IRAQ - HumanitarianResponse
13
HEALTH CLUSTER BULLETIN #4 (June 2015) Iraq Humanitarian Crisis IRAQ Dahuk, Iraq © ACF - The Iraq HRP 15 was officially launched on June 4 th , 2015 in Brussels. - An estimated 7.82 million people – close to 20 per cent of the population – are in need of essential health care services. - 84% health care delivery points supported by health partners effectively closed on 30 th June, 2015 in the absence of new sources of funding to the health cluster affecting over 2 million affected people. - In response to recent mass-displacement from Anbar Governorate, a quick response by health cluster partners lead by WHO launched delivery of life-saving services to IDPs and affected host communities. - During the month of June, sixty seven sentinel sites including eight refugees, fifty nine internally displaced people’s (IDP) camps and ten mobile clinics submitted their weekly reports timely and completely.
Transcript of IRAQ - HumanitarianResponse

HEALTH CLUSTER BULLETIN #4 (June 2015) Iraq Humanitarian Crisis
IRAQ
Dahuk, Iraq © ACF
- The Iraq HRP 15 was officially launched on
June 4th, 2015 in Brussels.
- An estimated 7.82 million people – close to 20
per cent of the population – are in need of
essential health care services.
- 84% health care delivery points supported by
health partners effectively closed on 30th
June, 2015 in the absence of new sources of
funding to the health cluster affecting over 2
million affected people.
- In response to recent mass-displacement
from Anbar Governorate, a quick response by
health cluster partners lead by WHO launched
delivery of life-saving services to IDPs and
affected host communities.
- During the month of June, sixty seven sentinel sites including eight refugees, fifty nine internally displaced people’s (IDP) camps and ten mobile clinics submitted their weekly reports timely and completely.
HEALTH CLUSTER COORDIANTOR 2
Humanitarian Situation and Public Health Risks
An estimated 7.82 million people – close to 20 per cent of the population – are in need of essential
health care services. Up to 53 per cent of these are estimated to be women and an estimated 18 per
cent are under the age of five. Political instability and expanding conflict have not only disrupted the
optimal delivery of health care services, but have also increased the overall need for emergency
medical services, including reproductive health and referral services, along with emergency casualty
management and delivery of Mental Health and Psychosocial Support (MHPSS). With the new
waves of conflict and mass displacement in South and Central Iraq, more than three million
people are living as IDPs in camps or outside the camps as over two million people are living in areas
controlled by armed groups with minimal access to health care services. The health care services
needs are continuously increasing, creating an even greater burden on thinly stretched and
insufficient healthcare services. Health services provided by the Government of Iraq are reduced
to minimum in most of conflict affected areas, mainly due to security threats. There is lack of
medicines and medical supplies including vaccination cold-chain, damaged health facilities and
with their displaced workforce.
The uncertain funding situation is straining the capacity of the health cluster partners in
delivering the minimum package of health care services outlined in the humanitarian strategic
plan 2015.
The health cluster partners and stakeholders are providing the health services delivery to the
IDPs and refugees in camps and in host communities but now they are facing enormous
challenges in their response due to shortage of funding for delivery of essential life-saving
health care services to affected people including pregnant women and children. The impact of
shortage of funding will result in closure of all the critical emergency life-saving health care services
which will have a direct impact of the health status of the affected population including children and
women.
Compromised water and sanitation services, in the absence of reliable surveillance and interrupted
immunization services together expose the affected population to a high risk of communicable
diseases, particularly waterborne and vaccine preventable diseases like cholera, bloody diarrhea,
typhoid, acute Jaundice syndrome and measles.

HEALTH CLUSTER COORDIANTOR 3
Public Health Priorities, Needs and Gaps
Ensure improved access to essential package of life-saving health care services to all vulnerable groups of boys, girls, men and women among affected population.
Enhancing local capacities to reduce the risk, prepare for, detect and respond to outbreak of diseases among the conflict affected population.
Ensure maximum level of vaccine coverage through monitoring of immunization coverage and launching of immunization mass campaigns as needed.
Contribute to maintaining maternal and child mortality stable through ensuring minimum emergency obstetric and child health services for the IDPs, refugees and other affected communities.
