49 abdominal hernias
40
49 Abdominal Hernias
-
Upload
muhammad-bin-zulfiqar -
Category
Education
-
view
48 -
download
2
Transcript of 49 abdominal hernias

49 Abdominal Hernias

CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
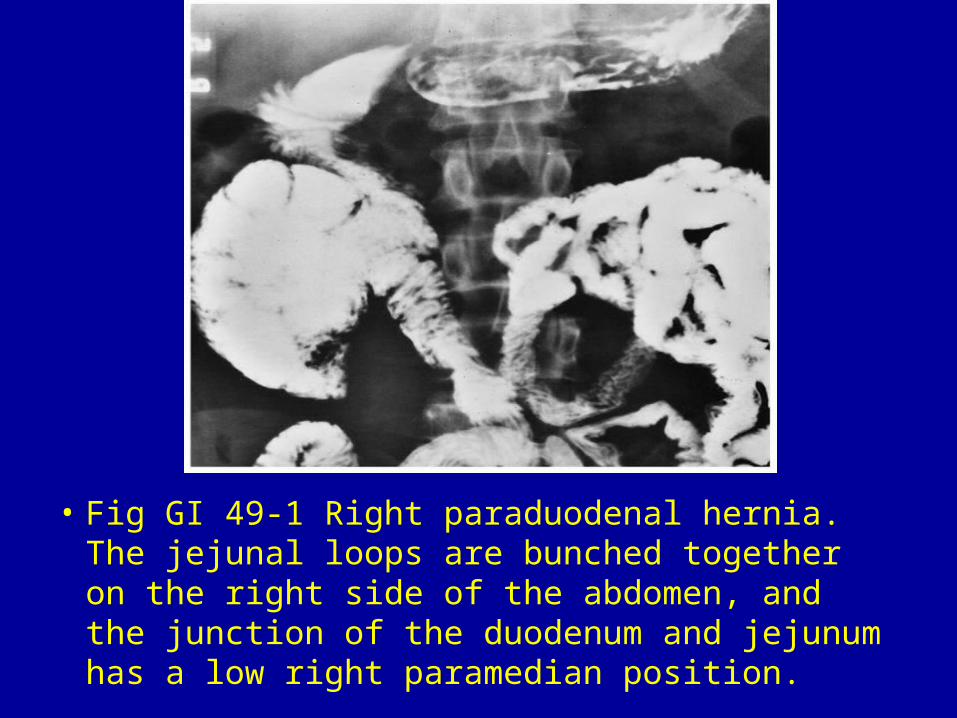
• Fig GI 49-1 Right paraduodenal hernia. The jejunal loops are bunched together on the right side of the abdomen, and the junction of the duodenum and jejunum has a low right paramedian position.
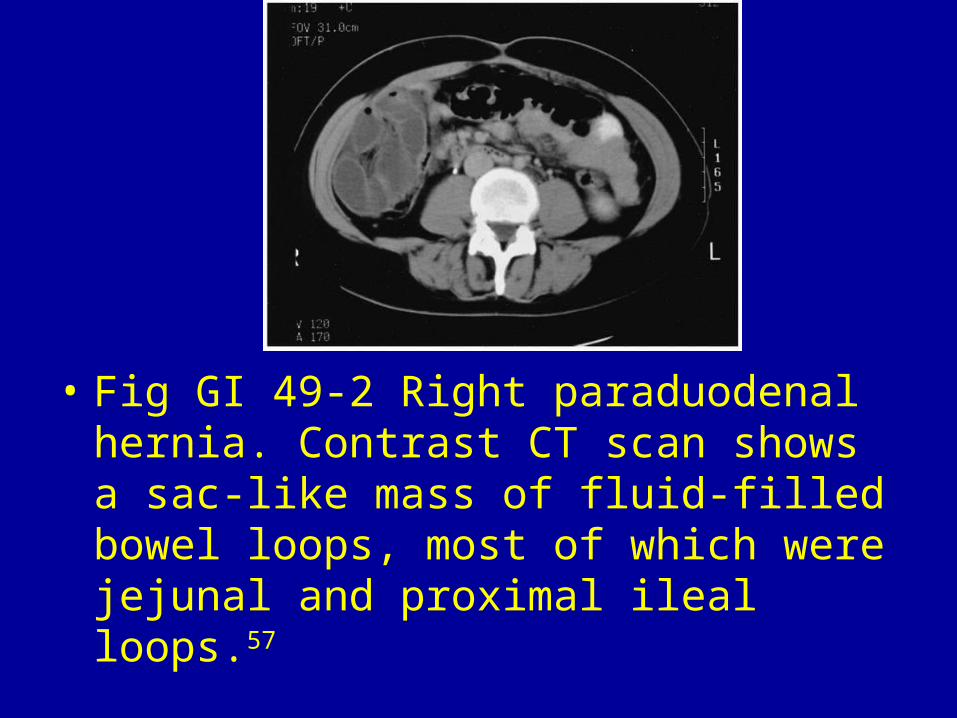
• Fig GI 49-2 Right paraduodenal hernia. Contrast CT scan shows a sac-like mass of fluid-filled bowel loops, most of which were jejunal and proximal ileal loops.57

• Fig GI 49-3 Left paraduodenal hernia. Small bowel loops are clustered in the left upper quadrant lateral to the fourth portion of the duodenum and stomach.
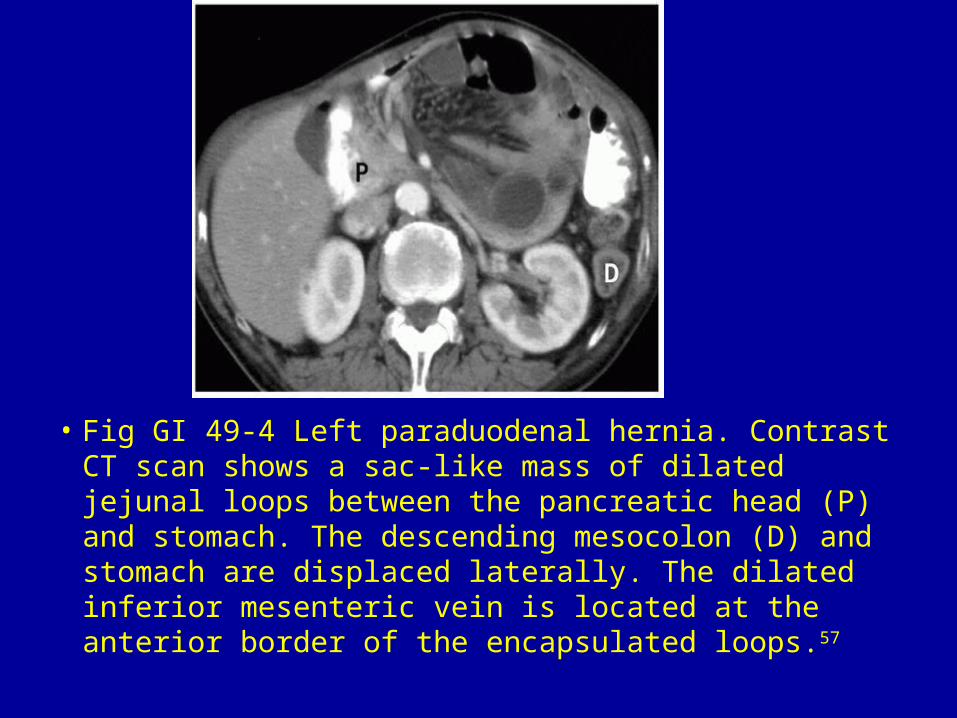
• Fig GI 49-4 Left paraduodenal hernia. Contrast CT scan shows a sac-like mass of dilated jejunal loops between the pancreatic head (P) and stomach. The descending mesocolon (D) and stomach are displaced laterally. The dilated inferior mesenteric vein is located at the anterior border of the encapsulated loops.57
