Hypertension in Chronic Kidney Disease
83
Hypertension in Chronic Kidney Disease Andrew Bomback, MD, MPH Columbia University College of Physicians & Surgeons
Transcript of Hypertension in Chronic Kidney Disease
Hypertension inChronic Kidney Disease
Andrew Bomback, MD, MPH
Columbia University College of Physicians & Surgeons

HTN in CKD: Outline
• Volume/salt– Theory of pressure natriuresis
• The renin angiotensin ALDOSTERONE system– CKD = state of relative hyperaldosteronism?
• Chronotherapy– Timing of drugs = dosing of drugs?
• BP goals in CKD– What should we shoot for? 140/90? 130/80? 120/80?

Volume/Salt

Chronic kidney disease
• The prevalence of resistant HTN >50% in nephrology clinics
– 5-15% range in general medical practices
• “Pressure-natriuresis” theory renal handling of sodium is the ultimate determinant of blood pressure
– Normal renal function effectively excrete Na loads
– Impaired renal function must raise BP to efficiently excrete Na and stay in steady state

The effect of dry-weight reduction on interdialyticambulatory systolic (A) and diastolic (B) blood pressure in hypertensive hemodialysis patients in the DRIP trial.
Agarwal R, Alborzi P, Satyan S, Light RP. Dry-weight reduction in hypertensive hemodialysis patients (DRIP): a randomized, controlled trial. Hypertension. Mar 2009;53(3):500-507.

Prevalence of resistant hypertension in the United States, 2003-2008. Hypertension. 2011 Jun;57(6):1076-80.

Blood Pressure Follows the Kidney
genetically hypertension-prone rat normotensive rat

Blood Pressure Follows the Kidney
• The human version of the experiment
LEFT: Bill Evans (publicist, kidney donor, friend)RIGHT: Neil Simon (playwright, kidney recipient, friend)
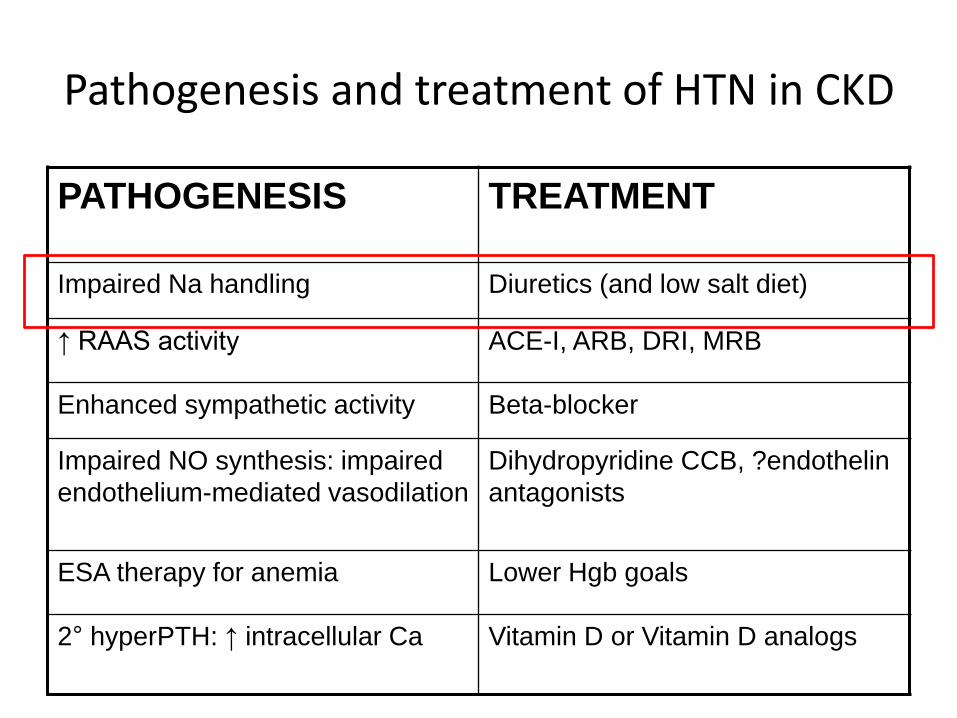
Pathogenesis and treatment of HTN in CKD
PATHOGENESIS TREATMENT
Impaired Na handling Diuretics (and low salt diet)
↑ RAAS activity ACE-I, ARB, DRI, MRB
Enhanced sympathetic activity Beta-blocker
Impaired NO synthesis: impaired
endothelium-mediated vasodilation
Dihydropyridine CCB, ?endothelin
antagonists
ESA therapy for anemia Lower Hgb goals
2° hyperPTH: ↑ intracellular Ca Vitamin D or Vitamin D analogs
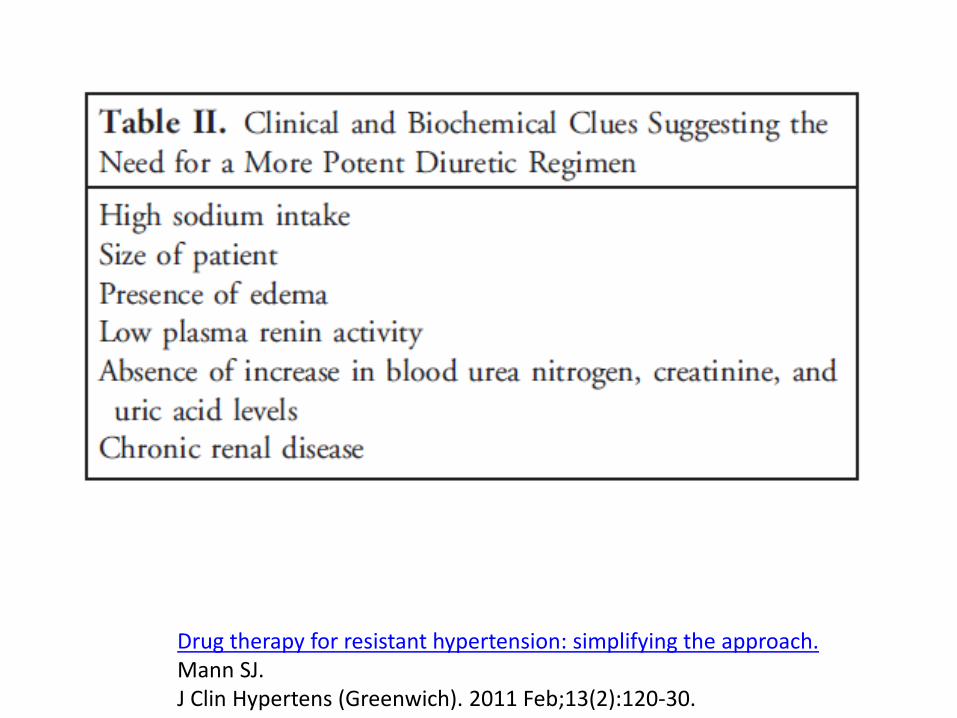
Drug therapy for resistant hypertension: simplifying the approach.Mann SJ.J Clin Hypertens (Greenwich). 2011 Feb;13(2):120-30.

