High-Throughput Time-Resolved FRET Reveals Akt/PKB...
14
Integrated Systems and Technologies High-Throughput Time-Resolved FRET Reveals Akt/PKB Activation as a Poor Prognostic Marker in Breast Cancer Selvaraju Veeriah 1 , Pierre Leboucher 1,2 , Julien de Naurois 1,3 , Nirmal Jethwa 1 , Emma Nye 4 , Tamara Bunting 4 , Richard Stone 4 , Gordon Stamp 4 ,V eronique Calleja 1 , Stefanie S. Jeffrey 5 , Peter J. Parker 3,6 , and Banafsh e Larijani 1,7,8 Abstract Dysregulation of the Akt/PKB pathway has been associated with poor prognosis in several human carcinomas. Current approaches to assess Akt activation rely on intensity-based methods, which are limited by the subjectivity of manual scoring and poor specificity. Here, we report the development of a novel assay using amplified, time- resolved F€ orster resonance energy transfer (FRET), which is highly specific and sensitive and can be adapted to any protein. Using this approach to analyze primary breast tissue microarrays, we quantified levels of activated pAkt at a spatial resolution that revealed molecular heterogeneity within tumors. High pAkt status assessed by amplified FRET correlated with worse disease-free survival. Our findings support the use of amplified FRET to determine pAkt status in cancer tissues as candidate biomarker for the identification of high-risk patients. Cancer Res; 74(18); 1–13. Ó2014 AACR. Introduction Dysregulation of Akt/PKB (protein kinase B) signaling is considered to be a hallmark of many human cancers (1). In cancer, Akt plays a central role in cell proliferation, survival, glucose metabolism, genome stability, and neovascularization (2, 3). Akt also contributes to tumor invasion and metastatic spread by induction of epithelial–mesenchymal transition (4). Breast cancer is the most common malignancy diagnosed in women worldwide (1). In breast cancer, Akt activation is correlated with advanced disease, poor prognosis, reduced patient survival, and resistance to radiotherapy (5, 6). Akt is a member of the AGC family of protein serine/threonine kinases and contains an N-terminal pleckstrin homology (PH) domain, which interacts with PtdIns(3,4)P 2 and PtdIns(3,4,5)P 3 (7). Various mechanisms contribute to activation of the Akt pathway in human tumors, including disruption of PTEN, upregulation of PI3K and mTOR, as well as mutation of Akt itself (8, 9). Stimulation of the EGFR by EGF leads to activation of Akt in a PI3K-dependent manner (1, 10). Because Akt activation is both an early event in tumor progression and also a characteristic of many advanced carcinomas, Akt acti- vation status (as opposed to Akt expression level) may repre- sent a useful prognostic biomarker as well as a predictive biomarker in both adjuvant and metastatic settings (11). The appreciation of functional molecular heterogeneity of tumors has far reaching implications for the development of person- alized medicine and improving tumor biopsy methodologies for predictive biomarkers (12). The assessment of molecular heterogeneity at the protein level has not been extensively reported, in part due to a lack of technologies that can accurately perform this task directly on histologic samples. The accurate quantification of Akt activation status as well as its molecular heterogeneity in patient samples is expected to be highly informative. At present, the detection of endogenous oncoproteins in fixed tumor samples faces several important challenges: (i) the accurate quantification of posttranslational modifications such as phosphorylation; (ii) the simultaneous localization of these oncoprotein epitopes in preserved tissue architecture; and (iii) the acquisition and processing of a large quantity of data in an automated, high-throughput manner. IHC is the most readily available method to assess activation of intracel- lular proteins such as Akt; however, it is limited by the absence of precise quantification and the lack of a standardized scoring system. In addition, it is a "one-site" assay (including fluor- ophore-based confocal assays) producing results that can only be obtained from measuring the intensity of one label at a time, 1 Cell Biophysics Laboratory, Cancer Research UK, London Research Institute, London, United Kingdom. 2 Centre Emotion, H^ opital de la Piti e Salpetriere, Paris, France. 3 Protein Phosphorylation Laboratory, Cancer Research UK, London Research Institute, London, United Kingdom. 4 Experimental Histopathology Laboratory, Cancer Research UK, London Research Institute, London, United Kingdom. 5 Stanford University School of Medicine, Stanford, California. 6 Cancer Division King's College London, London, United Kingdom. 7 Cell Biophysics Laboratory, Unidad de Biofísica (CSIC-UPV/EHU), Sarriena s/n, Leioa, Spain. 8 Ikerbasque, Basque Foun- dation for Science, University of the Basque Country, Sarriena s/n, Leioa, Spain. Note: Supplementary data for this article are available at Cancer Research Online (http://cancerres.aacrjournals.org/). S. Veeriah, P. Leboucher, and J. de Naurois contributed equally to this work. Corresponding Author: Banafsh e Larijani, Cell Biophysics Laboratory, Unidad de Biofísica, Ikerbasque, Basque Foundation for Science, Univer- sity of the Basque Country, Sarriena s/n, 48940 Leioa, Spain. Phone: 34-94-601-8505; Fax: 34-94-601-3360; E-mail: [email protected] doi: 10.1158/0008-5472.CAN-13-3382 Ó2014 American Association for Cancer Research. Cancer Research www.aacrjournals.org OF1 Research. on August 11, 2019. © 2014 American Association for Cancer cancerres.aacrjournals.org Downloaded from Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382
Transcript of High-Throughput Time-Resolved FRET Reveals Akt/PKB...

Integrated Systems and Technologies
High-Throughput Time-Resolved FRET Reveals Akt/PKBActivation as a Poor Prognostic Marker in Breast Cancer
Selvaraju Veeriah1, Pierre Leboucher1,2, Julien de Naurois1,3, Nirmal Jethwa1, Emma Nye4, Tamara Bunting4,Richard Stone4, Gordon Stamp4, V�eronique Calleja1, Stefanie S. Jeffrey5, Peter J. Parker3,6, andBanafsh�e Larijani1,7,8
AbstractDysregulation of the Akt/PKB pathway has been associated with poor prognosis in several human carcinomas.
Current approaches to assess Akt activation rely on intensity-basedmethods, which are limited by the subjectivityof manual scoring and poor specificity. Here, we report the development of a novel assay using amplified, time-resolved F€orster resonance energy transfer (FRET), which is highly specific and sensitive and can be adapted toany protein. Using this approach to analyze primary breast tissue microarrays, we quantified levels of activatedpAkt at a spatial resolution that revealed molecular heterogeneity within tumors. High pAkt status assessedby amplified FRET correlated with worse disease-free survival. Our findings support the use of amplified FRETto determine pAkt status in cancer tissues as candidate biomarker for the identification of high-risk patients.Cancer Res; 74(18); 1–13. �2014 AACR.
IntroductionDysregulation of Akt/PKB (protein kinase B) signaling is
considered to be a hallmark of many human cancers (1). Incancer, Akt plays a central role in cell proliferation, survival,glucose metabolism, genome stability, and neovascularization(2, 3). Akt also contributes to tumor invasion and metastaticspread by induction of epithelial–mesenchymal transition (4).Breast cancer is the most common malignancy diagnosed inwomen worldwide (1). In breast cancer, Akt activation iscorrelated with advanced disease, poor prognosis, reducedpatient survival, and resistance to radiotherapy (5, 6). Akt isa member of the AGC family of protein serine/threoninekinases and contains an N-terminal pleckstrin homology (PH)
domain, which interacts with PtdIns(3,4)P2 and PtdIns(3,4,5)P3(7). Various mechanisms contribute to activation of the Aktpathway in human tumors, including disruption of PTEN,upregulation of PI3K and mTOR, as well as mutation of Aktitself (8, 9). Stimulation of the EGFR by EGF leads to activationof Akt in a PI3K-dependent manner (1, 10). Because Aktactivation is both an early event in tumor progression andalso a characteristic of many advanced carcinomas, Akt acti-vation status (as opposed to Akt expression level) may repre-sent a useful prognostic biomarker as well as a predictivebiomarker in both adjuvant and metastatic settings (11). Theappreciation of functional molecular heterogeneity of tumorshas far reaching implications for the development of person-alized medicine and improving tumor biopsy methodologiesfor predictive biomarkers (12). The assessment of molecularheterogeneity at the protein level has not been extensivelyreported, in part due to a lack of technologies that canaccurately perform this task directly on histologic samples.The accurate quantification of Akt activation status as well asits molecular heterogeneity in patient samples is expected tobe highly informative.
