Immune complex glomerulonephritis in C4- and C3-deficient mice
11
CELL BIOLOGY - IMMUNOLOGY - PATHOLOGY Immune complex glomerulonephritis in C4- and C3-deficient mice RICHARD J. QUIGG,ALICE LIM,MARK HAAS,JESSY J. ALEXANDER,CHUN HE, and MICHAEL C. CARROLL Departments of Medicine and Pathology, The University of Chicago, Chicago, Illinois, and Department of Pathology, Harvard Medical School, Boston, Massachusetts, USA Immune complex glomerulonephritis in C4- and C3-deficient mice. In this study, we examined the roles of C4 and C3 in immune complex glomerulonephritis by actively immunizing C4-deficient (C4 2/2), C3 deficient (C3 2/2) and wild-type mice with apoferritin. Wild-type animals with an intact complement system produced anti-apoferritin IgG and IgM antibodies, and developed mesangial proliferative glomerulonephritis characterized by hypercellularity, matrix expansion, deposition of IgG, IgM, IgA and C3, and the presence of electron dense deposits. In the majority of animals, the peripheral capillaries also contained IgG, C3 and subendothelial and subepithelial electron dense deposits. In contrast to wild-type animals, all apoferritin-immunized C4 2/2 and C3 2/2 mice had serum cryoprecipitates containing polyclonal IgM and the variable presence of polyclonal IgG. These animals also developed immune complex glomerulonephritis, but their disease manifestations were dis- tinctly different from that of their wild-type littermates. In apoferritin- immunized C4 2/2 and C3 2/2 mice, IgG was either absent or present in reduced quantities in glomeruli, yet IgM and IgA were present in greater intensity in glomeruli. Capillary wall IgG deposits were absent in all C4 2/2 and C3 2/2 animals. C4 2/2 animals also had significant glomerular C3 deposition, hypercellularity and neutrophil infiltration, which were not present in C3 2/2 animals. These results illustrate the complex interplay between the effects of complement to process immune complexes and to lead to inflammation and tissue injury. The complement system consists of over 30 plasma and cell- associated proteins. This system is tightly regulated, being con- strained in its activation, as well as being inhibited by a number of regulatory proteins once activation occurs. For the most part, the activation of complement is proinflammatory, leading to recruit- ment and stimulation of neutrophils and monocytes, as well as to direct tissue damage [1, 2]. Furthermore, an intact complement system is necessary for an appropriate and optimal humoral immune response [3– 6]. Since the early studies performed by Kurtz and Donnel [7], and Unanue and Dixon [8], and later studies by Salant and coworkers [9], a considerable amount of research has been performed in experimental glomerular disease models showing that complement activation is pathogenic. By extrapolation to human glomerular diseases in which complement activation products are present in glomeruli, and in some in- stances, systemic complement consumption is apparent, comple- ment is likely to be pathogenic in these disorders. On the other hand, immune complex disease commonly occurs in patients with complete deficiencies of any one of the early classical pathway components, C1 (C1q or C1r/s), C4, or C2 [10, 11]. In some cases, there is an associated immune complex glomerulonephritis, although these tend to be mild [12, 13]. Deficiency of C3, which occupies a central position in both alternative and classical pathways, is typically associated with recurrent pyogenic infections, although glomerulonephritis can occur in such patients [12, 14]. Since the complement system plays an important role in immune complex metabolism [15, 16], it seems likely that patients with early complement protein deficien- cies process immune complexes abnormally [12, 17]. There are animals with inherited complete deficiencies of complement components, such as C4- and C2-deficient guinea pigs, and C3-deficient dogs [18]. Although most of these animals are clinically normal, C3-deficient dogs have been reported to develop membranoproliferative glomerulonephritis [19]. Furthermore, some C2- and C4-deficient guinea pigs have laboratory evidence for immune complex disease, such as the presence of serum rheumatoid factors [20]. To further investigate the role of complement deficiencies in glomerular disease, we have utilized gene targeting in embryonic stem cells to generate mice totally deficient in C4 (C4 2/2) or C3 (C3 2/2) [6, 21]. Save for the complement protein deficiency, unmanipulated C4 2/2 and C3 2/2 animals are phenotypically normal. In this study, we induced immune complex glomerulone- phritis in mice by chronic active immunization with the foreign protein, apoferritin. We show that wild-type, C4 2/2, and C3 2/2 mice have distinct differences in the resultant disease. METHODS Animals and disease protocol Wild-type, C4 2/2, and C3 2/2 mice, all 129SvJ and C57Bl/6 mixed strains, were generated as previously described [6, 21]. All animals were kept in standard, non-pathogen free housing in the University of Chicago Animal Care Facility. Immune complex glomerulonephritis was induced by immunizing 6- to 8-week-old female mice for 10 weeks with a daily intraperitoneal dose of 4 mg horse spleen apoferritin (Sigma Chemical Co., St. Louis, MO, USA), which was dialyzed against phosphate buffered saline (PBS) and sterile filtered. In previous studies, this high dose of Key words: immune complex glomerulonephritis, C3- and C4-deficient mice, inflammation, tissue injury. Received for publication June 9, 1997 and in revised form August 4, 1997 Accepted for publication August 6, 1997 © 1998 by the International Society of Nephrology Kidney International, Vol. 53 (1998), pp. 320 –330 320
Transcript of Immune complex glomerulonephritis in C4- and C3-deficient mice

CELL BIOLOGY - IMMUNOLOGY - PATHOLOGY
Immune complex glomerulonephritis in C4- and C3-deficientmice
RICHARD J. QUIGG, ALICE LIM, MARK HAAS, JESSY J. ALEXANDER, CHUN HE, and MICHAEL C. CARROLL
Departments of Medicine and Pathology, The University of Chicago, Chicago, Illinois, and Department of Pathology, Harvard MedicalSchool, Boston, Massachusetts, USA
Immune complex glomerulonephritis in C4- and C3-deficient mice. Inthis study, we examined the roles of C4 and C3 in immune complexglomerulonephritis by actively immunizing C4-deficient (C4 2/2), C3deficient (C3 2/2) and wild-type mice with apoferritin. Wild-type animalswith an intact complement system produced anti-apoferritin IgG and IgMantibodies, and developed mesangial proliferative glomerulonephritischaracterized by hypercellularity, matrix expansion, deposition of IgG,IgM, IgA and C3, and the presence of electron dense deposits. In themajority of animals, the peripheral capillaries also contained IgG, C3 andsubendothelial and subepithelial electron dense deposits. In contrast towild-type animals, all apoferritin-immunized C4 2/2 and C3 2/2 micehad serum cryoprecipitates containing polyclonal IgM and the variablepresence of polyclonal IgG. These animals also developed immunecomplex glomerulonephritis, but their disease manifestations were dis-tinctly different from that of their wild-type littermates. In apoferritin-immunized C4 2/2 and C3 2/2 mice, IgG was either absent or presentin reduced quantities in glomeruli, yet IgM and IgA were present ingreater intensity in glomeruli. Capillary wall IgG deposits were absent inall C4 2/2 and C3 2/2 animals. C4 2/2 animals also had significantglomerular C3 deposition, hypercellularity and neutrophil infiltration,which were not present in C3 2/2 animals. These results illustrate thecomplex interplay between the effects of complement to process immunecomplexes and to lead to inflammation and tissue injury.