Drug therapy for resistant hypertension: simplifying the approach.Mann SJ.J Clin Hypertens (Greenwich). 2011 Feb;13(2):120-30.

Prevalence of resistant hypertension in the United States, 2003-2008. Hypertension. 2011 Jun;57(6):1076-80.

Choice of diuretic
Khosla N, Chua DY, Elliott WJ, Bakris GL. J Clin Hypertens (Greenwich). Jun 2005;7(6):354-356

Copyright ©2011 American Heart Association
Dorsch, M. P. et al. Hypertension 2011;57:689-694
Adjusted event-free probability of CVEs

Meta-Analysis of Dose–Response Characteristics of Hydrochlorothiazide and Chlorthalidone: Effects on Systolic Blood Pressure and PotassiumMichael E. Ernst, Barry L. Carter, Shimin Zheng and Richard H. Grimm Jr
American Journal of Hypertension 2010; 23 4, 440–446

Chlorthalidone Versus HCTZ for the Treatment of HTN in Older Adults
Ann Intern Med. 2013;158(6):447-455. doi:10.7326/0003-4819-158-6-201303190-00004
Primary outcome: composite of death or hospitalization for heart failure, stroke, or myocardial infarction
Hospitalization with hypokalemia
Hospitalization with hyponatremia
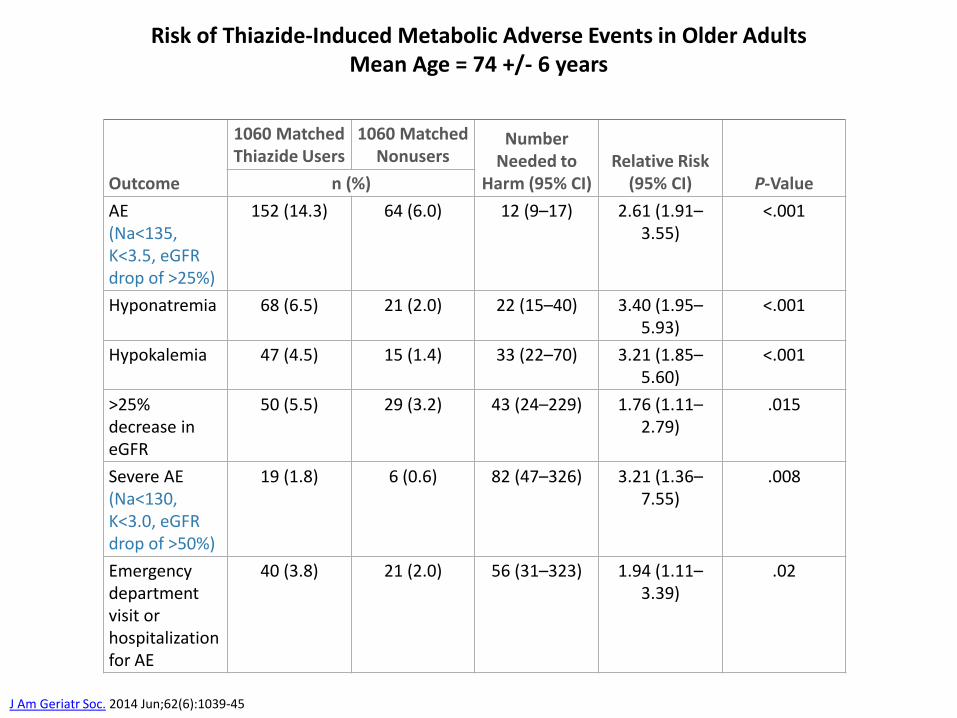
Outcome
1060 Matched Thiazide Users
1060 Matched Nonusers
Number Needed to
Harm (95% CI)Relative Risk
(95% CI) P-Valuen (%)
AE(Na<135,K<3.5, eGFRdrop of >25%)
152 (14.3) 64 (6.0) 12 (9–17) 2.61 (1.91–3.55)
<.001
Hyponatremia 68 (6.5) 21 (2.0) 22 (15–40) 3.40 (1.95–5.93)
<.001
Hypokalemia 47 (4.5) 15 (1.4) 33 (22–70) 3.21 (1.85–5.60)
<.001
>25% decrease in eGFR
50 (5.5) 29 (3.2) 43 (24–229) 1.76 (1.11–2.79)
.015
Severe AE(Na<130, K<3.0, eGFRdrop of >50%)
19 (1.8) 6 (0.6) 82 (47–326) 3.21 (1.36–7.55)
.008
Emergency department visit or hospitalization for AE
40 (3.8) 21 (2.0) 56 (31–323) 1.94 (1.11–3.39)
.02
Risk of Thiazide-Induced Metabolic Adverse Events in Older AdultsMean Age = 74 +/- 6 years
J Am Geriatr Soc. 2014 Jun;62(6):1039-45

The Renin AngiotensinALDOSTERONE System

The first RAAS blocker
PREDATOR = Bothrops jararaca
PREY = Yanomamo Indians
Of snakes and men
• Hunter-gatherers were low-salt cultures
• Relied on RAAS-dependent normotension
• Low mean BP = 93.2-108.4 / 58.6-69.4 mm Hg
• Very high mean urinary aldosterone = 74.52 micrograms/24 hrs
• Very high mean PRA = 13.10 mg/ml/hr
Bomback AS, Bove RM, Klemmer PJ. Of snakes and men: the evolution of ACE inhibitors. J Renin Angiotensin Aldosterone Syst. 2007;8(1):1-2
Oliver WJ, Cohen EL, Neel JV. Blood pressure, sodium intake, and sodium related hormones in the Yanomamo Indians, a "no-salt" culture. Circulation. 1975;52(1):146-51

