.
3) Problem-solve solutions for the successful
assessment and treatment of the
head and neck cancer patient.
2
Swallowing Therapy for Head and Neck Cancer Patients, Therapy improves function during,
after cancer treatment. OncoLog, February 2016, Volume 61, Issue 2 – Dr. Kate Hutcheson -
The University of Texas MD Anderson Cancer Center.
In patients with head and neck cancer, loss of swallowing function may result
from radiation therapy, surgery, or the cancer itself and lead to poor health and reduced
quality of life.
“A large body of evidence suggests that preventive swallowing therapy is the
best practice for patients who are going to receive radiation therapy to the head and
neck,” Dr. Hutcheson said.
“We know that patients who keep their swallowing system engaged during
the course of their radiation therapy have a better chance of recovering meaningful
swallowing ability after their therapy.
USE IT OR LOSE IT!
“Swallowing is a huge quality of life issue. The key to improving swallowing
function is early and individualized therapy, A dysphagia-specialized speech
pathologist—whether seen at MD Anderson or elsewhere—can help maximize a patient’s
outcome.”
3
MANAGEMENT OF SWALLOWING
AND VOICE IN HEAD AND NECK
CANCER PATIENTS
Clinical Grand RoundsNoah Parker, MD, Laryngologist,
Voice Clinic of Indiana
Dawn Wetzel, MAT, CCC-SLP,
Clinical Associate Professor,
Purdue University
Parker & Wetzel, ISHA 2016 4

4/20/2016
2
Disclosure
• Financial:
– I receive a salary from Purdue University.
– I occasionally provide prn services for IU Health
Arnett Hospital for which I am compensated.
– I will receive an honorarium for this presentation.
• Non-Financial:
– None
Parker & Wetzel, ISHA 2016 5
Patient History
• 65 year old happily married musician
• Played trumpet professionally with numerous
big bands and musicians
• Recorded CDs
• Provided private instruction
Parker & Wetzel, ISHA 2016 6
Patient History
• Diagnosed with right tonsillar cancer in 2001
• Underwent surgical resection and
chemoradiation at University of Chicago Hospital
• At the time of treatment experienced significant
mucositis and edema
• Used PEG tube for 7 months
• Participated in therapy
• VFSS swallow sufficient. PEG removed.
Parker & Wetzel, ISHA 2016 7
Impact of Cancer Treatment
• Surgical
– Sensory
– Base of tongue involvement?
– Palate involvement?
– Lymph nodes?
– Pharyngeal constrictor involvement?
Parker & Wetzel, ISHA 2016 8
4/20/2016
3
Impact of Cancer Treatment
• Acute Radiation Changes
– Xerostomia
– Edema
– Mucositis
Parker & Wetzel, ISHA 2016 9
Impact of Cancer Treatment
• Progressive Radiation Changes
– Decreased salivary flow
– Taste reduction
– Muscle change
• Fibrosis
• Sclerosis
• Muscle edema
• Atrophy/Disuse
Parker & Wetzel, ISHA 2016 10
First Presented To Us
• Increasing symptoms of dysphagia 2010
• VFSS revealed moderate-severe dysphagia with
reduced tongue base retraction, epiglottic inversion,
laryngeal elevation/anterior hyoid movement, and
vestibular closure, and decreased sensation.
• Aspiration of liquids and puree
• Significant pharyngeal residue
• Outcome: Wished to continue to eat unrestricted
diet.
• Continued therapy in his hometown
Parker & Wetzel, ISHA 2016 11
Initial Complications 2013
• Hospitalized with pneumonia in December
2013
– Repeat VFSS- Similar findings
– Aspiration of thin liquids. Severe pharyngeal
residue.