At present, the detection of endogenous oncoproteins infixed tumor samples faces several important challenges: (i) theaccurate quantification of posttranslational modificationssuch as phosphorylation; (ii) the simultaneous localization ofthese oncoprotein epitopes in preserved tissue architecture;and (iii) the acquisition and processing of a large quantity ofdata in an automated, high-throughput manner. IHC is themost readily available method to assess activation of intracel-lular proteins such as Akt; however, it is limited by the absenceof precise quantification and the lack of a standardized scoringsystem. In addition, it is a "one-site" assay (including fluor-ophore-based confocal assays) producing results that can onlybe obtained frommeasuring the intensity of one label at a time,
1Cell Biophysics Laboratory, Cancer Research UK, London ResearchInstitute, London, United Kingdom. 2Centre Emotion, Hopital de la Piti�eSalpetriere, Paris, France. 3Protein Phosphorylation Laboratory, CancerResearch UK, London Research Institute, London, United Kingdom.4Experimental Histopathology Laboratory, Cancer Research UK, LondonResearch Institute, London, United Kingdom. 5Stanford University Schoolof Medicine, Stanford, California. 6Cancer Division King's College London,London,UnitedKingdom. 7Cell Biophysics Laboratory,UnidaddeBiofísica(CSIC-UPV/EHU), Sarriena s/n, Leioa, Spain. 8Ikerbasque, Basque Foun-dation for Science, University of the Basque Country, Sarriena s/n, Leioa,Spain.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
S. Veeriah, P. Leboucher, and J. de Naurois contributed equally to thiswork.
Corresponding Author: Banafsh�e Larijani, Cell Biophysics Laboratory,Unidad de Biofísica, Ikerbasque, Basque Foundation for Science, Univer-sity of the Basque Country, Sarriena s/n, 48940 Leioa, Spain. Phone:34-94-601-8505; Fax: 34-94-601-3360; E-mail:[email protected]
doi: 10.1158/0008-5472.CAN-13-3382
�2014 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org OF1
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

therefore limiting specificity (13). Here, nonspecific antibodybinding cannot be excluded. When using color-based (3,30-diaminobenzidine; DAB) IHC, the sensitivity is an issue andIHC techniques based on fluorescence benefit from sensitivityas much as 1,000 times higher than DAB-based IHC (14, 15). Inthe context of these issues, it is notable that there are con-flicting results for the prognostic significance of Akt activationin primary breast carcinomas using IHC (5, 16).
To address these challenges, we devised a novel methodthat would be sensitive and quantitative, and would alsolend itself to analysis of any molecular pathway. The pos-sibility of detecting molecular heterogeneity in tumors isalso retained by this nonpopulation-based approach, poten-tially a critical parameter in prognosis (17–19). Two maintypes of determinations of F€orster resonance energy transfer(FRET) are possible. These are steady state and time-resolved (detection of fluorophore lifetime) measurements.Time-resolved measurements yield additional informationabout FRET. One of the major advantages of measuringfluorescence lifetime is the fact that it is independent offluorophore concentration, unlike steady state, which isintensity based (20). In contrast with steady state measure-ments, where a change in intensity of the recorded emissionwould be observed, this method becomes prone to artifactsthat lead to overestimation of FRET efficiency. We have usedtime-resolved FRET for sensitive analysis. FRET detected byfluorescence lifetime imaging microscopy (FLIM) has beenproven to be a highly effective method in quantifying thephosphorylation status of intracellular molecules inarchived formalin-fixed paraffin-embedded (FFPE) tumortissue (21–27). Coincidence (two-site) FRET describes themethod of simultaneously labeling a single protein on twodistinct sites with donor- and acceptor-conjugated probes,and detecting the FRET between them. When using two-siteFRET, notwithstanding that this method also relies onantigen-antibody immune complexes (IHC), F€orster's energytransfer is the most efficient when the distance between thetwo antibodies (pAkt and panAkt) is less than 10 nm, withinthe same antigen. Two-site FRET is therefore necessarilymore specific. The method has gained recent popularity dueto its high specificity and its relative insensitivity to intensityartifacts (24, 26). To date studies of endogenous proteinsusing FLIM have been limited because of the lack of sen-sitivity. Our method solves this problem by amplifying thesignal.
In this study, we have developed a high-throughput, quan-titative coincidence amplified FRET assay. This assay com-bines immunofluorescence tyramide signal amplification(TSA) with labeled Fab fragment secondary antibodies tomaximize sensitivity, specificity, and portability. In parallel,we have developed an imaging platform based on a multiplefrequency fluorescence lifetime imagingmicroscope (mfFLIM)and accompanying software to automatically map a tissuemicroarray (TMA), acquire FLIM images, and distinguishbetween regions of interest in cells and tumors, in a high-throughput manner with minimal user supervision. Weapplied this assay to quantify Akt activation status in fixedSKBR3 breast tumor cells as well as FFPE human breast TMAs.
We sought to explore the clinical relevance and molecularmechanisms underlying the activation of Akt in breast carci-noma. Here, we identified that high Akt activation assessed byamplified FRET, but not by IHC, was correlated with poorerprognosis. We were also able to identify molecular heteroge-neity of Akt activation within the same patient. The resultsfrom our study suggest that this new methodology will havedirect clinical applications in guiding targeted therapeuticsand in developing companion diagnostic tools.
Materials and MethodsAntibodies and reagents
Monoclonal primary antibodies, mouse anti-panAkt(40D4; #2920), rabbit anti-P-Akt (pT308; C31E5E; #2965)were obtained from Cell Signaling Technology. IRDye-con-jugated secondary antibodies, goat anti-mouse IgG-IRDye800CW (#926-32210), and goat anti-rabbit IgG-IRDye 680LT(#926-68021) were purchased from LI-COR Biosciences.Affinity-purified Fab fragments antibody conjugate and goatF(ab0)2 anti-rabbit IgG-HRP (#A120-118P) were purchasedfrom Bethyl laboratories. Affinity-purified F(ab0)2 fragmentsantibody, AffiniPure donkey Fab fragment anti-mouse IgG(#715-006-150) were purchased from Jackson ImmunoRe-search. PVDF Immobilon-FL (#IPFL00010) transfer mem-brane was purchased from Millipore Corporation. Odysseyblocking buffer (#927-40000) was purchased from LI-CORBiosciences. Complete, mini protease inhibitor cocktailtablets (#11836153001) were from Roche. Dimethylforma-mide (DMF), sequencing grade (#20673), Peroxidase Sup-pressor (#35000), and Pierce BCA protein assay kit waspurchased from Thermo Fisher Scientific. Amine-reactivedye, Oregon Green 488 NHS-ester (ORG488, #O-6147),DMEM GlutaMAX (#31966021), and TSA kit with AlexaFluor 594 tyramide (#T-20925), Pre-Cast SDS-PAGE gel,NuPAGE Novex 4% to 12% Bis-Tris Gel (NP0335BOX) werepurchased from Invitrogen Life Technologies. PI3K inhibi-tor, InSolution LY294002 (#440204), and EGF (#324831-200UG) were purchased from Calbiochem. PD-10 dyeremoval columns and PD MiniTrap G-25 (#28-9180-07) werepurchased from GE Healthcare Life Sciences.
Conjugation of Fab-fragment with ORG488-NHS dyeOregon Green 488-NHS (ORG488) conjugation to the anti-
mouse–specific Fab secondary antibody (1 mg/mL) was per-formed using NHS (N-Hydroxy Succinimide)-ester conjugationprotocol (22). Briefly, the ORG488-NHS-ester dye (Life Tech-nologies Ltd) was reconstituted in anhydrous DMF to a con-centration of 1 mg/mL and added (125 mg of dye/1 mg ofprotein) to the Fab fragment antibody solution. The reactionmixture was incubated with constant agitation at room tem-perature for 1 hour. Purification of labeled antibodies wasperformed using pre-equilibrated (PBS, pH 7.2) gravity flowPD-10 dye removal columns (GEHealthcare Life Sciences). Theconcentrations of labeled Fab fragment-ORG488 conjugateand the degree of labeling (DOL: 4.01) were calculated on thebasis of the absorbance at 280 and 556 nm (ORG488),respectively.