Communicable Diseases
During the month of June, sixty seven reporting sites including eight refugees, fifty nine internally displaced people’s (IDP) camps and ten mobile clinics submitted their weekly reports timely and completely.
The total number of consultations reported was 55,198 (male=24,786 and female=30,266)
During June, acute respiratory tract infections (ARI) (n=20,558), acute diarrhea (n=5,294) and skin diseases (n=2,939) were the leading cause of morbidity in all the camps.
In the last two weeks of June, The proportions of Acute Diarrhea in IDP camps have increased gradually by two percent since week 25 (week 25: 9% and week 26:11%) while proportions of Acute Diarrhea trend in refugee camps has increased by one percent since last week (week 25=7% and week 26=9%).
The trends of lower ARI is generally decreasing with the advent of summer although proportion of upper ARI in week 26 increased by 1% and lower ARI decreased by 1% as well when compared with week 25, (week 25: Upper ARI=88% & Lower ARI=12% and week 26: Upper ARI=89% & Lower ARI=11%).
A total of eighty two alerts were generated by EWARN in June; eighteen alerts were generated from refugee camps and sixty four from IDP camps. Forty four of these were verified as true for further investigation and appropriate response by respective governorates DOH/who and thirty eight alerts did not follow the case definitions thresholds.

HEALTH CLUSTER COORDIANTOR 4
Trends of Water borne Diseases in IDP camps: The below graph shows the trends of waterborne diseases (Acute Diarrhea, Bloody Diarrhea and Acute Jaundice Syndrome) from IDP camps, indicating a steady increase in waterborne diseases during summer . The trend indicates a gradual increase in the proportion of waterborne diseases in IDP camps since week 17. (See below graph)
Figure VIII: Trend of Waterborne diseases from IDP camps, from week 1 to 26
Trends of waterborne diseases in Refugee camps: The below graph shows the trends of proportion of waterborne diseases (Acute Diarrhea, Bloody Diarrhea and Acute Jaundice Syndrome) from refugee camps, indicating a steady increase of 1% per week since week 22.
Figure IX: Trend of Waterborne Diseases (Acute Diarrhea, Bloody Diarrhea and Acute Jaundice Syndrome) as one of the leading communicable diseases from Refugee camps, weeks 1 to 26
HEALTH CLUSTER COORDIANTOR 5
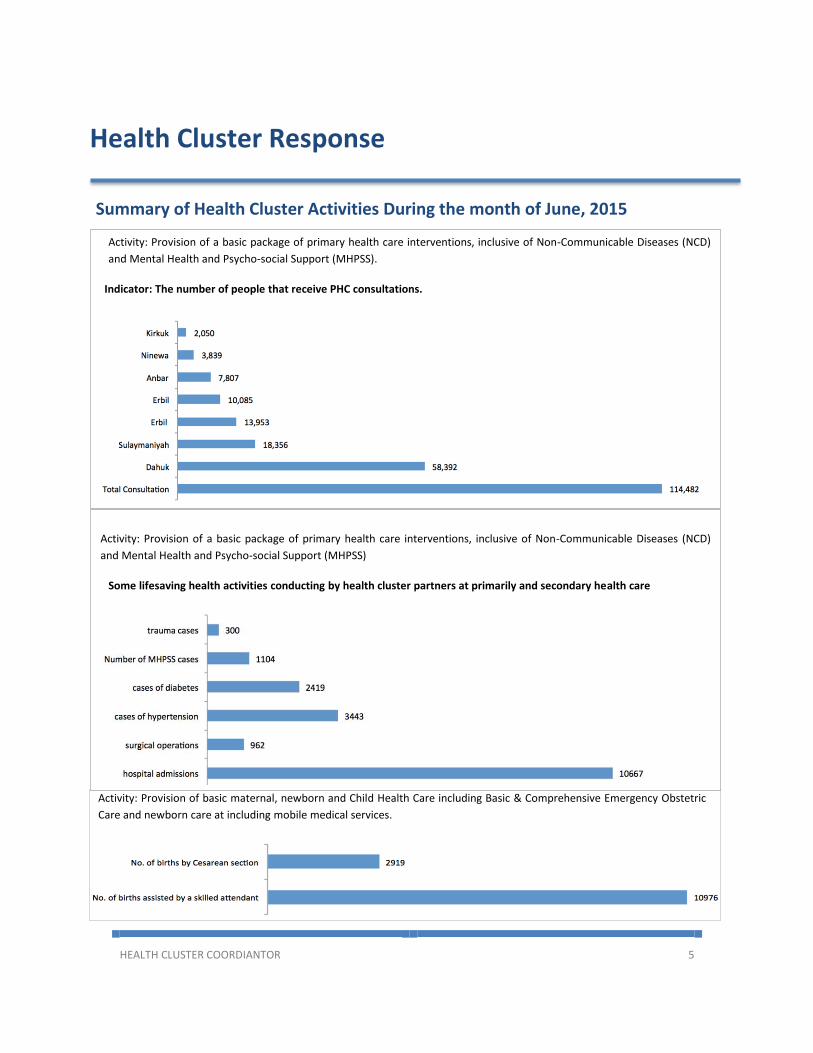
Health Cluster Response
Summary of Health Cluster Activities During the month of June, 2015
Partners Report
Activity: Provision of a basic package of primary health care interventions, inclusive of Non-Communicable Diseases (NCD)
and Mental Health and Psycho-social Support (MHPSS).