– Patient’s wishes: Continue to eat unrestricted diet
– Strategies: Limit bolus size, cough re-swallow, right
head turn
– Swallowing therapy as an inpatient
Parker & Wetzel, ISHA 2016 12
4/20/2016
4
VIDEO
Parker & Wetzel, ISHA 2016 13
Swallowing Strategies
• Super supraglottic swallow
• Modified Mendelsohn
• Second swallow
• Purposeful cough
• Safe sip and bite size
Parker & Wetzel, ISHA 2016 14
Rehabilitative Exercises
• Gargle/Tongue Pull Back
• Masako
• Mendelsohn
• Super Supraglottic Swallow
• Effortful Swallow
• Shaker
• Chin Tuck Against Resistance
Parker & Wetzel, ISHA 201615
Treatment( Adapted from Burkhead, ASHA, 2013)
Direct exercise
• Mendelsohn
• Effortful swallow
• Tongue hold swallow
(Masako)
• Skill specific
Indirect exercise
• Shaker
• EMST
• Lingual strengthening
• Strength training
Parker & Wetzel, ISHA 2016 16
4/20/2016
5
Mendelsohn Maneuver
• Can be used as strengthening/ROM or as a maneuver
• Load= holding larynx in elevated position against resistance
• Using with bolus may increase salience, load
• Increased activation of submental muscles
• Increased vertical-anterior duration & extent of hyoid & laryngeal movement
• Increased A-P diameter and duration of UES opening
• Improved coordination
• Improved timing
• Increased pressure/BOT-PPW
Parker & Wetzel, ISHA 2016 17
Effortful Swallow
• Impacts submental muscle activation
• May consequently affect airway protection and UES activation earlier onset/longer duration /extent motion
• Increased generation of oral pressure-dependent upon instruction
• Increased pharyngeal pressure BOT/PPW with longer duration and UES relaxation
• Potential for increase load/resistance by increasing bolus viscosity
• Task-oriented form of skill training with a strength component from greater muscular activation
Parker & Wetzel, ISHA 2016 18
Masako/Tongue Hold
• Designed to improve swallow physiology in individuals demonstrating decreased bolus clearance in upper pharynx due to decreased tongue base retraction or upper pharyngeal constrictor anterior ward motion
• Created in response to observation of increased anterior bulging of posterior pharyngeal wall after oral resection-passive load
• Conflicting findings: pharyngeal pressure –H/N pharyngeal pressures - nls
Parker & Wetzel, ISHA 201619
Shaker
• Incorporates passive resistance
• Isometric and isokinetic contractions
• Strap muscles of the neck and suprahyoid
musculature
• Increased laryngeal anterior excursion and
cross sectional opening of the UES
• Improved swallowing function noted with
decreased post-swallow aspiration
Parker & Wetzel, ISHA 2016 20
4/20/2016
6
Chin Tuck Against Resistance(Yoon et al )
• Used for patients with dysphagia due to upper esophageal sphincter dysfunction
• Participants found the sitting position of CTAR to be less strenuous
• Greater maximum sEMG values were noted during the CTAR isokinetic and isometric exercises than during the equivalent Shaker exercises
• CTAR isometric exercise showed significantly greater sEMG values than the Shaker isometric exercise.
• Additional research needed
Parker & Wetzel, ISHA 2016 21
Increasing Difficulty
• Within next year two bouts of pneumonia for which
he was not hospitalized
• Hospitalized with PNA for 16 days in December
2014.
• PEG tube placed through IR
• NPO
• Tried both Jevity and Ensure. Adverse side effects
and 20-lb weight loss.
• Real Food Blends (tube feeding product) plus
fortified protein mixtures stabilized weight.
Parker & Wetzel, ISHA 2016 22
Another VFSS…………
• Presented for a repeat video swallow study
with goal of removing tube
• Severe pharyngeal dysphagia with reduced
tongue base retraction, anterior hyoid
movement, and pharyngeal stripping, absent
epiglottic inversion, and limited
cricopharyngeal opening
Parker & Wetzel, ISHA 2016 23
Referral to Laryngology 3/15
• Quite indurated soft tissues of the neck on exam with suggestion of velopharyngeal escape on phonation
• Pharyngeal, laryngeal, and cricopharyngeal findings on MBSS
• What can the surgeon add in this case to augment therapy?
• What is the risk/benefit profile?
