Hydatidiform mole
47
Hydatidiform Mole Extern Sarawut Hongyim
-
Upload
gio-arki -
Category
Health & Medicine
-
view
4.730 -
download
4
description
Transcript of Hydatidiform mole

Hydatidiform MoleExtern Sarawut Hongyim

History
• หญิ�งไทย คู่� อาย� 17 ปี�
• Menache 14 yr.
• LMP 9 มคู่. 56 *3 day pad 1-2 ผื�น/วั�น มาสม��าเสมอ no dysmenorrhea
• SI 1st 15 yr. single partner
• Oral contraception 2 yr หย�ดได� 2 เด�อน
• No Hx. STD, dyspareunia, post coital bleeding, abortion

History
• CC : แพทย�น�ดนอนโรงพยาบาลเน��องจากตั้�'งคู่รรถ์�ไข่�ปีลาอ�ก
• PI : 1d PTA ผื�ปี*วัยปีระจ�าเด�อนข่าด 2 เด�อน ตั้รวัจการตั้�'งคู่รรถ์�ด�วัยตั้นเอง พบวั�าตั้�'งคู่รรถ์� จ,งไปีพบแพทย�ท-�คู่ล�น�คู่ เพ��อฝากคู่รรถ์� แพทย� ultrasound พบล�กษณะการตั้�'งคู่รรถ์�ไข่�ปีลาอ�ก จ,งแนะน�าให�มานอนโรงพยาบาล• ปีฏิ�เสธอาการคู่ล��นไส�อาเจ-ยน เล�อดออกผื�ดปีกตั้�ทางช่�องคู่ลอด ไม�ปีวัดท�อง• ปีฏิ�เสธโรคู่ปีระจ�าตั้�วั • ปีฏิ�เสธการแพ�ยาและอาหาร

Physical exam• Vital sign : BP 100/70 mmHg, PR 86 bmp, RR 18 /min, Temp 37 oC
• Wt. 52 kg Ht. 155 cms
• General appearance : thai teenage women, good consciousness
• HEENT : not pale, no icteric sclera
• Lymph node : no lymphadenopathy
• Heart : normal s1 s2, no murmur
• Lung : normal breath sound, no adventitious sound
• Abdomen : BS +ve, not tender
• Neuro : E4V5M6 pupil 3 mm RTL BE

Physical exam
• Affected part
• Uterus 12 wk size
• PV exam
• NIUB normal
• Vagina normal discharge
• Cervix no abnormal lesion, os closed, not tender
• Adnexa no adnexa mass, not tender

Ultrasound

Lab investigation
• CBC : Hct 36.2 % Platelet 233,000 WBC 6,220 cu.mm.
• UA : protein & sugar –ve, RBC 2-3, WBC 1-2, Epi 5-10
• Urine BHCG : 1,600 – 3,200
• Serum BHCG : ย�งไม�ได�ผืล
• BUN 12 mg/dl, cr 0.61 mg/dl
• LFT : total protein 7.6, alb 4.6, total bilirubin 1.02, direct bilirubin 0.15, ALP 70, AST 8, ALT 29

Diagnosis
• Molar pregnancy

Molar pregnancyHydatidiform Mole

Molar pregnancy
• is characterized histologically by abnormalities of the chorionic villi that consist of trophoblastic proliferation and edema of villous stroma.
• complete or partial

Epidemiology
• vary dramatically in different regions of the world
• molar pregnancy in Japan (2 per 1,000 pregnancies)
• in Europe or North America (about 0.6 to 1.1 per 1,000 pregnancies)

Risk Factors
• Age
• adolescents and women aged 36 - 40 years have a 2-fold risk and those > 40 years have 10-fold risk
• Prior Molar Pregnancy
• recurrent moles was 1.3 %, 1.5 % complete mole and 2.7 % partial mole
• 2 prior molar pregnancies third mole 23 %

Complete versus Partial Hydatidiform Mole
• Gross morphology
• Histopathology
• Karyotype

Complete Hydatidiform Mole
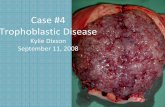
• Grossly
• mass of clear vesicles
• vary in size from barely visible to a few centimeters
• hang in clusters from thin pedicles.
• Histologically
• hydropic degeneration and villous edema
• absence of villous blood vessels
• absence of embryonic fetus and amnion.