Indicator: The number of people that receive PHC consultations.
Activity: Provision of basic maternal, newborn and Child Health Care including Basic & Comprehensive Emergency Obstetric
Care and newborn care at including mobile medical services.
Activity: Provision of a basic package of primary health care interventions, inclusive of Non-Communicable Diseases (NCD)
and Mental Health and Psycho-social Support (MHPSS)
Some lifesaving health activities conducting by health cluster partners at primarily and secondary health care
17,746

HEALTH CLUSTER COORDIANTOR 6
Health & Nutrition-IDP Crisis: UNICEF June 2015
In Bagdad, Anbar and Kerbala during June 2015, 24,231 under 15 year old children from high-risk areas vaccinated against polio, and 17,890 children aged 9 months to 15 years against measles
UNICEF continues supporting MOH to transfer vaccine share for 3 month to Anbar district (MMR, Measles, OPV, Tetra, Rota, BCG, and Hepatitis. B child, HEB B adult, Meningococcal, ATS, Typhoid, Influenza vaccine, syringes)
6000 leaflets containing messages for IDPs on prevention of scabies, lice and personal hygiene, and installed 6 billboard in 5 IDPs camps and distributed 6000 leaflets containing messages on the important of immunization specially polio.
UNICEF had Supported Dyilaa DOH to conduct rapid nutrition assessment for U5 IDPs in camps in Dyilaa, the assessing 1800 child. Results are yet to come.
In Duhok EPI training courses was conducted for 10 staff (8 female) under the same project and these trained staff will provide vaccination services to 15000 U5 children and > 3000 PLW. Health and Nutrition supplies had delivered to DOH/Duhok, these supplies consisted of therapeutic nutrition, IEHK kit-medicines, zinc tablets, First aid kit A, measuring scales and other essential supplies, and these will fill the needs of 500,000 IDP and Refugee inside and outside camps.
Another training courses was conducted for 165 health staff working in 116 main PHCC on measuring height/weight of U5 children, updated WHO growth monitoring chart, and MOH/ child booklet the trained staff will total of 200,000 U5 children in 8 districts of Erbil governorates.
In Kirkuk, Six field health education teams participated in field activities to prompt IDPs awareness on preventing communicable diseases and insure IYCF counselling
# of location visited 319, # of IDPs families educated 9318(24352), # of mass meetings 177, # of individual meetings 13990, # of health messages distributed 14319.
30 teams each of 2 members participated in field vaccine defaulters activities for 10 days in June 2015. A total of 14516 defaulters among IDPs vaccinated in 300 location visited.