Parker & Wetzel, ISHA 2016 24

4/20/2016
7
Improving Pharyngo-Esophageal
Bolus Movement – When Glottally
Competent
VelopharyngealClosure
CricopharyngealOpening
Laryngeal Elevation
& Protraction
Must Balance Risks with Chances of
Improvement
Less Morbid/Minimally Invasive
Procedures?Parker & Wetzel, ISHA 2016 25
Addressing Deficits Procedurally
• Due to findings of poor cricopharyngeal opening and subjective VPI, discussion of an intervention was made
– Cervical esophageal balloon dilation
– Botulinum toxin injection into cricopharyngeus to allow for several months of muscular weakness
– Posterior pharyngeal wall injection augmentation to improve VP closure – Resorbable gel
Parker & Wetzel, ISHA 2016 26
Post-Surgical Course-Swallowing
• Noted less resistance to swallowing following his procedure
• Referred back to speech pathology immediately to continue therapy
• VFSS results similar
• Considering additional treatments
– I EaT Clinic
– Swallow Strong
• Oral Care:
– 2x/day prescription fluoride toothpaste
– Brush
– Floss
– Fluoride treatments
– Coconut oil: pulling
Parker & Wetzel, ISHA 2016 27
Post-Surgical Course-Swallowing
• Advanced from thin liquids to soft solids
• Initially incorporated SSG
• Gradually increased to 1-2 meals per day
• No longer needed O2 when walking
• Questionable episode of URI/PNA
• Treated/released in ED
• He was happy with his swallowing
Parker & Wetzel, ISHA 2016 28
4/20/2016
8
Post-Surgical Course-VPI with Trumpet
Playing
• Had worsening of his velopharyngeal insufficiency
– Unable to perform his high-level trumpet playing (holding notes for 5-7 seconds only)
• Visually appeared to close the velopharynx
• Importance of using temporary injections for such purposes
– Gel lasts 2-3 months typically, resorbed late for patient
• Offered repeat injection or referral for dental appliance to close VP
• Opted for dental referral
• Prosthesis created that closed VP, but uncomfortable with playing
– Essentially no helpful literature on this topic
• Chose not to pursue further treatmentParker & Wetzel, ISHA 2016 29
Prosthetic Management
Parker & Wetzel, ISHA 2016 30
Continuous Positive Airway Pressure
• Limited research evaluating efficacy of
treating VPD in individuals with cleft palate
and TBI
• Premise: delivery of air pressure via nasal
passages provides resistance to soft palate
and pharyngeal wall muscles while patient
produces specific sound combinations
Parker & Wetzel, ISHA 2016 31
CPAP Protocol (Kuehn 1991)
• Incremental changes in the amount of time and pressure over eight-weeks/six days per week at-home
• Gradual increase in treatment time from 10 to 24 minutes.
• Pressure increases from 4 to 8.5 cm H20 throughout the program.
• Utterances in the form of a VNCV sequence (v=vowel, n=nasal, c= “pressure” consonant) are produced with emphatic stress on the second syllable. Followed by sentences.
Parker & Wetzel, ISHA 2016 32

4/20/2016
9
CPAP Outcomes
• Perceptual and instrumental gains in reduction of hypernasality inconsistently noted across patients and studies
• No clear evidence of maintenance effects
• Limitations
– Small sample sizes
– Ideal candidate unclear
– Ideal protocol unknown
– Intensive
– Associated costs
Parker & Wetzel, ISHA 2016 33
Expiratory Muscle Strength Training
• Exhaling into a device with a one-way, spring-loaded pressure release valve
• Threshold to set release of the valve set at 60%-80% of max expiratory pressure
• Allows progressive quantifiable increase in resistance
• Transference –training neural substrates and muscles common to respiration and swallowing
• Potential effect on suprahyoid muscle recruitment, expiratory driving pressures for cough, vocal loudness
Parker & Wetzel, ISHA 2016 34
Expiratory Muscle Strength Training
• Sapienza (ASHA 2015) reported case of
improved stress VPI in woodwind player
• Our question: Does EMST provide greater
resistance than that achieved when actually
playing the trumpet?
• To be continued………………….
Parker & Wetzel, ISHA 2016 35
We must not forget that a
quality life is a life full of
meaning and purpose.
We must consider a broad
range of life domains, and
individual values when
treating this patient
population.
Parker & Wetzel, ISHA 2016 36

4/20/2016
10
Parker & Wetzel, ISHA 2016 37
• Swallowing problems related to H&N cancer
and its treatment can be devastating.
• Historically we have tried to effect change in
function after completion of CRT and fibrotic
changes to muscle .
• We are rethinking this with prophylactic
exercise. The evidence regarding treatment
type, frequency, and duration is not clear
• BUT we are gaining on it………
References
• Ashford J., McCabe D., Wheeler-Hegland K, Frymark T., Mullen R., Musson N., Schooling T., Smith Hammond C., (2009)Evidence-Based Systematic Review: Oropharyngeal dysphagia behavioral treatments part III – impact of dysphagia treatments on populations with neurological disorders. Journal of Rehabilitation Research, and Development, Vol 46, 195-204.
• Burkhead LM, Sapienza CM, Rosenbek JC. (2007) Strength-training exercise in dysphagia rehabilitation: principles, procedures, and directions for future research. Dysphagia 22:251-265.
• Carnaby-Mann G, M.P.H. Ph.D., Michale Crary Ph.D., Ilona Schmalfuss M.D., and Robert Amdur M.D. (2012) “Pharyngocise”: randomized controlled trial of preventative exercises to maintain muscle structure and swallowing function during head- and-neck chemoradiotherapy. International Journal of Radiation Oncology Biology.PhysicsVol. 83, No. 1, pp. 210-219.
• Clark, H. (2005) Therapeutic exercise in dysphagia management: philosophies, practices, and challenges. Perspectives on Swallowing and Swallowing Disorders SIG 13, June.