The complement system consists of over 30 plasma and cell-associated proteins. This system is tightly regulated, being con-strained in its activation, as well as being inhibited by a number ofregulatory proteins once activation occurs. For the most part, theactivation of complement is proinflammatory, leading to recruit-ment and stimulation of neutrophils and monocytes, as well as todirect tissue damage [1, 2]. Furthermore, an intact complementsystem is necessary for an appropriate and optimal humoralimmune response [3–6]. Since the early studies performed byKurtz and Donnel [7], and Unanue and Dixon [8], and laterstudies by Salant and coworkers [9], a considerable amount ofresearch has been performed in experimental glomerular diseasemodels showing that complement activation is pathogenic. Byextrapolation to human glomerular diseases in which complement
activation products are present in glomeruli, and in some in-stances, systemic complement consumption is apparent, comple-ment is likely to be pathogenic in these disorders.
On the other hand, immune complex disease commonly occursin patients with complete deficiencies of any one of the earlyclassical pathway components, C1 (C1q or C1r/s), C4, or C2 [10,11]. In some cases, there is an associated immune complexglomerulonephritis, although these tend to be mild [12, 13].Deficiency of C3, which occupies a central position in bothalternative and classical pathways, is typically associated withrecurrent pyogenic infections, although glomerulonephritis canoccur in such patients [12, 14]. Since the complement system playsan important role in immune complex metabolism [15, 16], itseems likely that patients with early complement protein deficien-cies process immune complexes abnormally [12, 17]. There areanimals with inherited complete deficiencies of complementcomponents, such as C4- and C2-deficient guinea pigs, andC3-deficient dogs [18]. Although most of these animals areclinically normal, C3-deficient dogs have been reported to developmembranoproliferative glomerulonephritis [19]. Furthermore,some C2- and C4-deficient guinea pigs have laboratory evidencefor immune complex disease, such as the presence of serumrheumatoid factors [20].
To further investigate the role of complement deficiencies inglomerular disease, we have utilized gene targeting in embryonicstem cells to generate mice totally deficient in C4 (C4 2/2) or C3(C3 2/2) [6, 21]. Save for the complement protein deficiency,unmanipulated C4 2/2 and C3 2/2 animals are phenotypicallynormal. In this study, we induced immune complex glomerulone-phritis in mice by chronic active immunization with the foreignprotein, apoferritin. We show that wild-type, C4 2/2, and C32/2 mice have distinct differences in the resultant disease.
METHODS
Animals and disease protocol
Wild-type, C4 2/2, and C3 2/2 mice, all 129SvJ and C57Bl/6mixed strains, were generated as previously described [6, 21]. Allanimals were kept in standard, non-pathogen free housing in theUniversity of Chicago Animal Care Facility. Immune complexglomerulonephritis was induced by immunizing 6- to 8-week-oldfemale mice for 10 weeks with a daily intraperitoneal dose of 4 mghorse spleen apoferritin (Sigma Chemical Co., St. Louis, MO,USA), which was dialyzed against phosphate buffered saline(PBS) and sterile filtered. In previous studies, this high dose of
Key words: immune complex glomerulonephritis, C3- and C4-deficientmice, inflammation, tissue injury.
Received for publication June 9, 1997and in revised form August 4, 1997Accepted for publication August 6, 1997
© 1998 by the International Society of Nephrology
Kidney International, Vol. 53 (1998), pp. 320–330
320

antigen led to severe disease in Swiss albino mice [22]. For thesestudies, immune complex glomerulonephritis was induced in 13wild-type, 13 C4 2/2, and 10 C3 2/2 animals. In control studiesperformed in parallel, 10 wild-type, 4 C4 2/2, and 7 C3 2/2animals were immunized with equivalent volumes of PBS alone.Thus, a total of 57 animals were studied, of which 23 werewild-type, and 17 each had C4 2/2 and C3 2/2 genotypes. Allanimals survived to the end of the protocol. At the end of thestudy, an 18-hour urine collection was obtained in metaboliccages. Animals were then sacrificed by cardiac puncture andcervical dislocation, and renal tissue was collected for the studiesdescribed below.
Anti-apoferritin ELISA
Polystyrene plates were coated overnight with 5 mg/ml apofer-ritin in 0.05 M carbonate buffer, pH 9.5. Plates were then washed3 times with PBS-T (PBS with 0.05% Tween-20) followed by ablocking step with PBS-T containing 1% BSA (wt/vol) and threeadditional washes with PBS-T. Serial dilutions of serum samples,or affinity purified mouse anti-horse ferritin IgG (Jackson Immu-noResearch Labs, West Grove, PA, USA) were incubated for twohours, followed again by three PBS-T washes. Biotinylated-anti-mouse heavy chain specific antibody (a, g, or m; Sigma) at 1:5000dilutions were incubated for two hours, followed by three PBS-Twashes. Bound biotinylated anti-mouse immunoglobulins weredetected with streptavidin-horseradish peroxidase (Calbiochem,San Diego, CA, USA) at a 1:1000 dilution. After washing twotimes with PBS-T and three times with water, peroxidase wasdeveloped with o-phenylenediamine, and the OD450 determined.All steps were performed at room temperature, except whendissolved cryoprecipitates were analyzed (see below), in whichcase, the antibody step was performed at 37°C.
To determine whether formation of apoferritin-anti-apoferritinimmune complexes affected antibody measurements by ELISA,the following in vitro assay was performed. Anti-ferritin IgG wasmixed with amounts of free apoferritin ranging from 60-foldantibody excess to 15-fold antigen excess. After a 30 minuteincubation at 37°C, this mixture was subjected to anti-apoferritinELISA.
Cryoprecipitate analysis
Blood collected from animals by cardiac puncture was allowedto clot at 37°C and then sera were isolated and stored for five daysat 4°C. Sera were then examined for the presence of cryoprecipi-tates. To characterize the immunoglobulin content of cryoprecipi-tates, sera were centrifuged at 16,000 3 g and cryoprecipitateswere washed with cold PBS. Cryoprecipitates were then dissolvedin PBS at 37°C. Immunofixation electrophoresis [23] was per-formed using a Beckman Instruments’ Paragon system (Fullerton,CA, USA) according to the manufacturer’s instructions. Fivemicroliter samples were applied to individual lanes of the agarosegel. Following electrophoretic separation, anti-mouse heavy chainspecific antibodies (a, g, or m; Sigma) were applied to separatelanes. Gels were washed, stained, destained and then dried. Thepresence of IgA, IgG, and IgM was visually assessed.
