
Interceptive management of oral habit-related · Arcari SR, Biagi R. ORAL HABITS-Evidence...
70
Interceptive management of oral habit-related malocclusions Arcari SR, Biagi R
Transcript of Interceptive management of oral habit-related · Arcari SR, Biagi R. ORAL HABITS-Evidence...

Interceptive management of oral habit-related
malocclusionsArcari SR, Biagi R
ORALHABITS
-Evidence based-
ORAL HABITS• Guidance of the developing dentition and
occlusion is an important role of the pediatric dentist and starts from the child's first visit.
• A right understanding of common oral habits and the impact of these upon craniofacial development ensures anticipatory guidance, timely diagnosis, and appropriate management.
• This leads to the greatest chance of developing a healthy and esthetic dentition in adulthood.
Silva M, Manton D. Oral habits – Part 2: beyond nutritive and non nutritive
sucking. J Dent Child 2014; 81(3): 140-46.
ORAL HABITS
Oral habit behaviors include, among others:
• digit sucking
• pacifier sucking
• mouth breathing
• lip sucking and biting
• tongue thrust
• bruxism
• self-injurious behavior
ORAL HABITS: SUCTION
ORAL HABITS: SUCTION
• Two main types of sucking have been described: nutritive (NS) and non-nutritive (NNS). The former is related to the process of obtaining nutrition, the latter is a habit which may involve sucking of objects (pacifiers and digits are the most common).
Harding C. An evaluation of the benefits of non-nutritive sucking for premature infants as described in the literature. Arch Dis Child 2009; 94: 636-40
ORAL HABITS: SUCTION• NN sucking behaviors have been used by
humans for thousands of years.
• It is a self-soothing action that occurs in 70-80% of infants in western countries asit may:
a) Soothe infants and young children
b) Assist with transitioning to sleep
c) Provide comfort during stressfulepisodes
d) Alleviate the discomfort of teethingLevine RS. Briefing paper: oral aspects of dummy and digit
sucking. Br Dent J 1999; 186(3): 108.
NUTRITIVE SUCTION• Concerning NUTRITIVE SUCKING,
there is some evidence that breast-feeding is likely to lead to lower rates of malocclusion than bottle-feeding, due to the different patterns of muscle activity between the 2 forms of feeding.
Romero CC, Scavone JH, Garib DG, Cotrim Ferreira FA, Ferreira FI. Breast-feeding and NNS patterns related to the prevalence of anterior open bite in primary dentition. J Appl Oral Sci 2011; 19: 161-68.
NUTRITIVE SUCTION• The lack of a continuous flow of milk
during breast-feeding places higher demands on the infant's orofacial muscle development and growth of the mandible. The action of the infant's mouth during breast-feeding is a squeeze of the mother's nipple, compared to a pistol-like action of the tongue during sucking of the nursing bottle teat.
Viggiano D, Fasano D, Monaco G, Strohmenger L. Breast feeding, bottle feeding, and non nutritive sucking: effects on occlusion in deciduous dentition. Arch Dis Child 2004; 89: 1121-23.
NUTRITIVE SUCTIONIn addition the nipple of mother's breast is positioned more anteriorly in the child's mouth compared to the teat of the nursing bottle which is directed back toward the pharyngeal wall, displacing the tongue anteriorly. These factors may lead to the development of irregular swallowing patterns such as tongue thrust which can contribute to malocclusion. Silva M, Manton D. Oral Habits -Part 1: the dental effects and management of nutritive and non-nutritive sucking. J Dent Child 2014; 81(3): 133-39.
MALOCCLUSION
• Recent studies have reportedthat the prevalence of malocclusion appears to be increasing in preschool and school children.
Peres KG et al. Deciduous-dentition malocclusionpredicts orthodontic treatment needs later: findings from a population-based birth cohortstudy. Am J Orthod Dentofacial Orthop 2015; 147(4): 492-498.
Children frequently engage in non-nutritive sucking, atypical swallowing as tongue thrusting, mouth breathing, lip sucking and bruxism. Although such behaviors may be harmless, habits of sufficient duration, frequency, and magnitude may lead to significant changes in craniofacial development, causing orthodontic problems that can compromise function and esthetics. Silva M, Manton D. Oral Habits -Part 1: the dental effectsand management of nutritive and non-nutritive sucking. J Dent Child 2014; 81(3): 133-39.
ORAL HABITS and MALOCCLUSION
MALOCCLUSION
• Malocclusions can be defined as the presence of an anomalousrelationships between the upper and lower teeth of eitherdental and/or alveolar origin. The types of occlusions can be classified as Class I (normal), Class II (distal), Class III (mesial) with or without maxillary contraction. These alterations can be associated to bad habits which, if continuously repeated can lead to anomalies of the orofacial musculature.
Saccomanno S et al. Patients treated with orthodontic-myofunctional therapeuticprotocol. Eur J Paediatr Dent 2012; 13(3): 241-244.