• Clark H., Shelton N.T. (2014) Training effects of the effortful swallow under three exercise conditions. Dysphagia 29, 553-563.
• Cousins, N., MacAulay, F., Lang, H., MacGillivray S., Wells, M.. (2013) A systematic review of interventions for eating and drinking problems following treatment for head and neck cancer suggests a need to look beyond swallowing and trismus. Oral Oncology, 49(5), 387-400.
Parker & Wetzel, ISHA 2016 38
References
• Kuehn, D. P. (1991). New therapy for treating hypernasal speech using continuous positive airway pressure (CPAP). Plastic and Reconstructive Surgery, 88(6), 959-969.
• Kuehn, D. P., Imrey, P. B., Tomes, L., Jones, D. L., O'Gara, M. M., Seaver, E. J., & Wachtel, J. M. (2002). Efficacy of continuous positive airway pressure for treatment of hypernasality. The Cleft Palate-Craniofacial Journal, 39(3), 267-276.
• Lazarus, C., Logemann, J.A., Huang, C.F., and Rademaker, A.W.(2003) Effects of two types of tongue strengthening exercises in young normals. Folia Phoniatr Logop 55, 199-205.
• Lazarus, C.L., (2005) Lingual strengthening and swallowing. Swallowing and Swallowing Disorders SIG 13 Perspectives, June.
• Lazarus, C. (2006) Tongue strength and exercise in healthy individuals and head and neck cancer patients. Seminars in Speech-Language Pathology, 27,260-267.
• Logemann, J.L., Pauloski, B.R., Rademaker, A.W., Lazarus, C.L., Gaziano, J., Stachowiak, L., Newman, L., MacCracken, E., Santa, D., Mittal, B., (2008) Swallowing disorders in the first year after radiation and chemoradiation, Head and Neck Journal, 30(2): 148-158.
Parker & Wetzel, ISHA 2016 39
References
• Malick D., Moon J., Canady J., (2007) Stress velopharyngeal incompetence: prevalence, treatment, and management practices. The Cleft Palate-Craniofacial Journal, Jul;44(4):424-33.
• Robbins J.A., Butler S., Daniels S., Gross R.D., Langmore S., Lazarus C., Martin-Harris B., McCabe D., Musson N., Rosenbek J.C.,(2008 ) Swallowing and dysphagia rehabilitation: translating principles of neural plasticity into clinically oriented evidence. Journal of Speech, Language, and Hearing Research, Vol 51, S276-S300.
• Wheeler–Hegland, K.M., Rosenbek, J.C . Sapienza, C.M., (2008) Submental sEMG and hyoid movement during Mendelsohn maneuver, effortful swallow, and expiratory muscle strength training. Journal of Speech, Language, and Hearing Research, Vol. 51, 1072–1087.
• Yoon, W. L., Khoo, J. K. P., Rickard Liow, S. J. (2014). Chin Tuck Against Resistance (CTAR): New method for enhancing suprahyoid muscle activity using a Shaker-type Exercise. Dysphagia, 29(2), 243-248.
ASHA Presentations
• Burkhead-Morgan, L. PhD, CCC-SLP, “Working Out Dysphagia with Exercise Based Treatments” ASHA Presentation 2013
Parker & Wetzel, ISHA 2016 40
4/20/2016
11
Evidence Review for Dysphagia
Rehabilitative Therapy in Patients
with
Head and Neck Cancer
Jaime Bauer Malandraki, MS, CCC-SLP
Clinical Instructor / Purdue University
Clinical Director / Purdue I-EaT Swallowing Research Clinic
Outline
• Evidence Review
– Types and levels of research evidence
• Chronological review of recent research
– First: General dysphagia tx in HNC
– Second: Prophylactic dysphagia tx in HNC
• Conclusions
Disclosures
• Disclosures for Jaime Bauer Malandraki
– Salary: Purdue University
– No other relevant disclosures
EBP
• True evidence-based practice comes from the
synergistic relationship of three types of
evidence
Image: ASHA.org

4/20/2016
12
Levels of Research Evidence
(Burns et al. 2012)
Rehabilitative Intervention
in HNC
• Most Common Outcome Variables
(Goals) Assessed
– Airway invasion (PA Scale)
– Residue scales
– Xerostomia assessments
– Diet level and type (NOMS, FOIS, or similar
scale)
– QOL (MDADI, HNCI)
Rehabilitative Intervention
in HNC
• Types of Interventions
– Compensatory (postures and diet
modification)
– Strengthening exercises (tongue strengthening,
effortful swallow)
– ROM [with strengthening components] (head
raise, Mendelsohn, Masako, supraglottic
swallow, Therabite, pitch elevation)
– Electrical stimulation
– Dilatation or surgical interventions
Kraaijenga et al. 2014
COMBINE
Treatment post CRT and surgery
Highest Level of Evidence• Lazarus et al. 2014 “Effects of Exercise on Swallowing and Tongue
Strength in Patients with Oral and Oropharyngeal Cancer Treated with Primary Radiotherapy with or without Chemotherapy”
– RCT
– Outcome variables: tongue strength, VFSS variables (OPSE), QOL (HNCI), xerostomia assessment
– Patients: Stage II-IV oral or oropharyngeal cancer, no hx of c-spine surg.