In Sulaimanyah and Garmian: In Salih agha, Kula IDP camp, Kefir, She Langat, Quorate camp and village and with the three check points vaccination team was initiated and supported by UNICEF for immunizing all newly arrived IDPs for (polio and measles), data shows that: 3047 children aged between 0- 15 year vaccinated and 2,922 children 9 month – 15 year vaccinated against measles

HEALTH CLUSTER COORDIANTOR 7
Reproductive Health: (UNFPA)
UNFPA and its partners continue to deliver humanitarian interventions in both GBV and RH and
strengthen the coordination efforts.
UNFPA managed to transport and distribute 17,321 (data for more governorates to come yet) dignity kits, 2,000 clean delivery kits to IDPs settling in the southern and northern conflict affected governorates in June 2015. Additionally, following table describes other kits provided during June 2015.
Erbil Microgynon Pharmaceutical Products (Oral Contraceptives ED Fe)
Pack 58,950
Erbil 28052 Intrauterine Devices (IUD) PCS 833
Erbil Microlut Pharmaceutical Products (Oral Contraceptives)
Pack 25,240
Erbil 4645 Syringe, 1 ml, with needle, single use Pack 106
Erbil 611458 Male Latex Condoms Box 5,480
Erbil Depo- Provera STERILE AQUEOUS SUSPENSION 150MG/ML
Pack 767
Erbil RH KIT 6B Clinical delivery assistance (1,2,3,4 of 5) Kits 1
Erbil 28281 Azithromycin tablets 500mg 4MK 150 Jar 28
Erbil 20150302 Autoclave UNIT 6
Erbil RH KIT 6A Clinical delivery reusable Kits 4
Erbil 0289500 Dressing trolley, 2 flat shelves UNIT 4
Erbil 28186 (Item 12) Light, examination, mobile UNIT 4
In spite of extreme challenges, UNFPA has already distributed RH kits in the affected governorates and ensuring RH services in 10 affected governorates.
Governorate Beneficiaries for Dignity Kits Total
Women Infants
Babylon 4240 - 4240
Baghdad 8335 - 8335
Diyala 140 - 140
Kerbala 1506 - 1506
Najaf 3100 - 3100
Sulaymeniyah 6000 - 6000
Ongoing insecurity, fuel shortage and other logistical challenges hampered full implementation of the ongoing humanitarian assistance. Poor telecommunications links have also hindered full reporting by partners. UNFPA has taken onboard the GBVIMS expert to rollout GBV IMS in Iraq. International procurement of RH kits continues on need basis.

HEALTH CLUSTER COORDIANTOR 8
Handicap International (HI)
In the framework of its current emergency activities for Internally Displaced Population, HI is conducting Conventional Weapons (CWs) and Improvised Explosive Devices risk prevention and victim assistance. HI’s activities are, by nature, transversal between protection and health sectors: the identified objective is to raise protection concerns (awareness, identification, victims referral) and to address the victims’ specific needs (physical rehabilitation and psychosocial support).
In Chamishku camp, where HI is running both protection and health activities, a 12 year old boy became injured as he was playing with old ammunition he had found with his friends. As he and his friends were throwing rocks at the ammunition, one of the shells exploded and his left hand was seriously injured.
After surgery, the young boy was referred to HI teams, which provided emergency physical rehabilitation and psychosocial support.
HI is continuing prevention activities in order to limit the negative impact of CWs and IEDs in its areas of intervention. HI aims at developing victim assistance everywhere it will be needed in Iraq.”
Médecins du Monde (MdM)
In response to the current crisis situation, MdM has been developing activities focused on access to health, mainly for IDPs in Dohuk Governorate (Dowadia camp and Chamishko camp), and in Kirkuk governorate for IDP and vulnerable host communities through PHCC (Primary Health Care Center) and MC (Mobile Clinic) support. In line with development of health care services in PHCC in the camps, SRH activities were launched in June. Dawodia Camp was the first to develop those, providing antenatal and postnatal cares to pregnant women.