Urinary albumin and creatinine determinations
To measure urinary albumin, we used the protocol described byMayadas et al [24]. Microtiter plates were coated overnight with 5mg/ml affinity purified goat anti-mouse albumin (Bethyl Labora-
tories, Montgomery, TX, USA) in 0.05 M carbonate buffer, pH9.5. Wells were washed with PBS-T and blocked with PBS-T with1% BSA. Serial dilutions of urine, or a mouse albumin standard(Sigma) in PBS-T were incubated for two hours, followed by threewashes with PBS-T. Subsequently, horseradish peroxidase-labeledaffinity purified goat anti-mouse albumin (Bethyl Laboratories) at1:1000 in PBS-T was incubated for two hours. Following washingwith PBS-T and water, peroxidase was detected with o-phenylene-diamine, and the OD450 determined. In our hands, this assay waslinear from 1 to 100 ng/ml mouse albumin. Urine and serumcreatinine concentrations were determined with a Beckman Au-toanalyzer. To normalize urinary albumin excretion, data areexpressed as mg urinary albumin/mg urinary creatinine.
Histology and glomerular nuclear counts
Renal cortical tissue for light microscopy was fixed in bufferedformalin. Five micrometer sections were cut and stained withPAS. For each individual animal, nine photographs at 3200magnification were taken of random areas of cortex which in-cluded 1 to 4 glomeruli, and then the 35 mm slides were convertedto TIFF files using a Polaroid Sprint Scan (Cambridge, MA, USA)at a resolution of 2700 dots per inch. Glomerular nuclear countswere obtained on a computer monitor screen using Photoshopsoftware (Adobe Systems Inc., San Diego, CA, USA). Onlyequatorially sectioned glomeruli were counted. All slides werecoded so that the origin of the tissue was unknown to the observer.
Immunohistochemistry and immunofluorescence microscopy
Tissue was snap frozen in isopentane on dry ice. Four micro-meter cryostat sections were processed for direct immunofluores-cence (IF) microscopy as described previously [25]. Fluoresceinisothiocyanate-conjugated antibodies to mouse C3, and heavychain specific antibodies to mouse a, g, and m chains wereobtained from Cappel (Organon Teknika Corp., Durham, NC,USA). For use in double-label immunofluorescence, anti-mouseC3 (Cappel) was tetramethylrhodamine-conjugated using a kitfrom Pierce Chemical Co. (Rockford, IL, USA). At least 30glomeruli from each animal were examined, and a semiquantita-tive score of staining intensity and distribution from 0 to 41 wasgiven, as previously detailed [26]. Glomeruli were visualized andphotographed with a BX-60 immunofluorescence microscope anda PM-30 Exposure Control Unit (Olympus Optical Co., Ltd.,Tokyo, Japan). Illustrative staining patterns are shown in Figures2C (11), 3A (21), and 3B (31). For immunohistochemistry,sections were fixed with 4% paraformaldehyde. Monoclonal anti-bodies F4/80 and 7/4 (Serotec, Ltd., Oxford, UK) were used todetect mouse macrophages and neutrophils, respectively. TheABC staining kit from Vector Laboratories (Burlingame, CA,USA) was used according to the manufacturer’s instructions. Thenumber of positively stained cells in at least 50 glomeruli peranimal were counted. In each of these instances, the observer wasblinded as to the origin of the individual specimen.
Electron microscopy
For electron microscopy, 1 mm3 blocks of renal cortical tissuewere fixed in 2.5% glutaraldehyde in 1.87% sodium phosphatebuffer, pH 7.4, washed with this same buffer, and post-fixed in 1%OsO4. The tissue was dehydrated in graded ethanols followed bypropylene oxide, and embedded in Epon. One-micrometer sec-tions were prepared from each block and stained with toluidine
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice 321

blue to visualize the tissue prior to preparation of ultrathinsections; the latter sections prepared from each block contained atleast two glomeruli. Ultrathin sections were stained with uranylacetate and lead citrate and were viewed in a Philips CM10electron microscope. Tissues were coded so that their origin wasunkown to the observer.
Statistics
Statistical analyses were performed with the Minitab software(College Park, PA, USA). Data are expressed as mean 6 SEM. Foreach variable, the experimental and control groups were com-pared by one-way analyses of variance. When a significant differ-ence (P , 0.05) was identified, individual groups were comparedusing Fisher’s pairwise comparisons, with an individual errorrate # 0.02 considered statistically significant.
To determine if any of the measured variables were correlatedwithin a specific experimental group of animals, Pearson’s corre-lation was employed. Those variables that were correlated werethen examined by regression analysis for statistical significance.
RESULTS
Antibody response to chronic immunization with apoferritin
In this study, mice were immunized daily with high doses of theexogenous protein apoferritin. Wild-type, C4 2/2, and C3 2/2animals developed anti-apoferritin IgM and IgG antibodies (Ta-ble 1). On average, wild-type animals had higher concentrations ofIgM antibodies, but these were not different statistically from C42/2 and C3 2/2 animals. In contrast, wild-type mice immunizedwith apoferritin had significantly greater anti-apoferritin IgGantibody levels measured by ELISA than C4 2/2 or C3 2/2mice. Nonetheless, anti-apoferritin IgG antibodies were detect-able in every animal. Specific anti-apoferritin IgA antibodiescould not be detected in animals from any group.
To determine the effect of immune complexes on the measure-ment of anti-apoferritin antibody levels, we performed a study inwhich various quantities of apoferritin were added to anti-apoferritin IgG in vitro. As shown in Figure 1, measured anti-apoferritin IgG declined by ;75% when antigen excess wasreached, indicating that antibody in immune complexes was notmeasured effectively. Since the primary focus of this study was onthe renal effects of chronic serum sickness, we did not suspendantigen administration in animals to allow clearance of the ;450kDa apoferritin and immune complexes prior to assessing anti-body titers.
At sacrifice, all 13 C4 2/2 and 10 C3 2/2 animals immunizedwith apoferritin had easily detectable cryoprecipitates. Immuno-chemical characterization revealed polyclonal IgM and IgG ineach C4 2/2 cryoprecipitate. In the C3 2/2 animals, polyclonalIgM was present in all samples, while polyclonal IgG was variably
present. In only a single wild-type animal immunized with apof-erritin and one C4 2/2 animal immunized with PBS werecryoprecipitates identified, both of which were small. In these,polyclonal IgM was faintly detectable and IgG was absent. IgAwas not detected in any cryoprecipitate.
