Hernias
53
Hernias Prof.Dr.Gamal Karrouf
-
Upload
drgamal-karrouf -
Category
Documents
-
view
750 -
download
6
Transcript of Hernias

Hernias
Prof.Dr.Gamal Karrouf

Definition
• It is the protrusion of a portion of the abdominal contents through an aperture (congenital or normal physiologioal opening or an acquired opening) in the wall of the abdomen to lay beneath the skin which remains intact. Or A hernia comprises the protrusion of an organ or part of an organ through the wall of the cavity normally containing it.

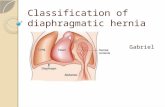
Classification of hernias
: hernia may be classified as direct or indirect, internal or external. A direct hernia occurs through a rent or tears whereas an indirect hernia occurs through natural passage such as the inguinal canal or umbilicus

• 1- External hernias: it occurs through the body wall producing a visible and palpable swelling covered by skin as umbilical H. and Ventral H
• 2- Internal hernias: it occur within the abdominal cavity. As diaphragmatic H.

3-Incisional or postoperative hernias:
• encountered relatively frequently following abdominal surgery. Improper closure of the incision, suture breaking or tearing through tissues, postoperative wound infection, are contributory factors. The weakened abdominal wall undergoes loss of continuity and a hernia develops often a delay of several weeks or months

Parts of the hernia: surgically, a hernia consists of
1- Hernial opening or ring or orifice: it may be accidental rupture in the abdominal wall (ventral H) or a persistent prenatal opening (umbilicus) or normal passage (inguinal canal). The size of the opening varies from that which admits the passage of a finger to about 4 fingers, or may be much larger. Its shape may be round, oval, slitlike or irregular or in the form of a passage (inguinal H)

• 2- Hernial swelling:• The size varies from that of a grap to that of a
man's head or rarely much larger. The shape may be hemispherical, cylindrical or conical. It comprises of two parts:
• a. Hernial sac: it encloses the hernial contents and is formed of skin, perhaps some few muscular fibres, fibrous tissue and the parietal layer of the peritoneum and the later may be absent, if it is ruptured by the causal agent. The sac has a neck, body and a fundus.

• The neck is the nearest portion to the abdominal wall, the fundus is the lowest part and the body is the intervening region. The inner surface is smooth and thus greatly favours the passage of the abdominal viscera into the cavity and it throwns into folds at its neck

• b. Hernial contents: these usually comprise a loop of the bowel with its ingensta and mesentric attachment (enterocele), or omentum (epiplocele) or both (entero-epiplocele) or rarely the stomach (gastrocele) or bladder (vesciocele)

Fig.2: Umbilical hernias in Fig.2: Umbilical hernias in buffalo calf (A) and cow buffalo calf (A) and cow calf (B) and closure of the calf (B) and closure of the hernial ring by a series of hernial ring by a series of interrupted horizontal interrupted horizontal mattress sutures using of mattress sutures using of Polyglycolic acid (C) . Polyglycolic acid (C) .

Fig.3: Umbilical hernia Fig.3: Umbilical hernia in foal (A), after in foal (A), after dissection and freeing of dissection and freeing of the hernial sac 1cm the hernial sac 1cm peripheral to the hernial peripheral to the hernial ring (B). Herniorrhaphy ring (B). Herniorrhaphy was obtained by a series was obtained by a series of interrupted horizontal of interrupted horizontal mattress sutures using of mattress sutures using of silk (C) .silk (C) .

Fig.9: Umbilical hernias in buffalo calf (A) and cow calves (B&C) and closure of the hernial ring by a series of interrupted horizontal mattress sutures using of silk (D) .

Fig.4: Large umbilical hernia repaired with a hernial tape.

Types of hernia:
• hernia is classified as follows
• 1. According to their situation: e.g. umbilical H. (omphalocele or exomphalos), inguinal H. (bubonocele), scrotal H. (oscheocele), or ventral H., femoral H. and perineal hernia.

• 2. According to the nature of the hernial contents: e.g. that containing the bowel with the mesentry (enterocele), omentum (epiplocele) and bladder (vesicocele).

• 3. According to the condition of the hernial contents:
• This may be: 1. Reducible or mobile hernia (more common)
• In which the hernial contents can be returned to the abdominal cavity through the hernial ring.

• 2. Irreducible hernia: in which the contents can not be returned to their normal location. It comprises three types:-
• A- Incarcerated hernia: is one in which the passage of the ingesta through the protruding loop of intestine is arrested. The blood flow in its wall, however is maintained

• B- Strangulated hernia: is one in which both irreducible and incarcerated and in which the blood circulation is also arrested and the lumen of the bowel is obstructed resulting in gangrene within 24 hours unless speedy relief is afforded..
• C- Hernia with adhesion: inflammatory adhesions may have united the contents to the lining of the sac. They prevent the complete reduction of the hernia and may cause strangulation by constricting the bowel.

• Aetiology: I- Predisposing causes:• 1- Congenital or herditary as umbilical and
inguinal hernias . • 2- Weak abdominal wall e.g. imperfect occlusion
of the umbilicus.• 3- Deep wounds, contusions and abscesses.• 4- Increased intra-abdominal pressure e.g.
straining from constipation or diarrhoea or parturition, fits of coughing or intestinal tympany.

II. Exciting causes:
• 1- Mainly increased intra-abdominal pressure with rupture of the rigid muscles tends to force the viscera via weak points in the abdminal wall.
• 2- Violent impact against a blunt object with rupture of the muscle while the skin is intact.

