EFFECTIVENESS OF A MEDICAL EDUCATION INTERVENTION TO TREAT HYPERTENSION IN PRIMARY CARE
Upload
sfhpCategory
view
848download
5
HYPERTENSION
“THE SILENT KILLER”
أحمد الشمسخلف الغامديفالح المطيريمحمد الحقباني
يزيد المعشوق
Sunday 23 October 2011421 Primary Health Care
CourseUnder the supervision of
Dr. Hussein Saad

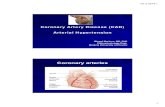
HYPERTENSION Definition of BP Epidemiology of HT Diagnosis of HT Measuring & confirming of HT Approach to hypertensive patients Risk factors of HT Complications of HT Lowering & prevention of HT Investigation Management Highlights Cases

DEFINITION OF BP
The pressure of blood flowing through your blood vessels against the vessel walls
Systolic BP: during heart beat “written on top”
Diastolic BP: during heart relaxation “written on bottom”

DEFINITION OF HT
It is a sustained elevated blood pressure more than 140 mmHg systolic and more than 90 mmHg diastolic

EPIDEMIOLOGY
World epidemiology:
Based on data collected in the 1999 to 2000 National Health and Nutrition Examination Survey (NHANES), the estimated overall prevalence of hypertension in 2000 was 28.7%. Among 1565 participants with hypertension, 68.9% were aware of the problem, and 58.4% were under pharmacological treatment. Overall, only 31.0% of individuals had hypertension controlled to a blood pressure of <140 mm Hg systolic and 90 mm Hg diastolic. This figures implies that >40 million adults have uncontrolled hypertension in the United States.
Us epidemiology: Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States,
1988–2000. JAMA. 2003; 290: 199–206.

KSA epidemiology :In Saudi Arabia at a recent study
it was found that the prevalence
of hypertension was found to be 26.1% in general in subjects between 30 to 70.
prevalence in males was at 28.6 %.In females it was at 23.9 %.
Prevalence of CAD between hypertensive subjects was 8.2 %.In normotensive patients it was 4.5 %.
ksa epidemiology : Al-Nozha MM, Abdullah M, Arafah MR, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007 Jan;28(1):77-84.

4758 subjects participated in recent study.
51% was female. The prevalence was 25.5%. 27.1% males, 23.9% females. 55.3% of the patients were unaware of
their disease.(5)
Abdalla A. Saeed, Nasser A. Al-Hamdan, Ahmed A. Bahnassy, et al. Prevalence, Awareness, Treatment, and Control of Hypertension among Saudi Adult Population: A National Survey. International Journal of Hypertension. Volume 2011 (2011): 8.

DIAGNOSIS
The American Heart Association has recommended guidelines to define normal and high blood pressure.
Normal blood pressure less than 120/80
Pre-hypertension 120-139 / 80-89
High blood pressure (stage 1) 140-159 / 90-99
High blood pressure (stage 2) higher than 160/100


HOW TO MEASURE BP
Blood pressure is measured with a blood pressure cuff (sphygmomanometer). This may be done using a stethoscope and a cuff and gauge or by an automatic machine
IMPORTANT : measuring alone isnot completely enough, it hasto go hand in hand with a properhistory regarding ….??

To measure the blood pressure correctly the patient has to be :
1) sitting2) has not smoked orconsumed caffeine productsin the last 30 min3) rest for 5 minutes prior tomeasuring4) if it is elevated recheck the other arm
* use a cuff of a proper size for the particular patient, place it 3 cm over the elbow crease.

Patient has a reading of 145/95 mmHg is he hypertensive?
145
95

BE WARE !!!
WCH ??
What’s the opposite?

1) Medical History Age, sex & race Family Hx (1st degree relatives) Chronic dis.
(CV, diabetes, renal, vascular, …) Diet, smoking, alcohol Medications (like OCP) previous and current feeling tired, dizzy, blurred vision, headache at the
back of the head,… Activity and lifestyle
APPROACH

2) Examination Measuring BP correctly CV examination (HR & pulse) Height & weight (BMI < 26) Chest, neck, abdomen and lungs Fundoscpoic examination of
eyes

3) Routine & optional lab tests
4) Treatment with and without drugs
Canadian Guidelines of Hypertension 2011 updated• www.hypertension.ca CHEP 2011 guidelines• JNC 7 May 2003

RISK FACTORS Family history Age > 60 (after menopause) Sex (M>F) Race (black > white) Diabetes Pregnant and OCP Renal diseases Vascular ,, Obesity Inactivity (lack of physical activities) Smoking Alcohol Stress Diet: salt & fat (indirectly) ------------------------------------------
• Canadian guidelines of HT 2011• JNC7

COMPLICATIONS
Cardiac events (HF, angina and strokes) Vascular (Heart, brain and peripheral vascular
disease) Eye (including blindness)
Retinopathy Angina

Renal (kidney damage) Role of kidney in keeping healthy BP HT CKD HT heart work harder damage blood
vessels including renal ↓ removing wastes & extra fluids increase fluids in blood vessels HT
Dangerous cycle HT one of the leading causes of KF (ESRD)
Canadian guidelines of Hypertension 2011• JNC7• www.medicinenet.com

LOWERING OF BP : PREVENTION
Physical exerciseWeight reductionAlcohol consumptionDietary recommendationsSodium intake and caffeineStop smoking