Lessons from the snake• Hyperactive RAAS without salt OK
(Yanomamo)
• Hyperactive RAAS with salt Not OK
• Modern hypertension the kidney’s attempt to reconcile a mismatch between conserved RAAS activity and high salt intake
• Pressure natriuresis re-establishes salt balance• Cost is HTN-related cardiovascular and renal injury
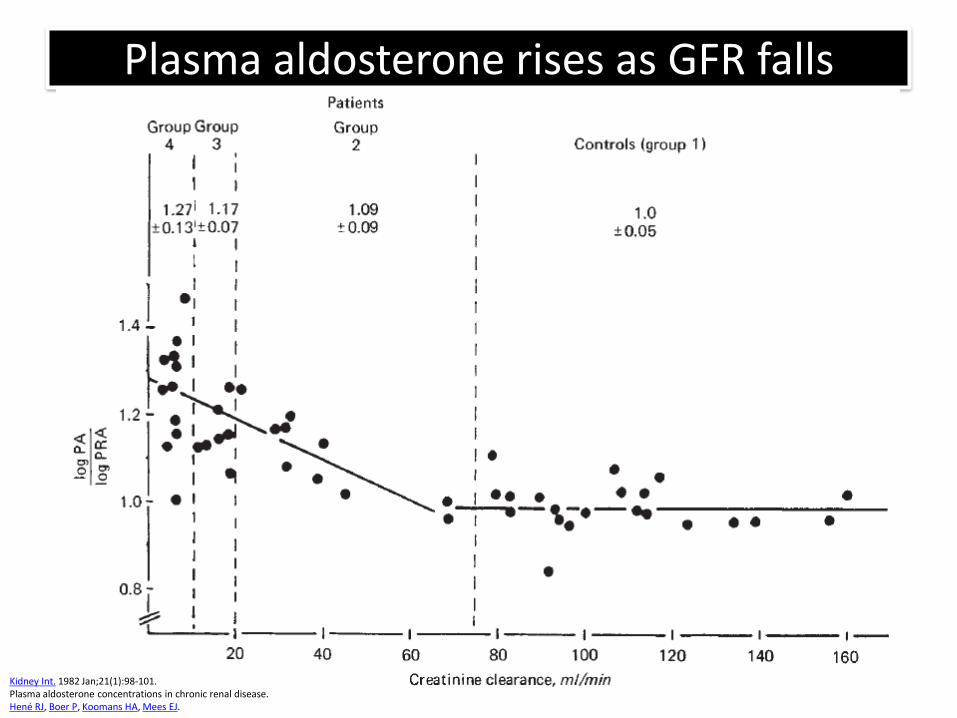
Plasma aldosterone rises as GFR falls
Kidney Int. 1982 Jan;21(1):98-101.Plasma aldosterone concentrations in chronic renal disease.Hené RJ, Boer P, Koomans HA, Mees EJ.

Aldosterone and Sodium Cofactor (ECV):“Relative hyperaldosteronism”
0
5
10
15
20
10 150 300
Sodium Cofactor
Ald
oste
ron
e
Normals
HTN, CKD, CHF, OBESITY
Inappropriately high aldosterone, in the presence of salt cofactor, activates the mineralocorticoid receptor to initiate non-epithelial, pro-fibrotic effects
Klemmer PJ, Bomback AS. Blood Purification 2009; 27:92-98.
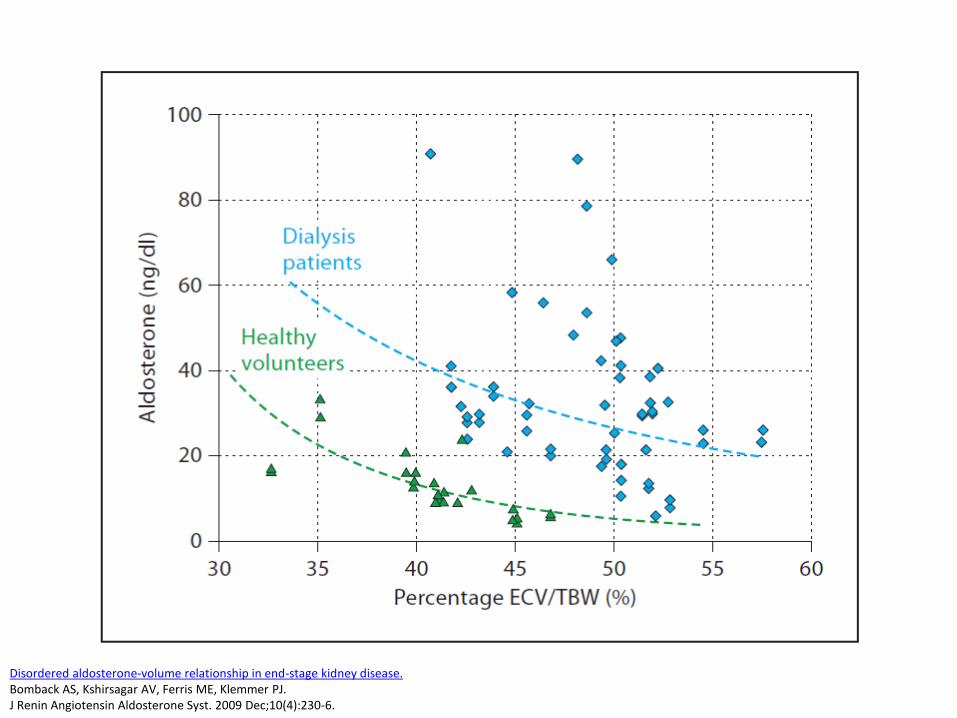
Disordered aldosterone-volume relationship in end-stage kidney disease.Bomback AS, Kshirsagar AV, Ferris ME, Klemmer PJ.J Renin Angiotensin Aldosterone Syst. 2009 Dec;10(4):230-6.

“Relative hyperaldosteronism” in all stages of CKD
Volk MJ, Bomback AS, Klemmer PJ. Curr Hypertens Rep. 2011 Aug;13(4):282-8. Bomback AS, Klemmer PJ. Blood Purif. 2012;33(1-3):119-24.
Sodium Cofactor/Extracellular Volume
Ald
ost
ero
ne
No CKD
CKD 3
CKD 4
CKD 5

Aldosterone BreakthroughC
han
ge in
se
rum
ald
ost
ero
ne
du
rin
g R
AA
S b
lock
ade
0
+
-
6 months 12 months
Expected decline in aldosterone on ACE-I and/or ARB therapy
Aldosteronebreakthrough
Bomback AS, Klemmer PJ. Nat Clin Pract Nephrol. 2007;3(9):486-92
60-70% patients
30-40% patients


ASCOT: Use of spironolactone for resistant hypertension in 1411 subjects
Chapman N, Dobson J, Wilson S, et al. Hypertension. Apr 2007;49(4):839-845.

Hypertension 2011; 57(6): 1069-1075

Figure 2. Home systolic and diastolic blood pressures comparing
spironolactone with placebo, doxazosin, and bisoprolol
Bryan Williams, Thomas M MacDonald, Steve Morant, David J Webb, Peter Sever, Gordon McInnes, Ian Ford, J Kennedy Cruickshank, Mark J Caulfield,
Jackie Salsbury, Isla Mackenzie, Sandosh Padmanabhan, Morris J Brown
Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a
randomised, double-blind, crossover trialLANCET 2015; Volume 386: 2059–2068

Prevalence of resistant hypertension in the United States, 2003-2008. Hypertension. 2011 Jun;57(6):1076-80.