– One month post-CRT randomized in 1 of 2 groups
1. Treatment: 6 weeks of traditional therapy plus lingual strengthening (tongue depressors) [Treatment]
2. 6 weeks of traditional therapy (ROM exercises & Mendelsohn) [Control]
– Results:• 23 pts; 12 � Tx arm; 11 � control group [16 ended up doing the study]
• Compliance: Tx group: only 3 subjects fair to good compliance
• NO significant differences in tongue strength, OPSE, salivary flow, minimal improvements in QOL

4/20/2016
13
Treatment post CRT and surgery
Highest Level of Evidence• Logemann et al. 2009 “A Randomized Study Comparing the
Shaker Exercise with Traditional Therapy: A Preliminary Study”
– Outcome variables: Aspiration, residue, diet level (PSSD), hyolaryngealbiomechanics,
– Patients: HNC and stroke (with at least 3 months hx of severe dysphagia with reduced UES opening)
– 1 of 2 groups
1. 6 weeks of Shaker with 2 visits/week [treatment]
2. 6 weeks of a series of exercises (super-supraglottic swallow, Mendelsohn, tongue retraction) 5 min 10x / day [control]
– Results:• 14 pts; 5 � Tx arm; 9 � control group
• Improvements in: aspiration (3/5 of tx group and 0/9 in control group); hyolaryngeal biomechanics (both groups)
• No improvements in residue
Treatment post CRT and surgery
Highest Level of Evidence• Langmore et al. 2015 “Efficacy of Electrical Stimulation and Exercise for
Dysphagia in Patients with Head and Neck Cancer: A Randomized Clinical Trial”
– Outcome variables: PAS, OPSE, hyoid excursion, diet level (PSS), QOL (HNCI)
– Patients: HNC 3 months post CRT/RT with moderate to severe dysphagia
– 1 of 2 groups
1. 12 weeks of E-stim with 3 exercises (super-supraglottic, Mendelsohn, effortful) [treatment]
2. 12 weeks of sham E-stim with same exercises [control]
Protocol: 2x/day, 6 days/week
– Results:• 170 pts; 116 � Tx arm; 54� control group (although analysis included less)
• PAS scores: improved in control group (but small effect size); no change in txgroup
• No other physiological improvements in either group
• BUT: significant improvements in diet and QOL!
• Compliance: ~50% for both groups
Treatment post CRT and surgery
Conclusions – in a nutshell
• Treatment post CRT/RT for pts with chronic severe
oropharyngeal dysphagia: NOT effective in
improving swallowing physiology
• Improvements seen in QOL and diet level
• These results should be interpreted with caution
• Prophylactic exercises may be more promising
Treatment DURING CRT/RT
Prophylactic exercises• Van der Molen et al. 2011 “A Randomized Preventative Rehabilitation Trial in
Advanced Head and Neck Cancer Patients Treated with Chemoradiotherapy: Feasibility, Compliance, and Short-Term Effects”
– Outcome variables: PAS, residue, MIO (maximum interincisor mouth opening), BMI, FOIS, pain assessment
– Patients: HNC with advanced (stages III and IV) SCC with CRT
– 1 of 2 groups
1. “Standard”: 10 weeks of standard exercises (ROM exercises, effortful, Masako and supraglottic) [Control]
2. “Experimental Preventative” 10 weeks of ROM with Therabite and strengthening with swallow with open mouth [Treatment]
