inflammatory bowel disease (IBD)
55
Ghali Abduljalil Abubakar
-
Upload
abubakar-ghali-abduljalil -
Category
Health & Medicine
-
view
85 -
download
5
Transcript of inflammatory bowel disease (IBD)
Slide 1
Ghali Abduljalil Abubakar
IntroductionInflammatory bowel disease or IBD is a chronic, relapsing inflammation of bowel possibly due to abnormal immune response to enteric flora.The two major forms of IBD are recognized as:-Crohns disease (CD) which affect any part of the GI tract from gum to bum.Ulcerative colitis (UC) which affect only the colon.
There is a degree of overlap between these two conditions, in there clinical features, histological and radiological abnormalities. In 10% of cases of IBD causing colitis a definitive diagnosis is either UC or CD is not possible and the diagnosis is term as colitis of undetermined type and etiology (CUTE). Its clinical useful to distinguished between these two conditions because of differences in their management, although in reality they may represent two aspect of the same disease.
Epidemiology The incidence and prevalence of IBD are highest in westernized nations, the incidence of CD varies from country to country but is approximately 4-10 per 100000 annually with the prevalence 25-100 per 100000.The incidence of UC is stable at 6-15/10000 annually with a prevalence of 80-150/100000. The disease is more prevalent in the west, particularly Caucasian and eastern European Jews.
EtiologyGenetic factors Smoking NSAIDsHygieneNutritional factors Appendectomy The intestinal microbiota The intestinal immune system
CROHNSCrohns disease is a chronic inflammatory condition that affect any part of the GI tract from mouth to anus but has the tendency to affect the ileum and ascending colon (ileocolonic disease).The disease can involve one small areas with relatively normal bowel in between (skip lesion). It may also involve the whole of the colon (total colitis) sometimes without macroscopic small bowel involvement.
Macroscopic features of CDThe involved bowel is usually thickened and is narrowed. Deep ulcers and fissures in mucosa produce a cobblestones appearance. Fistula and abscesses maybe seen which reflect penetrating disease.
An early features is aphthoid ulceration, usually seen at colonoscopy; later larger and deeper ulcers appears in a patchy distribution again producing a cobblestone appearance.
Microscopic features of CDThe earliest lesions are aphthoid ulceration and focal crypt abscesses with loose aggregations of macrophages, which form non-caseating granulomas in all layers of the bowel wall. Granulomas can be seen in lymph node, mesentery, peritoneum, liver and pancreas. Although granulomas are a pathognomic features of CD, there are rarely found on mucosal biopsies.
Sign and Symptoms of CDMAJOR SYMPTOMS:-Watery DiarrheaAbdominal painWeight loss CONSTITUTIONAL SYMPTOMS:-Malaise, lethargy, anorexia, nausea, vomiting, and low great fever maybe present and 15% no gastrointestinal symptoms.
DiagnosisHow can you diagnose CD?:-
History and Examination Presenting complain:- insidious or acutely abdominal pain. Non-bloody Diarrhea but sometimes it maybe bloody and Steatorrhea systemic review is very important because of extra GI manifestations
Family history is important because of genetic predisposition. Drug and social history due to NSAIDs and smoking which is said to exacerbate CD.
Examination:-Loss of weight and sign of malnutrition. aphthous ulcer in the mouth is often seen.
Abdominal examination:- Maybe normal or shows tenderness and or right iliac fossa mass are occasionally found.The anus should be examined to look for edematous anal tags, fissures or perianal abscesses.And the presence of extra GI features should not be forgotten.
InvestigationsComplete blood count (CBC):- for the presence of anemia either normocytic normochronic anemia of chronic diseases. However iron deficiency and or folate also occur.Erythrocyte sedimentation rate (ESR) & C-reactive protein (CRP) may raised, white cells & platelets count is also high.Hypoalbuminemia is present in severe disease or as part of an acute phase response to inflammation associated with raised CRP.
Liver function test (LFT)Blood culture for suspected septicemia Serologic test:- anti-saccharomyces cerevisiae antibodies (ASCA) often positive.Stool culture for C. difficile toxin assay should always be performed if diarrhea is present.
Endoscopy & radiological imagingColonoscopy/sigmoidoscopy in patient with severe disease.Upper GI endoscopy to exclude esophageal & gastroduedenal involvement.Small bowel imaging is mandatory in patient with CDPerianal MRI or endoanal ultrasound. Capsule endoscopy in CD with normal radiological findings. Radionuclide scan.
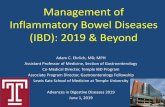
MRI shows linear fluid-filled perianal fistula in the right ischioanal fossa
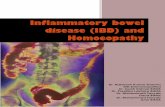
Capsule endoscopy show ulceration & narrowing of the intestinal lumen
Complications of CDMalaborptionPeritonitis Intestinal obstruction in 40%Massive hemorrhage Skin tags Ischiorectal abscess Anorectal Fistula
Medical Management The aim of management is to induce and maintain clinical remission & achieve mucosal healing to prevent complications.Stop smoking Induction of remission:- oral or I.V glucocortic0steriods (e.g. 6 mercaptorine, methotrexate) and TNF antibodies (e.g. infliximab, adalimumab)
Maintaince of remission:- Azathioprine, 6-MP, methotrexate, mycophenolate, mofitil & TNF antibodies.Perianal disease:- ciprofloxacin, metronidazole, azathioprine & TNF antibodies.