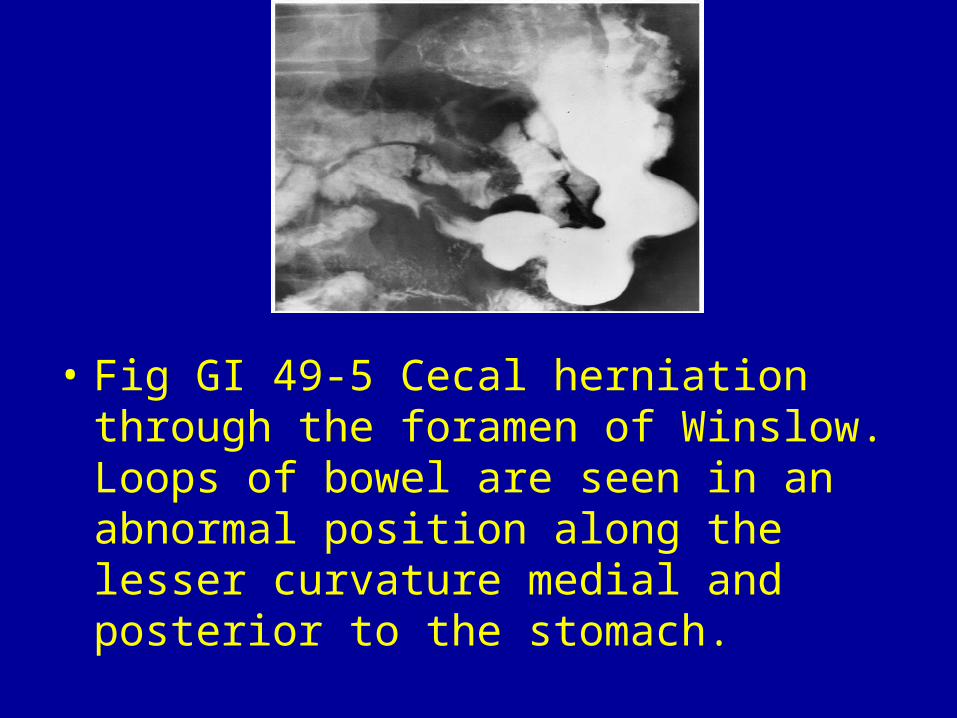
• Fig GI 49-5 Cecal herniation through the foramen of Winslow. Loops of bowel are seen in an abnormal position along the lesser curvature medial and posterior to the stomach.
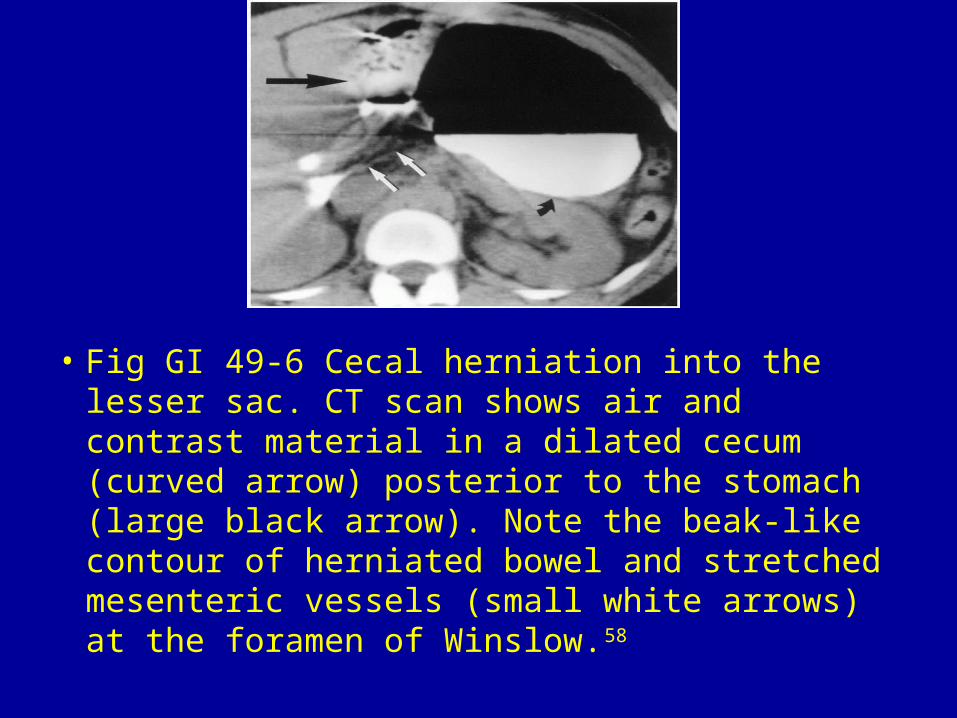
• Fig GI 49-6 Cecal herniation into the lesser sac. CT scan shows air and contrast material in a dilated cecum (curved arrow) posterior to the stomach (large black arrow). Note the beak-like contour of herniated bowel and stretched mesenteric vessels (small white arrows) at the foramen of Winslow.58

• Fig GI 49-7 Lesser sac hernia. CT scan shows a cluster of dilated small bowel loops (arrowheads) in the lesser sac. There are stretched and converging mesenteric vessels (arrow) between the portal vein in the hepatoduodenal ligament (H) and the inferior vena cava (I).57
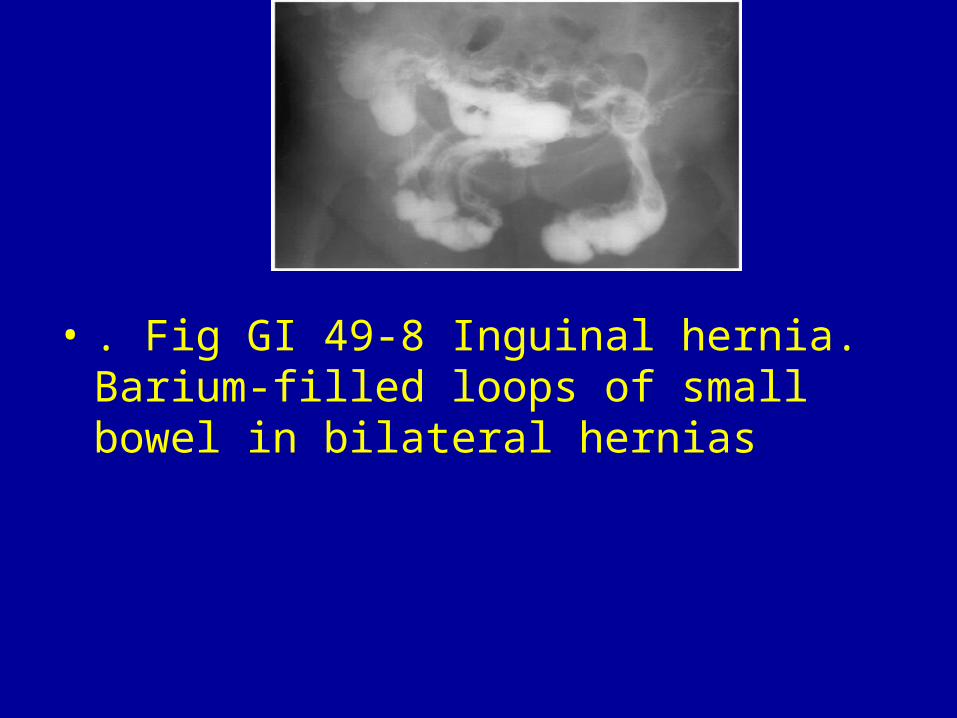
• . Fig GI 49-8 Inguinal hernia. Barium-filled loops of small bowel in bilateral hernias