Risk of hyperkalemia with MRBs
Khosla N, Kalaitzidis R, Bakris GL: Predictors of Hyperkalemia Risk following Hypertension Control with Aldosterone Blockade. Am J Nephrol 2009;30:418-424
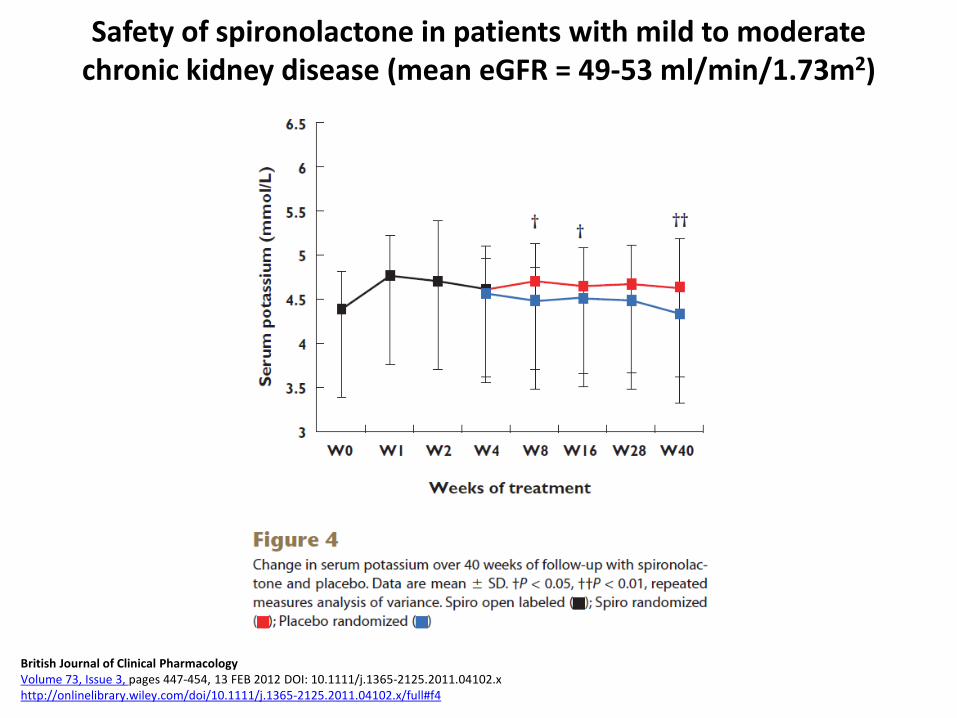
Safety of spironolactone in patients with mild to moderate chronic kidney disease (mean eGFR = 49-53 ml/min/1.73m2)
British Journal of Clinical PharmacologyVolume 73, Issue 3, pages 447-454, 13 FEB 2012 DOI: 10.1111/j.1365-2125.2011.04102.xhttp://onlinelibrary.wiley.com/doi/10.1111/j.1365-2125.2011.04102.x/full#f4

Eur Heart J. 2013 Aug;34(31):2453-63. Safety and tolerability of the novel non-steroidal mineralocorticoid receptor antagonist BAY 94-8862 in patients with chronic heart failure and mild or moderate chronic kidney disease: a randomized, double-blind trial.Pitt B1, Kober L, Ponikowski P, Gheorghiade M, Filippatos G, Krum H, Nowack C, Kolkhof P, Kim SY, Zannad F.
Lower risk of hyperkalemia with non-steroidal MRA

GL Bakris et al. N Engl J Med October 23, 2020. DOI: 10.1056/NEJMoa2025845
FIDELIO STUDY: Finerenone in Diabetic CKD

Mineralocorticoid Receptor Antagonists for Hypertension Management in Advanced Chronic Kidney Disease:
BLOCK-CKD Trial
Hypertension 2020 Jul;76(1):144-149

Rajiv Agarwal et al. Kidney360 2021;2:425-434
©2021 by American Society of Nephrology

Chronotherapy
Rationale for chronotherapy
• Many, if not all, specific human physiological functions are under the control of a circadian timing system– includes kidney function and, by extension, the control of blood
pressure– most obvious example of circadian rhythmicity of renal function
is the well-recognized difference in urine volume formation and excretion between daytime and nighttime
• Urinary excretion of all major solutes – including sodium –also follows a circadian pattern; when this pattern is impaired, disease may ensue– Abnormal circadian rhythm for renal sodium reabsorption is
considered one of the major factors leading to the loss of nocturnal blood pressure dipping
Burnier M, Coltamai L, Maillard M, Bochud M. Semin Nephrol. Sep 2007;27(5):565-571.
Bankir L, Bochud M, Maillard M, Bovet P, Gabriel A, Burnier M. Hypertension. Apr 2008;51(4):891-898.

Chronobiol Int. 2013 Mar;30(1-2):145-58.Comparison of ambulatory blood pressure parameters of hypertensive patients with and without chronic kidney disease.Mojón A1, Ayala DE, Piñeiro L, Otero A, Crespo JJ, Moyá A, Bóveda J, de Lis JP, Fernández JR, Hermida RC; Hygia Project Investigators.
http://www.ncbi.nlm.nih.gov/pubmed/?term=Moy%C3%A1%20A%5bAuthor%5d&cauthor=true&cauthor_uid=23181690

Timing of drugs in resistant HTNSystolic blood pressure
-12
-10
-8
-6
-4
-2
0
2
Diurnal mean Nocturnal
mean
24-hr mean
% c
han
ge f
rom
baseli
ne B
P
All drugs on awakening
1 drug at bedtime
Diastolic blood pressure
-14
-12
-10
-8
-6
-4
-2
0
2
4
Diurnal mean Nocturnal
mean
24-hr mean
% c
han
ge f
rom
baseli
ne B
P
All drugs on awakening
1 drug at bedtime
Hermida RC, Ayala DE, Fernandez JR, Calvo C. Hypertension 2008;51(1):69-76.

Chronotherapy in 1794 subjects with “true” resistant HTN
Am J Hypertens. 2010 Apr;23(4):432-9. Effects of time of antihypertensive treatment on ambulatory blood pressure and clinical characteristics of subjects with resistant hypertension.Hermida RC, Ayala DE, Mojón A, Fernández JR.

Chronotherapy in CKD (mean eGFR 46 ml/min/1.73m2) restores nocturnal dipper status
Minutolo R, Gabbai FB, Borrelli S, et al. Am J Kidney Dis 2007;50(6):908-917

Survival curves as a function of time-of-day of
hypertension treatment in CKD patients
Hermida R C et al. JASN 2011;22:2313-2321
Total CV events
Major CVD events = cardiovascular deaths, MI, ischemic CVA, and hemorrhagic CVA

Eur Heart J, Volume 41, Issue 48, 21 December 2020, Pages 4565–4576, https://doi.org/10.1093/eurheartj/ehz754
The content of this slide may be subject to copyright: please see the slide notes for details.
Kaplan–Meier cumulative hazard curves for cardiovascular disease outcome
as a function of hypertension treatment-time regimen

Eur Heart J, Volume 41, Issue 48, 21 December 2020, Pages 4565–4576, https://doi.org/10.1093/eurheartj/ehz754
The content of this slide may be subject to copyright: please see the slide notes for details.
Adjusted hazard ratio of cardiovascular disease outcome as a function of
hypertension treatment-time regimen
Blood Pressure Goals in CKD

JAMA. 2014;311(5):538

The full implementation of the 2014 HTN Guidelines would result in approximately
• 56,000 fewer CV events/year
• 13,000 fewer deaths from CV causes/year

Isolated systolic hypertension in the elderly
Chobanian AV. N Engl J Med. Aug 23 2007;357(8):789-796.

ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents.Aronow WS et al. Circulation 2011 May 31;123(21):2434-506.