The presence of anti-apoferritin antibodies in cryoprecipitateswas evaluated by dissolving cryoprecipitates and performing theELISA at 37°C. By this analysis, all cryoprecipitates containeddetectable anti-apoferritin IgG and IgM antibodies. In the case ofanti-apoferritin IgG, the cryoprecipitates contained from 0.09 to3.33 mg IgG antibody, corresponding to a concentration of 0.23 to8.33 mg/ml in the original sera. Notably, the measured anti-apoferritin IgG and IgM concentrations in cryoprecipitates didnot correlate with the measured sera levels. These data illustratethe limitations in drawing conclusions from antibody measure-ments alone, particularly in the C4 2/2 and C3 2/2 animals, allof which had cryoprecipitates.
Glomerular immunofluorescence and electron microscopy
Wild-type animals immunized with apoferritin developed im-mune complex glomerulonephritis characterized by mesangialdeposition of IgG, IgM, IgA and C3 (panel A in Figs. 2 to 5),which for all except IgA staining were statistically greater than thefindings in wild-type animals immunized with PBS. Graphicalscoring of IF data for all groups of animals is shown in Figure 6.Ten out of 13 wild-type animals also had finely granular periph-eral capillary wall deposits of IgG (Fig. 2E), which in 50% ofanimals was associated with faint (1⁄2 to 11⁄21) C3 staining asdetermined by double-labeling immunofluorescence.
C4 2/2 and C3 2/2 animals immunized with apoferritin haddistinctly different patterns of glomerular IF staining. In C4 2/2immunized with apoferritin, IgG staining was absent in 10 out of13 animals while two others had only trace mesangial staining(Fig. 2B), and a single C4 2/2 animal had 31 mesangial IgGstaining. C3 2/2 immunized animals had staining for mesangialIgG that was detectable, but was to a lesser extent than that of thewild-type animals (Fig. 2C). In contrast to apoferritin-immunizedwild-type animals, peripheral capillary wall IgG staining was notidentified in any of the C4 2/2 or C3 2/2 animals. A similar lowlevel of glomerular IgG staining was seen in C4 2/2 and C3 2/2
10
5
00.05 0.1 1 10 100 200
Apoferritin input, nM
Mea
sure
d an
ti-ap
ofer
ritin
IgG
, nM
Fig. 1. Effect of increasing apoferritin input on the measurement ofanti-apoferritin IgG antibodies. Anti-apoferritin IgG (1 mg/ml) wasincubated with increasing amounts of free apoferritin, followed by deter-mination of anti-apoferritin IgG by ELISA. Each data point is the averageof three measurements.
Table 1. Anti-apoferritin antibody levels
Anti-apoferritin IgGng/ml
Anti-apoferritin IgMOD450 units/ml
Wild-type mice 88.8 6 12.2a (29.3–185.0) 193.4 6 28.4 (63.0–424.2)C4 2/2 mice 27.1 6 3.3 (5.3–40.9) 150.4 6 14.6 (78.0–261.6)C3 2/2 mice 24.7 6 3.9 (11.1–52.2) 152.6 6 23.2 (42.6–237.0)
Data are mean 6 SEM with the range given in the parentheses.a P , 0.001 vs. C4 2/2 and C3 2/2 mice
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice322

animals immunized with PBS, with no statistical differencesbetween these animals and those C4 2/2 and C3 2/2 miceimmunized with apoferritin. Figure 2D shows a representativeglomerulus from one of the PBS-immunized C4 2/2 animals, allfour of which had 11 staining for IgG.
In apoferritin-immunized C4 2/2 and C3 2/2 mice, intensemesangial staining for IgM was present (Fig. 3B and C), which was
significantly greater than in wild-type animals. All three groupsof animals immunized with PBS also had mesangial IgMdeposits (Fig. 3D), but these were significantly less thanapoferritin-immunized animals. We have also seen such mesan-gial IgM in unmanipulated animals, so this cannot be ascribed tothe experimental protocol.
As noted above, apoferritin-immunized wild-type animals had
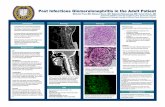
Fig. 2. Immunofluorescence staining for IgG in representative glomeruli. Apoferritin-immunized wild-type mice (A, E), apoferritin-immunized C42/2 mice (B), apoferritin-immunized C3 2/2 mice (C), and PBS-immunized C4 2/2 mice (D) (magnification 3400 A-D, 31000 E).
Fig. 3. Immunofluorescence staining for IgMin representative glomeruli. Apoferritin-immunized wild-type mice (A), apoferritin-immunized C4 2/2 mice (B), apoferritin-immunized C3 2/2 mice (C), and PBS-immunized C4 2/2 mice (D) (magnification3400).
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice 323

detectable mesangial IgA staining (Fig. 4A), but this was notstatistically different from that of PBS-immunized wild-type ani-mals. Among apoferritin-immunized animals, both C4 2/2 andC3 2/2 groups had significantly greater IgA deposition thanPBS-immunized controls (Figs. 4B and C). The IgA deposition inC3 2/2 animals was statistically greater than that of all otheranimals. All PBS-immunized animals had minimal IgA staining(Fig. 4D).
Despite the absence of C4, all C4 2/2 mice had 11 to 31
mesangial staining for C3 (Fig. 5B), and this was undistinguish-able from wild-type mice (Fig. 5A). Since C4 2/2 mice cannotactivate the classical pathway of complement, this indicates thatthe alternative pathway was activated in these animals. As ex-pected, C3 2/2 mice had absent C3 staining (Fig. 5C). Inaddition, the intermittent Bowman’s capsule and tubular base-ment membrane staining for C3 seen in all animals, includingPBS-immunized C4 2/2 mice (Fig. 5D) was absent in every C32/2 animal. Thus, C3 appears to be activated by the alternative
Fig. 4. Immunofluorescence staining for IgAin representative glomeruli. Apoferritin-immunized wild-type mice (A), apoferritin-immunized C4 2/2 mice (B), apoferritin-immunized C3 2/2 mice (C), and PBS-immunized C4 2/2 mice (D) (magnification3400).
Fig. 5. Immunofluorescence staining for C3 inrepresentative glomeruli. Apoferritin-immunized wild-type mice (A), apoferritin-immunized C4 2/2 mice (B), apoferritin-immunized C3 2/2 mice (C), and PBS-immunized C4 2/2 mice (D) (magnification3400).
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice324

pathway in the interstitial compartment, as others have speculated[27, 28].
It should be noted that while the IF data are semiquantitative,the pattern of IF staining was unique for each of the six groups ofanimals. That is, given slides from an unknown animal that werestained for IgG, IgM, IgA, and C3, it was an easy matter todetermine from which group the tissue emanated.