Veeriah et al.
Cancer Res; 74(18) September 15, 2014 Cancer ResearchOF2
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

Colocalization of endogenous panAkt and pT308 usingFab fragment-based TSA assay in fixed MCF7 and SKBR3cellsA time course (5, 15, 20, and 30 minutes) was performed to
establish the optimum time required for the TSA reaction inMCF7 cells. AFab fragment-based TSA assay was performedusing SKBR3 cells in two 8-well glass chamber slides. The cellson the first and second chamber slides were further incubatedwith species-specific Fab fragment secondary antibodies, Fabanti-mouse ORG488 (20 mg/mL) Fab fragment, and Fab anti-rabbit-HRP (10 mg/mL) conjugate, respectively, for 2 hours atroom temperature. The cells on second chamber slide werethen labeled using Alexa-594 TSA system for 15minutes. At thistime point, the amplification reached a plateau and the signalwas not amplified further. The stained SKBR3 cells weremounted as described in Supplementary Materials and Meth-ods, before inspection using a Zeiss LSM 710 inverted laserscanning confocal microscope.
Colocalization of endogenous panAkt and pT308 usingFab fragment-based (TSA) assay in FFPE-fixed humanbreast tumorTwo identical FFPE breast tumor tissue sections were
dewaxed, rehydrated, and subjected to heat-induced antigenretrieval in TRIS-EDTA (pH 9.0) buffer for 10 minutes. Toquench the background fluorescence signal, these slideswere incubated with fresh sodium borohydride (1 mg/mL inPBS) for 10 minutes at room temperature and blocked with 1%BSA/PBS. The first slide was incubated with primary mouseanti-panAkt (1:50); the second slide was incubated withboth primary mouse anti-panAkt (1:50) and primary rabbitanti-pT308 antibodies (1:200). For both slides, incubation wasovernight at 4�C. Slides were washed three times with PBS. Thefirst slidewas labeledwith anti-mouse FabORG488 (20mg/mL)secondary antibody. The second slide was labeled with anti-mouse Fab ORG488 and anti-rabbit Fab-HRP (10 mg/mL)secondary antibodies, which was then detected by usingAlexa-594-TSA assay. For each immunofluorescent labelingexperiment, a negative control was included by replacing theprimary antibody with BSA at the same volume as the primaryantibody. All tissues samplesweremounted before observationunder a confocal microscope.
High-throughput automatedmultiple frequency domainFLIMThe multiple frequency domain FLIM is a lifetime imaging
microscope from Lambert Instruments modified in a new wayto set up an automated multiple frequency high-throughputlifetime imaging microscope. For details of the algorithmimplementation, see Supplementary Materials and Methods.Lifetime calculation: to improve the precision of the lifetimecalculation within all tumor sectors, we developed an algo-rithm that automatically excludes data below a predefined anduniversally applied threshold, by applying the "active contoursmethod" (28). Data analysis: we determined the FRET efficien-cy (Ef), using the following formula: Ef (%) ¼ [[1 � (tDA/tD)] �100]; where (upon FRET tD/A « tD); tD is donor lifetime and tD/Ais the donor plus acceptor lifetime.
Coincidence amplified FRET assay for quantification ofpAkt (pT308) in human breast FFPE tissue
Amplified FRET assay for quantification of pT308 wasperformed on 4-mmsections of two identical FFPE-fixed breastcancer tissue samples. Following de-waxing and rehydration,sections were subjected to heat antigen retrieval by micro-waving in TRIS-EDTA (pH 9.0) buffer, for 10 minutes at 800 W.Sections were then incubated in freshly prepared sodiumborohydride (1 mg/mL in PBS) buffer for 10 minutes at roomtemperature, followed by blocking with 1% BSA/PBS. Tissuessections were incubated with peroxidase suppressor (ThermoScientific Pierce) for 15minutes. For the amplified FRET assay,the first slide was incubated with mouse anti-panAkt (1:50),and the second slide with mouse anti-panAkt (1:50) and rabbitanti-pT308 (1:200) primary antibodies, overnight at 4�C. Thefirst slide was further immunolabeled with ORG488-conjugat-ed anti-mouse Fab fragment secondary antibody (20 mg/mL).The second slide was immunolabeled with ORG488-conjugat-ed anti-mouse Fab fragment (20 mg/mL) and horseradishperoxidase (HRP)-conjugated anti-rabbit Fab fragment sec-ondary antibody (10 mg/mL), which was detected by usingAlexa-594-TSA assay. As a control to address the specificity ofthe phosphorylation signal, calf intestinal alkaline phosphatase(CIP) was incubated with the tissue sections. CIP (10 U/slide)was diluted in 1�New England Biolabs buffer 3 and incubatedfor 30 minutes at room temperature. Also, the substitution ofthe specific primary antibodies by 1% BSA in tissue sectionswas used as a negative control. These control slides were alsoprepared as described above before mounting all tissues sec-tions with ProLong Gold anti-fade. The donor lifetimes ofORG488 were determined from at least 10 regions of thetumors, each performed in triplicate unless otherwise indicat-ed. The FRET efficiency was calculated as described above.
High-throughput quantification of pAkt (pT308) inhuman breast TMAs by amplified coincidence FRETassay
TMAs containing 230 cores of breast tissue, originating frombiopsies were taken from a large case mix of estrogen receptor(ER)-positive and ER-negative breast cancer patients from thetumor bank at Guys Hospital, London, United Kingdom. Allbiopsies had been taken before treatment, and linked tohistologic and clinical data comprehensively stored in a data-base. These were a consecutive series of breast cancers frompatients diagnosed between 1993–94. Before immunofluores-cence labeling, two identical TMA sections were processed asdescribed above. The coincidence amplified FRET assay wasalso performed as above. Lifetime measurements were per-formed using both donor-labeled and donor plus acceptor-labeled TMAs, for each core. Only samples with donor intensityof at least four times higher than the background intensitywereincluded for FRET efficiency calculations. ThemaximumFRETefficiency of four sectors within each core was calculated, asdescribed above.
Statistical analysisStatistical analysis was performed using the GraphPad
Prism software (GraphPad Prism software). Results are shown
pAkt Is a Poor Prognostic Marker in Breast Cancer
www.aacrjournals.org Cancer Res; 74(18) September 15, 2014 OF3
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

as mean values � SEM. Statistical significance between thegroups was calculated with the Mann–Whitney test (valuesare indicated in the box and whiskers plots; ref. 24, 28).Differences were considered statistically significant whenP � 0.05. Disease-free survival (DFS) was measured as thetime from diagnosis to event or last seen if the patient hadno event. Overall survival (OS) was calculated by the timefrom diagnosis to death or last seen if the patient lived.Potential prognostic factors (for e.g., systemic therapy, radi-ation, mastectomy, and lumpectomy) were analyzed byunivariate and multivariate analysis for prognostic signifi-cance for DFS and OS. DFS and OS rates were estimatedusing the Kaplan–Meier method (24). The differences in thesurvival curves were compared by the log-rank test and thistest was used to assess the HRs. An unpaired t test was usedto compare the average FRET efficiency between ER� andERþ. We compared the patients in the lower two tertileswith those in the upper tertile.
ResultsDevelopment and validation of a novel amplified FRETimaging assay for quantification of endogenous Aktactivation status in SKBR3 cells
We evaluated the binding specificity of human anti-Aktantibodies (panAkt, pT308) by two-color Li-COR Westernblot detecting endogenous Akt in SKBR3 cells (Supplemen-tary Fig. S1). SKBR3 cells were treated with or without thepan PI3K inhibitor, LY294002 (50 mmol/L) for 30 minutes, �EGF (100 ng/mL) for 5 minutes. Cells were lysed and totalprotein lysates evaluated by Li-COR Western blot analysis(Supplementary Materials and Methods). Single bands dem-onstrated specificity of the anti-Akt (panAkt, pT308) anti-bodies (Supplementary Fig. S1A and S1B). Incubating bothpanAkt and pT308 antibodies followed by the addition ofspecies-specific NIR-dye–conjugated secondary antibodies,on a single blot, did not affect the specificity of eitherprimary antibody (Supplementary Fig. S1C). The Li-CORWestern showed that Akt phosphorylation was enhancedby EGF and inhibited by LY294002 in SKBR3 cells (Supple-mentary Fig. S1D). These results confirmed the specificity ofanti-Akt antibodies.