HYVET: Hypertension in Very Elderly Trial
Beckett NS et al. N Engl J Med. 2008;358(18):1887-1898

HYVET: Hypertension in Very Elderly Trial
Beckett NS et al. N Engl J Med. 2008;358(18):1887-1898

The SPRINT Research Group. N Engl J Med 2015;373:2103-2116.
SPRINT TRIAL: New BP Goals?

SPRINT participants:• aged >50 years• SBP 130-180
and• > 1 of the following CV risk factors
• age > 75 years• clinically evident CV disease (i.e. previously
documented CAD, PAD, or CVD)• subclinical CV disease (i.e. ↑ coronary artery
calcification score by CT scan, LVH, or an ABI <0.9)
• eGFR 20-59 mL/min/1.73 m2
• 10-year Framingham Risk Score > 15%
SPRINT excluded: DM, symptomatic CHF, CVA history, proteinuria > 1 g/day, and nursing home residents
SPRINT used automated oscillometric blood pressure (AOBP), which averages multiple consecutive readings with the patient resting alone in a room. In general, systolic pressure readings are 5-10 mmHg lower with AOBP than with manual measurement

The SPRINT Research Group. N Engl J Med 2015;373:2103-2116
• Patients with DM excluded• DM = #1 cause of CKD
• CKD with eGFR 20-60 was considered a CV risk suitable for enrollment
• <30% had CKD• Among those with CKD, mean eGFR ~48
• Primary Outcome in subjects with CKD• Intensive treatment 8.1%• Standard Treatment 9.6%• HR 0.82 (0.63-1.07)
• Primary Outcome in subjects without CKD• Intensive treatment 4.0%• Standard Treatment 5.7%• HR 0.70 (0.56-0.87)
The SPRINT Research Group. N Engl J Med 2015;373:2103-2116.

The SPRINT Research Group. N Engl J Med 2015;373:2103-2116.

ACCORD TRIAL: Mean Systolic BP Levels at Each Study Visit in Diabetics
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585.

ACCORD TRIAL: Kaplan–Meier Analyses of Selected Outcomes
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585.

AASK: Blood-Pressure Levels in Patients with Chronic Kidney Disease
Appel LJ et al. N Engl J Med 2010;363:918-929.

Appel LJ et al. N Engl J Med 2010;363:918-929.
AASK: Event rates for primary and secondary outcomes

AASK: Incidence of the composite primary outcome (doubling of Scr, ESRD, or death) according to baseline proteinuria
Appel LJ et al. N Engl J Med 2010;363:918-929.

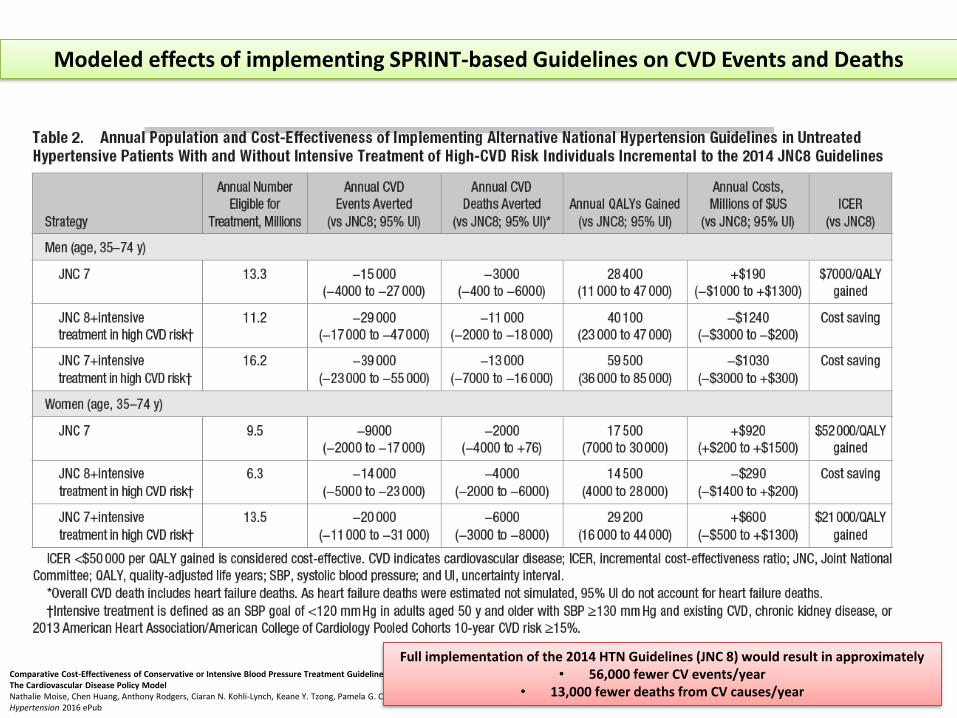
Comparative Cost-Effectiveness of Conservative or Intensive Blood Pressure Treatment Guidelines in Adults Aged 35–74 YearsThe Cardiovascular Disease Policy ModelNathalie Moise, Chen Huang, Anthony Rodgers, Ciaran N. Kohli-Lynch, Keane Y. Tzong, Pamela G. Coxson, Kirsten Bibbins-Domingo, Lee Goldman, Andrew E. MoranHypertension 2016 ePub
Modeled effects of implementing SPRINT-based Guidelines on CVD Events and Deaths
Full implementation of the 2014 HTN Guidelines (JNC 8) would result in approximately
• 56,000 fewer CV events/year• 13,000 fewer deaths from CV causes/year
Comparative Cost-Effectiveness of Conservative or Intensive Blood Pressure Treatment Guidelines in Adults Aged 35–74 YearsThe Cardiovascular Disease Policy ModelNathalie Moise, Chen Huang, Anthony Rodgers, Ciaran N. Kohli-Lynch, Keane Y. Tzong, Pamela G. Coxson, Kirsten Bibbins-Domingo, Lee Goldman, Andrew E. MoranHypertension 2016 ePub
Modeled effects of implementing SPRINT-based Guidelines on CVD Events and Deaths
Full implementation of the 2014 HTN Guidelines (JNC 8) would result in approximately• 56,000 fewer CV events/year
• 13,000 fewer deaths from CV causes/year

CardioSurve survey, American College of Cardiology

Proteinuric CKD(other than DM)
Non-proteinuric CKD Diabetic CKDCKD with CV fragility
<125/75 <130/80 <140/90
2017 Blood Pressure Goals in CKD?