NNS AND MALOCCLUSION
• The etiology of malocclusions is related to the interaction of HEREDITARY AND ENVIRONMENTAL VARIABLES, including stimuli -as the habits- during the formation and development of orofacial structures.
Heimer MV, Tornisiello Katz CR, Rosenblatt A. Non-nutritive sucking habits, dental malocclusions and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod2008; 30: 580-84.
NNS AND MALOCCLUSION
• It is important to investigate the relashionship between the presence of NNS and development of malocclusion in the deciduous dentition because it is a public dental healthproblem in young children and may affect their quality of life. Prolonged periods of NNS may lead to imbalance in the orofacial structures and these disorders could affect the child’sphysical, social and psychological wellbeing.
Lopes Freire GM et al. Non-nutritive sucking habits and their effects on the occlusion
in the deciduous dentition in children. Eur J Paediatr Dent 2016; 17(4): 301-306.
ORAL HABITS: NN SUCTION• The development of malocclusion can be
avoided through measures of NNS. Interruption of NNS as early as possible is a very important measure to prevent malocclusions. It is essential to promote efforts and health promotion policies to reduce the frequency of oral habits and malocclusions in children.
Lopes Freire GM et al. Non-nutritive sucking habits and theireffects on the occlusion in the deciduous dentition in children. Eur J Paediatr Dent 2016; 17(4): 301-306.
ORAL HABITS: NN SUCTION
• The prevalence of NNS in children aged 3 years or more has been estimated between 40% and 76.1%.
Fernandes IB et al. NNS habits after 3 years of age. J IndianSoc Pedod Prev Dent 2015; 33(3): 19-24.

ORAL HABITS: NN SUCTION
• After two or three years of age the adverse effects of sucking habits can manifest themselves; therefore the transversal, the vertical and the sagittal occlusal relations should be evaluated at these ages and proper treatment must begin at this stage.
Gois EG, Vale MP, Paiva SM, Abreu MH, Serra-Negra JM, PordeusIA. Incidence of malocclusionbetween primary and mixed dentitions among Brazilian children: a 5-year longitudinal study. Angle Orthod 2012; 82: 495-500.
ORAL HABITS: NN SUCTION
• The frequency of dental visits influenced the relationship between maternal education and the age of pacifier withdrawal: dental visits considerably shortened pacifier use among children with low and medium-educated mothers.
Pérez- Surez V, Carrillo-Diaz M, Crego A, Romero M. Maternal education, dentalvisits and age of pacifier withdrawal: pediatric dentist role in malocclusionprevention. Clin Pediatr Dent 2013; 37(3): 315-319.
ORAL HABIT: NN SUCTION• Pediatric dentists play a critical role in the
correction of unhealthy oral habits such as prolonged pacifier use. The educational component of pediatric dentist could reverse the lack of knowledge or misinformation among high-risk groups (low maternal education). As consequence, children should start dental visits at an early age and with high frequency.
Pérez- Surez V, Carrillo-Diaz M, Crego A, Romero M. Maternaleducation, dental visits and age of pacifier withdrawal: pediatricdentist role in malocclusion prevention. Clin Pediatr Dent 2013; 37(3): 315-319.
• Of great concern is the influence of NNS on the mixed and particularly on the permanent dentitions. NNS for more than 36 months was found to significantly increase the risk of malocclusion.
Warren JJ, Slayton RL, Bishara SE et al. Effects of nonnutritive sucking habits on occlusal characteristics in the mixed dentition. Pediatr Dent 2005; 27: 445-50.
ORAL HABITS AND MALOCCLUSION