Protocol: 3x/day (varied reps/durations depending on activity)
Results:• 55 pts; 27� Tx arm; 28� Control group (analysis done on 49 pts)
• Short-term Clinical Effects, Overall:
– Positive: Sig. less residue with liquids, puree, cookie
– Negative: No sig diff in PAS or pain pre- and post-tx; sig decrease in MIO; sig weight loss; sig decrease in FOIS scores
• Short-term Clinical Effects, Group Comparison:
– Experimental group showed sig. less residue with cookie
– No other sig. difference between groups
4/20/2016
14
Treatment DURING CRT/RT
Prophylactic exercises• Carnaby-Mann et al. 2011 “Pharyngocise”: Randomized Controlled
Trial of Preventative Exercises to Maintain Muscle Structure and Swallowing Function During Head-and-Neck Chemoradiotherapy”– Outcome variables: muscle size (MRI); FOIS; MASA; several other physiological
and diet outcomes
– Patients: HNC with CRT/RT (no prior hx of dysphagia d/t cancer)
– 1 of 3 groups
1. Usual care (counseling and feeding precautions)
2. Standardized sham therapy (buccal extension maneuver and diet modification)*
3. Pharyngocize: falsetto, tongue press, hard swallow, Therabite*
*Protocol: 10 reps in 4 10-min cycles � 45 min sessions
Results:• 58 pts; 20 usual care; 18 sham; 20 Pharyngocize
• Moderate compliance (more in the sham group)
• More preservation in 3 muscles with Pharyngocize (although all declined)
• Better MASA scores and mouth opening for Pharyngocize
• NO difference in VFSS and FEES physiologic parameters or in weight
Treatment DURING CRT/RT
Prophylactic exercises• Kotz et al. 2012 “Prophylactic Swallowing Exercises in Patients with
Head and Neck Cancer Undergoing Chemoradiation”
– Outcome variables: PSS-H&N; FOIS assessed at baseline, post CRT and 3, 6, 9 and 12 months post CRT
– Patients: newly dx HNC with CRT
– 1 of 2 groups
1. Standard care (Ax and tx AFTER CRT if dysphagia present) [Control]
2. Tx group (5 exercises: effortful, 2 tongue retraction, super-supraglottic, Mendelsohn) [Treatment]
*Protocol: 3 sets of 10 reps of each exercise daily
Results:• 26 pts
• No significant difference in FOIS and PSS-H&N post CRT
• Better FOIS and PSS-H&N scores at 3 and 6 months post CRT
• BUT! No difference again at 9 and 12 months
Treatment DURING CRT/RT
Prophylactic exercises
• Hutcheson et al. 2013 “Eat and Exercise During Radiotherapy or Chemoradiotherapy for Pharyngeal Cancers: Use It or Lose It”
– Design: Retrospective observational study
– Patients: 497 pts with RT or CRT for pharyngeal CA between 2002-2008
– Independent outcome variables: PO status; adherence
– Dependent outcome variables: last diet level post CRT/RT; length of G-tube dependencei
– All patients: prophylactic exercises (a total of 10 exercises) performed daily; some also on G-tubes (but not all)
Results:• 26%: no oral intake post CRT/RT
• 58%: exercise adherence
• Oral intake during CRT/RT and adherence were independently associated better long –term diet level AND shorter duration of g-tube dependency
Treatment DURING CRT/RT
Conclusions – in a nutshell
• Treatment during CRT/RT: possibly effective
• Data from retrospective and few well controlled
RCTs