Picture: © Handicap International
Physiotherapy session for a 12 y.o boy injured by CWs / Chamishku Camp
Picture: © Médecins du Monde - Women
consultation in Dawodia Camp

HEALTH CLUSTER COORDIANTOR 9
MdM is continuing consultation, nursing cares, psychosocial support and prevention activities to vulnerable populations attending PHCC and Mobile Clinics (MC). All activities have been developed in close collaboration with DOH from the area of intervention
IOM health response
IOM is supporting the National Tuberculosis Program (NTP) with one mobile team in each of following governorate Erbil, Duhok, Sulymaniah and Kirkuk.asM mobile teams had supported 234 confirmed TB cases in KRI by providing transportation assistance, observing their treatment (Applying DOTs) for the cases, distribution of 56 food package of high protein diet, 78 contact relatives were traced, and 137 TB presumptive cases were screened (by X-ray and/or sputum).
IOM donated two Safety Cabinets to Sulymaniyah main NTP center to protect their laboratory staff from any danger of mycobacterium tuberculosis germ during their daily work.
In coordination with Community Stabilization and Reintegration Unit of IOM , IOM health unit conducted awareness sessions for Syrian refugees, two sessions in Duhok in Domiz 1& 2 and Gawilan camps; four sessions in Erbil in Qushtapa,Kawrgosk,Darashakran and Basirma camps; two sessions in Sulymaniyah in Arbat refugee camp; these sessions were about communicable diseases (respiratory including TB, water borne diseases, general hygiene and skin diseases) the lecturer explained the definitions , clinical manifestations, most important ways of transmission and the preventive measures. A total of 238 refugees attended the awareness sessions.
WHO response updates:
WHO, as health cluster lead, has been working very closely with health partners to respond to
health needs. The following were identified as the most pressing health needs:
1. Ensuring access to essential life-saving health care and supporting the provision of
primary health care (PHC) services, including mental health and non-communicable
diseases.
2. Supporting the early detection of and response to communicable diseases.
During the June 2015, 5 IOM mobile medical teams (MMT) in Erbil, Sulymaniyah, Duhok and Kirkuk conducted 5168 PHC consultations among IDPs and Host Communities. Furthermore, IOM static clinic in Shekhan camp, Duhok received 3180 patient visits. From all the above mentioned cases, 346 cases had been referred for further investigations or treatment to secondary or tertiary health facilities.

HEALTH CLUSTER COORDIANTOR 10
3. Supporting maternal and nutritional health services in locations with identified gaps.
4. Supporting referral services through providing equipment, kits and personnel to
secondary and tertiary health facilities so as to ensure continuum of care for
complicated cases.
In addition to its on-going effort in supporting the Ministry of in Health in respect to the above mentioned health needs, the following were achieved during the month of June:
In Kirkuk WHO supported eight mobile medical teams (MMTs) by paying incentives medical staff providing therapeutic and preventive services to IDPs and host community in hard to reach areas. The teams also distributed chlorine tablets to support water purification at household levels and held health education and hygiene sessions with the IDPs with a focus in prevention of communicable and waterborne diseases.
WHO in collaboration with the Directorate of Health in Dohuk trained 25 medical and paramedical health staff on cholera case management.
On 7 to 9 June 2015, thirty health workers including doctors, paramedics and nurses in Kirkuk were trained on communicable disease prevention measures with the objective of strengthening health promotion initiatives at community and health facilities levels.
On 8 to 9 June 2015, WHO supported the DOH, Diyala to train 22 individuals from the Department of Public Health on rapid response mechanism to prepare teams (RRT) in readiness for any outbreak potential in the governorate .
Two Mobile Medical Clinics (MMCs) donated by WHO with support to MOH, 10 ambulances and six Mobile Medical Teams (MMTs) were involved in the mission conducted by WHO team joined by the DMOH and Al-Anbar DOHs, ICRC and IOM to Al-Salam camp south of Baghdad Governorate on 6 June 2015.
UIMS response updates: WHO response updates: In response to situation in Al-Qaim, UIMS run the PHC center in Al-Obeidi camp for Syrian
refugees in the border district. The number of consultation in June was 283 patients as the
center is weekly report and EWARN report to health cluster and WHO, respectively.
In Ameriyat Al-Fallujah, UIMS provide primary health services for IDPS through the PHCC
supported by WHO with a total number of 5156 consultations during the month of June,
physical examinations, lab services, pharmacy, dental clinic, and specialized diagnosis. UIMS
keeps sending weekly report and EWARN report to health cluster and WHO, respectively.