Proteinuric CKD(other than DM)
Non-proteinuric CKD Diabetic CKDCKD with CV fragility
<125/75 <130/80 <140/90
2017 Blood Pressure Goals in CKD?
IF NO SIDE EFFECTS IF NO SIDE EFFECTS

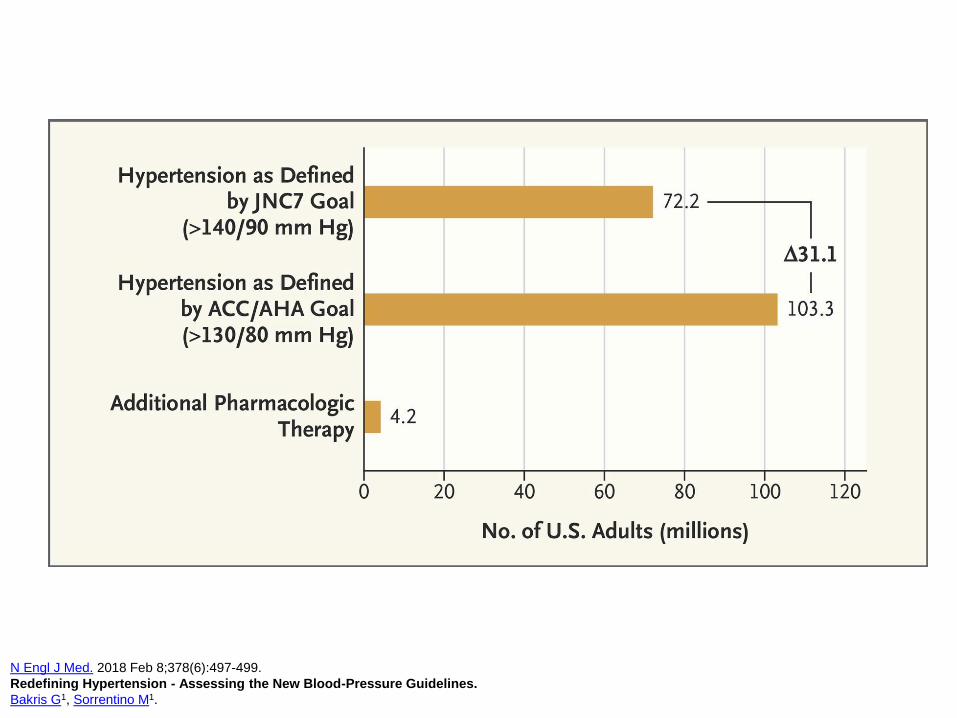
N Engl J Med. 2018 Feb 8;378(6):497-499.
Redefining Hypertension - Assessing the New Blood-Pressure Guidelines.
Bakris G1, Sorrentino M1.
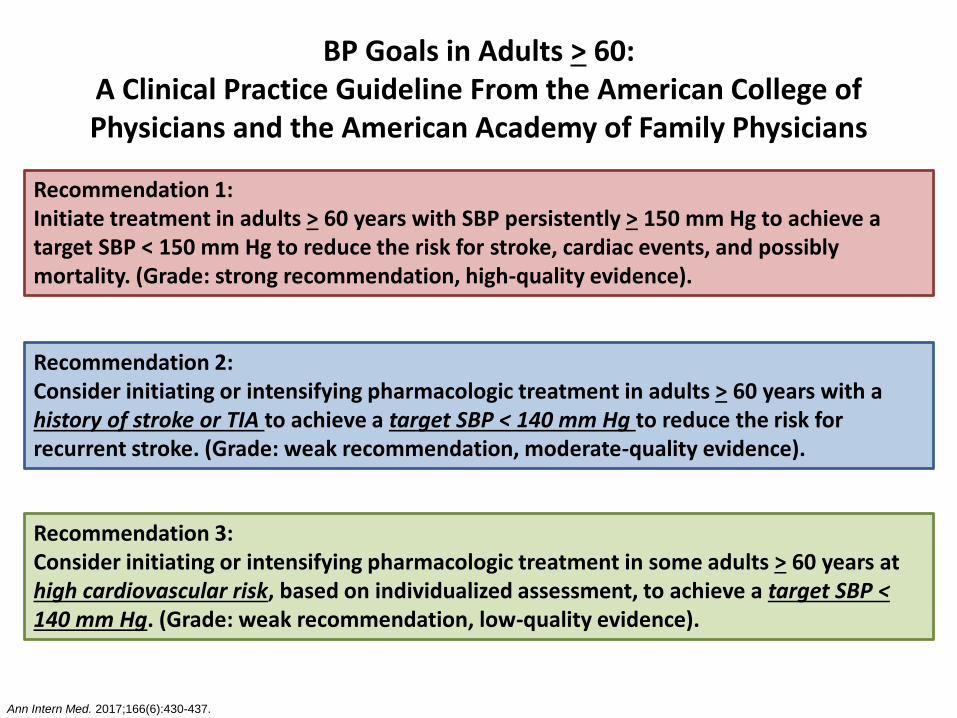
BP Goals in Adults > 60:A Clinical Practice Guideline From the American College of Physicians and the American Academy of Family Physicians
Recommendation 1:Initiate treatment in adults > 60 years with SBP persistently > 150 mm Hg to achieve a target SBP < 150 mm Hg to reduce the risk for stroke, cardiac events, and possibly mortality. (Grade: strong recommendation, high-quality evidence).
Ann Intern Med. 2017;166(6):430-437.
Recommendation 2:Consider initiating or intensifying pharmacologic treatment in adults > 60 years with a history of stroke or TIA to achieve a target SBP < 140 mm Hg to reduce the risk for recurrent stroke. (Grade: weak recommendation, moderate-quality evidence).
Recommendation 3:Consider initiating or intensifying pharmacologic treatment in some adults > 60 years at high cardiovascular risk, based on individualized assessment, to achieve a target SBP < 140 mm Hg. (Grade: weak recommendation, low-quality evidence).
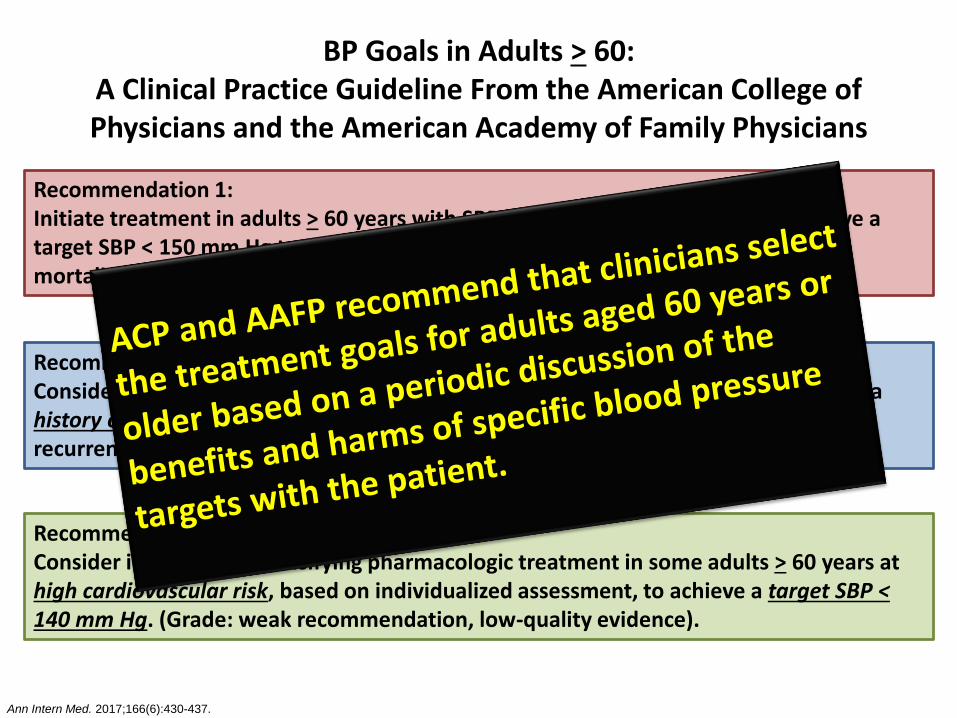