• Children with NNS had 2.55 times an increased risk of malocclusion compared to those without NNS habits. Children with a history of finger sucking had specifically 4.25 times increased risk of malocclusion.
Lopes Freire GM et al. Non-nutritive sucking habits and their effects on the occlusion in the deciduous dentitionin children. Eur J Paediatr Dent 2016; 17(4): 301-306.
ORAL HABITS and MALOCCLUSION

The effects on the development of the dentofacial structures with the persistence of NNS depend on:
• Frequency and duration of the habit
• Intensity of the sucking habit
• Relationship of the dental arches
• Child’s physical health
• Direction of the force exherted by the finger Jyoti S, Pavanalakshmi GP. Nutritive and NNS habits effect on the developing oro-facial complex; a review. Dentistry 2014: 4:203.
ORAL HABITS AND MALOCCLUSION
The dental manifestations of NNS include:
• anterior open bite
• posterior crossbite
• increased overjet
• high risk of developing Class II malocclusion
Silva M, Manton D. Oral Habits -Part 1: the dental effectsand management of nutritive and non-nutritive sucking. J Dent Child 2014; 81(3): 133-39.
ORAL HABITS AND MALOCCLUSION
ORAL HABITS AND MALOCCLUSION• Although the genetic pattern of facial
growth that has to be considered, ANTERIOR OPEN BITE is the occlusalanomaly most commonly associatedwith dysfunctional habits: a persistentperiod of oral habits could haveimplications in the genesis of thismalocclusion.
Urzal V, Braga AC, Ferreira AP. Oral habits as risk factors for anterior open bite in the deciduous and mixed dentitioncross-sectional-study. Eur J Paed Dent 2013; 4: 299- 302.
Pacifier and digit sucking have been shown to alter dental development differently:1. Extended pacifier use has been associated with anterior open bite, Class II molar relationship. The anterior bite is usually symmetrical, due to the shape of pacifier which pushes the maxillary four incisors together as a block.Bell RA, Dean JA, McDonald RE, Avery DR. Managing the developing occlusion. Dentistry for the child and adolescent. 9°ed.St.Louis, Mosby Elsevier; 2011: 572-8.
ORAL HABITS: NN SUCTION
2. Digit sucking may manifest in anterior open bite and increased overjet. The open bite here is often asymmetric as dictated by the position of the digit in the mouth, with the upper incisors proclinedand spaced. Bell RA, Dean JA, McDonald RE, Avery DR. Managingthe developing occlusion. Dentistry for the child and adolescent. 9°ed.St.Louis, Mosby Elsevier; 2011: 572-8.
ORAL HABITS: NN SUCTION
ORAL HABITS • The malocclusion resulting from NNS
improves after cessation of the habit, although this process is dependent on various factors, including growth pattern, duration of the habit, and the presence of other oral habits such as tongue thrust (atypical deglutition).
Heimer MV. Tornisiello Katz CR, Rosenblatt A. Nonnutritivesucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod 2008; 30: 580-585.
ORAL HABITS: NN SUCTION
• Creating a positive environmentaround the child and receiving goodcooperation from the family are twoessential factors to help the childovercome the habit.
Yoshida Y, Ohno T, Shikano R. An approach to digit-suckingcases: some ideas in giving instructions. Int J OrofacialMyology 1991; 17(1): 5-9
ORAL HABITS: NN SUCTION
• In cooperative children who express a willingness to cease the habit digit sucking but require additional assistance, either prevention therapy and appliance therapy may be successful.
Al-Emran DS, Al-Jobbair DA. An assessment of a new reminder therapy technique for ceasing digit sucking habits in children. J Clin Paediatr
Dent 2006;30: 35-8.
ORAL HABITS: PREVENTION• Prevention therapy is aimed at either
physically preventing children from placing their fingers in their mouth or providing an unpleasant taste that discourages children from engaging in the habit. Products such as thumb guards, bandages, gloves and bitter-tasting medicaments have been found to be effective in ceasing both daytime and nocturnal digit sucking.
Silva M, Manton D. Oral Habits -Part 1: the dental effects and management of nutritive and non-nutritive sucking. J Dent Child 2014; 81(3): 133-39.
ORAL HABITSBeing relatively easy to use and inexpensive, they are recommended as an alternative when reward and positive reinforcement have failed to curb a NNS habit. However children often ignore these reminders or remove them, which limits their effectiveness: appliance therapy may be a possible solution.Silva M, Manton D. Oral Habits -Part 1: the dental effects and management of nutritive and non-nutritive sucking. J DentChild 2014; 81(3): 133-39.
ORAL HABITS
Cooperation among pediatric dentists, pediatricians and orthodontists is essential to intercept behaviors which would lead to unbalanced sequelae should they not be corrected at an early stage.Silva M, Manton D. Oral Habits -Part 1: the dentaleffects and management of nutritive and non-nutritive sucking. J Dent Child 2014; 81(3): 133-39.