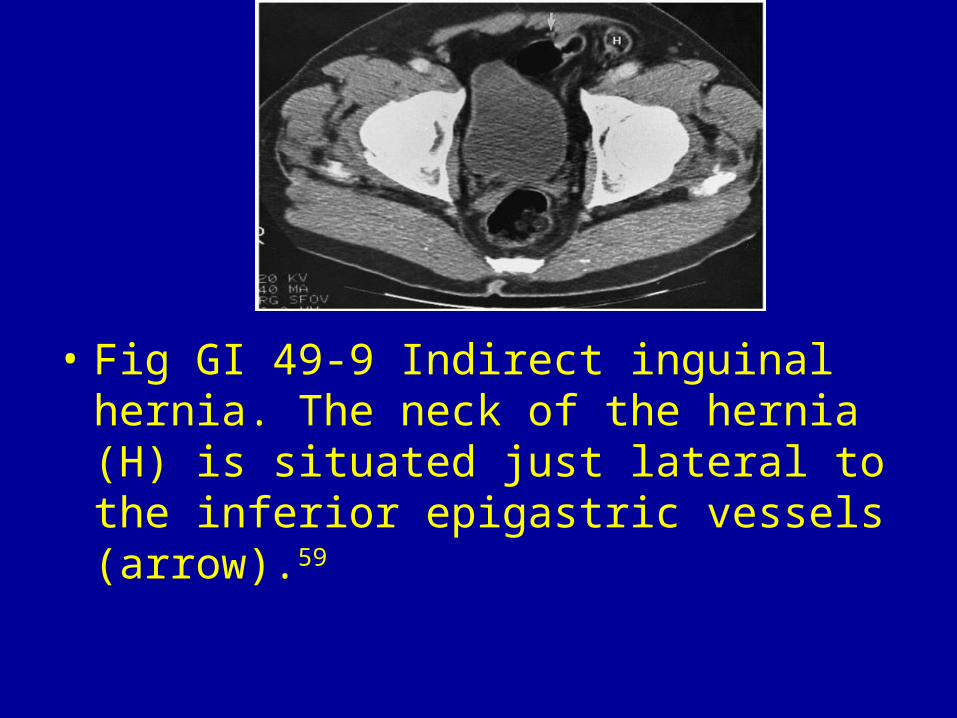
• Fig GI 49-9 Indirect inguinal hernia. The neck of the hernia (H) is situated just lateral to the inferior epigastric vessels (arrow).59
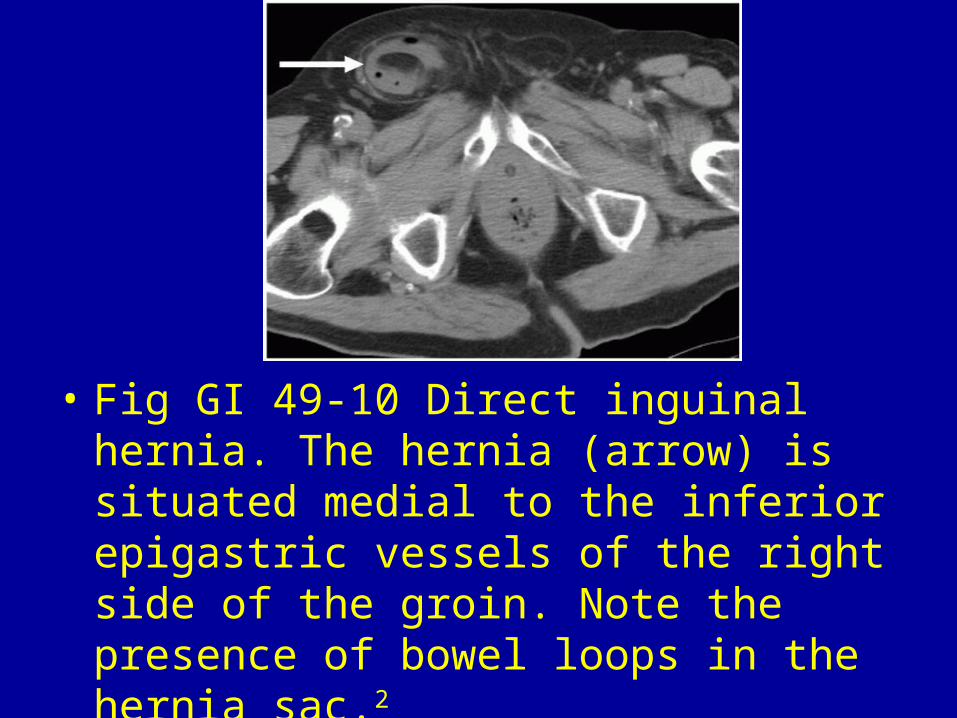
• Fig GI 49-10 Direct inguinal hernia. The hernia (arrow) is situated medial to the inferior epigastric vessels of the right side of the groin. Note the presence of bowel loops in the hernia sac.2
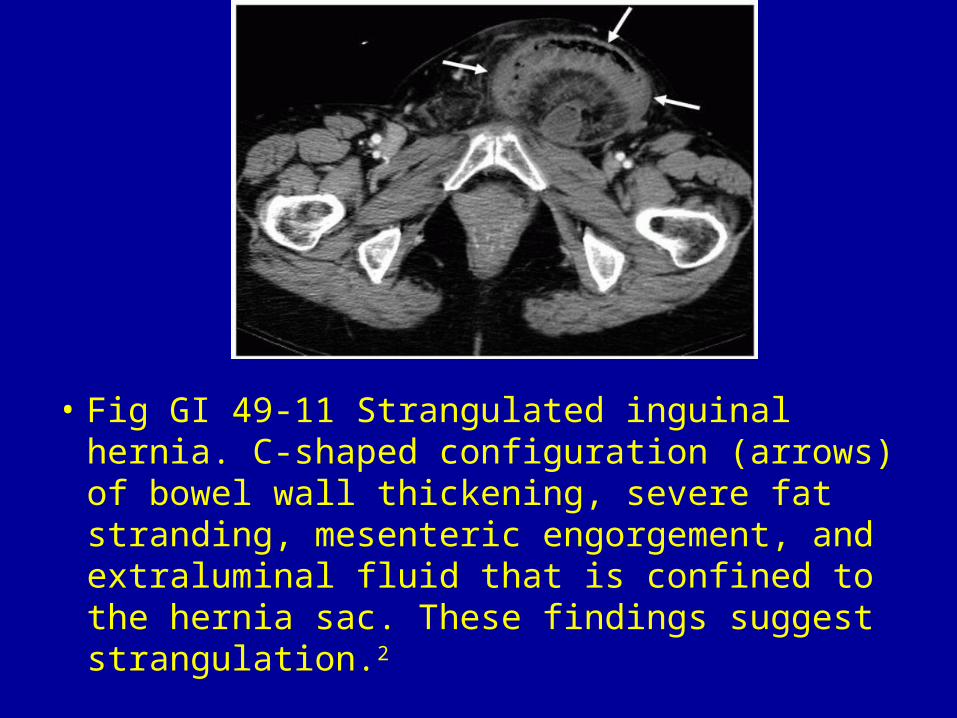
• Fig GI 49-11 Strangulated inguinal hernia. C-shaped configuration (arrows) of bowel wall thickening, severe fat stranding, mesenteric engorgement, and extraluminal fluid that is confined to the hernia sac. These findings suggest strangulation.2
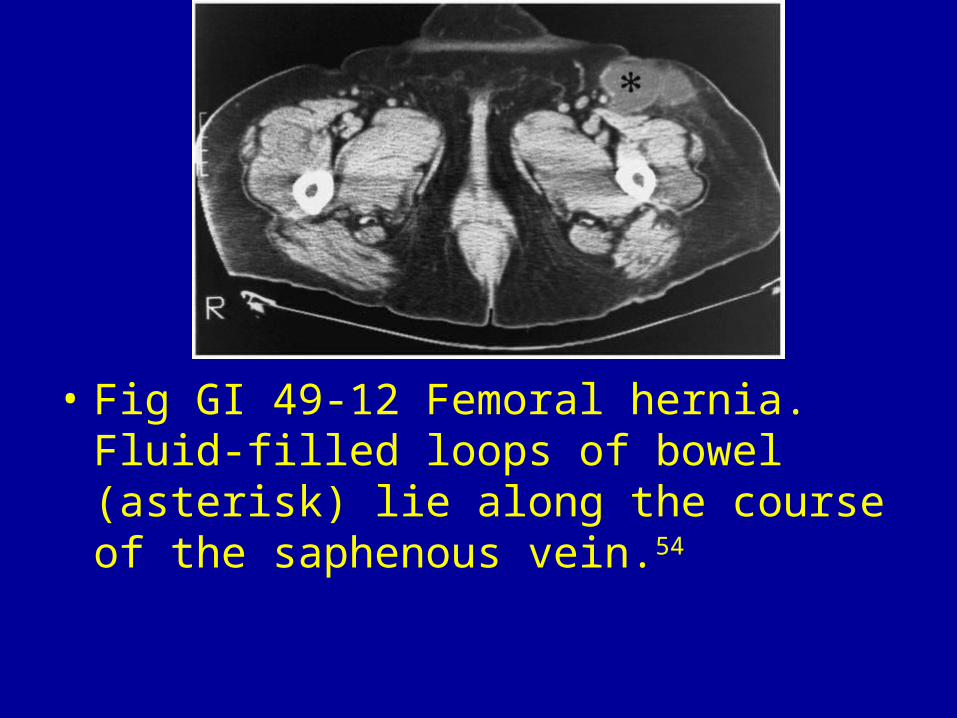
• Fig GI 49-12 Femoral hernia. Fluid-filled loops of bowel (asterisk) lie along the course of the saphenous vein.54
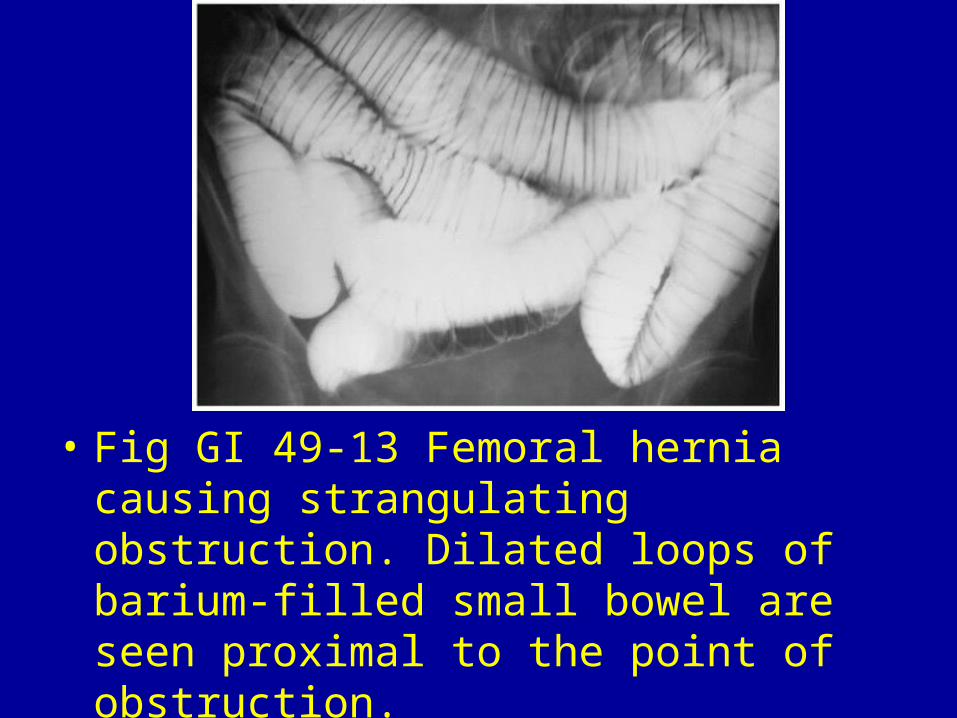
• Fig GI 49-13 Femoral hernia causing strangulating obstruction. Dilated loops of barium-filled small bowel are seen proximal to the point of obstruction.