Surgical management of CDApproximately 80% of patient will required surgery at some course of the disease.INDICATION FOR SURGERY ARE:-Failure of medical therapy with acute or chronic symptoms producing ill-health Complications (e.g. toxic dilation, obstructions, perforation, abscesses and enterocutenous fistula)Failure to grow in children despite medical therapy Presence of perianal sepsis
Surgical intervention Colectomy Stricturoplasty Ileorectal anastomosis Panprocolectomy with an end ileostomy (if the whole colon & rectum is involved)
Problems associated with ileostomiesMechanical problem Dehydration particularly if there is a short length of small bowel remaining.Psychosexual problemsErectile dysfunction in men and reduced fueundity in women (due to prior surgery)Recurrence of CD
Ulcerative colitis
Ulcerative colitis UCUlcerative colitis (UC) can affect the rectum alone (proctitis) & can extend to proximally to involved the sigmoid and descending colon (left sided colitis) or may involve the whole colon (extensive colitis). In a few of these patients there is also inflammation of the distal terminal ileum (backwash ileitis).
Macroscopic changes in colitis The mucosa looks reddened, inflamed and bleed easily (friability). In severe disease there is extensive ulceration with the adjacent mucosa appearing as inflammatory (pseudo) polyps.
Microscopic changes in UCThe mucosa shows a chronic inflammatory cells infiltrate in the lamina propria. Crypt abscesses and goblet cell depletion are also seen.
Sign & symptoms of UCBloody Diarrhea with mucus Lower abdominal discomfortMalaiseLethargy Anorexia Weight loss more often in UC than CD
Diagnosis History and examination:-History:- patient usually complain about frequent passage of blood and mucus in his stool with urgency and tenesmus. And frequency of defecation. About 10-20 liquid of stool per day. Diarrhea mainly occurs at night with incontinence and urgency.In system review extra GI symptoms, +/- family history
Examinations In general there are no specific sign in UC but the abdomen maybe slightly distended or tender to palpation.Pyrexia, tachycardia, are sign of severe colitis and require urgent admission. Rectal examination will show presence blood.Rigid sigmoidoscopy is usually abnormal, showing an inflamed, bleeding, friable mucosa.
Sigmoidoscopy
Investigations Complete blood count (CBC):- iron deficiency and raised WBC & platelet.ESR & CRP are often raised Liver function test (LFT)Serologic test:- perinuclear anti-neutrophil cytoplasmic antibodies (pANCA) often positive Stool culture for C.difficile toxin.Colonoscopy with mucosal biopsy is the gold standardX-ray
Pseudopolyps Ulcerative colitis
Complications of UCShort term complication:-Toxic megacolonHemorrhage Perforation Long term complication:-Stricture leading to obstruction Dysplasia leading to cancer.
Medical Management Multidisplinary term Aminosalicyclic acid (5-ASA)(e.g. sulfasalazine, balsaladize & olsalazine)Suppositories and enemas of 5-ASA can be use Oral prednisolone In severe cases admission give I.V hydrocortisone 100mg 6 hourly with subcutaneous low molecular weight heparin to prevent thromboembolism
Salvage therapy To avoid Colectomy is required for patient with CRP>40mg/L or more than eight bowel motions after 3 days of hydrocortisone.Oral cyclosporine 2mg/kg/dayInfliximab 5mg/kg as an Infusion SMOKING?
Surgical Management While the treatment of UC remains primarily medical, surgery continues to have a central role because it maybe life saving is curative and eliminated the long term risk of cancer. Acute disease:- subtotal Colectomy with end ileostomy Severe disease:- proctectomy with permanent ileostomy.
Indications for surgery Fulminate acute attack:- failure of medical therapy Toxic dilation Hemorrhage Imminent perforation Chronic disease:- Incomplete response to medical treatment Dysplasia on surveillance colonoscopy
Differential diagnosis of IBDCauses of infectious diarrhea such as:-Clostridium difficile ,Amoebiasis, Ileocolonic tuberculosis.Others:-Celiac disease Microscopic colitis Lactose intolerance Irritable bowel syndrome (IBS)Functional diarrhea
Behcet disease AIDSColorectal malignancy (e.g. adenocarcinoma and lymphoma)C1 esterase deficiency, hereditary angioedema Ischemic colitis e.t.c
Features that distinguished CD from UCCrohn's gives GIFTS:-GranulomasIleum Fistula and fissure Transmural Skip lesions
Cancer in inflammatory bowel diseasesPatients with UC and extensive Crohns colitis have an increased incidence of developing dysplasia and subsequent colon cancer. The risk of dysplasia is related to the extent and duration of disease as well as the presence of untreated mucosal inflammation.
Pregnancy and inflammatory bowel diseaseWomen with inactive IBD have normal fertility. Fertility, however, may be reduced in those with active disease, and patients with active disease are twice more likely to suffer spontaneous abortion than those with inactive disease.
Listen to your patient he is telling you the diagnosis. Dr. Williams Osler
54
Thank You



![Inflammatory Bowel Disease - BSWHealth.med · Inflammatory Bowel Disease: ... • Infectious colitis: Salmonella, E. coli, ... IBD Path Pitfalls Handout.ppt [Compatibility Mode]](https://static.fdocuments.in/doc/165x107/5cc8e3e088c9937c048b644f/inflammatory-bowel-disease-inflammatory-bowel-disease-infectious.jpg)