By electron microscopy, electron dense deposits were present inmesangial areas of all apoferritin-immunized wild-type, C4 2/2,and C3 2/2 animals (Fig. 7A). In the wild-type animals, subepi-thelial deposits with focal foot process effacement (Fig. 7B) andsubendothelial deposits (Fig. 7C) were apparent in glomeruli fromall four animals examined. In apoferritin-immunized C4 2/2animals, subepithelial and subendothelial deposits were seen in 1of 10 glomeruli from four mice, the positive glomerulus emanatingfrom the C4 2/2 animal with 31 mesangial IgG staining by IFmicroscopy. In three apoferritin-immunized C3 2/2 animals, raresmall subendothelial and subepithelial deposits were seen in 1 of7 and 5 of 7 glomeruli, respectively. There was also focal footprocess effacement noted, which was not necessarily in areas ofdeposits (Fig. 7A, arrow). Consistent with the IF data, PBS-immunized C4 2/2 animals also had mesangial electron-densedeposits, although these were less than in animals immunized withapoferritin.
Assessment of glomerular disease
Mesangial hypercellularity was evident in all apoferritin-immu-nized animals (Figs. 8A-C). However, since control mice often-
times also appear to have mild mesangial hypercellularity (Fig.8D), this was quantified more accurately by glomerular cellcounts. By this analysis, wild-type and C4 2/2 animals immunizedwith apoferritin had significantly more cells per glomerulus thanthe same animals immunized with PBS (Fig. 9), while apoferritin-immunized C3 2/2 animals did not have increased cellularitycompared to their controls. Interestingly, PBS-immunized C42/2 and C3 2/2 animals had significantly more glomerular cellscompared with PBS-immunized wild-type animals. Increased mes-angial matrix was also seen in apoferritin-immunized animals,being most pronounced in C4 2/2 and C3 2/2 animals. Al-though these animals also had increased mesangial IgM comparedto apoferritin-immunized wild-type mice, suggesting these twovariables might be related, there was no correlation between theIgM staining score and a semiquantitative score for matrixexpansion.
For glomerular neutrophil counts, the only group that had asignificant increase was apoferritin-immunized C4 2/2 mice,which had 0.24 6 0.03 neutrophils per glomerulus, this beingstatistically greater than apoferritin-immunized wild-type mice(0.09 6 0.01) and PBS-immunized C4 2/2 mice (0.10 6 0.01).The presence of glomerular macrophages was decidedly rare in allgroups, with only single monoclonal antibody F4/80-positive cellsbeing found in 40 to 80 glomeruli in all groups. Such lowmacrophage counts in normal animals have been seen by others,as well as in the anti-glomerular basement membrane nephritismodel in mice [29].
Urinary albumin excretion was mildly elevated in all groups of
Imm
unof
luor
esce
nce
scor
e(0
to 4
)
A B
2.50
2.00
1.50
1.00
0.50
0.00
3.50
3.00
2.50
2.00
1.50
1.00
0.50
0.00
C D
¶
*
*
§¶
*¶¶ §¶
¶
*¶ *¶
*
Apoferritin PBS
Imm
unof
luor
esce
nce
scor
e(0
to 4
)
PBSApoferritin
2.50
2.00
1.50
1.00
0.50
0.00Apoferritin PBS
Imm
unof
luor
esce
nce
scor
e(0
to 4
)
2.50
2.00
1.50
1.00
0.50
0.00Apoferritin PBS
Imm
unof
luor
esce
nce
scor
e(0
to 4
)
Fig. 6. Scores for IgG (A), IgM (B), IgA (C), and C3 (D) staining by immunofluorescence microscopy in wild-type (f), C4 2/2 (o), and C3 2/2 mice(s) immunized with apoferritin and PBS. In each case, the groups were statistically different by one-way analysis of variance. Individual comparisonswere made by Fisher’s pairwise comparisons, and statistically significant differences are indicated. P , 0.02 vs.: ¶matched PBS-immunized control;*apoferritin-immunized wild-type, §apoferritin-immunized C3 2/2.
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice 325

animals actively immunized with apoferritin (29.3 6 3.5, 30.1 63.1, and 33.8 6 3.1 mg creatinine/mg albumin in wild-type, C42/2, and C3 2/2 animals, respectively) but only the values fromC3 2/2 animals were statistically different from those of PBS-immunized wild-type or C3 2/2 animals (20.3 6 1.4 and 17.4 62.7 mg creatinine/mg albumin). Serum creatinine levels werenormal in all groups of animals, with mean values 0.24 to 0.31mg/dl.
Correlations among data
Data were analyzed to determine whether any of the histolog-ical or disease variables were related. In wild-type mice immu-nized with apoferritin, there was a strong correlation betweenmesangial IgG and C3 deposition (Fig. 10A; r 5 0.92, P , 0.001),suggesting that mesangial IgG activated complement. In contrast,in apoferritin-immunized C4 2/2 animals there was no relation-ship between glomerular IgG, IgM, or IgA and glomerular C3staining. However, in this group, there was a significant positivecorrelation between mesangial C3 deposition and glomerularnuclear counts (Fig. 10B; r 5 0.62, P 5 0.023). In apoferritin-immunized C3 2/2 animals, glomerular nuclear counts werepositively correlated with mesangial IgM scores (r 5 0.67; P 50.033; not shown). No other correlations were noted.
DISCUSSION
In this study, we have examined the roles of C4 and C3 in amodel of immune complex glomerulonephritis induced by activeimmunization with apoferritin. Wild-type animals with an intact
complement system produced anti-apoferritin IgG and IgM anti-bodies, and developed mesangial proliferative glomerulonephri-tis, characterized by hypercellularity, matrix expansion, depositionof IgG, IgM, IgA and C3, and the presence of electron densedeposits. In the majority of animals, the peripheral capillaries alsocontained IgG, C3 and subendothelial and subepithelial electrondense deposits. Thus, this model is typical of immune complexglomerulonephritis, of which lupus nephritis is the prototype.Actively immunized C4 2/2 and C3 2/2 animals also developedimmune complex glomerulonephritis, but their disease manifes-tations were distinctly different from that of their wild-typelittermates. In these animals, IgG was either absent or present inreduced quantities in glomeruli, yet IgM and IgA were present ingreater intensity in glomeruli, and the mesangial proliferation wasof equal or greater severity than the wild-type animals.
Despite the absence of C4, and the consequent inability toactivate the classical pathway of complement, C4 2/2 animalshad glomerular C3 staining equivalent to that of the wild-typeanimals. Given the lack of C4 in C4 2/2 animals, and theconsequent inability to activate the classical pathway, this indi-cates that the alternative pathway of complement was activated inthese animals. Although IgG in immune complexes is capable ofactivating the alternative pathway [30], IgG was not detectable inglomeruli of the majority of these animals, and therefore, isunlikely to be involved in complement activation. It is, however,conceivable that mesangial IgA, which was present in C4 2/2glomeruli, activated C3 via the alternative pathway [31].
The positive correlation between C3 staining intensity and
Fig. 7. Ultrastructural appearances of glomeruli from apoferritin-immunized C3 2/2 mice (A) and apoferritin-immunized wild-type mice (B and C).Mesangial electron dense deposits were present in apoferritin-immunized C3 2/2 mice (asterisks), but the peripheral capillary loops were free ofdeposits. Subepithelial (B, arrow) and subendothelial deposits (C, arrow) were present in apoferritin-immunized wild-type mice (magnifications: A,38200; B, 323,400; C, 39000).