Our assay uses Fab fragments combined with TSA signalamplification; hence we compared the localization of pT308in starved SKBR3 cells, with and without TSA amplification,using labeled Fab fragments. Although an increased plasmamembrane localization of pT308 was visible upon EGFstimulation in nonamplified cells, the signal was greatlyenhanced by TSA amplification. In both cases, the signalwas significantly reduced in EGFþLY treated cells (Supple-mentary Fig. S2A and S2B). Evidently TSA amplificationincreases sensitivity without a corresponding increase inbackground signal.
Because the Fab fragment-based TSA assay resulted in ahigher signal-to-noise, we used this method to investigateendogenous expression and colocalization of panAkt andpT308 in FFPE human breast tumor sections. Confocal imagesshowed a clear colocalization of panAkt and pT308 at theplasma membrane (Supplementary Fig. S2C). The pT308 was
predominantly at the plasmamembrane, indicating specificityof TSA labeling in tissue. Control experiments (SupplementaryFig. S2C) omitting primary antibodies produced a very weaksignal, thus confirming the specificity of the Fab fragment-based TSA system in tissues. To establish the optimum timerequired for the TSA reaction to occur, time courses wereperformed in stimulated MCF7 cells. After 5 minutes, thepT308 signal was very weak, from 10 to 15 minutes the pT308signal increased, before signal saturation was reached at 30minutes. Fifteen minutes were therefore chosen as the opti-mum time for TSA amplification (Supplementary Fig. S3).These results demonstrate that, combined with labeled Fabfragments, TSA amplification can be exploited routinely insamples where the target proteins and their phospho-sites arepoorly expressed.
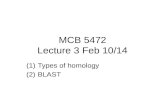
We next exploited the Fab fragment-based TSA assay todevelop a more sensitive and generic coincidence FRET assay,to measure Akt activation in cells and tumor sections. Resultsare presented as FRET efficiency (Ef; Materials and Methods).Higher Ef indicates increased Akt phosphorylation. Figure 1Ashows a schematic of ourmfFLIM,whichwe use to detect time-resolved FRET. Figure 1B shows the principle of the coinci-dence amplified FRET assay using Fab fragment secondaryantibodies.
Cellswere starved or EGF stimulatedwith orwithout LY, andfixed according to the amplified FRET protocol. Figure 1C (firstpanel) shows that the lifetime map of cells labeled with donor(panAkt) alone did not change upon EGF stimulation. How-ever, the lifetime of the cells labeled with both donor andacceptor (pT308) decreased and hence the average FRETefficiency of cells increased upon EGF stimulation (Fig. 1C,second). The detected FRET efficiency was only 7% (Fig. 1C,second). The same coincidence FRET experiment but with TSAamplification showed an increase in FRET efficiency (Ef > 16%)with EGF, clearly visible at the plasmamembrane, as seen fromthe lifetime map images. This is indicative of a significantincrease in pT308 at the plasma membrane (Fig. 1D), demon-strating that TSA amplification significantly improved thedynamic range of the FRET efficiency. These results demon-strate that the amplifiedFRETassay canquantify the activationstatus of endogenous Akt in fixed cells with a high sensitivityand specificity.
QuantificationofAkt activation status by amplifiedFRETin fixed FFPE human breast tumors
After optimizing amplified FRET in SKBR3 cells, we assessedactivated Akt in FFPE breast cancer patient samples. For theseexperiments, we used the high-throughput mfFLIM platformto acquire images and analyze automatically the average FRETefficiencies. The average FRET efficiency varied from 2.5% to6.0%, suggesting that our amplified FRET assay is able to detectthe variation in the activation status of Akt between patients(Fig. 2A, right). Control experiments were performed with CIPto nonspecifically dephosphorylate any phospho-proteinspresent (Fig. 2B). The FRET efficiency was significantlyreduced from 6.0% to 1.5%, confirming the specificity of theamplified FRET assay toward phosphorylated proteins in fixedtissue.
Veeriah et al.
Cancer Res; 74(18) September 15, 2014 Cancer ResearchOF4
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

Sample
Imageintensifier
CCDCamera
Emissionfilter
Excitationfilter
Computer
Signal generator
Light source
Phase frequency
20–100 MHz
515-nm laser
473-nm laser
Wavelength
Signalswitch
Las
er s
wit
ch
DichroicMirror TIRF
FRET (<9 nm)
Akt/PKBP
= mouse a-panAkt = Fab a-mouse-ORG488
= Fab a-rabbit-HRP
= TSA-ALX594
= rabbit a-pAkt (pT308)
Amplified FRET using labeled Fab fragments
FRET using labeled Fab fragments
panAkt (donor)
panAkt (donor)
panAkt (donor) + pT308 (acceptor)
panAkt (donor) + pT308 (acceptor)
Intensity
Intensity Intensity
IntensityLifetime map
Lifetime map Lifetime map
Lifetime map
(+)
LY +
EG
F(+
) LY
+ E
GF
(+)
EG
F(+
) E
GF
(-)
EG
F(-
) E
GF
FR
ET
eff
icie
ncy
(%
)F
RE
T e
ffic
ien
cy (
%)
FR
ET
eff
icie
ncy
(%
)F
RE
T e
ffic
ien
cy (
%)
25
20
15
10
5
0
−5
25
20
15
10
5
0
−5
25
20
15
10
5
0
−5
25
20
15
10
5
0
−5
(−) E
GF(+)
EGF
(+) LY
, EGF
(−) E
GF(+)
EGF
(+) LY
, EGF
(−) E
GF(+)
EGF
(+) LY
+ E
GF
(−) E
GF(+)
EGF
(+) LY
+ E
GF
ns ns
ns ns
panAkt
panAkt
panAkt + pT308
panAkt + pT308
1.2 1.8 2.2 2.6 3.0
A
C
B
D
Figure 1. Quantification of endogenous pAkt (pT308) in fixed SKBR3 cells shows significantly higher dynamic range of FRET efficiency by amplified FRET. A,schematic diagram of the mfFLIM experimental setup. B, schematic diagram showing the principle of the amplified FRET assay. Akt is labeled with primaryantibodies on site 1 (panAkt) and site 2 (pT308). Fab fragments are used as secondary antibodies, conjugated to ORG488 (donor) or HRP/TSA-ALX594(acceptor). C, SKBR3 cells were pretreated with LY294002 (50 mmol/L) for 30 minutes before EGF stimulation (100 ng/mL) for 6 minutes as indicated. Thepanels show the intensity images and lifetimemaps of the donor alone (panAkt) or donorþ acceptor (panAktþ pT308). Fab-ALX495was used as acceptor. D,same experiment as in C but with TSA signal amplification (blue, low FRET efficiency; red, high FRET efficiency). FRET efficiencies are also shown asbox, andwhiskers plots represent themean�SEM for at least twenty different cells. (���,P < 0.0001; ns, not significant). Box andwhiskers plots represent themean � SEM of the FRET efficiency (���, P < 0.0001; ns, not significant).
pAkt Is a Poor Prognostic Marker in Breast Cancer
www.aacrjournals.org Cancer Res; 74(18) September 15, 2014 OF5
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

panAkt (donor) panAkt (donor) + pT308 (acceptor)
panAkt (donor) + pT308 (acceptor)
panAkt (donor) + pT308 (acceptor)
Intensity
Intensity
IntensityLifetime map
Lifetime map
Lifetime mapP
atie
nt
1P
atie
nt
2P
atie
nt
3
(+)
CIP
(+)
CIP
(-)
CIP
panAkt (donor)
A
B
FR
ET
eff
icie
ncy
(%
)F
RE
T e
ffic
ien
cy (
%)
FR
ET
eff
icie
ncy
(%
)
FR
ET
eff
icie
ncy
(%
)
8
6
4
2
0
−2
8
6
4
2
0
−2
8
6
4
2
0
−2
8
6
4
2
0
−2
panAkt
panAkt
panAkt
+ p
T308
panAkt
+ p
T308_
(-) C
IP
panAkt
+ p
T308_
(+) C
IP
2.5 2.7 2.9 3.1 3.1
Figure 2. Quantification of endogenous pAkt (pT308) in fixed FFPE human breast tumor using amplified FRET. A, intensity images and lifetime maps (scalesare relative and in pseudo-color) of FFPE human breast tumors from three different patients labeled with donor alone (panAkt) or donor þ acceptor(panAktþ pT308). FRET efficiencies are shown as a box, and whiskers plots represent themean� SEM for at least ten different regions from the same tissuesection (���, P < 0.0001). The increased FRET efficiency represents the phosphorylation status of endogenous Akt and shows the variability frompatient to patient. B, tissue sections were treated with CIP (10 U/slide) for 30 minutes, then labeled with panAkt or panAkt þ pT308. FRET efficienciesare shown as a box, and whiskers plot represents the mean � SEM for at least ten different regions from the same tissue section (���, P < 0.0001).