• More research is required with larger sample sizes
and more cohesive/uniform treatment regimens
4/20/2016
15
A new treatment approach
adapted for HNC pts(Malandraki and Bauer Malandraki)
8-week rehabilitation protocol with 3 parameters:
1. Evidence-based oropharyngeal training increasing gradually in intensity
2. Targeted swallowing practice (TSP) increasing gradually in complexity
3. Adherence-inducing features
Malandraki et al. 2016, Arch Phys Med Rehab
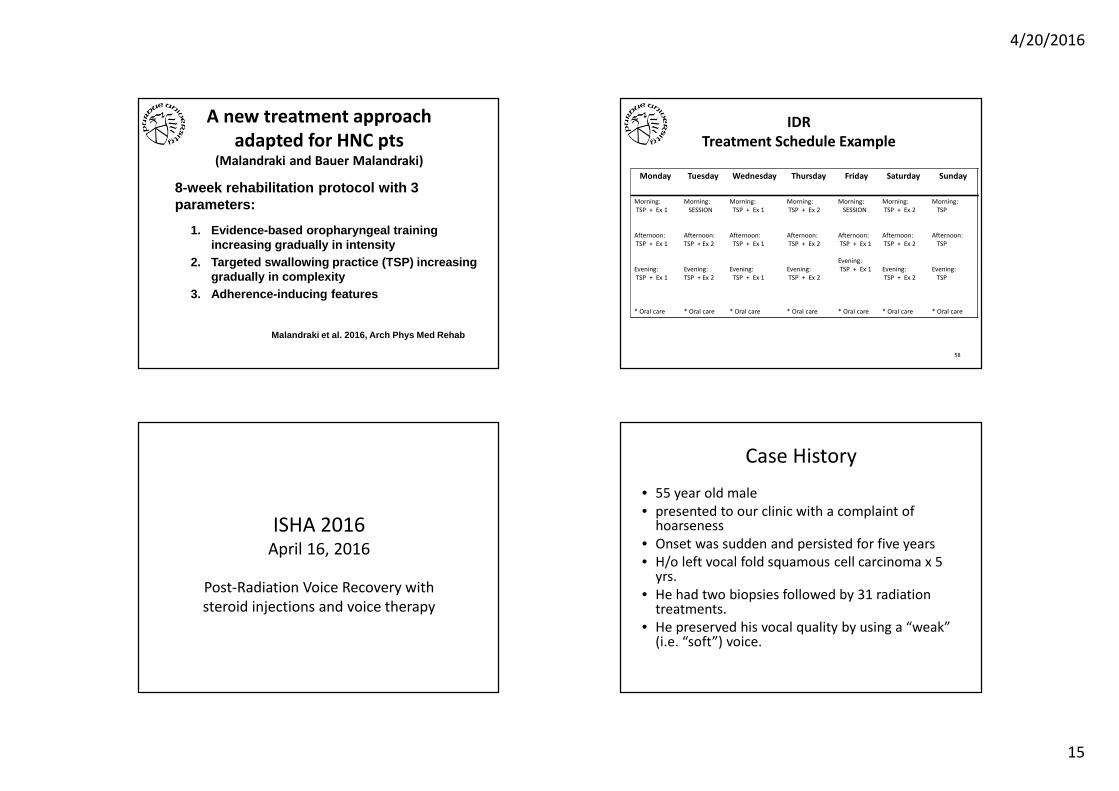
IDR
Treatment Schedule Example
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Morning:
TSP + Ex 1
Afternoon:
TSP + Ex 1
Evening:
TSP + Ex 1
* Oral care
Morning:
SESSION
Afternoon:
TSP + Ex 2
Evening:
TSP + Ex 2
* Oral care
Morning:
TSP + Ex 1
Afternoon:
TSP + Ex 1
Evening:
TSP + Ex 1
* Oral care
Morning:
TSP + Ex 2
Afternoon:
TSP + Ex 2
Evening:
TSP + Ex 2
* Oral care
Morning:
SESSION
Afternoon:
TSP + Ex 1
Evening:
TSP + Ex 1
* Oral care
Morning:
TSP + Ex 2
Afternoon:
TSP + Ex 2
Evening:
TSP + Ex 2
* Oral care
Morning:
TSP
Afternoon:
TSP
Evening:
TSP
* Oral care
58
ISHA 2016April 16, 2016
Post-Radiation Voice Recovery with
steroid injections and voice therapy
Case History
• 55 year old male
• presented to our clinic with a complaint of hoarseness
• Onset was sudden and persisted for five years
• H/o left vocal fold squamous cell carcinoma x 5 yrs.
• He had two biopsies followed by 31 radiation treatments.
• He preserved his vocal quality by using a “weak” (i.e. “soft”) voice.

4/20/2016
16
Patient report about his voice
• He was a singer for "all my life". Sang in a band, and was on a record label for several years.
• Frustration: His voice required a 30-min warm up in order to sing for 10 minutes before he was too fatigued to continue.
• breathy / raspy, husky and rough (after talking for awhile). There has been associated upper register compression, vocal fatigue.
• upper middle to falsetto register break ("no falsetto whatsoever").
More Case/Social History
• The patient was re-evaluated at the VA by an ENT who noted white exudate, and recommended he see Dr. Halum.
• Previous medical history included esophageal web repair x 18 months.
• Social: The patient drinks about 1 bottle water daily; caffeine: 1 cup coffee daily + Diet Mountain Dew (24 oz daily); ETOH: none; TOB: cigarettes 1 ppd x 20 yrs, quit 20 yrs ago. Smoked cigars for a few years, but nothing after throat cancer until about 6 months ago…
Videostrobe #1 Initial Findings
• The patient’s dysphonia is related to L vocal fold scarring / sulcus vocalis.
• “We discussed that unfortunately at this point we have no cure for vocal fold scarring, although we do have some treatment options that may improve the overall quality of the voice.
• While we can surgically excise the scar tissue or sulcus, there is a risk of worsening scarring and worsened voice outcome if scar / sulcus excision alone is performed.
• Alternatively, we could also perform serial steroid injections, which has no risk of increasing the scarring, and can improve the vocal fold compliance/mucosal waveform to help the voice.