• Fig GI 49-14 Obturator hernia containing sigmoid colon.
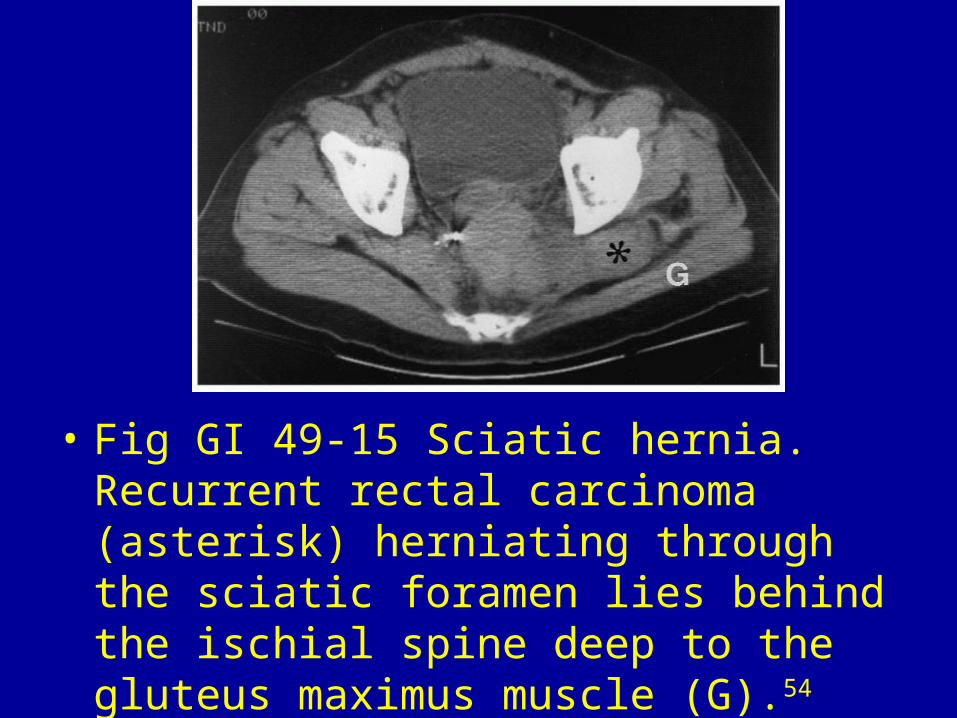
• Fig GI 49-15 Sciatic hernia. Recurrent rectal carcinoma (asterisk) herniating through the sciatic foramen lies behind the ischial spine deep to the gluteus maximus muscle (G).54
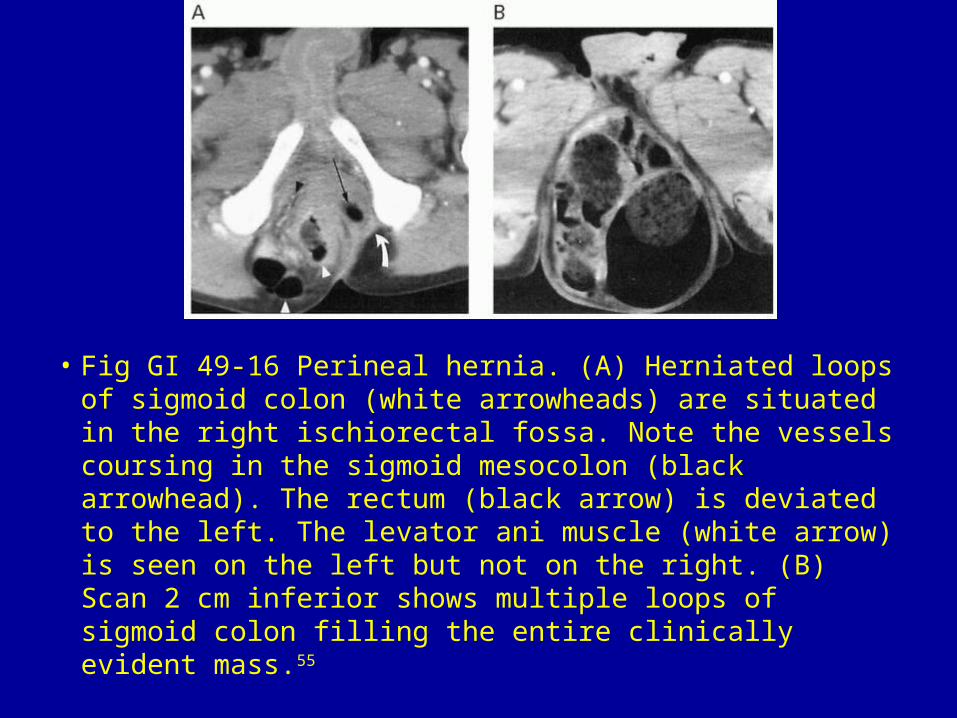
• Fig GI 49-16 Perineal hernia. (A) Herniated loops of sigmoid colon (white arrowheads) are situated in the right ischiorectal fossa. Note the vessels coursing in the sigmoid mesocolon (black arrowhead). The rectum (black arrow) is deviated to the left. The levator ani muscle (white arrow) is seen on the left but not on the right. (B) Scan 2 cm inferior shows multiple loops of sigmoid colon filling the entire clinically evident mass.55
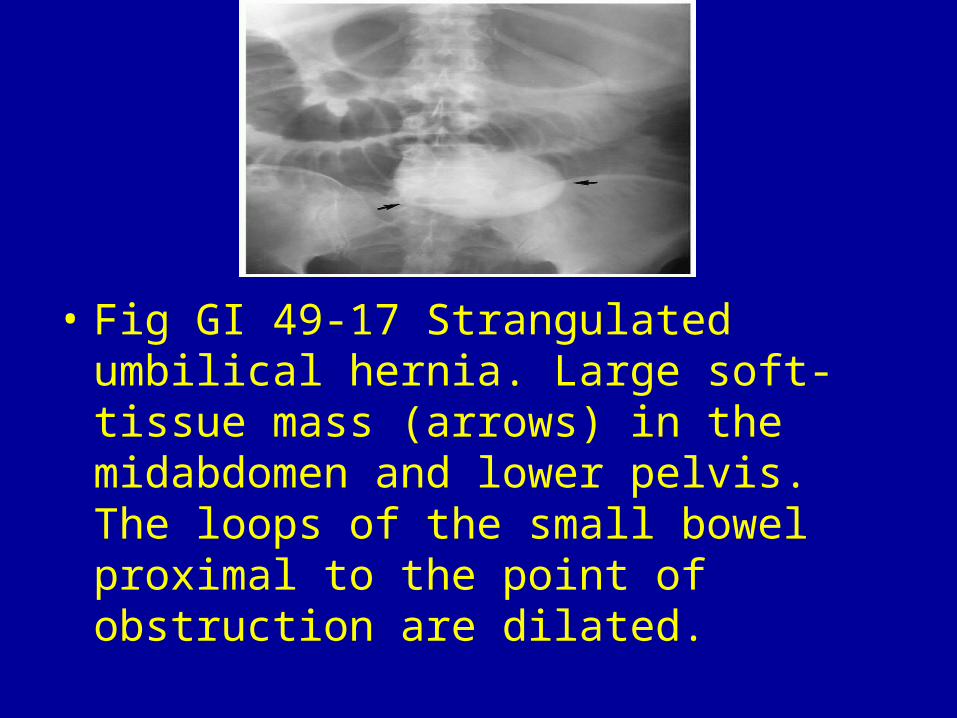
• Fig GI 49-17 Strangulated umbilical hernia. Large soft-tissue mass (arrows) in the midabdomen and lower pelvis. The loops of the small bowel proximal to the point of obstruction are dilated.