DEGLUTITION

DEGLUTITIONThe investigation of tongue function is an important part of oral diagnosis. Many studies have demonstrated that tongue thrust plays an important role in the etiology of open bite as well as in the relapse of treated open bite patients. It is therefore important to identify patients with abnormal swallowing patterns.Peng CL, Jost-Brinkmann PG, Yoshida N, Miethke RR, Lin CT. Differential diagnosis between infantile and mature swallowing with ultrasonography. Eur Journal Orth 2003; 25: 451-456.

DEGLUTITIONAlteration of the tongue pressure:
• Macroglossia
• Enlarge tonsils
• Enlarged adenoids
• Ankiloglossia (short lingual frenulum)
• Oral habits as thumb sucking and certain types of artificial nipples used in feeding infants
• Oral breathing
• Hereditary factors
• Postural alteration of the tongue and mandible
• Postural alteration of head and body
DEGLUTITION
• The act of swallowing seems simple. It is something we do unconsciously; however the successful execution of a swallow requires the intricate coordination between several cranial nerves and 30 to 40 muscles of the face, mouth, pharynx and esophagus.
Bronwyn J. Normal and abnormal swallowing. Second Edition. Springer Science, New York 2003.
DEGLUTITION• In infancy the tongue is positioned
anteriorly between the gum pads and rests on the lower lip to facilitate sucking in a swallow pattern described as "infantile swallowing". This swallow pattern involves contraction of the muscles of the lip.
Delaney AL, Arvedson JC. Development of swallowing and feeding: prenatal through first year of life. Dev Disabil Res Rev 2008; 14: 105-117.
DEGLUTITION• By 2 to 4 years of age, with the eruption
of the primary molars and transition to cup feeding, children start to adopt an "adult swallow pattern". This is characterized by:
1. Relaxed perioral musculature
2. Contact of posterior teeth
3. Positioning of the tongue against the alveolar process behind the maxillary incisors during swallowing