• Use of the pKTP laser is also an option that I have seen help increase compliance of scarred vocal folds. Finally, in severe cases, scar elevation with insertion of a fascial or fat graft is the most aggressive approach to improve the voice, and I have generally found mild improvements after this procedure (with the worst outcomes just not seeing dramatic improvement or change).
• After discussing risks, benefits, and alternatives of all of these options with the patient, the decision was made to proceed with serial kenalog steroid injections and work with our speech language pathologist.”
4/20/2016
17
Progression of treatment
• Serial Kenalog Injections – 3 injections over a period of 6 weeks.
• LPR therapy: RSI = 4, RFS = 20. Twice daily Omeprazole 40 mg.
• Voice therapy
• 3/18 first kenalog injection
• 3/24: voice evaluation + therapy session
• 4/1: second kenalog injection
• 4/7 voice therapy session #2
• 4/15: third kenalog injection
• 5/26 final voice therapy session, #3.
Videostrobe #2 - kenalog injection #1
Voice therapy
• Compliance issues, somewhat related to his work schedule. He attended 3 of the 4-6 recommended.
• So, no discharge notes, b/c comparison measures couldn’t be taken.
• Phone call made for 6-month follow-up.
Main tools in voice therapy for this patient:
1. Vocal Function Exercises
2. Resonant Voice (LMRVT)
Voice therapy session 1
• Along with being an avocational singer, he installed corporate telecommunications, and used to record corporate client’s greetings, but no longer could. He also did employee training for 2-4 hour sessions, and this was increasingly problematic.
• Introductions to vocal hygiene/LPR support and VFE

4/20/2016
18
Voice therapy 1, continued.• Hygiene: patient drank
about 16 oz water, and used multiple diuretics under physician supervision due to advanced kidney and liver disease. He was not under hydration restrictions, so recommended he trial up to 64 oz daily, with caveat that he monitor wrist/ankle swelling”.
• Omeprazole 40 mg twice daily
Videostrobe #3: second kenalog
injection 2 weeks later.
Voice therapy session #2
• 1 week post second injection
• VFE: times averaged to 13.77 seconds overall with range from 10-18 seconds.
• Cues: used a wall press for breath support, then branched down to a lunge over the knee. Also had the patient walk around while sustaining sound so that he couldn’t hold his breath.
Voice therapy session #2,
continued.
• Introduced resonance, with good return of demonstration.
• He could discern “good buzzy” (resonance) vs. “bad buzzy” (glottal fry). This was initially confusing, but when he got it he reported “This is blowing my mind, man!”
• Directly correlated to decreased effort and a clearer voice for him.
4/20/2016
19
Kenalog injection #3. Voice therapy session 3
• Hygiene: AT GOAL.
• VFE #4: average MPT: 15.30 seconds with a range of 11-20 sec.
• Now, more effort associated with higher pitches. This didn’t show up before, because he didn’t have them.
• Cued patient for a “lighter, clearer sound”
Voice therapy session 3,
continued.
• Other cues: – “Walk with energy”
– Clarity
– “don’t push air” –“release air”
• Successfully achieved good balance in sustained sound, and applied right away to vocalises and singing voice while standing still.
• Very happy with his singing voice in this session.
Vocal Scarring
• The diagnosis of “vocal fold scar” was an “end game” diagnosis for years, whether a result of injury or a result of surgery, with little recourse for the patient.
• Studies have recently been published regarding office based injections:
– Mortensen, M., & Woo, P. (2006). Office steroid injections of the larynx. The Laryngoscope, 116(10), 1735-1739; and
– Rosen, C. A., Amin, M. R., Sulica, L., Simpson, C. B., Merati, A. L., Courey, M. S., Johns, M. M. and Postma, G. N. (2009), Advances in office-based diagnosis and treatment in laryngology. The Laryngoscope, 119: S185–S212. doi: 10.1002/lary.20712 ) ….

4/20/2016
20
Vocal Fold Scarring
• …And treatment of chronic vocal fold scarring using different agents, including hyaluronic acid-based injectables:– Bless, D. M., & Welham, N. V. (2010). Characterization of vocal
fold scar formation, prophylaxis and treatment using animal models. Current opinion in otolaryngology & head and neck surgery, 18(6), 481.
– Thibeault, S. L., VanGroll, P. J., Kriesel, K. J., Chan, R. W., Bless, D. M., Suzuki, T., & Ford, C. N. (2002). Treatment of vocal fold scarring: rheological and histological measures of homologous collagen matrix. Annals of Otology, Rhinology & Laryngology, 111(10), 884-889.
• In cases of vocal fold scarring, as well as many other diagnostics, there is more hope than ever for our patients.
Come see us at
The Voice Clinic of Indiana!