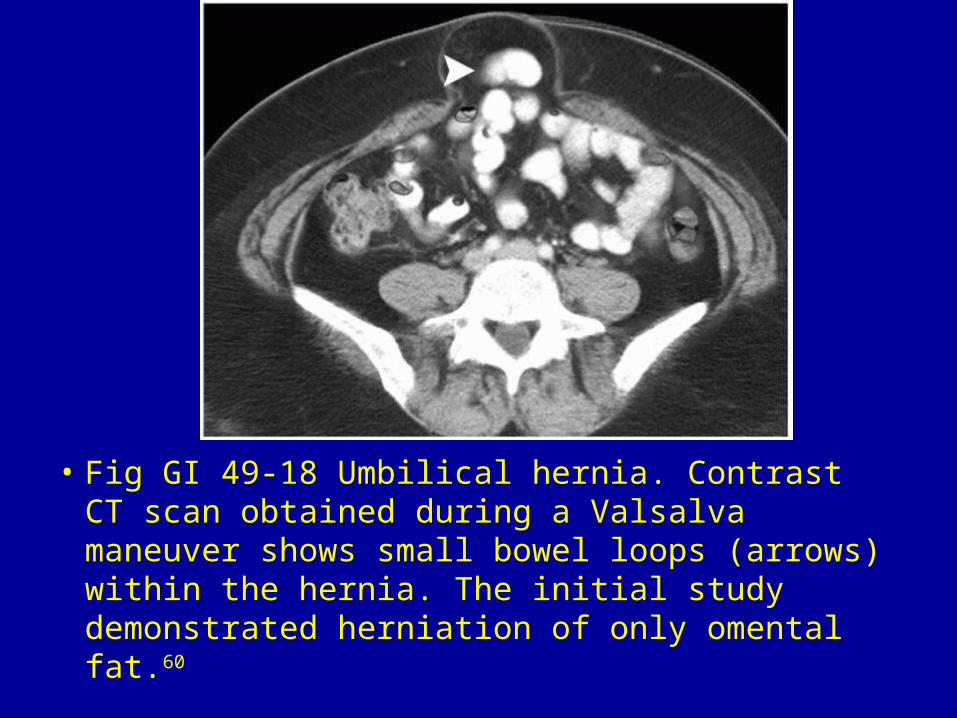
• Fig GI 49-18 Umbilical hernia. Contrast CT scan obtained during a Valsalva maneuver shows small bowel loops (arrows) within the hernia. The initial study demonstrated herniation of only omental fat.60
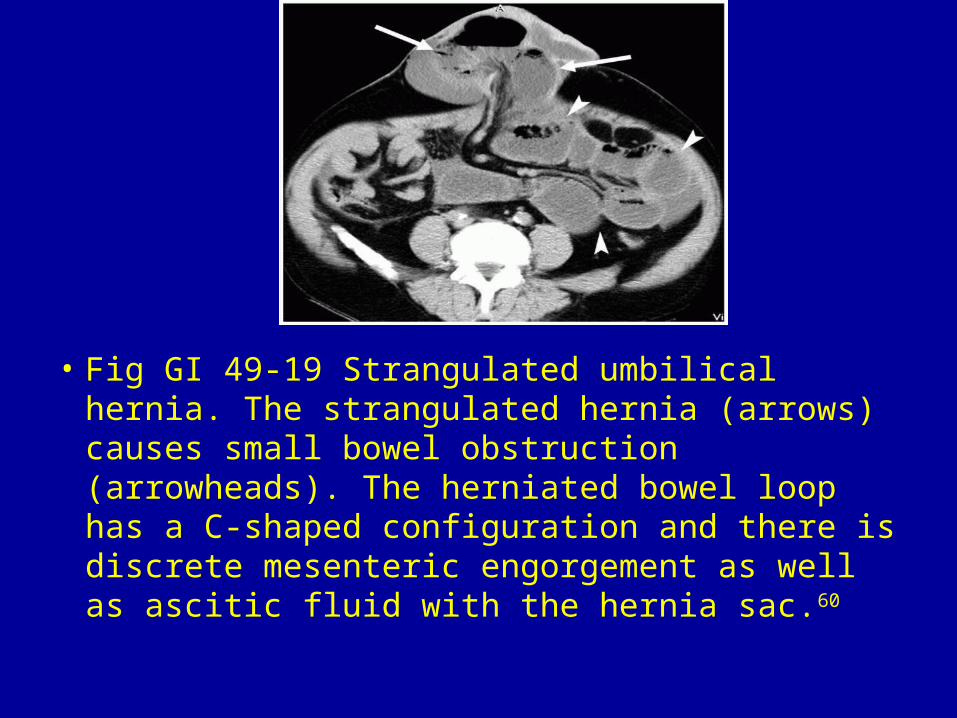
• Fig GI 49-19 Strangulated umbilical hernia. The strangulated hernia (arrows) causes small bowel obstruction (arrowheads). The herniated bowel loop has a C-shaped configuration and there is discrete mesenteric engorgement as well as ascitic fluid with the hernia sac.60

• Fig GI 49-20 Epigastric hernia. The hernia (arrows) contains the transverse colon and small bowel loops. Note also the interparietal hernia through the right lateral aspect of the abdominal wall (arrowhead) containing the hepatic flexure of the colon.60

• Fig GI 49-21 Obstructed incisional hernia. Dilated loops of bowel (B) extend into the abdominal wall through a defect in the region of the linea semilunaris (arrows). This was the site of a previous surgical incision.59
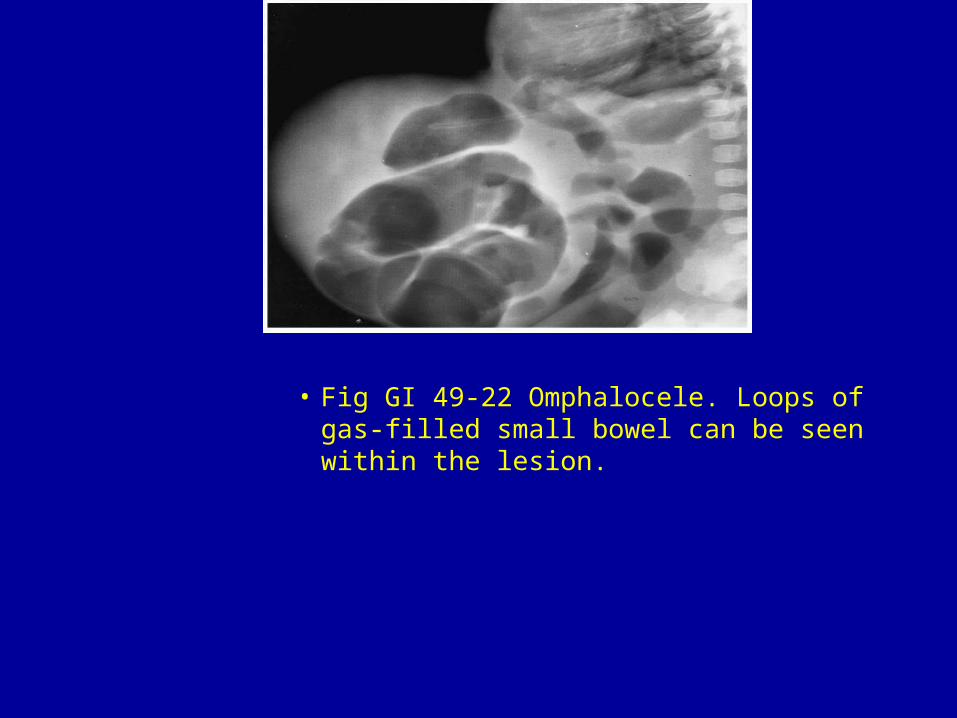