SOMATIC AND VISCERAL DEGLUTITION
DEGLUTITIONIn patients with anterior open bite, as it often occurs in children using pacifiers, it is difficult to obtain closure of the mouth to prevent spilling of fluids during swallowing; the position of the tongue between the arches represent a physiological adaptation with the purpose to restore the anterior seal. Almost every patient with anterior open bite is affected by this type of deglutition, but the contrary is not necessarily true.Proffit WR. The etiology and development of orthodontic problems. In: Proffit WR, Fields HW Jr, Sarver DM, eds. Contemporary Orthodontics 4th ed. St. Louis, Mo: Mosby; 2007: 130-161.
DEGLUTITION
Observation of tongue movements during swallowing with the lips apart is the simplest clinical method for diagnosing visceral swallowing.Peng CL, Jost-Brinkmann PG, Yoshida N, MiethkeRR, Lin CT. Differential diagnosis between infantile and mature swallowing with ultrasonography. Eur Journal Orth 2003; 25: 451-456.
Management of concurrent habits, such as NNS and mouth breathing may also lead to resolution of tongue thrusting. Silva M, Manton D. Oral habits – Part 2: beyond nutritive and non nutritive sucking. J Dent Child 2014; 81(3): 140-46.
DEGLUTITION
ORAL BREATHING
ORAL BREATHING
Mouth breathing is a parafunctional habit whereby air passes through the mouth either entirely or partially rather than the nose.Silva M, Manton D. Oral habits – Part 2: beyond nutritive and non nutritive sucking. J Dent Child 2014; 81(3): 140-46.

ORAL BREATHING• Congenital causes
a) Choanal atresia
b) Nasal atresia
c) Nasal septum deviations
• Acquired causes
a) Adenotonsillar hypertrophy
b) Allergic conditions
c) Asthma
d) Nasal polyposis
e) Benign and malignant neoplasms

ORAL BREATHING
The prevalence of mouth breathing among children reduces with age, being more common in younger children. There is a strong association between mouth breathing and malocclusion.Gois EG, Ribeiro Junior HC, Vale MPP. Influence of NNS, breathing pattern and adenoid size on the development of malocclusion. Angle Orthod 2008; 78: 647-54.
ORAL BREATHING
Mouth breathing and dummy use were associated with a reduction in the intercanine distance in the maxillary arch. Mouth breathing in particular causes a reduction in the size of both arches width. Aznar T, Galan AF, Marin I, Dominguez A. Dental arch diameters and relationships to oral habits. Angle Orthod 2006; 76(3): 441-445.
ORAL BREATHINGThe reduction of transverse diameters in the upper maxilla seems to be related to pathological oral breathing by which some young patients are affected, due either to a real nasopharyngeal obstruction (forced oral breathing) or bad habit. The upper arch shows reduction given the scares use of nasal airways and pressure imbalance between muscular power of cheeks and lips, and the inner muscles of the tongue, which is low and protruding.Cossellu G, Farronato G, Nicotera O, Biagi R. Transverse maxillary deficit and its influence on the cervical vertebrae maturation index. Eur J Paediatr 2016; 17(2): 147-150.
ORAL BREATHINGOral breathing affects also the cranio-cervical posture since in order to increase patency of the oropharyngeal airways a patient with nasal obstruction assumes a posture which entails overextension of the cranio-cervical complex to obtain proper ventilation. Cossellu G, Farronato G, Nicotera O, Biagi R. Transverse maxillary deficit and its influence on the cervical vertebrae maturation index. Eur J Paediatr 2016; 17(2): 147-150.
ORAL BREATHING• Mouth breathing results in aberrant
positioning of the mandible, which is rotated downward and posteriorly, and of the tongue, which is positioned downward to enable the flow of air through the oral cavity.
• In these subjects the nostrils may be narrowed and the lips incompetent, with the upper lip hypotonic.
Giuca M, Pasini M, Galli V, Casani A, Marchetti E, MarzoG. Correlations between transversal discrepancies of the upper maxilla and oral breathing. Eur J Paediatr Dent 2009; 10: 23-28.
ORAL BREATHINGIn a growing child these changes manifest as distinctcraniofacial features (facies adenoidea) including:
• mandibular retrusion –skeletal Class II
• increased anterior facial height
• Increased overjet
• maxillary transverse deficiency
• unilateral or bilateral crossbite
• dentoalveolar anterior open bite Giuca M, Pasini M, Galli V, Casani A, Marchetti E, Marzo G. Correlations between transversal discrepancies of the upper maxilla and oral breathing. EurJ Paediatr Dent 2009; 10: 23-28.