HEALTH CLUSTER COORDIANTOR 11
In June UIMS opened a delivery room in Ameriyat Al-Fallujah supported by UNFPA, which
started providing services to the IDPs. The delivery room is located close to our PHCC in
Ameriyat Al-Fallujah and being used as a referral center for obstetric cases.
UIMS also operated another PHC center located in Al-Nakheeb IDPs camp, which is also
supported by WHO. The center provides primary health services to the IDPs as the number
of consultations in June reached to 1,430 cases. UIMS keep sending weekly report and
EWARN report to health cluster and WHO, respectively.
Health Cluster Coordination
The Health Cluster in Iraq has been working within the Iraqi Humanitarian Response Plan
framework along with national and international health partners towards maximization of
access to life-saving essential health services for affected population and mitigation, preparing
for and responding to public health risks with focus on control of communicable diseases and
hence preventing avoidable morbidity and mortality.
The Health Cluster mechanism remained fully functional at the national level in Erbil and sub-
national levels in Erbil, Sulaimania and Dohuk hubs. The partners had regular biweekly and ad
hoc meetings as required, sharing the information on health situation and ongoing activities
(through 3Ws) as the health cluster regularly produced weekly cluster monitoring reports and
produced health cluster maps including the map of health facilities closing end of June due to
lack of funding.
The Health Cluster also actively participated in the Inter-Cluster Coordination meetings (ICCG)
and deliberations and it remained instrumental in the development and finalization of
humanitarian response plan (HRP 2015) and contributed to the development of contingency
plan.
In view of dynamic context of evolving conflict in the center and south and the need for
expansion of health cluster activities to the conflict affected areas and in order to ensure closer
coordination with the Federal Ministry of Health, the cluster held its first coordination meeting
in Baghdad on June 1st 2015 attended by the leadership of ministry of health and major health
partners. This will be followed up by regular monthly health cluster meetings in Baghdad.
Within the cluster partners, the medical referral WG is at the last stage of finalizing the project