• Fig GI 49-22 Omphalocele. Loops of gas-filled small bowel can be seen within the lesion.

• Fig GI 49-23 Spigelian hernia. Small bowel is trapped in the hernia sac (arrow), which arises along the left semilunar line.

• Fig GI 49-24 Spigelian hernia. Herniation of fat through a defect in the aponeurosis between the left rectus abdominis (curved arrow) and the aponeurosis of the left transversus abdominis and internal oblique muscles. The lateral margin of the hernia sac is the external oblique muscle and fascia (straight arrow).61

• Fig GI 49-25 Lumbar hernia through the superior triangle. Note the multiple bony anomalies.
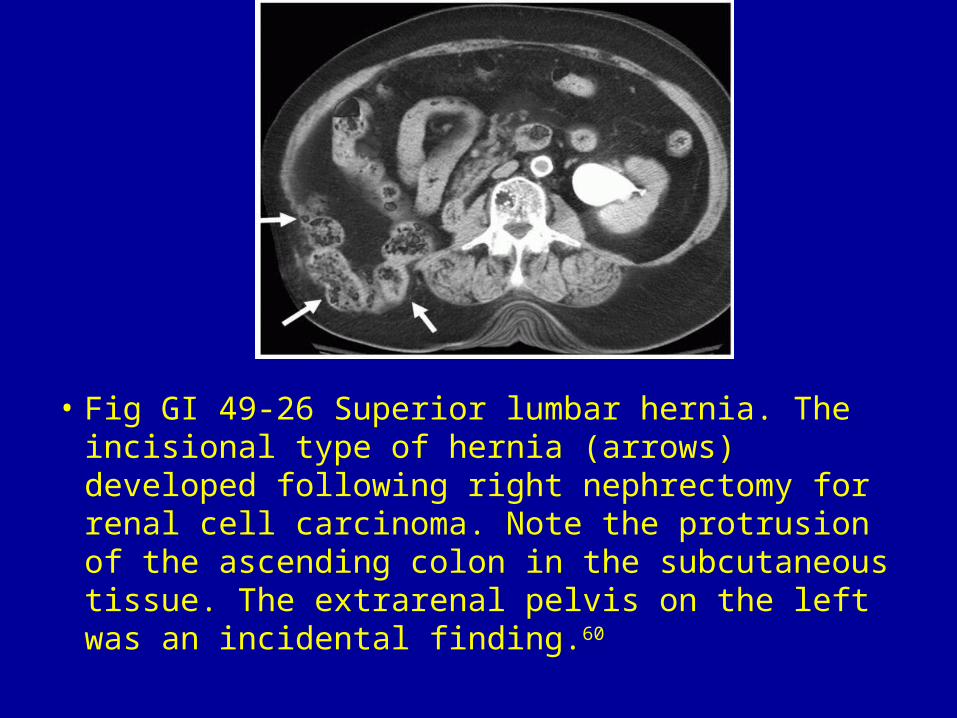
• Fig GI 49-26 Superior lumbar hernia. The incisional type of hernia (arrows) developed following right nephrectomy for renal cell carcinoma. Note the protrusion of the ascending colon in the subcutaneous tissue. The extrarenal pelvis on the left was an incidental finding.60
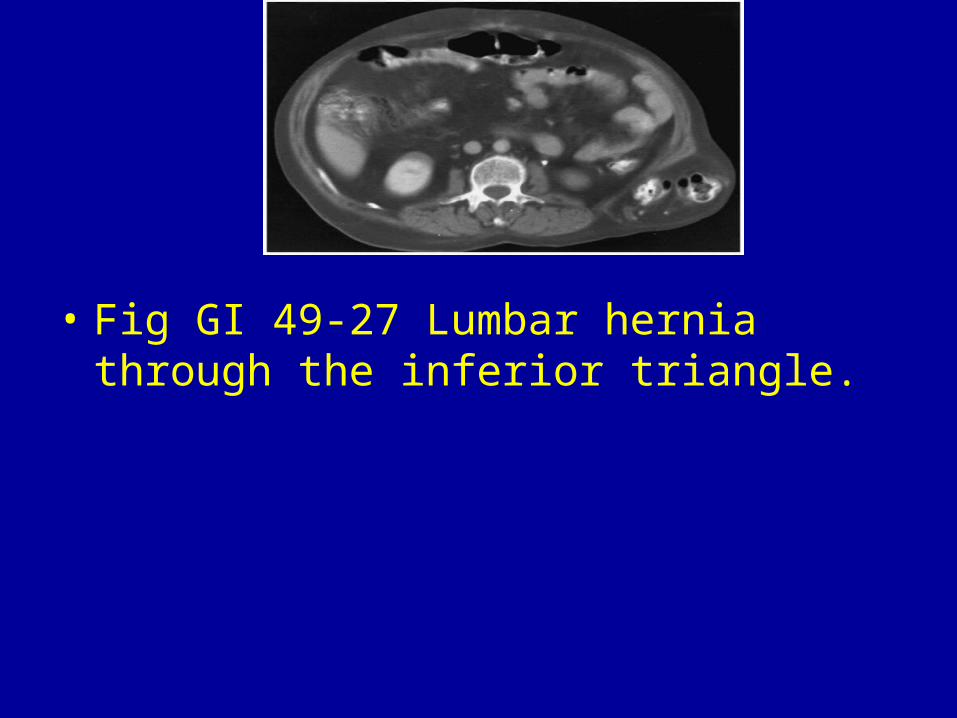
• Fig GI 49-27 Lumbar hernia through the inferior triangle.