Veeriah et al.
Cancer Res; 74(18) September 15, 2014 Cancer ResearchOF6
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

Molecular heterogeneity of pAkt (pT308) expression inhuman breast tumors by amplified FRETTomap and quantify the molecular heterogeneity of the Akt
activation status within patient tumors, we prepared TMAsfrom breast tumor biopsies obtained from ten patients. Thesepatients had a variable ER and HER2 expression status. Foreach patient, four cores were selected from different regionswithin each biopsy. Hematoxylin and eosin (H&E) stainingconfirmed that each core contained tumor tissue (Fig. 3A).In total there were 40 tumor cores per TMA (i.e., 4 cores � 10patients). TMAs were labeled with anti-Akt (panAkt, pT308)primary antibodies, followed by TSA amplification.We used the mfFLIM platform to map the position of each
core on the TMA, automatically acquire images, and analyzethe FRET efficiencies. The software randomly segments eachtumor core into four sectors (shown in Fig. 3A). The intensityand the corresponding FLIM images are shown for all coresin Fig. 3B and C. The maximum FRET efficiency value of thefour sectors is shown in Fig. 3D. We detected that there wassignificant variability in Akt activation between patients (e.g.,between patient 1 and patient 5); and also between cores fromthe same patient, representing different regions of the sametumor (e.g., patient 8; Fig. 3D).Averaging the FRET efficiency of the four cores resulted in
a loss of localized information reporting on the activationstatus of Akt (Fig. 3D, inset). These results demonstrate thecoexistence of high and low FRET efficiency in differentregions of the same patient biopsy, demonstrating molecularheterogeneity of the activation status of Akt within breasttumors. Hence, analysis of localized FRET efficiency iscritical in breast tumors to avoid loss of potentially valuableinformation.
Prognostic value of pAkt expression in human breastcancers assessed by high-throughput—amplified FRETversus intensity-based IHCThe main objective here in exploiting this analytical plat-
form was to assess the prognostic value of pAkt in primarybreast carcinomaand compare the resultswith intensity-basedIHC (calculated as the intensity ratio of pT308 divided bypanAkt). A broad case mix of tumor samples representing230 patients was obtained from King's Health Partners TumorBank in TMA format, with linked 15-year follow-up clinicaldata. The casemix consisted of 76% of tumors ERþ and 24% ER(�) with amix of grade 1, grade 2, and grade 3 tumors (Table 1).The presence of tumor tissue (>50%) was confirmed by H&Estaining for each breast tumor core (Fig. 4A). The TMAs werefixed and stained according to the amplified FRET protocol.Using the automated FLIM platform, wemapped and acquiredimages from each tumor core position. It is important to notethat our software enabled the rapid acquisition and analysis of230 tumor cores with minimal intervention, thereby removinga large amount of human error and subjectivity from thesample analysis. The differences in Akt activation status ofhistologically homogeneous and heterogeneous samples canbe appreciated in Fig. 4B (right). We used normal breast tissueto assess the basal FRET efficiency as a negative control. Thebasal FRET efficiency values ranged from 2.3% to 5.7% with
median average FRET efficiency of 4% (Supplementary Fig.S7). Figure 4B (bar graphs) shows the variability of FRETefficiency between the four sectors from the same patient, aswell as between different patient cores, ranging from low (3.9%)to a high (25.1%) FRET efficiency. Figure 4C illustrates themaximum FRET efficiency of each tumor core, arranged fromhigh (27.8%) to low (0.5%), indicating the high dynamic range ofthe amplified FRET assay.We investigated whether there was arelationship between pAkt status assessed by amplified FRET(black dots) and by intensity ratio (gray dots). The linearregression showed there was no correlation between the twomethods.
We then evaluated the prognostic value of Akt activationassessed by amplified FRET compared with intensity ratio in164 cases, consisting of 125 ERþ and 39 ER (�) tumors. Patientswere ranked according to their FRET efficiency or intensityratio, and split into two groups for comparison, upper tertile(high pAkt) and lower two tertiles (low pAkt). Fifteen years ofclinical follow-up data were used to generate Kaplan–Meierplots for DFS and OS, to compare the two groups (Fig. 5).Whenassessed by amplified FRET, high pAkt significantly correlatedwith reduced DFS [P ¼ 0.036, HR ¼ 0.634; 95% confidenceinterval (CI), 0.385–0.694)] and OS (P¼ 0.013, HR¼ 0.570; 95%CI, 0.331–0.876) compared with low pAkt (Fig. 5A and B).Importantly, when assessed by intensity ratio, high pAkt wasnot associated with reduced DFS (P ¼ 0.890, HR ¼ 0.699; 95%CI, 0.616–1.521) or OS (P ¼ 0.746, HR ¼ 1.082; 95% CI, 0.670–1.750) compared with low pAkt (Fig. 5C and D).
We studied the ERþ subgroup separately (n ¼ 125),splitting this cohort into high and low pAkt groups as before.As shown in Fig. 6A and B, when assessed by amplified FRET,there was a significant association between high pAkt andreduced DFS (P ¼ 0.029, HR ¼ 0.566; 95% CI, 0.299–0.936)and OS (P ¼ 0.033, HR ¼ 0.284; 95% CI, 0.284–0.946). Incontrast, using the intensity ratio, high pAkt was not asso-ciated with DFS (P ¼ 0.800, HR ¼ 0.932; 95% CI, 0.535–1.618)or OS (P¼ 0.759, HR¼ 1.098; 95% CI, 0.607–1.983; Fig. 6C andD). Moreover, patient age (mean 60 years) did not seem tocorrelate with the poor DFS or OS (Supplementary Fig. S6D).Furthermore, 11 factors of potential prognostic significancewere evaluated by univariate analysis (see Table 2). The dataanalysis revealed that increased Ef of pAkt associatedwith diminished OS (P ¼ 0.041) but not with intensity ratio(P ¼ 0.218; Table 2). In the univariate analyses, the histologygrade was the most significant independent prognosticfactor for DFS and OS. These findings show that FRETefficiency, as an indicator of Akt activation status, but notintensity ratio, predicts poorer DFS and OS in patients withERþ primary breast carcinoma.
In conclusion, these results highlight that, using amplifiedFRET (but not the IHC intensity ratio), high Akt activation inprimary breast carcinoma predicts poorer outcome in thesepatients.
DiscussionThe direct quantification of the activation state of endog-
enous proteins in cells or in tissue using a coincidence FRETassay has been a challenge (24, 29). Previously we have
pAkt Is a Poor Prognostic Marker in Breast Cancer
www.aacrjournals.org Cancer Res; 74(18) September 15, 2014 OF7
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

conjugated dyes directly to primary antibodies to obtainsufficient signal to monitor endogenous biomarker activation(24). However, we encountered several limitations: First, theconjugation process can result in the presence of multiple dyemolecules at the antigen recognition site, with adverse con-sequences on antibody-antigen specificity (30). Second, thesignal obtained is limited by the maximum number of dyemolecules that can be bound to each antibody molecule whilemaintaining epitope recognition (22). Third, cost becomes alimiting factor due to the large amount of primary antibodiesrequired for dye conjugation, making routine screening ofoptimum antibody pairs prohibitive. This is compounded bythe fact that commercially available labeled primary antibodieswith compatible FRET pairs are difficult to find (30).