BENEFITS OF LOWERING BP
Benefits In Clinical Trials, lowering of BP is associated
with ↓ in:
Stroke incidence 35-40%MI 20-25%Heart Failure > 50%

INVESTIGATIONS
Routine laboratory tests : CBC Urine analysis & Microalbuminuria Urea, electrolytes and calcium Fasting plasma glucose Lipid profile ECG Chest X-Ray

Optional laboratory tests : Serum uric acid 24 Hrs urinary protein Creatinine clearance Echocardiography Ultrasonography Thyroid stimulating hormone 24 Hrs urinary vanyl mandelic acid 24 Hrs urinary free hydrocortisol
JNC 7&European Association of Hypertension

MANAGEMENTThe ultimate public health goal of
antihypertensive therapy is the reduction of cardiovascular and renal morbidity and mortality.

BP TARGETS : BP targets are (systolic/diastolic):
≤140/90 mmHg in all patients with hypertension.
≤130/80 mmHg in patients with diabetes and in high-risk.
It may be difficult to achieve BP targets, especially in elderly and diabetic patients, and in patients with CV damage.

MANAGEMENT :
Non-pharmacological
pharmacological

LIFESTYLE MODIFICATIONS (NON-PHARMACOLOGICAL MANAGEMENT) :Life style :
* Weight Reduction * Dietary sodium reduction * Physical Activity * Avoid alcohol consumption * Type of food

Approximate SBPReduction (Range)
Recommendation Modification
5–20 mmHg/10 kgweight loss
23,24
Maintain normal body weight
Weight reduction
8–14 mmHg25,26
Consume a diet rich in fruits, vegetables,
and low fat dairy products with a
reduced content of saturated and total
fat .
Adopt DASH eating plan
2–8 mmHg25–27
Reduce dietary sodium intake to no more than 100 m
mol per day (2.4 g sodium or 6 g
sodium chloride.)
Dietary sodium reduction
4–9 mmHg28,29
Engage in regular aerobic physical
activity such as brisk walking
(at least 30 min per day, most
days of the week .)
Physical activity
2–4 mmHg30
Limit consumption to no more than 2
drinks s
Moderation of alcohol consumption

PHARMACOLOGICAL MANAGEMENT
There are five major classes of such agents licensed for initiation or maintenance of hypertension, alone or in combination:
Angiotensin converting enzyme inhibitors (ACEIs)
Angiotensin receptor blockers (ARBs) Beta-blockers (BBs) Calcium channel blockers (CCBs) Thiazide-type diuretics

PHARMACOLOGICAL MANAGEMENT
Without Compelling indication
With compelling Indication

CHOICE OF THERAPY FOR ADULT WITH PT WITHOUT COMPELLING INDICATION Initial therapy should be monotherapy with a
thiazide diuretics.
Hypokalemia??
if target BP not achieved with standard dose of monotherapy?
combination : thiazide diuretic - CCB CCB + ACEI Other combination ACEI –ARB – not recommended

COMPELLING INDICATIONS:# Ischemic Heart Disease most common form of target organ
damage associated with hypertension. Pt. with hypertension and coronary
artery disease , an ACE inhibitor or ARB is recommended
Pt. with stable angina → B blocker Pt. had a recent MI → B blocker and
ACEI

DIABETIC HYPERTENSION
Combinations of two or more drugs are usually needed to achieve the target
goal of <130/80 mmHg. Thiazide diuretics, BBs, ACEIs, ARBs, and
CCBs are beneficial in reducing CVD and stroke incidence in patients with diabetes.
ACEI- or ARB-based treatments favorably affect the progression of diabetic nephropathy and reduce albuminuria have been shown to reduce progression to macroalbuminuria.

PT WITH CHRONIC KIDNEY DISEASE target BP <130/80 mmHg Initial therapy should be an ACEI or ARB
if there is intolerance to ACEI Thizide diuretic are recommended as
additive therapy

HIGHLIGHTS:
Gestational hypertension: pregnant woman developing high blood pressure after 20 weeks of pregnancy

Who is at more risk
1) Obese women2) Women who have chronic hypertension3) Pregnant women under the age of 20 or over the age of 40. 4) Women who are pregnant with more than one baby5) Women with diabetes, kidney disease, rheumatoid arthritis, lupus or scleroderma

Resistant hypertension
Blood hypertension in despite of use of 3 Concurrent antihypertensive of different classes.
One of the agents is diuretics and all of the agents should be used at optimal doses.


CASE 1 A 55 year old man, who is known case
of diabetes on insulin. BP: 160 ∕ 100 P: 92 ∕ min. Wt: 86 kg Ht: 1.68 cm.
How are you going to manage this patient ?

CASE 2 A 63 year old man who is a known case
of hypertension, came for follow up. He is regular on lisinopril 10 mg daily.
His BP is 156 ∕ 104 .
How are you going to manage this patient ?

CASE 3 A 22 year young patient present to your
clinic with high blood pressure after 2 documented reading.
BP:160 ∕ 110
How are you going to manage this patient ?

MCQs

REFERENCES 1) American Heart Association http://circ.ahajournals.org/content/112/11/1651.full
2) http://www.medicinenet.com/pregnancy_induced_hypertension/page2.htm
3) Canadian Hypertension Guidelines
4) European Association of Hypertension
5) JNC 7