• Symptoms Physical symptoms• 1- It is due to the presence of hernial swelling
which varies in shape and size.• 2- In enterocele, it is elastic and in epiplocele it is
doughy to feel; manipulation of the former may produce a gurgling sound.
• 3- If the herniated portion of the intestine is distended with gses, it will be tympanic on percussion and if it is containing a quantity of fluid it will fluctuate on palpation.

• 4- In entero-epiplocele there is a combination of the foregoing characters.
• 5- In the vast majority of cases, gentle pressure on the protruding swelling will reduce the hernia, allowing identification of the hernial ring, which should be assessed for size, shape and rigidity. Reduction of the bowel is more easily and sudden than the reduction of other organs.

• 6- Incarcerated hernias present as tense, painful swelling which are usually irreducible occasionally gas in the entrapped. Intestine may have been dispersed during transport to a surgical facility or by gentle pressure allowing reduction to be achieved

• Umbilical hernia 'omphalocele- exomphalos'
• Definition: an umbilical hernia is that one which its hernial ring is formed by the umbilicus.

• Occurrence: it occurs in all animals .
• Aetiology: the condition may either congenital due to failure of abdominal wall to close or develop at 3-4 weeks of age. Excessive straining to defecate or micturate and infection of the umbilicus may be causative factor

Symptoms
• An umbilical hernia usually shows an oval localized soft not painful compressible and mostly reducible swelling vary in size from one to several centimeters in diameter. At the depth of the hernia one can easily detect the hernial ring which is passable for 2-3 fingers.
• Course: the majority of small hernias close spontaneously as the animal get older; and it has customary to wait until the animal is 6-12 months old before attempting surgery. Large defects show little tendency to spontaneous closure.

Fig.3: Umbilical hernia in Fig.3: Umbilical hernia in foal (A), after dissection foal (A), after dissection and freeing of the hernial and freeing of the hernial sac 1cm peripheral to the sac 1cm peripheral to the hernial ring (B). hernial ring (B). Herniorrhaphy was Herniorrhaphy was obtained by a series of obtained by a series of interrupted horizontal interrupted horizontal mattress sutures using of mattress sutures using of silk (C) .silk (C) .

• Diagnosis: hernia may confuse with an abscess at the navel, confirmation is done through an exploratory puncture, the presence of the hernial ring and reducibility. It must be differntiated also from the tumours in the region of the umbilicus and urachal cysts as the forementioned abscess formation in the said region by the exploratoy puncture.

Ventral hernia
• A ventral hernia is one that occurs through any part of the abdominal wall other than the umbilical or inguinal canal.
• Aetiology: they may be traumatic in origin or incisional kicks, collisions with blunt objects and straddling gates are common cause
• It may develop from rupture of the abdominal muscles e.g. the rectus abdominis as may happen in cases of advanced pregnancy

• Occasionally the abdominal wall may be so weakaned by an abscess that, following its evacuation, a hernia froms. This fact must be taken into consideration when opening abdominal wall's abscesses. Here the hernial sac consists only of the skin and parts of the subcutis since to peritoneum is usually ruptured together the musculature

• In recent lesions there is a swelling often covered by a haematoma. The hernial ring is often not palpable until after regression of the haematoma and tissue reaction caused by the trauma.
• In small hernias, the hernial contents usually consist of omentum or intestine but a large tear will allow a large mass of viscera (e.g. large colon) to escape from the abdomen, but the size of the swelling is not necessarily an indication of the size of the defect because a considerable length of small intestine can escape through a small rent

• When the acute symptoms have disappeared, it is usually possible to palpate the hernial ring as a slit or very often as a tear with irregular edges (diagnostic).
• Size: Varies from that of a fist to a man's head and may be larger.


Diagnosis
• Is confirmed as soon as the hernial ring has been found, the ability to reduce the hernial parts further confirms the diagnosis (Reducibility). Sometimes adhesion between the sac and the contents of the hernia may interfere with the process of reduction of the later. In doubtful cases it may be necessary to carry out an exploratory puncture with a fine bore trocar under aseptic precautions.
• In may cases, rectal examination may also be of great value. It must be remembered that haematoma and abscesses may cover and completely mask a traumatic ventral hernia.

Treatment
• The aim of treatment is to replace and then to ensure retention of the hernial contents. In dogs and cats, it is ensured with the use of a bandage. In cattle and horses, this is done by a gauze pressure-cushion which is fixed in position with a purse string suture placed as deeply in the tissue as possible.

• In both small and large animals operative interference is contra-indicated between the first to the tenth day of development of the hernia when the hernia is not accompanied by signs of intestinal obstruction, it is advisable to delay surgery for 3-6 weeks until some swelling has subsided and deposition of collagen has increased the tensile strength of the damaged tissues as one cannot expect sutures to hold in the infiltrated tissues surrounding it

• The rent in the abdominal wall is closed by overlapping the edges with a heavy suture material and the technique is same as described for umbilical hernia. Interrupted sutures can be placed between the overlapping sutures for reinforcement.

• When the defect is very large or its edges are too rigid to appose by suture, satisfactory repair may be achieved using mesh. Following closure of the peritoneum and transverse muscle by suture, a piece of polypropylene mesh is sutured to the deep face of the internal oblique aponeurosis.

• N.B. When the hernia is apparently harmless, herniorrhaphy is elective and not an emergency operations while signs of depression, abdominal discomfort and cessation of defecation indicate intestinal obstruction requiring prompt intervention.
• Postoperative management: the amount of feed should be reduced to half for about a week after surgery. A supportive bandage may be placed around the abdomen to relieve tension on the healing tissue