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice326

glomerular cellularity in the C4 2/2 animals suggests that com-plement has a role in this process. Such a role for complement,and in particular, the C5b-9 membrane attack complex, in medi-ating mesangial cell proliferation has been shown in a rat model ofmesangial proliferative glomerulonephritis [32, 33]. Consistentwith a role of complement to result in glomerular cell prolifera-tion is that apoferritin-immunized C3 2/2 animals did not haveincreased cellularity compared to PBS-immunized C3 2/2 ani-mals. Interestingly, apoferritin-immunized C4 2/2 animals alsohad a significant increase in glomerular neutrophils, although theabsolute numbers were small and did not account for the bulk ofincreased cells in glomeruli. Although the complement activationproducts C3b, C3a, and C5a can recruit and activate neutrophils,it is not clear whether the observed glomerular neutrophil in-crease was due to an effect of the complement system, becausethere was no correlation between neutrophil counts and glomer-ular C3 deposition in apoferritin-immunized C4 2/2 animals.Furthermore, wild-type animals with comparable C3 depositiondid not have a similar increase in glomerular neutrophils.
Our findings suggest that complement is involved in thepathogenesis of immune complex glomerulonephritis, which sup-ports earlier observations made by Falk and Jennette in thismodel [34]. In these studies, C5 deficient B.10.D2.OSN mice werecompared with congenic C5 sufficient B.10.D2.NSN animals. Nodifference in anti-apoferritin levels were detected between thetwo groups. However, disease manifestations were significantly
reduced in C5 deficient animals, as measured by glomerular andtubulointerstitial pathology and by serum creatinine concentra-tions. Nonetheless, there still was detectable disease in some of
Fig. 8. Histological appearances of representative glomeruli. Figures are from apoferritin-immunized wild-type mice (A), apoferritin-immunized C42/2 mice (B), apoferritin-immunized C3 2/2 mice (C), and PBS-immunized C4 2/2 mice (D) (magnification 3400).
60
55
50
45
40
3510
0
Glo
mer
ular
cel
lula
rity,
cel
ls/g
lom
Apoferritin PBS
¶
¶* §
# #
Fig. 9. Glomerular cell counts in wild-type (f), C4 2/2 (o), and C3 2/2(s) mice immunized with apoferritin and PBS. The groups were statisti-cally different by one-way analysis of variance. Individual comparisonswere made by Fisher’s pairwise comparisons, and statistically significantdifferences are indicated. P , 0.02 vs.: ¶matched PBS-immunized control;*apoferritin-immunized wild-type, §apoferritin-immunized C3 2/2;#PBS-immunized wild-type.
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice 327

the C5 deficient B.10.D2.OSN animals in association with glomer-ular deposition of immune complexes and C3. These resultsindicate that immune complex glomerulonephritis is mediated inpart by C5a recruitment and activation of inflammatory cells,and/or by C5b-9 mediated glomerular cell injury with resultantproliferative events [33]. Since disease was not completely elimi-nated in C5 deficient animals, proximal complement components,such as the C3a and C3b cleavage products of C3, or non-complement mediators of disease must also be playing a role inthis model of glomerulonephritis [34]. The finding of C5-indepen-dent, yet C3-dependent disease has been observed in anothermurine model of immune complex glomerulonephritis, in whichmice were immunized with cationized bovine serum albumin [35].
It has long been appreciated that complement activation is keyto mount a proper humoral immune response to an administeredantigen. This has been shown by studies in which C3 has beendepleted with cobra venom factor [36], and by studies in congen-itally C4-, C2-, and C3-deficient humans and animals [37–39]. Ourrecent data with the same C4 2/2 and C3 2/2 mice used in thecurrent studies have extended these observations [6]. A majorfactor in the complement enhancement of the humoral responseis covalent attachment of classical pathway-activated C3 to anti-gen which results in coligation of the CD21/CD19/TAPA-1 core-
ceptor complex with the B lymphocyte receptor [3–5]. A consis-tent theme in these studies is that the impaired antibody responsecan be partially overcome by increasing the antigen dose. Thus, wereasoned that the high dose of antigen used in the current studymight bypass the complement dependence of the humoral im-mune response. Although there was no difference between wild-type, C4 2/2 and C3 2/2 anti-apoferritin IgM antibody levels,C4 2/2 and C3 2/2 had serum anti-apoferritin IgG concentra-tions that were roughly 1⁄3 that of wild-type animals. However, it isdifficult to draw firm conclusions about these levels, given thepresence of cryoprecipitates in C4 2/2 and C3 2/2 animals,which contained anti-apoferritin antibodies that in some caseswere in considerable excess of those found in wild-type sera. Thelatter findings show that the C4 2/2 and C3 2/2 animals did nothave a suboptimal humoral immune response to the administeredapoferritin.
The effect of complement activation on immune complexprocessing is complicated. Complement activation can both solu-bilize and inhibit the precipitation of immune complexes [17, 40].The presence of cryoprecipitates in all apoferritin-immunized C42/2 and C3 2/2 animals is consistent with this role of comple-ment to keep immune complexes in solution. Furthermore, C4band C3b on immune complexes interact with complement recep-tors on primate erythrocytes and non-primate platelets [41–43],which appear to facilitate their clearance by the mononuclearphagocyte system [16]. In this study, IgG deposited in mesangial,subendothelial, and subepithelial locations of wild-type animals.In contrast, despite the presence of anti-apoferritin IgG antibod-ies in all actively-immunized C4 2/2 and C3 2/2 animals, little tono glomerular deposition of IgG was evident in the C4 2/2animals and an intermediate amount of glomerular IgG was foundin C3 2/2 animals. Taken together, these data suggest thatclassical pathway complement activation facilitates deposition ofIgG-containing immune complexes in the mesangium and periph-eral capillary wall of the glomerulus. Evidently, activation up toC4 leads to partial deposition in glomeruli. Whether these effectsare related to the sizes of the complexes [44], which should besmaller in the wild-type complement-replete animals, and/or tointeractions with resident glomerular or blood cell complementreceptors [43, 45, 46] remains to be defined.
In contrast to IgG, IgM was present in greater intensity in themesangial areas of actively-immunized C4 2/2 and C3 2/2animals compared to the wild-type mice. These results suggestthat activation of the classical pathway through C3 facilitates theclearance of IgM-containing immune complexes in wild-typeanimals. Lastly, IgA was significantly greater in apoferritin-immu-nized C3 2/2 mice compared to all other groups. Since IgA-containing immune complexes have been reported to directlyactivate C3 via the alternative pathway [31], it may be that anintact alternative pathway, present in wild-type and C4 2/2animals, is sufficient to effectively clear IgA. It should be notedthat no specific anti-apoferritin IgA antibodies were detected, norwas IgA found in any of the cryoprecipitates, so the origin of theglomerular IgA is not clear. It is also possible that local synthesisof C3 secondary to the inflammatory response resulted in C3deposition independent of IgA [47–49].