ORAL BREATHINGImprovement of the skeletal structures (i.e. resolution of crossbite) must not necessarilymean the clinical success of the condition of oral breathers. Therefore the application of a targeted myofunctional treatment is alsoadvisable to enable the young patient to electively breath again through his/her nose.Giuca M, Pasini M, Galli V, Casani A, Marchetti E, Marzo G. Correlations between transversal discrepancies of the upper maxilla and oral breathing. Eur J Paediatr Dent 2009; 10: 23-28.
LIP SUCTION
LIP SUCTION
Lip-sucking most commonly involves the lower lip and is characterized by excessive activity of the mentalis muscle, leading to contraction of the symphyseal tissues.
LIP SUCTIONThe habit of lip sucking mostcommonly involves the lower lip and ismore often an adaptive response to increased overjet but may exacerbatethe underlying sagittal discrepancy by proclining the upper incisors and retroclining the lower incisors.Silva M, Manton D. Oral habits – Part 2: beyond nutritive and non nutritive sucking. J Dent Child 2014; 81(3): 140-46.
ORAL HABITSSUMMARY
• Oral habit behaviors include, among others, digit sucking, pacifier sucking, lip sucking, mouth breathing, and tongue thrust.
• Because persistent nonnutritive sucking habits may result in long-term problems, professional evaluation has been recommended for children beyond the age of 3 years, with subsequent intervention to cease the habit if indicated.
American Academy of Pediatric Dentistry. Policy on oral habits. Reference Manual 2015/16
FUNCTIONALREMOVABLE
DEVICES
REMOVABLE APPLIANCES
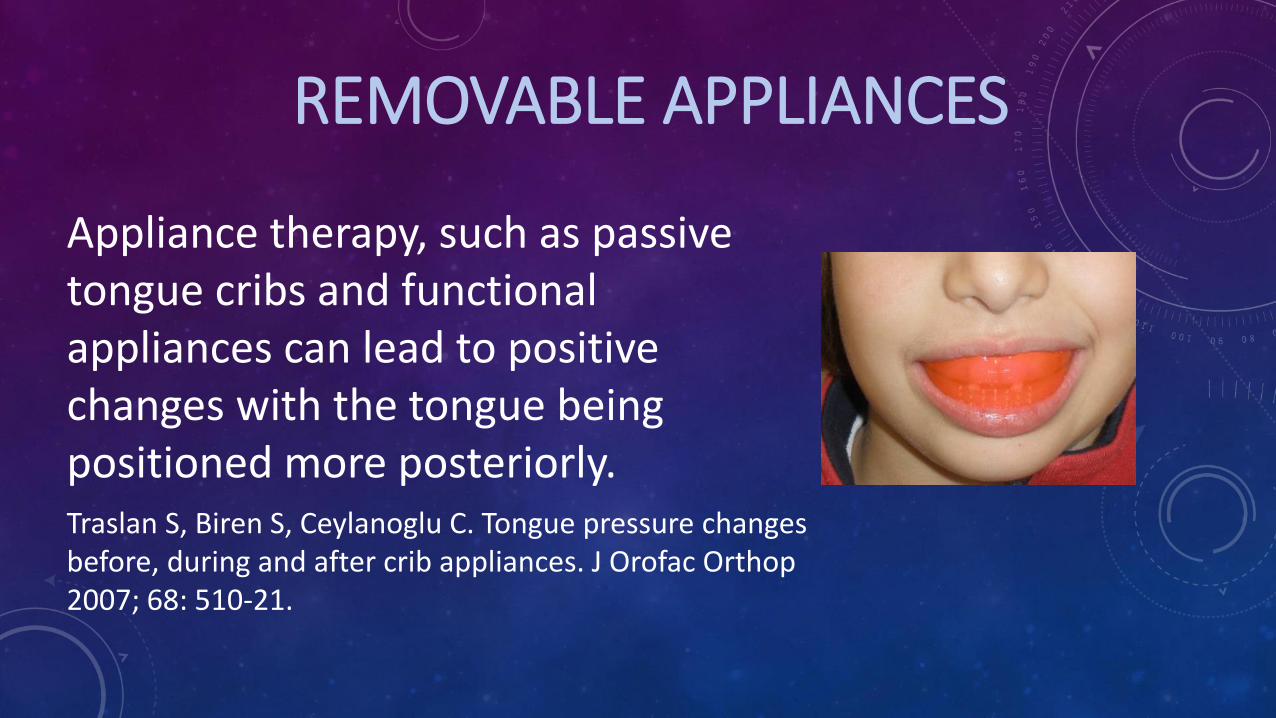
Appliance therapy, such as passive tongue cribs and functionalappliances can lead to positive changes with the tongue beingpositioned more posteriorly.Traslan S, Biren S, Ceylanoglu C. Tongue pressure changesbefore, during and after crib appliances. J Orofac Orthop2007; 68: 510-21.
MYOFUNCTIONAL APPLIANCES
Myofunctional removable appliances used in pediatric age aim to prevent and intercept dental and skeletal malocclusions in primary and mixed dentition.Condò R, Costacurta M, Perugia C, Docimo R. Atypicaldeglutition: diagnosis and interceptive treatment. A clinicalstudy. Eur J Paediatr Dent 2012; 13: 209-214.
The first myofunctional removable appliances were conceived by Bergersen in 1987 in order to:
- Prevent or correct the consequences of an anomalous tongue thrust
- Intercept the occurrence and persistence of the open bite
- Reeducate and correct the majority of bad habits
Bergersen EO. Preventive and interceptive orthodontics in the mixeddentition with the myofunctional eruption guidance appliance: correction of overbite and overjet. J Pedod 1988; 12(3): 386-414.
MYOFUNCTIONAL APPLIANCES