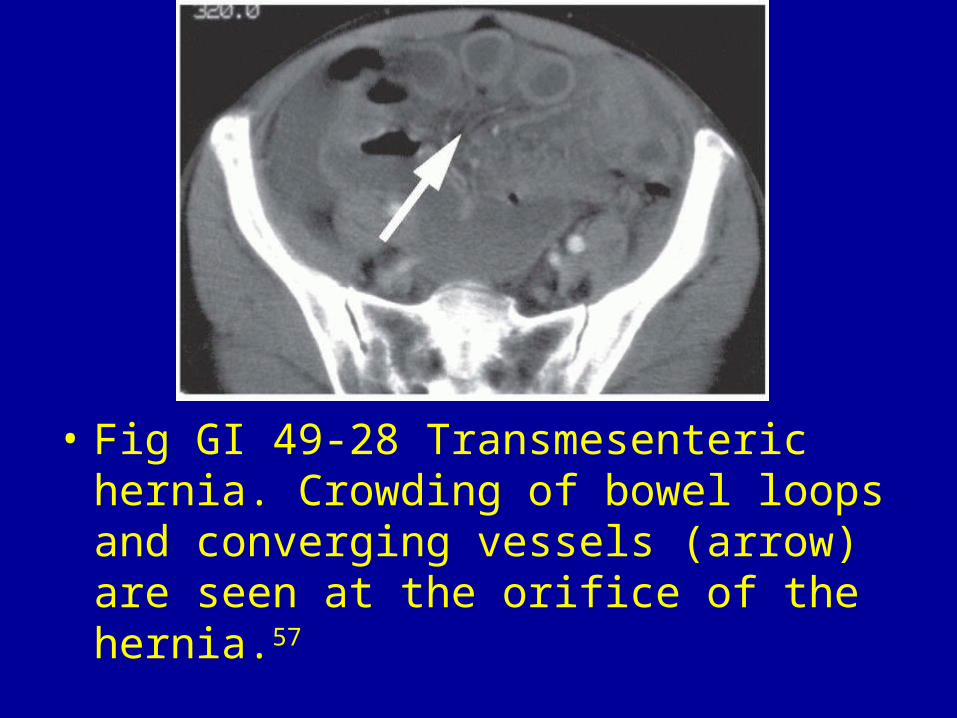
• Fig GI 49-28 Transmesenteric hernia. Crowding of bowel loops and converging vessels (arrow) are seen at the orifice of the hernia.57
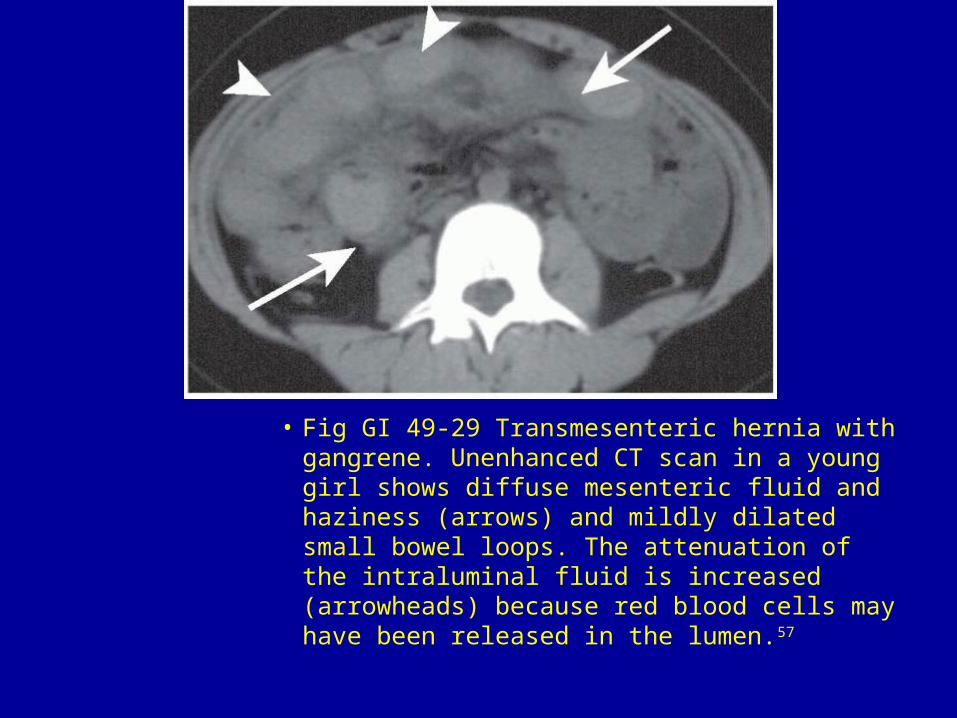
• Fig GI 49-29 Transmesenteric hernia with gangrene. Unenhanced CT scan in a young girl shows diffuse mesenteric fluid and haziness (arrows) and mildly dilated small bowel loops. The attenuation of the intraluminal fluid is increased (arrowheads) because red blood cells may have been released in the lumen.57

• Fig GI 49-30 Transomental hernia. Contrast CT of the pelvis shows a cluster of fluid-filled small bowel loops (arrowheads) with poor or absent enhancement of bowel walls adjacent to the mid-abdominal wall. The mesenteric vascular pedicle (arrow), which is crowded and engorged with vessels, is seen at the orifice of the hernia.57
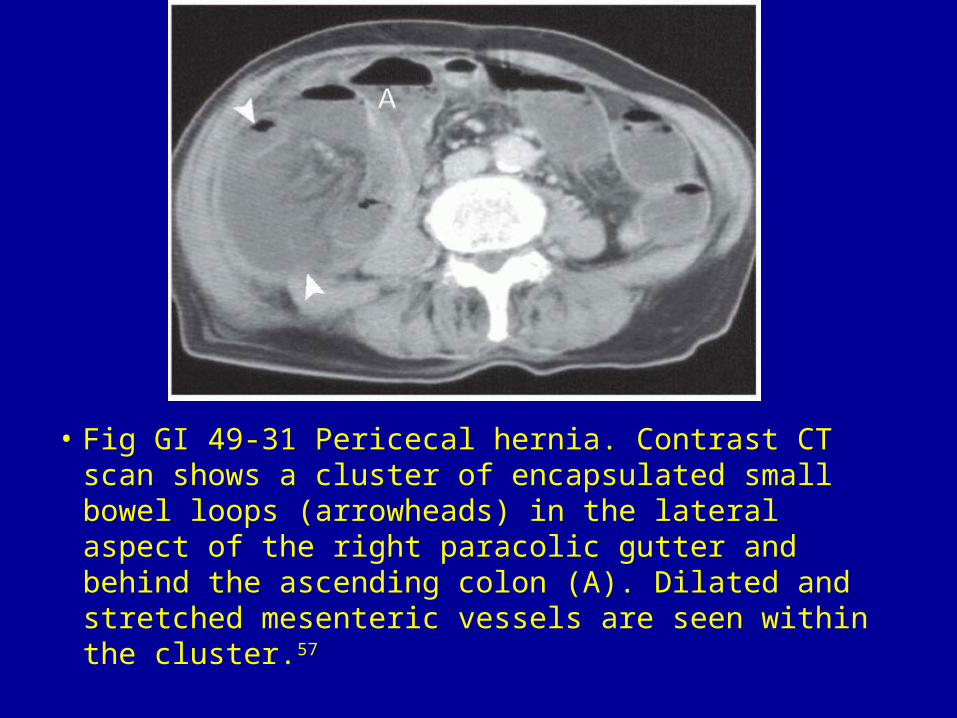
• Fig GI 49-31 Pericecal hernia. Contrast CT scan shows a cluster of encapsulated small bowel loops (arrowheads) in the lateral aspect of the right paracolic gutter and behind the ascending colon (A). Dilated and stretched mesenteric vessels are seen within the cluster.57