BP Goals in Adults > 60:A Clinical Practice Guideline From the American College of Physicians and the American Academy of Family Physicians
Recommendation 1:Initiate treatment in adults > 60 years with SBP persistently > 150 mm Hg to achieve a target SBP < 150 mm Hg to reduce the risk for stroke, cardiac events, and possibly mortality. (Grade: strong recommendation, high-quality evidence).
Ann Intern Med. 2017;166(6):430-437.
Recommendation 2:Consider initiating or intensifying pharmacologic treatment in adults > 60 years with a history of stroke or TIA to achieve a target SBP < 140 mm Hg to reduce the risk for recurrent stroke. (Grade: weak recommendation, moderate-quality evidence).
Recommendation 3:Consider initiating or intensifying pharmacologic treatment in some adults > 60 years at high cardiovascular risk, based on individualized assessment, to achieve a target SBP < 140 mm Hg. (Grade: weak recommendation, low-quality evidence).
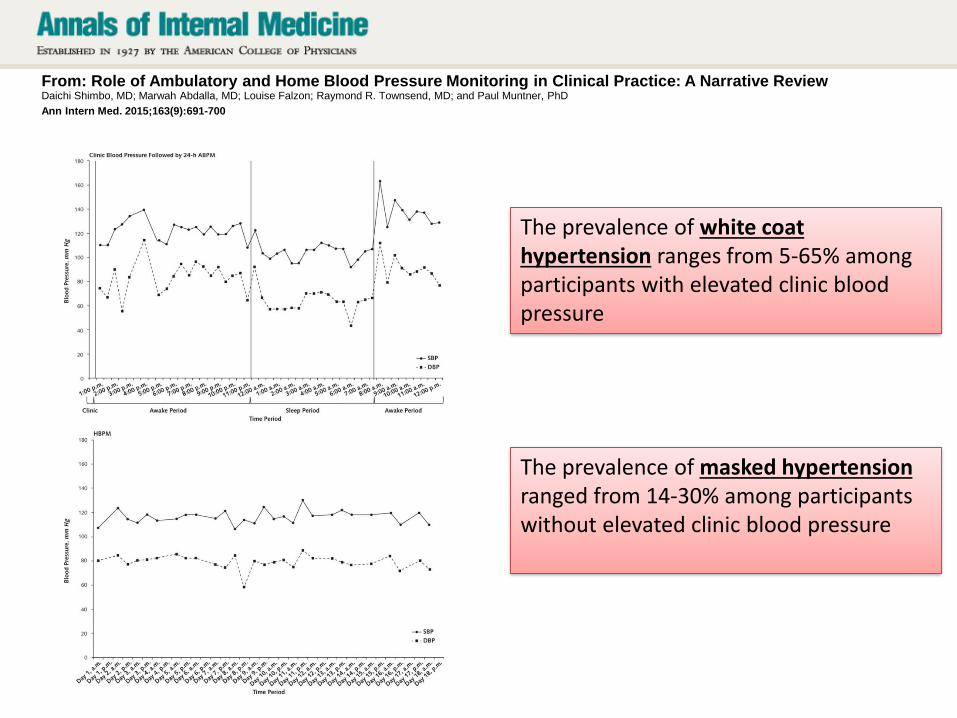
From: Role of Ambulatory and Home Blood Pressure Monitoring in Clinical Practice: A Narrative ReviewDaichi Shimbo, MD; Marwah Abdalla, MD; Louise Falzon; Raymond R. Townsend, MD; and Paul Muntner, PhD
Ann Intern Med. 2015;163(9):691-700
The prevalence of white coat hypertension ranges from 5-65% among participants with elevated clinic blood pressure
The prevalence of masked hypertensionranged from 14-30% among participants without elevated clinic blood pressure
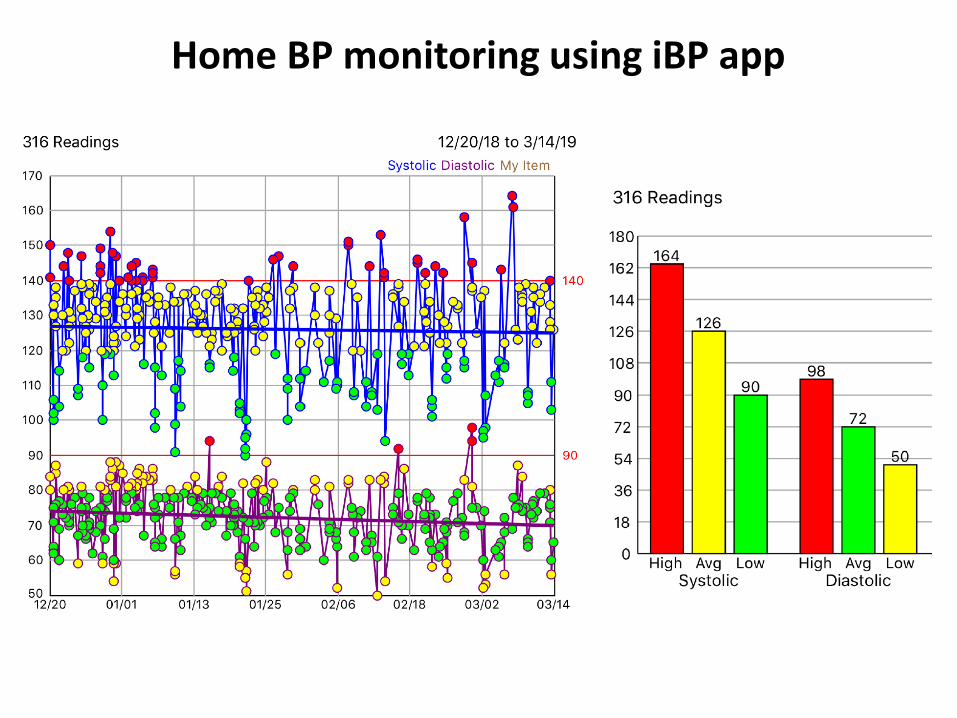
Home BP monitoring using iBP app