The results of these studies have relevance to human disease.The association between hereditary deficiencies of early comple-ment components and immune complex diseases is well known.Although congenital deficiencies of C4 or C3 are rare, associated
0 1 2 3 4
A
Mesangial IgG staining
Mesangial C3 staining
4
3
2
1
0
70
60
50
40
Mes
angi
al C
3 st
aini
ngG
lom
erul
ar c
ellu
larit
yce
lls/g
lom
B
0 1 2 3 4
Fig. 10. Correlations between mesangial IgG and C3 staining in apofer-ritin-immunized wild-type mice (A) and mesangial C3 staining andglomerular cellularity in apoferritin-immunized C4 2/2 mice (B).
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice328

glomerulonephritis has been reported in these patients [13, 50,51]. In the cases of early complement component deficiencies, ithas been difficult to ascribe a pathogenic potential to complementactivation in these conditions in which immune complexes depositin tissue, as it is expected that complement activation cannotoccur. Here we show that C3 does deposit in the mesangium of allC4 2/2 animals, and that it is correlated with mesangial hyper-cellularity. While complement activation is unlikely to be the solemediator of glomerular injury, it is likely to play a role in theglomerular injury seen. The results of our studies illustrate thecomplex interplay between the anti- and pro-inflammatory effectsof the complement system in immune complex diseases affectingthe glomerulus.
ACKNOWLEGMENTS
These studies were supported by National Institutes of Health GrantsDK-41873 (R.J.Q.), AI-32544 (M.C.C.), and HD-1746 (M.C.C.), a Bio-medical Science Grant from the Arthritis Foundation (M.C.C.), and agrant from the Arthritis Foundation, Greater Chicago Chapter (R.J.Q.).Dr. J. Alexander is supported by NIH training grant DK-07510 and Dr. M.Haas by an Established Investigatorship Award from the American HeartAssociation. We also acknowledge the support of BASF Corporation(Worcester, MA, USA). We thank Dr. Y. Nakagawa for performing all ofthe creatinine assays, Dr. Ronald McLawhon for his generous help withcryoprecipitate analysis, and Steve Dove for excellent technical assistancewith electron microscopy.
Reprint requests to Dr. Richard Quigg, The University of Chicago, Sectionof Nephrology, 5841 S. Maryland Ave., MC 5100, Chicago, Illinois 60637,USA.E-mail: [email protected]
REFERENCES1. KINOSHITA T: Biology of complement: The overture. Immunol Today
12:291–295, 19912. QUIGG RJ: Glomerular injury induced by antibody and complement.
Semin Nephrol 11:259–267, 19913. HEYMAN B, WIERSMA EJ, KINOSHITA T: In vivo inhibition of the
antibody response by a complement receptor-specific monoclonalantibody. J Exp Med 172:665–668, 1990
4. AHEARN JM, FISCHER MB, CROIX D, GOERG S, MA M, XIA J, ZHOUX, HOWARD RG, ROTHSTEIN TL, CARROLL MC: Disruption of the Cr2locus results in a reduction in B-1a cells and in an impaired B cellresponse to T-dependent antigen. Immunity 4:251–262, 1996
5. MOLINA H, HOLERS VM, LI B, FUNG Y, MARIATHASAN S, GOELLNERJ, STRAUSS-SCHOENBERGER J, KARR RW, CHAPLIN DD: Markedlyimpaired humoral immune response in mice deficient in complementreceptors 1 and 2. Proc Natl Acad Sci USA 93:3357–3361, 1996
6. FISCHER MB, MA M, GOERG S, ZHOU X, XIA J, FINCO O, HAN S,KELSOE G, HOWARD RG, ROTHSTEIN TL, KREMMER E, ROSEN FS,CARROLL MC: Regulation of the B cell response to T-dependentantigens by classical pathway complement. J Immunol 157:549–556,1996
7. KURTZ HM, DONNELL GN: The effect of depression of complementon nephrotoxic renal disease in rats. Bact Proc 87, 1962
8. UNANUE E, DIXON FJ: Experimental glomerulonephritis. IV. Partici-pation of complement in nephrotoxic nephritis. J Exp Med 119:965–982, 1964
9. SALANT DJ, BELOK S, MADAIO MP, COUSER WG: A new role forcomplement in experimental membranous nephropathy in rats. J ClinInvest 66:1339–1350, 1980
10. LOKKI ML, COLTEN HR: Genetic deficiencies of complement. AnnMed 27:451–459, 1995
11. RATNOFF WD: Inherited deficiencies of complement in rheumaticdiseases. Rheum Dis Clin NA 22:75–94, 1996
12. MATHIESON PW, PETERS DK: Deficiency and depletion of comple-ment in the pathogenesis of nephritis and vasculitis. Kidney Int44(Suppl 42):S13–S18, 1993
13. WELCH TR, MCADAMS AJ, BEISCHEL LS: Glomerulonephritis associ-
ated with complete deficiency of the fourth component of comple-ment. Response to intravenous immunoglobulin. Arthritis Rheum38:1333–1337, 1995
14. SINGER L, COLTEN HR, WETSEL RA: Complement C3 deficiency:Human, animal, and experimental models. Pathobiology 62:14–28,1994
15. SCHIFFERLI JA, TAYLOR RP: Physiological and pathological aspects ofcirculating immune complexes. Kidney Int 35:993–1003, 1989
16. HEBERT LA: The clearance of immune complexes from the circulationof man and other primates. Am J Kidney Dis 27:352–361, 1991
17. SCHIFFERLI JA, STEIGER G, HAUPTMANN G, SPAETH PJ, SJOHOLM AG:Formation of soluble immune complexes by complement in sera ofpatients with various hypocomplementemic states. Difference be-tween inhibition of immune precipitation and solubilization. J ClinInvest 76:2127–2133, 1985
18. FRANK MM: Animal models for complement deficiencies. J ClinImmunol 15:113S–121S, 1995
19. CORK LC, MORRIS JM, OLSON JL, KRAKOWKA S, SWIFT AJ, WINKEL-STEIN JA: Membranoproliferative glomerulonephritis in dogs with agenetically determined deficiency of the third component of comple-ment. Clin Immunol Immunopathol 60:455–470, 1991
20. BOTTGER EC, HOFFMANN T, HADDING U, BITTER-SUERMANN D:Guinea pigs with inherited deficiencies of complement componentsC2 or C4 have characteristics of immune complex disease. J Clin Invest78:689–695, 1986