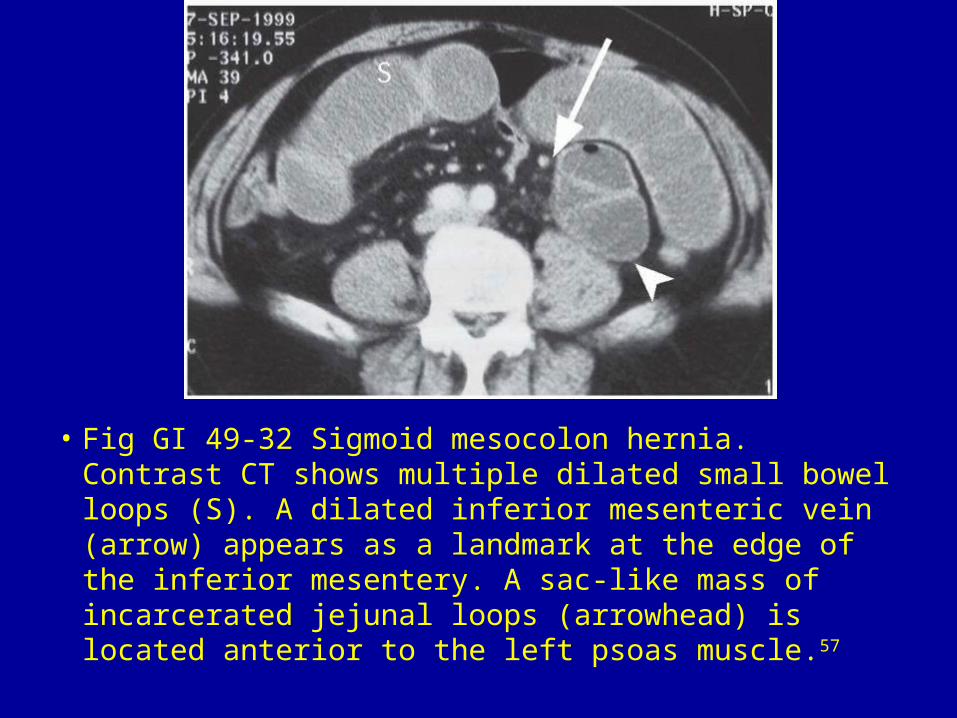
• Fig GI 49-32 Sigmoid mesocolon hernia. Contrast CT shows multiple dilated small bowel loops (S). A dilated inferior mesenteric vein (arrow) appears as a landmark at the edge of the inferior mesentery. A sac-like mass of incarcerated jejunal loops (arrowhead) is located anterior to the left psoas muscle.57
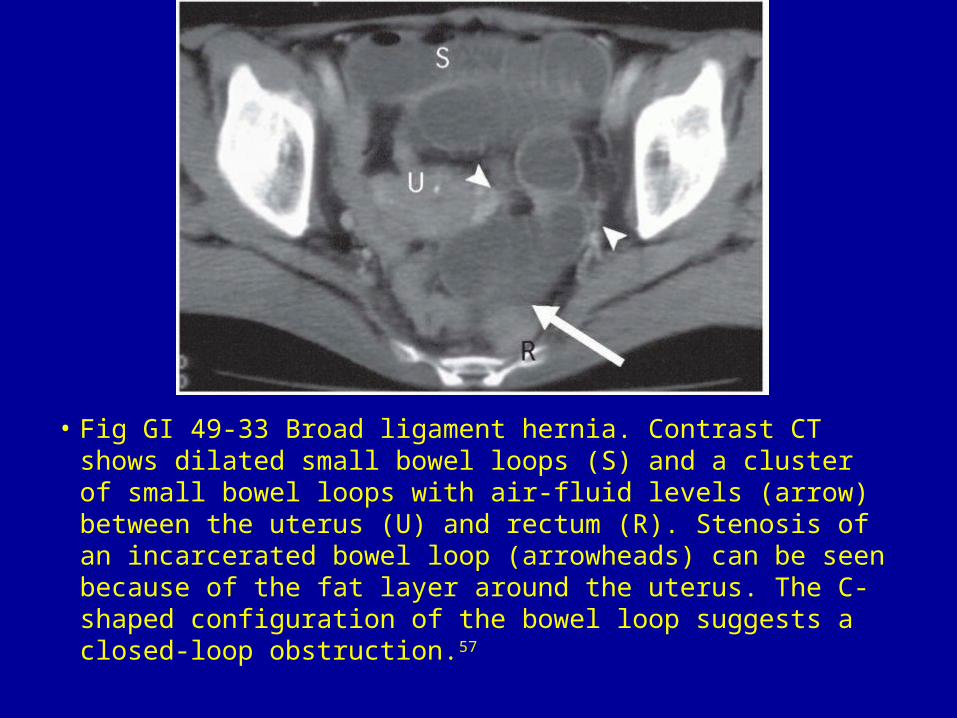
• Fig GI 49-33 Broad ligament hernia. Contrast CT shows dilated small bowel loops (S) and a cluster of small bowel loops with air-fluid levels (arrow) between the uterus (U) and rectum (R). Stenosis of an incarcerated bowel loop (arrowheads) can be seen because of the fat layer around the uterus. The C-shaped configuration of the bowel loop suggests a closed-loop obstruction.57

• Fig GI 49-34 Perirectal hernia. Contrast CT scan shows dilated and fluid-filled small bowel loops (S). A cluster of dilated bowel loops (arrow) is located to the right of the rectum (R) and behind the uterine cervix (U).57