as they are collecting all the contact information for the referral resources available.

HEALTH CLUSTER COORDIANTOR 12
Stock of Essential Medicines and Available (WHO) No Description Unit form Erbil Total Stock
29/6/2015 Sulaymaniyah Total Stock
29/6/2015
Dahuk Total Stock 29/6/2015
1 IDDK (Diarrhoeal Support Module)
Kit 21.00 Kits 4.00 Kits
2 IDDK (Diarrhoeal Basic Module)
Kit 22.00 Kits 22.00 Kits 1.00 Kits
3 IDDK (Diarrhoeal Infusion Module)
Kit 17.00 Kits
4 IDDK (Diarrhoeal ORS Module)
Kit 23.00 Kits 5.00 Kits
5 IEHK BASIC (Medicines) Kit 125.00 Kits 80.00 Kits 30.00 Kits
6 IEHK SUPPLEM.UNIT (Boxes 1 to 30)
Kit 10.00Kits 2.00 Kits
7 NSTITUTION KIT WITH 4 FILTERS
12.00 KITS 12.00 Kits
8 TRAUMA KIT A Kit 6.00Kits 1.00 Kits
9 TRAUMA Kit B (Support for Kit A)
Kit 11.00Kits 3.00 Kits
10 ALUMINIUM HYDROXIDE tab 34,600.00Tablet Oral
11 SALBUTAMOL tab 481000 Tablet Oral 4 mg
12 SALBUTAMOL Aerosol 3,760.00 Aerosol Inhalation Aerosol Inhalation 0.5% in 20 ml
13 SALBUTAMOL Aerosol 5,880.00Aerosol Inhalation 100 mcg
14 ATENOLOL tab 2,277,000.00Tablet Oral 50 mg
15 ATENOLOL tab 2,188,000.00Tablet Oral 100 mg
16 CAPTOPRIL tab 1,493,480.00Scored Tablet Oral 25 mg
17 DIGOXIN tab 88,700.00Tablet Oral 250 μg
18 GLIBENCLAMIDE tab 4,212,500.00Tablet Oral 5 mg
19 OXYTOCIN Injection 3,000.00 Ampoule Injection 10 IU in 1-ml
20 ADHESIVE TAPE->Silkplast adhesive tape
SURGICAL SUPPLIES 9,500.00Units 10,000.00Units
21 BANDAGE crepe SURGICAL SUPPLIES 18,440.00 Units
22 Zinc Oxide Tape SURGICAL SUPPLIES 11,252.00 Units
HEALTH CLUSTER COORDIANTOR 13
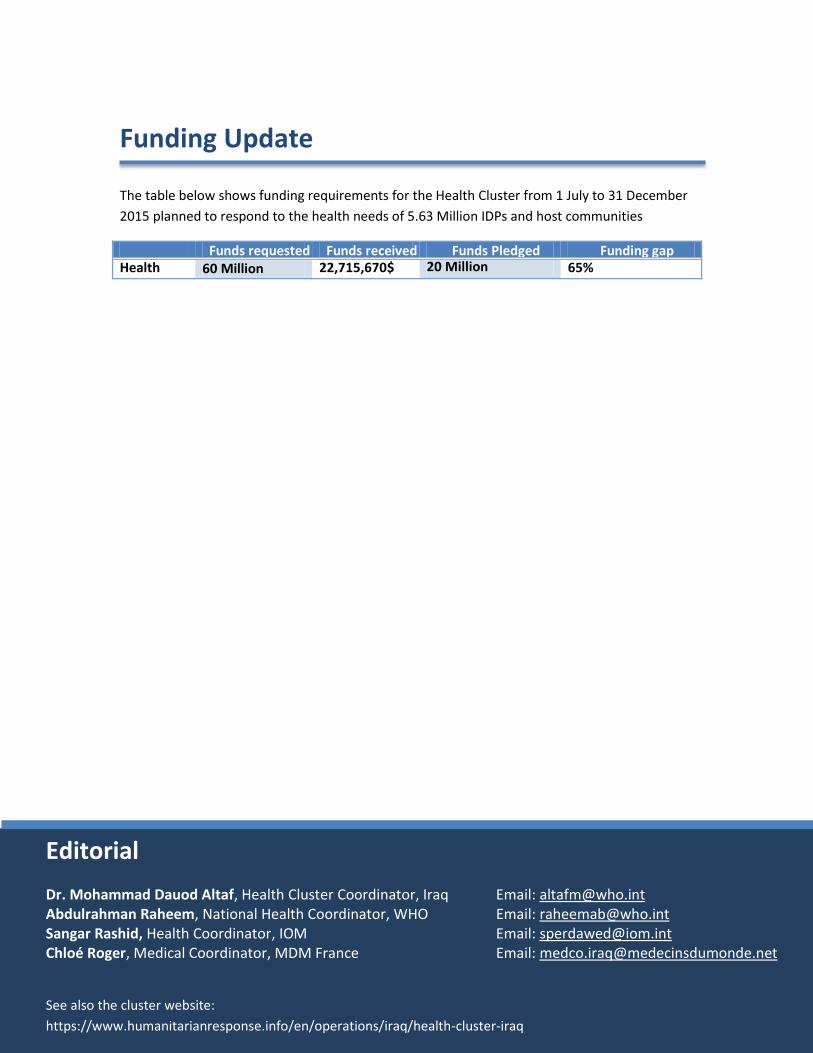
Funding Update
The table below shows funding requirements for the Health Cluster from 1 July to 31 December
2015 planned to respond to the health needs of 5.63 Million IDPs and host communities
Funds requested Funds received FundFunds
Funds Pledged Funding gap Health
Cluster 60 Million 22,715,670$
Million
Editorial
See also the cluster website:
https://www.humanitarianresponse.info/en/operations/iraq/health-cluster-iraq
Dr. Mohammad Dauod Altaf, Health Cluster Coordinator, Iraq Email: [email protected] Abdulrahman Raheem, National Health Coordinator, WHO Email: [email protected] Sangar Rashid, Health Coordinator, IOM Email: [email protected] Chloé Roger, Medical Coordinator, MDM France Email: [email protected]
20 Million 65%