MYOFUNCTIONAL APPLIANCESDuring the last decades, better functional appliances have been developed and have been reported to produce significant changes in oral function as well as to stimulate mandibular growth. Idris G, Hajeer MY, Al-Jundi A. Acceptance and discomfort in growing patients during treatment with two functional appliances: a randomised controlledtrial. Eur J Paediatr Dent 2012; 13(3): 219-224.
The corrections expected by means of functional devices are more easily achievable in mixed dentition, because the skeletal and dentoalveolarstructures are still in full change, but the pubertal peak is still far away. Arcari SR, Biagi R. Oral habits and induced occlusal-skeletaldisarmonies. J Plastic Dermat 2015; 11(1): 73-78.
MYOFUNCTIONAL APPLIANCES
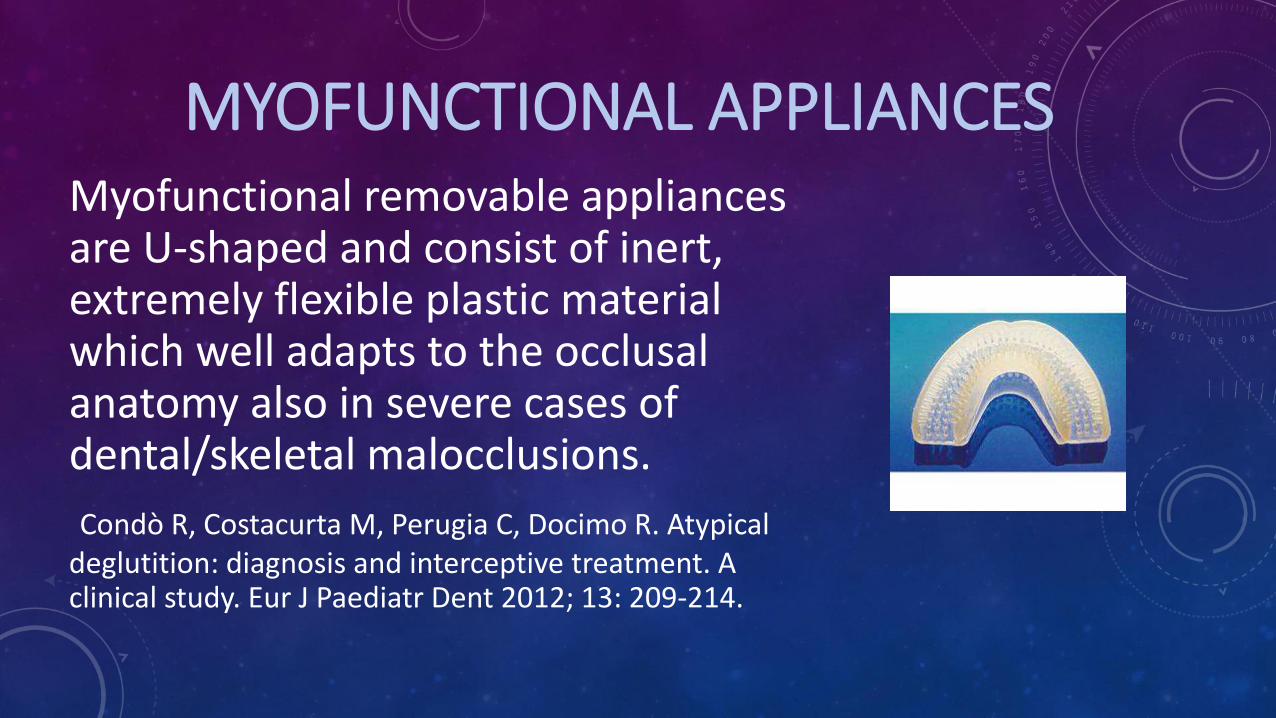
MYOFUNCTIONAL APPLIANCESMyofunctional removable appliances are U-shaped and consist of inert, extremely flexible plastic material which well adapts to the occlusal anatomy also in severe cases of dental/skeletal malocclusions.
Condò R, Costacurta M, Perugia C, Docimo R. Atypicaldeglutition: diagnosis and interceptive treatment. A clinical study. Eur J Paediatr Dent 2012; 13: 209-214.