With these considerations in mind, we designed a coin-cidence FRET assay compatible with labeled secondaryantibodies. Using pairs of whole secondary antibodies (IgG)is not appropriate for FRET as the dimensions of theIgG (150–180 kDa) result in donor-acceptor fluorophoredistances above 10 nm, with a consequent loss of FRET(Supplementary Fig. S4). In contrast with whole IgG, Fabfragments have several important advantages: (i) due totheir small size (50–100 kDa), they remain within the 10-nm FRET limit; (ii) they penetrate more easily fixed samplesand bind to their targets (31); and (iii) they lack the Fcregion, therefore any background that results from nonspe-cific binding to endogenous Fc receptors is abolished (32).The use of Fab fragments permits us to use any
Breast tissue 40 cores from 10 breast tumor patients
Four regions
Sector_1 Sector_2
Sector_3Sector_4
×4 ×10
×20
×40
4321
1
2
3 4
panAkt (donor)
panAkt (donor) + pT308 (acceptor)In
ten
sity
Inte
nsi
tyL
ifet
ime
map
Lif
etim
e m
apPatients
Patients
1 2 3 4 5 6 7 8 9 10
1 2 3 4 5 6 7 8 9 10
2-mm
core
TM
A
A B
D C
1.6 2.0 2.2 2.4 2.8
1.6 2.0 2.2 2.4 2.8
FR
ET
eff
icie
ncy
(%
)
FR
ET
eff
icie
ncy
(%
)24
21
18
15
12
9
6
3
0
24
21
18
15
12
9
6
3
0
Patien
t 1
Patient 1 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8 Patient 9 Patient 10Patient 2
Patien
t 2
Patien
t 3
Patien
t 5
Patien
t 6
Patien
t 7
Patien
t 8
Patien
t 9
Patien
t 10
Patien
t 4
Co
re 1
Co
re 2
Co
re 3
Co
re 4
Co
re 5
Co
re 6
Co
re 7
Co
re 8
Co
re 9
Co
re 1
0C
ore
11
Co
re 1
2C
ore
13
Co
re 1
4C
ore
15
Co
re 1
6C
ore
17
Co
re 1
8C
ore
19
Co
re 2
0C
ore
21
Co
re 2
2C
ore
23
Co
re 2
4C
ore
25
Co
re 2
6C
ore
27
Co
re 2
8C
ore
29
Co
re 3
0C
ore
31
Co
re 3
2C
ore
33
Co
re 3
4C
ore
35
Co
re 3
6C
ore
37
Co
re 3
8C
ore
39
Co
re 4
0
Figure 3. Molecular heterogeneity of Akt activation in human breast TMA revealed by amplified FRET. A, H&E staining of breast TMAs prepared from breasttumor biopsiesobtained from tenpatients. For eachpatient, four cores (circles 1–4)were selected fromdifferent regionswithin eachbiopsy. In total, forty tumorcores (4�10patients)were spotted tomake theTMA. Thebottom imageshowsanexpandedviewof onecoredivided into four sectors for further analysis. Thepanels on the right show three different magnifications of sector 4. Intensity images and lifetime maps (scales are relative and in pseudo-color; ns,nanoseconds) of the TMAs stained with panAkt (B) or panAkt þ pT308 (C), followed by TSA- amplification. TMAs were mapped and images automaticallyacquired using our FRET/FLIM platform. D, for each patient, the maximum FRET efficiency of each core is shown; inset, for each patient the mean FRETefficiency for the four cores is shown.
Veeriah et al.
Cancer Res; 74(18) September 15, 2014 Cancer ResearchOF8
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

commercially available primary antibodies, potentiallyextending the use of our assay to assess the activation ofany signaling pathway in the cell.In addition, we exploited TSA to increase the detection
threshold for very weakly expressed proteins (33). We firstconfirmed that TSA amplification resulted in an increasein intensity when detecting pT308 in SKBR3 cells. Theincreased intensity was not accompanied by an increase in
background (Supplementary Fig. S2). Refinements to ouroriginal FRET assay (24) allowed us to quantify the low levelsof endogenous pAkt in breast cancer tissue (Fig. 2).
Other non-FRET coincidence assays that quantify proteincomplex formation or posttranslational proteinmodifications,such as the in situ proximity ligation assay (PLA), are poten-tially able to detect molecules within 30 to 40 nm of oneanother (34). However, due to the 10-nm range, FRET will onlyoccur between directly interacting proteins or a posttransla-tional modification on the same protein (35). We tested the insitu PLA in FFPE breast tissue but we were unable to quantifythe pT308 due to the low dynamic range in the context of thenonspecific background observed with PLA in these Akt assays(unpublished data).
Breast cancer is heterogeneous at both the histologic andmolecular levels (17). A better understanding of tumor hetero-geneity at the molecular level among a large cohort of patientswill aid to identify the subgroups who respond more favorablyto chemotherapy or targeted therapy (18). We prepared TMAsfrom breast tumor biopsies. We also tested the capability ofthe amplified FRET assay to detect the molecular heterogeneityof Akt activation in colon TMAs prepared from seven patients(Supplementary Fig. S5). In both tissues, we were able to detectmolecular heterogeneity of Akt activation between differentregions of the same tumor. In addition, we observed the hetero-geneity of Akt activation in some breast tumor cores whencomparing the FRET efficiencies of adjacent sectors (Fig. 4B),highlighting the spatial resolution of our imaging platform.
Several studies have attempted to determine the prognosticvalue of Akt activation in breast cancer using IHC, with varyingresults (5, 16). We obtained TMAs representing 164 primaryhuman breast tumors representative of breast cancer subtypestreated in tertiary referral centers. We used amplified FRET/FLIM platform and also the IHC intensity ratio to investigatewhether pAkt might be associated with poor prognosis todemonstrate the validity of both methods. In a recent study,Tokunaga and colleagues demonstrated that high levels ofpAkt assessed by IHC failed to demonstrate prognostic value inpatients with breast cancer before hormone therapy (16).Consistent with these findings, our results using the IHCintensity ratio in breast TMAs did not show an associationbetween Akt activation and DFS or OS (Fig. 5C and D and Fig.6C and D). However, contrary to these limited methodologies,we show by coincidence amplified FRET that in primary breastTMAs, there was a significant difference between high and lowpAkt groups in terms of DFS and OS. This applies to the totalgroup of 164 patients [comprising ER(þ) and ER(�); Fig. 5Aand B], aswell as for the 125 ER(þ) patients (Fig. 6A and B). Thecoincidence amplified FRET assay is therefore a promisingapproach for assessing protein activation compared withtraditional IHC. Our data confirm that enhancedAkt activationin primary breast carcinoma patients is associated with worseprognosis. Because we have shown that high pAkt is associatedwith reduced survival, we postulate that patients with highpAkt might be suitable candidates for the targeted PI3K/Aktpathway inhibitors.
We observed that Akt activation was significantly higher inER (�) than in ER (þ) patients when assessed by coincidence
Table 1. Patient characteristics for breast TMAsamples and mean FRET efficiency
Median age 57.0Median FRET efficiency 11.8Median intensity ratio (pT308/panAkt) 1.7Grade %Grade 1 17.1Grade 2 31.7Grade 3 42.7Unknown 7.9
ER %ERþ 76.2ER� 22.0Unknown 1.8
PR %PRþ 55.5PR� 42.7Unknown 1.8
HER2 %HER2þ 9.1HER2� 37.2Unknown 53.7
Adjuvant therapy %Adjuvant therapy (total) 86.0Tamoxifen 62.8CMF þ tamoxifen 12.8CMF 8.5None 5.5EFC 3.7Ov Abl þ tamoxifen 2.4FEC þ tamoxifen 2.4Ov abl 1.2APD 0.6
Surgery %Mastectomy 44.5Conservation 55.5
Radiation therapy %Yes 55.5No 44.5
Abbreviations: ECF, epirubicin, cisplatin, and continuousinfusion 5-fluorouracil; CMF, cyclophosphamide, metho-trexate, and 5-fluorouracil; FEC, fluorouracil, epirubicin, andcyclophosphamide; APD, aprepitant, palonosetron, anddexamethasone.