Wearable BP monitors on the horizon…
Omron’s HeartGuideAsus’s VivoWatch BP

Conclusions for HTN in CKD
• Volume…salt….volume…salt
– Need adequate diuresis and salt restriction
• The RAAS
– Relative hyperaldosteronism in CKD – rationale for using MRB therapy
– Hyperkalemia is an issue, particularly when eGFRfalls <45 ml/min/1.73m2

Conclusions for HTN in CKD
• Chronotherapy– Flip at least 1 medication from AM to PM dosing
• Improves dipping pattern• May improve overall CV outcomes
• BP goals in CKD– 130/80 by 2017 HTN Guidelines is appropriate– Reasonable to target lower (120/70) if young/highly
functional/non-diabetic patient with proteinuria– Reasonable to allow higher (140/70) if isolated systolic
HTN pattern

Initial Diagnosis of Resistant Hypertension
Office BP >130/80 mm Hg in proteinuric CKD or >140/90 mm Hg in non-proteinuric CKD
+
Prescribed ≥3 antihypertensive agents at optimal doses, ideally including a diuretic
or
BP at goal but requires ≥4 antihypertensive agents to do so
Exclude Pseudo-resistance
•Ensure proper blood pressure measurement technique
•Confirm adherence to prescribed treatment
•Evaluate the antihypertensive regimen for suboptimal dosing and combination of agents
•Avoid clinician inertia
Obtain 24-hour ambulatory blood pressure monitoring (ABPM)
•Rule out “white-coat” hypertension
•Identify the presence of a “nondipper” vs. “dipper” pattern
Physiologic Assessment of Volume Excess: Indications for Uptitrating
Diuretic Regimen
• Low PRA
• 24-hour urine sodium >150 mmol/d
• Edema
• Reduced eGFR
Clues of Hypertension Mediated by the
SNS
• Tachycardia
• Congestive heart failure
•Anxiety symptoms
Optimize Diuretic Regimen
•Change HCTZ to chlorthalidone
•Maintain thiazide and add MRB (spironolactone or eplerenone)
•Change thiazide to loop diuretic if eGFR <40 ml/min/1.73m2
•Combine loop diuretic with distally acting diuretic (thiazide, amiloride)
Add or substitute β- orα- + β-blockadeOptimize RAAS Blockade
•Uptitrate ACE-I or ARB to “ultrahigh” doses
•Add MRB (spironolactone or eplerenone)
Chronotherapy: Change > 1 antihypertensive agents from AM to PM dosing
• For all patients vs. only non-dippers
Hyperactive RAAS
•High PRA
•Aldosterone breakthrough
•Reduced eGFR
•Refractory BP or proteinuria on escalating doses of ACE-I or ARB
Nephrol Dial Transplant. 2014 Jul;29(7):1327-1335.Definition, identification and treatment of resistant hypertension in chronic kidney disease patients.Drexler YR, Bomback AS.
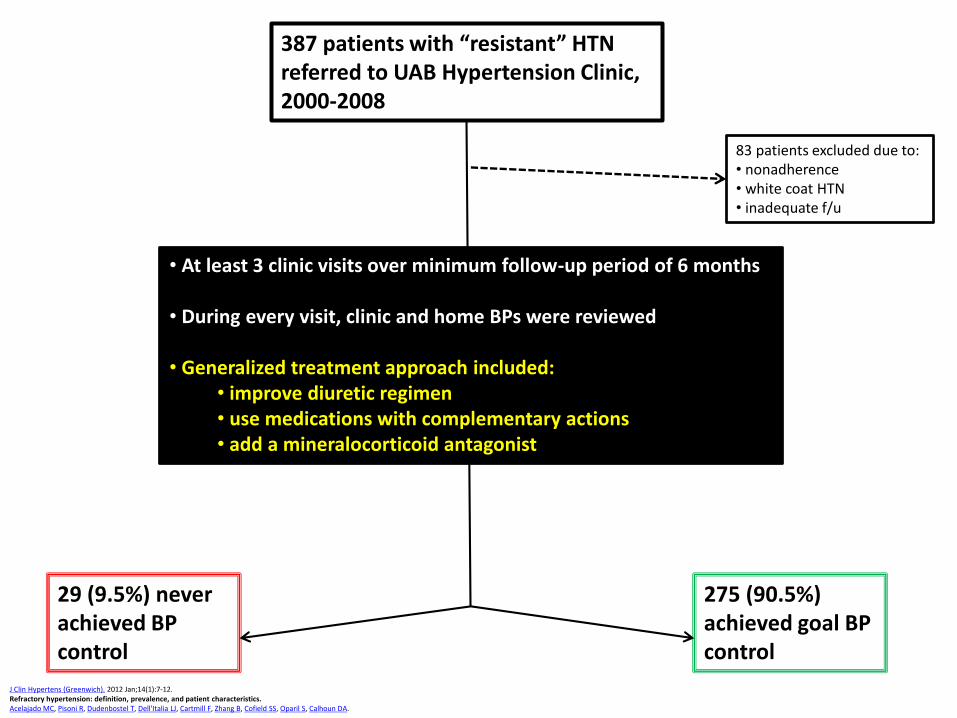
387 patients with “resistant” HTN referred to UAB Hypertension Clinic, 2000-2008
83 patients excluded due to:• nonadherence• white coat HTN• inadequate f/u
29 (9.5%) never achieved BP control
• At least 3 clinic visits over minimum follow-up period of 6 months
• During every visit, clinic and home BPs were reviewed
• Generalized treatment approach included:• improve diuretic regimen• use medications with complementary actions• add a mineralocorticoid antagonist
275 (90.5%) achieved goal BP control
J Clin Hypertens (Greenwich). 2012 Jan;14(1):7-12.Refractory hypertension: definition, prevalence, and patient characteristics.Acelajado MC, Pisoni R, Dudenbostel T, Dell'Italia LJ, Cartmill F, Zhang B, Cofield SS, Oparil S, Calhoun DA.
Question 1
• A 62 year old man with CKD stage 4 (eGFR 24 ml/min/1.73m2) due to IgA nephropathy presents to your clinic with a systolic blood pressure of 160/90. What should be his goal blood pressure?
A. <130/80
B. <125/75
C. <140/80
D. <140/90
E. <140/70

Question 2
• A 50 year old man with BP 145/88 on amlodipine 5 mg daily is seen in clinic. You add chlorthalidone 25 mg daily to his regimen. When should you check a basic metabolic panel?
A. 3-5 days after starting chlorthalidone
B. 5-7 days after starting chlorthalidone
C. 2-3 weeks after starting chlorthalidone
D. 1-2 months after starting chlorthalidone

Question 3
• A 70 year old woman with BP 149/91 on amlodipine 5 mg daily is seen in clinic. You add chlorthalidone 25 mg daily to her regimen. When should you check a basic metabolic panel?
A. 3-5 days after starting chlorthalidoneB. 1 week after starting chlorthalidone and again at
3 weeks after starting chlorthalidoneC. 3 weeks after starting chlorthalidone and again
at 5 weeks after starting chlorthalidoneD. Once montly for first 6 months after starting
chlorthalidone
Question 4
• The FIDELIO study showed reductions in hard CV endpoints in which population of CKD patients using finerenone vs. placebo?
A. IgA nephropathy
B. Hypertensive, non-proteinuric CKD
C. Diabetic CKD
D. Polycystic kidney disease

Your Questions