MYOFUNCTIONAL APPLIANCESThe material is a polyurethane. Prefabricated functional appliances are claimed to be easy to use and to correct malocclusions at an early age by acting on muscular dysfunction while repositioning the mandible. Das UM, Reddy D. Treatment effects produced by preorthodontic trainer appliance in patients with Class II division I malocclusion. J Indian Soc Pedod Prev Dent2010; 28(1): 30-33.
MYOFUNCTIONAL APPLIANCES
The construction bite, in sagittal terms, is based on an incisor-to-incisor ratio, which is important to correct the marked overjet.
Condò R, Costacurta M, Perugia C, Docimo R. Atypical
deglutition: diagnosis and interceptive treatment. A clinicalstudy. Eur J Paediatr Dent 2012; 13: 209-214.
MYOFUNCTIONAL APPLIANCES
Teeth sensitivity is mainly located at the upper incisors, because of the elasticity of the appliance; it is a very common consequence of wearing functional appliances. Sergl HG, Klages U, Zentner A. Functional and social discomfort during orthodontic treatment: effects on compliance and prediction of patients adaptation by personality variables. Eur J Orthod 2000; 22: 307-315.

MYOFUNCTIONAL APPLIANCES
Clinicians might improve acceptance by selecting an appliance design which would allow comfortable wear and facilitate adaptation to the appliance.Idris G, Hajeer MY, Al-Jundi A. Acceptance and discomfort in growing patients during treatment with two functionalappliances: a randomised controlled trial. Eur J PaediatrDent 2012; 13(3): 219-224.

e
MOTIVATION
CLINICALCASES















![Assessment of Parafunctional Oral Habits among a Sample of ...spc.kau.edu.sa/Files/320/Researches/52125_22257.pdf · oral habits and occlusal abnormalities[1]. Oral habits include,](https://static.fdocuments.in/doc/165x107/5ffd691e53cc544e164cc7bf/assessment-of-parafunctional-oral-habits-among-a-sample-of-spckauedusafiles320researches5212522257pdf.jpg)