pAkt Is a Poor Prognostic Marker in Breast Cancer
www.aacrjournals.org Cancer Res; 74(18) September 15, 2014 OF9
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

250 Cores from 250 breast tumor patients
Sector _1 Sector _2
Sector _4 Sector _3
×40
×20
×10×4
panAkt (donor) panAkt (donor) + pT308 (acceptor)Intensity IntensityLifetime map Lifetime map
Heterogeneous ROI with high FRET efficiency
Homogeneous ROI with high FRET efficiency
Homogeneous ROI with low FRET efficiency
e.g
., P
atie
nt
3e.
g.,
Pat
ien
t 2
e.g
., P
atie
nt
1
1 2
4 3
1 2
4 3
1 2
4 3
FR
ET
eff
icie
ncy
(%
)F
RE
T e
ffic
ien
cy (
%)
FR
ET
eff
icie
ncy
(%
)
FR
ET
eff
icie
ncy
(%
)
FRET efficiency (%)
Int.Ratio (pT308/panAkt)
30
20
10
0
30
20
10
0
30
20
10
0
panAkt
panAkt
panAkt
panAkt + pT308
panAkt + pT308
panAkt + pT308
1 2 43 1 2 3 4
1 2 43 1 2 3 4
1 2 43 1 2 3 430
25
20
15
10
5
0Patient (n = 164)
Int.R
atio (p
T308/p
anA
kt)
5
4
3
2
1
0
R 2 = 0.3414
1-mm
core
TM
A
1 2
4 3
1
4 3
34
1 2
2
A
B
C 1.0 1.6 2.2 2.4 2.8
Figure 4. High-throughput quantification of Akt activation in human breast TMAusing amplified FRET/FLIMplatform. A, H&E staining of breast TMAs preparedfrom breast tumor biopsies obtained from 250 patients. Each core is a representative tissue sample from a single patient. The panels on the right show threedifferent magnifications of sector 4. B, intensity images and lifetime maps (scales are relative and in pseudo-color; ns, nanoseconds) of the TMAs stainedwith panAkt alone or panAkt þ pT308, followed by TSA amplification. TMAs were mapped and images automatically acquired using our FRET/FLIMplatform. The three graphs present the FRET efficiency of each sector of the same patient core, for three representative patients. C, patients were orderedby descending FRET efficiency. For each patient, we plotted the FRET efficiency (black dots, left y-axis) and the intensity ratio (gray dots, right y-axis). Theregression line for the intensity ratio (gray line, R2 ¼ 0.3414) is shown for comparison with FRET efficiency.
Veeriah et al.
Cancer Res; 74(18) September 15, 2014 Cancer ResearchOF10
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

amplified FRET but not by IHC intensity ratio (SupplementaryFig. S6E and S6F). A higher proportion of ER (�) patients hadhigh pAkt compared with the ER (þ) patients (SupplementaryFig. S6G). This result suggests that ER-independent signalingpathways are involved in the activation of Akt. Finally, weobserved that amongst ER (�) patients, more than half exhib-ited high Akt activation, compared with one third of ER (þ)patients (Supplementary Fig. S6H). We suggest that the ERþ
population may benefit from stratification based on a mea-sured value of Akt activation. Currently, ER (þ) breast tumorsare treated with hormone-based therapy—this could be sup-plemented with targeted Akt inhibition for those patients withhigh Akt activity. In contrast, stratification of ER (�) patientswould allow the introduction of Akt inhibition to a subset ofpatients who, until now, have not had many targeted thera-peutic options.In summary, we have designed and evaluated an original
coincidence FRET assay, which combines signal amplificationwith the flexibility of labeled secondary antibodies. This pro-vides a highly sensitive, specific, and portable methodology forthe quantification of low levels of endogenous protein activa-tion in a wide range of signaling pathways. In parallel, we havedeveloped a high-throughput FRET/FLIM imaging platformcapable ofmapping TMAs, automatically acquiring images andprocessing FRET data, requiring minimal intervention from a
nonspecialist user. The instrument is suitable for furtherdevelopment in a clinical setting. Moreover, the TMA samplepreparation was 2 days (identical to classical IHC), whichinvolves antigen retrieval, antibody incubation, and rinsing/washing. Acquisition of lifetime to calculate FRET using theFLIM involves a day's work, in our case for 230 samples in TMA.Steps include mapping of samples, followed by calculation ofthe FRET efficiency, which is performed by the automatedalgorithm. In our case, for 230 samples, the interpretation timetook an hour. This compares very favorably with the interpre-tation time required by a pathologist to manually scorea similar number of samples labeled with classical IHCtechniques.
We have shown that, in primary breast carcinoma, high Aktactivation measured by amplified FRET (but importantly, notby IHC intensity ratio) was correlated with poorer DFS and OS.The method applied was able to quantify heterogeneity of Aktactivation at two levels: (i) between multiple cores taken fromdifferent regions of the same tumor (>2 mm range), and (ii)between sectors of a single tumor core (<1 mm range). Themethodology worked equally well when used to analyze othertissue types such as colon carcinoma. This assay is able todirectly monitor Akt pT308 as a read-out of protein activationin both cells and FFPE breast tissue, and could be used moregenerally to monitor posttranslational modifications or
Figure 5. Kaplan–Meier survivalcurves for all patients with breastcarcinoma (ER�/ERþ) comparinghigh and low Akt activation.Kaplan–Meier survival plotsdemonstrating DFS (A) and OS (B)of patients with high Akt activation(upper tertile, red) or low Aktactivation (lower tertiles, blue) asdetermined by amplified FRET.Results of log-rank tests areshown.CandD, the correspondingresults when Akt activation isassessed by intensity ratio(calculated as pT308 divided bypanAkt intensity).
www.aacrjournals.org Cancer Res; 74(18) September 15, 2014 OF11
pAkt Is a Poor Prognostic Marker in Breast Cancer
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

protein–protein interactions in any signaling pathway.The ability to accurately quantify oncoprotein activation hasseveral major implications for translational medicine, in par-ticular: drug screening in tissue culture; the discovery andvalidation of prognostic and predictive biomarkers; patientstratification based on oncoprotein activation; and validating
the mode of action of drug inhibition, for example, duringneoadjuvant therapy or window trials.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: S. Veeriah, P. Leboucher, J. de Naurois, P.J. Parker,B. LarijaniDevelopment of methodology: S. Veeriah, P. Leboucher, J. de Naurois,N. Jethwa, P.J. Parker, B. LarijaniAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): S. Veeriah, P. LeboucherAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): S. Veeriah, P. Leboucher, J. de Naurois, G. Stamp,S.S. Jeffrey, P.J. Parker, B. LarijaniWriting, review, and/or revision of themanuscript: S. Veeriah, J. de Naurois,N. Jethwa, G. Stamp, P.J. Parker, B. LarijaniAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): S. Veeriah, P. Leboucher, J. de Naurois,N. Jethwa, E. Nye, T. Bunting, R. Stone, G. Stamp, B. LarijaniStudy supervision: S. Veeriah, J. de Naurois, B. LarijaniOther (participated in the creation of themixed tissue array, cut sectionson the microtome, and provided technical assistance): T. BuntingOther (scientific discussion): V. Calleja, S.S. Jeffrey
AcknowledgmentsThe authors thank the King's Health Partners Tumor Bank for the case mix
samples, Christopher J. Applebee for themechanical set up of themfFLIM and itshardware optimizations, Richard D. Byrne in Cell Biophysics Laboratory for
Figure 6. Kaplan–Meier survivalcurves comparing high and low Aktactivation for ERþ breastcarcinoma patients. Kaplan–Meiersurvival plots demonstrating DFS(A) and OS (B) of patients with highAkt activation (upper tertile, red) orlow Akt activation (lower tertiles,blue) as determined by amplifiedFRET. Results of log-rank tests areshown.C andD, the correspondingresults when Akt activation isassessed by intensity ratio(calculated as pT308 divided bypanAkt intensity).
Table 2. Univariate analysis of factorsassociated with prognostic significance
Variable P (OS) P (DFS)
Histology grade 0.000 0.000DIAG no path nodes 0.701 0.702ER status 0.066 0.116PR status 0.006 0.011HER2 status 0.327 0.634Tumor size 0.010 0.005Adjuvant therapy 0.009 0.003Surgery 0.104 0.131Radiotherapy 0.028 0.040Int. ratio (A/D) 0.218 0.248FRET tertiles 0.041 0.149
Cancer Res; 74(18) September 15, 2014 Cancer ResearchOF12
Veeriah et al.