21. WESSELS MR, BUTKO P, MA M, WARREN HB, LAGE AL, CARROLLMC: Studies of group B streptococcal infection in mice deficient incomplement component C3 or C4 demonstrate an essential role forcomplement in both innate and acquired immunity. Proc Natl Acad SciUSA 92:11490–11494, 1995
22. MCLEISH KR, GOHARA AF, GUNNING WT III: Chronic serum sicknessin the mouse. Relationship of antigen dose to glomerular pathology.Nephron 31:82–88, 1982
23. DUC J, MOREL B, PEITREQUIN R, FREI PC: Identification of mono-clonal gammopathies: A comparison of immunofixation, immunoelec-trophoresis and measurements of kappa- and lambda-immunoglobu-lin levels. J Clin Lab Immunol 26:141–146, 1988
24. MAYADAS TN, MENDRICK DL, BRADY HR, TANG T, PAPAYIANNI A,ASSMANN KJM, WAGNER DD, HYNES RO, COTRAN RS: Acute passiveanti-glomerular basement nephritis in P-selectin-deficient mice. Kid-ney Int 49:1342–1349, 1996
25. QUIGG RJ, ABRAHAMSON DR, CYBULSKY AV, BADALAMENTI J,MINTO AWM, SALANT DJ: Studies with antibodies to cultured ratglomerular epithelial cells: Subepithelial immune deposit formationafter in vivo injection. Am J Pathol 134:1125–1133, 1989
26. HAAS M: IgG subclass deposits in glomeruli of lupus and nonlupusmembranous nephropathy. Am J Kidney Dis 23:358–364, 1994
27. NATH KA, HOSTETTER MK, HOSTETTER TH: Pathophysiology ofchronic tubulo-interstitial disease in rats. Interactions of dietary acidload, ammonia, and complement component C3. J Clin Invest 76:667–675, 1985
28. NATH KA, HOSTETTER MK, HOSTETTER TH: Ammonia-complementinteraction in the pathogenesis of progressive renal injury. Kidney Int36(Suppl 27):S52–S54, 1989
29. SCHRIJVER G, BOGMAN MJ, ASSMANN KJ, DE WAAL RM, ROBBENHC, VAN GASTEREN H, KOENE RA: Anti-GBM nephritis in the mouse:Role of granulocytes in the heterologous phase. Kidney Int 38:86–95,1990
30. GADD KJ, REID KB: The binding of complement component C3 toantibody-antigen aggregates after activation of the alternative path-way in human serum. Biochem J 195:471–480, 1981
31. STAD RK, BOGERS WM, THOOMES-VAN DER SLUYS ME, VAN ES LA,DAHA MR: In vivo activation of complement by IgA in a rat model.Clin Exp Immunol 87:138–143, 1992
32. YAMAMOTO T, WILSON CB: Complement dependence of antibody-induced mesangial cell injury in the rat. J Immunol 138:3758–3765, 1987
33. BRANDT J, PIPPIN J, SCHULZE M, HANSCH GM, ALPERS CE, JOHNSONRJ, GORDON K, COUSER WG: Role of the complement membraneattack complex (C5b-9) in mediating experimental mesangioprolifera-tive glomerulonephritis. Kidney Int 49:335–343, 1996
34. FALK RJ, JENNETTE JC: Immune complex induced glomerular lesionsin C5 sufficient and deficient mice. Kidney Int 30:678–686, 1986
35. SAWTELL NM, HARTMAN AL, WEISS MA, PESCE AJ, MICHAEL JG: C3
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice 329

dependent, C5 independent immune complex glomerulopathy in themouse. Lab Invest 58:287–293, 1988
36. PEPYS MB: Role of complement in induction of antibody productionin vivo. Effect of cobra factor and other C3-reactive agents onthymus-dependent and thymus-independent antibody responses. J ExpMed 140:126–145, 1974
37. OCHS HD, WEDGWOOD RJ, FRANK MM, HELLER SR, HOSEA SW: Therole of complement in the induction of antibody responses. Clin ExpImmunol 53:208–216, 1983
38. MCNEIL KM, OCHS HD, HELLER SR, CORK LC, MORRIS JM, WINKEL-STEIN JA: Role of C3 in humoral immunity. Defective antibodyproduction in C3-deficient dogs. J Immunol 140:1939–1945, 1988
39. OCHS HD, NONOYAMA S, ZHU Q, FARRINGTON M, WEDGWOOD RJ:Regulation of antibody responses: The role of complement andadhesion molecules. Clin Immunol Immunopathol 67:S33–S40, 1993
40. MILLER GW, NUSSENZWEIG V: A new complement function: Solubi-lization of antigen-antibody aggregates. Proc Natl Acad Sci USA72:418–422, 1975
41. FEARON DT: The human C3b receptor, in Complement, edited byMULLER-EBERHARD HJ, MIESCHER PA, New York, Springer-Verlag,1983, p 101
42. QUIGG RJ, HOLERS VM: Characterization of rat complement recep-tors and regulatory proteins, CR2 and Crry are conserved, and theC3b receptor of neutrophils and platelets is distinct from CR1.J Immunol 155:1481–1488, 1995
43. QUIGG RJ, ALEXANDER JJ, LO CF, LIM A, HE C, HOLERS VM:
Characterization of C3 binding proteins on mouse neutrophils andplatelets. J Immunol 159:2438–2444, 1997
44. MANNIK M: Pathophysiology of circulating immune complexes. Arthri-tis Rheum 25:783–787, 1982
45. QUIGG RJ, GALISHOFF ML, SNEED AE, KIM D: Isolation and charac-terization of complement receptor type 1 (CR1) from rat glomerularepithelial cells. Kidney Int 43:730–736, 1993
46. ALEXANDER JJ, HE C, ADLER S, HOLERS VM, QUIGG RJ: Character-ization of C3 receptors on cultured rat glomerular endothelial cells.Kidney Int 51:1124–1132, 1997
47. SACKS S, ZHOU W, CAMPBELL RD, MARTIN J: C3 and C4 geneexpression and interferon-gamma-mediated regulation in human glo-merular mesangial cells. Clin Exp Immunol 93:411–417, 1993
48. WELCH TR, BEISCHEL LS, WITTE DP: Differential expression ofcomplement C3 and C4 in the human kidney. J Clin Invest 92:1451–1458, 1993
49. AULT BH, COLTEN HR: Cellular specificity of murine renal C3expression in two models of inflammation. Immunology 81:655–660,1994
50. LHOTTA K, THOENES W, GLATZL J, HINTNER H, KRONENBERG F,JOANNIDIS M, KONIG P: Hereditary complete deficiency of the fourthcomponent of complement: Effects on the kidney. Clin Nephrol39:117–124, 1993
51. BORZY MS, GEWURZ A, WOLFF L, HOUGHTON D, LOVREIN E:Inherited C3 deficiency with recurrent infections and glomerulone-phritis. Am J Dis Child 142:79–83, 1988
Quigg et al: Glomerulonephritis in C4- and C3-deficient mice330