Complete Hydatidiform
Mole

Normal chorionic villi
http://radiology.uchc.edu/eAtlas/Images/GYN/5801b.gif

Complete Hydatidiform
Mole
http://www.webpathology.com/image.asp?case=585&n=2

Complete Hydatidiform
Mole
http://www.webpathology.com/image.asp?n=3&Case=585

Complete Hydatidiform Mole
• usually diploid and of paternal origin
• 85 % are 46,XX with both of chromosomes paternal origin
• androgenesis, ovum is fertilized by a haploid sperm, which duplicates its own chromosomes after meiosis, ovum chromosomes absent or inactivated.
• other complete moles, may be 46,XY due to dispermic fertilization

Complete Hydatidiform Mole
Malignant Potential
• higher incidence of malignant sequela
• 15 - 20 % had evidence of persistent trophoblastic disease

85 %
androgenesisComplete
Hydatidiform Mole

Partial Hydatidiform Mole
• fetal tissue and Hydatidiform changes that are focal and less advanced
• avascular chorionic villi and vascular villi
• typically is triploid—69, XXX, 69,XXY, or much less commonly, 69,XYY

Partial Hydatidiform Mole
• Grossly
• Smaller volume of tissue
• Mixture of grossly vesicular and normal villi
• Fetus / embryo is usually present, although often abnormal • syndactyly of digits 3
& 4 of both hands and feet
• Histologically
• Mixture edematous villi & normal villi
• Less conspicuous central cistern formation (internal clefting)
• Mild focal trophoblast hyperplasia without atypia
• Villous scalloping

Partial Hydatidifor
m Mole

Partial Hydatidifor
m Mole

Partial Hydatidifor
m Mole

Partial Hydatidiform
Mole

Partial Hydatidiform Mole
• Malignant Potential
• lower than complete molar
• Seckl and associates (2000) documented 3 of 3000 of partial moles to be choriocarcinoma
• Growdon and co-workers (2006) higher hCG levels increased risk for persistent disease
• levels 200 mIU/mL in the third through 8 week post evacuation at least a 35-% risk of persistent disease

Twin Molar Pregnancy
• not rare
• Vejerslev (1991) found that of 113 such pregnancies, 45 % progressed to 28 weeks, and 70 % neonates survived

Twin Molar Pregnancy

Clinical Presentation
• Vaginal Bleeding 84%
• Theca Lutein Ovarian Cysts 46 %
• Excessive Uterine Size 28%
• Hyperemesis Gravidarum 8%
• Preeclampsia 1 %
• Hyperthyroidism rarely
• Trophoblastic Embolization rarely
Complete Mole Partial Mole
• incomplete or missed abortion 91.3%• vaginal bleeding 72.8%• Excessive uterine size 3.7%

Diagnosis
• History & physical exam• Mole pass in vagina
• pregnancy testing and sonography

Sonography
• complete mole • complex, echogenic uterine mass with numerous
cystic spaces and no fetus or amnionic sac
• partial mole • thickened, hydropic placenta with fetal tissue
Snow storm appearance

complete mole

Partial Hydatidiform Mole
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0100-39842010000200014&lng=en&nrm=iso&tlng=en

Management
• Evaluation
• Termination of pregnancy
• Follow up

evaluation
• Evaluated medical complications
• Preeclampsia
• Hyperthyroidism
• electrolyte imbalance
• Anemia
• Lab investigation
• CXR
• CBC
• UA
• BUN, Cr
• Electrolyte
• LFT
• PT, PTT

Terminaton of pregnancy
• Suction & curettage
• Hysterectomy
• Prophylactic chemotherapy

Suction Curettageregardless of uterine size & preserve fertility following steps:
• Oxytocin infusion before the induction of anesthesia.
• Cervical dilation
• Suction curettage the uterus may decrease dramatically in size, and the bleeding is well controlled. The use of a 12-mm cannula is strongly advised to facilitate evacuation. If the uterus is larger than 14 weeks of gestation, one hand should be placed on top of the fundus, and the uterus should be massaged to stimulate uterine contraction and reduce the risk of perforation.
• Sharp curettage When suction evacuation is believed to be complete, gentle sharp curettage is performed to remove any residual molar tissue

Hysterectomy
• If no further pregnancies are desired
• aged > 40 yr.
• Uterine perforate

Prophylactic Chemotherapy
• Prophylactic chemotherapy not only prevented metastasis but also reduced the incidence and morbidity of choriocarcinoma
• But• can’t absolutely to prevent choriocarcinoma
• After TOP 80-90 % of Molar pregnancy are cure
• and choriocarcinoma are cure by currently chemotherapy
Actinomycin D, Methotrexate

Follow-up
• Human Chorionic Gonadotropin
• Contraception
• Chemotherapy

Human Chorionic Gonadotropin
• monitored q weekly B-hCG levels until normal for 3 consecutive weeks
• followed q monthly until normal for 6 consecutive months

Contraception
• Prevent pregnancy for a minimum of 1 yr. using hormonal contraception
• oral contraceptives safely after molar evacuation during the entire interval of hormonal follow-up

chemotherapy
• If• B-hCG level rising or plateau
• Rising = increase B-hCG > 2-fold
• Plateau = no change or increase < 2-fold

Further of pregnancy
• Recurrent 5 - 10-fold of pregnancy
• Reassurance women if desire pregnancy but early ANC

Reference
• Berek, Jonathan S. Gestational Trophoblastic Disease. Berek & Novak's Gynecology, 14th Edition.
• Chapter 11. Gestational Trophoblastic Disease. Williams Obstetrics, 23 Edition