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

many helpful discussions, and Dr. Gavin Kelly (Department of Bioinformaticsand Biostatistics, Cancer Research UK, LondonResearch Institute) for univariateanalysis of the prognostic factors using R.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby marked
advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate thisfact.
Received December 3, 2013; revised June 2, 2014; accepted June 19, 2014;published OnlineFirst June 26, 2014.
References1. Bellacosa A, Kumar CC, Di Cristofano A, Testa JR. Activation of AKT
kinases in cancer: implications for therapeutic targeting. Adv CancerRes 2005;94:29–86.
2. Chin YR, Toker A. Function of Akt/PKB signaling to cell motility,invasion and the tumor stroma in cancer. Cell Signal 2009;21:470–6.
3. Scheid MP, Woodgett JR. PKB/AKT: functional insights from geneticmodels. Nat Rev Mol Cell Biol 2001;2:760–8.
4. Grille SJ, BellacosaA,Upson J, Klein-Szanto AJ, vanRoy F, Lee-KwonW, et al. The protein kinase Akt induces epithelial mesenchymaltransition and promotes enhanced motility and invasiveness of squa-mous cell carcinoma lines. Cancer Res 2003;63:2172–8.
5. Kirkegaard T, Witton CJ, McGlynn LM, Tovey SM, Dunne B, Lyon A,et al. AKT activationpredicts outcome inbreast cancer patients treatedwith tamoxifen. J Pathol 2005;207:139–46.
6. Li H-F, Kim J-S, Waldman T. Radiation-induced Akt activation mod-ulates radioresistance in human glioblastoma cells. Radiat Oncol(London, England) 2009;4:43.
7. Thomas CC, Deak M, Alessi DR, van Aalten DMF. High-resolutionstructure of the pleckstrin homology domain of protein kinase b/aktbound to phosphatidylinositol (3,4,5)-trisphosphate. Curr Biol 2002;12:1256–62.
8. Carpten JD, Faber AL, Horn C, Donoho GP, Briggs SL, Robbins CM,et al. A transforming mutation in the pleckstrin homology domain ofAKT1 in cancer. Nature 2007;448:439–44.
9. Sarbassov DD, Guertin DA, Ali SM, Sabatini DM, D Sarbassov D, AGuertin D, et al. Phosphorylation and regulation of Akt/PKB by therictor-mTOR complex. Science 2005;307:1098–101.
10. Heeg S, Hirt N, Queisser A, Schmieg H, ThalerM, Kunert H, et al. EGFRoverexpression induces activation of telomerase via PI3K/AKT-medi-ated phosphorylation and transcriptional regulation through Hif1-alpha in a cellular model of oral-esophageal carcinogenesis. CancerSci 2011;102:351–60.
11. Wong K-K, Engelman JA, Cantley LC. Targeting the PI3K pathwayin cancer. Current Opinion in Genetics and Development 2010;20:87–90.
12. Gerlinger M, Rowan AJ, Horswell S, Larkin J, Endesfelder D, GronroosE, et al. Intratumor heterogeneity and branched evolution revealed bymultiregion sequencing. N Engl J Med 2012;366:883–92.
13. Simon R, Mirlacher M, Sauter G. Immunohistochemical analysis oftissue microarrays. Methods Mol Biol (Clifton, NJ) 2010;664:113–26.
14. Davies J. Introduction to Immunocytochemistry. J Anat 2003;202:251–2.
15. Guibault GG, ed. Practical Fluorescence. Vol 3. Boca Raton, Florida:CRC Press, 1990.
16. Tokunaga E, Kimura Y, Oki E, Ueda N, Futatsugi M, Mashino K, et al.Akt is frequently activated in HER2/neu-positive breast cancers andassociated with poor prognosis among hormone-treated patients. IntJ Cancer 2006;118:284–9.
17. Bertucci F, Birnbaum D. Reasons for breast cancer heterogeneity.J Biol 2008;7:6.
18. Polyak K. Heterogeneity in breast cancer. J Clin Invest 2011;121:3786–8.
19. Auguin D, Barthe P, Aug�e-S�en�egas M-T, Stern M-H, Noguchi M,Roumestand C. Solution structure and backbone dynamics of thepleckstrin homology domain of the human protein kinase B (PKB/Akt). Interaction with inositol phosphates. J Biomol NMR 2004;28:137–55.
20. Calleja V1, Leboucher P, Larijani B. Protein activation dynamicsin cells and tumor micro arrays assessed by time resolvedF€orster resonance energy transfer. Methods Enzymol 2012;506:225–46.
21. Calleja V, Alcor D, LaguerreM, Park J, Vojnovic B, Hemmings BA, et al.Intramolecular and intermolecular interactions of protein kinaseB define its activation in vivo. PLoS Biol 2007;5:e95.
22. Calleja V, Leboucher P, Larijani B. Protein activation dynamics in cellsand tumor micro arrays assessed by time resolved F€orster resonanceenergy transfer. Methods Enzymol 2012;506:225–46.
23. F€orster T. Zwischenmolekulare Energiewanderung und Fluoreszenz.Annalen der Physik 1948;437:55–75.
24. Kong A, Leboucher P, Leek R, Calleja V, Winter S, Harris A, et al.Prognostic value of an activation state marker for epidermal growthfactor receptor in tissue microarrays of head and neck cancer. CancerRes 2006;66:2834–43.
25. Ng T. Imaging protein kinase C activation in cells. Science 1999;283:2085–9.
26. Pietraszewska-Bogiel A, Gadella TWJ. FRET microscopy: fromprinciple to routine technology in cell biology. J Microsc 2011;241:111–8.
27. Voss TC, Demarco IA, Day RN. Quantitative imaging of protein inter-actions in the cell nucleus. BioTechniques 2005;38:413–24.
28. Vartiainen MK, Guettler S, Larijani B, Treisman R. Nuclear actin reg-ulates dynamic subcellular localization and activity of the SRF cofactorMAL. Science 2007;316:1749–52.
29. Calleja V, Laguerre M, Parker PJ, Larijani B. Role of a novel PH-kinasedomain interface in PKB/Akt regulation: structural mechanism forallosteric inhibition. PLoS Biol 2009;7:1.
30. Vira S, Mekhedov E, Humphrey G, Blank PS. Fluorescent-labeledantibodies: balancing functionality and degree of labeling. Anal Bio-chem 2010;402:146–50.
31. Nelson AL. Antibody fragments: hope and hype. mAbs 2010;2:77–83.
32. Chames P, Van Regenmortel M, Weiss E, Baty D. Therapeutic anti-bodies: successes, limitations andhopes for the future.Br JPharmacol2009;157:220–33.
33. Toda Y, Kono K, Abiru H, Kokuryo K, Endo M, Yaegashi H, et al.Application of tyramide signal amplification system to immunohis-tochemistry: a potent method to localize antigens that are not detect-able by ordinary method. Pathol Int 1999;49:479–83.
34. S€oderberg O, Gullberg M, Jarvius M, Ridderstra�le K, Leuchowius K-J,
Jarvius J, et al. Direct observation of individual endogenous proteincomplexes in situ by proximity ligation. Nat Methods 2006;3:995–1000.
35. Stryer L. Fluorescence energy transfer as a spectroscopic ruler. AnnuRev Biochem 1978;47:819–46.
www.aacrjournals.org Cancer Res; 74(18) September 15, 2014 OF13
pAkt Is a Poor Prognostic Marker in Breast Cancer
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382

Published OnlineFirst June 26, 2014.Cancer Res Selvaraju Veeriah, Pierre Leboucher, Julien de Naurois, et al. Activation as a Poor Prognostic Marker in Breast CancerHigh-Throughput Time-Resolved FRET Reveals Akt/PKB
Updated version
10.1158/0008-5472.CAN-13-3382doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2014/07/21/0008-5472.CAN-13-3382.DC1
Access the most recent supplemental material at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://cancerres.aacrjournals.org/content/early/2014/08/29/0008-5472.CAN-13-3382To request permission to re-use all or part of this article, use this link
Research. on August 11, 2019. © 2014 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 26, 2014; DOI: 10.1158/0008-5472.CAN-13-3382